Feelings are not supposed to be logical. Dangerous is the man who has rationalized his emotions.
~ David Borenstein
“Waaaaa!” cries the baby in a vociferous protest, only to take a deep breath in order to begin again, louder and with more determination, “Waaaaaaaaa!”
Is this baby being rude and disrespectful because the parent is on an important phone call and cannot be interrupted? Of course not.
This baby is communicating that he* is in a state of stress; he is voicing his needs. He is unequipped to self-regulate, and he is unable to calm his own nervous system down. He does not have the ability to self-regulate and he is acting from an instinctual place to communicate his need for nurturing, food, or some other unmet need. In other words, this baby is unaware of anybody else’s agenda. He cares nothing about his parent’s important phone call; he refuses to be quiet even when his parent whispers “shhhhhh”; and he is demanding that his needs be met.
Does this sound familiar to how a student with difficult behaviors is often described in the classroom?
“Billy is selfish, disregards the classroom rules, interrupts the teacher when she is teaching an important lesson, refuses to stop talking even when reminded to settle down, disrupts the other children, and pays no attention to the feelings of his peers.”
Billy and the crying baby are more alike than what we have been able to realize in the past. Both children are “dysregulated” and both children are acting in the only way they know how in order to return back to being “regulated.” Each is seeking to find happiness and peace in this world but is grossly ill-equipped to know how to do this with polite manners. Each needs the help, guidance, and nurturing of a regulated adult to move back to a state of calm and peace.
Hyper- and Hypo-arousal. The crying of the baby and the behavior of Billy described above are examples of how children respond to stressful situations. These negative behaviors are natural human stress responses.
When children (as well as adults) become overly distressed, they react from a place of fight or flight. The fight response puts a child into a “hyper-aroused” state; conversely, the flight response puts a child into a “hypo-aroused” state. Definitions of these terms follow, and the corresponding behaviors for each are shown in Table 2.1.
Hyper-arousal is an increase in psychological and physiological tension, manifested by a reduction in pain tolerance, increased anxiety, exaggeration of startle responses, insomnia, panic, rage, and an accentuation of personality traits.
Hypo-arousal is the decrease in psychological and physiological tension marked by such effects as emotional indifference, flattened affect, irritability, low-grade nervousness, disengagement, depression, and hopelessness.
Table 2.1. Behaviors associated with hyper-arousal and hypo-arousal
The “Good” Child vs. the “Bad” Child. When a child is either hyper-aroused or hypo-aroused, he is “dysregulated.” When a child is in a balanced state, in a state of homeostasis, he is “regulated.” Some children, due to their early life experiences, live more chronically in a state of dysregulation than in a state of regulation. This is not a matter of choice or a matter of “good” child verses “bad” child; it is simply an imprint from their past histories.
To demonstrate these concepts, let me introduce two children we will be following throughout this book. These two children are based on children I have worked with clinically in the past. Their histories and stories are more real than what I could fictitiously create on my own. Please give a warm welcome to Andy and Billy:
Andy: As Andy was developing as a fetus, his mother was happy to be pregnant. She wanted to be a mother and adjusted her life to take care of herself during the pregnancy. She took her prenatal vitamins, ate well, and exercised. She decreased the stress in her life and had a supportive spouse who took care of and supported her. Andy reached full term and had a noneventful, easy delivery and was healthy when born. His mother breast-fed him, and both his mother and father cared for him around the clock. When he cried, he was soothed and nurtured. He stayed home for the first three years of his life under the care of one of either of his parents and never attended day care. He was gradually introduced to the school environment through short days at preschool and then moved to a small kindergarten environment by age five. When challenges happened in the home, as when his grandma passed, Andy was supported, given emotional space, and encouraged to express his feelings. By age eight, Andy was thriving in third grade and was an exemplary student.
Billy: As Billy was developing as a fetus, his mom was furious about being pregnant. Her boyfriend had lied to her about not being fertile. She tried to hide her pregnancy from her family but was discovered and kicked out of her home. She had no alternative but to go live with an abusive boyfriend. Billy was delivered four weeks premature, needed immediate medical attention, and was in an Isolette for the first two weeks of his life. Upon coming home from the hospital, his mother found a new job and placed him in day care at six weeks old. His mother had difficulty keeping employment and thus they moved frequently during the first five years of his life. He had multiple caregivers during this time. When his mother was home with him, she was quite unresponsive due to being overwhelmed, stressed, and without financial or emotional support. Billy had difficulty even in kindergarten, and by age eight his experiences in the school environment were more about being disciplined and punished than about learning and creating. He was the child the teachers dreaded having in class.
