1 The Extraoral and Intraoral Soft Tissue Head and Neck Screening Examination
It is paramount that the dental clinician establish a repeatable, logical, sequentially organized, and systematic approach to screening the soft tissues of the head and neck region. It should be understood that this is not an “oral cancer screening,” since all abnormal conditions should be detected. Performing an oral cancer screening means looking for a single condition, cancer, at a single point in time; the dental clinician performs a complete exam, looking for all soft tissue abnormalities at a single point in time. There is no universally acknowledged step-by-step approach; therefore, the following is the one we adhere to and it can be modified as desired. The important point is, whatever sequence is established, it should be strictly adhered to each time to ensure that no step is omitted. A suggested ideal sequence of steps for a complete oral mucosal screening procedure of a new patient includes the following:
Introduction to the patient
Patient's chief complaint
History of the present illness
Medical (including social) and dental histories
Physical examination (to detect the site, morphology, and color of abnormalities)
Review of data and formulation of a clinical differential diagnosis
Additional clinical and laboratory tests ordered, as indicated
Final definitive diagnosis with a treatment/management plan formulated
Certainly, the clinician should establish a pleasant rapport with the patient so that excellent communication and trust are established. Often, the most critical or important piece of information a patient possesses does not get transmitted to the many forms filled out at the initial dental appointment. Once the patient's trust, confidence, and respect have been secured, the patient's chief complaint must be established. This can be a specific dental problem or a more generic goal such as “I need a checkup exam.”
If the patient voices a specific reason for the dental appointment, it is very important to gather as much subjective information from him or her as possible. The collective sets of subjective information are the patient's symptoms. Symptoms include descriptions such as pain, burning, dry mouth, soreness, swelling, roughness, and paresthesia. Whatever the symptom, its specific nature should be questioned, such as onset, duration, periodicity, nature or character, severity, and triggering factors or association. This information helps establish the history of the present illness. The clinician gathers a pocketful of diagnostic clues provided by the patient and combines them with the clinician's pathology knowledge to guide him or her to ask appropriate and insightful follow-up questions. Thus, the clinician acts as a detective and must possess foundational knowledge of head and neck disease and pathology in order to learn more about the patient and gather more clues for the formulation of a well-honed clinical differential diagnosis. Subsequent chapters of this book provide foundational knowledge—both general and specific—of the most common soft tissue head and neck pathology.
Following determination of the history of the patient's present illness, the medical history is reviewed with the patient. Typically, the patient has previously completed a detailed form providing the clinician with basic information about childhood diseases; vaccinations; hospitalizations and prior surgeries; any current medical care; date of the last physical examination; and medications (i.e., prescription and over-the-counter, including herbs) being taken or previously used, especially in the past 6 months. Details about the medications, including name, dosage, and duration of use, are recorded. A complete review of systems (e.g., cardiovascular, pulmonary, renal, endocrine, nervous system) is performed to gather more details than the initial “yes” or “no” responses. In addition, the medical history also includes the patient's psychological and socioeconomic profiles as well as social habits (e.g., tobacco and alcohol abuse).
Next, the dental history, including details of any oral habits, is gathered. It is important to note decayed, missing, and restored teeth as well as any active caries; periodontal disease; history of extractions and other oral surgery procedures; tooth vitality status; and any need for patient premedication. Any previous problems during dental care are discovered and discussed. Oral habits include the patient's technique and frequency of flossing, brushing, use of mouthrinse, and occlusal disharmonies.
Physical Examination
It is popular to compare the left and right side for bilateral symmetry while understanding that perfect symmetry is often not present within the range of normal. This is particularly important in order to visualize enlarged lymph nodes or parotid glands.
Extraoral Sites
Specific sites include the following:
Hair and facial skin
External eyes
External ears
Temporomandibular joints
Facial muscles
Nasal vestibule
Thyroid gland (anterior neck)
Lymph nodes (lateral and posterior neck, supraclavicular notch)
Parotid gland
Assess the hair for thickness and loss; carefully examine the sun-exposed facial skin for ultraviolet damage and lesion development, as well as the neck, ears, forehead, nasal bridge and alae, malar region, eyebrows/eyelids/eyelashes, vermilion of the lips, and the chin. Next, perform careful palpation of each of these sites to rule out the presence of deeper, mesenchymal and other types of tissue swellings.
