Background
Proper patient positioning is mandatory to provide optimal surgical access.
Incorrect positioning is a risk factor for potentially severe long-term complications.
Patients cannot communicate pain or other symptoms during surgery under general anesthesia.
The lithotomy position can cause increased intracompartmental pressure (ICP) especially in the calf.
Epidemiology
One of the first and critical steps for any surgery is proper patient positioning. Its importance is often underestimated or performed by less experienced personnel. It is important to ensure adequate surgical exposure and optimal surgical access. Careful positioning also minimizes the risk of perioperative complications. Optimal perioperative positioning depends on the procedure and the surgeons’ preferred approach. In the United States, 16% of surgically treated patients claim neural injuries while under anesthesia. In medical malpractice cases, injuries to the ulnar nerve (28%) or brachial plexus (20%) were most commonly claimed. Nearly half (45%) of these patients received a median payment of USD 35,000 for their claims [1]. Of these malpractice claims, 21.5% reported pressure ulcers due to inadequate surgical positioning [2]. The less physiologically the patient is positioned, the higher the risks for position-related complications.
An equally severe perioperative complication is compartment syndrome due to improper patient positioning. Its development is particularly dangerous because patients are unable to express pain and discomfort. Orthopedic and trauma surgeons are familiar with compartment syndrome treatment. However, other surgical specialties may only be confronted with compartment syndrome in the face of improper patient positioning of their own patients. Compartment syndrome develops most commonly in the calf. Prolonged positioning with intrusion of the forearm heightens the risk of development of a compartment syndrome. Further, one general risk factor that must always be considered is coagulopathy.
