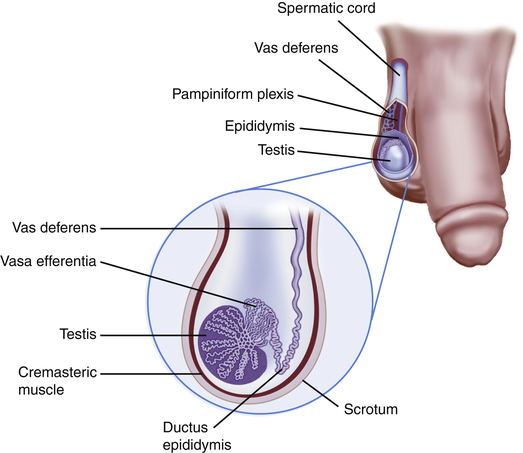
Male Genitalia
Examination
Have patient lying or standing to start examination.
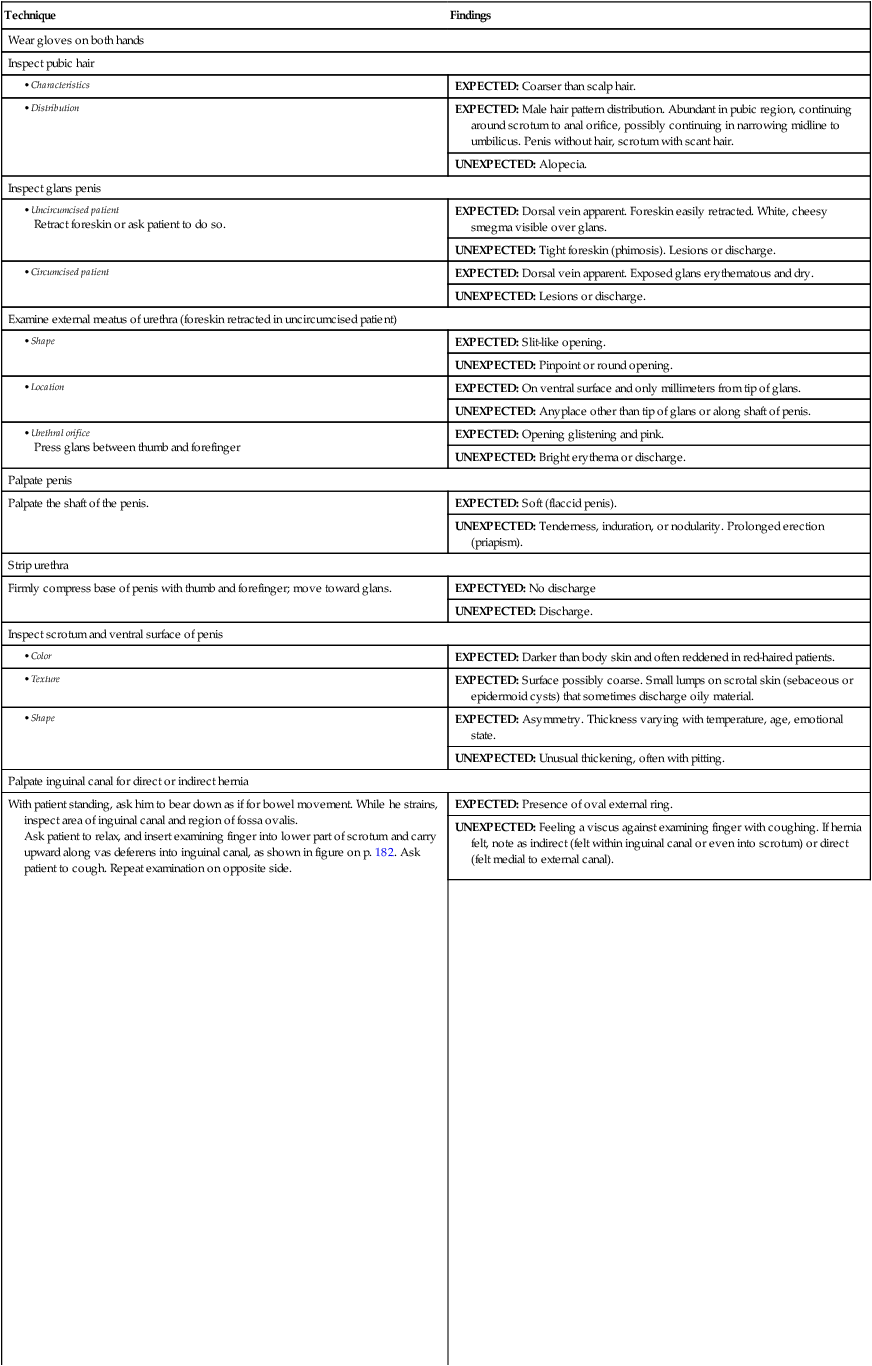
| Technique | Findings |
| Wear gloves on both hands | |
| Inspect pubic hair | |
| EXPECTED: Coarser than scalp hair. | |
| EXPECTED: Male hair pattern distribution. Abundant in pubic region, continuing around scrotum to anal orifice, possibly continuing in narrowing midline to umbilicus. Penis without hair, scrotum with scant hair. | |
| UNEXPECTED: Alopecia. | |
| Inspect glans penis | |
| EXPECTED: Dorsal vein apparent. Foreskin easily retracted. White, cheesy smegma visible over glans. | |
| UNEXPECTED: Tight foreskin (phimosis). Lesions or discharge. | |
| EXPECTED: Dorsal vein apparent. Exposed glans erythematous and dry. | |
| UNEXPECTED: Lesions or discharge. | |
| Examine external meatus of urethra (foreskin retracted in uncircumcised patient) | |
| EXPECTED: Slit-like opening. | |
| UNEXPECTED: Pinpoint or round opening. | |
| EXPECTED: On ventral surface and only millimeters from tip of glans. | |
| UNEXPECTED: Anyplace other than tip of glans or along shaft of penis. | |
| EXPECTED: Opening glistening and pink. | |
| UNEXPECTED: Bright erythema or discharge. | |
| Palpate penis | |
| Palpate the shaft of the penis. | EXPECTED: Soft (flaccid penis). |
| UNEXPECTED: Tenderness, induration, or nodularity. Prolonged erection (priapism). | |
| Strip urethra | |