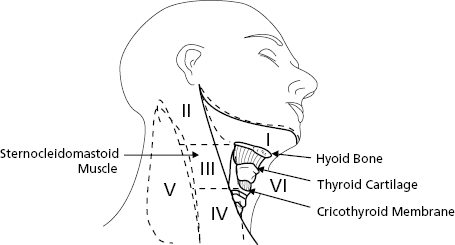
Palpate all lymph nodes and note any enlargement for additional testing since normal lymph nodes are soft and not palpable (Fig. 1.1). Specifically, the subcutaneous tissue is digitally kneaded with a rotating motion in the areas of lymph nodes based on the clinician's knowledge of anatomy. This process can begin in the submental area, below and lingual to the chin, against the mylohyoid muscles. Next, palpate the submandibular nodes by pressing the tissue below the jaw against the medial side of the mandible or by bimanual palpation with one finger in the mouth and the other externally pushing up. Next, palpate the parotid gland and its associated lymph nodes—look and feel anterior and posterior to the ear. Next, palpate the cervical lymph node chain. The posterior cervical chain is along the back of the neck, and the anterior and deep cervical chain is along the front. An anatomical landmark for the latter nodes is the sternocleidomastoid muscle—trace from behind the ear to the clavicle, kneading deep and medial to it. The postauricular and retrosternomastoid region should also be palpated along with the back of the neck. Lastly, palpate the thyroid gland by placing fingers gently over it and have the patient swallow. Sometimes, in order to discover an enlargement, the grouped fingers are placed on one side of the larynx and pushed laterally while palpating the opposite side.
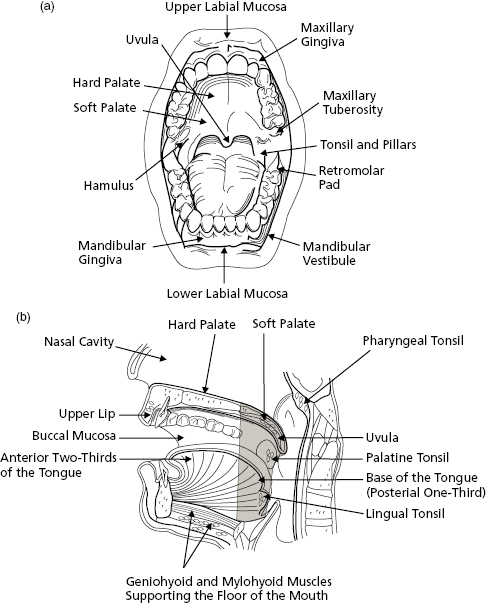
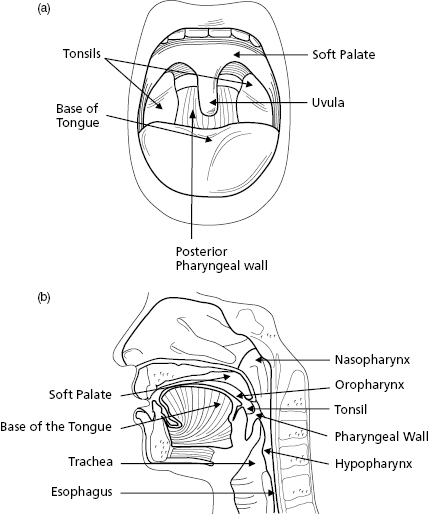
Figure 1.2 (a) Oral cavity proper, frontal view. (b) Major components forming the boundaries of the oral cavity proper, sagittal view. The oral cavity (unshaded area) is divided from the oropharynx (shaded area) anteriorly/posteriorly at the posterior extent of the anterior two-thirds of the tongue; the superior/inferior extent of the oral cavity is the hard palate and floor of mouth; the superior/inferior extent of the oropharynx is the nasopharynx and hypopharynx.Figure 1.3 Oropharynx. (a) Frontal view, (b) sagittal view.