Positioning should maximize pressure distribution to avoid compression injuries to soft tissues or underlying neural structures. Every potential surgical position has advantages and pitfalls that medical personnel should be familiar with and consider when preparing for the procedure. This chapter serves to highlight specific risk factors in patient positioning for operative and nonoperative procedures in a variety of surgical subspecialties.
Compartment Syndrome
General Causes of Compartment Syndrome During Patient Positioning
Prolonged direct pressure of the affected compartment. This scenario leads to edema, which increases compartmental pressure.
Venous obstruction can elevate compartment pressures. Decreased venous drainage leads to extracellular fluid accumulation and edema.
Insufficient perfusion. Diminished perfusion decreases tissue oxygen saturation leading to hypoxia, cellular edema, and ultimately cell death.
Positioning of extremities alone can change intracompartmental pressures. For example, sustained dorsiflexion of the ankle physiologically increases intracompartmental pressure of the calf.
Inappropriate fluid accumulation, for example, during misplaced/extravasal IV line.
Increased bleeding due to coagulopathy.
Duration of the procedure: After more than 5 hours of surgery, the risk of compartment syndrome rises significantly.
Summary of general risk factors in the development of a compartment syndrome during patient positioning or during surgical procedure
Prolonged surgery time (>5 hour) Lithotomy position Pressure on extremities Vascular obstruction Vascular procedures Inappropriate fluid accumulation |
Prolonged pressure |
Hypoperfusion Coagulopathy |
Specific Surgical Positions Associated with Compartment Syndrome
Supine Position
Pressure on the extremity due to fixation or a surgeon leaning against an extremity
Extremities elevated above the level of the heart such as in angulated supine positioning
Venous obstruction such as thoracic outlet syndrome
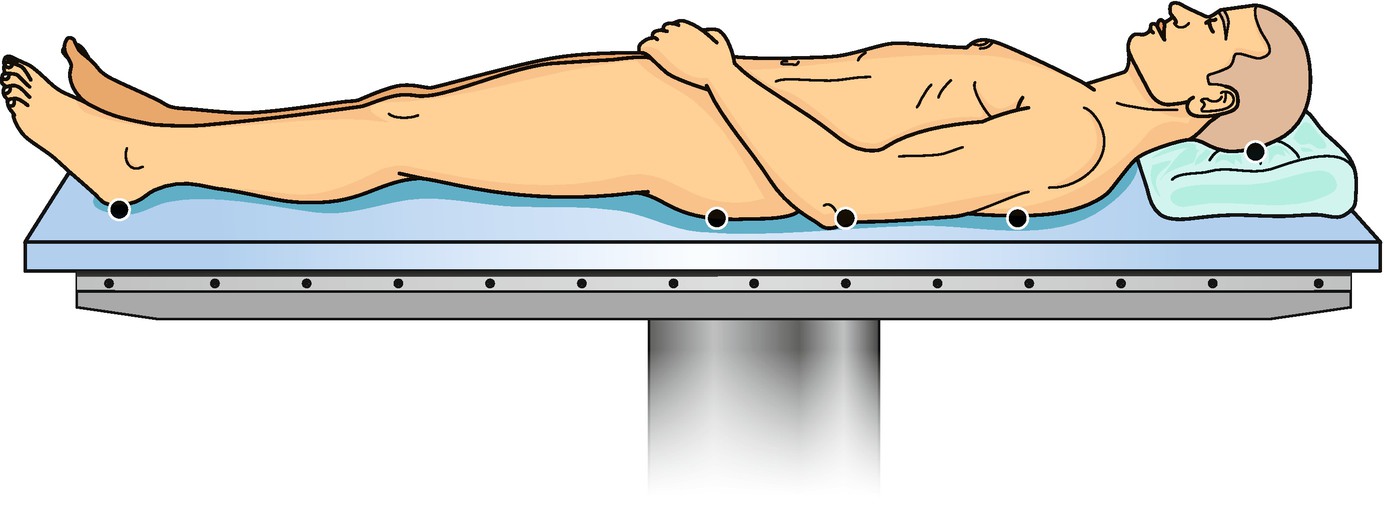
Supine position with typical pressure points
Lateral Decubitus Position
Pressure on the contralateral lower extremity
Venous obstruction in the inguinal region due to hip flexion
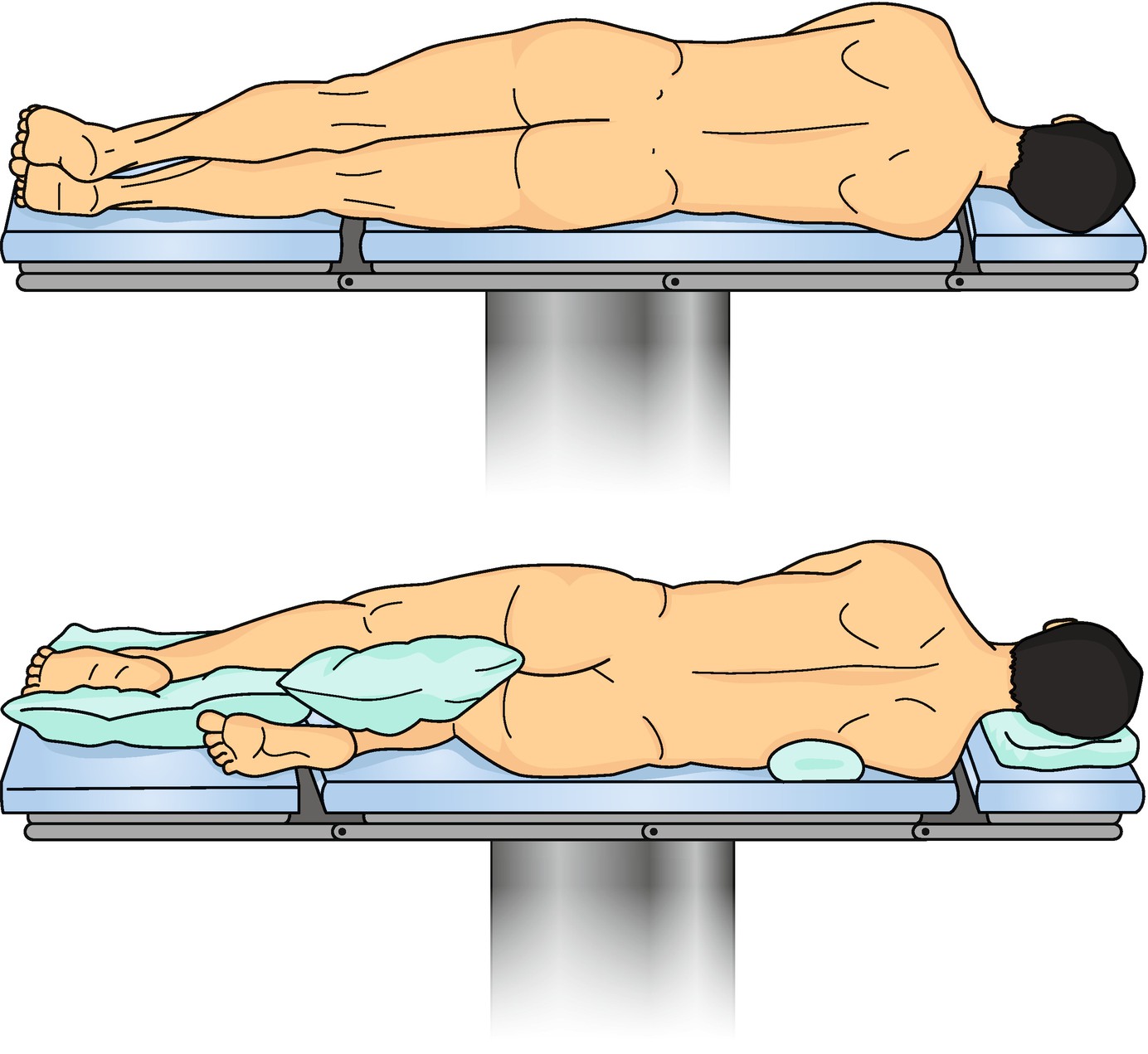
Example of lateral decubitus position
