CHAPTER 59
Anaphylaxis
Introduction
Anytime a patient receives a drug or is exposed to a chemical substance, an adverse reaction or an allergic reaction is possible. During the perioperative period, patients can be exposed to a wide variety of drugs. The anesthetic team must be vigilant for reactions and be ready to diagnose and treat reactions quickly. In some cases, reactions to medications can be severe or even life threatening. Anesthesia technicians must be ready to provide prompt assistance and technical support to the anesthesia team during a crisis.
Reactions to drugs and chemical substances can be categorized by the mechanism of the reaction. An adverse drug reaction is one that is known to be associated with the use of the drug, and the effect follows a predictable course. Some examples of adverse drug reactions include relative drug overdose, drugs being given too rapidly producing exaggerated effects, known side effects such as nausea, and topical, mechanical, or chemical irritation from skin exposure. It is important to understand the difference between an adverse drug reaction and a true allergic reaction to a drug or substance because the etiology, mechanism of the reaction, and the treatment are different for the two types of reactions. Adverse drug reactions are not true drug allergies. True allergy to a drug or substance involves an immune reaction.
The most serious allergic reaction to a drug or chemical substance is called anaphylaxis. This chapter covers the following important aspects of an anaphylactic reaction:
- Pathophysiology
- Clinical presentation
- Common triggers for anaphylaxis in the perioperative setting
- Diagnosis and treatment
- Prevention
Anaphylaxis is an immune reaction to a drug or foreign substance that is rapid in onset, unpredictable in severity, and unanticipated and can be life threatening. It is a systemic immune reaction against a foreign substance, or antigen. This reaction involves specific immune system proteins referred to as antibodies. The antibodies attach to the foreign antigen, which then triggers a cascade of inflammatory responses within the body. Proinflammatory and inflammatory mediators are released into the bloodstream, which can rapidly result in the clinical syndrome of anaphylaxis: skin rash, hemodynamic instability and hypotension, airway compromise from tissue swelling, bronchospasm with oxygenation and ventilation difficulties, possible cardiac depression, and dysrhythmias (Fig. 59.1). True anaphylaxis is a medical emergency. The anesthetic team must be prepared to recognize, diagnose, and rapidly treat these reactions and provide supportive care, without delay, for the best patient outcome.
