4
Psychological Theories of ADHD
In this chapter I shall describe the changes in information processing seen in ADHD such as memory, impulsivity, and executive function. The sheer volume of information about the cognitive changes, and theories that attempt to account for those changes, means that this chapter focuses heavily on neuropsychological accounts of ADHD (see [379–380] for reviews). However, that is not to say that there are not any alternatives: there are Freudian theories [381] and behavioral theories [382], for example.
The data derived from neuropsychological studies have been used to conceptualize ADHD as a disorder that can be explained by cognitive deficits [383]. In particular, behaviors attributed to the frontal lobes are implicated – hence the neuroanatomical connections in the brain are fundamentally important to understanding ADHD. The behaviors that are thought to emanate from the frontal lobes are collectively known as executive functions, and in evolutionary terms the frontal lobes are the most recently developed part of the brain (see chapter 6).
Executive functions are a collection of high-level cognitive processes that control and regulate other lower-level processes; the essence of executive function (EF) is that it is the manager of many workers that together produce a product (behavior). EF deals with inputs from the world around us, organizes the inputs, and selects a response output (behavior/symptom). The exact nature of EF is hard to define. In fact there are many definitions, but as Jurado and Rosselli suggest, the common-ground definition of EF has four components: goal formation, planning, execution of goal-related plans, and effective performance [384]. Thus executive functions are involved in (1) the identification of what we want/need to do/achieve; (2) how we are going to go about achieving the objective; (3) arranging these objectives into a sequence of actions according to the plan; and (4) monitoring performance and correcting mistakes or changing plans when the evidence suggests a plan is faulty.
We are not born with a set of fully formed executive functions; they develop throughout childhood, and can decline in old age. The development of EF in childhood and adolescence is correlated with neural changes in the frontal lobe. These periods of growth occur between birth and 2, then between 7 and 9 years, and finally between 16 and 19 years, with brain complete by approximately 25 years (see [384]). This fact raises the importance of developmentally appropriate control groups when comparing those with ADHD and those who do not have a diagnosis – there is no point in having widely disparate ages in your groups, yet some studies do!
The neural development at the different stages has an impact on behavior and cognition. The nature of these developmental changes is also important. The developmental trajectories of specific behaviors may differ: what behaviors remain in adult cases of ADHD may resemble the core deficit, whereas other cognitive problems are only evident at earlier ages. As the brain changes, some problems abate or at least the impact of them is reduced.
In general, EF has been shown to be compromised in people with ADHD regardless of age or sex and is further exacerbated by comorbidities [385] which may have EF deficits in their own right. The role of EF in ADHD is still subject to a great deal of scrutiny, but it is becoming clear that the problems seen in ADHD are not restricted to EF but also include other lower level cognitive processes, such as word reading and colour naming [386].
The frontal lobes are also associated with a Theory of Mind (ToM) – the phrase given to the ability to have the knowledge that others have thoughts, ideas, beliefs, and opinions separate from our own (see [387]). ToM is a concept that develops through early childhood and is affected in some developmental disorders. Interestingly enough, whilst both autistic children and ADHD children have EF deficits, it is often only autistic children who fail ToM tasks [388–389]. However, a failure of ToM tasks in ADHD only occurred in tasks involving inhibitory control [390]. A further problem in assessing ToM in ADHD is that comorbidities such as ODD and CD have been shown to have to have impairments in their own right [391–392]. What this tells us is that those with ADHD have an understanding about others’ beliefs, wishes, and emotions, but they cannot regulate or inhibit their behavior to account for others. In other words, they are impulsive, and this impulsivity is the symptom that has generated most concern.
One should note that despite the wide use of neuropsychological tests as research tools, they have been of little diagnostic utility. Many tests have been deployed to characterize the neuropsychological profile of ADHD, but this has been done with “little emphasis on conceptual and theoretical analysis of the constructs underlying them” [393] (p. 294). This lack of theoretical base may be, in part, due to the lack of discriminant validity that the neuropsychological tests possess both across different disorders and within the subtypes of ADHD [394]. Furthermore, laboratory-based neuropsychological tasks do not correlate well with rating scales. The rating scales provide a measure of functional impairments outside of the laboratory – where it actually counts [395–397]. Thus the real-life application of neuropsychological tests is not immediately apparent; they only appear to have a modest amount of ecological validity [102–103]. Sugalski et al. deployed a plethora of neuropsychological tests on a child with suspected ADHD. They found variability in these tests, which took a long time to conduct, but concluded
that not even the most comprehensive battery of neuropsychological assessments can replace clinical experience buttressed by parental reports, school records, the clinical interview, direct behavioural observations, and a well-taken medical history. [398] (p. 374)
Specific measures of EF have not been shown to predict impairment of adaptive functioning, and deficits in EF may only be linked with the ADHD-I subtype in adults [399–400]. However, children’s scores on neuropsychological tests correlated with parents’ rating of attentiveness and hyperactivity [395]. Furthermore, not all people with ADHD have deficits in EF [385, 394], and in those who have there is considerable variability with a wide range of scores being possible [401]. Thus the clinical utility of EF measures is minimal. It is important to note that measures of EF were not designed for the complexities of ADHD, but were born out of the necessity to assess patients with frontal lobe damage – a very different goal; after all, we have moved away from the label MBD! Whilst the EF tests are not diagnostic, that is not to say measuring EF is a pointless exercise. The knowledge derived from studying EF in children and adults with ADHD has provided some of the strongest and most thought-provoking theoretical positions.
Using a battery of tests to assess EF in ADHD children, Professor Tim Shallice and colleagues found all the measures able to detect dysfunction compared to normal control children; the ADHD children made more errors and were slower. The exception was for letter fluency, a task in which you have to produce as many words as possible (no countries, names, or towns) that begin with a particular letter (C, S, or P), in which ADHD could not be differentiated [402]. In brain-damaged patients, letter fluency deficits occur if the lesion is in left frontal or medial regions of the brain, and in ADHD the neuroanatomical abnormalities are predominantly on the right side [403].
Adults also show impaired performance across a number of neuropsychological domains such as sustained and focused attention, verbal memory, and visual/verbal fluency (which assesses productivity and creativity) [404]. A meta-analysis of 24 studies did not highlight EF as a particular problem in adults [404]. This result is in contradiction to the many neurocognitive theories of childhood ADHD, but can be explained as the result of brain maturation processes most notably in the frontal lobe.
