CHAPTER 150
The Skin and Disorders of the Heart
Sonja Molin and Thomas Ruzicka
Department of Dermatology and Allergology, Ludwig Maximilian University, Munich, Germany
Introduction
There are several diseases in which both cardiac and skin involvement may be found (Table 150.1). Most of these are part of a syndrome or are systemic disorders affecting other organs as well [1, 2]; most conditions are discussed in other chapters, but some are briefly described here. Disorders of blood vessels are not included here. The effects of skin disease on the heart (e.g. cardiac failure due to erythroderma) and indirect effects, such as anaemia due to immunosuppressive agents used to treat the skin, are not discussed here either. Numerous infections may occasionally cause myocardial disease and may also present with an exanthem (e.g. parvovirus B19), but these are not discussed individually. Drug reactions due to cardiac medications are described in Chapters 118 and 119.
Table 150.1 Conditions that affect the heart and skin.
| Disease | Main cardiac feature and/or comment |
| Congenital/inherited | |
| Ehlers–Danlos syndrome | Dilated main vessels, mitral or tricuspid insufficiency, cardiac/vascular rupture (type IV) |
| Cutis laxa | Early CAD, aortic aneurysm, mitral valve prolapse |
| Marfan syndrome | Aortic aneurysm, aortic regurgitation, mitral valve prolapse or regurgitation |
| Pseudoxanthoma elasticum | Arterial calcification, CAD, mitral valve prolapse |
| Werner disease | Early CAD |
| Progeria | Early CAD |
| Cockayne syndrome | Early CAD |
| Cornelia de Lange syndrome | Septal defects, persistent ductus arteriosus, pulmonary stenosis |
| Fabry disease | Conduction defects, arrhythmias, hypertension, left ventricular hypertrophy, mitral valve prolapse; see text |
| RASopathies:Noonan syndrome | See text Pulmonary stenosis, septal defects, hypertrophic cardiomyopathy, aortic abnormalities, other features |
Noonan syndrome with multiple lentigines (LEOPARD syndrome) Neurofibromatosis |
ECG abnormalities (various forms of heart block), pulmonary stenosis, also subaortic stenosis and hypertrophic cardiomyopathy Hypertension (renovascular or phaeochromocytoma) |
Rubinstein–Taybi syndrome Tuberous sclerosis |
Aortic coarctation, persistent ductus arteriosus, pulmonary stenosis, septal defects Cardiac rhabdomyomas |
| Incontinentia pigmenti | Patent ductus arteriosus, tricuspid insufficiency |
| Alagille syndrome | Pulmonary artery hypoplasia/stenosis |
| Di George syndrome | Tetralogy of Fallot, aortic arch defects |
| Lymphoedema–distichiasis syndrome | Tetralogy of Fallot, patent ductus arteriosus |
| Naxos disease | Arrhythmogenic right ventricular cardiomyopathy |
Chromosomal syndromes Carney complex |
Various, includes Down syndrome, Turner syndrome, trisomy 13, trisomy 18 See text |
| Inflammatory diseases, connective tissue disease, vasculitis | |
| Systemic lupus erythematosus | Vegetations (especially mitral, Libman–Sacks endocarditis), pericarditis, myocarditis, aortic/mitral regurgitation |
| Neonatal lupus erythematosus | Neonatal heart block (various patterns), septal defects, persistent ductus arteriosus, tricuspid/mitral insufficiency |
| Systemic sclerosis | Pericarditis and effusion, conduction defects, myocardial fibrosis, cardiomyopathy, cor pulmonale |
| Limited systemic sclerosis (CREST) | Pulmonary hypertension |
| Polyarteritis nodosa | Coronary artery vasculitis, ECG abnormalities, hypertension |
| Behçet disease | Pericarditis, pulmonary and coronary artery aneurysm |
| Antiphospholipid syndrome | Vegetations, valvular heart disease, coronary artery thrombosis, pericardial effusion, CCF |
| Degos disease | Pericarditis, pericardial effusion |
| Eosinophilic granulomatosis with polyangiitis (EGPA; former Churg–Strauss syndrome) | Pericarditis, cardiac fibrosis, pericardial effusion |
| Granulomatosis with polyangiitis (GPA) | Cardiomyopathy |
| Cholesterol emboli | Coronary artery occlusion |
| Other vasculitides | Coronary artery vasculitis |
