CHAPTER 10 Health Care Information System Standards
In order to achieve interoperability, portability, and data exchange, health care information systems must employ standards. Systems that conform to different standards cannot communicate with one another. For a simple analogy, think about traveling to a country where you do not speak the language. You would not be able to communicate with that country’s citizens without a common language or translator. Think of the common language as the standard to which all parties agree to adhere. Once you and others agree on a common language, you and they can communicate. You may still have some problems, but generally these can be overcome.
A plethora of information technology (IT) standards, including standards for messaging, content and coding, networks, electronic data interchange, and electronic health records, are important to health care information systems. Some of these standards compete with one another. In 2004, Bazzoli had identified 450 voluntary and mandated standards from 150 organizations, and this number has certainly increased over time. It is important to recognize that, although they will not be discussed in this chapter, many IT standards that do not specifically address health care also have a tremendous impact on health care information systems, such as basic communication protocols and extensible markup language (XML), which has emerged as a messaging standard not only in business-related Internet transactions but also in health care transactions and communications.
In the sections that follow we provide an overview of the standards development process and introduce several key initiatives, some formal and some less so, that have led to the development of standards to facilitate interoperability among health care information systems. These standards will be reviewed in four main categories:
Classification standards
Vocabulary and terminology standards
Data interchange standards
Health record content and functional standards
We will conclude this chapter with a discussion of the impact of federal regulations and the efforts of the Office of the National Coordinator for Health Information Technology on the adoption of health care information standards to facilitate interoperability.
STANDARDS DEVELOPMENT PROCESS
When seeking to understand why so many different IT and health care information standards exist, it is helpful to look first at the basic standards development process that exists in the United States (and internationally) and the changes that have occurred in this process over the past decade. In general the methods used to establish health care IT standards can be divided into four categories (Hammond & Cimino, 2006):
Ad hoc. A standard is established by the ad hoc method when a group of interested people or organizations agrees on a certain specification without any formal adoption process. The Digital Imaging and Communications in Medicine (DICOM) standard for health care imaging came about in this way.
De facto. A de facto standard arises when a vendor or other commercial enterprise controls such a large segment of the market that its product becomes the recognized norm. The SQL database language and the Windows operating system are examples of de facto standards. XML is becoming a de facto standard for health care and other types of industry messaging.
Government mandate. Standards are also established when the government mandates that the health care industry adopt them. Examples are the transaction and code sets mandated by the Health Insurance Portability and Accountability Act (HIPAA) regulations.
Consensus.Consensus-based standards come about when representatives from various interested groups come together to reach a formal agreement on specifications. The process is generally open and involves considering comment and feedback from the industry. This method is employed by the standards development organizations (SDOs) accredited by the American National Standards Institute (ANSI). Most health care information standards are developed by this method, including Health Level Seven (HL7) standards and Accredited Standards Committee (ASC) X12N standards.
Libicki, Schneider, Frelinger, and Slomovic (2000) outline a two-by-two matrix topology for IT standard-setting organizations. They classify the organizations that set IT standards by membership type (open to all or members only) and by process (democratic or dependent on “a strong leader”). The organizations with the most formal standard-setting processes, such as the International Organization for Standardization (ISO), ANSI, and the ANSI-accredited SDOs, fall into the member-only, democratic classification. The relationships among the various standard-setting organizations can be confusing. Not only do many of the acronyms sound similar, but the organizations themselves, as voluntary, member-based organizations, can set their own missions and goals. Therefore, although there is a formally recognized relationship among ISO, ANSI, and the SDOs, there is also some overlap in activities. Table 10.1 outlines the relationships among these formal standard-setting organizations and for each one gives a brief overview of important facts and a current web site.
Table 10.1. Organizations responsible for formal standards development
Organizations
Facts
International Organization for Standardization (ISO), www.iso.org
Members are national standards bodies from many different countries around the world ANSI is the U.S. national body member Oversees the flow of documentation and international approval of standards developed under the auspices of its member bodies
American National Standards Institute (ANSI), www.ansi.org
U.S. member of ISO Accredits standards development organizations (SDOs) from a wide range of industries, including health care Oversees the work of the SDOs, technical committees, subcommittees, and working groups Does not develop standards itself, but accredits the organizations that develop standards Publishes the 10,000+ American National Standards developed by accredited SDOs
Standards development organizations (SDOs)
Must be accredited by ANSI Develop standards in accordance with ANSI criteria
SDOs that develop health care–related standards discussed in this chapter
Can use the label “Approved American National Standard”
ASTM International (formerly American Society for Testing and Materials), www.astm.org
Currently, there are 270+ ANSI-accredited SDOs representing many industries, including health care
All the ANSI-accredited SDOs must adhere to the guidelines established for accreditation; therefore, they have similar standard-setting processes. According to ANSI, this process includes
Consensus on a proposed standard by a group or “consensus body” that includes representatives from materially affected or interested parties
Broad-based public review and comment on draft standards
Consideration of and response to comments submitted by voting members of the relevant consensus body and by public review commenters
Incorporation of approved changes into a draft standard
Right to appeal by any participant that believes that due process principles were not sufficiently respected during the standards development in accordance with the ANSI-accredited procedures of the standards developer [ANSI, 2012]
In the last decade the IT industry in general has experienced a movement away from the process of establishing standards via the SDOs. The Internet and World Wide Web standards, for example, were developed by groups with much less formal structures. However, the SDOs continue to have a significant impact on the IT standards for the health care industry.
