APPENDIX A
PERSPECTIVES ON PSYCHIC DIAGNOSIS
by C. Norman Shealy, M.D.
 The interest in clairvoyant diagnosis-or psychic diagnosis, if you prefer-almost certainly goes back to the days of Hippocrates. Many famous physicians throughout the history of the world seem to have been involved in things which we today would call parapsychology, and many of them were probably psychic themselves. Paracelsus is one example of such an individual; Mesmer, who some 200 years ago laid the foundations of psychiatry and psychology, is another. To my knowledge, however, the first formal study of clairvoyant diagnosis occurred about 130 years ago, when a British physician, John Elliotson, began to work with mesmerism. Dr. Elliotson had introduced to England the stethoscope, the use of narcotics, and a variety of other medical advances. He was the leading internist in London and a professor of medicine at University Hospital, University College, London. But suddenly he became bored with what was going on in medicine and got involved in mesmerism. He then learned that patients who were mesmerized could properly diagnose difficult medical cases. He would carry one of his mesmerized patients through the wards and have him diagnose patients
whose illnesses had confounded the faculty. He even staged public demonstrations in the hospital amphitheater. Among the people who attended these demonstrations were Charles Dickens and William Thackeray. (Thackeray later dedicated one of his books to Elliotson, who in the book is called Dr. Goodenough.)
The interest in clairvoyant diagnosis-or psychic diagnosis, if you prefer-almost certainly goes back to the days of Hippocrates. Many famous physicians throughout the history of the world seem to have been involved in things which we today would call parapsychology, and many of them were probably psychic themselves. Paracelsus is one example of such an individual; Mesmer, who some 200 years ago laid the foundations of psychiatry and psychology, is another. To my knowledge, however, the first formal study of clairvoyant diagnosis occurred about 130 years ago, when a British physician, John Elliotson, began to work with mesmerism. Dr. Elliotson had introduced to England the stethoscope, the use of narcotics, and a variety of other medical advances. He was the leading internist in London and a professor of medicine at University Hospital, University College, London. But suddenly he became bored with what was going on in medicine and got involved in mesmerism. He then learned that patients who were mesmerized could properly diagnose difficult medical cases. He would carry one of his mesmerized patients through the wards and have him diagnose patients
whose illnesses had confounded the faculty. He even staged public demonstrations in the hospital amphitheater. Among the people who attended these demonstrations were Charles Dickens and William Thackeray. (Thackeray later dedicated one of his books to Elliotson, who in the book is called Dr. Goodenough.)
As anyone acquainted with the history of medicine might expect, such innovative ideas were not well received among his conservative colleagues. They finally suggested that if Elliotson wished to continue to practice medicine, he should give up that nonsense. His reaction was: “Gentlemen, I resign.” He then went out and continued to practice mesmerism, demonstrating, among other things, that mesmerized patients could be successfully operated on, apparently without feeling any pain. Elliotson, because of his tilting at the windmill of traditional medicine, is not well known today, and no serious scientific study of clairvoyant diagnosis has been done since his time.
In 1951, as an undergraduate student at Duke University, I was invited by the Duke Players, of which I was a member, to write a radio skit on parapsychology. I spent three-and-a-half months working with Dr. J.B. Rhine, not as one of his subjects, but observing what he was doing and conducting an investigation of his work. I was totally convinced that clairvoyance, telepathy, and psychokinesis were very real phenomena, and I wondered why, after almost 30 years of experimentation, we were still playing with cards and dice and not using these techniques in a practical way. Then the rigors of medical school caused me to put aside my interest in parapsychology until about five years ago, when I became intensely interested in it again after reading Psychic Discoveries Behind the Iron Curtain and Breakthrough to Creativity.