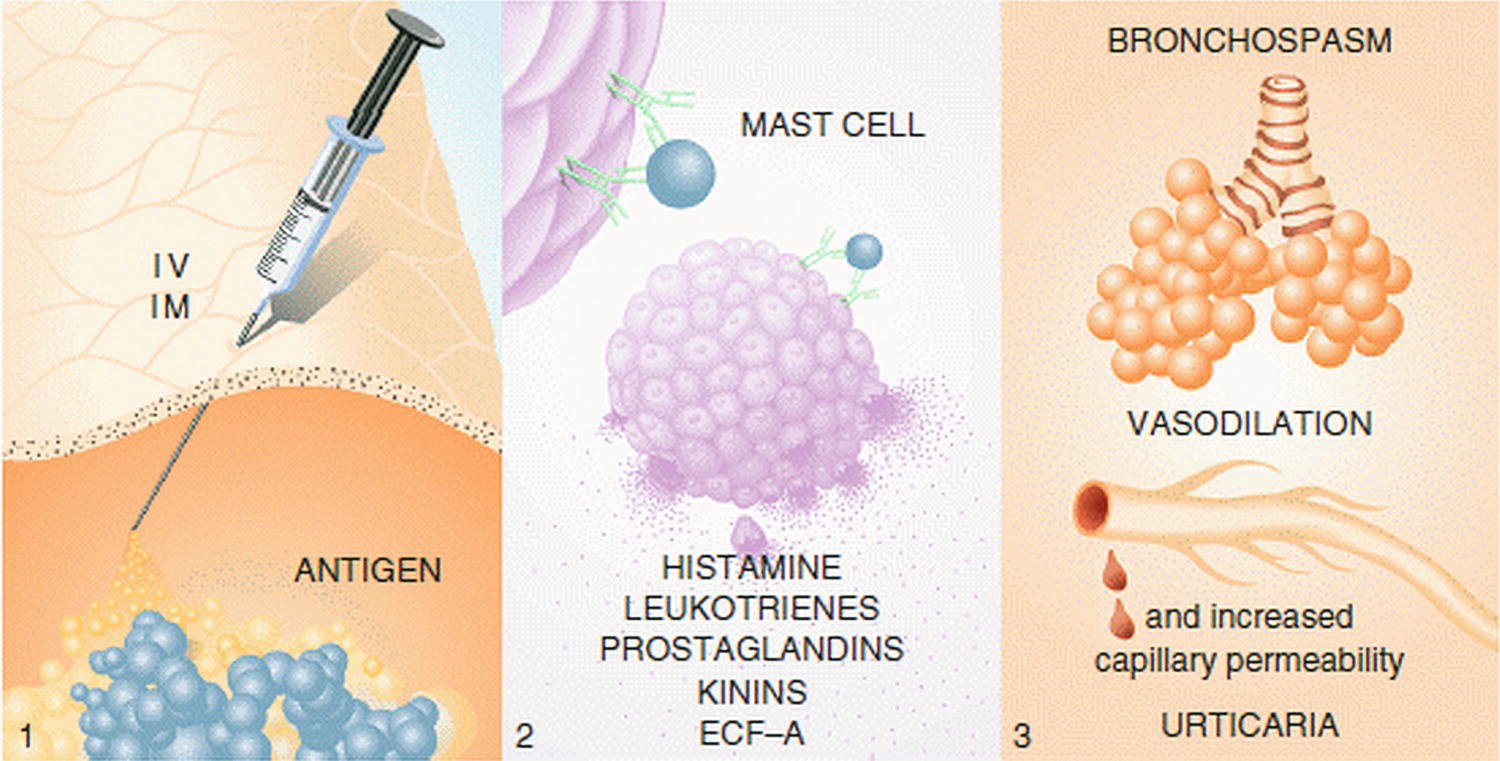
FIGURE 59.1. Physiology of allergic reaction. (Reprinted from Levy JH. Identification and Treatment of Anaphylaxis: Mechanisms of Action and Strategies for Treatment Under General Anesthesia. Chicago, IL: Smith Laboratories; 1983, with permission.)
Pathophysiology
Anaphylaxis is a specific type of allergic reaction that involves immunoglobulin E (IgE) antibodies interacting with a foreign antigen, causing mast cell and basophil degranulation. An antibody is a specific protein that can recognize and bind to a specific antigen. An antigen is a molecule (or molecule-protein complex) that is capable of stimulating an immune response. An initial exposure to an antigen (e.g., various drugs, latex, prep solutions) is needed to produce sensitization, which is the production of specific antibodies to this specific antigen by cells called plasma cells. These IgE antibodies attach to the surface of specific immune cells called mast cells (in the tissues) and basophils (in the circulation). On reexposure to this foreign antigen, these specific IgE antibodies (on the immune cells) bind to the antigen. Cross-linking of the IgE antibodies occurs, causing the mast cells and basophils to degranulate and release preformed inflammatory mediators, such as histamine, tryptase, and chemotactic factors. This degranulation activates a systemic inflammatory cascade with further release of leukotrienes, prostaglandins, kinins, and cytokines. These released mediators cause the systemic clinical manifestations of anaphylaxis.
There are other immune reactions to antigens that can occur that do not involve IgE antibodies, but do involve the release of histamine and other inflammatory mediators from mast cells. This is called non–IgE-mediated histamine release (anaphylactoid) and can involve other types of antibodies (IgG, IgM) and inflammatory mediators (complement). It is also possible for a drug, without an antibody interaction, to directly interact with the mast cell and cause histamine release. The amount of histamine released is related to the total dose of the drug and how rapidly it is given. An example of a drug that can do this is vancomycin. This effect for some drugs can be lessened by giving the drug slowly and carefully by using a timed infusion pump.
