CHAPTER 61
Fire Safety
Introduction
A fire that occurs in the operating room (OR) area is an obvious emergency with potentially devastating consequences. It poses a threat to all who are present in the OR, including patients, surgeons, anesthesiologists, nurses, and other staff. Patients are especially vulnerable because they are unable to flee, seek shelter, or take any steps to protect themselves. Prevention is arguably the single most important step to ensure fire safety. Fire prevention and the response, should a fire occur, are everyone’s responsibility. This chapter reviews fire prevention strategies, including an overview of how OR fires start and steps to reduce or eliminate the possibility that a fire will occur, the consequences of a fire in the OR, and actions to take in the event a fire should occur in the OR.
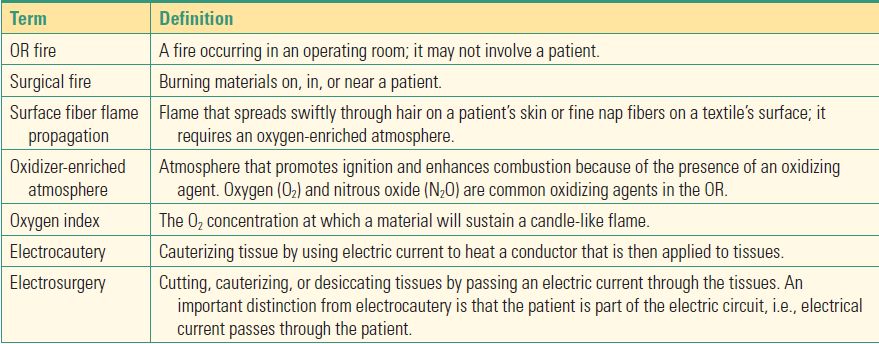
Several different types of fires can occur in the OR. These are broadly classified as airway fires, surgical fires, and OR fires (Table 61.1). Fires can also occur elsewhere in the facility. Airway fires occur in the airway, surgical fires occur elsewhere on the patient’s body, and OR fires take place elsewhere in the OR and do not directly involve the patient. Current estimates indicate that approximately 600 fires occur in the OR each year. However, this is likely to be an underestimate, since reporting requirements vary from state to state and many fires are unreported. About a third of fires occur in the airway, with ignition of an endotracheal tube (ETT), usually by electrosurgical instruments or a laser. Another quarter of fires involve the face, often during head and neck, ophthalmic, or plastic surgical procedures on the face or nearby areas; another quarter occur on other parts of the body. These commonly result from ignition of OR materials, such as surgical drapes. About 15% of fires occur inside the body, the result of igniting intestinal gases, for example, when the bowel is entered using an electrosurgical device. OR fires can result in thermal injuries (burns) that cause direct injury to skin and underlying tissues and smoke inhalation that results in lung injury and respiratory compromise.
Table 61.1. Terminology Related to Fire Safety and Prevention
Preventing and Responding to Fires: General Principles
The Fire Triangle
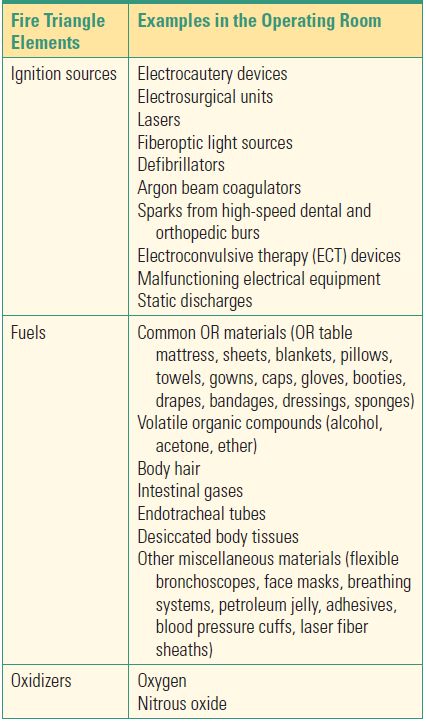
Fires in the OR can arise from a variety of sources, but all fires share one common characteristic: three elements must be present for a fire to occur. This is known as the fire triangle (Fig. 61.1). For a fire to occur, there must be a fuel, an ignition source, and an oxidizer (Table 61.2). Preventing OR fires essentially comes down to eliminating one or more elements from the fire triangle. For example, limiting the amount of oxygen (and nitrous oxide) will eliminate the risk of combustion in many circumstances. Alternatively, eliminating the fuel, such as removing an ETT from the airway during laser surgery, or the source of heat, such as ensuring that fiberoptic light sources are not placed on surgical drapes, will also prevent a fire from occurring.