| Dermatomyositis | Conduction defects, arrhythmias, cardiomyopathy, CCF, (rarely) pulmonary hypertension |
| Relapsing polychondritis | Mitral or aortic insufficiency, dissecting aortic aneurysm, pericarditis, myocardial ischaemia, heart block, aortitis |
| Rheumatic fever | Mitral and aortic valve disease |
| Kawasaki disease | Conduction defects, coronary artery aneurysms, pericardial effusion, cardiomegaly |
| Multicentric reticulohistiocytosis | Pericarditis, cardiomegaly, CAD, CCF |
| Hypereosinophilic syndrome | Eosinophilic endomyocarditis, valvular scarring, CCF, restrictive cardiomyopathy |
| Sarcoidosis | Conduction defects, arrhythmias, CCF |
| Reactive arthritis | Conduction defects, aortic regurgitation |
| Deposition, metabolic and endocrine disorders | |
| Amyloidosis | Conduction defects, cardiomegaly, CCF |
| Haemochromatosis | Arrhythmias, cardiomyopathy, CCF |
| Wilson disease | Arrhythmias, cardiomyopathy |
| Mucinoses: scleromyxoedema | Cardiomyopathy, CCF |
| Hyperlipidaemias | CAD |
| Diabetes | CAD, cardiomyopathy |
| Hyperthyroidism | Tachycardia, atrial fibrillation, mitral regurgitation |
| Hypothyroidism | Bradycardia, CAD, pericardial effusion |
| Acromegaly | Left ventricular hypertrophy, CCF |
| Carcinoid syndrome | Tricuspid or pulmonary stenosis, right heart failure |
| Phaeochromocytoma | Variable heart rate, hypertension/hypotension |
| Mastocytosis | Tachycardia, hypotension, arrhythmia, angina |
| Homocystinuria | Atherosclerosis |
| Embolic diseases: | |
| Infective endocarditis | Vegetations, valvular incompetence |
| Cholesterol emboli | Usually from proximal arteries rather than cardiac |
| Atrial myxomas | See text |
| Infections | |
| Lyme disease | Myocarditis, heart block |
| Syphilis | Aortitis, aortic aneurysm, aortic and mitral regurgitation, obstructed coronary arteries |
| Varicella | Myocarditis |
| Septicaemia | Pustules, infarcts, disseminated intravascular coagulopathy |
| Congenital rubella | Pulmonary artery and valve stenosis, patent ductus arteriosus |
| Whipple disease | Pericarditis, myocarditis, valve deformity (especially mitral valve endocarditis) |
| Drugs | |
| Used in cardiology, causing rash | For example, amiodarone (photosensitivity, pigmentation) |
| Cardiotoxic and cause skin eruptions | For example, doxorubicin (cardiotoxic, anagen effluvium, pigmentation) |
| Used for skin disease, cardiovascular side effects | For example, ciclosporin (hypertension) |
| Teratogenic, causing both skin and cardiac defects | For example, alcohol, phenytoin, retinoids |
| Miscellaneous | |
| Earlobe crease | CAD |
| POEMS syndrome | Cardiac failure |
| Mycosis fungoides, Sézary syndrome | Heart is infiltrated in advanced disease |
| Kaposi sarcoma | Heart is commonly involved |
| Diffuse neonatal haemangiomatosis | High-output cardiac failure |
| Erythroderma, any cause | High-output cardiac failure |
| Pacemaker reactions | Infection, contact dermatitis, mechanical issues |
| Clubbing of nails | Cyanotic congenital heart defects |
| Red lunulae | Occur in CCF |
CAD, coronary artery disease; CCF, congestive cardiac failure; CREST, calcinosis, Raynaud's phenomenon, esophageal disease, sclerodactyly, telangiectasia (syndrome); ECG, electrocardiogram; LEOPARD, lentigines, ECG abnormalities, ocular hypertelorism, pulmonary stenosis, abnormalities of genitalia, retardation of growth, deafness (syndrome); POEMS, polyneuropathy, organomegaly, endocrinopathy, M protein, skin changes (syndrome).
Skin signs of cardiac disease
Dermatological consequences of cardiac disease include skin colour changes such as cyanosis, erythema due to secondary polycythaemia, and a combination of the two that may occur in congenital heart disease (and which has been termed erythraemia). Finger clubbing is a consequence of congenital cyanotic heart disease (Figure 150.1), but occurs in other situations as well. A visible pulsation of the nail bed in time with the pulse is a sign of aortic regurgitation due to the wide pulse pressure in this disorder (Quincke pulsation) [1, 2].