When first reading the neuropsychological theories, they can appear to be just elaborate descriptions of the fine detail of the behaviors observed in many cases of ADHD. However, neuropsychological theories have much more to offer than pure description; they have become central to our understanding of ADHD. The functional importance of the frontal lobes has been elaborated upon by many and includes the concepts of working memory [405] and the Supervisory Attentional System [406]. When applied to ADHD, such theories can account for some of the cognitive deficits. Whilst the theories can explain symptoms via cognitive processing in ADHD, they do not commit to etiology. The neuropsychological theories provide an understanding of what is going wrong in ADHD, but it does not state why it has gone wrong in the first place.
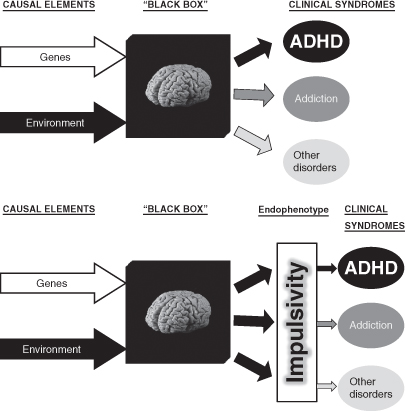
The use of neuropsychological accounts of ADHD has been put forward as a possible endophenotype linking the disorder to genes. The jump between gene and disorder is too great, and the endophenotype is an intermediate level of explanation that may be simpler to evaluate. The concept of an endophenotype in psychiatry “was adapted for filling the gap between available descriptors and between the gene and the elusive disease processes” [407] (p. 637). Thus between the genes that are most likely to cause ADHD (e.g. DRD4) and the disorder is a theoretical account of ADHD (e.g. behavioral inhibition/impulsivity) linking the physical (gene/brain) to the behavioral. The endophenotype is therefore a link between the genotype and the ADHD phenotype (Figure 4.1). The endophenotype may well be closer to a genetic basis rather than the disorder itself, or at least closer to the genes in a pathway to the disorder [408].
Figure 4.1 The endophenotype: in this case impulsivity bridges the gap between biological mechanisms and clinical symptoms. Upper panel: genes and the environment interact to bring about neural changes that underlie ADHD. Lower panel: the endophenotype allows for the neurobiology of impulsivity as a symptom to be evaluated
A set of criteria have been proposed for the identification of endophenotypes [407]. The endophenotype is passed on to offspring who may or may not have ADHD, but there is a higher incidence of the endophenotype in families with ADHD. Clearly, using this approach sees ADHD symptoms at the end of a continuum of normality rather than as a discrete and readily differentiated disorder; you can possess the endophenotype but also be asymptomatic. Furthermore, the endophenotype should have sound psychometric properties of reliability and validity, and this would be best served by a quantifiable measure [408], such as has been suggested for impulsivity and behavioral inhibition.
Impulsivity and Behavioral/Response Inhibition
Of all the neuropsychological deficits that can be seen in ADHD, behavioral inhibition (BI) (or response inhibition) stands out. BI is a neuropsychological concept that is considered as central to the symptoms of ADHD. BI can be defined as the ability to stop a particular response when signaled to do so. BI is akin to self-control and is the process that stops us responding to stimuli; BI is not case of free-will, but a case of free-won’t! A deficit in BI has been described as the bedrock of the impulsivity seen in ADHD.
Clinically the individual may be seen to be engaging in impulsive behavior. The child may appear to be extremely reactive and stimulus-driven without giving due care to the effects of their behavior on others. Impulsivity is one part of the three core symptoms in the diagnostic manuals. Despite a near consensus in the neuropsychological literature that there is a BI deficit in those with ADHD, there is still a debate regarding the extent to which BI is affected, and furthermore what type of BI is affected.
Several accounts of BI have been offered and applied to ADHD.
Barkley’s neuropsychological account – behavioral inhibition
Despite the myriad of cognitive deficits that appear to plague those with ADHD, early studies have demonstrated that children with ADHD (and more recently adults) have problems with BI [409–410]. Such is the importance of BI in ADHD research that it has recently been considered as a suitable endophenotype for studying the genetic basis of ADHD [408]. Leading the study of BI is Professor Russell Barkley. Barkley has been extremely influential in conceptualizing ADHD as a disorder arising from a failure of the BI system [48, 411–412]. The clinical manifestation of a BI deficit is most obvious in impulsivity; however, the effects of BI are thought to extend beyond just this symptom.
Barkley’s theory is one of EF in general, but with a clear application to ADHD. Barkley sees a failure to inhibit responses to be the cause of all the other EF deficits seen in ADHD. In fact Barkley sees deficits in BI as so well established in the ADHD population that it should be treated as a “fact” [413]. Fact is not a word that is used in the behavioral sciences very often. However, whilst the use of the term fact highlights the importance placed upon BI and the data supporting a deficit, BI should not be considered without question.
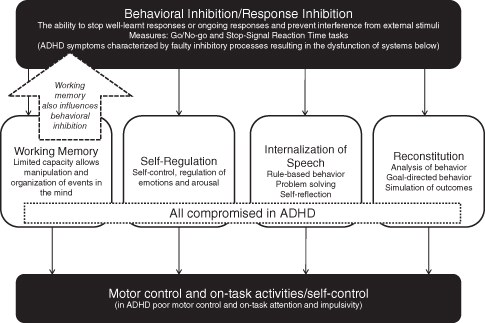
The necessity of BI in behavior is argued to manifest itself in four EF domains: (1) nonverbal working memory; (2) internalization of speech (verbal working memory); (3) self-regulation of affect/motivation/arousal; and (4) reconstitution (planning) [414]. Thus Barkley see BI as at the top of an EF hierarchy. BI consists of three main components: (1) inhibiting the initial prepotent or immediate/dominant response as determined by reinforcement history (to stop a response that has become already likely because of previous experience and learning); (2) stopping an ongoing response, therefore permitting a delay in deciding to respond; and (3) protection of this decision-making process during this delay from interference. This is all about thinking and decision making.
How does this affect ADHD? Firstly, an inability to inhibit the prepotent response means that an individual will not be able to assess the task demands and the possible outcome of responding. Secondly, a failure to interrupt ongoing behavior may lead to an individual following a well-learnt behavioral pattern even when feedback is stating that the well-learnt response is erroneous. The third process is all about avoiding being distracted when a response is required. In order to deal with the modern world, we have to delay our rewards, check what we are doing is going to work, and modify accordingly. For someone with ADHD, BI is difficult and has ramifications for the whole of the EF (see Figure 4.2).
Figure 4.2 Behavioral inhibition is considered to have effects on working memory, self-regulation, internalization of speech, and reconstitution. Due to a fault in BI these can all be dysfunctional in ADHD. This view has been also argued to be a result of a working memory deficit that feeds into a dysfunctional BI system. Based upon [412] and [519]
The question remains: “Is a deficit in behavioral inhibition the same as impulsivity?” At first the answers appears to be obvious – yes! However, a more detailed investigation finds a debate within the literature. Barkley’s fact is a bold claim, but how significant it is to the symptoms of ADHD is not so clear.
