
The word flexibility is derived from the Latin flectere or flexibilis “to bend,” and a practical sports definition is the range of motion (ROM) available in muscle, tendons, and connective tissue around a joint or group of joints. It is generally accepted that a minimum level of flexibility is required for competitive athletes, specifically tennis players, to improve performance and aid in the reduction in injuries. However, what this minimal level is and how best to obtain it, is still up for scientific as well as practical debate.
In the last 15 years hundreds of studies have investigated the how, what, when, and why of flexibility training and the impact on physical performance and injury prevention. Some very interesting and sometimes misinterpreted results have led to better, more effective methods of training athletes. This chapter on flexibility will provide many research studies to help coaches and trainers develop appropriate flexibility and stretching guidelines to help improve the performance of tennis athletes and reduce the likelihood of injury.
Many terms have been used and misused to describe different stretching and flexibility movement patterns.
Stretching—the manual increase in ROM.

Figure 5.1: Active stretching.
Active Stretching—the athlete is the person providing the force to stretch the muscle.

Figure 5.2: Passive stretching.
Passive Stretching—a partner or machine is used to provide the force to stretch the muscle.

Figure 5.3: Static stretching.
Static Stretching—The muscle is stretched and held at a certain length with no movement. This can be accomplished either actively or passively.
Ballistic Stretching—When the muscle is stretched via bouncing, bobbing, and/or rebounding and the muscle is not held at the end-point. There is continual movement. The theory behind ballistic stretching is that momentum is used to help the athlete stretch further than would be possible under a controlled movement.
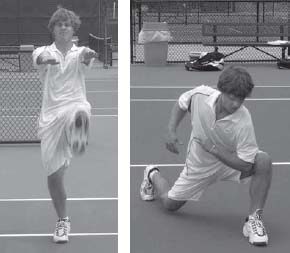
Figure 5.4: Dynamic stretching.
Dynamic Stretching—Is when the muscle is stretched under a controlled movement pattern. It differs from ballistic as the muscle is elongated under a controlled lengthening and shortening process as opposed to quick jerky movements typical of ballistic stretching.
PNF (Proprioceptive Neuromuscular Facilitation)—PNF refers to any of several stretching techniques in which a muscle group is passively stretched, then contracts isometrically against resistance while in the stretched position, and then is passively stretched again through the resulting increased range of motion. PNF stretching usually employs the use of a partner to provide resistance against the isometric contraction and then later to passively take the joint through its increased range of motion. It may be performed, however, without a partner, although it is usually more effective with a partner’s assistance.
AIS (Active Isolated Stretching)—AIS is theorized to work via two major mechanisms. The first is called reciprocal inhibition, which means that if you want to lift your arm, your nervous system has to shut off the muscles that bring your arm down. This means that AIS involves your nervous system in the stretch, making it easier for the muscles to elongate. The second principle is to avoid the stretch reflex. This is achieved by holding the stretch for 1.5 to 2 seconds, and no longer. Holding a stretch for longer than 2.5 to 3 seconds will cause the body to engage a protective reflex known as the stretch reflex. This stretch reflex will cause a muscle contraction in the muscle trying to be stretched. The stretch is repeated 8 to 10 times in a set. By repeating the stretch multiple times, blood flow is increased to the area ROM is gently increased.
All forms of flexibility exercises may be appropriate for the tennis athlete, but important research has been undertaken to determine which forms should be applied during warm-up and which forms are more appropriate immediately postexercise and during recovery sessions. The timing of different stretching exercises is also important from a performance enhancement perspective. Although stretching has been construed as a typically positive exercise for tennis players, certain types of stretching before playing tennis can actually reduce tennis-related performance.
The warm-up for practice and competition is an important period not only for preparing the mind for the emotional and mental battle about to be undertaken, but it is also an important period to help prepare the body physically to improve performance and potentially reduce the likelihood of injury. Although most coaches and trainers want to help their athletes improve and perform better, the traditional warm-up, which included a period of static stretching, has actually been shown to reduce strength, speed, and power movements in subsequent exercise (2, 12, 13, 15, 20, 21, 34, 36, 40-42, 61, 62). Therefore, a large majority of well-meaning coaches and trainers are reducing their athletes’ performance instead of the opposite intended positive effect. Although the reductions in performance have varied across different studies, the reduction in performance has ranged from 5%-30% (2, 12, 13, 15, 20, 21, 34, 40-42, 61, 62). How many athletes would you keep if you told them that after working with you they would be 30% worse?
