Therapeutic Potential of Flaxseed
Ankit Goyal; Ami Patel; Manvesh K. Sihag; Nihir Shah; Beenu Tanwar Mansinhbhai Institute of Dairy & Food Technology (MIDFT), Mehsana, Gujarat, India
Abstract
Flaxseed, also known as linseed, is one of the most prominent emerging functional foods. It has been reported that consumption of flaxseed helps in reducing the risks of cardiovascular diseases, rheumatoid arthritis, autoimmune, and neurological disorders. Several clinical and epidemiological studies have indicated that flaxseed oil, the richest plant source of omega-3 fatty acid, is also associated in reduction of dyslipidemia and chronic kidney diseases due to its antiinflammatory properties. A number of studies have shown that flaxseed proteins possess potential angiotensin I-converting enzyme (ACE) inhibitor activities, antioxidative, and antihypertensive properties. Similarly, several researchers have proven that flax fibers and lignans (secoisolariciresinol diglucoside, SDG) are positively associated for the treatment and prevention of obesity, bowel syndrome, and hormone-sensitive cancerous diseases. Ayurveda and traditional Chinese medicine share many common approaches and have a long history in the practice of using flaxseeds as a remedy of cough, skin, and gastro-intestinal disorders. Various nutraceutical preparations of flax and flaxseed oil, such as Essentiale, Lipostabil, Efamol, and Essaven are available in global market for the treatment of general fatigue, pain, atherosclerosis, eczemas, and different diseases. The purpose of this chapter is to delineate the recent findings of flaxseed on the physiological functionality of nutraceutical formulations, along with their applications in foods.
Keywords
Flaxseed; Dietary fibers; Nutraceuticals; Omega-3 fatty acids; Cardiovascular disease; Health benefits
1 Introduction
“Let food be thy medicine and medicine be thy food,” espoused Hippocrates, nearly 2500 years ago. This proclamation is receiving renewed interest about the health enhancing role of specific foods or physiologically-active food components, so-called functional foods, and nutraceuticals. Nutraceuticals, a scientific area generated all over the world, and a portmanteau of the words “nutrition” and “pharmaceutical,” is a food or food product that reportedly provides health and medical benefits, including the prevention and treatment of diseases.
Nutraceuticals are available in the form of isolated nutrients, dietary supplements, and specific diets of genetically engineered foods, herbal products, and processed foods, such as cereals, soups, and beverages. Nutraceuticals provide energy and nutrient supplements, which are required for maintaining optimal health, and are widely used in the food and pharmaceutical industries. Due to increased consumer awareness and the profound effect of nutraceuticals on human health, the global nutraceutical market was estimated to be $149.5 billion in 2011 with the United States, Europe, and Japan being the largest regional markets, accounting for nearly 93% of the global nutraceutical demand. As these markets are nearing maturity, nutraceutical manufacturers are looking toward developing countries such as India and China as key growth regions. The nutraceutical market in India is estimated to grow to US $2731 million in 2016 at a CAGR of 13% (Biospectrum Asia Edition, 2012).
Many nutraceuticals, functional foods, and naturally occurring compounds, have been investigated and reports of various studies reveal these products are extremely active, have profound effects on cell metabolism and often have little adverse effects, if any. In the last decade, flaxseed, principally known as linseed in the United Kingdom, has emerged as a prime functional food ingredient, as evident from the work of several researchers. Flaxseed is one of the oldest crops, having been cultivated since the beginning of civilization (Laux, 2013). The Latin name of the flaxseed is Linum usitatissimum, which means “very useful.” Flax was first introduced in United States by colonists, primarily to produce fiber for clothing (Laux, 2013). Every part of the flaxseed plant is utilized commercially, either directly or after processing. The stem yields good quality fibers having high strength and durability (Singh et al., 2011). Until the 1990s flax had been used principally for the fabrication of cloths (linen) and papers, while flaxseed oil and its subproducts were used in animal feed formulation (Singh et al., 2011). There is a small difference in using the terms flaxseed and linseed. Flaxseed is used to describe flax when consumed as food by humans, while linseed is used to describe flax when it is used industrially and for animal feed.
Recently, flaxseed has been the focus of increased interest in the field of diet and disease research, due to the potential health benefits associated with some of its biologically active components. Flaxseeds have nutritional characteristics and are rich source of ω-3 fatty acid: α-linolenic acid (ALA), short chain polyunsaturated fatty acids (PUFA), soluble, and insoluble fibers, phytoestrogenic lignans (secoisolariciresinol diglycoside, SDG), proteins, and an array of antioxidants (Goyal et al., 2014; Ivanova et al., 2011; Singh et al., 2011). Its growing popularity is attributed to its imparting numerous health benefits to consumers, including reducing the incidence of cardiovascular diseases, decreased risk of cancer (particularly of the mammary and prostate gland), antiinflammatory activity, laxative effect, and alleviation of menopausal symptoms and osteoporosis (Goyal et al., 2015a).
Several stable preparations of flax in the form of nutraceuticals, like neat oil, capsules, and microencapsulated powders, are also available to consumers. Flax lignans-isolated SDG preparations are also commercially available as a dietary supplement. Flaxseeds were used as medicines in ancient times as a cough remedy and to relieve the abdominal pain. In this chapter we present a brief overview of the nutraceutical properties, recent epidemiological studies, and health promoting benefits of flaxseed and its components.
2 Nutraceutical Components of Flaxseed
Flaxseed is one of the richest plant sources of the ω-3 fatty acid, that is α-linolenic acid (ALA) (Gebauer et al., 2006; Tonon et al., 2011) and lignans (phytoestrogens). The important flaxseed growing countries are Canada, China, the United States, India, and Ethiopia. Canada is the world’s largest producer with a production of 0.42 million tons in 2010 (FAO, 2012), and accounts for nearly 80% of the global trade in flaxseed (Oomah and Mazza, 1998). India ranks 4th with 0.15 million tons of total flaxseed production (FAO, 2012).
Flaxseeds are available in two basic varieties: (1) brown and (2) yellow or golden. Both have similar nutritional characteristics and equal numbers of short-chain ω-3 fatty acids. The exception is a type of yellow flax called solin (trade name Linola), which has a completely different oil profile and is very low in ω-3 fatty acids (Dribnenki et al., 2007). Brown flax is better known as an ingredient in paints, varnish, fiber, and cattle feed (Drouillard et al., 2000; Kozlowska et al., 2008; Faintuch et al., 2011). Various edible forms of flax are available in the food market: whole flaxseeds, milled flax, roasted flax, and flax oil. According to its physico-chemical composition, flaxseed is a multicomponent system with bio-active plant substances such as oil, protein, dietary fiber, soluble polysaccharides, lignans, phenolic compounds, vitamins (A, C, F, and E), and minerals (P, Mg, K, Na, Fe, Cu, Mn, and Zn) (Bhatty 1995; Jheimbach and Port Royal, 2009). The basic composition of flaxseed is shown in Table 1; and the nutraceutical components of flaxseed are discussed below.
Table 1
| Nutrients/Bioactive Compounds | Quantity/100 g of Seed | Nutrients/Bioactive Compounds | Quantity/100 g of Seed |
|---|---|---|---|
| Carbohydratesa | 29.0 g | Biotin | 6 mg |
| Protein | 20.0 g | α-Tocopherolb | 7 mg |
| Total fats | 41.0 g | δ-Tocopherolb | 10 mg |
| Linolenic acid | 23.0 g | γ-Tocopherolb | 552 mg |
| Dietary fiber | 28.0 g | Calcium | 236 mg |
| Lignans | 10–2600 mg | Copper | 1 mg |
| Ascorbic acid | 0.50 mg | Magnesium | 431 mg |
| Thiamin | 0.53 mg | Manganese | 3 mg |
| Riboflavin | 0.23 mg | Phosphorus | 622 mg |
| Niacin | 3.21 mg | Potassium | 831 mg |
| Pyridoxin | 0.61 mg | Sodium | 27 mg |
| Pantothenic acid | 0.57 mg | Zinc | 4 mg |
| Folic acid | 112 mg |

Data from Flax Council of Canada, 2007. Available from: http://www.flaxcouncil.ca/spanish/pdf/FlxPrmr-R11-Ch1_Span.pdf (Accessed 25 May 2012).
a Values include dietary fiber.
b Values in mg/kg of flaxseed lipids.