In a third-grade class, we have Andy and Billy, both eight years old and both adorable-looking little boys. Yet the contrast between these two children soon becomes painfully obvious to their teacher. Andy is able to pay attention, turns in his homework, follows the rules, plays well with his peers, and is helpful to the teacher.
Then there is Billy. Billy has a difficult time sitting still, fights the homework battle at home as if his life depends on it, is disruptive and loud in class, has social skills that are grossly immature, and fails to improve when given disciplinary action. This book is devoted to answering the ultimate and comparative question in order to find Help for Billy:
“Why are Andy and Billy, two children who appear to be so similar on the surface, so drastically different at every level?”
One word is the answer to this question: trauma.
In the Beginning, There Was Trauma. No fancy EEGs, brain scans, or other specialized pediatric tests are needed to explain why Billy is different from Andy. Billy has experienced childhood trauma of the worst order; he has experienced trauma within the context of the parent-child relationship.
Trauma is defined as any event that is more overwhelming than which is ordinarily expected. Such an event puts a child in the place of feeling out of control, scared, terrified, worthless, unlovable, insecure, and even endangered. When a child is belittled, degraded, ridiculed, threatened physically, threatened to be abandoned, withheld affection, withheld care and love, or neglected emotionally or physically, trauma has occurred. Less obvious and unrecognized traumatic events occur when a child feels as if his only value lies in meeting someone else’s needs.
In Utero. When a woman is pregnant and she experiences stress, her body produces chemicals that become part of the growing fetus’s makeup. Elevated levels of the stress hormones cortisol, epinephrine, and norepinephrine are released within the mother’s body and have a negative influence over the fetus’s ability to develop optimally. These stress hormones constrict blood vessels, resulting in a reduction of oxygen to the uterus.1
One study showed that children exposed to elevated levels of cortisol in the womb may have trouble paying attention or solving problems later in life.2 Other studies continue to show that children born from stressful womb environments may be at greater risk for a variety of other stress-related pathologies and that the stress in the womb can affect a baby’s neurobehavioral development.3 If a fetus could talk to his mother, he would likely say, “Mom, you’re stressing me out!”4
This stressful in utero experience marks the initial imprint of a child’s ability to self-regulate. The effects of this nine-month experience can show up eight, ten, twelve years later for children like Billy—students who cannot sit still and are unable to pay attention in the classroom because their nervous systems were hardwired at an elevated level. It is not a case of “won’t” but “can’t” sit still.
Early Childhood Trauma. Children are vulnerable. In an optimal environment, they are not expected to experience this vulnerability until later in life when their minds and nervous systems are equipped to handle elevated levels of fear, stress, and overwhelm. Parents and caretakers are charged with the responsibility of creating environments of safety, security, and love for their children. Yet, the key phrase here is “optimal environment.” Unfortunately, we live in the “real” world, so children will often find themselves in situations that are far beyond their window of stress tolerance. Trauma is prevalent in everyday life. Not all trauma can be avoided, and there is not a child who emerges from childhood unscathed to some extent.
Childhood trauma happens at both the emotional and psychological level and it becomes defined by the child’s perception of the event. Any situation or event that leaves a child feeling overwhelmed and alone needs to be considered trauma.
In general, a stressful event is likely to become a traumatic experience if:
During the traumatic event, the impact is even greater if the child believes he is:
The last three—powerless, helpless, and hopeless—are the big three. When a child experiences one or all of the big three, he begins to believe the world is dangerous. Repeated experiences of these feelings will create, within this child, a lasting imprint from which he operates and behaves. A framework based in fear and survival becomes the child’s viewpoint of the world around him. The more frightened and helpless a child believes he is, the deeper the fear imprint, the deeper the trauma.
Table 2.2 lists various possible childhood events that can be considered traumatic. These specific events, however, do not guarantee that the child will be traumatized simply because of the event itself. It is the perception and the emotional interpretation of the event that classifies it as trauma or not. It is about the feeling of being safe or not and it is always determined by the child’s perspective—not reality.
Table 2.2. Events with the potentiality of childhood trauma
While many of these types of events occur frequently in our society, such as divorce (which is the death of a family), the way a child perceives them should never be minimized or considered “normal.”
