CAGE Questionnaire: A Framework for Detecting Alcoholism
The CAGE questionnaire was developed in 1984 by Dr. John Ewing, and it includes four interview questions designed to help diagnose alcoholism. The acronym “CAGE” helps practitioners quickly recall the main concepts of the four questions (Cutting down, Annoyance by criticism, Guilty feeling, Eye-openers).
Probing questions may be asked as follow-up questions to the CAGE questionnaire.
Many online resources list the complete questionnaire (e.g., http://addictionsandrecovery.org/addiction-self-test.htm). The exact wording of the CAGE Questionnaire can be found in: Ewing JA: Screening for Alcoholism using CAGE: cut down, annoyed, guilty, eye opener, JAMA 280(2): 1904-1905, 1984.
|
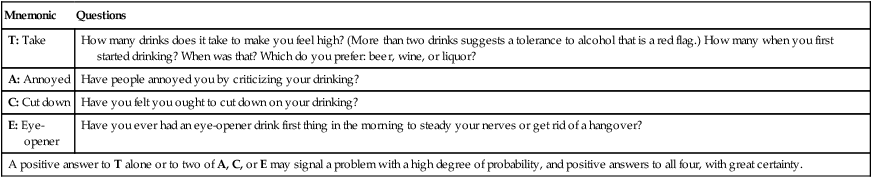
TACE Questionnaire: A Framework for Prenatal Detection of Risk Drinking
| Mnemonic |
Questions |
| T: Take |
How many drinks does it take to make you feel high? (More than two drinks suggests a tolerance to alcohol that is a red flag.) How many when you first started drinking? When was that? Which do you prefer: beer, wine, or liquor? |
| A: Annoyed |
Have people annoyed you by criticizing your drinking? |
| C: Cut down |
Have you felt you ought to cut down on your drinking? |
| E: Eye-opener |
Have you ever had an eye-opener drink first thing in the morning to steady your nerves or get rid of a hangover? |
| A positive answer to T alone or to two of A, C, or E may signal a problem with a high degree of probability, and positive answers to all four, with great certainty. |
From Sokol et al, 1989.
The CRAFFT Questionnaire: A Framework for Detecting Recreational Substance Use Disorders in Adolescents
The CRAFFT questionnaire was developed in 2002 as a screening tool for alcohol and substance abuse in adolescents. The CRAFFT acronym helps practitioners remember the main concepts of the six questions: Car, Relax, Alone, Forget, Friends, Trouble.
The exact wording of the CRAFFT questions can be found here: Knight JR et al., Validity of the CRAFFT Substance Abuse Screening Test Among Adolescent Clinic Patients. Arch Pediatr Adolesc Med 156:607-614, 2002 (available online at http://archpedi.jamanetwork.com/article.aspx?articleid=203511).
|
Domestic Violence: Three Questions as a Brief Screening Instrument
1. Have you been hit, kicked, punched, or otherwise hurt by someone within the past year?
2. Do you feel safe in your current relationship?
3. Is a partner from a previous relationship making you feel unsafe now?
|
| A positive response to any one of the three questions constitutes a positive screen for partner violence. |
| The first question, which addresses physical violence, has been validated in studies as an accurate measure of 1-year prevalence rates. |
| The last two questions evaluate the perception of safety and estimate the short-term risk of further violence and the need for counseling, but reliability and validity evaluations have not yet been established. |
From Feldhaus et al, 1997.
Brief Screening Tool for Domestic Violence: HITS
Verbal abuse is as intense a problem as physical violence. HITS stands for Hurt, Insult, Threaten, or Scream. The wording of the question is, “In the last year, how often did your partner:
Hurt you physically?”
Insult or talk down to you?”
Threaten you with physical harm?”
Scream or curse at you?”
From Sherin et al, 1998.
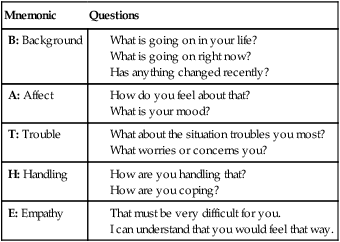
BATHE Questionnaire: A Framework for Understanding the Patient in the Context of His or Her Total Life Situation
| Mnemonic |
Questions |
| B: Background |
What is going on in your life?