The physiologic response to the release of the mediators of anaphylaxis includes smooth muscle spasm in the respiratory bronchial tree and in the gastrointestinal tract; increased mucous production and airway edema; increased vascular permeability, with capillary leak and tissue edema resulting in intravascular volume loss (in some cases, up to 30% of the circulating blood volume); and vasodilation. The vasodilation and intravascular fluid loss result in decreased venous return of blood to the heart. The effect of these physiologic changes can produce hypotension with poor tissue perfusion (shock), cardiac dysfunction, life-threatening arrhythmias, and bronchospasm with oxygenation and ventilation difficulties. The clinical syndrome produced by anaphylactic and anaphylactoid reactions can be similar; however, anaphylactic reactions tend to be far more severe.
Clinical Manifestations of Anaphylaxis
The clinical manifestations of anaphylaxis can vary (Fig. 59.2). In an awake patient, the patient may complain of respiratory symptoms, such as difficulty breathing, nasal congestion, and chest discomfort; skin rash and itching; or cardiovascular symptoms such as dizziness and a sense of impending doom. Patients may have nausea or vomiting and abdominal cramps. Vital signs may show tachycardia, hypotension, and a rapid respiratory rate with noisy labored breathing. Objectively, the patient may have skin flushing and/or a rash. There may be difficulty breathing from laryngeal edema or wheezing from bronchospasm.
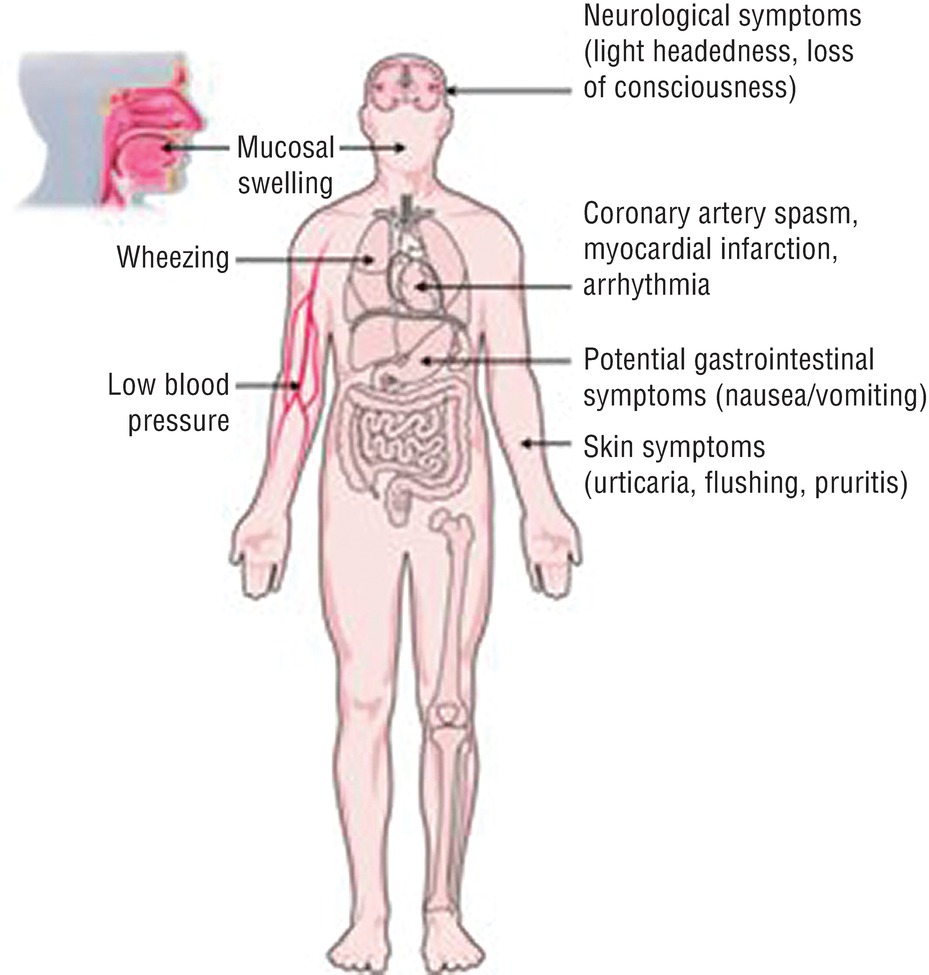
FIGURE 59.2. Clinical syndrome of anaphylaxis. (Reprinted from Miller MD, Chhabra AB, Konin J, et al. Sports Medicine Conditions: Return to Play: Recognition, Treatment, Planning. 1st ed. Philadelphia, PA: Wolters Kluwer; 2013, with permission.)