Obviously, every child is going to experience some degree of trauma. Whether or not the trauma is going to have a lasting effect on the child depends on the how well the fundamental needs of physical safety, emotional connection, and predictability are met for the child. When children are given environments of support, love, and attention and when needs are met, the impact of traumatic experiences is minimized, and in many cases, avoided.
Bruce Perry, M.D., explains that “a confident, well-regulated adult can take a child out of a fire and have less trauma than an anxious dysregulated adult conveying fear to a child who falls off his bike.”5 An event is not traumatic for a child based on the event itself; it is traumatic based on the response to the event from the caretaker.
The Impact of Trauma. Hence, we have Andy and Billy and it is Billy for whom we need to find help. To understand both Andy and Billy, it takes understanding their histories, the nature of their relationships, and the environments in which they have lived.
Andy, when experiencing increased levels of stress (high arousal), was met with the care, love, and emotional and physical safety of his caretakers. He was calmed and thus quickly and easily returned back to a state of homeostasis and balance (calm arousal). Research shows that “the broader the range of emotions that a child experiences, the broader will be the emotional range of the self that develops.”6 By eight years old, Andy has confidence in himself and a regulatory system that is sufficient to function successfully in a classroom.
Billy, on the other hand, has not been as fortunate. He experienced chronic overarousal in utero. He was baked in cortisol before he even entered into human history. The disruptive lifestyle of his mother kept him living in a state of perpetual stress and fear, with little relief. He has an overabundance of high arousal experiences with a drastic shortage of calm arousal experiences. Billy only knows chaos and fear. This is his familiar. This is Billy’s reality and this is his normal. Research continues to show that early and prolonged trauma in childhood affects an individual’s ability and capacity to self-regulate.
To compare Billy to Andy or to expect Billy to act like Andy is not only unfair, it is judgmental. Unconditional love is about accepting someone perfectly, completely, and without a different expectation. Unconditional love requires us to accept Billy for exactly who he is. He cannot be different at this present moment. He is perfectly normal based on his history.
Billy’s behavioral issues in the classroom are thus no longer behavioral issues. They are manifestations of trauma. They are stress-induced responses stemming from an insufficient regulatory system. His trauma has sensitized him to be either over-reactive or under-reactive (hyper- or hypo-aroused); there is no other option. This is his programming.
The challenge then presents itself to Billy’s educators and caretakers as to how to help, guide, and teach him to calm his nervous system. He needs to be able to integrate his traumatic experiences in order to help him return to an internal state of peace and calm. His fundamental level of reactivity must be addressed first to equip him to be able to sit in the classroom and be an engaged and motivated student achieving academic success.
Internal Regulation. Internal regulation relates to the child’s ability to regulate both physiologically and psychologically. From a physiological perspective, “the body bears the burden.”7 A child who has not had the experience of being settled, loved, and nurtured during times of heightened stress (as in the case of Billy), has an internal regulatory system that is not equipped to self-regulate.
When babies are born, they do not have an internal system equipped to self-regulate or self-soothe. When they cry, it is a cry for help to attract the attention of their caregiver to have their basic needs met. The biological design is for the caregiver to be the external regulator for the child since the child’s internal system is underequipped. The infant is at the mercy of the caretaker to mold and develop its internal system of regulation. The infant is learning how to maintain a constant internal environment of homeostasis through this relationship.
When a child does not have his basic needs met from his caretaker, he does not learn how to respond or restore himself back to a calm state when stress-inducing events occur. The child has a limited ability to maintain a calm internal presence when the external environment presents challenges.
Neuroscience has shed light on the fact that the two-way interaction between a baby and its primary caretaker constantly adjusts and modulates the baby’s exposure to environmental stimuli. This interaction serves as a regulator for the developing baby’s internal sense of balance and homeostasis, creating an early childhood blueprint of peace and safety.8 The regulatory role of the caretaker to the child is an essential ingredient to the normal development of the brain. In other words, relationship drives brain development (Figure 2.1).
John Bowlby, the “father of attachment theory,” used the analogy of the thermostat to explain how a child is hardwired to depend upon the regulatory efforts of the caregiver. When a room becomes too warm, the thermostat sends a signal for the air conditioner to be activated. The air conditioner then turns on and re-regulates the comfort level of the room. Similarly, the baby is sending the signal that he is becoming dysregulated. He is trying to “activate” the parent. The baby needs the care, attention, nurturing, and calm presence of the parent in order to calm down his internal system ... he simply cannot do it on his own. The parent serves as the regulator and becomes the child’s secure base.9
Figure 2.1. A healthy parent-child relationship drives healthy brain development.