The deficit in performance following static stretching has been shown to last approximately 60 minutes after the stretching routine (21) and may be due to changes in reflex sensitivity, muscle/tendon stiffness, and/or neuromuscular activation (13, 19, 21, 58). The actual causes and mechanisms for why there is a reduction in athletic performance are still being investigated.
A tennis-specific study looking at static stretching and the subsequent performance on service speed showed no difference in performance of serve speed (positive or negative) (33). The static stretching routine had no effect on either speed or accuracy (performance) of an explosive tennis serve (33). A suggested reason for why static stretching prior to the tennis serve did not reduce performance as observed in other studies was that the preactivity stretching may not decrease performance in high-speed and/or accuracy-related movements (33). This theory has not typically been supported, as was seen in a recent study looking at sprint speed times (which involves high speed explosive movements) in highly trained athletes over short distance (<20 meters) (40). It was found that static stretching reduced performance by a significant increase in 20 meter sprint speed time (slower time) compared to no stretching (40). This result is of interest to tennis trainers, coaches, and athletes as it uses a population (well trained sprinters) and is measured over distances similar to that encountered during tennis play. The vast majority of studies support the notion that static stretching before activity reduces performance (2, 12, 13, 15, 20, 21, 34, 36, 40-42, 61, 62). From the available research it is clear that static stretching before exercise is not beneficial to performance and in most cases produces negative results on subsequent performance.
If static stretching does not improve performance if used during the warm-up, does it reduce the chance of injury? The widely-held belief that preactivity static stretching may reduce injury is linked to the theory that a “tight” muscle-tendon unit is less flexible, meaning that it cannot be stretched to as great a degree (23, 27). This assumption has resulted in the long-held belief that stretching may prevent muscle and tendon related injuries (23). Current research, however, does not support this assumption, supporting instead the opposing view that static stretching before activity does not reduce the occurrence of sport induced injury (11, 23, 24, 26, 27, 38, 44, 45, 51-54, 60).
At the time of this edition, little tennis-specific research is available on this topic, but multiple studies have looked at sport movement patterns which are seen during tennis play. A study looking at the prevention of lower-limb injuries in 1,538 male army recruits found that preexercise static stretching had no effect on injury rates after a 12-week stretching protocol (45). In 2001, an extensive review of stretching studies on running injuries found that there was no strong evidence to suggest static stretching exercises are effective in preventing lower limb injuries (60). This finding has been supported in previous reviews looking at stretching and overall injury rates (24, 26, 36, 53, 60).
To provide a fair and balanced review of the scientific literature, it must be mentioned that a small number of studies have shown a tentative link between reduced injury rates and preactivity stretching (5, 14, 17); however, the large majority of studies and review articles have found no link between preactivity stretching and a reduction in injury rates (1, 23, 24, 26, 27, 38, 51-54, 60). The evidence is heavily slanted to support the conclusion that static stretching before tennis play will not improve performance, and typically even reduces performance. It will also have no clear benefit on reducing the likelihood of injury.
When designing programs, static stretching should not be included in the preactivity warm-up. However, limited or poor muscle and joint range of motion can reduce performance and increase the risk of injury (55). Therefore, increasing ROM to an appropriate length is required and static stretching can be used to accomplish this—just not before exercise. Static stretching is a great tool that is easy for the athletes to perform and is the safest method of stretching. A good time to perform static stretching routines are immediately post-practice/competition and during the evening.
Other forms of warm-up, including general muscle warming exercise (i.e., jump rope or jogging) and/or dynamic (active) range of motion exercises, may be the most beneficial in improving physical performance (4, 7, 20, 50). Although more research is needed to make definitive conclusions about pre-tennis warm-ups, some positive results have shown significantly faster 20-meter sprints times following dynamic warm-ups compared to static stretching during the warm-up period (20). Although limited peer reviewed scientific studies are available (to date) on dynamic ROM training, it has been used by athletes and coaches for many years with great anecdotal results. The major benefit with this dynamic ROM training, if performed correctly, is that it can also correct muscle imbalances in both strength and flexibility and can actually help the athlete improve functional strength in the muscles and movements required to play tennis at a competitive level. Dynamic warm-up exercises can be used to help muscle imbalances, strength weaknesses, and balancerelated problems. The benefits of these types of exercises can be far greater than just improving ROM.