What is going on right now?
Has anything changed recently?
|
| A: Affect |
How do you feel about that?
What is your mood?
|
| T: Trouble |
What about the situation troubles you most?
What worries or concerns you?
|
| H: Handling |
How are you handling that?
How are you coping?
|
| E: Empathy |
That must be very difficult for you.
I can understand that you would feel that way.
|
From Stuart and Lieberman, 1993; Lieberman, 1997.
HOPE Questionnaire: A Framework for Spiritual Assessment
| Mnemonic |
Questions |
| H: Hope—sources of hope, meaning, comfort, strength, peace, love, and connection |
We have been discussing your support systems. I was wondering, what is there in your life that gives you internal support?
What are your sources of hope, strength, comfort, and peace?
What do you hold on to during difficult times?
What sustains you and keeps you going?
For some people, their religious or spiritual beliefs act as a source of comfort and strength in dealing with life’s ups and downs; is this true for you?
If the answer is yes, go on to O and P questions. If the answer is no, consider asking, “Was it ever?” If the answer is yes, ask, “What changed?”
|
| O: Organized religion |
Do you consider yourself part of an organized religion? How important is this to you?
What aspects of your religion are helpful and not so helpful to you?
Are you part of a religious or spiritual community? Does it help you? How?
|
| P: Personal spirituality/practices |
Do you have personal spiritual beliefs that are independent of organized religion?
What are they?
Do you believe in God? What kind of relationship do you have with God?
What aspects of your spirituality or spiritual practices do you find most helpful to you personally? (Examples include prayer, meditation, reading scripture, attending religious services, listening to music, hiking, communing with nature.)
|
| E: Effects on medical care and end-of-life issues |
Has being sick (or your current situation) affected your ability to do the things that usually help you spiritually (or affected your relationship with God)?
As a doctor, is there anything that I can do to help you access the resources that usually help you?
Are you worried about any conflicts between your beliefs and your medical situation/care/decisions?
Would it be helpful for you to speak to a clinical chaplain/community spiritual leader?
Are there any specific practices or restrictions I should know about in providing your medical care (e.g., dietary restrictions, use of blood products)?
If the patient is dying: How do your beliefs affect the kind of medical care you would like me to provide over the next few days/weeks/months?
|
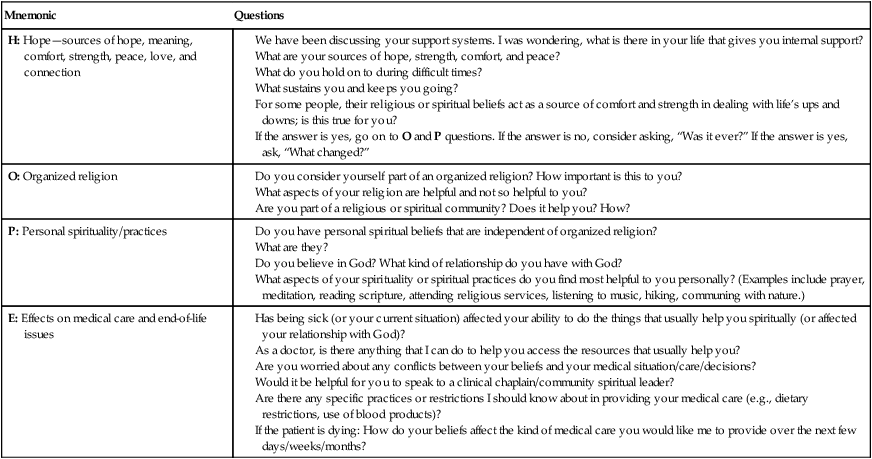
From Anandarajah and Hight, 2001.
SPIRIT Questionnaire: A Framework for Spiritual Assessment
| Mnemonic |
Questions |
| S: Spiritual belief system |
What is your formal religious affiliation?
Name or describe your spiritual belief system.
|
| P: Personal spirituality |
Describe the beliefs and practices of your religion or spiritual system that you personally accept.