What is impulsivity? Impulsivity has been used to describe the inability to defer obtaining immediate access to reinforcement of a small reward rather than that of a larger but temporally distant reward – a phenomenon tested in tasks such as delay discounting [415–416]. Impulsivity is not a single unitary construct, but a multidimensional construct (see [417–418]), and alterations in the different dimensions of impulsivity could account for the differing subtypes of ADHD [419]. Impulsivity has been associated with inattentive and hyperactive subtypes [420–421].
It has been argued to fit into two broad domains: reward drive and rash impulsiveness [422–423]. Although these two facets of impulsivity have not been linked explicitly to ADHD, they have been linked to other impulse control problems such as addiction. Reward drive is a motivational component of impulsivity, whereas rash impulsiveness is the varying ability of being able to stop a response. In ADHD this could translate with goals that are immediate and desired, but cannot be delayed until a more appropriate time when such actions are warranted. In this format much of the impulsivity data focuses on the rash impulsiveness aspect of ADHD typified by BI tasks.
BI may well be the underlying neuropsychological construct that gives rise to impulsive behavior. In fact it is highly likely – but that it not to say we should accept it without criticism. BI deficits are certainly a phenomenon that is evident and measurable in neuropsychological tests; BI is, after all, what tests of BI measure (e.g. Go/No-go and the Stop-Signal Reaction Time tasks). Thus BI is often operationally defined and serves as a reminder of the old saying about intelligence put forward by Professor Boring in 1923: intelligence is whatever it is that intelligence tests measure (see [424]).
Measures of behavioral inhibition
As I have emphasized the role of BI measures in defining BI, it is necessary to describe these tests for clarification. There are two tests that are frequently used: the Go/No-go task and the Stop-Signal Reaction Time test (SSRT). Both tasks require the suppression of a well-learnt response and are thought to reflect motor BI [425].
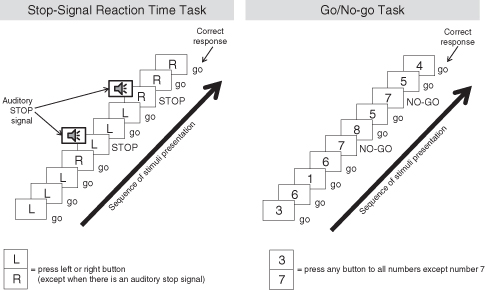
In the Go/No-Go task, individuals are told to respond quickly (e.g. press a button) to a particular stimulus on the Go trials, but to withhold responses when presented with a No-Go stimulus, e.g. press Go for the digits 0–9 appearing randomly, except for the number 7 (No-go). The inclusion of more Go than No-go stimuli means that the Go responses become prepotent (learnt). The number of inappropriate responses to No-go stimuli – pressing the button when you should not (an error of commission) – measures BI. Thus the Go/No-go task measures the ability, or in the case of ADHD the inability, to stop responding.
The SSRT task involves participants having to withhold a response to a Go signal whenever it is followed by a Stop signal. The Stop signal can be an auditory beep during the presentation of visually displayed Go stimuli. The difference between the two processes can be seen in Figure 4.3.
Figure 4.3 The Stop-Signal Reaction Time task (SSRT) and Go/No-go task are measures of behavioral inhibition (see text for details)
A great deal has been written about these two paradigms in both healthy and psychiatric groups. However, the measurement of BI is not restricted to these tasks, and interested readers are referred to a review by Joel Nigg [426].
The use of BI to explain ADHD symptoms is extremely useful and potentially powerful, but one has to remember that BI deficits are not unique to ADHD. Other disorders such as Obsessive-Compulsive Disorder (OCD), Borderline Personality Disorder, and addiction exhibit deficits on BI measures [427–430]. Thus BI tests do not have discriminant validity. A recent study has demonstrated that BI deficits are associated with the prefrontal cortex in ADHD compared with the temporal-parietal area in Conduct Disorder [431]. This study is important as it highlights that the deficits in BI can arise from different regions of the brain and may explain why different disorders can all have deficits in BI. Another issue in assessing BI is that it is not stable across the lifespan: there are developmental differences which mean that BI increases throughout childhood and into adulthood [432–434]. These developmental changes in BI may account for why ADHD was originally considered a disorder of childhood that one grows out of. However, this appears not to be the case. ADHD symptoms could be argued to be less severe in adulthood, but this is debatable when you look at the functional impact and some of the experimental data [435].
Owing to the reliance on the Go/No-go and the SSRT tasks in dissecting BI, the very nature of these tasks becomes important, from both a theoretical and a clinical perspective. Recent reviews on these tasks have questioned their application to explaining ADHD symptoms.
A breakdown in BI occurs when there are competing options and the strongest (prepotent) yet incorrect response is selected over the correct response. This quick reaction to stimuli presentation has been argued to be the basis of impulsivity. Impulsivity itself is a phenomenon that needs further elucidating in this context; not surprisingly, agreement about the nature of impulsivity is limited in the literature.
If Barkley’s BI is the same as impulsivity (i.e. a neuropsychological measure of impulsivity), then this is the cardinal symptom of ADHD, which affects all other symptoms. However, Barkley makes it clear that deficits in working memory (for which there is extensive evidence, see below) may be separate and distinct from BI but they may also co-arise [414]. A recent study from Cambridge University investigated the SSRT task and a Spatial Working Memory (SWM) task in adults with ADHD and patients with lesions of the right frontal lobe [403]. The SWM task assessed the ability of a person to search for hidden tokens in boxes without revisiting already-tried boxes – you need to know where you have been to avoid revisiting empty boxes. These two measures were correlated in both ADHD patients and frontal lobe patients, promoting the speculation of an association between the two constructs, thus supporting Barkley’s view that they are not distinct.
Failures in BI were associated with the severity of ADHD symptoms, and accounted for the symptoms of ADHD more than other cognitive variables [436]. In one study, BI was predictive of performance on working memory tasks, but not attention-based tasks [437]. Further studies using the SSRT in adult groups with ADHD found that they had difficulty in switching attention to the Stop signal (i.e. they did not have the necessary input for them to be able to inhibit the response), prompting Bekker et al. to argue that a measure of BI could also be explained in terms of faulty attention [438]. Another failure to find a deficit in the Go/No-go task whilst finding other executive and non-executive deficits also challenges the significance of BI in ADHD [439]. However, it has been observed that, when directly testing the attentional hypothesis, adult ADHD groups had more variable-choice responses and made more inappropriate change responses in a switching task than controls, which may be reflective of enhanced impulsivity [435]. A meta-analysis of the SSRT task revealed that it is measuring a more generalized problem within attention and cognition rather than a specific deficit of BI [440–441]. Such studies therefore cast doubt on the importance of BI, but also more importantly on using the tasks as descriptors of the BI construct. The theory is only as good as the task.