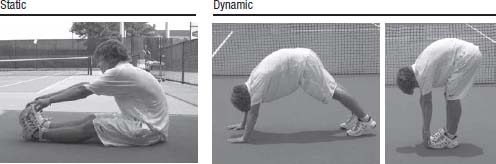
Figure 5.5: Comparison of a static Hamstring/Lower back stretch versus dynamic flexibility exercise: Left photo is a static stretch and hold. Middle and right photos show hamstring stretch by dynamic walking out on hands.
Post-tennis practice and competition is an important time to implement a structured flexibility program. Many competitive tennis players do not perform adequate post exercise stretching routines. The benefits of performing flexibility training postexercise are numerous. Static stretching after training/competition and before bed has resulted in 50% fewer injuries according to a 1998 study in the American Journal of Sports Medicine (25). The muscle temperature is already warm from the training/competition period, allowing for the muscle and tendon units to be stretched comfortably and to a greater range than when the muscle is cooler. As a result of the increased muscle temperature, greater improvements in muscle and joint ROM can be made. Another possible benefit of performing postexercise or evening stretching exercise may be the reduction in delayed onset of muscle soreness (DOMS) (26). DOMS is the pain or soreness athletes feel during the days following a hard exercise session. DOMS typically peaks between 48-72 hours postexercise and the cause is multifaceted. One of the major causes of DOMS is unaccustomed eccentric exercise. Movements requiring a lot of stop-start and change of direction are typical on-court causes of DOMS, whereas the eccentric (negative) portion of strength training movements are a major off-court cause. However, using stretching to reduce the symptoms of DOMS is still being debated, with both positive and negative studies concerning the effect of stretching on reducing DOMS (26,
56).
How long each static stretch should be held varies depending on the athlete, level of player, training and genetic flexibility capabilities. In a study to determine whether 15, 30, 45 or 60 seconds produces the greatest increase in flexibility, researchers had participants stretch five days a week over a six week period. The groups that stretched 30 or 60 seconds produced the most increases in ROM. The authors concluded that the 30 second hold of the static stretch produces the most time-effective results (3).
Tennis imposes large demands on the shoulder area in terms of ROM, loads, and velocities. The time of contact between the ball and racquet is very short, only between 0.003-0.006 seconds (47), and the racquet and ball must be in optimal orientation to execute the desired stroke. Epidemiologic data indicates that shoulder injuries are prevalent in many tennis players (32, 59) and the shoulder is the most often injured joint in competitive tennis (32, 46, 59).
The sport of tennis imposes adaptive strength changes in the dominant arm. Primarily, these changes occur by increasing the strength of the internal rotator muscle groups without subsequent strengthening of the external rotator muscle groups. Selective ROM patterns appear to occur from repetitive tennis play, that results in musculoskeletal adaptations that may predispose tennis players to injury if left undetected (18, 31).
The shoulder and elbow of the player’s dominant arm is of interest because of the excessive ranges of motion, repetitive high speed movements, and resultant high loads and forces that these joints experience hundreds of times daily. Shoulder movements are the result of a complex interplay between structural bony anatomy and biomechanics and between static ligament and tendon restraints and dynamic muscle forces. Injury to one or more of these components can lead the entire shoulder region to be at an increased risk of overuse acute shoulder injuries.
The interaction between static and dynamic stabilizers and the favorable joint structure allow the shoulder the greatest ROM of any joint in the body. This large ROM makes maintaining stabilization in the shoulder joint a major concern to the tennis player. The difficulty in maintaining this stabilization is a result of the rapid velocity of the tennis strokes. Peak velocity of a tennis racquet in the serve has been reported at 62 to 72 miles per hour (30), which corresponds to ball velocities between 83 to 125 miles per hour (8). These velocities are likely to be higher in today’s high level junior, collegiate and professional tennis players as this research was performed in early 1990s, before the advent of the new racquet and string technology.