Under anesthesia, however, the initial signs of anaphylaxis may be cardiovascular collapse, with low blood pressure and either a rapid or slow heart rate. These early signs are frequently attributed to other causes leading to confusion in the actual diagnosis. Bronchospasm may occur, making ventilation difficult, with subsequent hypoxia. The end-tidal carbon dioxide level will increase, causing a respiratory acidosis. Both acidosis and hypoxia, in combination with hypotension and poor perfusion, can lead to myocardial depression and cardiovascular collapse. Cutaneous signs of allergy, such as urticarial rash or skin flushing, may not be present or appreciated under anesthesia, as an anesthetized patient cannot report itching, and the patient is covered by drapes.
It is important to appreciate there is a spectrum of clinical presentation associated with anaphylaxis. A patient may not present with all of these symptoms, and the severity of symptoms may vary. The most life-threatening presentation is hypotension and cardiovascular collapse. The incidence of anaphylaxis under anesthesia is hard to estimate, but ranges from 1/3,500 to 1/20,000, with a mortality rate between 3% and 6%. The most common clinical features of anaphylaxis under anesthesia were cardiovascular symptoms (74%), cutaneous symptoms (70%), and bronchospasm (44%).
Triggers of Perioperative Anaphylaxis
During the course of anesthetic care, multiple drugs are given over a relatively short period of time. With the induction of general anesthesia, it is not uncommon for five or more drugs from different classes, with different chemical structures and mechanisms of action, to be given together in succession. The majority of anaphylactic reactions will occur within the first 10 minutes after the drug is given. The patient is at the highest risk for an anaphylactic reaction just after the induction of general anesthesia, at a time when there is a lot of distracting activity in the operating room. Other conditions can present with similar symptoms, such as a relative anesthetic overdose with hypotension, wheezing after intubation from light anesthesia, or a vasovagal reaction. These conditions are known and anticipated, and they are treated routinely by the anesthesia provider. It is when the usual adjustments and medications are not correcting the situation readily, and the hypotension or bronchospasm is persistent, that the anesthetic team must consider the diagnosis of anaphylaxis and quickly initiate the treatment.
After an anaphylactic reaction, it is often unclear which drug was the offending agent. Patients can be referred later to allergy centers to be tested for antibodies to specific drugs that were given perioperatively. This allergy testing referral system is fairly developed in Europe and less developed in the United States. According to the European literature, based on information gathered from preoperative allergy testing centers, the most common triggers of anaphylaxis under anesthesia are muscle relaxants (69%), latex exposures (16%-20%), and antibiotics (15%).