2.1 Flaxseed Oil
Flaxseed is the richest plant source of the ω-3 fatty acid, that is α-linolenic acid (ALA) (Sharma et al., 2012; Goyal et al., 2016a). Flaxseed oil is low in saturated fatty acids (9%), moderate in monosaturated fatty acids (18%), and rich in polyunsaturated fatty acid (73%) (Cunnane et al., 1993). In flaxseed oil, α-linolenic acid is the major fatty acid, ranging from 39.00% to 60.42% followed by oleic, linoleic, and palmitic and stearic acids, which provides an excellent ω-6:ω-3 fatty acid ratio of approximately 0.3:1 (Pellizzon et al., 2007). Although flaxseed oil is naturally high in antioxidants like tocopherols and beta-carotene, traditional flaxseed oil is easily oxidized after being extracted and purified (Holstun and Zetocha, 1994; Goyal et al., 2016b, 2017). The bioavailability of ALA is dependent on the type of flax ingested; ALA has greater bioavailability in oil than in milled seed, and by comparison, the least bioavailability in whole seed form (Austria et al., 2008).
2.2 Flax Proteins
The protein content of flaxseed varies from 20% to 30%, constituting approximately 80% globulins (linin and conlinin) and 20% glutelin (Hall et al., 2006). Flaxseed has an amino acid profile comparable to that of soybeans, and contains no gluten (Hongzhi et al., 2004; Oomah 2001). Flax protein is not considered to be a complete protein, due to the presence of limited amino acid—lysine (Chung et al., 2005). It also contains peptides with bioactivities related to the decrease in risk factors of CVD (Udenigwe and Aluko, 2010). Whole flaxseed, flaxseed meal, and isolated proteins are rich sources of glutamic acid/glutamine, arginine, branched-chain amino acids (valine and leucine), and aromatic amino acid (tyrosine and phenylalanine). The total nitrogen content in flaxseed is 3.25 g/100 g of seed.
2.3 Flax Dietary Fibers
Flax fibers are among the oldest fiber crops in the world. The use of flax for the production of linen goes back at least to ancient Egyptian times. Flax fiber is extracted from the skin of the stem of the plant. The components of the total flax plant is approximately 25% seed and 75% stem and leaves (Lay and Dybing, 1989). The stem or nonseed parts are about 20% fiber, which can be extracted by chemical or mechanical retting. A flax fiber is a natural and biodegradable composite, which exhibits good mechanical properties and low density (Singh et al., 2011). Flax fiber is soft, lustrous, and flexible; bundles of fiber have the appearance of blonde hair, hence the description “flaxen.” It is stronger than cotton fiber but less elastic (Singh et al., 2011). Flax fiber is also a raw material for the high-quality paper industry, used to print banknotes, rolling paper for cigarettes, and tea bags (Carter, 1993).
Flax fibers include both soluble and insoluble dietary fibers. The proportion of soluble to insoluble fiber varies from 20:80 to 40:60 (Morris, 2003). The major insoluble fiber fraction consists of cellulose and lignin, and the soluble fiber fractions are the mucilage gums (Vaisey-Genser and Morris, 2003). The mucilage can be extracted by water and has good foam-stabilizing properties. Mucilage gums are polysaccharides that become viscous when mixed with water or other fluids and have an important role in laxatives (Singh et al., 2011). The optimal pH range for viscosity of flaxseed mucilage is 6–8; the pH in human intestines. Only 10 g of flaxseed in the daily diet increases the daily fiber intake by 1 g of soluble fiber and by 3 g of insoluble fiber. Insoluble fiber helps to improve laxation and prevent constipation, mainly by increasing fecal bulk and reducing bowel transit time (Greenwald et al., 2001). On the other hand, water-soluble fiber helps in maintaining blood glucose levels and lowering the blood cholesterol levels (Kristensen et al., 2012).
2.4 Flax Lignans
Plant lignans are phenolic compounds formed by the union of two cinnamic acid residues. Lignans are ubiquitous within the plant kingdom and are present in almost all plants (Tarpila et al., 2005). Lignans act as both antioxidants and phytoestrogens. Phytoestrogens can have weak estrogen activity in animals and humans. Flax contains up to 800 times more lignans than other plant foods (Mazur et al., 1996). Lignan content in flaxseed is principally composed of secoisolariciresinol diglucoside (SDG) (294–700 mg/100 g), matairesinol (0.55 mg/100 g), lariciresinol (3.04 mg/100 g), and pinoresinol (3.32 mg/100 g) (Tourre and Xueming, 2010; Milder et al., 2005). Johnsson et al. (2000) reported SDG content in the range of 11.7–24.1 mg/g and 6.1–13.3 mg/g in defatted flaxseed flour and whole flaxseed, respectively. Besides lignans, other phenolic compounds found in flaxseed are p-coumaric acid, and ferulic acid (Strandas et al., 2008). The SDG found in flax and other foods is converted by bacteria in the gut to the lignans—enterodiol and enterolactone, which can provide health benefits due to their weak estrogenic or antiestrogenic effects, as well as their antioxidant effects (Adlercreutz, 2007). Flax lignans have shown promise in reducing growth of cancerous tumors, especially hormone-sensitive ones, such as those of the breast, endometrium, and prostate.
3 Health Promoting Effects of Nutraceutical Components of Flaxseed
3.1 Flaxseed in Cardiovascular Diseases
CVDs are a group of disorders of the heart and blood vessels; they include: coronary heart disease, cerebrovascular disease, peripheral arterial disease, rheumatic heart disease, congenital heart disease. About 17.5 million people died from CVDs in 2012, which was 31% of all global deaths (WHO, 2015).