The HIPAA rules identify a subset of SDOs and other organizations as Designated Standards Maintenance Organizations (DSMOs), whose responsibility it is to maintain the transaction standards that fall under the HIPAA rules. The current HIPAA DSMOs are
Accredited Standards Committee X12
Dental Content Committee of the American Dental Association
Health Level Seven
National Council for Prescription Drug Programs
National Uniform Billing Committee
National Uniform Claim Committee
CLASSIFICATION STANDARDS
The most widely recognized coding and classification systems—ICD, Current Procedural Terminology (CPT), and diagnosis related groups (DRGs)—were discussed in Chapter One. Although these systems and the other systems discussed in this section do not meet the criteria for full clinical vocabularies, they are used to classify diagnoses and procedures and are the basis for information retrieval in health care information systems. Most were originally developed to facilitate disease and procedure information retrieval, but have been adopted to code for billing services as well. Several of the most commonly used classification systems are actually incorporated across more robust standard vocabularies such as SNOMED-CT and UMLS®.
The HIPAA rules specify specific code sets for diagnoses and procedures that are to be used in any transactions by a covered entity. The code sets required by HIPAA are
HCPCS (ancillary services or procedures) (see Chapter One)
ICD-9 (ICD-10 as of October 2014 for diagnoses and hospital inpatient procedures) (see Chapter One)
NDC (national drug codes) (CMS, 2012a)
The HITECH “meaningful use” final rule (discussed in Chapter Four) also includes ICD-9, with the transition to ICD-10, as its classification standard.
Code on Dental Procedures and Nomenclature
The American Dental Association (ADA) publishes the CDT, Code on Dental Procedures and Nomenclature. This set of codes is designed to support accurate recording and reporting of dental treatments. The ADA (2012) strives to maintain an up-to-date set of codes that reflect actual practice. The code set is divided into twelve sections as follows (Washington Dental Service, 2012):
Diagnostic (D0000–D0999)
Preventative (D1000–D1999)
Restorative (D2000–D2999)
Endodontics (D3000–D3999)
Periodontics (D4000–D4999)
Prosthodontics (D5000–D5899)
Maxillofacial prosthetics (D5900–D5999)
Implant services (D6000–D6199)
Prosthodontics (D6200–D6999)
Oral and maxillofacial surgery (D7000–7999)
Orthodontics (D8000–8999)
Adjunctive General Services (D9000–D9999)
National Drug Codes
The National Drug Code (NDC) is the universal product identifier for all human drugs. The Drug Listing Act of 1972 requires registered drug companies to provide the Food and Drug Administration (FDA) a current listing of all drugs “manufactured, prepared, propagated, compounded, or processed by it for commercial distribution” (FDA, 2012). The FDA, in turn, assigns the unique, three-segment NDC (listed as package code in the following example) and maintains the information in the National Drug Code Directory. The NDC Directory is updated twice each month. Data maintained for each drug include up to sixteen fields. The information for the common over-the-counter drug Tylenol PM (Extra Strength), for example, is as follows:
Product NDC: 50580–176
Product Type Name: Human OTC Drug
Proprietary Name: Tylenol PM (Extra Strength)
Non-proprietary Name: Acetaminophen and Diphenhydramine Hydrochloride
Package Description: 1 Bottle, Plastic in 1 Carton (50580–176–10) > 100 tablet, coated in 1 Bottle, Plastic
DEA classification: <blank> (FDA, 2012)
VOCABULARY AND TERMINOLOGY STANDARDS
One of the most difficult problems in exchanging health care information and building longitudinal electronic health records (EHRs) is coordinating the vast amount of health information that is generated in diverse locations for patients and populations. The vocabulary and terminology standards discussed in this section serve similar purposes—to create a common language that allows different information systems or vendor products to communicate unambiguously with one another. In a very simplified example, a standard vocabulary would ensure that the medical term “myocardial infarction,” for example, is “mapped” to the term “heart attack” and that both terms share exactly the same attributes. An effective standard vocabulary must also standardize the very complex hierarchy and syntax of the language used in the health industry. This is a complicated and detailed endeavor to say the least. So it is not surprising that to date, no single vocabulary has emerged to meet all the information exchange needs of the health care sector.