It is recommended that the same examination sequence be followed each time, first by visual examination and then palpation. As mentioned previously, any sequence can be used as long as it is organized and there is understanding of the findings and the significance of deviations from normal. Palpation should be bimanual or bidigital and, whenever possible, by direct vision. The following is a detailed suggested descriptive narrative:
Lips—Have the patient slightly part his or her lips to examine the upper and lower vermilion borders and the left and right commissures. Then, with the patient's teeth occluded, evert both the upper and lower lips to expose the labial mucosa. Observe the maxillary frenum, which at times may exhibit a mucosal tag, a variation of normal. As the upper and lower labial mucosa become dry, observe the minor salivary glands and attempt to express mucin from them. While the lips are everted, the anterior maxillary and mandibular vestibules can be observed.
Labial and buccal mucosa/alveolar mucosa and attached gingiva/trigone—Slide your fingers posterior on the left and right buccal mucosa as well as the posterior portion of the vestibules. The parotid papilla overlying Stensen's duct should be of normal coloration. To verify function, dry it, and then have the patient's mouth wide open so that the cheek is stretched taut. Place four fingers flat on the face over the parotid gland in the preauricular area and milk the gland by using digital pressure to compress it against the masseter muscle or ramus area. Most patients exhibit a subtle white line at the occlusal plane of the buccal mucosa (i.e., linea alba), which is considered a variation of normal. While retracting the cheeks use mirror-assisted indirect vision to examine the tuberosity/hamular notch area and then, with direct vision, use the fingers and a mirror face to retract the buccal and labial mucosa, and observe the facial alveolar mucosa, mucogingival junction, attached gingiva, and free marginal gingiva on the maxilla and mandible as well as on the lingual mandible. Lastly, inspect and then palpate the retromolar pads and trigone area.
Hard palate—Examine its anterior portion, the rugae (firm folds), and then the posterior, which at times exhibits a subtle pink-white change due to slight amounts of extra keratin on the surface. Laterally, in the posterior hard palate area, many minor salivary glands (mucinous) are present and thus the palate can have a subtle pink-blue appearance. Often, the most posterior extent of the hard palate's midline has two small paired depressions, the fovea palatine.
Tongue—Gently hold the anterior tip with gauze and pull forward and to the left and right. While the tongue is in this position examine the lateral and ventral surfaces of the tongue, including the most posterior lateral extent which is occupied by foliate papillae. The anterior two-thirds of the dorsum should demonstrate filiform papillae, and often there is a mild white coating caused by slough of the keratin from the filiform papillae. Note, among the filiform papillae, the larger and fewer dome-shaped fungiform papillae. At the junction with the posterior one-third, the dorsal surface exhibits an upside-down “V” linear series of circumvallate papillae. After freeing the tongue, instruct the patient to protrude the tongue, move it left and right, and touch the hard palate with its tip. In this way, the tongue's full mobility is confirmed and the latter movement enables further inspection of the tongue's ventral surface.
Floor of mouth—Examine the anterior portion with its left and right sublingual plicae (V-shaped caruncula with its vertex toward the face), which contain the opening of the sublingual glands. At the most anterior extent of the plicae, there are raised areas that possess the opening of the submandibular glands (i.e., Wharton's duct). The posterior portion of the floor is also examined. Palpate both the sublingual and submandibular glands by supporting the external chin with one hand and extending a finger downward in the floor of the mouth. To test salivary flow, dry the lingual carunculae, and then place one or two outstretched fingers under the chin and alongside the inferior mandible. Upward pressure directed to the submandibular gland area should produce saliva from Wharton's duct orifice.
Oropharynx—With the patient's mouth wide open, and using a tongue depressor, ask the patient to say “ah”; at this point the vibrating line (i.e., where the palatal bone ends) at the beginning of the soft palate moves and, centrally and posteriorly, the pendulous uvula should be present. In this area, a circular distribution of lymphoid tissue is present, Waldeyer's ring, which includes the palatine tonsils, lingual tonsils (intermixed with the foliate papillae), and scattered focal collections of lymphoid tissue on the pharyngeal wall, as well as on the posterior soft palate and floor of mouth. Visualize all aspects of the oropharynx, especially the posterior pharyngeal wall. The latter is particularly difficult to visualize in some patients and the adenoids and base of the tongue cannot be seen by direct or indirect vision with standard dental equipment. Particular attention should be paid to the tonsillar pillars (i.e., palatoglossal and palatopharyngeal folds) and tonsillar tissue fossa area. Lastly, examine the posterior wall of the oropharynx, taking note of any normal aggregates of lymphoid tissue.