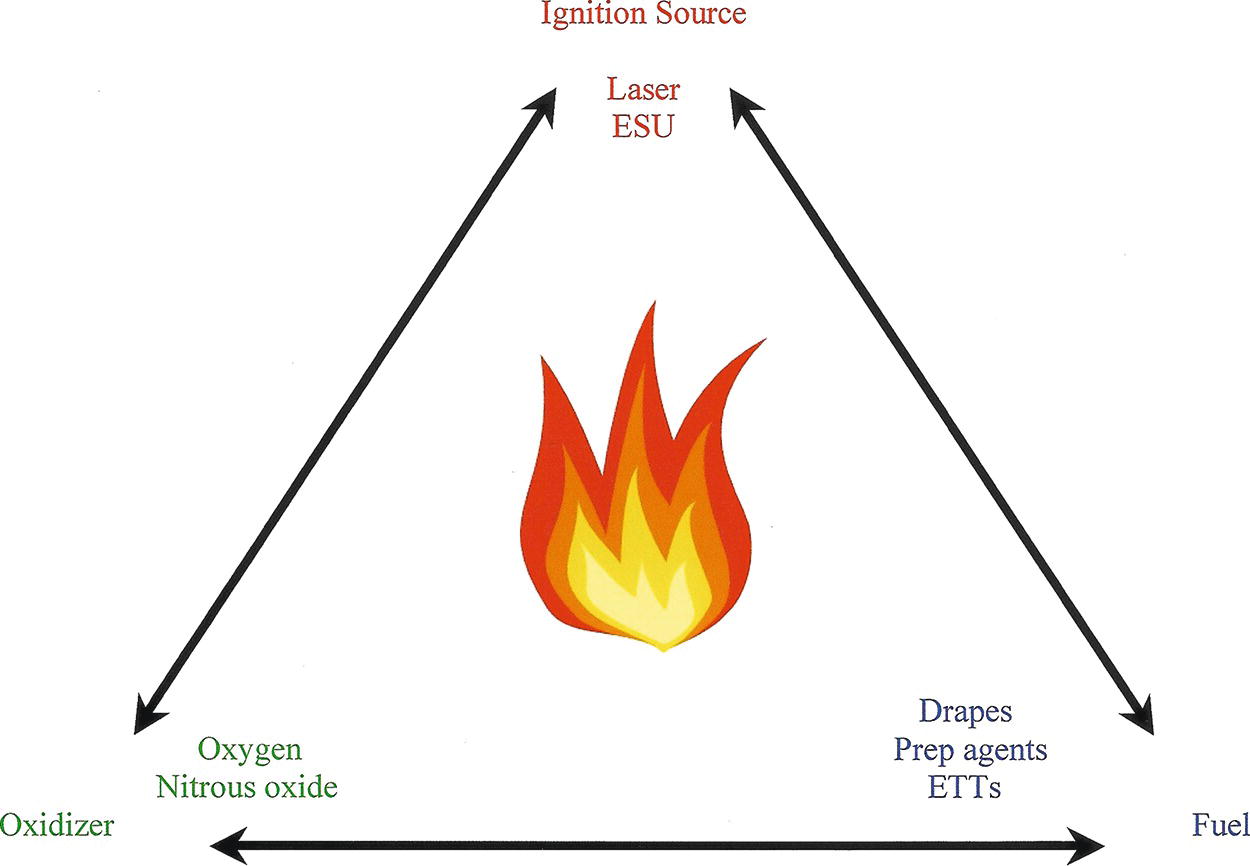
FIGURE 61.1. The fire triangle (also known as the fire triad). All three elements of the triangle must be present for combustion to occur. ESU, electrosurgical unit; ETT, endotracheal tube.
Table 61.2. The Three Elements of the Fire Triangle, with Examples of Each That Are Present in the Operating Room
Fire Prevention
Preventing an OR fire depends to some extent on the specific type of fire being considered. For example, preventing an airway fire involves different factors than preventing ignition of surgical drapes. Nonetheless, they all share some common factors, relating to the roles of the different parts of the fire triangle. Removing any element of the fire triangle will successfully eliminate the risk of a fire. For example, by not creating an oxygen-enriched atmosphere under surgical drapes, a fire can be prevented by eliminating the oxidizing agent. Similarly, safe practices involving the use of ignition sources, such as lasers, or taking steps to keep fuels wet, such as soaking gauze pads used in the pharynx, markedly reduce the risk of a fire in the airway.
Each element of the fire triangle generally falls within the scope of different OR staff, but best practice requires that everyone who is in the OR assumes responsibility for any and all aspects of fire prevention. Surgeons are usually the ones involved in the use of ignition sources, while anesthesia providers are typically in control of oxidizing agents and nursing staff are primarily concerned with the fuel sources in the OR. There is some overlap of responsibilities, however. For example, certain fuel sources, such as ETTs, are the anesthesia provider’s responsibility, surgeons sometimes apply prep agents, and nurses often participate in controlling lasers and electrosurgical units. As such, good communication practices and teamwork are essential aspects of fire prevention. Even with these general steps to prevent OR fires, through attention to the various parts of the fire triangle, there are also specific steps that depend largely on the type of equipment being used, such as the type of ignition source being considered (electrosurgical instrument vs laser), or the type of surgery being performed (airway vs nonairway).