The National Committee on Vital and Health Statistics (NCVHS) has the responsibility, under a HIPAA mandate, to recommend uniform data standards for patient medical record information (PMRI). Although no single vocabulary has been recognized by NCVHS as the standard, they have recommended the following as a core set of PMRI terminology standards:
Systematized Nomenclature of Medicine—Clinical Terms (SNOMED CT)
Logical Observation Identifiers Names and Codes (LOINC) laboratory subset
Several federal drug terminologies, including RxNorm (NCVHS, 2003)
The HITECH “meaningful use” final rule (discussed in Chapter Four) also includes vocabulary standards—LOINC, SNOMED-CT, RxNorm, and CVX (clinical vaccines administered).
In this section we will describe SNOMED CT, LOINC, CVX, and RxNorm, along with the National Library of Medicine’s Unified Medical Language® (UMLS®) (of which RxNorm is one component), which has become the standard for bibliographical searches in health care and has the potential for other uses as well.
Systematized Nomenclature of Medicine—Clinical Terms
Systematized Nomenclature of Medicine—Clinical Terms (SNOMED CT) is a comprehensive clinical terminology developed specifically to facilitate the electronic storage and retrieval of detailed clinical information. It is the result of collaboration between the College of American Pathologists (CAP) and the United Kingdom’s National Health Service (NHS). SNOMED CT merges CAP’s SNOMED Reference Terminology, an older classification system used to group diseases, and the NHS’s Clinical Terms Version 3 (better known as Read Codes), an established clinical terminology used in Great Britain and elsewhere. As a result, SNOMED CT is based on decades of research. As of April 2007 SNOMED is owned, maintained, and distributed by the International Health Terminology Standards Development Organisation (IHTSDO), a nonprofit association based in Denmark. The National Library of Medicine is the U.S. member of the IHTSDO and distributes SNOMED at no cost within the United States (NLM, 2012a).
Logical Observation Identifiers Names and Codes
The Logical Observation Identifiers Names and Codes (LOINC) system was developed to facilitate the electronic transmission of laboratory results to hospitals, physicians, third-party payers, and other users of laboratory data. Initiated in 1994 by the Regenstrief Institute at Indiana University, LOINC provides a standard set of universal names and codes for identifying individual laboratory and clinical results. These standard codes allow users to merge clinical results from disparate sources (LOINC, 2012).
LOINC codes have a fixed length field of seven characters. Current codes range from three to seven characters long. There are six parts in the LOINC name structure: component/analyte, property, time aspect, system, scale type, and method. The syntax for a name follows this pattern (Case, 2011):
5193–8:Hepatitis B virus surface Ab: ACnc:Pt:Ser:Qn:EIA
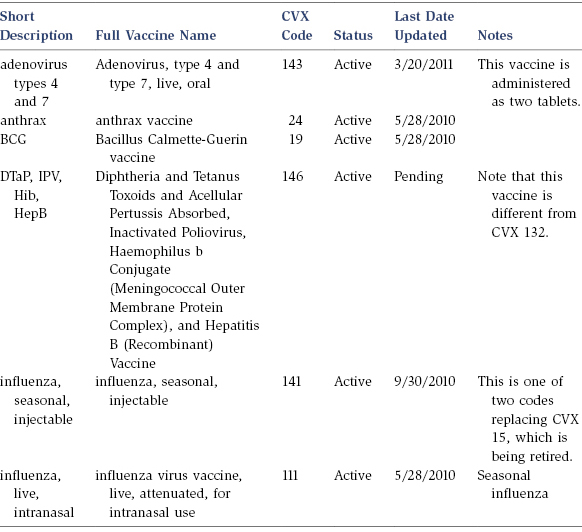
Clinical Vaccines Administered
The Centers for Disease Control and Prevention (CDC) National Center of Immunization and Respiratory Diseases (NCIRD) developed the Clinical Vaccines Administered (CVX) as a table for use with HL7 messaging standard (see the HL7 section later in this chapter for more explanation.) Table 10.2 is an excerpt from the full CVX table (CDC, 2012).
Table 10.2. Excerpts from CVX (clinical vaccines administered) table
RxNorm
The National Library of Medicine (NLM) produces RxNorm, which serves two purposes, as “a normalized naming system for generic and brand name drugs and as a tool for supporting semantic interoperation between drug terminologies and pharmacy knowledge based systems” (NLM, 2012b). The goal of RxNorm is to allow disparate health information systems to communicate with one another in an unambiguous manner.