I tried to obtain an introduction to clairvoyance through Dr. Karagulla, author of Breakthrough to Creativity, but she would not divulge any of her secret connections. Finally, thanks to Dr. Paul Dudley White, I was asked to speak at a meeting of the Academy of Parapsychology and Medicine at Stanford just three years ago. This immediately put me in contact with individuals who eventually led me to meet my first known psychic, the Reverend Henry Rucker of Chicago. I was so intrigued by Henry's analysis of me, whom he had never met before, that I invited him and his colleagues to come to La Crosse so that I might see how good they would be at doing psychic diagnoses.
During that first weekend we saw 17 patients. Each patient was brought into a room for about 10 minutes. The patient was then escorted out of the room, and each of the sensitives was asked a variety of questions concerning the patient's personality and physical condition. We then pooled the results; only when a clear majority of the sensitives agreed on a given diagnosis was it considered the proper answer. Pooling the results of the eight psychics and considering their responses to eight individual questions, we found this group to be 98% accurate in making personality diagnoses and 80% accurate in diagnosing physical conditions. For instance, they clearly distinguished between three totally separate cases of paraplegia—paralysis from the waist down-one traumatic, one infectious, and one degenerative in nature.
A more formal research project was then done with 54 different questions. Each patient to be studied was known to me, had been examined by me, and had taken an elaborate personality test, the Minnesota Multi-Phasic Personality Inventory. A color Polaroid photograph of each patient was taken by my research assistant, and the patient's name and birth date were written on the back of the photograph. Handwriting samples, using a standard request, were obtained from each patient, and palm prints were taken.
All six clairvoyants were supplied with the photographs, names and birth dates. A numerologist used only the patients' names and birth dates. The graphologist was given the handwriting sample, and the palmist evaluated the palm prints. Each sensitive was asked to fill out the same questionnaire, having had no other contact with the patient. (Seethe Research Data Form at the end of this article.)
Controls consisted of my filling out the same questionnaire to serve as the “correct” answer sheet. In addition, random choices were made by two psychology students who filled out questionnaires. A professor of psychology, with no known psychic ability, did his own “guessing” of the answers, using the patients' photographs.
Unfortunately, I could not be certain of a number of the answers on the personality test, and so the master sheet had to be shortened. We settled on retaining two categories of questions: (1) Where does the patient have difficulty or pain? and (2) What is the major and primary cause of the patient's illness? In answering these questions the sensitives showed significant positive results, as determined by computerized evaluation of the various answer sheets.
We had complete data on some 78 patients and at least one or more clairvoyant diagnoses carried out on almost 200. Two of the clairvoyants were 75% accurate and a third was 70% accurate in locating the site of the pain. (Numerology was 60% accurate, astrology 35%, and palmistry and graphology 25%—the same as chance.) In determining the cause of the pain, the clairvoyants ranged from 65% accuracy down to 30%. Here there was only a 10% probability of obtaining the correct diagnosis by chance.
In a separate study of personality, one outstanding psychic, Dr. Robert Leichtman, an internist and probably one of the most talented clairvoyants in this country today, was 96% accurate in giving very lengthy and elaborate descriptions of the patients' personalities. He used only photographs and the patients' names and birth data to do his psychic tune-in.
These statistics clearly show that clairvoyant diagnosis not only is possible but can be highly successful. The real question is where it fits into the scheme of healing and medicine today.
Although physicians are at least 80% accurate in their primary diagnostic attempts, we are frustrated in determining the exact diagnoses for a variety of illnesses. Furthermore, many of the diagnostic tests carry a significant risk of damage to the patient. In instances such as these, it seems most obvious that the opinion of two or three talented clairvoyants could help us avoid risky diagnostic tests and help both physician and patient rest more comfortably in the knowledge that everything reasonable has been done to make the proper diagnosis.