Responding to a Fire
The generic response to a hospital fire is encapsulated in the acronym RACE: Rescue, Alarm, Contain, and Evacuate (or Extinguish). The first priority is to rescue the patient, removing him or her from the dangerous situation. Several rescuers will likely be needed. However, it is not recommended that rescuers place themselves at severe risk. Second, sound the alarm; alert others as to what is happening. Nearby staff should be aware of what is happening and kept informed in case they will need to evacuate their patients. In addition, fire alarm systems should be activated. Often, these will summon assistance from within the facility and may also call the fire department. Next, efforts should be made to contain and control the situation, such as by closing fire doors. Medical gas valves should be shut off, and air duct dampers can help to prevent the spread of smoke. Central smoke evacuator systems (used to remove surgical smoke) should also be shut off. Also, electrical power should be shut off at the circuit breaker panel, as this will prevent electrical fires from being sustained and reduce the risk of an electrical shock. Finally, an attempt may be made to extinguish the fire; however, it may be necessary instead to first evacuate patients and any personnel from the area. The evacuation should be orderly and patients taken to a preplanned area. Note that these steps may occur nearly simultaneously.
In the OR, the response may be somewhat different, however, depending on the specific type of fire. It will also depend on the extent of the fire. Does it involve only the patient (as most surgical fires do) or a single OR room? Is the entire suite of ORs involved, or the larger facility, such as a hospital or freestanding surgical center?
There are several consequences to a fire in the OR. The risk of injury has already been mentioned. In addition, there are costs due to damage from the fire: damaged equipment and facilities, for example. There is also the impact on OR operations, including whether they can continue on that day or whether damage has been extensive enough to curtail operations for an extended period of time.
The response to a fire in the OR will depend on the type of fire. Each of these will be considered separately below, although it may not be possible to specify every possible type of fire that can occur in the OR. Regardless, if any type of fire occurs, it should be quickly announced so that the entire surgical team is aware that there is a fire. The easiest fire to deal with is one that is small and confined to a specific area, for example, a gauze pad that has been ignited. If the fire is not on the head or neck, and the full extent of the fire is easily seen, it is reasonable to pat it out or smother it with a gloved hand or towel, thus extinguishing it. It is still important to check for embers or smoldering materials that could reignite, especially if there is a possibility of an enriched oxygen atmosphere.
Preventing and Responding to Fires: Specific Situations
Airway Fires
An airway fire is one of the most concerning, and most common, fires that can occur in the OR. Airway fires start when an ignition source, usually a laser or electrosurgical device, is used to perform surgery in the airway in the presence of an ETT (fuel source) and an enriched oxygen (or oxygen/nitrous oxide) atmosphere. Typical situations in which an airway fire will occur include laser surgery of airway lesions or tracheostomy. Several methods for minimizing the risk of igniting an airway fire have been promulgated and are listed in Table 61.3. One of the most important is the use of a laser-resistant ETT with the cuff filled with saline, rather than air (see Chapter 55, Laser Safety). Airway fires produce a thermal injury from the blowtorch-like flame that comes out from the end of the ETT and injury to the lungs from the toxic products of combustion of the ETT (Fig. 61.2).
Table 61.3. Recommended Practices to Help Prevent an Airway Fire, Grouped According to the Cause of Ignition
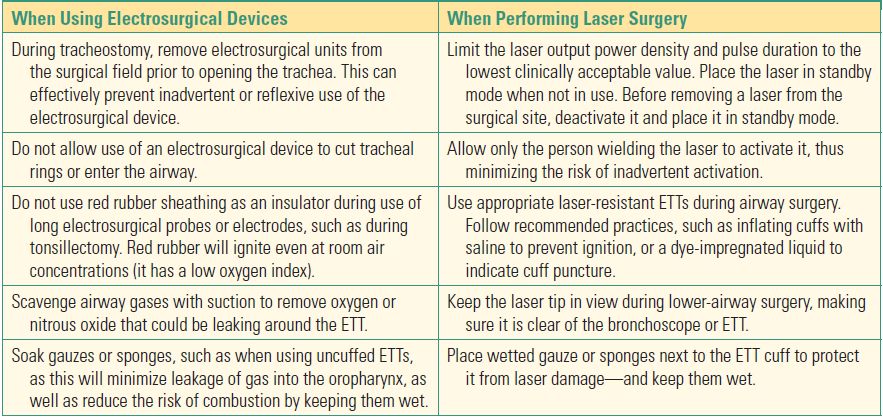

FIGURE 61.2. Ignition of an ETT results in a fire that resembles a blowtorch. What cannot be appreciated from the photo are the acrid products of combustion, which can significantly impair respiratory function.