There are twelve separate RxNorm data files that are released on a monthly basis. The files show
Drug names and unique identifiers
Relationships
Attributes
Semantic types
Data history (three files)
Obsolete data (three files)
Metadata (two files)
The following example from the first RxNorm data file represents the “concept,” Azithromycin 250 MG Oral Capsule, with the unique identifier 141962 (NLM, 2012b):
The National Library of Medicine (NLM), an agency of the National Institutes of Health, began the Unified Medical Language System (UMLS) project in 1986, and it is ongoing today. The purpose of the UMLS project is to “to facilitate the development of computer systems that behave as if they ‘understand’ the meaning of the language of biomedicine and health. The UMLS provides data for system developers as well as search and report functions for less technical users” (NLM, 2008, p. 1).
The UMLS has three basic components, called knowledge sources:
UMLS Metathesaurus®, which contains over one million biomedical concepts from over one hundred source vocabularies. All the common health information vocabularies, including SNOMED CT, ICD, and CPT, along with approximately one hundred other vocabularies, including RxNorm, are incorporated into the metathesaurus. The metathesaurus project’s goal is to incorporate and map existing vocabularies into a single system.
UMLS Semantic Network, which defines 133 broad categories and fifty-four relationships between categories for labeling the biomedical domain. The semantic network contains information about the categories (such as “Disease or Syndrome” and “Virus”) to which metathesaurus concepts are assigned. The semantic network also outlines the relationships among the categories (for example, “Virus” causes “Disease or Syndrome”).
SPECIALIST Lexicon and Lexical Tools. The lexicon contains information for many terms, component words, and English language words that do not appear in the metathesaurus.
The UMLS products are widely used in NLM’s own applications, such as PubMed. They are available to other organizations free of charge, provided the users submit a license agreement (NLM, 2008).
Data Interchange Standards
The ability to exchange and integrate data among health care applications is critical to the success of any overall health care information system, whether an organizational, regional, or national level of integration is desired. Although there is some overlap, these standards differ from the vocabulary standards because their major purpose is to standardize the actual “messaging” between health care information systems. Much of the health care information standards development activity has been in the area of standards for data interchange or integration. In this section we will look at a few of the standards that have been developed for this purpose. There are others, and new needs are continually being identified. However, the following groups of standards are recognized as important to the health care sector, and together they provide examples of both broad standards addressing all types of applications and specific standards addressing one type of application.
Health Level Seven standards
Digital Imaging and Communications in Medicine (DICOM)
National Council for Prescription Drug Programs (NCPDP)
ANSI ASC X12N standards
It is important to note that the HIPAA rules include specified standards for electronic transactions, which fall into this category of data exchange standards. HIPAA specifically required covered entities to comply with specific ANSI X12N and NCPCP standards.
Health Level Seven Standards
Health Level Seven International (HL7) is an ANSI-accredited standards development organization that was founded as an ad hoc group in 1987. HL7 was founded with a purpose of developing a messaging standard to support the “exchange, management, and integration of data that support clinical patient care” (Marotta, 2000). This purpose has expanded over time to include standards defining
System integration and interoperability
Tools and “building blocks” used to build the standards
Messaging and document standards
EHR functional models and profiles
Since its inception, HL7 has grown from a small group of fourteen individuals to a large organization with over 2,300 health care provider, vendor, and consultant members. HL7’s five hundred corporate members represent more than 90 percent of health care information systems vendors (HL7, 2012).
HL7 v3 messaging standards incorporate the root elements of XML and, as such, are a significant change from early versions. See the HL7 Perspective for an example of HL7 v3.
Digital Imaging and Communications in Medicine
The growth of digital diagnostic imaging (such as CT scans and MRIs) gave rise to the need for a standard for the electronic transfer of these images between devices manufactured by different vendors. The American College of Radiology (ACR) and the National Electrical Manufacturers Association (NEMA) published the first standard, a precursor to the current Digital Imaging and Communications in Medicine (DICOM) standard, in 1985. The goals of DICOM are to “achieve compatibility and to improve workflow efficiency between imaging systems and other information systems in healthcare environments worldwide.” It is used by all of the major diagnostic medical imaging vendors, which translates to its use in nearly every medical profession that uses images (DICOM, 2012).