Although not a formal part of this paper, it seems necessary that I also mention some experiences I have had with healers. I have visited, talked with, and had readings by approximately 60 clairvoyants in the past several years. I consider half a dozen of these to be outstanding individuals; most of them do healing through the laying on of hands. I have seen two patients with breast cancer apparently be cured or have “spontaneous remissions” following the laying on of hands by Dr. Olga Worrall of Baltimore. I know of other cases in which healing seems to have occurred. Again, these cases need more careful scientific study. In addition, we need to do a study in which 100 patients with a known physical illness, such as cancer, are treated by a given healer, to see exactly what percentage of such patients are helped in this way. On the other hand, when medicine fails to cure a patient and we have nothing else to offer, it seems quite reasonable that healers may be used to benefit patients for whom no alternative therapy is possible.
Author's note:
One of the most difficult problems facing physicians is the collection of data concerning the results of treatment. What criteria satisfy scientific requirements for success of any treatment? The big question is that of psychosomatic influence. I should be most interested in soliciting physician reports concerning:
1. “spontaneous” cures in diseases otherwise thought incurable;
2. documented cases where such cures seem to be the result of faith or spiritual healing.
I am particularly interested in cancer cases where tissue diagnosis is available and the physician is willing to certify the “cure” beyond any reasonable doubt. Obviously, physicians' names will be confidential.
C. Norman Shealy, M.D., Fellow, American College of Surgeons, received his medical degree from Duke University in 1956. He is Clinical Associate, Department of Psychology, University of Wisconsin, and Associate Clinical Professor, Universities of Wisconsin and Minnesota. As Director of the Pain Rehabilitation Center at LaCrosse, Wisconsin, he has had broad experience in alternative, therapeutic modalities.
Research Data Form
Sex: Male ____ Female ____
Personality Inventory
Is the patient:
1. Depressed—Avg. (50-60)();
Slight (60-70) ();
Marked (70-80) ();
Severe (80 +) ().
2. Hostile—Avg. (50-60) ();
Slight (60-70) ();
Marked (70-80) ();
Severe (80 + ().
3. Hypochondriacal—Avg. (50-60) ();
Slight (60-70) ();
Marked (70-80) ();
Severe (80 +) ().
4. Hysterical—Avg. (50-60) ();
Slight (60·70) ();
Marked (70-80) ();
Severe (80 + ().
PSYCHIC DIAGNOSIS
5. Sexual adjustment-Poor (); Good (); Avg. ().
6. Hetero drive—Avg. (); Decreased (); Increased ().
Homo drive—Avg. (); Decreased (); Increased ().
Adjustment: Poor (); Fair (); Good ().
7. Hetero interest: Avg. (); Decreased (); Increased ().
Homo interest: Avg. (); Decreased (); Increased ().
Adjustment: Poor (); Fair (); Good ().
8. Is the patient: Passive (); Aggressive (); Balanced (). (60 and up good).
9. Paranoia—Mild (); Moderate (); Extreme ().
10. Conflicts with:
a. father—yes (); no ()
b. mother—yes (); no ()
c. siblings—yes (); no ()
d. offspring—yes (); no ()
e. authorities (teachers, civil, physicians)—yes (); no ()
f. spouse—yes (); no ()
g. lover—yes (); no ()
h. everybody—yes (); no ().
11. Is the patient mentally:
a. clear—yes (); no ()
b. confused—yes (); no ()
1. from physical problems—yes (); no ()
2. from emotional instability—yes (); no ()
3. from drugs—yes (); no ().