| Firmly compress base of penis with thumb and forefinger; move toward glans. | EXPECTYED: No discharge |
| UNEXPECTED: Discharge. | |
| Inspect scrotum and ventral surface of penis | |
| EXPECTED: Darker than body skin and often reddened in red-haired patients. | |
| EXPECTED: Surface possibly coarse. Small lumps on scrotal skin (sebaceous or epidermoid cysts) that sometimes discharge oily material. | |
| EXPECTED: Asymmetry. Thickness varying with temperature, age, emotional state. | |
| UNEXPECTED: Unusual thickening, often with pitting. | |
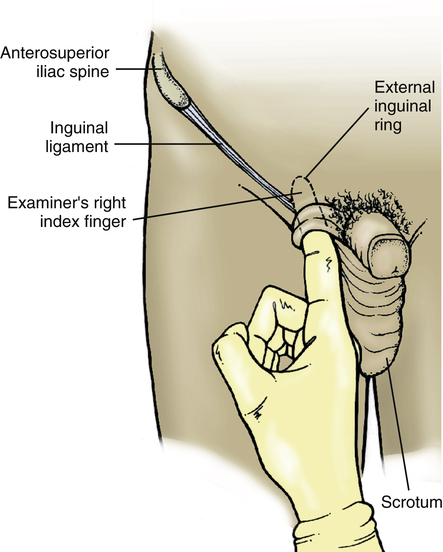
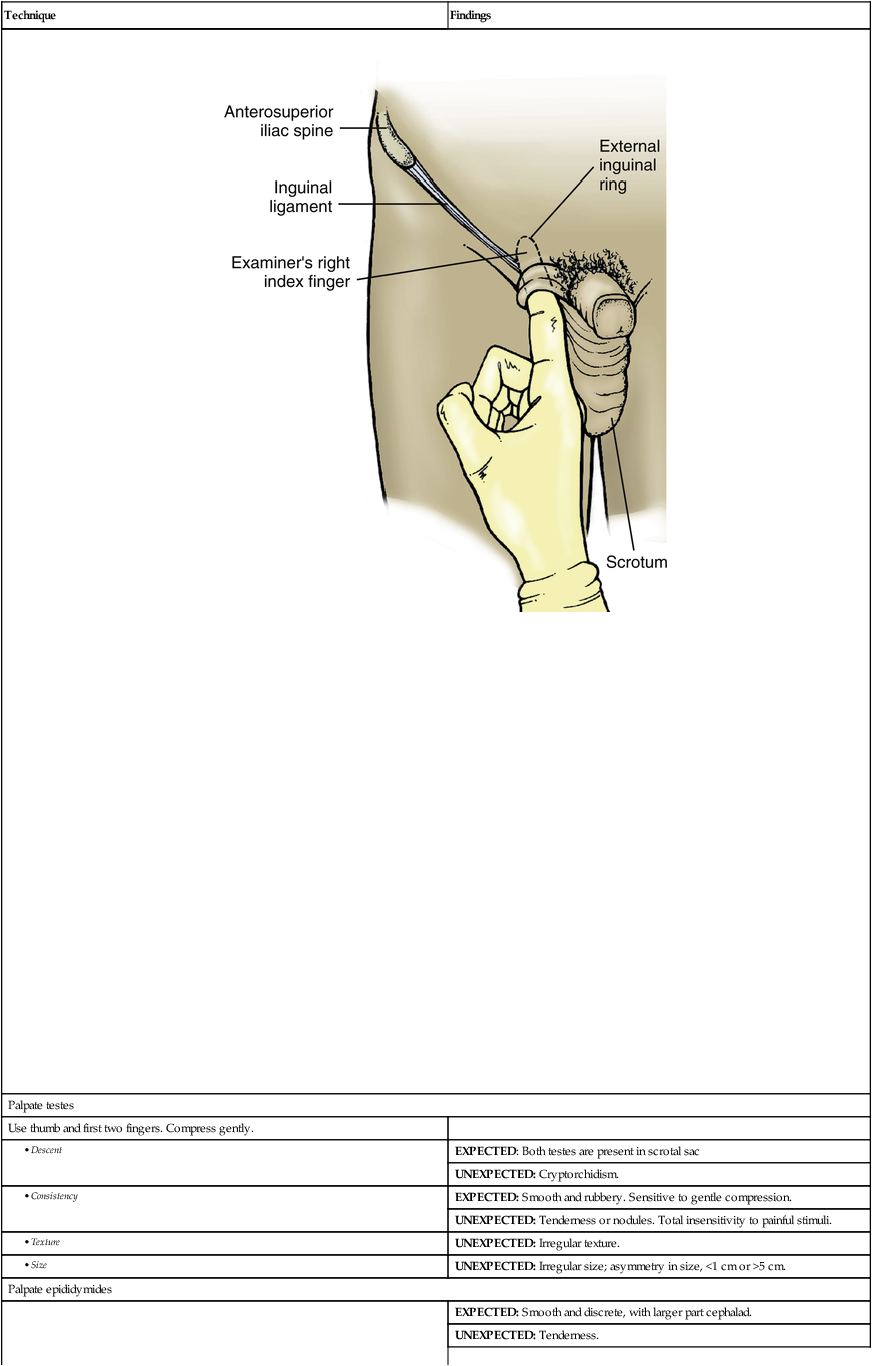
| Palpate inguinal canal for direct or indirect hernia | |
| With patient standing, ask him to bear down as if for bowel movement. While he strains, inspect area of inguinal canal and region of fossa ovalis. Ask patient to relax, and insert examining finger into lower part of scrotum and carry upward along vas deferens into inguinal canal, as shown in figure on p. 182. Ask patient to cough. Repeat examination on opposite side. |
EXPECTED: Presence of oval external ring. |
| UNEXPECTED: Feeling a viscus against examining finger with coughing. If hernia felt, note as indirect (felt within inguinal canal or even into scrotum) or direct (felt medial to external canal). | |
 |
|
| Palpate testes | |
| Use thumb and first two fingers. Compress gently. | |
| EXPECTED: Both testes are present in scrotal sac | |