Describe the beliefs or practices you do not accept.
Do you accept or believe (specific tenet or practice)?
What does your spirituality/religion mean to you?
What is the importance of your spirituality/religion in daily life?
|
| I: Integration with a spiritual community |
Do you belong to any spiritual or religious group or community? What is your position or role?
What importance does this group have to you? Is it a source of support? In what ways?
Does or could this group provide help in dealing with health issues?
|
| R: Ritualized practices and restrictions |
Are there specific practices that you carry out as part of your religion/spirituality (e.g., prayer or meditation)?
Are there certain lifestyle activities or practices that your religion/spirituality encourages or forbids? Do you comply?
What significance do these practices and restrictions have to you?
Are there specific elements of medical care that you forbid on the basis of religious/spiritual grounds?
|
| I: Implications for medical care |
What aspects of your religion/spirituality would you like me to keep in mind as I care for you?
Would you like to discuss religious or spiritual implications of health care?
What knowledge or understanding would strengthen our relationship as physician and patient?
Are there any barriers to our relationship based on religious or spiritual issues?
|
| T: Terminal events planning |
As we plan for your care near the end of life, how does your faith affect your decisions?
Are there particular aspects of care that you wish to forgo or have withheld because of your faith?
|
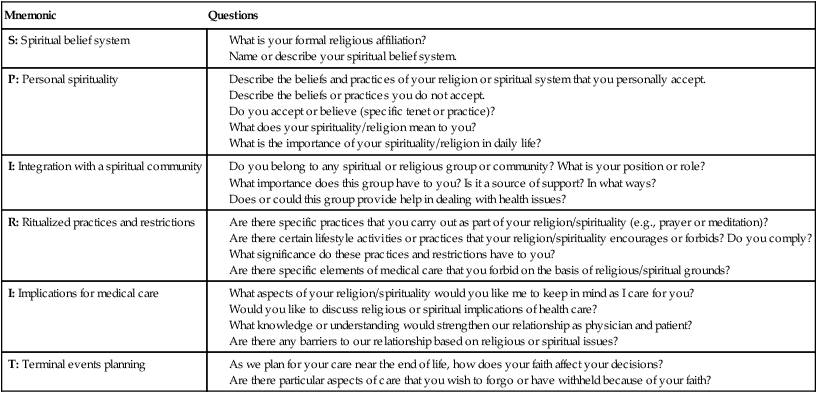
From Maugans, 1996.
ETHNIC Questionnaire: A Framework for Culturally Competent Clinical Practice
| Mnemonic |
Questions |
| E: Explanation |
Why do you think you have these symptoms? What do friends, family, and others say? Do you know others with this problem? Have you seen it on TV, heard about it on the radio, or read about it in the newspaper? |
| T: Treatment |
Do you take any treatments, medicines, or home remedies to treat the illness or to stay healthy? What kinds of treatment are you seeking from me? |
| H: Healers |
Have you sought advice from friends, alternative folk healers, or other nondoctors? |
| N: Negotiate |
Negotiate mutually acceptable options; incorporate patient’s beliefs. Ask results patient hopes to achieve from intervention. |
| I: Intervention |
Determine an intervention with your patient. May include incorporation of alternative treatments, spirituality, healers, or other cultural practices (e.g., foods to be eaten or avoided). |
| C: Collaborate |
Collaborate with the patient, family, health team members, healers, and community resources. |
Modified from Levin et al, 1997.
The HEEADSSS Psychosocial Interview for Adolescents (Essential Questions)
| Mnemonic |
Questions |
| H: Home |
Who lives with you? Where do you live? Do you have your own room?
What are relationships like at home?
To whom are you closest at home?
To whom can you talk at home?
Is there anyone new at home? Has someone left recently?
Have you moved recently?
Have you ever had to live away from home? (Why?)
|
| E: Education and employment |
What are your favorite subjects at school?
Your least favorite subjects?
How are your grades? Any recent changes?
Any dramatic changes in the past?
Have you changed schools in the past few years?
What are your future education/employment plans/goals?
Are you working? Where? How much?
|
| E: Eating |
What do you like and not like about your body?