A review of the literature on impulsivity supports the notion for the importance of BI underlying the impulsivity, in which “the term ‘response [behavioral] inhibition’ refers to the ability to inhibit or suppress simple motor responses that have been rendered prepotent … and deficits in this ability are implicated in impulsivity” [442] (p. 607). An important point to note here is that when discussing BI, most accounts are referring to the suppression of a motor response, as in the Go/No-go or the SSRT task. It has been argued that BI is only evident for motor responding and has been overextended for the inclusion of cognitive control [443]. This may be the case for ADHD, where motor BI but not attentional inhibition was compromised [444], although these latter experiments did not use the Go/No-go or the SSRT task, but instead looked at saccadic eye movements and the attentional blink paradigm, thereby making direct comparisons difficult.
Aron [443] claims that there are a number of reasons why BI cannot be used in the context of cognitive control:
1 It is not economically viable for neural resources to be occupied on BI, instead amplification of stimuli would be a more suitable mechanism – a simple stimulus–response association being strengthened.
2 Lesions of the prefrontal cortex produce BI, but that is not to say that the prefrontal cortex is the site of BI. The prefrontal cortex has been reported to be involved in ADHD and BI.
3 There are better accounts of the performance deficits that are encountered, e.g. working memory (see below).
A study which increased the working memory component of the Go/No-go task demonstrated that ADHD children had a primary deficit in BI and that tasks demanding EF influenced error rates in the same way as controls [445]. A general criticism of the Go/No-go and the SSRT tasks is that obtaining baselines of behavior is arbitrary and that the stop-signal trial may influence following go-trials in terms of speed and accuracy: that is, there is a carry-over effect of one trial to another, and when compared to their own baselines there was little dysfunction seen in ADHD [446]. Differentiating higher order cognitive processes, such as EF, from lower level cognitive processes (such as encoding, perception, and response organization) needs to be accomplished because it has been demonstrated that deficits are not only accounted for by disturbances in EF but could rather be explained as dysfunction of lower level cognitive processes [446], which fits with accounts that play down the role of the prefrontal cortex in ADHD [447].
In a study measuring the brain’s activity using surface-placed electrodes, Banaschewski et al. [448] have been able to detect neural events associated with motor preparation, motor response execution, and motor response inhibition on a Go/No-go task. They investigated a particular set of brain waves that are called event-related potentials (ERPs), of which the two that they specifically looked at are called N2 and P3, which are recorded in response to a stimulus at different sites on the scalp and therefore correspond to different brain regions (see [449] for review). The N2 ERP is associated with frontal areas of the brain and with BI; the P3 is associated more with central-frontal regions. ADHD-C children demonstrated significant differences in the N2 amplitude during motor preparation (and ongoing responses with the SSRT task [450]), indicating reduced attentional resource allocation, whereas the N2 and P3 did not differentiate between ADHD-C and ADHD-C with comorbidities. Only comorbid individuals demonstrated problems with motor preparation and execution, leading the authors to the view that they had difficulty in monitoring the incoming information from their outgoing behavior [448], a view that has some consistency with Lopez et al. [451], who saw a difference in the P300 ERP (another type of potential) in ADHD-C children which was indicative of a processing deficit in the later stages of response organization.
The question remains as to how the remaining subtypes would present under such conditions. A South Korean study demonstrated that ADHD-C had worse inhibitory control than ADHD-I and ADHD-H subtypes, but all subtypes showed deficits compared to controls [72]. In contrast a study using the Go/No-go task in ADHD-I children found them to be over-inhibited [452]. Clearly BI is not uniform across subtypes of ADHD and those with comorbidities; therefore the importance of BI in ADHD still needs more evidence and clarification before it can be regarded as a fact.
Another minor difficultly with the impulsivity/BI debate centers on the neurochemical basis of the construct. The neurochemical serotonin (5-HT) has long been associated with impulsivity [453–454]. Others have argued that impulsivity can be subdivided into different types with different biological bases [418]. The Go/No-go task is possibly mediated by serotonin (or 5-HT), whereas the SSRT task may be mediated by noradrenaline [455]. At this point we should note that serotonergic drugs do not work in ADHD and have limited effects in BI paradigms [456]. The drugs that are used to treat ADHD and are effective in reversing the deficits in BI, e.g. methylphenidate and atomoxetine, work on both dopamine and noradrenaline (see chapters 7 and 9). The neurochemical that is frequently associated with BI is noradrenaline, whereas the use of feedback is associated with serotonin [457]. Thus two systems may be in operation during BI tasks, and in ADHD the one that is most likely implicated is the noradrenergic system.
Impulsive behaviors may appear to be automatic and executed without thinking. They may appear to be quick, knee-jerk responses that have little intention, attention, awareness, or insight. Another hypothesis that may possibly account for BI could be automatic responding. According to Aron [443], response amplification might be more economical than BI. The prepotent response, as in the Go/No-go task, is to have well-learnt responses to Go stimuli that become over-inclusive and are difficult to stop. Another way to describe the data is via the notion of automaticity, i.e. have learnt to respond in a particular way to stimuli. This response is automatic and does not deal with the constraints of the experimental situation. Thus it appears that they react impulsively – without consideration of the task. Automaticity of responses is defined as a “simple, elegant, efficient processing which takes advantage of assumed relationships” [458] (p. 17). Whilst this does not change the general view of BI as the core to ADHD, it does provide an account of how such processing could, under certain circumstances, be advantageous. Therefore impulsivity can be considered as a case of evolutionary adaptiveness (see chapter 5). It is only when the assumed relationships of a stimulus and response cannot be upheld (i.e. a prepotent response is no longer appropriate) that the problems arise. For example, school work does not require impulsive actions, which may be somewhat disruptive to the status quo of the classroom; however, impulsive reactions may be very useful in field sports. When automatic responses are no longer appropriate, conscious awareness of the changes in the environment becomes necessary and then BI may be required. The cortical–subcortical connections appear to be important in accounts of automaticity [458], impulsivity [427], and BI [443], although the exact nature and extent of overlap and differences still remain uncertain.
Nigg [426] elaborates further on the nature of the deficit in BI and states that, on the basis of the evidence, there are two distinct types of inhibition relevant to ADHD: (1) executive inhibition, consistent with Barkley; and (2) reactive or motivational inhibition, which is more reflexive and responsive to emotionally salient stimuli, e.g. reward and punishment, unexpected mismatches, and social unfamiliarity. This latter view is perhaps more closely linked to what we think of as impulsivity. Which one of these accounts of BI is dominant, if indeed one of them can be, is uncertain.