This condition can lead to limb complications including ischemia, transient paresthesias, and rhabdomyolysis with the subsequent potential for renal failure. In one study, transient neurologic symptoms occurred after 5 hours and 45 minutes, with persistent neurologic deficits occurring after 8 hours. Another study that measured compartment pressures in healthy volunteers found that anterior tibial compartmental pressures in the bottom positioned contralateral leg could reach 240 mm Hg [3]. Compartment pressures of the anterior compartment of the bottom leg during compression by the upper leg showed elevated maximum average pressures of 57 mm Hg when padded on a soft surface and rises to an average 64 mm Hg on hard surfaces. The bottom upper extremity, compressed by the torso, showed maximum average compartment pressures of 100 mm Hg in the anterior flexor compartments. When the risk factors of pressure and vascular obstruction are combined, the risk of compartment syndrome rises significantly, especially in the bottom lower limb.
Prone Position
Vascular obstruction in the inguinal region due to the patients’ weight
Pressure on the thighs
Intra-orbital edema due to increased pressure in the fascial region
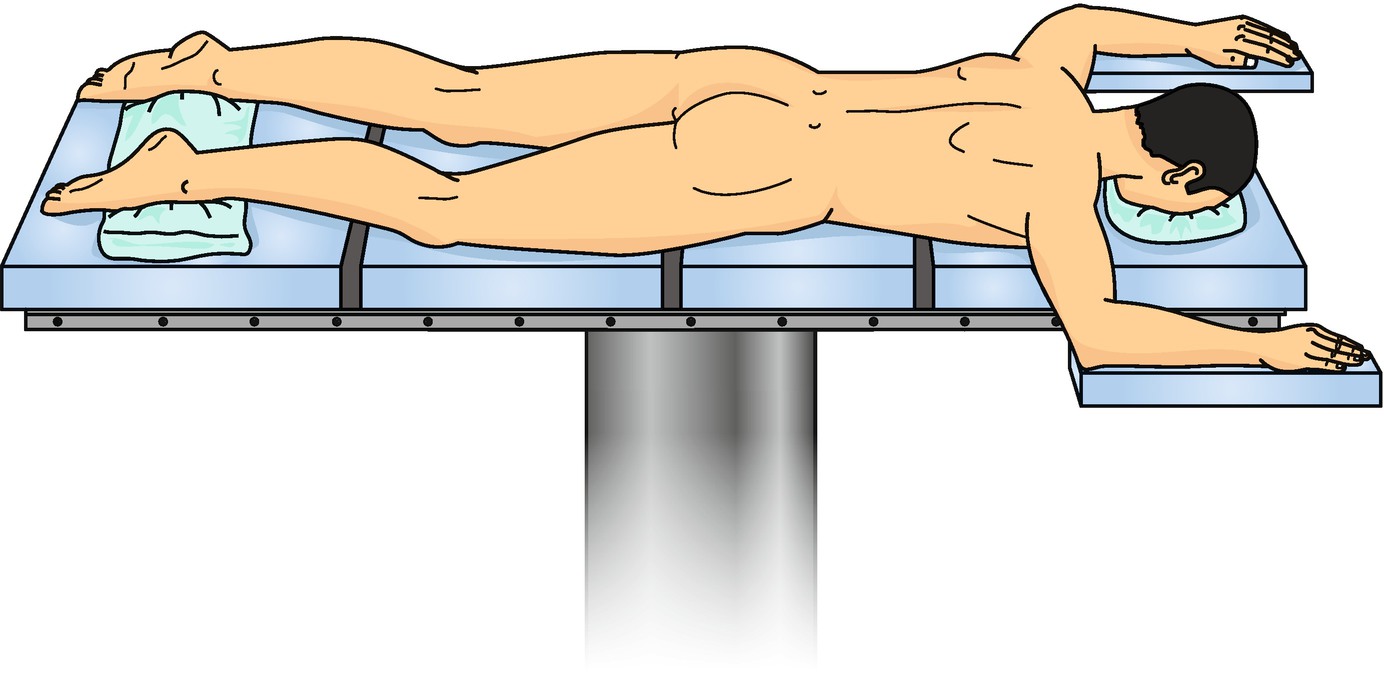
Prone position: This position is more complex because it requires more personnel and higher anesthesiologic attention prior and during positioning
Fortunately, no wide-spread reports of compartment syndrome are available. One case [4], however, reported a compartment syndrome of the anterior compartment of the thigh after a procedure on the lumbosacral spine in prone position. Vascular obstruction in the inguinal region was postulated as the most likely cause of this complication. The combination of diminished inguinal blood flow and increased local pressure on the thigh in overweight patients raises the risk of developing compartment syndrome. Visual loss is also a known complication associated with prone positioning. Should a patient’s head be positioned improperly on a soft headrest device, particularly if direct pressure on the eye is observed, the risk of orbital edema and subsequent compartment syndrome rises. While this complication is very rare, cases of ischemic orbital compartment syndrome have been reported in the literature [5].