Airway fires require immediate action to prevent or minimize patient injury. Most importantly, the supply of oxygen to the ETT must be removed. This can be accomplished by disconnecting the breathing circuit or by turning off the flow of oxygen, such as at a flowmeter. This will immediately extinguish the fire. Simply dousing the ETT with water is not sufficient, as such fires can continue to burn underwater (Fig. 61.3). As soon as the oxygen supply is eliminated or, ideally, at the same time, the ETT must be removed from the airway. In addition, any other material in the airway should be removed. Any material removed from the airway should be extinguished with water or saline in a basin or sink or with a wet towel; otherwise, there is a risk of igniting drapes or other flammable matter. Care must be taken to not use a flammable liquid such as alcohol that might be present in or near the surgical field. A quick airway exam should then be performed to check for smoldering embers or other materials that could reignite once a new ETT is placed and oxygen flow resumes. Saline or water can be poured into the airway to extinguish any remaining burning material. Once this is done, a new ETT can be placed in the airway. Use room air until it is absolutely certain nothing is burning. As oxygen is reintroduced, attention must be paid to whether any ignition takes place. As already mentioned, any embers or other ignition sources remaining in the airway can reignite the fire once oxygen begins to flow again. At this time, a more thorough inspection of the airway can be conducted, carefully assessing the extent of injury.
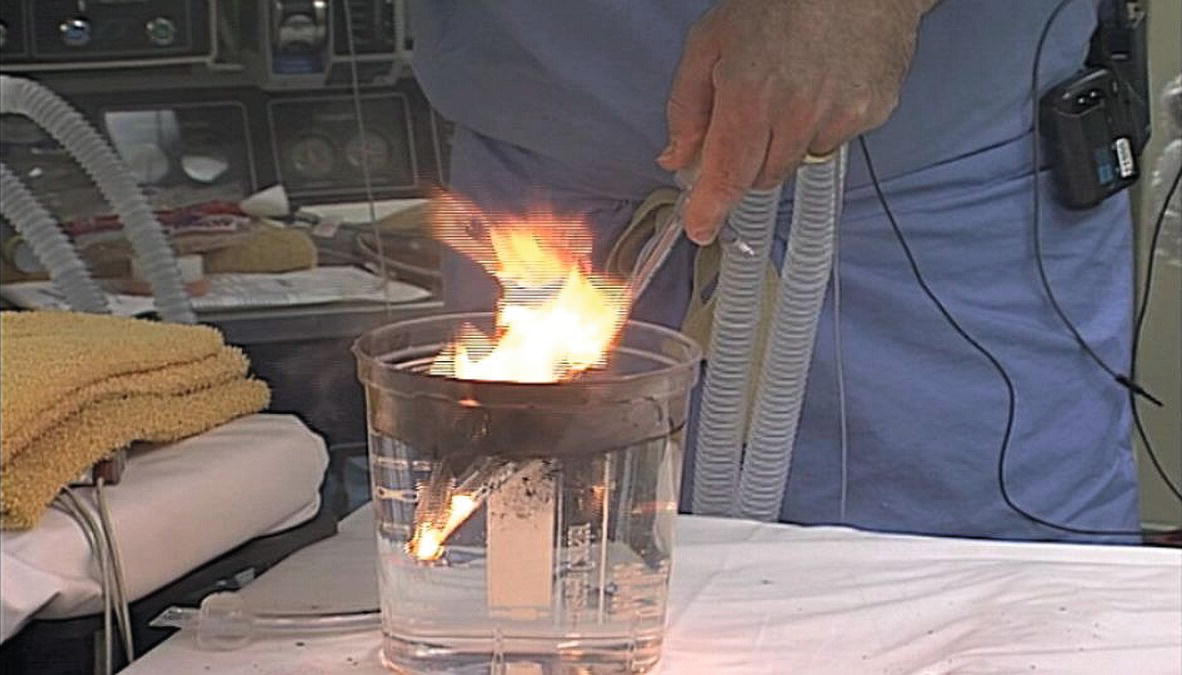
FIGURE 61.3. An ETT on fire continues to burn, despite being submerged underwater. Note the fire present within the portion of the tube that is below the surface of the water.
Surgical Fires
A surgical fire is defined as one that directly affects the patient and involves the ignition of surgical drapes or other flammable materials, such as gauze or towels. It can occur in a variety of situations and, once ignited, can spread rapidly to other areas of an OR. A surgical fire may then extend beyond the room in which it began. If not immediately managed, it poses a threat to all present.