Maintaining stability in the joints is achieved in two ways: static and dynamic stabilization. Static stability of the shoulder is achieved via the capsuloligamentous structures, including the glenoid labrum, glenohumeral joint capsule, glenohumeral ligaments, and intra-articular pressure providing static joint stability (39). Dynamic stability of the shoulder is achieved by the rotator cuff (supraspinatus, infraspinatus, teres minor, subscapularis), deltoid, bicep brachii, teres major, latissimus dorsi and pectoralis major (39).
The interaction between the static and dynamic components of functional stability is mediated by the sensorimotor system. This sensorimotor system includes the sensory, motor and central integration and processing components of the central nervous system (CNS) involved in maintaining functional joint stability (57). Sensory information (proprioception) travels through afferent pathways to the CNS where it is integrated with input from other levels of the nervous system, causing efferent motor responses (neuromuscular control) vital to coordinated movement patterns and functional stability of the shoulder region.
The rotator cuff is a group of muscles consisting of the supraspinatus, infraspinatus, teres minor, and subscapularis that acts as a steering mechanism for the humeral head. The humeral head is the top of the bone that connects into the shoulder joint. Three dimensional movements or rotations of the humeral head are the result of the rotator cuff muscles and static stabilizers. Rotator cuff activation results in humeral head rotation and depression in positions of abduction. Given this anatomical location, the rotator cuff is well situated to provide stability to a dynamic fulcrum during glenohumeral abduction—which is the typical position during most tennis strokes.
The rotator cuff functions to dynamically rotate the humerus, depress the humeral head, and provide joint stability both during tennis strokes and at rest between points. For the rotator cuff to be able to perform its functions, the scapula must provide a stable base at the origin of the cuff muscles. Therefore, the muscles that stabilize the scapula play a large role in dynamic internal and external rotation of the shoulder (9). The rotator cuff functions to provide both acceleration of the humerus during the tennis serve and forehand as well as eccentric deceleration during follow-through (48).
The research on tennis shoulder function and improved performance has produced some information that can be helpful for coaches, clinicians, and players. The unilateral nature of tennis causes asymmetries between the dominant and nondominant shoulder. More torque is produced in internal rotation at 60 and 300 deg/sec in the dominant arm compared to the nondominant arm in tennis players (9). This is a result of the adaptation of training—specifically the service motion. However, tennis players have a decreased internal shoulder range of motion (ROM), that has been explained as an adaptation of the posterior shoulder musculature and capsular structures to the tennis stroke (10). The muscles of the posterior shoulder in the serving arm must decelerate the shoulder via eccentric muscle contractions during the follow-through. The faster the serve, the more strength is required to decelerate the arm. As the game of tennis has evolved with technological and training advancements, the speed of the serve has increased substantially in the last 15 years and will likely continue.
The physical demands of tennis cause musculoskeletal adaptations, sometimes positive, like increases in strength, while sometimes negative — decreased joint ROM. These repeated demands to produce force by muscle shortening can cause a cycle of microtrauma to the tight muscle, followed by scar formation, followed by more microtrauma with continued use (22, 32). These adaptations become maladaptations, reducing joint range of motion, changing biomechanical patterns, and decreasing the efficiency of force production, increasing the chance of injury to the muscle (10). Shoulder injuries are typically due to inflammation and/or impingement of the rotator cuff muscles and tendon. Inflammation is usually caused by the repetitive microtrauma received from the stresses imposed by hitting groundstrokes and overhead serving, while impingement is the direct compression of soft tissue between the harder (bony) parts of the joint. Both are usually associated with instability of the glenohumeral joint (6).
Although there could be multiple causes for rotator cuff injuries in tennis players, a large number of injuries are a result of a player’s poor technique and strength imbalances between external and internal shoulder rotators. At the time of maximum external rotation where the arm is ready to execute the contact of the ball, the shoulder’s internal rotator muscles contract eccentrically, generating a high force. The resultant forward movement produces high accelerations that must be decelerated at the end of the range of movement. Shoulder muscles are susceptible to injury at these two extreme positions in the movement (37).
To further explore the internal/external shoulder ratio, a study looking at the consequence of repetitive elite level tennis was undertaken on the juniors of the United States Tennis Association’s National Team and also on touring professionals. The results identified increases in dominant-arm internal rotation deficiencies relative to the nondominant arm as related to increases in both player age and number of years of competitive tennis (49). They found decreases in dominant arm internal ROM and recommended corrective training to enhance performance and prevent injury.