Motivational inhibition
The concept of motivational inhibition (MI) is not new, but its application to ADHD has not yet been fully explored [426]. The use of MI to ADHD can be traced back to the work of the late Professor Jeffery Gray [459–460]. Gray proposed two components of MI: a Behavioral Inhibition System (BIS) and a Behavioral Approach System (BAS).
The BIS and the BAS of Gray’s theory have been argued to fall under the concept of the reward drive component in impulsivity [423]. The BAS is activated when the environment is indicating reward or punishment (and is dopaminergic-mediated). The BIS detects mismatches between the environment and expectations by stopping ongoing behavior and directing cognitive resources to the mismatch. When the BIS is activated, the BAS is inhibited. Psychopathologies such as ADHD are associated with a dysfunction in one or more of these systems, which can account for impulsivity, e.g. a weak BIS which allows approach behaviors to be maintained despite input to the contrary[461–462] or a strong BAS [463].
Despite the intuitive appeal of such accounts the evidence to support a deficient MI is limited and unable to differentiate between those with ADHD and other disorders [464]. Furthermore, the BAS was predictive whereas the BIS was not predictive of hyperactive-impulsive symptoms, but this was in a non-clinical population of undergraduates [465].
The evidence is much more convincing for BI [419, 426]. However, when MI is measured using tasks like the Go/No-go but with the addition of reward incentives, there is little conclusive evidence for a problem in ADHD-C, whereas it impacts on those with Conduct Disorder [419]. By comparison, BI (non-motivated) was a problem in the ADHD-C subgroup on parent ratings but not laboratory measures compared to ADHD-I [397]. Thus the repetitive problem of diagnostic subtypes and comorbidities impacts on this area of research.
With regard to the third criteria for an endophenotype (that it should be state-independent [407]), the general population trait of impulsivity was not associated with BI [466], siblings of those with ADHD did not demonstrate deficits in BI [446], and deficient inhibitory motor control is different in children compared with adults with ADHD [467]. How a failure to inhibit a motor response develops and changes from childhood through to adulthood is, as yet, unknown. However, it may be the very specific effortful BI, which is measured by stopping a motor response, that is associated with particular developmental trajectories of ADHD [468].
As has already been stated, ADHD-C patients showed greater deficits on motor preparedness components of the Go/No-go task with comorbid groups having greater problems monitoring their responses [448]. In ADHD-C children, cognitive inhibition was seen to be less affected than motor inhibition [421] and in adults decision making remained intact [469].
An area that could be of potential use in untangling the BI mechanisms in ADHD is the use of error detection. Are ADHD children cognitively able to inhibit or is the failure in motor programs? Do they know that they have made an error? Error detection is compromised in ADHD children [470–471] and has been associated with reduced activity in the cingulate cortex [472–473]. Using the SSRT task, error detection was reported to be weak in ADHD children whilst not related to BI itself [474]. Although error detection in some of these studies was a neural measure after the onset of a motor response, it may well be interesting to observe the conscious awareness of error in ADHD. Using feedback about the progress of one’s strategies for achieving a goal is an important part of monitoring a plan of action. Error is used to correct the plan; we learn by our mistakes. Error awareness has recently been shown to be reduced in ADHD [471]. Patients with frontal lobe damage are unable to spot their own errors; however, when they were required to observe someone else perform the task, they were able to spot the errors [475]. Similarly some patients with Parkinson’s disease are unable to use self-generated plans and require information provided by the experimenter [476]. Parkinson’s disease is a disorder of reduced dopamine in the brain and deficits in BI are seen [477]. If we accept the theory that the symptoms seen in ADHD are a result of faulty BI with an underlying hypofunctioning dopaminergic fronto-striatal (frontal lobe to striatum) system (see chapter 6), it would be interesting to determine whether or not the BI deficits seen in ADHD are limited to their own internalized generation of motor programs or if they reflect a general misperception of the task requirements. If it were only motor inhibition, then one would assume that they would not be able to perform the tasks (as is evident), but if they were unable to detect errors in other people’s execution of a task, this may suggest deficits in other EF domains, e.g. attention or working memory. Recent reports suggest that there is an early sensory/attentional processing deficit in a Go/No-go task in ADHD-I [478], but this needs clarification.
My concerns over the use of BI tasks in the building theoretical accounts of ADHD rather than the concept of BI are based on the artificial nature of the tasks in question. In everyday life we are not confronted with a vast array of competing signals to stop or go. Furthermore, the notion of impulsivity and BI being one and the same is not fully supported. For instance, the data obtained from a BI task could also be obtained from a test that measures well-learnt stimulus–response associations (an impulsive reaction or reflex). Such associations are simple and may well be the product of a lower subcortical region of the brain. Such a theoretical concept has been put forward to account for addiction [479–481] and anxiety disorders [481] and can be extended to ADHD. In these accounts automatic processes are difficult to control, are efficient or effortless, and can occur unintentionally or outside of conscious awareness; they are therefore reactive and dependent upon stimulus input. An imaging study utilizing the Go/No-go task has demonstrated that in the well-habituated Go response there were no neural differences between ADHD children and non-ADHD children, whereas there was a difference during the No-go trials, indicating learning had taken place at Go trials [482]. In the real world we are more likely to be confronted by Go stimuli, and this behavior is therefore more economical, whereas No-go signals are less frequent and fall into the domain of socialization.
In a study using the SSRT task, children with ADHD had slower and more variable reaction times to Go stimuli whereas the Stop-signal delay was not different between ADHD and control groups. Additionally both control and ADHD groups demonstrated a slowing of reaction times when Go trials were followed by meaningful stimuli, thus indicating interference in the processing of a second stimulus [441]. Alderson et al. [441] suggest that deficits in ADHD, rather than being in BI, are more likely to be a function of a compromised working memory.
Deficits in BI are pervasive in other impulse control disorders, and quite how a deficit in BI translates into one disorder (e.g. ADHD) and not another, (e.g. addiction) is uncertain, although it could be neuroanatomical [431]. As we have already seen, ADHD is highly comorbid with other disorders that also have deficits in BI; what we do not know is whether these comorbid disorders increase the deficits of BI in those with ADHD, and if they do, whether the interaction is additive or synergistic.
As research progresses, it becomes apparent that the theories based on faulty BI in ADHD are far from fact. It has been argued that a heterogeneous disorder such as ADHD, with its subtypes and comorbidities, is unlikely to be the result of a single causative construct [483]. To state that BI is involved in the symptom formation in ADHD, and possibly the core problem, is insufficient to help us fully understand the disorder. We need to understand why deficits in BI appear as particular subtypes of ADHD, or as substance abuse disorder or schizophrenia. The work ahead is clearly challenging, but it is important to determine if BI really is the core deficit in ADHD. Other neuropsychological accounts of ADHD have been regarded to provide more parsimonious endophenotypes, e.g. working memory or temporal processing [484], and these also maybe related to BI [485].