Lithotomy Position
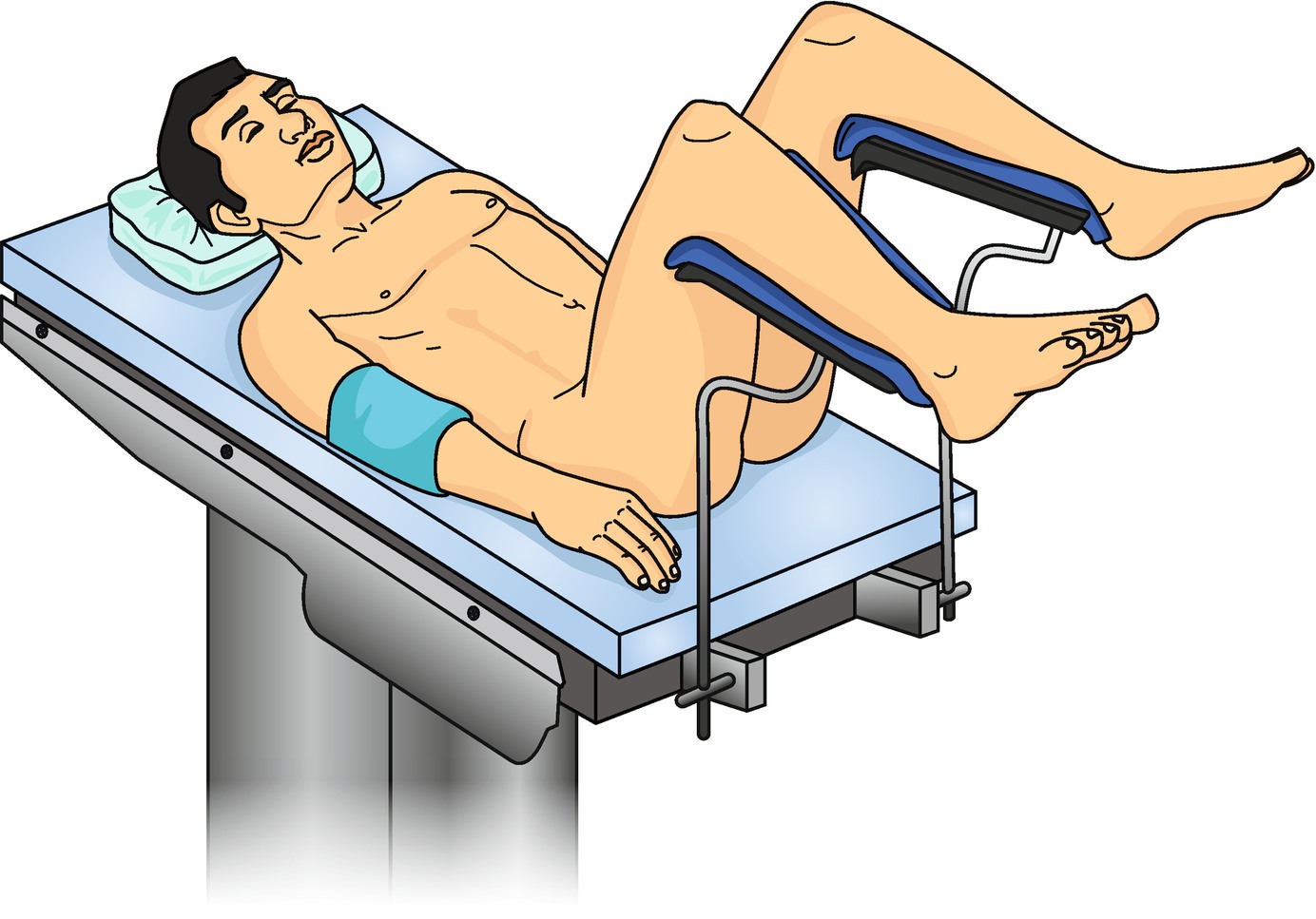
Lithotomy position: During procedure, the surgeon gains good access to the perineal region. The elevated legs and the flexion in the hip are next to the pressure on the lower extremities considered as risk factors in the development of compart syndrome most commonly in the calf region
Pressure on the lower legs due to fixation of the legs on a support
Legs elevated above the level of the heart
Venous obstruction in the inguinal region due to hip flexion
The fixation of the legs produces increased external pressure, which subsequently causes intracompartmental edema, thereby raising intracompartmental pressure which may ultimately lead to compartment syndrome. Elevation of the legs above the level of the heart lowers local tissue perfusion, inducing hypoxia and producing edema or even tissue necrosis. In extreme cases, rhabdomyolysis and compartment syndrome result. Oftentimes, the lithotomy position requires hip flexion of at least 90°. Venous obstruction in the inguinal region may result, thereby lowering venous return, which allows interstitial fluid to accumulate, causing edema and increased compartment pressure.