The same is true for older children who did not receive these early childhood experiences of soothing. They missed these pacifying experiences and have not been taught through the context of the relationship how to calm down. Their internal stress systems are at a heightened level and, like Billy, by third grade (or even as far as middle school or high school) the new “normal” of their stress response system is far more elevated than their peers.
Their internal regulatory systems have been compromised and they are ill-equipped to handle stress, pain, or overwhelm. These children live in a perpetual state of internal dysregulation because they have never had a structure to assimilate and integrate stress. Hence, their behaviors are demonstrative of the internal chaotic world churning inside of them.
External Regulation. When the teacher says to Andy, “Andy, can you please settle down and quietly have a seat?” Andy has the internal regulatory ability to respond appropriately to his teacher. However, when Billy is asked the same question, his response is much different. He takes the long way around the classroom to his seat, he continues to not only talk but projects his voice across the room as if he is still out in the playground, and once seated continues to squirm and wiggle.
Traditionally, we have interpreted Billy as a disruptive child, pasted the label ADHD (attention deficit hyperactivity disorder) onto him, and reprimanded him for his “naughty” behavior. What we have failed to see is that Billy cannot settle down on his own. His internal system has not experienced the appropriate patterning to know how to be well behaved like his classmate Andy.
The brain-body system is a pattern-matching machine. A child with little internal self-control will pattern himself according to his past external experiences. If his past experiences have been chaotic, disruptive, and overwhelming, he will continue acting this way until new patterns are established. Thus, a child coming into a calm and safe classroom is still likely to be acting as if he is in his previous chaotic environment. A child can be taken out of trauma but not so easily can the trauma be taken out of the child. Past patterns of chaos are now the current framework for navigating his world; he knows no different.
The most effective way to change these patterns comes through safe, nurturing, attuned, and strong human connection. For the student in the classroom, it comes through the teacher-student relationship. The reality is, for Billy to learn and achieve academically, he must also be engaged at the relational level.
Environmental factors also play a significant role in providing a child external regulation. The ability to influence a child’s internal system by external means has been demonstrated in scientific studies. In the 1970s, scientists reported that sound and musical rhythms could change a child’s bodily processes. In Johannes Kneutgen’s paper “On the Effects of Lullabies,” he reported that the soothing effects of lullabies changed infants’ breathing rhythms.10 Other similar studies reported that heart rate changes were directly correlated to changes in the tempo of music.
Does this mean we should play lullabies in the classroom to settle children like Billy down? Perhaps, but what it essentially means is that we must take the responsibility to create environments for children that are designed to externally regulate them. A regulated environment can mean everything to a child who has a compromised internal regulatory system. Consider taking Billy and Andy to Chuck-E-Cheese’s. What would be the difference between these two children in this type of setting?
Chuck-E-Cheese’s is overwhelmingly stimulating with loud noises, lights blinking off and on, the promise of winning that special toy, and children running around with high energy. Andy would be able to have fun and could tolerate this level of external stimulation. Billy, on the other hand, would decompensate very quickly if left to his own internal devices.
The same holds true for a child like Billy in the classroom. Providing a classroom to support Billy’s regulation is a responsibility that cannot be ignored or minimized. Failure to do so puts Billy at risk for cycling into a negative academic experience that can have lifelong consequences to reaching his full potential. (See Part Two of this book for more “when the rubber hits the road” ways to create a Beyond Consequences classroom for children.)
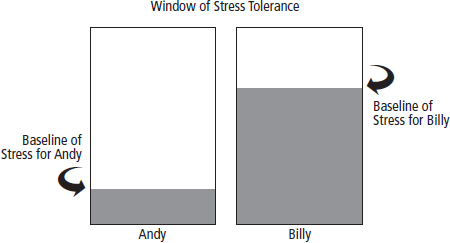
Window of Stress Tolerance. A child’s window of stress tolerance is defined by his ability to withstand pressure, overwhelm, and fear without becoming dysregulated and without reaching his “breaking point.” Each one of us has a certain level of stress from which we operate, as well as a point at which we reach complete overwhelm, where we essentially “blow.”
Figure 2.2 shows the average level of stress both Andy and Billy typically live with—their internal baseline of stress when they start each day. We see that Andy’s internal baseline of stress is low while Billy’s internal baseline of stress is high.
Figure 2.2. Baseline levels of stress for Andy and Billy.