On a final note, the role of impulsivity is dependent on context and perspective. Is impulsivity always a bad thing? The answer can be found in evolutionary accounts of behaviors (see chapter 5). A report by Gullo and Dawe [486] identifies positive attributes of impulsivity linked to, for example, leadership skills that are reflected in various occupations [487–489]. Even though rash impulsiveness has little that can be seen positive associated with it, risk-taking behavior has been associated with success in business, especially in those who seek venture growth [490]. Although this study was used as to illustrate the positive aspects of impulsivity, 2001 was a good year; midway through 2010, we have seen these qualities as negatives again as world recession looms. This point illustrates the social context in which science, and the interpretation of science, takes place: 2001 a good thing, 2010 a very bad thing – same behavior just a different context.
Alerting, Orienting, and Executive Functioning – Separate Circuits in ADHD
The theoretical perspective developed by Swanson et al. [109] starts with the idea that separate and distinct neural circuits work independently on (1) alerting, (2) orienting, and (3) executive functioning [491]. Alerting is when background neural activity (noise) is inhibited, thus removing interference of other stimuli – this is the signal-to-noise ratio in which signals should gain strength over background noise derived from competing signals. Orienting activates appropriate resources favoring specialized processes to deal with the input stimuli whilst inhibiting unnecessary processes, thus a favorable response is selected (similar to the Supervisory Attentional System – see below). Executive control refers to overseeing the many specialized neural responses and directs behavior towards achieving the goal. These three systems therefore work to produce an economic use of limited neural resources.
The symptoms of ADHD have been attributed to each of the three processes [109]. Poor sustained attention is thought to be attributed to an alerting deficit which is associated with noradrenaline in the right frontal lobe. This is consistent with noradrenaline having an important role in arousal [492]. Poor selective attention is a reflection of an orienting deficit associated with acetylcholine in the bilateral parietal lobe. Finally, impulsivity is associated with a defect in executive function related to the anterior cingulate area and is dopamine-mediated [493]. Imaging data obtained during BI tasks support the anterior cingulate as an important region [473].
Swanson et al.’s theoretical perspective, together with its neuroanatomical and neurochemical basis, lends itself to accounting for symptoms and subtypes independently. A deficit in one process may lead to one set of symptoms, whilst another could lead to a different set of symptoms. Thus an alerting deficit may be evident in ADHD-I subtypes, an orienting deficit in ADHD-I and ADHD-C, and a deficit in executive functions in ADHD- H and ADHD-C. Although the distinction between the subtypes is not crystal-clear, this theory offers the possibility to test the basis of subtype differences. And furthermore, one or more of the systems may be dysfunctional in any one individual with ADHD with or without comorbidities.
The data supporting such a demarcation of attention and executive functions are sparse. Using an attention network test to look at orienting, conflict, and alerting systems in response to a warning stimulus, Booth et al. [494] found only differences in alerting effects in ADHD-I compared to ADHD-C groups, but these differences were not statistically significant when compared against controls. A normal alerting response was also seen in the ADHD-I subgroup, but not in the ADHD-C subgroup [495]. As is becoming increasingly obvious, the ADHD-C groups in particular have deficits in EF, but not exclusively. At present, differentiation of the neuropsychological deficits in the subtypes is difficult, yet extremely important, but any search for a single defining deficit may be futile [496]. Swanson’s account of ADHD sensibly allows for multiple systems being compromised and avoids the loss of a single process as being the core problem. Sadly the data do not fit so neatly with the theory!
Working Memory
Working memory (WM) has become a widely accepted and dominant neurocognitive construct since its first outing in the early 1970s [497]. Since then it has evolved into a comprehensive theory of mental life with a huge body of literature supporting it [498]. WM’s endurance in the psychological literature demonstrates its powerful application to understanding behavior [499]. It has been implicated and researched in the context of many disorders, and ADHD is no exception.
But what is WM? Let us start with what it is not. It is not just memory. WM is much more to do with attentional mechanisms and allocation of resources for information processing. WM is not one entity, but a set of processes that construct, maintain, and manipulate the psychological representation of stimuli. WM is another way of discussing executive functions.
Information within working memory is stored temporarily and has a limited capacity. To use a computer analogy to describe working memory, we have two types of memory in a computer: the hard-drive and RAM. The hard-drive is like long-term memory. To access these memories (files) using the necessary software, we need RAM. RAM is like our WM: it is the fluid memory that holds the information whilst it is being worked upon. Thus, WM provides temporary storage of psychological representations of stimuli for processing and permits higher order functions to occur, e.g. understanding language – we need to hold the words of a sentence together in order to gain the meaning of the sentences rather than have a series of disconnected words in list.
WM is made up of a number of separate but interconnected components (see Figure 4.4). At the core of working memory is the Central Executive. Continuing with the computer analogy, the central executive is like the dual core processors, and the software works upon the information depending on the nature of that information, e.g. iTunes works with music files whereas Photoshop works with picture files.
Figure 4.4 Working memory (see text for details)
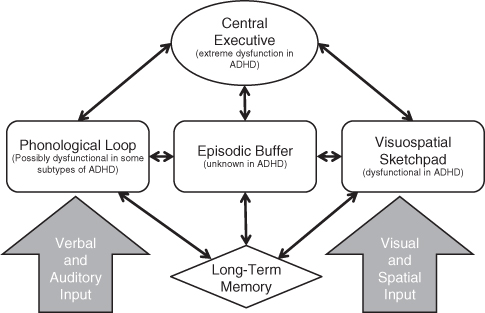
The Central Executive is an attentional control system similar to that outlined by Norman and Shallice (see below). Additional to the Central Executive are two slave systems: the Visuospatial Sketchpad and the Phonological Loop. The Visuospatial Sketchpad holds information that can be broken down into visual, spatial, and kinesthetic components, all of which are associated with areas within the right hemisphere of the brain. The Phonological Loop holds verbal and acoustic information. More recently the WM model has included an episodic buffer [498]. The episodic buffer is a temporary storage system that can integrate information from different sources. The Central Executive controls and retrieves information from the Episodic Buffer in the form conscious awareness, which can then be worked upon in problem-solving activities. The location of both the Central Executive and the Episodic Buffer is regarded to be in the frontal lobes, with different cortical subregions being involved in different mental processes. Thus WM is not a box of tools with one identifiable function, but rather a set of theoretical processes that work on different information in different regions of the brain. We cannot put our finger on the exact location of WM, but this might be the strength of the theory in explaining the many faces of ADHD.