National Council for Prescription Drug Programs
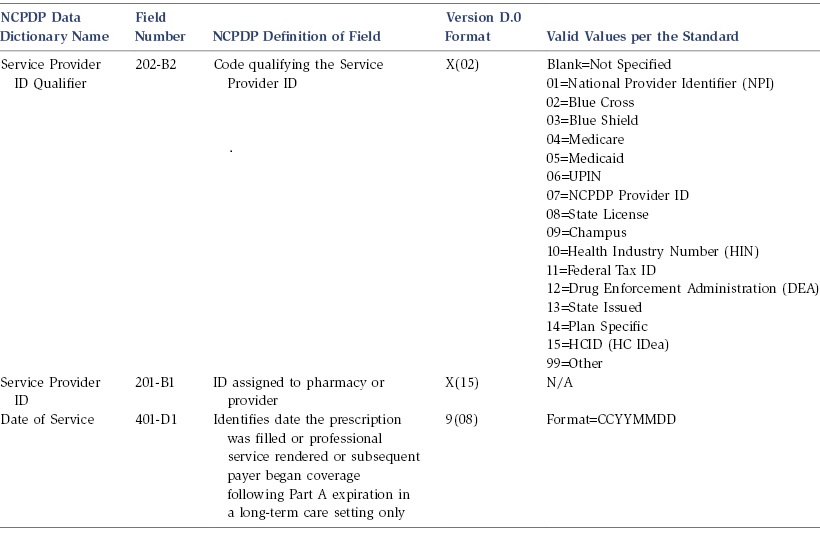
The mission of the National Council for Prescription Drug Programs (NCPDP) states that “NCPDP provides a forum wherein our diverse membership can develop business solutions, including ANSI-accredited standards, and guidance for promoting information exchanges related to medications, supplies, and services within the healthcare system. Through a consensus building process in collaboration with other industry organizations, our members develop these solutions to improve safety, privacy and healthcare outcomes for patients and healthcare consumers, while reducing costs in the system.” To this end the NCPDP, an ANSI-accredited SDO with over 1,600 members representing the pharmacy services industry, has developed a set of standards for the electronic submission of third-party drug claims (NCPDP, 2012).
These standards not only include the Telecommunication Standards and Batch Standards required by HIPAA, but also Uniform Healthcare Payer Data Standard, Retiree Drug Subsidy Standard, the SCRIPT standard for e-prescribing (required by CMS for Medicare and Medicaid e-prescribing), and the Manufacturers Rebate Standard, among others. Of note, the SCRIPT standard currently incorporates the RxNorm, discussed earlier in this chapter, as a standardized medication nomenclature. The NCPDP Provider Identification Number is a unique identifier of over 75,000 pharmacies. As of January 2012, HIPAA requires covered entities to comply with the NCPDP Telecommunications Standard Version D.0 and Batch Standards Version 1.2 for pharmacy claims transactions (Emdeon, 2012). Table 10.3 presents excerpts from the NCPDP Data Dictionary, which outlines a few of the Transmission Header Segment requirements. The entire Data Dictionary table is over seventy pages long (CMS, 2012c).
The ANSI Accredited Standards Committee (ASC) X12 develops standards, in both X12 and XML formats, for the electronic exchange of business information. One ASC X12 subcommittee, X12N, has been specifically designated to deal with electronic data interchange (EDI) standards in the insurance industry, and this subcommittee has a special health care task group, known as TG2. According to the X12 TG2 web site, “the purpose of the Health Care Task group shall be the development and maintenance of data standards (both national and international) which shall support the exchange of business information for health care administration. Health care data includes, but is not limited to, such business functions as eligibility, referrals and authorizations, claims, claim status, payment and remittance advice, and provider directories.” To this end ASC X12N has developed a set of standards that are monitored and updated through ASC X12N work groups. Table 10.4 lists the current X12 work group areas.
All HIPAA-covered entities were required to be compliant with the ASC X12 version 5010 by January 1, 2012. A portion of the X12 5010 Professional Claim standard is shown in Exhibit 10.1. The standard for Professional Claim alone is over ninety pages in length.
HEALTH RECORD CONTENT AND FUNCTIONAL STANDARDS
In this section we will look at four sets of health record content and functional standards.
HL7 EHR-S (Electronic Health Record-System) Functional Model
ASTM Health Record Content Standards
Continuity of Care Document
HITECH EHR Certification Criteria
HL7 EHR-S Functional Model
The HL7 Health Record-System (EHR-S) Functional Model, Release 1, is the result of a 2009 revision to the original HL7 Functional Model. The purpose of this functional model is to outline important features and functions that should be contained in an EHR. Targeted users of the functional model include vendors and care providers and it has been recognized by the ISO as an international standard (ISO 10781). The stated benefits (HL7, 2012) to the functional model are to
Facilitate describing end-user defined benefits such as patient safety, quality outcomes, and cost efficiencies in terms of standard EHR-S functions
Promote a common understanding of EHR functions from which developers, vendors, users, and other interested parties can plan and evaluate EHR-S functions
Provide the necessary framework to drive the requirements and applications of next level standards, such as EHR content, coding, information models, constructs, and interoperability for information portability between subsystems of and across EHR-Ss
Establish a standards-based method by which each realm (country) can apply these EHR functions to care settings, uses, and priorities
Inform those concerned with secondary use of EHR data and national infrastructure what functions can be expected in an EHR system
The EHR-S Functional Model includes a functional outline, functional profiles, and assigned priorities for the functions in the profile. The functional outline is divided into three sections: Direct Care, Supportive, and Information Infrastructure functions. Within these three main sections there are thirteen subsections and over 140 individual functions. Exhibit 10.2 depicts the overall functional model, and Exhibit 10.3 provides an example of two functions contained within the Information Infrastructure section.