Figure 150.1 Finger clubbing in association with congenital cyanotic heart disease and Eisenmenger syndrome.
HEREDITARY SYNDROMES
Cardiac involvement occurs in several congenital and inherited conditions, such as the RASopathies, Carney complex, Fabry disease and Alagille syndrome [1, 3], as well as in chromosomal abnormalities such as Turner syndrome and trisomy 13 or 18 [1].
Lymphoedema–distichiasis syndrome
The lymphoedema–distichiasis syndrome is an autosomal dominant genetic disorder due to mutations in the FOXC2 gene. Beyond lower extremity lymphoedema and distichiasis, a condition where eyelashes grow from abnormal locations on the eyelid, it has been linked to cardiac anomalies [4].
Cardiac rhabdomyomas, cardiomyopathy and supraventricular tachycardia are reported in patients with tuberous sclerosis (see Chapter 80) [1].
Fabry disease
In this rare inherited sphingolipidosis, cardiac involvement may be manifest as arrhythmias, hypertrophic cardiomyopathy, valvular abnormalities and coronary artery disease (see Chapter 81) [1, 2]. The cutaneous features include angiokeratoma corporis diffusum and hypohidrosis or anhidrosis (Figure 150.2) [3].
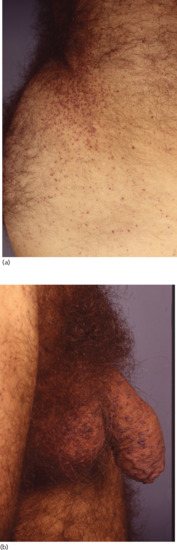
Figure 150.2 Fabry disease in a 46-year-old man with extensive involvement of (a) the buttocks and (b) the genitalia.
RASopathies
A number of genetic syndromes have been summarized under the term RASopathies [3]. Amongst them are the Noonan syndrome, Noonan with multiple lentigines syndrome (also known as the LEOPARD syndrome or multiple lentigines syndrome), Costello syndrome, cardiofaciocutaneous syndrome and neurofibromatosis 1. They share the common feature that mutations in the rat sarcoma–mitogen-activated protein kinase (Ras-MAPK) signal transduction pathway are pathogenic and lead to the development of cardiac and cutaneous malformations. The former include hypertrophic cardiomyopathy, pulmonary stenosis and atrial septal defects.
Characteristic for Noonan with multiple lentigines syndrome are widespread lentigines, electrocardiographic abnormalities, ocular hypertelorism, pulmonary stenosis, abnormal genitals, retardation of growth and deafness (hence LEOPARD syndrome). The cardiac involvement includes left axis deviation on an electrocardiogram (ECG), ventricular hypertrophy and arrhythmia.
Carney complex
The Carney complex was previously known as the LAMB (lentigines, atrial myxoma, mucocutaneous myxoma, blue naevi) syndrome or the NAME (blue naevi, atrial myxoma, myxoid neurofibromas, ephelides) syndrome. It is a result of mutations in the PRKAR1A gene (protein kinase, cAMP-dependent, regulatory, type I, alpha) [3, 5]. The inheritance is autosomal dominant with incomplete penetrance. It is characterized by recurrent myxomas, pigmented skin lesions, endocrine overactivity and neoplasms (e.g. growth hormone-producing adenoma often with acromegaly, Sertoli cell tumours and Cushing syndrome) [5]. Nearly 70% of patients have myxomatous cardiac tumours. Mucocutaneous myxomas (eyelids, external ear, breast and oro-pharynx) are present in one-third of patients (Figure 150.3). Pigmentary abnormalities such as blue naevi, café-au-lait macules and lentigines are commonly seen (in 75% of cases) [5].

Figure 150.3 Cutaneous myxoma in a patient with Carney complex.
CARDIAC INVOLVEMENT IN DERMATOSES OR SYSTEMIC DISEASES WITH SKIN FEATURES
Inflammatory disorders
Cardiac involvement is common in systemic disorders such as sarcoidosis (see Chapter 98) [6], mixed connective tissue disease (see Chapter 54) [7], dermatomyositis (see Chapter 53) [7], lupus erythematosus (see Chapter 51) [8, 9], systemic sclerosis (see Chapter 56) [10] and vasculitis (see Chapter 102) [12, 13], although it may be underestimated if symptoms are absent.
Sarcoidosis. Up to 25% of patients with sarcoidosis have heart involvement. Sudden death due to conduction defects and ventricular arrhythmias is the most important complication, and is particularly well recognized in sarcoidosis; cardiomyopathy may also occur [6].