12. Is the patient's pain perpetuated by some emotional conflicts? yes(); no()
13. Does the patient really desire pain relief? yes (); no ()
14. If freed of pain, will the patient return to normal activity? 25% (); 50% (); 75% (); 100% ()
15. Is the patient likely to have a “nervous breakdown"? yes (); no()
16. Does the patient contemplate suicide? Yes (); no ()
17. Is he likely to try to commit suicide? yes (); no ()
18. Extent of drug dependency—mild (); strong (); addicted ().
19. Does the patient have insight into his illness? Yes (); no()
Physical Inventory
Pain Problems
1. Location of pain. Circle the description or shade the numbered area(s):
a. trigeminal nerve
b. occipital nerve
c. neck
d. bilateral upper extremities
e. right upper extremity
f. left upper extremity
g. bilateral anterior thorax
h. bilateral posterior thorax
i. right hemithorax
j. left hemithorax
k. bilateral lower back
l. right lower back
m. left lower back
n. bilateral abdomen
o. right abdomen
p. left abdomen
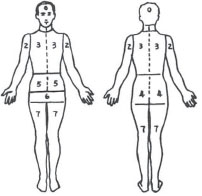
q. pelvis
left
right
r. perineal
genitalia
rectum
s. bilateral lower extremities
t. right lower extremity
u. left lower extremity
v. viscera (specify) _
w. other (specify)_
Comments:
Cause of Pain
1. Cancer
2. Amputation
3. Arthritis
4. Scar
5. Trauma
6. Infection
7. Birth
8. Multiple sclerosis
9. Other degenerative diseases
10. Stroke
11. Spine problems
a. neck
b. chest
c. lumbar
12. Spinal cord difficulty
a. congenital
b. infectious
c. traumatic
d. degenerative
e. tumor
f. vascular
13. Shingles
14. Compensation injury
Other Physical Problems
Remote Current
1. Eyes
2. Ears
3. Nose
4. Mouth-throat
5. Arms
6. Chest or trunk
Remote Current
7. Abdomen
8. Pelvic
a. bladder
b. prostate
c. uterus
d. rectum
9. Legs
10. Brain
11. Hands
12. Feet
13. Blood pressure
14. Heart
15. Lungs
16. Liver
17. Kidney
18. Stomach
19. Intestine
a. small
b. large
20. Gall bladder
21. Bone
22. Muscle-tendon
23. Nerve
24. Skin
25. Genitalia
26. Thyroid
27. Adrenals
28. Appendix
29. Spleen
30. Hair
31. Blood chemistries
32. Endocrine
33. Pancreas
Intensity of Pain
Most of time Occasional Intermittent Time of Pain
1. Severe
2. Moderate
3. Slight
4. None
Recent Physical Activity
1. Unrestricted
2. Slightly restricted
3. Moderately restricted
4. Inactive
Patient's Job
1. Housewife
2. Farmer
3. Laborer
4. Executive
5. Physician, nurse, medical field
6. Secretary
7. Teacher
8. Lawyer
9. Civil worker or military
10. Retired
11. Clerk
12. Recreation
13. Entertainment
14. Religious
15. Other
Recommended Treatment (1 or more)
1. Operant conditioning
2. Psychiatric
3. Psychic
4. Electrical stimulation across skin
5. Electrical stimulation of peripheral nerve
6. Electrical stimulation of dorsal columns
7. Electrical stimulation of brain
8. Facet rhizotomy
9. Cordotomy
10. Cingulumotomy
11. Disc surgery, laminectomy
12. Removal of tumor
13. Nerve destruction
14. Drugs (specify)
15. Magnetic
16. Diet (specify)
17. Vitamins
18. Massage
19. Herbs (specify)
20. X-ray
21. Autogenic training and/or biofeedback
Prognosis
1. For pain relief
a. good
b. fair
c. poor
d. uncertain
e. timing
2. For physical activity
a. good
b. fair
c. poor
d. uncertain
3. timing
3. For drug withdrawal
a. good
b. fair
c. poor
d. uncertain
e. timing
4. For life expectancy next 5 years
a. good
b. fair
c. poor
d. uncertain
e. timing
5. General health
a. good
b. fair
c. poor
d. uncertain
e. timing
6. Emotional stability
a. good
b. fair
c. poor
d. uncertain
e. timing
1. Physician's Name:_______________________________________
2. Astrological and Numerological:____________________________
3. Palmistry:______________________________________________
4. Handwriting:____________________________________________
5. Psychic:________________________________________________
6. Rev. Jack Schwarz:_______________________________________