ASTM Health Record Content Standards
ASTM International Committee E31 on Health Informatics has been working on consensus standards related to the maintenance and transfer of patient information since 1970. Since that time, several standards have been developed by E31 (ASTM, 2012):
E2369, Specification for Continuity of Care Record (CCR), which defines a core set of information to be sent to a health care provider when a patient is referred or transferred.
E1384, Practice for Content and Structure of the Electronic Health Record (EHR), which provides a structure for data collected in patient care records.
E1633, Specification for Coded Values Used in the Electronic Health Record, which provides detailed value sets for use with E1384.
Continuity of Care Document
The Continuity of Care Document (CCD) is a standard for the electronic exchange of patient summary information, so-called “transportable” patient care information. The current CCD standard is actually a merger of two other standards, the HL7 Clinical Document Architecture (CDA) standard and the ASTM Continuity of Care Record (CCR). There has been some discussion among experts about the CCR and CCD being competing standards, but HL7 has taken the position that CCD is an implementation of CCR and simply an evolution of the CCR (Rouse, 2010). Although discussed in this section, the CCD standard is not solely a content standard, but includes elements of a data exchange standard; it has an XML-based specification for patient summary data, but also includes a standard outline of its content. The current content outline for the CCD is as follows (Corepoint Health, 2012):
Header
Purpose
Problems
Procedures
Family history
Social history
Payers
Advance directives
Alerts
Medications
Immunizations
Medical equipment
Vital signs
Functional stats
Results
Encounters
Plan of care
HITECH EHR Certification Criteria
The details of the Health Information Technology for Economic and Clinical Health (HITECH) Act are discussed at length in Chapter Six. One of the significant components of this Act is the incentive program for electronic health records. To qualify for the incentive program, providers not only must ensure “meaningful use” of the EHR, but must also demonstrate that the EHR in use meets certification criteria. The certification criteria for the EHR under HITECH is divided into criteria for the Ambulatory Setting and for the Inpatient Setting. Table 10.5 outlines the EHR criteria to meet the Stage 1 Meaningful Use Objectives, along with relevant standards. For a full list of all EHR criteria, go to http://healthit.hhs.gov (HHS, 2012d). Eligible participants must meet all of the listed “Core Set” and five out of ten “Menu Set.”
Table 10.5. Excerpt from HITECH EHR certification criteria core set
CERTIFICATION CRITERIA 45 CFR 170.302 & 170.304
CERTIFICATION CRITERIA 45 CFR 170.302 & 170.306
*Ambulatory Setting*
**Inpatient Setting**
Computerized provider order entry. Enable a user to electronically record, store, retrieve, and modify, at a minimum, the following order types:
(1) Medications;
(2) Laboratory; and
(3) Radiology/imaging.
Computerized provider order entry. Enable a user to electronically record, store, retrieve, and modify, at a minimum, the following order types:
(1) Medications;
(2) Laboratory; and
(3) Radiology/imaging.
Drug-drug, drug-allergy interaction checks.
(1) Notifications. Automatically and electronically generate and indicate in real-time, notifications at the point of care for drug-drug and drug-allergy contraindications based on medication list, medication allergy list, and computerized provider order entry (CPOE).
(2) Adjustments. Provide certain users with the ability to adjust notifications provided for drug-drug and drug-allergy interaction checks.
Maintain up-to-date problem list. Enable a user to electronically record, modify, and retrieve a patient’s problem list for longitudinal care in accordance with:
(1) The standard specified in §170.207(a)(1); or
(2) At a minimum, the version of the standard specified in §170.207(a)(2).
Electronic prescribing. Enable a user to electronically generate and transmit prescriptions and prescription-related information in accordance with:
(1) The standard specified in §170.205(b)(1) or §170.205(b)(2); and
(2) The standard specified in §170.207(d).
Maintain active medication list. Enable a user to electronically record, modify, and retrieve a patient’s active medication list as well as medication history for longitudinal care.