| UNEXPECTED: Cryptorchidism. | |
| EXPECTED: Smooth and rubbery. Sensitive to gentle compression. | |
| UNEXPECTED: Tenderness or nodules. Total insensitivity to painful stimuli. | |
| UNEXPECTED: Irregular texture. | |
| UNEXPECTED: Irregular size; asymmetry in size, <1 cm or >5 cm. | |
| Palpate epididymides | |
| EXPECTED: Smooth and discrete, with larger part cephalad. | |
| UNEXPECTED: Tenderness. | |
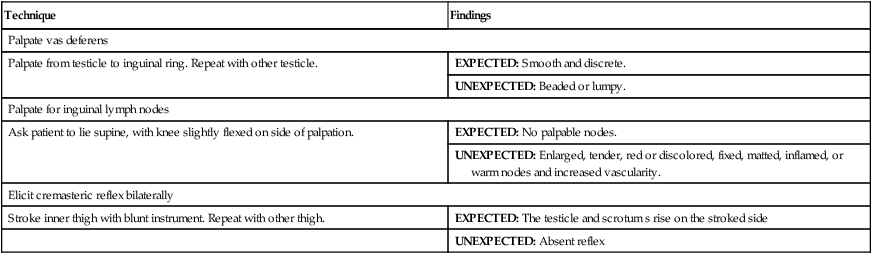
| Palpate vas deferens | |
| Palpate from testicle to inguinal ring. Repeat with other testicle. | EXPECTED: Smooth and discrete. |
| UNEXPECTED: Beaded or lumpy. | |
| Palpate for inguinal lymph nodes | |
| Ask patient to lie supine, with knee slightly flexed on side of palpation. | EXPECTED: No palpable nodes. |
| UNEXPECTED: Enlarged, tender, red or discolored, fixed, matted, inflamed, or warm nodes and increased vascularity. | |
| Elicit cremasteric reflex bilaterally | |
| Stroke inner thigh with blunt instrument. Repeat with other thigh. | EXPECTED: The testicle and scrotum s rise on the stroked side |
| UNEXPECTED: Absent reflex | |
AIDS TO DIFFERENTIAL DIAGNOSIS
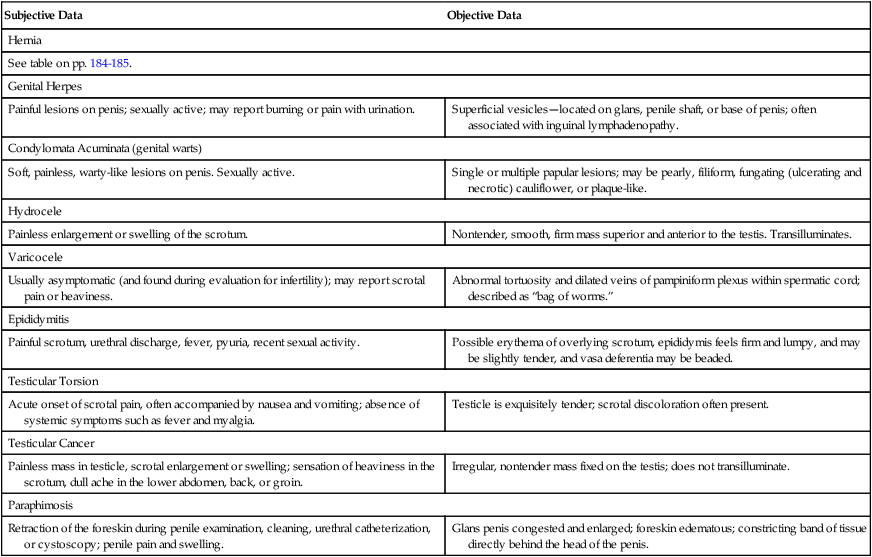
| Subjective Data | Objective Data |
| Hernia | |
| See table on pp. 184-185. | |
| Genital Herpes | |
| Painful lesions on penis; sexually active; may report burning or pain with urination. | Superficial vesicles—located on glans, penile shaft, or base of penis; often associated with inguinal lymphadenopathy. |