Mixed connective tissue disease. Clinically significant pericarditis, myocarditis and pulmonary hypertension may occur in mixed connective tissue disease but this is rare [7].
Dermatomyositis. The heart may be involved in dermatomyositis or polymyositis with the occurrence of congestive heart failure, coronary artery disease or conduction abnormalities [7].
Systemic lupus erythematosus. Cardiovascular disease is very frequent in systemic lupus erythematosus [8]. A number of cardiac complications occur, especially pericarditis, a high prevalence of atherosclerosis and an increased risk of myocardial infarction.
Neonatal lupus erythematosus. A congenital atrioventricular block (AVB) is the most common cardiovascular symptom of neonatal lupus erythematosus (LE). Mothers of affected children generally express the 52 and 60 kDa anti-SS-A (Ro) antibodies, even if they have no other features of LE [9]. Beyond AVB, the spectrum of heart involvement in neonatal LE varies widely and includes not only valve defects, but also cardiomyopathy or myocarditis.
Systemic sclerosis. Cardiac involvement in systemic sclerosis is not always clinically apparent but is believed to be a poor prognostic factor. Pericarditis, pericardial effusion, arrhythmias, myocardial fibrosis, conduction system defects, endothelial damage to coronary arteries and heart failure due to pulmonary arterial hypertension all occur [10]. Symptoms include heart failure, palpitations and myocardial infarction.
Antiphospholipid syndrome. In the antiphospholipid syndrome [11], about 50% of patients have valvular heart disease, either vegetations or thickening (see Chapter 52). The mitral valve is most frequently affected. There is also an increased incidence of atherosclerosis, coronary artery disease and myocardial infarction.
Vasculitides. The major vasculitides that affect the heart belong to one of the following groups: (i) small-vessel vasculitis (granulomatosis with polyangiitis (GPA), eosinophilic GPA (EGPA)); (ii) medium-vessel vasculitis (polyarteritis nodosa, Kawasaki disease); or (iii) large-vessel vasculitis (temporal arteritis, Takayasu arteritis) [12]. Cardiac involvement is commoner in EGPA than in GPA [13].
Amyloidosis. Cardiac involvement is frequent in primary amyloidosis [2, 14], causing features of cardiomyopathy such as congestive heart failure, low voltage on an ECG and conduction disturbances. Cutaneous signs, macroglossia and demonstration of amyloid deposition on skin histology support the diagnosis (see Chapter 58).
Kawasaki disease. Kawasaki disease (mucocutaneous lymph node syndrome) is an acute febrile disease principally of infants and children (Figure 150.4) and is due to an immune-mediated medium-vessel vasculitis that affects the coronary arteries (see Chapter 26). Clinical manifestations are prolonged fever and signs of acute inflammation [2]. Coronary artery aneurysms may develop in up to 25% of patients; other cardiac sequelae include myocardial infarction, conduction defects, pericardial effusion and cardiomegaly.

Figure 150.4 Kawasaki syndrome in a 16-year-old girl showing (a) a rash on her body and (b) the characteristic ‘strawberry tongue’.
Infections
Infective endocarditis. Infective endocarditis [2] typically occurs in patients with a past history of heart disease (rheumatic fever, congenital heart disease, degenerative valve disease, heart valve operation), intravenous drug use or recent dental surgery. Around 50% of cases of infective endocarditis develop in patients without a history of valve disease [15]. Up to 80% of cases are caused by staphylococcal or streptococcal infection. Cutaneous lesions may represent either septic emboli or immune complex disease due to circulating bacterial antigens [2]. The skin lesions may be purpuric, pustular or erythematous, and various patterns are described. Splinter haemorrhages of the nail fold or nail bed occur as well as conjunctival and palatal petechiae. Osler's nodes are small, tender, red papules situated mainly on the distal finger and toe pads; Janeway lesions are faint, red, macular lesions on the thenar and hypothenar eminences.
Rheumatic fever. Rheumatic fever is a complication of streptococcal infection [2]. It causes arthritis, carditis, neuromuscular disease (e.g. Sydenham chorea, muscle weakness) and cutaneous lesions. The latter include erythema marginatum and subcutaneous nodules on the extensor surface of the extremities, particularly near the joints. Erythema marginatum is a transitory gyrate erythema located mainly on the trunk and proximal extremities (Figure 150.5). Cardiac features include valvular disease, pericarditis, myocarditis and congestive heart failure.