Note: In patients who have undergone a tonsillectomy there is some residual tonsillar tissue as well as a whitish scar tissue at the site of the surgery.
Adjunctive Diagnostic Examination Methods and Devices
There has been a renewed interest in a more consistent and thorough head and neck soft tissue examination, particularly in an effort to detect potentially malignant lesions at an earlier stage of development. Unfortunately, this has led to the misnomer of performing an “oral cancer screening examination” and many dental manufacturers have developed and marketed various devices in order to provide the clinician a purported “enhanced” screening method in addition to the conventional white-light and palpation method just described. No scientific studies to date have proven that these methods or devices improve detection of any type of oral mucosal disease.1–5 Four categories of devices have been marketed: cytology, enhanced reflectance, narrowband imaging (autofluorescence), and saliva sampling.
Exfoliative Cytology
In the early 1950s the Pap smear was introduced in order to screen the cervical mucosa for earlier detection of cervical cancer. The technique was soon investigated by dental researchers for a possible similar use with oral mucosa; however, it was soon discovered that physically scraping the oral mucosa's upper-level epithelial cells and subsequently transferring them to a glass slide, stained and cover-slipped, resulted in an unacceptable number of false positives and false negatives. The crux of the matter is that, within the oral cavity, an inflammatory component often resides in the epithelium (i.e., inflammatory exocytosis) that causes keratinocytes to appear atypical due to a reactive change induced by the omnipresent inflammation; these atypical cells are then incorrectly interpreted as representing potentially malignant dysplasia—an abnormal maturation pattern of the stratified squamous epithelium.
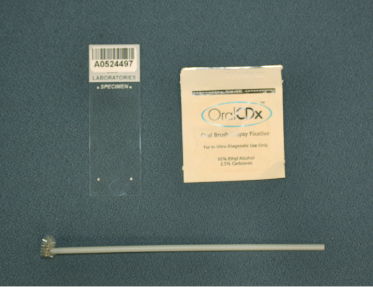
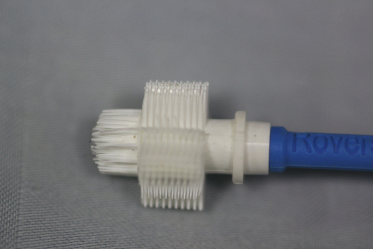
In 1999, a new version of oral cytology, Oral CDx's “brush biopsy” (marketed in dentistry as the BrushTest), was marketed in the United States by Oral Scan Laboratories (Suffern, NY).6 The dentist, a generalist or specialist, purchases the company's cytology kit, which contains bar-coded patient information forms and a patented nylon bristle brush designed to harvest an oral transepithelial specimen of disaggregated cells (Fig. 1.4, Fig. 1.5). Chairside, the clinician subsequently spreads these cells by brushing on a supplied bar-coded microscope slide. The cytology specimen is then immediately fixed with alcohol and sent, in a prepaid mailer, to the company's laboratory. A neural-net software program optically screens the slide specimen for atypical or malignant-appearing cells. Atypical cells are captured as digital images and reviewed by a cytopathologist who then issues a pathology report in one of three categories—normal, atypical, or malignant cells. If atypical or malignant cells are reported, then a mandatory gold-standard diagnostic tissue biopsy is recommended to obtain a definitive diagnosis. According to the company's information, lesions to be sampled include innocuous (i.e., unsuspicious) looking red or white “spots” within the oral cavity; in other words, lesions of the surface oral mucosa a clinician does not feel could be squamous cell carcinoma or potentially malignant (premalignant) lesions. Clinically suspicious lesions (e.g., erythroplakia in a high-risk site) are not an indication for the brush biopsy; rather, if that type of lesion has persisted for more than 14 days, then an incisional surgical tissue biopsy must be performed. Since it was introduced, the validity and positive predictive value of this cytology procedure have been challenged by some investigators and promoted by others.7–10 In addition, other companies in other countries (Second Step Laboratory Services—Perceptronix Medical Inc., Laboratories, Vancouver, BC, Canada) have offered similar morphological cytology tests with a different nylon bristle cytology brush (Rovers Medical Devices, The Netherlands; Fig. 1.6) and they also include DNA ploidy results.