Deficits in WM have been identified in ADHD (e.g. Barkley’s account and neurochemical accounts [500]), in experimental studies [501–503], and within subsections of intelligence tests [504]. WM, and in particular the Central Executive, is dysfunctional in many disorders and the same criticism can be made as with BI: namely there is no specificity of the WM deficit – it can be used to explain problems beyond that of ADHD [501]. A meta-analysis of working memory in ADHD indicates that there are widespread deficits across systems, but the spatial slave system and spatial wing of the Central Executive were the most affected [502]. In one study, ADHD patients had deficits on a visuospatial working memory task but not on the Go/No-go task [505], thus indicating a prominent deficit in WM and not BI, perhaps at the time of input and encoding of visuospatial information [506]. In contrast, Pasini and colleagues [437] did find a deficit in phonological and visuospatial working memory in males with ADHD-I and ADHD-C, but they also had deficits in BI and attention. However, another study found that children with ADHD did not differ from control children on spatial and verbal tasks, indicating that the two slave systems were not affected in ADHD, whereas tests of the Central Executive revealed that children had difficulties in tasks requiring dual processing of information which increased as a function of task difficulty, i.e. information overload [507].
Rapport and colleagues have used the WM concept and modified it to account for the symptoms of ADHD, including hyperactivity [508]. Hyperactivity in neuropsychological theories is often neglected.
In this model a component that is essentially the same as the Central Executive is compromised, resulting in haphazard and disorganized responding to input stimuli which can be seen in ADHD.
In addition to the disorganization in ADHD, and as a result of failures within WM and the associated cortical under-arousal, motivation to irrelevant stimuli is increased; this is not beneficial! Input to the slave systems of WM will induce increased activity levels to compensate for cortical under-arousal. Although Rapport et al. [508] are careful not to place WM in a specific neuroanatomical location, they find support for cortical under-activity from psychophysiological studies [509–511]. As the representations within WM fade rapidly, their loss is compensated for by increased input to working memory. Thus in this conceptualization of ADHD, WM becomes overloaded by incoming environmental stimuli; again this is not unique to ADHD but common to a number of psychiatric disorders. When WM is overloaded, those with ADHD will seek to escape (and eventually avoid) situations associated with this aversive state. As Rapport et al. note, redirecting attention to other stimuli can alleviate monotonous or difficult tasks (academic school work!), which can be observed as impulsivity and/or hyperactivity, i.e. the child gets out of his seat at school. In an elegant study by Rapport et al. (reported in [98]), all children who were given WM tasks demonstrated increased concurrent motor activity; however, those children with ADHD engaged in the escape/avoidance behavior when the task was made more difficult. This has led to the suggestion that arousal facilitates cognitive functioning in all. To illustrate this point, look at people when they are engaged in cognitive tasks in everyday life: when people try to solve crossword puzzles, for example, may rock their legs or shake their pencil. I could see this in my children when they were trying to learn to read. They would squirm and move around in their seat; the one with ADHD would be distracted and engage in all sorts of escape behaviors, whereas the one without ADHD would just move about but stay on task. However, ADHD children engage in more activity to compensate for the loss of cortical arousal, and this is consistent with the evidence suggesting that those with ADHD have a personality best described as sensation seeking or novelty seeking [12, 512–515]. Children with ADHD were seen to be more active than controls during times of no stimulation compared to times of stimulation, thus supporting a view of the ADHD child as a sensation seeker and using hyperactivity to obtain stimulation [516]. Furthermore, there has been a debate regarding the link between sensation seeking and the DRD4 gene [517], which has also been linked to ADHD [518]. However, it has been found that the DRD4 gene was linked with ADHD, but not novelty seeking [515], where one might expect the two to be linked.
Essentially, the failure of WM is seen as a core deficit upon which the symptoms of ADHD can be mapped. The data are generally supportive of such a case, but they are not conclusive. Rapport provides an elegant account of ADHD in terms of working memory and uniquely applies it to the hyperactive state – something other theories neglect. However, the specificity of a dysfunctional WM is not strong, with several other disorders showing WM deficits. The lack of specificity for ADHD is not such a problem for the WM concept. The conceptual basis of BI rests on the tasks, whereas with WM it is a true theoretical concept with multiple systems. Deficits in WM could be accounted for by deficits in one or more areas of WM, or the balance between the areas. BI addresses a single behavior – stopping a response; WM deals with a vast array of information processing (see Figures 4.2 and 4.4).
In my view, the WM deficit offers the most parsimonious account and assimilates the BI deficits seen in ADHD. It is not necessarily a case that Barkley and others are completely wrong; they are, in some cases, correct. It is a case of which model may best account for the symptoms. Rapport et al. suggest that “working memory processes must be invoked to evaluate stimuli (including situational cues) prior to the initiation of the inhibition process. … This suggests that behavioral inhibition is downstream of working memory processes” [98] (p. 375).
Whilst the focus on the Central Executive is entirely understandable, the other systems have not received similar attention. The deficits seen in ADHD are not restricted to the Central Executive (although the effects are strongest here), but also extend to visual and phonological sub-domains [519]. The most recent developments of the WM theory such as the Episodic Buffer need to be further clarified. Little is known about the episodic buffer in general, let alone in ADHD.
The Supervisory Attentional System
Baddeley’s notion of the Central Executive was not a lightning bolt of inspiration, but rather a carefully studied re-conceptualization of another theory [497, 520–521]. This influential model of attentional control was provided by Donald Norman and Tim Shallice [522]. Their model of cognitive functioning has central to it the Supervisory Attentional System (SAS); the SAS shares, unashamedly, marked similarities with Baddeley’s Central Executive. This is a theory of EF and how behavior is controlled. The theory is based on two premises: (1) the routine selection of routine operations is automated (well-learnt); and (2) the selection of non-routine operations is qualitatively different from routine selection and involves a general-purpose supervisory system that oversees behavior. There is also some similarity with what Weirs and Stacy have called implicit and explicit cognitions [479–481, 523].
In the Norman–Shallice model of executive control there are two levels of response programs: low-level and high-level processes. Low-level processes (or schemata as they are called) are activated when certain demands are created in the environment, e.g. driving a car activates schemata such as stopping at red lights. Not surprisingly, patients with ADHD have more accidents whilst driving than do controls [524]!