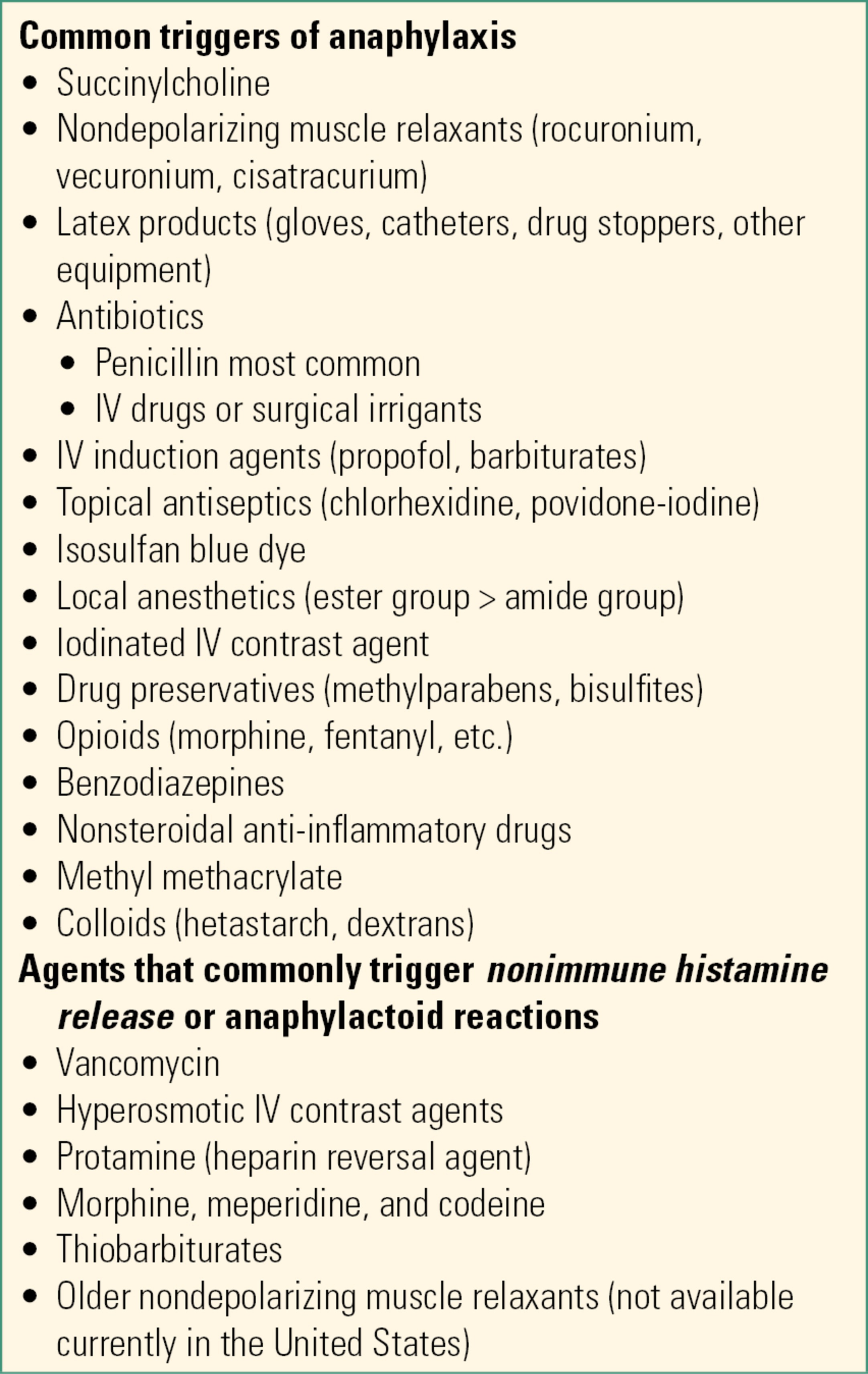
Known triggers of anaphylaxis in the perioperative period are listed in Table 59.1.
Table 59.1. Known Triggers of Anaphylaxis in the Perioperative Setting
Treatment of Perioperative Anaphylaxis
Early and prompt treatment can avert a major reaction. The initial treatment for anaphylaxis is as follows:
1. Stop the administration of the suspected antigen to limit further activation of mast cells.
2. Administer 100% oxygen, and provide airway support. Urgent intubation may be required: patients may have a progressively difficult airway due to airway swelling.
3. Anesthetic team must communicate with the surgeon and surgical team, and call for help.
4. Administer epinephrine IV early in the resuscitation to treat hypotension and bronchospasm. The epinephrine dose is titrated to effect. Epinephrine is given as graded boluses; however, an epinephrine infusion may be necessary.