As junior competitive tennis players age, there seems to be an increase in shoulder problems. A study looking at this scenario found a significant increase in internal ROM between ages 14 and 15 that remain stable at age 16, but decreases slightly at age 17 (49). It was also found that the total dominant and nondominant ROM of the players across the four age groups (14-17) revealed a strong significant main effect of age for the nondominant ROM’s but not for the dominant ROM’s. This study showed that dominant arm internal ROM decreased compared to nondominant internal ROM. External rotation ROM did not significantly change in nationally ranked junior tennis players tested between the ages of 14 and 17 years. This would suggest that junior competitive tennis player’s need to include an internal shoulder range of motion program to prevent the onset of flexibility imbalances that are common in players as they age.
Examination of force-velocity relationships (Figure 5.6) shows that muscle tension at the same velocity is always greater in eccentric work, and this difference becomes greater as a function of increases in contraction velocity (35). Eccentric muscular contractions play a role in normal functional activities, but in the tennis shoulder (rotator cuff), the infraspinatus and teres minor are of major importance during the follow through of both the groundstrokes, but more specifically the service motion. These two muscles undergo high decelerative eccentric muscle contractions to preserve healthy joint function (16). The role of the rotator cuff is essential in preventing overhead overuse injuries.
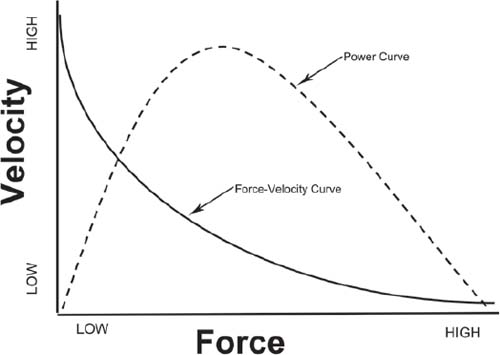
Figure 5.6: Force-velocity curve.
Many problems with the elbow can originate as a result of shoulder related issues. Lateral epicondylitis (tennis elbow) and medial epicondylitis in the elbow region can be caused by poor mechanics and muscle imbalance in the shoulder region (29).
The structures indicated in tennis elbow are primarily the tendon of the extensor carpi radialis brevis and secondarily the tendon of the extensor carpi radialis longus and extensor digitorum. While both an inflammation response and degeneration can occur in the tendon, the latter appears to be the more accepted mechanism causing “tennis elbow” (43). Shoulder inflexibility, which may alter a player’s technical form, can also be a factor in elbow injuries (10).
Today’s extreme grips and open stance groundstrokes to increase topspin place a great deal of stress on the shoulder, elbow, forearm, and wrist. These movements are mimicked by younger players who may not have adequate strength and/or coordination to perform them without risk of injury.
The back, core, and hips are of vital importance in tennis. They act as a center of rotation and are vital to transmit forces generated in the lower body up through the upper body and into the tennis stroke. Weakness or limitations in this area can reduce force and power transfer. In a six year study of US competitive junior tennis players competing in the boys’ national championships between 1986-1992, it was found that lower back injuries were the most common injury (28). Playing on hard court surfaces, which are highly prevalent in competitive junior and professional tennis, is likely to increase the occurrence of lower back injuries. This is due to the higher ground reaction forces on hardcourts as compared to softer surfaces such as grass or clay. For this reason, it is important that appropriate flexibility and strength training is prescribed for athletes, especially if the tennis player trains or competes on hard courts.
The three major lower back/core muscles involved during tennis play are (1) the posterior midline paraspinal musculature which are highly involved during the service motion (2), the quadratus lumborum or oblique muscles which are highly involved in the ground strokes and quick movements during the service motion, and (3) the rectus abdominus which is highly involved in the service motion and hitting overheads.
High level tennis competition requires the fine interplay of performance and injury prevention. Continual tennis play, without an appropriate physical conditioning program, results in reduced range of motion in the glenohumeral joint, and this can cause impingement and other injury and pain symptoms. As junior tennis players age, their internal shoulder ROM is decreased. Total ROM (combined ROM of internal and external rotation) typically increases in the nondominant arm of tennis players, but decreases or does not improve in the dominant arm. As a result all tennis players should have a daily flexibility program for the shoulder area focused on improving ROM.