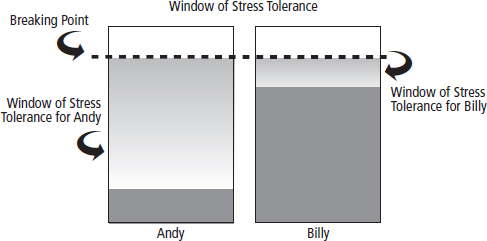
Working Within the Window. The point from this baseline to a child’s breaking point creates the “window of stress tolerance.” Figure 2.3 shows the large window of stress tolerance for Andy and the small window of stress tolerance for Billy.
Figure 2.3. Window of stress tolerance for Andy and Billy.
When a child has a large window of stress tolerance, he has the ability to function well in life and at school. Working within the window, he has the ability to maintain himself in the classroom because he has more tolerance when stressed. In this state, his executive functions are intact and he is able to demonstrate the following:
With this understanding, it makes sense why Andy can remember to bring his homework home, keep his backpack organized, show self-control when a classmate steals his pencil, and initiate a helping hand to his teacher. Andy has a much larger window, which gives him a large emotional range and emotional flexibility. He can navigate his way through his academic day with ease and flexibility.
Billy has a very small window. He lives only moments away from his breaking point. He is short on patience, is impulsive, has difficulty staying focused, and cannot comprehend why he cannot go to recess even after his teacher warned him three times earlier that if he did not behave he would miss his fun time. His executive functions are not on line because he is too stressed out to think clearly and rationally. He is living from a much deeper emotional place of internal chaos, fear, and survival. He has a much smaller emotional range, and struggles by expending a tremendous amount of energy to navigate his way through his academic day.
Changing the Window. When a child is placed in an environment that keeps him in his window without reaching his breaking point, he has a chance to increase his window. Being supported through an emotionally safe, nurturing, and calm relationship with his teacher allows his nervous system the chance to settle down. New neuropathways can be created and old behavioral programs that have kept him locked in a pattern of acting out can be rewritten.
Neuroscience is showing that the neuroplasticity of the nervous system can provide the answers for change and healing. “Plasticity” refers to the body’s ability to add and remove connections, even into adulthood. Childhood is when the brain is the most plastic. Profound changes and healing can occur when a child is placed in the right environment; when his needs are met; when the relationships in his life offer acceptance, trust, and understanding; and when he is given the chance to have positive repetitious experiences in order to override past negative repetitious experiences.
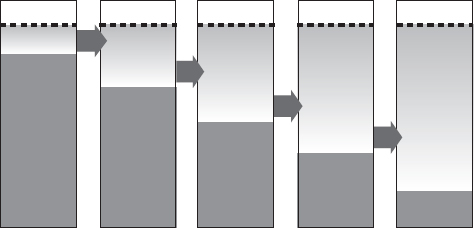
The series of graphs in Figure 2.4 illustrate the level of healing that is possible for a student like Billy. Each positive experience allows for Billy’s window of stress tolerance to increase, each time allowing new neuropathways to develop and new connections to be entrenched. While the healing process is not always as linear as depicted, over a period of time (sometimes as short as two weeks and certainly by six months) Billy’s ability to handle stress will be noticeably improved.
Unfortunately, for many students their window decreases over the school year, instead of increases. The stress of the school environment builds throughout the year, especially during the weeks around state testing; these tests determine whether or not the child is promoted to the next grade.
Figure 2.4. Increasing Billy’s window of stress tolerance.
Even students like Andy, who start the school year with a large window of stress tolerance, often show signs of their window decreasing and of getting closer to their breaking point. The amount of pressure students are asked to handle in academic environments frequently goes far beyond what their nervous systems are equipped to handle. Staying at this heightened level of stress diminishes their abilities to self-regulate and their abilities to learn.
Traditionally, we have failed to realize that limited learning will happen if the emotional needs of a child are not met first. The hierarchy of learning, as shown in chapter 1, has not traditionally been acknowledged. A child like Billy cannot learn when he is living at the edge of survival—at the edge of his breaking point. Trauma alters to what the brain pays attention, so all of Billy’s resources are dedicated to safety rather than academic achievement.
Instead of asking children to make a better “choice” in their behaviors, it is time that we ask ourselves to make a better choice in the creation of their environments. We must develop stronger relationships that will increase their window of stress tolerance and hence increase their capacity to learn, thrive, and succeed.
Figure 2.5. The necessary elements for change.