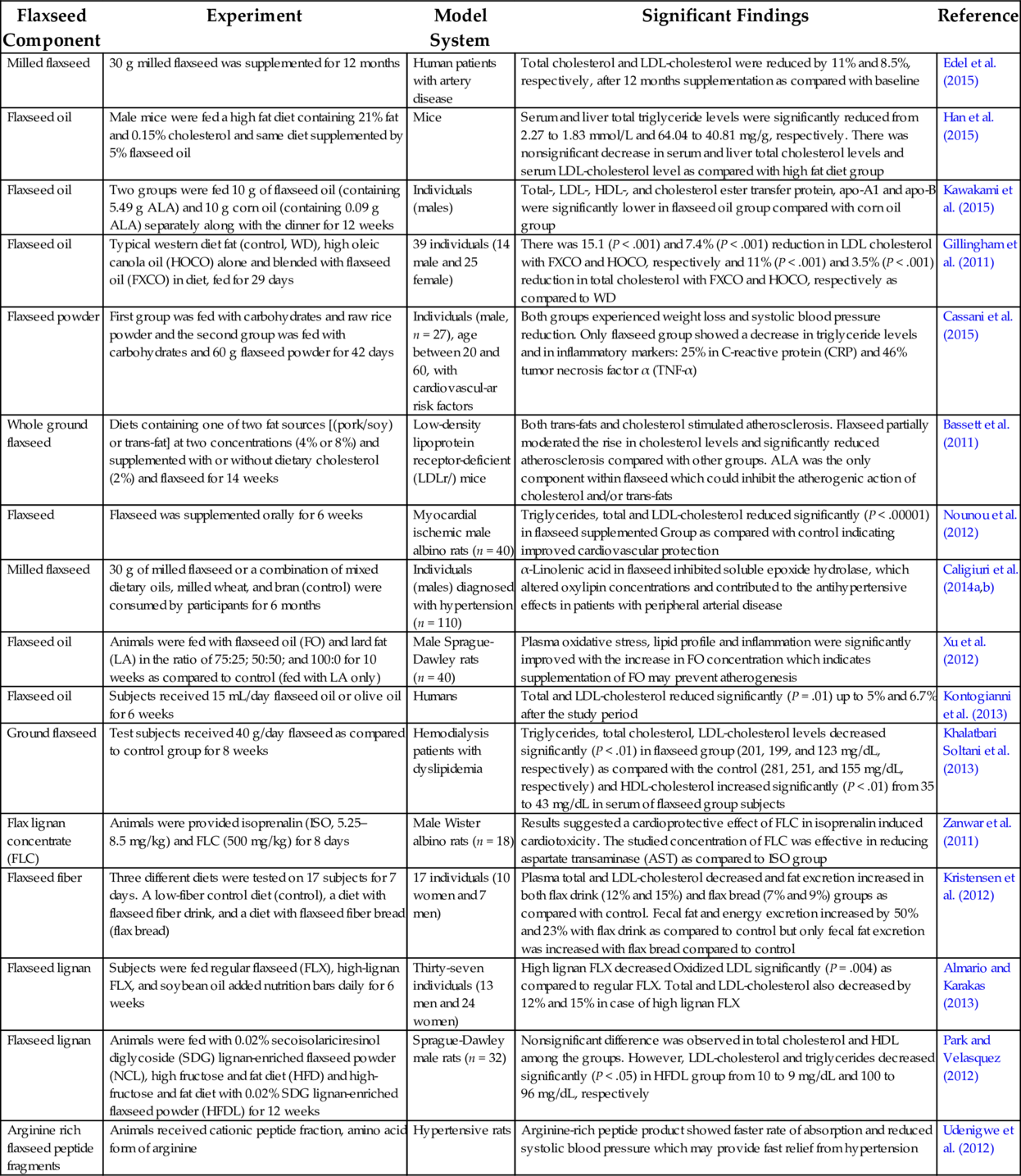
Plant foods have gained well deserved attention in recent years, due to quickly changing worldwide health scenarios and recognition of the bad effects of uncontrolled food processing. Recently, many studies have been carried out on the influence of dietary fat quality and CVD risk, and there is ample evidence in support of the use of unsaturated fatty acids for the reduction of CVD risk factors (Mente et al., 2009; Eckel et al., 2009; Mensink et al., 2003). Therefore, keeping in mind the cardio vascular health, dietary guidelines recommend replacing saturated fatty acid intake with unsaturated fatty acids. Omega-3 fatty acids, such as unsaturated fatty acids obtained from flaxseed, show a cardio protective role (Goyal et al., 2015b). Numerous epidemiologic, observational, and randomized controlled experiments have been conducted in the recent past to study this cardio protective effect; they are discussed in Table 2.
Table 2
| Flaxseed Component | Experiment | Model System | Significant Findings | Reference |
|---|---|---|---|---|
| Milled flaxseed | 30 g milled flaxseed was supplemented for 12 months | Human patients with artery disease | Total cholesterol and LDL-cholesterol were reduced by 11% and 8.5%, respectively, after 12 months supplementation as compared with baseline | Edel et al. (2015) |
| Flaxseed oil | Male mice were fed a high fat diet containing 21% fat and 0.15% cholesterol and same diet supplemented by 5% flaxseed oil | Mice | Serum and liver total triglyceride levels were significantly reduced from 2.27 to 1.83 mmol/L and 64.04 to 40.81 mg/g, respectively. There was nonsignificant decrease in serum and liver total cholesterol levels and serum LDL-cholesterol level as compared with high fat diet group | Han et al. (2015) |
| Flaxseed oil | Two groups were fed 10 g of flaxseed oil (containing 5.49 g ALA) and 10 g corn oil (containing 0.09 g ALA) separately along with the dinner for 12 weeks | Individuals (males) | Total-, LDL-, HDL-, and cholesterol ester transfer protein, apo-A1 and apo-B were significantly lower in flaxseed oil group compared with corn oil group | Kawakami et al. (2015) |
| Flaxseed oil | Typical western diet fat (control, WD), high oleic canola oil (HOCO) alone and blended with flaxseed oil (FXCO) in diet, fed for 29 days | 39 individuals (14 male and 25 female) | There was 15.1 (P < .001) and 7.4% (P < .001) reduction in LDL cholesterol with FXCO and HOCO, respectively and 11% (P < .001) and 3.5% (P < .001) reduction in total cholesterol with FXCO and HOCO, respectively as compared to WD | Gillingham et al. (2011) |
| Flaxseed powder | First group was fed with carbohydrates and raw rice powder and the second group was fed with carbohydrates and 60 g flaxseed powder for 42 days | Individuals (male, n = 27), age between 20 and 60, with cardiovascul-ar risk factors | Both groups experienced weight loss and systolic blood pressure reduction. Only flaxseed group showed a decrease in triglyceride levels and in inflammatory markers: 25% in C-reactive protein (CRP) and 46% tumor necrosis factor α (TNF-α) | Cassani et al. (2015) |
| Whole ground flaxseed | Diets containing one of two fat sources [(pork/soy) or trans-fat] at two concentrations (4% or 8%) and supplemented with or without dietary cholesterol (2%) and flaxseed for 14 weeks | Low-density lipoprotein receptor-deficient (LDLr/) mice | Both trans-fats and cholesterol stimulated atherosclerosis. Flaxseed partially moderated the rise in cholesterol levels and significantly reduced atherosclerosis compared with other groups. ALA was the only component within flaxseed which could inhibit the atherogenic action of cholesterol and/or trans-fats | Bassett et al. (2011) |
| Flaxseed | Flaxseed was supplemented orally for 6 weeks | Myocardial ischemic male albino rats (n = 40) | Triglycerides, total and LDL-cholesterol reduced significantly (P < .00001) in flaxseed supplemented Group as compared with control indicating improved cardiovascular protection | Nounou et al. (2012) |
| Milled flaxseed | 30 g of milled flaxseed or a combination of mixed dietary oils, milled wheat, and bran (control) were consumed by participants for 6 months | Individuals (males) diagnosed with hypertension (n = 110) | α-Linolenic acid in flaxseed inhibited soluble epoxide hydrolase, which altered oxylipin concentrations and contributed to the antihypertensive effects in patients with peripheral arterial disease | Caligiuri et al. (2014a,b) |
| Flaxseed oil | Animals were fed with flaxseed oil (FO) and lard fat (LA) in the ratio of 75:25; 50:50; and 100:0 for 10 weeks as compared to control (fed with LA only) | Male Sprague-Dawley rats (n = 40) | Plasma oxidative stress, lipid profile and inflammation were significantly improved with the increase in FO concentration which indicates supplementation of FO may prevent atherogenesis | Xu et al. (2012) |
| Flaxseed oil | Subjects received 15 mL/day flaxseed oil or olive oil for 6 weeks | Humans | Total and LDL-cholesterol reduced significantly (P = .01) up to 5% and 6.7% after the study period | Kontogianni et al. (2013) |
| Ground flaxseed | Test subjects received 40 g/day flaxseed as compared to control group for 8 weeks | Hemodialysis patients with dyslipidemia | Triglycerides, total cholesterol, LDL-cholesterol levels decreased significantly (P < .01) in flaxseed group (201, 199, and 123 mg/dL, respectively) as compared with the control (281, 251, and 155 mg/dL, respectively) and HDL-cholesterol increased significantly (P < .01) from 35 to 43 mg/dL in serum of flaxseed group subjects | Khalatbari Soltani et al. (2013) |
| Flax lignan concentrate (FLC) | Animals were provided isoprenalin (ISO, 5.25–8.5 mg/kg) and FLC (500 mg/kg) for 8 days | Male Wister albino rats (n = 18) | Results suggested a cardioprotective effect of FLC in isoprenalin induced cardiotoxicity. The studied concentration of FLC was effective in reducing aspartate transaminase (AST) as compared to ISO group | Zanwar et al. (2011) |
| Flaxseed fiber | Three different diets were tested on 17 subjects for 7 days. A low-fiber control diet (control), a diet with flaxseed fiber drink, and a diet with flaxseed fiber bread (flax bread) | 17 individuals (10 women and 7 men) | Plasma total and LDL-cholesterol decreased and fat excretion increased in both flax drink (12% and 15%) and flax bread (7% and 9%) groups as compared with control. Fecal fat and energy excretion increased by 50% and 23% with flax drink as compared to control but only fecal fat excretion was increased with flax bread compared to control | Kristensen et al. (2012) |
| Flaxseed lignan | Subjects were fed regular flaxseed (FLX), high-lignan FLX, and soybean oil added nutrition bars daily for 6 weeks | Thirty-seven individuals (13 men and 24 women) | High lignan FLX decreased Oxidized LDL significantly (P = .004) as compared to regular FLX. Total and LDL-cholesterol also decreased by 12% and 15% in case of high lignan FLX | Almario and Karakas (2013) |
| Flaxseed lignan | Animals were fed with 0.02% secoisolariciresinol diglycoside (SDG) lignan-enriched flaxseed powder (NCL), high fructose and fat diet (HFD) and high-fructose and fat diet with 0.02% SDG lignan-enriched flaxseed powder (HFDL) for 12 weeks | Sprague-Dawley male rats (n = 32) | Nonsignificant difference was observed in total cholesterol and HDL among the groups. However, LDL-cholesterol and triglycerides decreased significantly (P < .05) in HFDL group from 10 to 9 mg/dL and 100 to 96 mg/dL, respectively | Park and Velasquez (2012) |