Maintain active medication allergy list. Enable a user to electronically record, modify, and retrieve a patient’s active medication allergy list as well as medication allergy history for longitudinal care.
Federal Initiatives Affecting Health Care IT Standards
The federal government has several important initiatives related to health care information standards, several of which have been mentioned in previous sections of this chapter and in other chapters in this book. However, in this section we will take a summary view of these initiatives and their specific impact on health care IT standards. We will look at federal initiatives for health care IT standards as a part of HIPAA, CMS e-prescribing, and the Office of the National Coordinator for Health Information Technology. As discussed throughout this chapter, the HITECH Act also affects health care IT standards. However, it will not be discussed in this section. Refer to Chapter Six for a full discussion of this important, wide-sweeping legislation.
HIPAA
In August 2000, the U.S. Department of Health and Human Services published the final rule outlining the standards to be adopted by health care organizations for electronic transactions, and announced the designated standard maintenance organizations (DSMOs). Several modifications to this final rule have been subsequently published. In publishing this rule the federal government mandated that health care organizations adopt certain standards for electronic transactions and standard code sets for these transactions, and identified the standards organizations that would oversee the adoption of standards for HIPAA compliance. HIPAA transaction standards apply to all covered entities’ electronic data interchange (EDI) related to claims and encounter information, payment and remittance advice, claims status, eligibility, enrollment and disenrollment, referrals and authorizations, coordination of benefits and premium payment. The current HIPAA transaction standards are ASC X12N version 5010 (which accommodates ICD-10) along with NCPDP D.0 for certain pharmacy transactions. In addition to these transaction standards, several standard code sets, as listed earlier in the chapter, have been established for use in electronic transactions. The DSMOs, also listed earlier in this chapter, have the responsibility for the development, maintenance, and modification of relevant electronic data interchange standards (CMS, 2012a).
Centers for Medicare and Medicaid E-Prescribing
The Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA) established a Voluntary Prescription Drug Benefit program. There is no requirement in this Act that providers write prescriptions electronically, but those who choose to do so must comply with specific electronic prescribing (e-prescribing) standards. The current published CMS e-prescribing standards consist of three sets of existing health care IT standards as “foundation” standards, which include NCPDP’s SCRIPT Standard for e-Prescribing, ASC X12N standard for Health Care Eligibility Benefit and Response, and NCPDP’s telecommunications standard. In addition, the final rule identifies three additional electronic “tools” to be used in implementing e-prescribing: NCPDP Formulary and Benefit Standard Implementation Guide, which provides information about drugs covered under the beneficiary’s benefit plan; NCPDP SCRIPT Medication History Transactions, which provides information about medications a beneficiary has been taking; and Fill Status Notification (RxFill), which allows prescribers to receive an electronic notice from the pharmacy regarding the beneficiary’s prescription status (CMS, 2012b).
Office of the National Coordinator for Health Information Technology
In April 2004, President Bush established the Office of the National Coordinator for Health Information Technology (ONC) and charged the office with providing “leadership for the development and nationwide implementation of an interoperable health information technology infrastructure to improve the quality and efficiency of health care” (HHS, 2008). In 2009, the role of ONC was strengthened when the HITECH Act legislatively mandated ONC to provide this leadership and oversight (HHS, 2012a). Today, ONC is the “principal Federal entity charged with coordination of nationwide efforts to implement and use the most advanced health information technology and the electronic exchange of health information,” which is clearly reflected in their published mission statement (HHS, 2012a).
ONC’s mission:
Promoting development of a nationwide health IT infrastructure that allows for electronic use and exchange of information that
Ensures secure and protected patient health information
Improves health care quality
Reduces health care costs
Informs medical decisions at the time and place of care
Includes meaningful public input in infrastructure development
Improves coordination of care and information among hospitals, labs, physicians, and so on
Improves public health activities and facilitates early identification of and rapid response to public health emergencies
Facilitates health and clinical research
Promotes early detection, prevention, and management of chronic diseases
Promotes a more effective marketplace
Improves efforts to reduce health disparities
Providing leadership in the development, recognition, and implementation of standards and the certification of health IT products
Health IT policy coordination
Strategic planning for health IT adoption and health information exchange
Establishing governance for the Nationwide Health Information Network
Current ONC initiatives, in addition to implementing HITECH, include several that influence the development and implementation of health care IT standards (HHS, 2012b): cybersecurity (discussed more fully in Chapter Eleven), Nationwide Health Information Network, and state-level initiatives for health information exchange (HIE).