The greater an athlete’s internal shoulder rotational strength the greater the speed of the serve and forehand. Weak external shoulder rotational strength, which is the major contributor to deceleration, will lead to greater injury risk. So developing internal rotational strength without external rotational strength will only increase the imbalance between the internal and external rotation strength, leading to a greater chance of injury. All competitive tennis players should be on a resistance program focused on developing external rotational strength to reduce the muscle asymmetry in shoulder rotation strength.
Tennis training alone does not develop the appropriate shoulder strength or satisfactory ROM. Therefore, supplemental resistive shoulder exercises must be added to any competitive tennis player’s program. Exercises for tennis players to strengthen the shoulder in external rotation, including the posterior cuff muscles and the scapular stabilizers, will help maintain a favorable external/internal rotation strength balance and may prevent or lessen the severity of repetitive overload injuries. For a performance conditioning program, either preventative or rehabilitative, to address the needs of the individual tennis player, an appropriate evaluation of the athlete in terms of fitness and injury history must be obtained. From the initial screening a program designed to improve performance and prevent injury should be implemented.
1. Andersen, J. C. Stretching before and after exercise: Effect on muscle soreness and injury risk. Journal of Athletic Training. 40:218-220, 2005.
2. Avela, J., H. Kyröläinen, and P. V. Komi. Altered reflex sensitivity after repeated and prolonged passive muscle stretching. J Appl Physiol. 86:1283-1291, 1999.
3. Bandy, W. D. and J. M. Irion. The effect of time on static stretch on the flexibility of the hamstring muscles. Phys Ther. 74:845-850, 1994.
4. Bergh, U. and B. Ekblom. Physical performance and peak aerobic power at different body temperatures. Journal of Applied Physiology. 46:885-889, 1979.
5. Bixler, B. and R. L. Jones. High school football injuries: effects of a post-halftime warm-up and stretching routine. Fam Pract Res J. 12:131-139, 1992.
6. Blevins, F. T. Rotator cuff pathology in athletes. Sports Medicine. 24:205-220, 1997.
7. Blomstrand, E. V., B. Bergh, B. Essen-Gustavsson, and B. Ekblom. The influence of muscle temperature on muscle metabolism and during intense dynamic exercise. Acta Physiologica Scandinavica. 120:229-236, 1984.
8. Chandler, T. J. Exercise training for tennis. Clinics in Sports Medicine. 14:33-46, 1995.
9. Chandler, T. J., W. B. Kibler, E. C. Stracener, A. K. Ziegler, and B. Pace. Shoulder strength, power, and endurance in college tennis players. American Journal of Sports Medicine. 20:455-458, 1992.
10. Chandler, T. J., W. B. Kibler, T. L. Uhl, B. Wooten, A. Kiser, and E. Stone. Flexibility comparisons of junior elite tennis players to other athletes. American Journal of Sports Medicine. 18:134-136, 1990.
11. Comeau, M. J. Stretch or no stretch? Cons. Strength and conditioning Journal. 24:20-21, 2002.
12. Cornwell, A., A. G. Nelson, G. D. Heise, and B. Sidaway. The acute effects of passive muscle stretching on vertical jump performance. J Hum Mov Stud. 40:307-324, 2001.
13. Cornwell, A., A. G. Nelson, and B. Sidaway. Acute effects of stretching on the neuromechanical properties of the triceps surae muscle complex. Eur J Appl Physiol. 86:428-434, 2002.
14. Cross, K. M. and T. W. Worrell. Effects of static stretching program on the incidence of lower extremity musculotendinous strains. Journal of Athletic Training. 34:11-14, 1999.
15. DeVries, H. A. The “looseness” factor in speed and O2 consumption of an anaerobic 100-yard dash. Res Q. 34:305-313, 1963.
16. Duda, M. Prevention and treatment of throwing arm injuries. Physician Sports Medicine. 13:181-185, 1985.
17. Ekstrand, J. and J. Gillquist. The avoidability of soccer injuries. Int J Sport Med. 4:124-128, 1983.
18. Ellenbecker, T. S., E. P. Roetert, P. A. Piorkowski, and D. A. Schultz. Glenohumeral joint internal and external rotation range of motion in elite junior tennis players. J. Orthop. Sports Phys. Ther. 24:336-341, 1997.