| Arginine rich flaxseed peptide fragments | Animals received cationic peptide fraction, amino acid form of arginine | Hypertensive rats | Arginine-rich peptide product showed faster rate of absorption and reduced systolic blood pressure which may provide fast relief from hypertension | Udenigwe et al. (2012) |
3.2 Flaxseed in Rheumatoid Arthritis and Inflammation
Arthritis refers to a type of joint disorder that involves pain in joints, mainly due to uncontrolled inflammation and damage to the joint due to muscle strain and daily wear and tear of the joint. Studies had proved the beneficial role of ω-3 fatty acids from flaxseed in inflammation (Faintuch et al., 2011; Purushothaman et al., 2014). It has been proposed that the base of the antiinflammatory action of the omega-3 fatty acids of flaxseed oil stems from their ability to interact with arachidonic acid metabolism. This interaction may modulate the expression of some adhesion proteins which participate in leukocyte-endothelium interactions (De Caterina and Massaro, 2005); by modulation of the intracellular signaling pathways linked with the control of transcription factors and gene transcription (Novak et al., 2003). A change in gene expression of 1040 genes involved in inflammatory- and atherogenic-related pathways was confirmed by Bouwens et al. (2009) when human subjects received 1.8 g eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) for 26 weeks. Similarly, the enrichment of monocyte membranes with omega-3 fatty acids results in the synthesis and secretion of reduced quantities of cytokines, involved in the intensification of the inflammatory response (Novak et al., 2003).
Kaithwas and Majumdar (2010) observed the antiarthritic activity of flaxseed oil against turpentine oil-induced joint oedema, formaldehyde-induced and adjuvant-induced arthritis in albino rats. Various clinical trials on humans as well as mammals, as mentioned in Table 3, further support the beneficial role of flaxseed in treating inflammation and arthritis.
Table 3
| Flaxseed Component | Experiment | Model System | Significant Findings | Reference |
|---|---|---|---|---|
| Flaxseed oil | Flaxseed oil and fish oil (n-6:n-3 fatty acid ratio of 5:1) were fed to subjects (n = 42) for 12 weeks and compared with control (n-6:n-3 fatty acid ratio of 20:1) | Mature female cats | Flaxseed oil increased ALA and fish oil increased EPA and DHA in both, skin and plasma as compared with control. Fish and flaxseed oil reduced skin inflammatory responses in cats as indicated by lower leukocyte proliferative response and higher (P < .05) skin leukotriene LTB5 | Park et al. (2011) |
| Flaxseed oil | Animals were fed flaxseed oil (1–3 mL/kg) with regular diet | Albino rats | Protein exudation and leucocyte migration level in peritoneal fluid in flaxseed group (1.59 mg/mL; 3548.45 × 103/mm3) was comparable to the aspirin (1.57 mg/mL; 3654.88 × 103/mm3) group, indicating effectiveness of flaxseed oil against distinct phases of inflammation | Kaithwas and Majumdar (2013) |
| Flaxseed oil | Diet supplemented with flaxseed oil at 2.4 mL/kg body weight were provided to 10 subjects once a day for 3 weeks | Female dogs | Expression of genes involved in inflammation in WBCs (HSP90 and IL1β) was down regulated by flaxseed supplementation | Purushothaman et al. (2014) |
| Flaxseed oil | Subjects (n = 160) were divided in to two groups and were given the blind doses of flaxseed oil and mineral oil for a period of 120 days (1 g, twice a day) | Human patients with chronic renal failure | C-reactive protein levels significantly (P < .001) reduced in flaxseed oil group (8.1–4.2 mg/L) as compared with the control (4.4–3.7 mg/L); 33.3% of the flaxseed group and 16.9% of the mineral oil group changed from inflamed to noninflamed category during the study | Lemos et al. (2012) |
| Ground flaxseed | Subjects (n = 30) were divided in to two group; one group received 40 g/day flaxseed and the control group received the usual diet for 8 weeks | Hemodialysis patients with dyslipidemia | C-reactive protein (inflammation indicator) concentration in serum reduced significantly (P < .05) in flaxseed group (4.8 mg/L) as compared with the control (4.0 mg/L) | Khalatbari Soltani et al. (2013) |
| Milled flaxseed | 30 g of milled flaxseed/day was received in the form of a muffin by subjects (n = 20) divided into younger and older groups for 4 weeks | Humans | Pro-inflammatory oxylipins concentration in older group reduced and become equivalent to younger group after flaxseed consumption | Caligiuri et al. (2014a,b) |
| Flaxseed oil | 15 mL/day flaxseed oil or olive oil were received by subjects for 6 weeks | Humans | No significant difference was observed in inflammatory and biochemical markers (adiponectin, TNF-α, and C-reactive protein) after the study period indicating no effect of flaxseed on inflammation | Kontogianni et al. (2013) |
| Flaxseed powder | 60 g/day flaxseed powder and isoenergic cassava powder were received by subjects (n = 16) divided in to two groups for 12 weeks | Patients with obesity | Inflammatory markers i.e., white blood cell count, neutrophil count, C-reactive protein, serum amyloid A decreased and complement fraction 3 and 4 remained stable in flaxseed group compared to control | Faintuch et al. (2011) |
| Flaxseed | Flaxseed was supplemented orally for 6 weeks | Male albino rats (n = 40) | Inflammatory markers viz. interleukin 1 β, pentraxin-3 and TNF-α reduced significantly (P < .00001) to 34.7 pg/mL, 0.15 ng/mL and 22.4 pg/mL, respectively as compared to control (59.5 pg/mL, 0.16 ng/mL, and 26.6 pg/mL, respectively | Nounou et al. (2012) |

3.3 Flaxseed in Hypercholesterolaemia
Serum lipid profile is directly related to the risk factors of cardiovascular diseases. It is the most intensely investigated effect studied in animals and humans, after supplementation of flax in diet (Table 4). Studies of flaxseed and its bioactive components have been performed with postmenopausal women, showing positive effects, including hypocholesterolemic and antidiabetic effects (Patade et al., 2008; Bloedon et al., 2008). The effects of flaxseed on risk factors for CVD in studies performed on animals are similar to those conducted with humans. Rats, mice, and rabbits presented positive responses measuring biochemical parameters, indicating the hypocholesterolemic activity of flaxseed, generally related to the greater fecal content of lipids (Kristensen et al., 2011, 2012; Hassan et al., 2012; Park and Velasquez, 2012; Khalesi et al., 2011; Mani et al., 2011; De Franca Cardozo et al., 2010; Barakat and Mehmoud, 2011; Leyvaa et al., 2011). However, there remains controversy relating to effects on the high-density lipoprotein (HDL) fraction. Gillingham et al. (2011) reported reduced levels of HDL fraction in human serum after consuming flaxseed oil for 28 days. Similarly, researchers have also reported reduced or no change in HDL fraction in different animals (Faintuch et al., 2011; Prim et al., 2012). When type 2 diabetic patients ingested defatted flaxseeds for 2 months, patients showed significant reduction of plasma glucose, improvement in plasma lipid profiles and significant reduction of lipid peroxidation (Mohamed et al., 2012). Dietary flaxseed may also offer protection against ischemic heart disease, by improving vascular relaxation responses, and by inhibiting the incidence of ventricular fibrillation (Jennifer et al., 2010). However, Vedtofte et al. (2011) reported that higher intake of ALA was not significantly associated with decreased risk of ischemic heart disease among women or men. Various health promoting benefits of flaxseed components are shown in Fig. 1.