Beach Chair Position
Inguinal venous obstruction
Pressure on the extremity due to fixation
Elevation of the lower extremities due to Trendelenburg in modified beach chair positioning
In a case report of a laparoscopic robot-assisted cystoprostatectomy in modified beach chair position with Trendelenburg for 6 hours and total surgery time of 11 hours, Galyon et al. [9] reported compartment syndrome of limbs requiring fasciotomy. The etiology was postulated to be a combination of long duration of surgery, high BMI (33.9 Kg/m2), obstruction of venous outflow in the lower extremity, hypoperfusion, and pressure due to fixation.
Gluteal Compartment Syndrome
Prolonged immobilization
Epidural analgesia in the setting of joint arthroplasty
Infection
Trauma
Vascular surgery
Intramuscular drug abuse
Altered level of consciousness (alcohol or drug overdose)
Position-specific pathophysiologic response in the development of compartment syndrome
Lithotomy position | Elevation of the legs |
Pressure on legs due to fixation | |
Vascular obstruction in the inguinal region | |
Lateral decubitus position | Pressure on the lower extremities on the nonoperated site |
Obstruction of vascular structures in the inguinal region | |
Supine position | Pressure on extremities |
Vascular obstruction in the neck | |
Elevation of extremities in angulated supine positioning | |
Prone position | Vascular obstruction in the groin |
Pressure on the thigh | |
Increased pressure in the facial region | |
Beach chair position | Inguinal vascular obstruction |
Pressure on extremities due to fixation | |
Elevation of the extremity |
Intraoperative Diagnosis of Compartment Syndrome
Prolonged time of surgery (>5 hours)
Lithotomy position
Pressure on the extremities
Inguinal vascular obstruction
If a compartment syndrome is suspected intraoperatively, the authors recommend measuring intracompartmental pressures with an ICP device while the patient is under general anesthesia. Normal physiologic supine intracompartmental pressure of an extremity at heart level is 5 mm Hg. Compartment syndrome is defined as an intracompartmental pressure 30 mm Hg greater than the diastolic blood pressure and serves as the threshold for surgical decompression of the compartment [11].
Therapeutic Recommendations

Intraoperative documentation of an early compartment syndrome depicts immediately below the fasciotomy and swelling of the calf muscle as a sign of early compartment syndrome
Limitations and Pitfalls
The diagnosis of compartment syndrome is challenging, especially intraoperatively during general anesthesia, because patients are not able to express their symptoms. The lithotomy position is most commonly associated with the development of positional compartment syndrome. This position is mainly used for urologic and gynecologic procedures. Oftentimes, urologists and gynecologists are not routinely involved in treating compartment syndrome, as treatment is usually managed by general, orthopedic, or trauma surgeons. Physicians that are experienced in the diagnosis and treatment of compartment syndrome should be promptly consulted if a compartment syndrome is suspected intra- or postoperatively.
While technical and digital advances in surgery provide huge potential for minimally invasive surgery with less surgical complications and morbidity, it is also associated with new complications. This case is especially true in robotic surgery (e.g., DaVinci) as the surgeon is not directly next to the patient. While focus on the procedure is high, the overview of the patient as a whole decreases, which potentially risks missing perioperative complications around the operating field.
Future Directions
Compartment syndrome due to surgical positioning is an uncommon complication, but can be associated with severe impacts on patient quality of life. The development of noninvasive devices for monitoring intracompartmental pressure intraoperatively and postoperatively represents a useful direction for future research and development.

Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.