Lasers or electrosurgical devices can ignite a surgical fire. In addition, the tip of a light cord, such as from a headlamp or laparoscopic instrument, can be very hot. When placed on top of surgical drapes, it may also ignite a fire, usually in the presence of an oxygen-enriched atmosphere. Many operations are performed under sedation with supplemental oxygen provided by a face mask or nasal cannula. Because of the potential accumulation of oxygen under the drapes, these cases have a higher risk of a fire than those that do not use supplemental oxygen. This is particularly true when the surgery is on the face, near the supplemental oxygen supply. Finally, alcohol-based surgical prep solutions may remain on the patient and can ignite. Surgical fires can often be prevented through a combination of education and awareness on the part of OR staff, as well as implementation of recommended practices to reduce the likelihood of accidentally igniting a fire (Table 61.4).
Table 61.4. Recommended Practices That May Reduce the Risk of an OR Fire
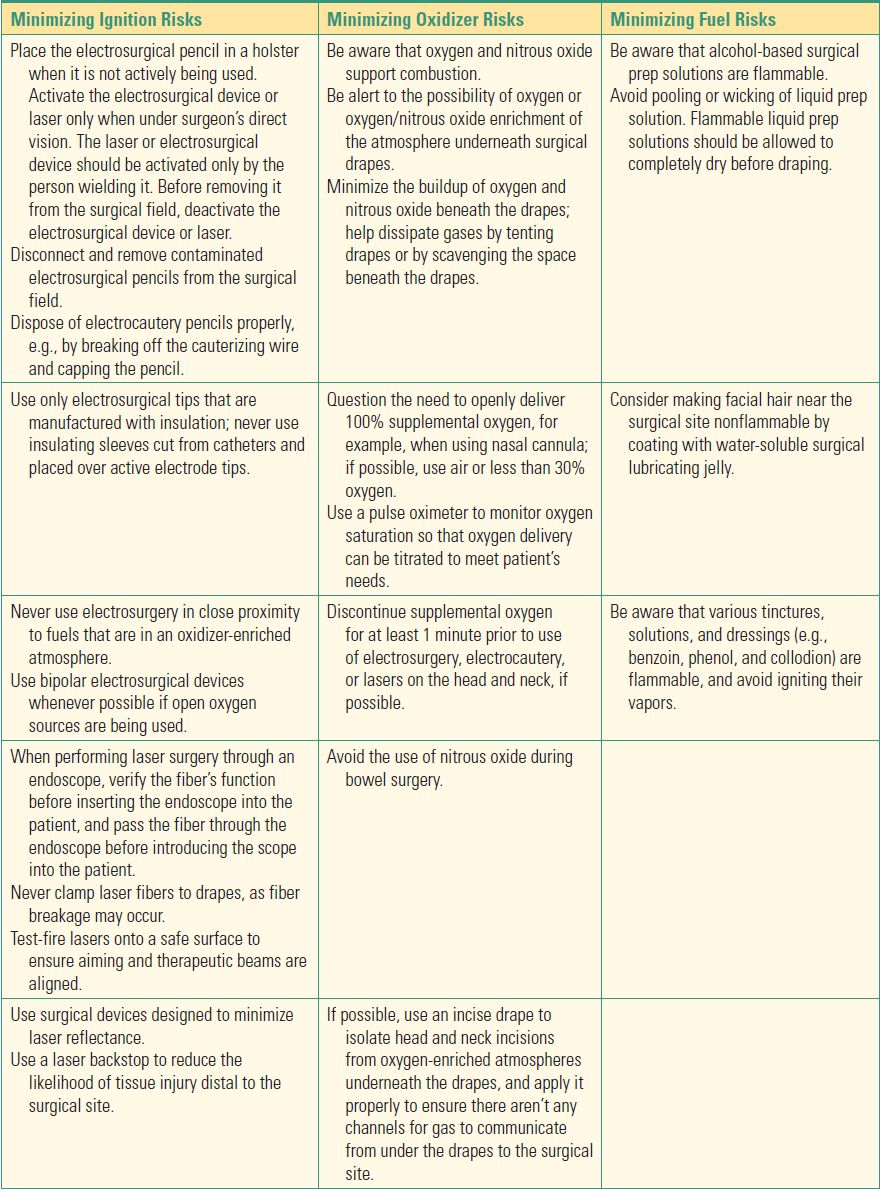
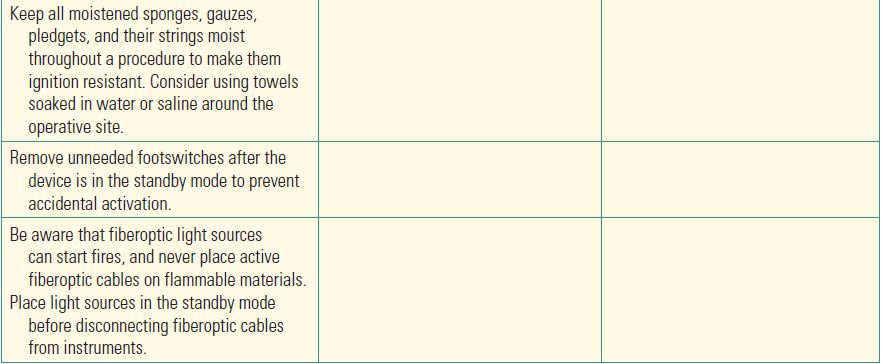
These recommendations are grouped according to whether they affect the risk from an ignition source, oxidizer, or fuel.