Table 4
| Experiment (Supplemented in Diet) | Model | TAG | Total Cholesterol | LDL-C | HDL-C | Reference |
|---|---|---|---|---|---|---|
| 70% energy from Flax oil for 28 days | Hypercholesterolaemic subjects (14 males and 25 females) | – | ↓ 11% | ↓ 15.1% | ↓ 8.5% | Gillingham et al. (2011) |
| 10 g flaxseed powder for 1 month | Type 2 diabetics | – | ↓ 14.3% | ↓ 21.8% | ↑ 11.9% | Mani et al. (2011) |
| 30 g/day of flaxseeds for 3 months | Women | No change | ↓ 7% | ↓ 10% | No change | Patade et al. (2008) |
| 50 g flaxseed provided as supplement for 4 weeks | Women | – | ↓ 9% | ↓ 18% | No change | Cunnane et al. (1993) |
| 50 g flaxseed provided as muffins for 4 weeks | Young adults | No change | ↓ 6% | ↓ 8% | No change | Cunnane et al. (1995) |
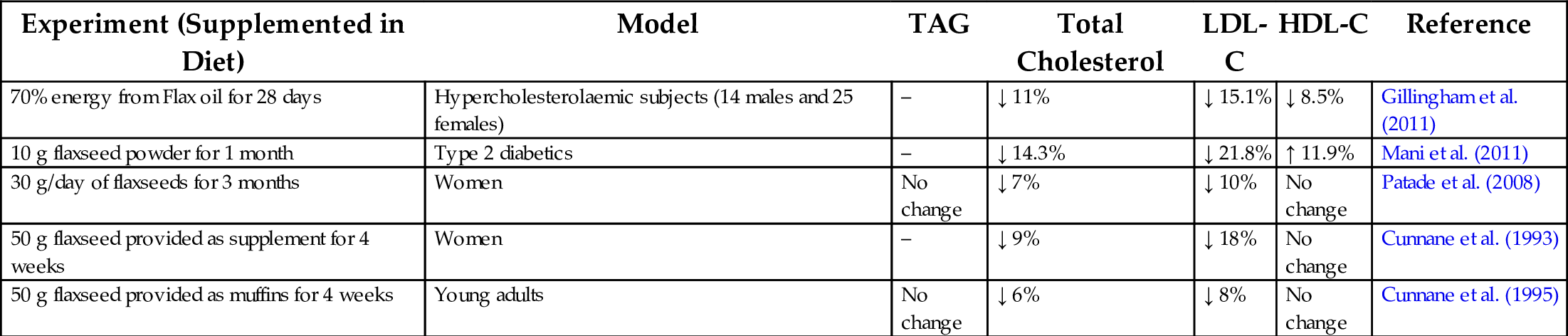
“↓” indicates decrease and “↑” indicates increase in values. HDL-C, high-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein-cholesterol; TAG, triacylglycerols.
3.4 Flaxseed in Diabetes
Diabetes mellitus is a disorder characterized by hyperglycemia; it is associated with an anomaly in carbohydrate, protein, and lipid metabolism, and usually results in developing secondary complications if not treated appropriately. These complications include impaired immune response, increased threat of inflammation, respiratory infections, and periodontal disease. Clinically it is well established and proven that the secondary complications can be controlled or postponed through appropriate diet and nutritional therapy. Flaxseed is rich in omega 3 fatty acids, and many antioxidants with lesser carbohydrate content (Mani et al., 2011). Flaxseed comprises 32%–45% of its mass as oil, of which 51%–55% is α-linolenic acid, a strong antioxidant component. However, flaxseed lignan secoisolariciresinol diglucoside (SDG) is also associated with the antioxidant activities, as well as hypolipidemic and hypoglycemic effects. Several animal and human studies indicate hypoglycemic and hypolipidemic properties of different components of flaxseed; a few recent clinical studies have been discuss in literature. Preliminary results of major studies are promising and may warrant greater research attention.
In a previous study, a dose of 40 mg SDG/kg per day in rats showed a delay in the onset of diabetes by 80% (Prasad, 2001). In a few animal studies, treatment of flaxseed lignan SDG was observed to reduce the incidence of type 1 diabetes, and also to delay the development of type 2 diabetes, by decreasing oxidative stress (Prasad and Dhar, 2016). Both type 1 and type 2 diabetes implicate oxidative stress. It was noticed that SDG treatment diminished the onset of diabetes using serum glucose levels by 75% in the streptozotocin induced diabetic rats, and by 72% in the Bio-Breed diabetic prone (BBdp) rats. These were associated with reduction in oxidative stress measured by serum and pancreatic malondialdehyde (MDA) (Prasad and Dhar, 2016).
Use of flaxseed for glycemic control may also be linked a decrease in the risk of obesity and dyslipidemia, because these are risk factors for the development of diabetes and insulin resistance. In this context, Saxena and Katare (2014) evaluated the therapeutic potential of flaxseeds in dyslipidemia, by supplementing roasted flaxseed powder for 3 months to 50 dyslipidemic subjects. Authors observed improvement in the body weight and body mass index (BMI), blood pressure, and lipid profile in the subjects, exhibiting cardio protective effect. Velasquez et al. (2003) established that flaxseed protein was more effective than soy protein in reducing proteinuria and renal histologic abnormalities in animal models of type 2 diabetes mellitus.
The association between omega-3 fatty acids, type 1, and type 2 diabetes is not yet fully understood, however, it is believed that the right proportion of omega-3 and omega-6 fatty acids diminish inflammation in the body (Bhardwaj et al., 2015). The outcome of several studies suggests that omega-3 and omega-6 fatty acids may affect the development of diabetes by modulation of insulin sensitivity in phospholipids membranes. It has been shown that ingestion of flaxseed oil has a positive impact on prediabetics as well as diabetics. According to Hussein et al. (2014a), flaxseed oil influences cell membrane structure and the incorporation of glucose transporters, resulting in a reduction of insulin resistance in diabetics. Different animal and clinical studies on flaxseed supplementation to investigate the effect on diabetes have been discussed in Table 5.