Figure 150.5 Erythema marginatum (rheumatic fever).
(Reproduced with permission of DermNet New Zealand Trust. http://www.dermnetnz.org/bacterial/rheumatic-fever.html. Last accessed April 2015.)
Miscellaneous
Coronary artery disease. Coronary artery disease and ischaemic heart disease may occur in premature ageing syndromes such as progeria and Werner syndrome; premature atherosclerotic vascular disease has also been reported in pseudoxanthoma elasticum [3]. Coronary artery disease may be associated with xanthelasma or xanthomas due to hyperlipidaemia [2]. The presence of a diagonal earlobe skin crease (Frank's sign) has been linked with coronary artery disease. This issue has been a matter of controversy over the years but current studies show a high positive correlation [16]. The coronary arteries are also involved in Kawasaki disease.
Skin problems related to cardiac pacemakers and implantable defibrillators. Cutaneous reactions over the site of implanted cardiac pacemakers have been reported. Most of these are either infections or mechanical problems (erosions, extrusions, capsular contracture, exposed generator or electrodes, bronchopleural cutaneous fistulae) and may respond to antibiotics or altered positioning of the pacemaker [17, 18]. Contact dermatitis from implanted cardiac rhythm devices is rare; allergy to cobalt, epoxy resin, mercury, nickel and titanium have all been described [19].
References
- Abdelmalek NF, Gerber TL, Menter A. Cardiocutaneous syndromes and associations. J Am Acad Dermatol 2002;46:161–83.
- Uliasz A, Lebwohl M. Cutaneous manifestations of cardiovascular diseases. Clin Dermatol 2008;26:243–54.
- O'Neill JL, Narahari S, Sane DC, et al. Cardiac manifestations of cutaneous disorders. J Am Acad Dermatol 2013;68:156–66.
- Sutkowska E, Gil J, Stembalska A, et al. Novel mutation in the FOXC2 gene in three generations of a family with lymphoedema-distichiasis syndrome. Gene 2012;498:96–9.
- Shetty Roy AN, Radin M, Sarabi D, et al. Familial recurrent atrial myxoma: Carney's complex. Clin Cardiol 2011;34:83–6.
- Dubrey SW, Falk RH. Diagnosis and management of cardiac sarcoidosis. Prog Cardiovasc Dis 2010;52:336–46.
- Lundberg IE. Cardiac involvement in autoimmune myositis and mixed connective tissue disease. Lupus 2005;14:708–12.
- Frostegård J. Systemic lupus erythematosus and cardiovascular disease. Lupus 2008;17:364–7.
- Hornberger LK, Al Rajaa N. Spectrum of cardiac involvement in neonatal lupus. Scand J Immunol 2010;72:189–97.
- Allanore Y, Meune C. Primary myocardial involvement in systemic sclerosis: evidence for a microvascular origin. Clin Exp Rheumatol 2010;28:S48–53.
- Tenedios F, Erkan D, Lockshin MD. Cardiac involvement in the antiphospholipid syndrome. Lupus 2005;14:691–6.
- Jennette JC. Overview of the 2012 revised International Chapel Hill Consensus Conference nomenclature of vasculitides. Clin Exp Nephrol 2013;17:603–6.
- Millet A, Pederzoli-Ribeil M, Guillevin L, et al. Antineutrophil cytoplasmic antibody-associated vasculitides: is it time to split up the group? Ann Rheum Dis 2013;72:1273–9.
- Kapoor P, Thenappan T, Singh E, et al. Cardiac amyloidosis: a practical approach to diagnosis and management. Am J Med 2011;124:1006–15.
- Hoen B, Duval X. Clinical practice. Infective endocarditis. N Engl J Med 2013;368:1425–33.
- Shmilovich H, Cheng VY, Rajani R, et al. Relation of diagonal ear lobe crease to the presence, extent, and severity of coronary artery disease determined by coronary computed tomography angiography. Am J Cardiol 2012;109:1283–7.
- Chua FS, Leininger BJ, Hamouda FA, Pifarre RF. Bronchopleural cutaneous fistula from infected pacemaker electrodes. Chest 1973;63:284–6.
- Har-Shai Y, Amikam S, Bolous M, Peled IJ. The management of soft tissue complications related to pacemaker implantations. J Cardiovasc Surg 1994;35(Suppl. 1):211–17.
- Kang J, Simpson CS, Campbell D, et al. Cardiac rhythm device contact dermatitis. Ann Noninvasive Electrocardiol 2013;18:79–83.