While a small, confined fire may be extinguished by the prompt action of a single person, for example, the surgeon or scrub nurse, oftentimes a surgical fire will generally require a coordinated response by numerous persons to control it, to keep it from spreading, and finally to extinguish it. In this situation, any staff present can contribute to successful management of this emergency. As with an airway fire, the first step is to immediately stop the flow of all airway gases to the patient. At the same time, immediately remove any burning material from the patient. Stopping the flow of airway gases will often cause the fire to go out or at least burn less intensely. Rapidly removing the burning material is the only way to protect the patient from the fire. In addition, the fire could reignite if oxidizers are reintroduced. A team member should be ready to extinguish the burning materials. If needed, a carbon dioxide (CO2) extinguisher should be used. It is important to note that surgical fires can spread extremely rapidly, and usually there will not be time to retrieve and use an extinguisher. Therefore, getting a fire extinguisher should not be an initial response, and one should be used only after other steps have been taken. Nonetheless, it is still important to know the location of fire extinguishers in the OR area, as well as their proper use.
The next step is to care for the patient, with resumption of ventilation, control of bleeding, and examination and treatment of any injuries. This should be done swiftly, as the patient may not be spontaneously breathing, may have severe bleeding, and may still be in contact with other burning materials. Initially, the anesthesia provider should use air when resuming ventilation until all possible sources of fire or reignition are out. The surgeon will need to attend to any patient injuries, and the nursing staff should help to extinguish any remaining burning materials, whether they are still on the patient or have been removed. If the room presents a danger from smoke or fire, the patient should be evacuated, in which case equipment will usually be needed to provide ventilation (resuming supplemental oxygen only after all fire is confirmed extinguished), an anesthetic, and monitoring. If the fire is not rapidly controlled, OR suite staff must be alerted and the fire department contacted and the room isolated to contain the smoke and prevent or slow the fire’s spread. Electrical power and medical gases to the room should be shut off.
OR Fires
An OR fire involves the ignition of material in the OR, but it does not necessarily immediately involve the patient. For example, an OR fire can be caused by improper disposal of an electrocautery device that ignites flammable material in a trash container. Even if an OR fire does not initially involve the patient, if it is not quickly contained and extinguished, it may well spread rapidly and threaten patients and staff. The response to an OR fire should be similar to that of a surgical fire. It may be necessary to halt the flow of oxygen and nitrous oxide. Preparations should begin to remove the patient from the room, if the fire cannot be promptly contained and extinguished. A CO2 fire extinguisher should be used to extinguish the fire, OR suite staff should be notified of the fire, and steps should be taken to limit the spread of the fire and smoke.
Fires Elsewhere in the Facility
A fire that exists outside the OR area, but within or near the facility, may not pose an immediate threat, but the danger is still imminent. It may still be necessary to halt operations or transfer patients. Smoke may enter the OR area and interfere with procedures, for example, or there may be a risk that the fire will spread into the OR. Making sure that fire doors are closed will help limit the risk, at the very least slowing the progression of the fire into new areas. If patient evacuation is necessary, the same steps as noted above will need to be taken.
The Role of the Anesthesia Technician
Fire prevention is the responsibility of every individual working in the OR. It cannot be emphasized enough that it is a team effort, nor that the single most important aspect of fire safety is fire prevention. Given that, perhaps the most important role for an anesthesia technician in fire safety is to participate as a member of an alert OR team in identifying safety hazards and helping institute steps to rectify them. For example, if it is observed that oxygen is being provided by nasal cannula in such a way that it can accumulate under drapes during facial surgery, and without regulating the delivered concentration of oxygen (i.e., open delivery of 100% supplemental oxygen), a gentle reminder to point out recommended best practice (delivered oxygen concentration should be kept below 30%) would be reasonable and might avert a catastrophe. In addition, there are a number of specific ways in which an anesthesia technician can be involved and help to reduce the risk of an OR fire. Understand the fire triangle and appreciate what constitutes a fuel, a source of ignition, and an oxidizing agent and recognize risky situations. The anesthesia technician can then be an informed member of the OR team, which can enhance participation in fire drills and rehearsing the response to a fire. Maintenance of equipment, for example, replacing or repairing frayed electrical cables, may prevent a stray spark that could ignite a fire. Placing signs and notices about hazards and recommended practices can provide important information regarding fire safety. Lastly, ensure that appropriate supplies are available, such as laser-resistant ETTs for laser airway surgery. It is appropriate for a technician to speak up in preparing a room for a booked laser case; “I see the nurses setting up the laser, do you want me to bring you a laser tube?” Safety is a team effort!