Have there been any recent changes in your weight?
Have you dieted in the last year? How? How often?
Have you done anything else to try to manage your weight?
How much exercise do you get in an average day? Week?
What do you think would be a healthy diet?
How does that compare to your current eating patterns?
|
| A: Activities |
What do you and your friends do for fun? (With whom, where, and when?)
What do you and your family do for fun? (With whom, where, and when?)
Do you participate in any sports or other activities?
Do you regularly attend a church group, club, or other organized activity?
|
| D: Drugs |
Do you and your friends use tobacco? Alcohol? Other drugs?
Does anyone in your family use tobacco? Alcohol? Other drugs?
Do you use tobacco? Alcohol? Other drugs?
Is there any history of alcohol or drug problems in your family? Does anyone at home use tobacco?
|
| S: Sexuality |
Have you ever been in a romantic relationship?
Tell me about the people that you’ve dated. OR Tell me about your sex life.
Have any of your relationships ever been sexual relationships?
Are your sexual activities enjoyable?
What does the term “safer sex” mean to you?
|
| S: Suicide and depression |
Do you feel sad or down more than usual?
Do you feel yourself crying more than usual?
Are you “bored” all the time?
Are you having trouble getting to sleep?
Have you thought a lot about hurting yourself or someone else?
|
| S: Safety (savagery) |
Have you ever been seriously injured? (How?) How about anyone else you know?
Do you always wear a seatbelt in the car?
Have you ever ridden with a driver who was drunk or high? When? How often?
Do you use safety equipment for sports and/or other physical activities (e.g., helmets for biking or skateboarding)?
Is there any violence at your school? In your neighborhood? Among your friends?
Have you ever been physically or sexually abused? Have you ever been raped, on a date or at any other time? (if not asked previously)
|
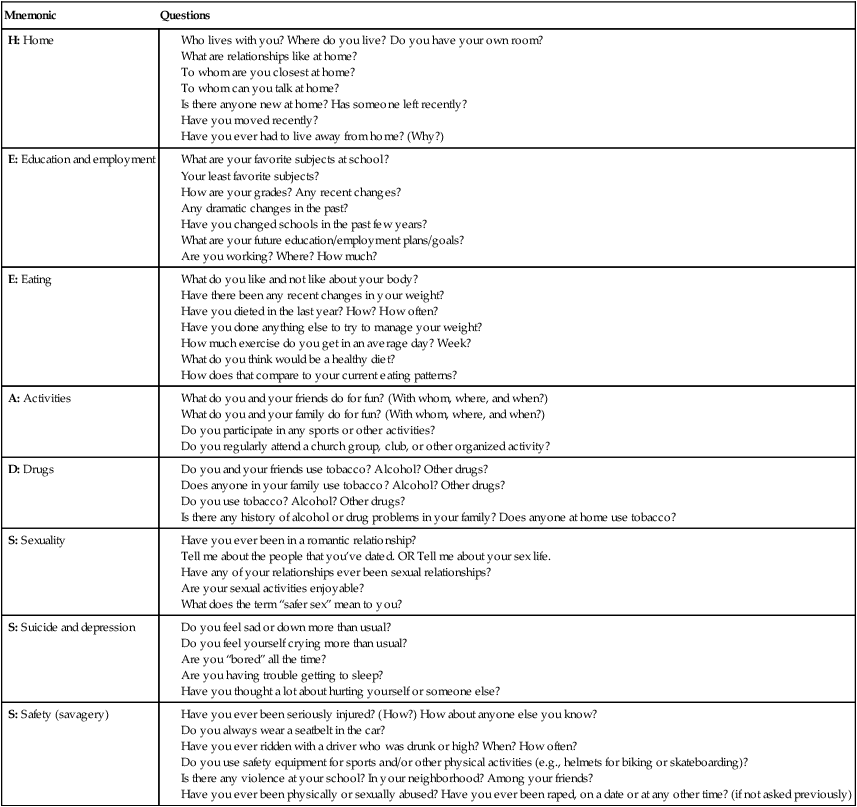
From Goldenring and Rosen, 2004.