Nationwide Health Information Network
The Nationwide Health Information Network (NwHIN) is defined by ONC as a set of standards, services, and policies that enable the secure exchange of health information over the Internet (HHS, 2012c). It is not a physical network, and it does not store any health care information. The NwHIN has evolved from its earliest model of a network of networks to an operational set of standards, services, and policies. The latest evolution of the NwHIN supports “public-private healthcare interoperability and partnerships,” the NwHIN Exchange. The participating organizations of the NwHIN share information using a common set of specifications, including those developed for NwHIN and other industry standards. There are currently twenty-five participating NwHIN organizations, including four federal agencies—CMS, DoD, SSA, and VA—and twenty-one private health care organizations (Sullivan, 2012).
HIEs and the NwHIN are still in the early stages of development. These efforts face daunting challenges of developing sustainable business models, managing patient privacy, ensuring effective governance, implementing data standards, and creating scalable technologies. Although establishing health IT interoperability across the country is a logical and necessary goal, achieving that goal will be a multiyear and complex undertaking.
SUMMARY
In this chapter we reviewed the processes by which health care information standards are developed and looked at some of the common standards that exist today, including standards in three main categories: classification, vocabulary, and terminology standards; data interchange standards; and health record content standards.
Multiple standard-setting organizations and health care professional organizations play a role in standards development. Standards can be developed through a formal process or by less formal mechanisms, including de facto designation.
The standards discussed in this chapter and other general IT standards enable health care information systems to be interoperable and portable and to exchange data. Without such standards, the EMR system and other health care information systems would have limited functionality.
The future of health care information systems is unknown; however, it is clear that the goal of having functional EHRs will not be realized until national standards are adopted. The government, as well as the private sector, plays a role in the development of national standards. HIPAA and HITECH, for example, have had a significant impact on the development of health care information standards. In addition, the creation of the Office of the National Coordinator for Health Information Technology has contributed to the movement toward true health care IT interoperability.
KEY TERMS
Accredited Standards Committee (ASC)
Ad hoc standard development
American National Standards Institute (ANSI)
ASTM International
Clinical Vaccines Administered (CVX)
Code on Dental Procedures and Nomenclature
Consensus standards
Content and functional standards
Continuity of Care Document (CCR)
Continuity of Care Record (CCR)
De facto standard development
Dental Content Committee of the American Dental Association (ADA DCC)
Designated standard maintenance organizations (DSMOs)
Digital Imaging and Communications in Medicine (DICOM)
Electronic data interchange standards
Electronic health record standards
European Committee for Standardization (CEN)
Government mandated standards
Health information exchange (HIE)
Health Level Seven International (HL7)
HIPAA transaction standards
HL7 EHR-S Functional Model
HITECH
HITECH EHR Certification Criteria
International Health Terminology Standards Development Organisation (IHTSDO)
Logical Observation Identifiers Names and Codes (LOINC)
Messaging standards
National Committee on Vital and Health Statistics (NCVHS)
National Council for Prescription Drug Programs (NCPDP)
National Drug Codes
National Library of Medicine (NLM)
National Uniform Billing Committee (NUBC)
National Uniform Claim Committee (NUCC)
Nationwide Health Information Network (NwHIN)
Network standards
Office of the National Coordinator for Health Information Technology (ONC)
RxNorm
Standards development organizations (SDOs)
Systematized Nomenclature of Medicine—Clinical Terms (SNOMED CT)
Unified Medical Language System (UMLS)
X12N standards
LEARNING ACTIVITIES
Standards development is a dynamic process. Select one or more of the standards listed in this chapter and conduct an Internet search for information on that standard. Has the standard changed? What are the current issues surrounding the standard?
Visit a hospital IT department and speak with a clinical analyst or other person who works with clinical applications. Investigate the standards that the hospital’s applications use. Discuss any issues surrounding these standards.
Interview the chief information officer (CIO) of a health care organization. Find out his or her views on the current state of health care IT standards or on the need for standards as the United States moves toward broader adoption of EMR systems.
As you reflect on the information in this chapter and your own research, compare and contrast the intent of “classification,” “functional,” “content,” “messaging.” and “transaction” health care IT standards.
Hammond, W., & Cimino, J. (2006). Biomedical informatics. In E. Shortliffe & J. Cimino (Eds.), Standards in biomedical informatics (pp. 265–311). New York: Springer-Verlag.
Libicki, M., Schneider, J., Frelinger, D., & Slomovic, A. (2000). Scaffolding the new web: Standards and standards policy for the digital economy. Santa Monica, CA: Rand.
Logical Observation Identifiers Names and Codes. (2012). LOINC background. Retrieved March 2012 from http://loinc.org/background
National Committee on Vital and Health Statistics. (2003, November 5). Letter to the secretary: Recommendations for PMRI terminology standards. Retrieved March 2012 from http://www.ncvhs.hhs.gov/031105lt3.pdf
 Ensures secure and protected patient health information
Ensures secure and protected patient health information