Effective response to a fire also requires everyone’s involvement. By understanding the concerns associated with a fire in the OR (or the facility), the response to an OR fire can be more effective and allow the technician to recognize issues and help in any way necessary. For example, in the event it is necessary to evacuate the OR, the anesthesia technician will need to provide oxygen sources and airway supplies, infusion pumps and intravenous medications, and monitors. It may be necessary to quickly disconnect the patient from equipment, such as the anesthesia machine and monitors and an electrosurgical unit. Transporting the patient may require moving him or her on the surgical table; since such tables are awkward to move, help will be needed. The following is a brief checklist for the anesthesia technician responding to a fire:
- Be prepared to transport an anesthetized patient.
- Gurney
- Airway supplies including self-inflating bag-valve-mask ventilation, oxygen supply, and reintubation supplies and equipment. Remember that it may not be appropriate to use supplemental oxygen in the presence of any potential embers or burning material; you will need an Ambu-style self-inflating system that can operate without supplemental gas flow until you are free of any fire area and can use an oxygen tank.
- Infusion pumps and anesthetic agents (e.g., propofol) to maintain anesthesia during transport
- Transport monitors
- Prepare to shut off oxygen to the room.
- Alert additional technicians to be prepared to transport multiple patients.
- Bring a CO2 fire extinguisher.
Fire extinguishers are rarely needed to extinguish a surgical fire. Historically, they have been needed in the rare instance when a fire engulfs a patient, has migrated off a patient, involves materials that continue to burn after being removed from a patient, or involves equipment. Nonetheless, it is essential to know where extinguishers are kept, as well as the different types of extinguishers (Table 61.5) and how to use them. While water-based, CO2, and dry powder extinguishers are all commonly available in the OR, the recommended extinguisher is a CO2 type.
Table 61.5. Different Types of Fire Extinguishers, Each Intended to Extinguish a Different Class of Fire
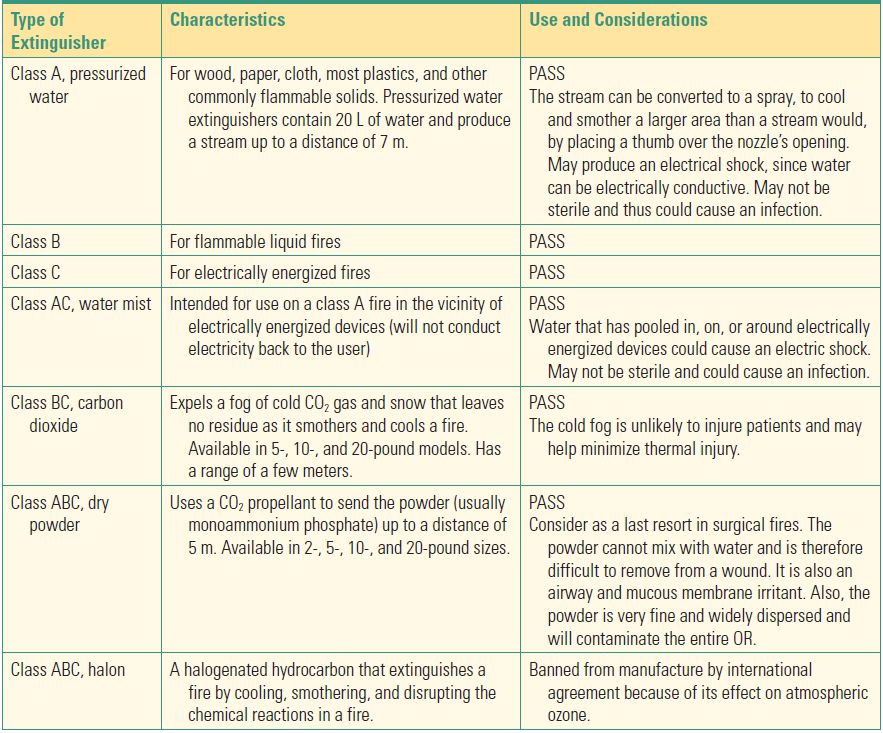
PASS—Pull the pin, Aim the horn or nozzle at the base of the fire, Squeeze the trigger, and Sweep from side to side to put out the fire.
Aqueous solutions can also be used to extinguish a fire, including bottled water or saline, or tap water, once burning material has been removed from a patient. Some institutions keep a bottle of saline, labeled “FOR FIRE,” in the room. However, surgical drapes are waterproof, and any water used to quench the fire may not reach the underlying burning material. Fire blankets (wool blankets treated with fire retardants) should not be used, for several reasons. If oxygen is being delivered to the patient and helping to sustain the fire, the blanket may not be effective. In fact, the blanket will burn in an oxygen-enriched atmosphere. In addition, the blanket may trap the fire next to or under the patient. Throwing a blanket on a patient may also displace surgical instruments. Either circumstance can result in additional injury.