Selection of a schema is dependent on the potential inputs that can act as a trigger; once a schema has been activated, other schemata are inhibited. The selection between routine actions is regarded as an automatic process without conscious awareness or allocation of attentional resources; it prevents conflict between potentially competing schemata. In this regard, when driving a car, component schemata are primed, and if the environmental circumstances dictate, e.g. a red light shows, the schema of braking will be activated and the accelerating schema will be inhibited. The automaticity of this action depends on learning and experience. Schemata are well-learnt response programs. Clearly our behavior is not all automatic, but it does allow us to economically perform actions without recourse to the effort of thinking. However, circumstances might arise when routine selection is inappropriate and the conscious awareness of environmental context becomes necessary; thinking is required and thinking requires energy. Situations that require planning and decision making, error correction and troubleshooting, or involve novelty or danger, or overcoming habitual responses and temptation, require conscious awareness (thinking), and this is when a higher level process called the Supervisory Attentional System (SAS) is needed. The SAS modulates the schemata’s activation level, thereby increasing the likelihood of the correct schema being triggered.
This theory accounts for the actions of the frontal lobe using evidence from studies involving lesions of various subregions to support the theory [406] in which frontal lobe damage is linked to dysfunctional components of the SAS [525]. Despite the obvious parallels with the ADHD symptoms and hypofrontality (reduced activity in the frontal lobes), surprisingly little has been said about ADHD and the SAS.
From the plethora of research suggesting a problem with executive functioning in ADHD, could these deficits be attributed to a breakdown of the SAS? I am aware of only one study that relates the symptoms of ADHD to a dysfunctional SAS. The study in question, by Bayliss and Roodenrys [526], used a number of neuropsychological tasks that assessed BI of a strongly triggered response and also impulsive behavior in the absence of dominant trigger. Their findings partially support the SAS concept, with ADHD children performing poorly on the tests on BI but with relative sparing of tests of impulsivity; the results also suggest that BI, as measured in neuropsychological tests, and impulsivity are separate. The frontal lobes are large areas of the brain and localization of function is attributed to subregions. Likewise the SAS can be decomposed into separate units that are functionally different [525]. This fractionation of the SAS permits the data to be accounted for, by ascribing inhibitory functioning to one part of the SAS and impulsivity in the absence of a strong trigger to another part. So can we really argue that BI is the same as impulsivity?
Like many other theories, the SAS account of ADHD symptoms was a deviation from its original intentions (explaining the data obtained from brain-damaged patients). Despite neuroimaging studies indicating structural and functional differences in the brains of ADHD patients, the brains are not damaged. The brains of ADHD people may have small statistically significant differences, but these differences have as yet to be verified as clinically significant in the etiology and pathology of ADHD. Therefore the application of the SAS theory to ADHD does not specify a cause, but it does provide a detailed description of the neuropsychological data and has been applied to disorders such as schizophrenia (e.g. [527]).
Brown’s Executive Functioning Model
Rather than apply a general theory of EF to ADHD, Brown [528] evaluated ADHD and placed the symptoms in a new theoretical framework of executive functions. One may consider this as fitting the data to your own theory, but it is not that different an exercise to the original concepts of the SAS and W.M. Brown evaluated reports highlighting the problems experienced by those with ADHD and compared them with normal controls. His endeavors resulted in the identification of six clusters within the domain of executive functions:
1 Activation: organizing tasks and materials, estimating time, prioritizing tasks, and getting started on work tasks.
2 Focus: focusing, sustaining focus, and shifting focus to tasks.
3 Effort: regulating alertness, sustaining effort, and processing speed.
4 Emotion: managing frustration and modulating emotions. Although the DSM-IV does not recognize any symptoms related to the management of emotion as an aspect of ADHD, many with this disorder describe chronic difficulties managing frustration, anger, worry, disappointment, desire, and other emotions.
5 Memory: utilizing working memory and accessing recall.
6 Action: monitoring and regulating self-action. Impulse control.
The six clusters are not mutually exclusive categories; they can overlap and influence each other. Brown does not ascribe any one particular deficit as being more important than the other, and therefore this is more of a description of executive function than a theoretical attempt to understand the processes. The six clusters have each been held to account as individual protagonists in the development of ADHD symptoms.
The Cognitive-Energetic Model
Sergeant [529–530] proposed another neuropsychological theory of ADHD called the Cognitive-Energetic Model. This model does not try to attribute the symptoms of ADHD to one primary deficit (e.g. BI), but rather sees a range of functions that may be differentially impaired which clearly fits with the heterogeneity of ADHD. The deficits that are found across disorders and within ADHD subtypes are dependent not only on the task or measure used, but also on the motivational/energetic state of the child; this is where the often-used notion of top-down and bottom-up processing comes into play. Top-down processing is to do with executive functions communicating with slave systems below; bottom-up is when these slave systems mediate and influence the processing characterized by EF.
The Cognitive-Energetic Model comprises three components: (1) computational processes, (2) energetic pools, and (3) management and evaluation mechanisms.
Computational processes are low-level cognitive acts that include encoding, search, decision, and motor organization. The energetic pools include effort, arousal, and activation. Management and evaluation mechanisms are the same as what is termed EF, and include planning, monitoring, error detection/correction, and BI.
These three levels of information processing are implicated in ADHD and other disorders. Apart from the well-documented deficits in EF seen in ADHD, Sergeant states that the effort and especially the activation of energetic pools are related to BI, where “ADHD children’s lack of response [behavioral] inhibition is modulated by their inability to adjust their state” [529] (p. 10). Recently van Mourik et al. [531] studied the effects of novelty in children with ADHD in which a novel stimulus increased the orienting response to that stimulus whilst reducing errors on a reaction-time task, thereby leading the authors to suggest that increased arousal was beneficial to task performance. Such an effect can also be seen in the clinic where a child in a novel situation does not present to the psychiatrist as symptomatic. This role of arousal in this model is similar to its role in WM. However, the concept of an arousal pool is theoretical and does not lend itself to empirical analysis [508] and thus limits the scope of the theory in ascribing causality to ADHD.
Summary
Have the neuropsychological theories really helped us understand ADHD? The cynics would say no, but perhaps they hoped for too much. Weaknesses in EF are neither necessary nor sufficient to cause all cases of ADHD [379], leaving some cases unresolved.
The neuropsychological theories are just that, theories, and as such they are profoundly important in stimulating discussion and argument which helps increase our understanding of ADHD. There are many questions that still need answering about executive functions in general, before we can even begin to get a better understanding of their effects in ADHD. A simple yet important question still remains: What are the tasks actually measuring? We have seen that this is not as straightforward as it sounds. A further question of extreme importance is: What part of EF is dysfunctional in ADHD and is it the same across subtypes? Is it BI or is it a whole myriad of processes that fall under the umbrella of executive functions? Can one component of executive function really account for all the other deficits, or is executive function a set of processes that are independent, yet interrelated? I don’t know the answer, and I am not alone. To coin a well-used phrase in science … more research needs to be done in this area.