19. Evetovich, T. K., N. J. Nauman, D. S. Conley, and J. B. Todd. Effect of static stretching of the bicep brachii on torque, electromyography, and mechanomyography during concentric isokinetic muscle action. Journal of Strength and Conditioning Research. 17:484-488, 2003.
20. Fletcher, I. M. and B. Jones. The effect of different warm-up stretch protocols on 20-m sprint performance in trained rugby union players. J Strength Cond Res. 18:885-888, 2004.
21. Fowles, J. R., D. G. Sale, and J. D. MacDougall. Reduced strength after passive stretch of the human plantar flexors. J Appl Physiol. 89:1179-1188, 2000.
22. Garrett, W. E. Basic science of musculotendinous injuries. In: The lower extremity and spine in sports medicine. E. B. Hershman (Ed.) St.Louis: CV Mosby, 1986, pp. 42–58.
23. Garrett, W. E. Muscle flexibility and function under stretch. In: Sports and exercise in midlife. S. L. Gordon, X. Gonzalez-Mestre, and W. E. Garrett (Eds.) Rosemont, IL: American Academy of Orthopaedic Surgeons, 1993, pp. 105–116.
24. Gleim, G. W. and M. P. McHugh. Flexibility and its effects on sports injury and performance. Sports Medicine. 24:289-299, 1997.
25. Hartig, D. E. and J. M. Henderson. Increasing hamstring flexibility decreases lower extremity overuse injuries in military basic trainees. Am J Sports Med. 27:173-176, 1999.
26. Herbert, R. D. and M. Gabriel. Effects of stretching before and after exercising on muscle soreness and risk of injury: Systematic review. Br Med J. 325:468-470, 2002.
27. Hunter, D. G. and J. Spriggs. Investigation into the relationship between the passive flexibility and active stiffness of the ankle plantar-flexor muscles. Clinical Biomechanics. 15:600-606, 2000.
28. Hutchinson, M. R., R. F. Laprade, Q. M. Burnett, R. Moss, and J. Terpstra. Injury surveillance at the USTA boys’ tennis championships: A 6-yr study. Med Sci Sport Exercise. 27:826-830, 1995.
29. Kibler, W. B. Clinical biomechanics of the elbow in tennis: implications for evaluation and diagnosis. Med Sci Sports Exerc. 26:1203-1206, 1994.
30. Kibler, W. B. and T. J. Chandler. Racquet Sports. In: Sports Injuries, Mechanisms, Prevention, Treatment. F. H. Fu and D. A. Stone (Eds.) Baltimore, MD: Williams & Wilkins, 1994.
31. Kibler, W. B., T. J. Chandler, B. P. Livingston, and E. P. Roetert. Shoulder range of motion in elite tennis players. American Journal of Sports Medicine. 24:279-285, 1996.
32. Kibler, W. B., C. McQueen, and T. Uhl. Fitness evaluations and fitness findings in competitive junior tennis players. Clin Sports Medicine. 7:403-416, 1988.
33. Knudson, D. V., G. J. Noffal, R. E. Bahamonde, J. A. Bauer, and J. R. Blackwell. Stretching has no effect on tennis serve performance. J Strength Cond Res. 18:654-656, 2004.
34. Kokkonen, J., A. G. Nelson, and A. Cornwell. Acute muscle stretching inhibits maximal strength performance. Res Q Exerc Sport. 69:411-415, 1998.
35. Komi, P. V. and H. Rusko. Quantitative evaluation of mechanical and electrical changes during fatigue loading of eccentric and concentric work. Scand J Rehab Med. 3:21-26, 1974.
36. Kovacs, M. S. The argument against static stretching before sport and physical activity. Athletic Therapy Today. 11:24-25, 2006.
37. Lees, A. Science and the major racket sports: a review. Journal of Sports Sciences. 21:707-732, 2003.
38. Levine, U., J. Lombardo, J. McNeeley, and T. Anderson. An analysis of individual stretching programs of intercollegiate athletes. Physician Sports Medicine. 15:130-136, 1987.
39. Myers, J. B. and S. M. Lephart. The role of the sensorimotor system in the athletic shoulder. J Athl Train. 35:351-363, 2000.