Table 5
| Flaxseed Component | Experiment | Model System | Significant Findings | Reference |
|---|---|---|---|---|
| Flaxseed oil and flour | Control group (CG), high fat group (HG), flaxseed oil group (FOG), and flaxseed flour group (FFG) | Rat (n = 24) | Diet with flaxseed flour and flaxseed oil avoided the cardiac remodeling of offspring from diabetic dams; Exposure to a hyperglycemic environment led to an increased systolic blood pressure, nevertheless FOG showed a significant reduction when compared to HG (P < .001) | Vicente et al. (2016) |
| Flaxseed | Animals were fed with flaxseed (0.714 g/kg body weight/day; orally) for 12 weeks | Diabetic rat | Flaxseed partially prevented the increase in 6PGDa (P < .05) and GR (P < .01), but unaffected G6PD in the lung of diabetic rats. Flaxseed has beneficial effects against diabetes-induced glucotoxicity by modulating G6PD, 6PGD, GR, and GST activities in tissues | Gok et al. (2016) |
| Flaxseed oil | High-fat group (HG); flaxseed oil group (FOG); and control group (CG) (nondiabetic rats) | Female Wistar rats (n = 12) | Flaxseed oil reduced the damage caused by maternal hyperglycaemia, promoting normal pancreas histomorphometry and β-cell mass in female offspring | Correia-Santos et al. (2015) |
| Lignan—secoisolariciresinol diglycoside (SDG) | Chronic SDG treatment (3, 10, or 30 mg/kg, twice per day for 3 weeks) | Mouse model of type 1 diabetes | Chronic SDG treatment can correct neuropathic hyperalgesia and allodynia in mice with type 1 diabetes. Mechanistically, the analgesic actions of SDG in diabetic mice may be associated with its antioxidant activity | Hu et al. (2015) |
| Flax lignans | Urinary concentrations of the lignan metabolites were assayed in participants | Type 2 diabetes human subjects | Lignan metabolites, especially enterolactone, are associated with a lower risk of type 2 diabetes in studied women | Sun et al. (2014) |
| Flax seed oil | Normal and diabetic animals received 1.2 mL flaxseed oil/kg/day for 8 weeks | Sixty male albino rats | Flaxseed oil supplementation increased erythrocyte membrane α-linolenic acid and decreased arachidonic acid which ultimately resulted in a prevention of protein kinase C isozymes elevation and improved insulin sensitivity in experimental diabetes | Hussein et al. (2014b) |
| Flaxseed oil or fish oil diets | Animals were fed with flaxseed oil or fish oil diets (10%, w/w) | Rat | Both diets downregulated the expression of hepatic inflammatory genes TNF-α, IL-6, MCP-1, INF-γ, and NF-κB, both the diets proved to be beneficial in preventing tissue injury and alleviating diabetic insults in the livers of STZ-NIC diabetic rats | Jangale et al. (2013) |
| Flaxseed powder | Experimental group’s diet was supplemented with 10 g of flaxseed powder for 1 month | Human (n = 29) | Supplementation with flaxseed reduced fasting blood glucose by 19.7% and glycated hemoglobin by 15.6%; a favorable reduction in total cholesterol (14.3%), triglycerides (17.5%), low-density lipoprotein cholesterol (21.8%), and apolipoprotein B and an increase in high-density lipoprotein cholesterol (11.9%) | Mani et al. (2011) |

a 6PGD, 6-phosphogluconate dehydrogenase; G6PD, glucose-6-phosphate dehydrogenase; GR, glutathione reductase; GST, glutathione-S-transferase.
3.5 Flaxseed in Obesity
The outcomes of available preclinical and clinical trials suggest that flaxseed can modulate biological processes, which lead to obesity including thermogenesis, visceral adipose deposition postprandial substrate trafficking/oxidation, and satiety (Marinangeli and Jones, 2012). The higher content of several amino acids, like the flaxseed proteins arginine and glutamine, may produce thermogenic effects. Evidence suggests flaxseed components may induce satiety by facilitating and extending secretion of cholecystokinin, and thus reducing food intake. While mechanistic studies are limited, there are indications that fibers have an impact on the expression of the genes that modulate metabolism. Flaxseed is a promising alternative for reducing the risk of diseases associated with excess body weight because it is rich in α-linolenic acid, lignans, and dietary fiber (Machado et al., 2015).
In one human study, a patient group comprised of overweight or obese men and postmenopausal women (n = 25) with prediabetes consumed 0, 13, or 26 g ground flaxseed for 12 weeks. Flaxseed intake as part of a habitual diet, decreased glucose and improved insulin sensitivity in overweight or obese individuals with prediabetes, while fructosamine, high sensitivity C-reactive protein, adiponectin, and high-sensitivity interleukin-6 demonstrated no significant change (Hutchins et al., 2013). In two single-blind randomized crossover acute studies, subjects (24 and 20) were exposed to soluble dietary fibers (2.5 g) of flaxseed. Flax-drink increased sensation of satiety and fullness as compared to the control, and a significant decrease in subsequent energy intake was observed (2937 vs 3214 kJ) (Ibrugger et al., 2012).
3.6 Flaxseed in Hypertension
Hypertension, a very common illness, is linked to the modern lifestyle. It is a major risk factor of cardiovascular diseases, and is also known to negatively impact various organs, including the heart, liver, and kidney. Advanced drug therapy helps to control both systolic blood pressure (SBP) and diastolic blood pressure (DBP), but results in numerous side effects. Polyunsaturated fatty acids, like omega-3 and omega-6, obtained from flaxseeds have been shown to lessen the effects of hypertension. Hypertension is commonly associated with peripheral artery disease (Rodriguez-Leyva et al., 2013). Outcomes of a few animal studies suggest that patients with artery disease may benefit from dietary supplementation of flaxseed (Table 6). A recently published review of systematic literature and metaanalysis of available randomized controlled trials established that supplementation with various flaxseed products results in significant reductions in both SBP and DBP (Ursoniu et al., 2016).
Table 6
| Flaxseed Component | Experiment | Model System | Significant Findings | Reference |
|---|---|---|---|---|
| Flax lignan | Animals were fed with flaxseed lignan concentrate (FLC, 400 and 800 mg/kg) with drug captopril and combinations | Wistar rats | FLC significantly (P < .01 and P < .001) decreased the elevated blood pressure levels; inhibited ACE and exerted antioxidant activities | Sawant and Bodhankar (2016) |
| Flaxseed | Subjects received 28 g/day of brown flaxseed (BF), golden flaxseed (GF), or the equivalent amount of wheat bran (control) in different preparations for 11 weeks | 75 overweight adolescents (33 boys, 42 girls) | Flaxseed consumption showed significant reduction in deep brain stimulation (DBS); both BF and GF did not differentially affect plasma lipid responses, plasma glucose and inflammatory profile, although all groups showed increased levels of TNF-α | Machado et al. (2015) |
| Flaxseed | Participants consumed 30 g of milled flaxseed for 6 months | Human with peripheral arterial disease (75% hypertensive) | Flaxseed group exhibited significant reductions in systolic (− 10 mmHg) and diastolic (− 7 mmHg) blood pressure; altered concentrations of plasma oxylipin exhibited an antihypertensive effects | Caligiuri et al. (2014b) |
| Flax proteins | Hypertensive animals were either fed a standard diet alone or a flaxseed-supplemented standard diet (FLX; 10%, w/w) for 8 weeks | Wistar rats | Rats fed the FLX-supplemented diet had significantly lower blood pressure, an improved lipid profile and decreased tissue marker levels measured after 4 and 8 week durations | Al-Bishri (2013) |
| Flaxseed | Patients ingested a variety of foods which contained 30 g of milled flaxseed for 6 months | Human (n = 110) | A significant reduction of 15 mmHg in systolic blood pressure and 7 mmHg in diastolic blood pressure DBP | Rodriguez-Leyva et al. (2013) |
| Flaxseed protein isolate (FPI) | Oral administration of the cationic peptides containing arginine (200 mg/kg body wt.) to spontaneously hypertensive animals | Rats | More rapid decrease in in systolic blood pressure when compared to similar amounts of FPI or the amino acid form of arginine; suggesting antihypertensive effect | Udenigwe et al. (2012) |

Researchers suggest that diverse biological mechanisms are responsible for the antihypertensive effect of flaxseed. Flaxseed lignan SDG is a phytoestrogen known to be an ACE inhibitor. This SDG is reported to reduce angiotensin I-induced increase of BP, through stimulation of guanylate cyclase enzyme in Sprague Dawley male rats (Prasad, 2013). Caligiuri et al. (2014b) concluded that flaxseed α-linolenic acid could have an inhibiting effect on soluble epoxide hydrolase and alter concentrations of plasma oxylipin in patients with peripheral arterial disease, and exhibited an antihypertensive effect. It is observed that pro-inflammatory oxylipins formed by soluble epoxide hydrolase are accountable for the loss of vasodilatation and development of inflammation in arterial hypertension (Caligiuri et al., 2014b). On the other hand, a human study by Caligiuri et al. (2014a) proved that flaxseed might lessen inflammation by diminishing pro-inflammatory oxylipins levels. Moreover, various studies indicate flaxseed may decrease in C-reactive protein, interferon-gamma, serum amyloid, A, and interleukin-1β, IL-2, IL-4, IL-6, and IL-10 (Pan et al., 2009; Lemos et al., 2012).