Figure 1.4 A brush biopsy (cytology) kit as supplied by Oral CDx (Oral Scan Laboratories, Suffern, NY).Figure 1.5 A close-up view of the Oral CDx proprietary brush biopsy nylon cellular collection device.Figure 1.6 A close-up view of the Rovers cellular collection device (Rovers Medical Devices, The Netherlands).
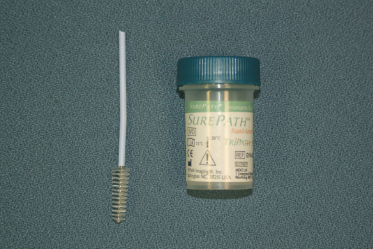
More recently, a cytobrush technique involving liquid fixative has been introduced not only in hospitals and physician offices but also in some oral pathology laboratories. In this cytology technique, a nylon bristle cytology brush developed for gynecological ectocervical and endocervical scrapings is used to obtain a full-thickness epithelium specimen from the oral or oropharyngeal mucosal surface (clinically indicated by pinpoint bleeding spots as seen with the BrushTest), but instead of the clinician then smearing the harvested cells (i.e., keratinocytes) directly onto a glass slide (frosted or clear type), the bristle end of the brush is immersed directly into an alcohol-based fixative for transport to the oral pathology laboratory (Fig. 1.7). At the laboratory, the harvested cells in the fixative and retained on the brush's bristles are collected and then segregated from the debris and inflammatory cells in the fixative by being placed in one of several competing manufacturers' processing machines. The harvested cells are affixed in a monolayer to the slide in a confined area, are stained and cover-slipped, and then are examined by the pathologist for cellular atypia, fungal hyphae (i.e., superficial candidiasis), or herpes-family cytopathogenic change.
Figure 1.7 A liquid cytology kit composed of an alcohol-based fixative transport medium and gynecological-type nylon cellular collection device.
Tissue Reflectance
In the early 2000s, Zila Pharmaceuticals (Division of Tolmar Corporation, Phoenix, AZ) introduced a single-use, disposable chemiluminescent screening device, Vizilite®, for early detection of leukoplakia. This FDA-cleared 501(k) medical device is based on a similar device (i.e., Speculite®) used by physicians for uterine cervical screening (Pap smear) to rule out early, potentially malignant microscopic change (i.e., cervical dysplasia). Subsequently, two other companies marketed similar devices, Microlux/DL (AdDent, Inc., Danbury, CT; Fig. 1.8) and Orascoptic DK (Kerr Corporation, Middleton, WI).11 After undergoing a conventional exam and agreeing to this additional test, the patient rinses his or her mouth for 30 seconds with, and then expectorates, a raspberry-flavored 2% acetic acid solution, which acts as a drying (desiccant) agent. Then a light stick is chemically activated that produces a diffuse, blue-white light (wavelength range 430–455 nanometers). As in the uterine cervix, the light is intended to highlight any subtle oral leukoplakias that may have been missed by the clinician during the previous conventional white-light soft tissue examination. A positive lesion is termed “acetowhite” and may indicate the need for invasive tissue biopsy. As with oral cytology screening, some investigators have found the specificity and sensitivity, as well as the positive predictive value, of this test is not sufficient enough for clinical use. False positives are due to increased DNA seen in reactive, atypical cells secondary to the concomitant and ubiquitous inflammation of the oral cavity.