| Condylomata Acuminata (genital warts) | |
| Soft, painless, warty-like lesions on penis. Sexually active. | Single or multiple papular lesions; may be pearly, filiform, fungating (ulcerating and necrotic) cauliflower, or plaque-like. |
| Hydrocele | |
| Painless enlargement or swelling of the scrotum. | Nontender, smooth, firm mass superior and anterior to the testis. Transilluminates. |
| Varicocele | |
| Usually asymptomatic (and found during evaluation for infertility); may report scrotal pain or heaviness. | Abnormal tortuosity and dilated veins of pampiniform plexus within spermatic cord; described as “bag of worms.” |
| Epididymitis | |
| Painful scrotum, urethral discharge, fever, pyuria, recent sexual activity. | Possible erythema of overlying scrotum, epididymis feels firm and lumpy, and may be slightly tender, and vasa deferentia may be beaded. |
| Testicular Torsion | |
| Acute onset of scrotal pain, often accompanied by nausea and vomiting; absence of systemic symptoms such as fever and myalgia. | Testicle is exquisitely tender; scrotal discoloration often present. |
| Testicular Cancer | |
| Painless mass in testicle, scrotal enlargement or swelling; sensation of heaviness in the scrotum, dull ache in the lower abdomen, back, or groin. | Irregular, nontender mass fixed on the testis; does not transilluminate. |
| Paraphimosis | |