Several researchers link the antioxidant potential of flaxseed components, especially peptides or amino acids (arginine), to their capability to control hypertension. A flaxseed derived peptide mixture containing high levels of branched-chain amino acids and low levels of aromatic amino acids, has shown antioxidant activities by scavenging 2,2-diphenyl-1-picrylhydrazyl (DPPH) radicals, and antihypertensive effects by inhibition of angiotensin I-converting enzyme (ACE) (Oomah, 2001). Fermented milks prepared using distinct strains of lactic acid bacteria have been reported to possess antihypertensive and antioxidative activities due to specific proteolytic action on milk proteins. Similarly, fermentation of rapeseed and flaxseed proteins with Lactobacillus helveticus and Bacillus subtilis resulted in products containing compounds with ACE-inhibitory and antioxidant effects (Pihlanto et al., 2012). Several cationic peptides detected in a trypsin and pronase digest of flaxseed proteins demonstrated moderate ACE inhibition in vitro assays, and were further proven to have antihypertensive effects in vivo (Udenigwe et al., 2012). Flaxseed protein digested with an in vitro digestion model showed presence of a pentapeptide Trp-Asn-Ile-Leu-Asn-Ile-Leu and a hexapeptide Asn-Ile-Leu-Asp-Thr-Asp-Ile-Leu (Marambe et al., 2011). However, these peptides have not been assessed individually, therefore, their ability to inhibit ACE in a pure form is not yet understood (Udenigwe et al., 2009, 2012; Marambe et al., 2011). Arginine-rich peptides can be generated from flaxseed protein isolate (FPI) and used as a source of nitric oxide, which can produce in vivo vasodilatory effects during hypertension (Udenigwe et al., 2012).
Khalesi et al. (2015) observed that when flaxseed is consumed as a whole seed for a specific time duration (> 12 weeks), its potential to decrease blood pressure, particularly DBP, may be superior to consumption of part of flaxseed in food. However other reports suggest that the milled flaxseed provides the best bioavailability for the bioactive components in flaxseed (Kuijsten et al., 2005; Austria et al., 2008). In the case of alpha-linolenic acid, maximum bioavailability seems to exist when ingested in the form of flaxseed oil, but its bioavailability was far less pronounced when ingested as a whole seed (Austria et al., 2008).
3.7 Flaxseed in Tumor and Cancer Treatment
Interest in research on the association between flaxseed ingestion and risk of cancer emerged when epidemiologic evidences suggested a beneficial relationship. Research in laboratories has shown that flaxseed inhibits the formation of colon, breast, skin, and lung tumors, and also reduces blood vessel cell formation in female rats, all suggesting a protective effect against breast, colon, and ovarian cancer (Truan et al., 2012). Higher levels of insulin and insulin-like growth factor 1 (IGF-1) increase cancer risk by stimulating cell proliferation, and increasing survival of DNA-damaged cells, through antiapoptotic mechanisms (Sturgeon et al., 2011). Blood insulin has also been associated with increased risk of pancreatic and colorectal cancers (Pisani, 2008). Various studies suggest that flaxseed added to the diet may lower circulating levels of insulin and IGF-1 (Chen et al., 2011a). However, Sturgeon et al. (2011) reported that incorporation of 7.5 g of flaxseed daily for 6 weeks, and 15 g of flaxseed for an additional 6 weeks, into the diet of healthy postmenopausal women had little short-term effect on blood levels of IGF-1. Flaxseed has a breast tumor reducing effect, possibly because of its high content of SDG lignan (Truan et al., 2012; Chen et al., 2011a). Enterodiol (ED) and enterolactone (EL) are produced from flax lignans in an animal’s body. Because they are structurally similar to human estrogen-17β-estradiol (E2), they have binding affinity to estrogen receptors (ER) (Penttinen et al., 2007). Flaxseed and its SDG component have been shown to attenuate tumorigenesis through a reduction in cell proliferation and angiogenesis, as well as an increase in apoptosis via modulation of the estrogen receptor (ER)- and growth factor-signaling pathways (Saggar et al., 2010). The potential breast cancer protective effect of flax lignans could be due to their weak estrogenic activity and antioxidant properties. Flaxseed oil, with its exceptionally high ALA content, has also been shown to reduce the growth of human estrogen receptor-positive breast tumors (MCF-7) by 33%, as compared to the control (Truan et al., 2010). Chen et al. (2007) studied groups of mice that received 5% and 10% flaxseed in their diet for 8 weeks; this inhibited tumor growth by 26% and 38%, respectively. The researchers suggested the ability of flaxseed to help maintain more early stages of cancer is due to the fact that flaxseed contains the highest level of plant lignans, which have antioxidant activities (Hall et al., 2006), and have also been shown to alter estrogen metabolism, which may decrease ovarian cancer risk and improve health (McCann et al., 2007).
3.8 Flaxseed in Kidney Diseases
Chronic kidney disease (CKD) is an important health problem among older adults and can lead to end-stage renal disease, requiring dialysis or organ transplant for survival (Lauretani et al., 2009; Coresh et al., 2007). Due to the antiinflammatory properties of ω-3 fatty acids, it has been suggested that these nutrients may protect the kidneys from damage in adults. PUFA supplementation was observed to reduce renal inflammation and fibrosis in animal models (Baggio et al., 2005). Gopinath et al. (2011) showed that increased dietary intake of long-chain ω-3 PUFA was inversely associated with the prevalence of CKD. Cicero et al. (2010) demonstrated long-term supplementation of omega-3 fatty acids to be a associated with a significant reduction in systolic and diastolic blood pressure. Hypertension is a risk factor for CKD, therefore, the influence of long-chain n-3 PUFA on blood pressure may be a potential mechanism for kidney protection. However, a positive association between α-linolenic acid and moderate CKD was observed by Gopinath et al. (2011). One possibility behind such results could be lesser conversion of α-linolenic acid into EPA and DHA, which have been shown to be cardioprotective (Wang et al., 2006). Various clinical studies dealing with effects of flaxseed and their components, in reducing the incidence of cancer and kidney diseases are discussed in Table 7.
Table 7
| Flaxseed Component | Experiment | Model System | Significant Findings | Reference |
|---|---|---|---|---|
| Defatted flaxseed meal | Animals were fed with 10% defatted flaxseed meal (n = 36) | Mice | Showed low multiplicity in lesions and also reduced the incidences of lesions | de Freitas Gomides et al. (2013) |
| Flaxseed oil | Animals received 20% or 5% flaxseed oil, respectively in diet in post initiation stage until the end | Male Wistar rats | Inhibited 1,2-dimethylhydrazine-induced colon carcinogenesis | Salim et al. (2011) |
| Dietary flaxseed lignan and/or oil | Animals were fed with SDG (1 g/kg diet), flaxseed oil (FO) (38.5 g/kg diet), or combined SDG and FO | Mice | Growth of TAM (tumor-associated macrophages) treated tumors was decreased with all treatments | Saggar et al. (2010) |
| Flaxseed derived enterolactone | 147 patients with prostate cancer had participated in presurgical trial of flaxseed supplementation (30 g/day) for 30 days | Human | Enterolacton may hinder cancer cell proliferation | Azrad et al. (2013) |
| Flaxseed | A total of 36 women were fed with ground flaxseed (25 g/day) through normal diet | Individuals (females) | Flaxseed supplementation did not alter the level of angiogenin & vascular endothelial growth factor (VEGF) but exert the similar effect on endostatin level as shown by tamoxifen | Aberg et al., 2011 |
| Flaxseed oil | Animals were prefed experimental diets (added with 15% flaxseed oil) for 10 days and then received a single dose of cisplatin (CP) (6 mg/kg body weight) intraperitoneally while still on diet | Adult male Wistar rats | Incorporation of flaxseed oil prior to and following CP administration showed resistance toward the deleterious effect of CP on kidneys (nephrotoxicity) | Naqshbandi et al. (2013) |
| Flaxseed oil | Animals were treated with 1000 mg/kg of corn oil, flaxseed oil and black seed oil, respectively | Mice | Flaxseed oil administration showed the protection against lead acetate-induced hepatotoxicity | Alarifi et al. (2012) |
| Flaxseed lignan complex (FLC) | Animals were fed 0% flaxseed, 10% flaxseed, 10% FLC or 20% FLC for 3 weeks, then irradiated with a single fraction (13.5 Gy) of X-ray radiation treatment (XRT) | Mice | FLC administration resulted into improved survival | Christofidou-Solomidou et al. (2012) |
| Flaxseed oil and probiotics | The germ-free piglets were treated with L. plantarum—Biocenol LP 96 and flaxseed oil | Piglets | Showed a significant antiinflammatory action | Chytilová et al. (2013) |
| Flaxseed oil | Animals were fed control, fish oil or flaxseed oil diets with n-6:n-3 fatty acid ratios of 20:1, 5:1 and 5:1, respectively, for 12 weeks | Cats | Indicated the antiinflammatory and immunosupressive role of flaxseed oil | Park et al. (2011) |

4 Estimated Intakes of Whole and Milled Flaxseed, ALA and Fibers
After reviewing various clinical studies regarding the health effects of flaxseed constituents, it can be concluded that flaxseed in different forms can be consumed, but the dietary intake is equally important. The intended uses of whole and milled flaxseed are recognized as generally safe (GRAS) (Jheimbach and Port Royal, 2009). The FDA previously authorized the addition of flaxseed to foods up 12% by weight, and for most foods, this may be understood as the maximum level to supplement (Jheimbach and Port Royal, 2009). While it may be technologically and organoleptically feasible to add a somewhat higher proportion of flaxseed to a few food products, for many products an addition of even 12% flaxseed is likely to be unattainable. Using the Reference Amounts Customarily Consumed (RACC) established by FDA, addition levels of 12% by weight can be converted to g/serving by multiplying the RACC by the intended addition percentage. Various recommended levels of flaxseed in food products are shown in Table 8.