A few years after the advent of Vizilite, Zila Pharmaceuticals gained FDA clearance to market Vizilite Plus® (Fig. 1.9). With this system, following a conventional light examination and the use of the Vizilite reflectance device, an additional marking step can be performed; it is not a standalone step. The marker is a large cotton swab of pharmaceutical-grade tolonium chloride (toluidine blue), marketed as TBlue630 (the numerical portion of the dye's trademark name represents the nanometer wavelength of the chemiluminescent blue-white light). Toluidine blue is a metachromatic dye with an affinity for DNA and can be used by the clinician to stain and subsequently photodocument a previously identified acetowhite lesion.12, 13
Figure 1.9 Vizilite Plus (Zila Pharmaceuticals, Division of Tolmar Corporation, Phoenix, AZ) oral mucosa reflectance adjunctive light-emitting diagnostic device with second-step marker system of trademarked toluidine blue.
Narrowband Imaging (Autofluorescence)
Late in the first decade of the 2000s a new type of adjunctive screening device began to be marketed, predicated on the FDA 501(k) medical device clearance granted Vizilite. Current examples include the VELscope Vx® (L.E.D. Dental, Inc., White Rock, BC, Canada; Fig. 1.10), Sapphire Plus® LD (DenMat Holdings, LLC), Identafi (StarDental, DentalEZ Group, Inc., Malvern, PA; Fig. 1.11), and DentLight D.O.E.™ Oral Exam System (DentLight, Inc., Richardson, TX; Fig. 1.12). Each uses the principle of tissue fluorescence as opposed to tissue reflectance.14–16
Figure 1.10 Narrowband emission autofluorescence VELscope Vx (L.E.D. Dental, Inc., White Rock, BC, Canada).Figure 1.11 Narrowband emission (autofluorescence and vascular evaluation) and white-light emission Trimira Identifi (StarDental, DentalEZ Group, Inc., Malvern, PA).Figure 1.12 Narrowband emission DentLight D.O.E. autofluorescence oral exam system (DentLight, Inc., Richardson, TX).
Normal oral mucosa, both surface epithelium and the underlying lamina propria's connective tissue, contain cellular structures—chromophores—that are involved in normal biochemical reduction–oxidation reactions (e.g., NADH and FADH). These chemical reactions cause a pale green wavelength emission that cannot be seen with the naked eye under normal lighting conditions since it is extremely faint and overwhelmed by the absorbance, reflectance, and scattering of white light within the oral cavity. The VELscope and the similar devices just mentioned use light-emitting diodes (LEDs) to produce a narrow band of blue or violet (Identafi) wavelength light that stimulates the chromophore-related green autofluorescence. Through a series of filters either contained within the machine or worn by the clinician, all other wavelengths of white light are eliminated so that normal oral mucosal tissue appears green and an area of mucosa with loss of fluorescence indicates a loss of chromophores. The latter could indicate mucosal pathology including the presence of epithelial dysplasia. Thus, narrowband emitting lights can be used in formulating a clinical differential diagnosis of mucosal pathology that has already been examined by white light. It is very important to understand that these devices are not diagnostic but, at best, adjunctive clinical information that can be used by the knowledgeable clinician. A prerequisite for the adjunctive use of narrowband reflectance is the knowledge of oral mucosal conditions that can provide a false positive or a false negative result. Once a mucosal lesion is detected by white light and loss of fluorescence is demonstrated by one of these devices, the patient should return in two weeks to confirm the lesion's persistence. If the lesion persists, then an incisional biopsy should be performed in order to provide the patient with an accurate definitive diagnosis and subsequent treatment based on that diagnosis.
Saliva Samples
There are two commercially available tests that claim to be helpful to the clinician in deciding whether to assign a patient over the age of 18 into a low-risk or high-risk group with respect to the development of oral cancer and, although unstated, specifically squamous cell carcinoma. It is very important to understand that, as of 2013, these tests do not have any research study results in peer-reviewed publications that confirm their reliability and validity and that both possess some “fatal flaws” with regard to their marketing claims about the detection or risk of development of oral cavity and oropharyngeal squamous cell carcinoma.17
The first test, OraRisk HPV (OralDNA Labs, Inc., Brentwood, TN) analyzes a resting saliva sample by polymerase chain reaction (PCR) to determine if human papilloma virus (HPV) type 16 is present in the patient's oral saliva. HPV16 is well known to cause uterine cervix squamous cell carcinoma (as well as vaginal and anal) as well as some cases of male anal and penile squamous cell carcinoma. It is a sexually transmitted DNA virus that persists within the mucosa's surface epithelium for years and may eventually invade the basal layer cells with possible integration into the host cell's DNA. If this sequence of cellular events occurs, the rate-controlling genes of the normal cell cycle undergo mutation and this results in cancerous growth.