| Retraction of the foreskin during penile examination, cleaning, urethral catheterization, or cystoscopy; penile pain and swelling. | Glans penis congested and enlarged; foreskin edematous; constricting band of tissue directly behind the head of the penis. |
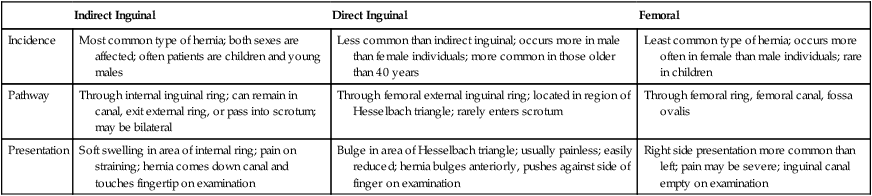
Distinguishing Characteristics of Hernias
| Indirect Inguinal | Direct Inguinal | Femoral | |
| Incidence | Most common type of hernia; both sexes are affected; often patients are children and young males | Less common than indirect inguinal; occurs more in male than female individuals; more common in those older than 40 years | Least common type of hernia; occurs more often in female than male individuals; rare in children |
| Pathway | Through internal inguinal ring; can remain in canal, exit external ring, or pass into scrotum; may be bilateral | Through femoral external inguinal ring; located in region of Hesselbach triangle; rarely enters scrotum | Through femoral ring, femoral canal, fossa ovalis |
| Presentation | Soft swelling in area of internal ring; pain on straining; hernia comes down canal and touches fingertip on examination | Bulge in area of Hesselbach triangle; usually painless; easily reduced; hernia bulges anteriorly, pushes against side of finger on examination | Right side presentation more common than left; pain may be severe; inguinal canal empty on examination |
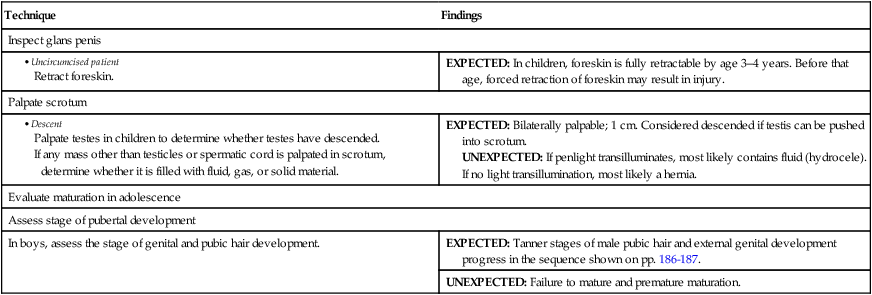
PEDIATRIC VARIATIONS
EXAMINATION
| Technique | Findings |