In the aftermath of a surgical fire, an investigation will need to be conducted. It is important that the OR, as well as any and all material involved in the fire, be secured. Statements from staff involved in the fire should be obtained as soon as possible after the incident. Information derived from accurately reporting and documenting the event can benefit the facility and help to prevent a surgical fire from happening again. Operations, quality improvement, and risk management entities within your facility will likely participate (see Chapter 65, Legal and Regulatory Issues).
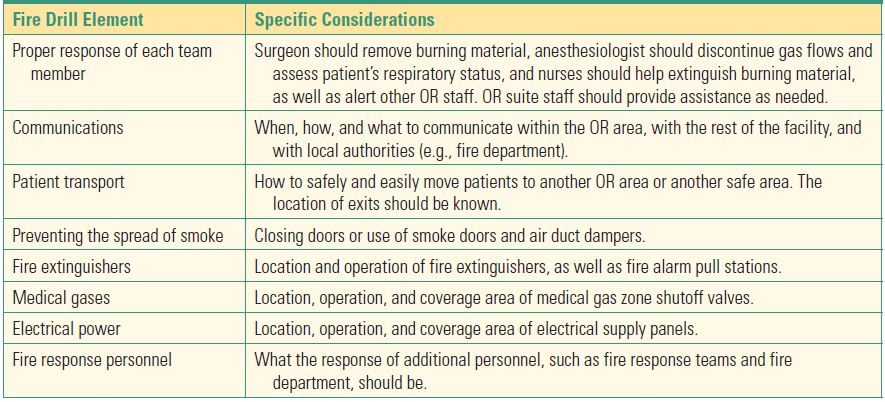
Fire drills are an important part of any attempt to fight an OR fire and should be conducted to help staff learn to plan and respond more expeditiously to a fire, as well as help the facility test the effectiveness of its fire plan. A number of things need to be considered when planning or conducting a fire drill (Table 61.6).
Table 61.6. The Various Aspects of a Fire Drill for the Operating Room
Summary
A fire in the OR can have devastating consequences for the patient and for OR staff. A rapid and coordinated response of OR personnel will be required to limit injuries to patients and staff and damage to the facility. The anesthesia technician is an important part of the OR team and should be prepared to respond to an OR fire. Initial steps involve stopping the flow of oxygen and removing burning material. The anesthesia technician should then be ready to assist with the resumption of ventilation and transport of an anesthetized patient, if necessary.
Review Questions
1. The three elements that are necessary for a fire to occur are
A) Fuel, flame, oxygen
B) Oxygen, fuel, paper
C) Fuel, ignition source, oxidizer
D) Electrocautery, sparks, oxidizer
E) None of the above
Answer: C
In order for a fire to occur, the three elements, or fire triangle, that need to be present are a fuel source, an ignition source, and an oxidizer, which can include oxygen or nitrous oxide.
2. RACE stands for
A) Remove, Alarm, Contain, Extinguish
B) Recover, Alarm, Cover, Evacuate
C) Rescue, Alarm, Contain, Evacuate
D) Respond, Alarm, Contain, Extinguish
Answer: C
Anesthesia technicians will be called upon in the event of a fire emergency in the OR. The RACE acronym describes, in order, the key steps to take during a fire emergency.
3. As an anesthesia technician, you may be asked to assist with various types of fire, which may include
A) Airway fires
B) OR fires
C) Surgical fires
D) Facility fire
E) All of the above
Answer: E
In a hospital setting, all of these types of fires are possible.
4. In the event of a fire in the OR, it is important to turn off the flow of oxygen, regardless of the oxygen saturation of the patient.
A) True
B) False
Answer: A
Shutting off the oxygen supply (removing the oxidizer part of the triangle) is important regardless of whether the fire is an airway fire, a surgical fire, an OR fire, or a facility fire. The continued flow of oxygen will sustain and even spread a fire, rapidly endangering not only the patient but also everyone in the room. In a surgical or OR fire, the patient can be ventilated with air while the fire is extinguished.
5. The recommended type of fire extinguisher for use in an OR is
A) CO2
B) Pressurized water
C) Halon.
D) Dry powder
E) None of the above
Answer: A
The recommended fire extinguisher for an OR is the CO2 extinguisher. CO2 extinguishers can be used for fires involving organic solids (e.g., paper, wood), flammable or combustible liquids (e.g., oil and grease fires), combustible metals, and cooking fat and oil.
SUGGESTED READINGS
ECRI Institute. New clinical guide to surgical fire prevention. Health Devices. 2009;38:314-332.
Smith TL, Smith JM. Electrosurgery in otolaryngology-head and neck surgery: principles, advances, and complications. Laryngoscope. 2001;111:769-780.