40. Nelson, A. G., N. M. Driscoll, M. A. Young, and I. C. Schexnayder. Acute effects of passive muscle stretching on sprint performance. J Sport Sci. 23:449-454, 2005.
41. Nelson, A. G., I. K. Guillory, A. Cornwell, and J. Kokkonen. Inhibition of maximal voluntary isokinetic torque production following stretching is velocity specific. J Strength Cond Res. 15:241-246, 2001.
42. Nelson, A. G. and J. Kokkonen. Acute ballistic muscle stretching inhibits maximal strength performance. Res Q Exerc Sport. 72:415-419, 2001.
43. Pluim, B. M. Rackets, strings and balls in relation to tennis elbow. In: Tennis Science and Technology. S. Haake and A. O. Coe (Eds.) Oxford: Blackwell, 2000.
44. Pope, R. P., R. D. Herbert, and J. D. Kirwan. Effects of flexibility and stretching on injury risk in army recruits. Australian Journal of Physiotherapy. 44:165-172, 1998.
45. Pope, R. P., R. D. Herbert, J. D. Kirwan, and B. J. Graham. A randomized trial of pre exercise stretching for prevention of lower-limb injury. Med Sci Sports Exerc. 32:271-277, 2000.
46. Priest, J. D., V. Braden, and S. G. Gerberich. The elbow and tennis, part 1. Physician Sportsmed. 8:81-91, 1980.
47. Renstrom, P. A. F. H. (Ed.). Tennis. Malden, MA: Blackwell, 2002.
48. Rhu, K. N., F. W. McCormick, F. W. Jobe, D. R. Moynes, and D. J. Antonell. An electromyographic analysis of shoulder function in tennis players. American Journal of Sports Medicine. 16:481-485, 1988.
49. Roetert, E. P., T. S. Ellenbecker, and S. W. Brown. Shoulder internal and external rotation range of motion in nationally ranked junior tennis players: A longitudinal analysis. Journal of Strength and Conditioning Research. 14:140-143, 2000.
50. Shellock, F. G. and W. E. Prentice. Warming up and stretching for improved physical performance and prevention of sports related injuries. Sport Med. 2:267-268, 1985.
51. Shrier, I. Does stretching improve performance?: a systematic and critical review of the literature. Clin J Sport Med. 14:267-273, 2004.
52. Shrier, I. Flexibility versus stretching. Br J Sports Med. 35:364, 2001.
53. Shrier, I. Stretching before exercise does not reduce the risk of local muscle injury. A critical review of the clinical and basic science literature. Clin. J. Sports Med. 9:221-227, 1999.
54. Shrier, I. and K. Gossal. Myths and truths of stretching. The Physician and Sports Medicine. 28:57-63, 2000.
55. Thacker, S. B., J. Gilchrist, and D. F. Stroup. The impact of stretching on sports injury risk: a systematic review of the literature. Med Sci Sport Exercise. 36:371-378, 2004.
56. Wessel, J. and A. Wan. effect of stretching on the intensity of delayed-onset muscle soreness. Clinical Journal of Sport Medicine. 4:83-87, 1994.
57. Wilmore, J. H. and D. L. Costill. Physiology of Sport and Exercise. 3rd ed. Champaign, IL: Human Kinetics, 2004
58. Wilson, G. J., A. J. Murphy, and J. F. Pryor. Musculotendinous stiffness: its relationship to eccentric, isometric, and concentric performance. J Appl Physiol. 76:2714-2719, 1994.
59. Winge, S., U. Jorgensen, and A. L. Nielsen. Epidemiology of injuries in Danish championship tennis. Int J Sports Med. 10:368-371, 1989.
60. Yeung, E. W. and S. S. Yeung. A systematic review of interventions to prevent lower limb soft tissue running injuries. Br J Sports Med. 35:383-389, 2001.
61. Young, W. and S. Elliott. Acute effects of static stretching, proprioceptive neuromuscular facilitation stretching, and maximum voluntary contractions on explosive force production and jumping performance. Res Q Exerc Sport. 72:273-279, 2001.
62. Young, W. B. and D. G. Behm. Effects of running, static stretching and practice jumps on explosive force production and jumping performance. J Sports Med Phys Fitness. 43:21-27, 2003.