- Epinephrine acts as a vasoconstrictor, inotrope, and bronchodilator and acts to stabilize mast cells to prevent further mast cell degranulation.
5. Anesthetic drugs should be stopped if the patient is significantly hypotensive. Scopolamine IV can provide amnesia without adding to vasodilation and hypotension.
6. Give volume resuscitation to treat hypovolemic shock. Placement of large-bore IVs and warmed fluids (crystalloids/colloids) with boluses of 2-4 L may be needed acutely.
7. Vasopressin may be added to the epinephrine to treat refractory shock (boluses, infusion).
8. Administer antihistamines. They do not prevent histamine release, but compete with histamine at histamine receptors, and lessen the effect of circulating histamine.
9. Administer corticosteroids (hydrocortisone, methylprednisolone), which act as anti-inflammatory agents.
10. Consider bronchodilators other than epinephrine if the patient continues to have bronchospasm once cardiovascular symptoms are treated.
11. Consider sodium bicarbonate for severe metabolic acidosis.
12. Draw and send a red-top tube to the laboratory to measure the serum tryptase level 30 minutes to 2 hours after the suspected anaphylactic reaction. A positive level is confirmatory for mast cell degranulation and an immune reaction as part of the etiology of a hypotensive event.
13. Consider invasive monitors such as an arterial line to monitor beat-to-beat blood pressures and measure arterial blood gases (assess oxygenation, ventilation, and acid-base status), central venous line to guide intravascular volume resuscitation, transesophageal echo to assess cardiac filling and function, and urinary catheter to follow urine output.
14. Provide postresuscitation supportive care, which may include disposition to the intensive care unit (ICU) for continued care and monitoring. The patient should be transported with full monitoring, possible sedation, and ventilation support.
15. Patient symptoms should be resolving and vital signs stable, as well as a careful airway evaluation should be performed before extubation.
16. Relapses are possible.
Prevention
It is important that all patients have an up-to-date allergy history recorded in their medical record. The anesthesia team must review and remain aware of known patient allergies and prior adverse reactions to drugs and substances. Offending agents should be avoided with alternative agents used, if possible. Formal allergy testing should be considered for patients that are suspected of having immune reactions to drugs that have no acceptable substitute or for drugs that may be necessary for their medical care in the future. Preoperative screening tests for patients to detect drug allergies are currently not practical due to expense and due to the fact that the available screening tests are not completely reliable. Maintaining a latex-free perioperative environment is the only way to prevent anaphylaxis to latex. The anesthesia team must be aware of equipment and products in the operating room environment that may contain latex. Examples include surgical gloves, drug vial stoppers, and catheters. Most operating rooms are moving toward the goal of a completely latex-free environment. Using a small amount of drug as a “test dose” to see if the patient will react is not necessarily safe, as anaphylaxis is not a dose-dependent reaction: a small amount of antigen can still trigger anaphylaxis. Pretreating patients with antihistamines and steroids before administering a questionable drug will not prevent histamine release in the event of an anaphylactic reaction.
Anaphylaxis and the Anesthesia Technician
Anesthesia technicians play an important role in any operating room emergency. They will be called upon to assist with airway management vascular access and other important tasks. Anaphylaxis can quickly (within minutes) escalate into a crisis with cardiovascular collapse and even cardiac arrest. The treatment options outlined above can guide the priorities and equipment needs of the anesthesia team (Table 59.2).
Table 59.2. Goals and Anesthesia Technologist Support in OR Anaphylaxis Emergency

Summary
Anaphylaxis is a true medical emergency. The onset can be rapid and potentially deadly even if the patient is young and otherwise previously healthy. Prompt recognition and treatment are essential for the best patient outcome. The anesthesia technician can play a key role in the successful resuscitation of a patient by providing timely, efficient, and thoughtful technical assistance to the anesthesia team. Understanding information about the syndrome of anaphylaxis and the rationale for its treatment will help the anesthesia technician better anticipate and support the acute needs of the anesthesia team.