| Inspect glans penis | |
| EXPECTED: In children, foreskin is fully retractable by age 3–4 years. Before that age, forced retraction of foreskin may result in injury. | |
| Palpate scrotum | |
| EXPECTED: Bilaterally palpable; 1 cm. Considered descended if testis can be pushed into scrotum. UNEXPECTED: If penlight transilluminates, most likely contains fluid (hydrocele). If no light transillumination, most likely a hernia. |
|
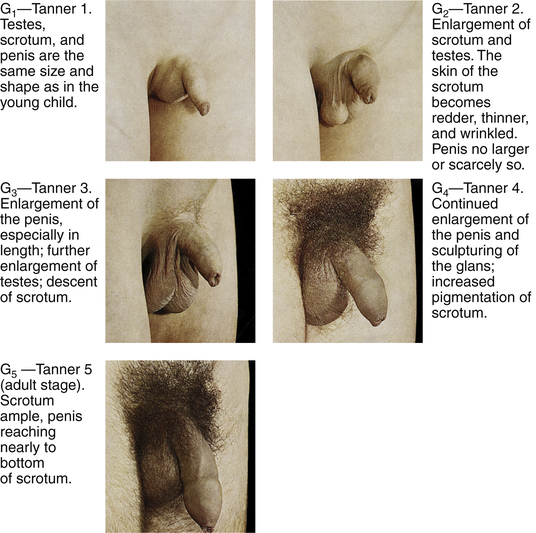
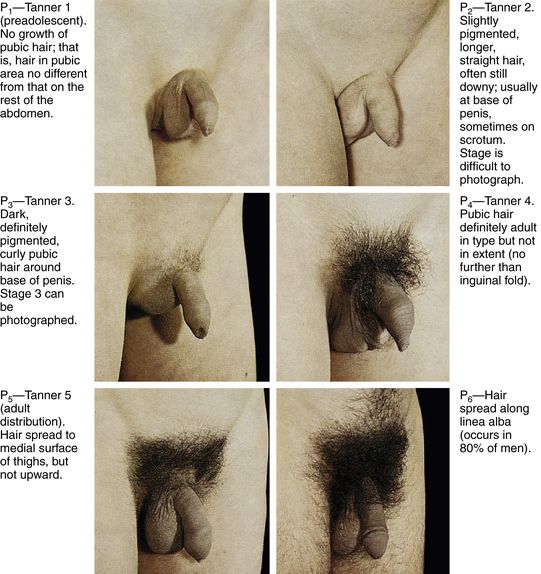
| Evaluate maturation in adolescence | |
| Assess stage of pubertal development | |
| In boys, assess the stage of genital and pubic hair development. | EXPECTED: Tanner stages of male pubic hair and external genital development progress in the sequence shown on pp. 186-187. |
| UNEXPECTED: Failure to mature and premature maturation. | |
Sample Documentation
Subjective
Thirty-seven-year-old man reports painful burning lesions on his penis. Present past few days. Is sexually active. No burning on urination.
Objective
Hair in male pattern distribution. Circumcised glans without lesions or discharge. Urethral meatus patent on ventral surface at tip of glans. No urethral discharges. Penile shaft with vesicles present. Testes descended bilaterally; smooth without nodularity. Scrotal contents smooth without tenderness. Inguinal areas without bulges or hernias. Inguinal nodes palpable bilaterally. Cremasteric reflex elicited.