Table 8
| Food Category | RACCa (g) | Maximum Flaxseed Contentb (g/serving) |
|---|---|---|
| Bread | 50 | 6.0 |
| Biscuits, bagels, tortillas | 55 | 6.6 |
| Doughnuts, muffins | 55 | 6.6 |
| Pancake/waffle mix | 40 | 4.8 |
| Pasta (dry weight) | 55 | 6.6 |
| Multi grain flours or meal | 30 | 3.6 |
| Breakfast cereals | 30 | 3.6 |
| Cookies | 30 | 3.6 |
| Nuts and seeds | 30 | 3.6 |
| Cheeses | 30 | 3.6 |
| Salad dressing | 30 | 3.6 |
| Mayonnaise | 15 | 1.8 |
| Margarine, table spreads | 15 | 1.8 |
| Yoghurt | 225 | 27.0 |
a Reference amount customarily consumed (21 CFR § 101.12).
b Based on addition of flaxseed at 12% by weight of the food.
For optimal health, many government and public health authorities recommend increasing ω-3 fatty acids in diet. In fact, as early as 1990, Health Canada recommended an ω-6:ω-3 fatty acid dietary ratio of 4:1 to 10:1 (Health and Welfare Canada, 1990). Supplemented products for clinical trials need to contain an amount and type of flaxseed that will significantly increase the levels of ALA in the blood, over and above the recommended daily amount of 1.6 g/day for males and 1.1 g/day for females (Health Canada, 2009). Flaxseed contains approximately 23 g ALA per 100 g (USDA, 2010) and thus, the recommended dietary amounts can be obtained by consuming about 9 g of flaxseed per day. The mean intake of dietary fibers among several European countries is 22 g/day, ranging from 12 to 34 g/day (Bingham et al., 2003), approximately 14.3 g/day in Japan, and 21.9 g/day in United States, ranging from 12 to 36 g/day. The commonly recommended dietary intake of fiber should be 30 g or more per day. This amount is expected to increase stool weight and frequency and normalize stool consistency.
5 Flaxseeds for a New Millennium
To achieve optimal nutrition and health benefits through the intake of healthy foods, food science, and technology experts are creating a new framework for food-based dietary recommendations, principally in the areas of food physics, methods of food storage and preservation, nutrient restoration, and fortification of foods, as well as the development of health-focused designer foods, functional foods, and nutraceuticals (FAO/WHO 1996; USDA, 2010). Initiatives have been undertaken by the food industry to increase the level of ω-3 fatty acids, dietary fibers, and antioxidants, as well as to develop nutraceuticals and value-added foods. Flaxseed has drawn the attention of scientists, researchers, and food industry product developers, due to its ω-3 fatty acids, lignans, and various health benefits. In the functional arena of the 21st century, flaxseed’s use is not limited to it being a source of dietary fiber; it has been extended to take advantage of various nutraceuticals and therapeutic attributes which make it a potent ingredient for added food value. If the FDA approves classification of flax as a whole grain, enormous growth in the variety of fortified food products can be expected. Flax is a rich source of ALA, dietary fibers, high quality proteins, antioxidants, and lignans, some of which offer synergistic health benefits. Flaxseed contains almost no digestible or glycemic carbohydrates. In all respects, flaxseed present an ideal model for whole grains or seeds, and underscores the recognition given to the nutritional value of “whole grains,” “whole seeds,” and “whole foods.” Some nutraceutical preparations based on flaxseed components have been shown in Table 9.
Table 9
| Product/Medicine Name | Formulation | Actions |
|---|---|---|
| Essentiale (Germany) | Essential phospholipids, α-linolenic acid, pyridoxine, cyanocobalamin, nicotinamide, etc. | Stimulates the detoxicating function of liver; restores and maintains the structure of liver cells |
| Lipostabil (Germany) | Contains choline phospholipids, as well as α-linolenic and oleic acids | A moderate vasodilatory action, normalizes the ratio of α- and β-lipoproteins in the blood |
| Essaven (Germany) | Contains phosphatidylcholine (linoleic acid, α-linolenic, and oleic acids) | Help in painful fatigue of legs; muscle contusions and strains; and superficial vein disorders |
| Linetol (Russia) | Represents a mixture of linseed fatty acid ethylates, including oleic (15%), linoleic (15%), and linolenic (57%) acids | In treatment of atherosclerosis and for external use in cases of skin burn and radiation damage |
| Efamol (Great Britain) | Capsules form containing linseed oil in combination with other oils and vitamin E | Shows a positive effect when used for the treatment of eczemas |
| Esoman-ointment (Great Britain) | Linseed PUFAs and hexachlorophane | Protect skin from aggressive agents such as acids, alkalis, formaldehyde, and phenols |
6 Conclusions
Based on the information available, it is evident that flaxseeds are the richest source of α-linolenic acid and lignans. It is also a significant potential source of soluble fiber, antioxidants and high quality protein. Its long journey, from being a medicine in ancient times to the health food source in 21st century, has opened the doors for improved health for a large population. The role of flaxseed lignans and ω-3 fatty acid in reducing the risks associated with cardiac and coronary disease, cancer (breast, colon, ovary, and prostate), and other human health risk factors, are now well known. When support of heart health is one of the most desired and highly demanded health benefits from functional foods and nutraceuticals, and where food industry’s goal is to develop innovative solutions to address nutritional challenges, flaxseed is going to play a vital role for both. Flaxseed can contribute to improving the availability of healthy food choices. This is especially the case with improving the nutrient profile of foods through reductions in salt, sugar, and saturated fat content, and by increasing the content of ω-3 fatty acids, as well as other bioactive compounds. With contributions from such factors, the worldwide market for healthy heart foods is estimated to grow rapidly in the coming years. As a result, flaxseed and flaxseed oil may become preferred ingredients of functional foods and nutraceuticals. There is no doubt that a change to an omega-3 rich and high fiber diet would be beneficial. Therefore, the use of flaxseed, in whole seed or ground form, can be recommended as a dietary supplement. Modern methods, such as high power ultrasound, micro-fluidization, spray granulation, and nanoencapsulation, will pave the way for new approaches to processing, stabilizing, and use of flaxseed oil. Additionally, enrichment in animal diet with flaxseed and flaxseed oil, for production of ω-3 enriched eggs, milk, meat, and other animal origin products, presents novel use of flaxseed to benefit health.