Review Questions
1. Anaphylaxis can typically present with the following symptoms:
A) Hypertension and bronchospasm
B) Hypotension and fever
C) Hypotension and bronchospasm
D) Bronchospasm and muscle rigidity
E) None of the above
Answer: C
Fever and muscle rigidity are typically not features of anaphylaxis. The release of inflammatory mediators leads to capillary leak, with resultant vasodilation and hypotension; there is also smooth muscle spasm with resultant bronchospasm.
2. During an anaphylactic reaction, tryptase is released by
A) Basophils
B) Capillary endothelium cells
C) Mast cells
D) Lung alveolar cells
E) A and C
Answer: E
Tryptase is a specific marker for mast cell and basophil degranulation. Elevated tryptase levels after an event can be diagnostic of an anaphylactic reaction.
3. The first step in the treatment of anaphylaxis is
A) Place two large-bore IVs and give 2 L of IV fluids quickly.
B) Administer IV steroids, such as dexamethasone.
C) Give epinephrine bolus for low blood pressure.
D) Give IV antihistamines.
E) Stop the administration of suspected triggering drug, give 100% oxygen, and manage the airway.
Answer: E
Discontinuing the suspected triggering agent and ensuring an open airway and oxygenation come first. Supporting the circulation with volume administration and epinephrine comes next. Use of antihistamines and steroids is considered to be secondary treatment.
4. Initial treatment for bronchospasm associated with anaphylaxis includes
A) Vasopressin IV
B) Dexamethasone IV
C) Epinephrine IV
D) Antihistamines
E) None of the above
Answer: C
Epinephrine is a mixed α- and β-agonist and affects β2-receptors in the bronchial tree to cause bronchodilation. Vasopressin is a direct-acting vasoconstrictor used to treat hypotension. Dexamethasone is a steroid with anti-inflammatory properties but a slow onset of action. Antihistamines compete with histamine at histamine receptors and will eventually decrease the adverse effects of histamine.
5. The most common triggers of anaphylaxis under anesthesia are
A) Latex, propofol, and muscle relaxants
B) Muscle relaxants, iodine prep, and antibiotics
C) Antibiotics, latex, and iodine prep
D) Muscle relaxants, antibiotics, and latex
E) Antibiotics, latex, and narcotics
Answer: D
All of the above substances have been reported to cause anaphylaxis in the perioperative period. However, statistically, muscle relaxants, antibiotics, and latex accounted for the majority of the cases.
6. Choose the statement that is FALSE:
A) Allergic reactions can occur anytime a patient is exposed to a drug.
B) Histamine release can cause vasodilation and hypotension.
C) True anaphylaxis involves IgE antibodies.
D) Epinephrine acts to destabilize mast cells, affecting their ability to degranulate.
E) Vasopressin is useful in treating the hypotension associated with anaphylaxis if the patient is unresponsive to epinephrine.
Answer: D
Epinephrine acts to “stabilize” mast cells and prevent further degranulation of mast cells. All of the other statements are true.
SUGGESTED READINGS
Galvao VR, Giavina-Bianchi MC. Perioperative anaphylaxis. Curr Allergy Asthma Rep. 2014;14:452.
Hepner D, Castells MC. Anaphylaxis during the perioperative period. Anesth Analg. 2003;97:1381-1395.
Kannan JA, Bernstein JA. Perioperative anaphylaxis: diagnosis, evaluation, and management. Immunol Allergy Clin North Am. 2015;35:321.
Levy JH, Ledford DK. Perioperative Anaphylaxis: Clinical Manifestations, Etiology, and Management. Wolters Kluwer; 2017. Available from: www.uptodate.com.
Mertes PM, Tajima K. Perioperative anaphylaxis. Med Clin N Am. 2010;94:761-789.
Schummer C. The pivotal role of vasopressin in refractory anaphylactic shock. Anesth Analg. 2008;107(2): 620-624.