The OraRisk manufacturer has established a proposed follow-up protocol for a patient who initially tests positive for HPV16 in their saliva. Unfortunately, too little is known about the association of HPV and oropharyngeal cancer of the base of tongue and tonsils as well as its life cycle in the oropharynx to know what a positive HPV16 saliva sample means. The presence of HPV in a person's saliva does not necessarily indicate infection much less cellular invasion or DNA integration, and in cervical mucosa over 90% of HPV16 infections subsequently clear on their own. Additionally, it is very important to know that none of the preceding has been proven to be a cause–effect relationship for oral cavity squamous cell carcinoma, which includes the known high-risk sites of lateral and ventral tongue as well as floor of mouth. Epidemiological studies to date indicate HPV16-related squamous cell carcinomas are overwhelmingly located in the oropharynx, much of which is not visible during the course of a general dentistry examination.
The other saliva test recently made available in the United States (except pending in New York State) is a saliva biomarker test (Advanced Laboratory Services, Sharon Hill, PA). The test claims to successfully screen for three biomarkers associated with oral squamous cell carcinoma. Since the company is based in Pennsylvania the medical practitioner ordering the test must be on that state's approved list, which includes a degree of MD, DO, CRNP, PA-C, and Certified Nurse Midwife but not a DDS or DMD. If an oral lesion deemed suspicious for oral squamous cell carcinoma is discovered, then 5 mL of resting saliva is obtained from the patient and placed in a testing tube that is submitted to the company. The PCR test initially screens for interleukin type 8 (IL-8). If the test is positive, then the person is considered to be in a high-risk group and a second PCR analysis for biomarkers IL-6 and IL-1 alpha is performed. If those biomarkers are also present, then the patient is referred for biopsy of the oral lesion; if negative, then the patient is put under increased oral cavity monitoring. Unfortunately, the three biomarkers screened for in this test are also seen in all types of inflammation within the oral cavity and thus their sensitivity, specificity, and positive predictive values are poor. Furthermore, if this test is employed as a screening test (i.e., all adult patients), where would one biopsy if the three biomarker levels are higher than the company's reference levels but no oral lesion is visible? The company's brochure and Web site claim the biomarker levels are also indicative of oral salivary gland cancer (i.e., adenocarcinoma) but there are no peer-reviewed references listed that support that claim.
Research is also being conducted on various salivary biomarkers, including using direct saliva transcriptome analysis or solcd44 levels as a possible screening tool for head and neck squamous cell carcinoma.18–20
Conclusion
The adjunctive oral mucosa pathology screening aids described in this chapter could possibly provide some additional information in the diagnostic and decision-making process, but they do not provide a diagnosis and are only to be performed after a routine conventional head and neck extraoral and intraoral examination has been completed. The latter examination under bright white light, with palpation, remains the highest standard in patient care.
The following chapters of this book are intended not only to aid the dentist in proper examination and documentation of detected oral and oropharyngeal (and possible facial skin) pathology but also to enhance differential diagnosis skills and aid in the decision of whether to observe, refer, or biopsy the lesion.
2. Lingen MW, Kalmar JR, Karrison T, Speight PM. Critical evaluation of diagnostic aids for the detection of oral cancer. Oral Oncol 2007. DOI: 10.1016/j.oraloncology.2007.06.011.
3. Patton LL, Epstein JB, Kerr AR. Adjunctive techniques for oral cancer examination and lesion diagnosis: a systematic review of the literature. JADA 2008;139:896–905.
4. Rethman MP, Carpenter W, Coehn EEW, et al. Evidence-based clinical recommendations regarding screening for oral squamous cell carcinomas. JADA 2010;141(5):509–520.
5. Siegel MA, Kahn MA, Palazzolo M. Oral cancer: a prosthodontics diagnosis. J Prosthodontics 2009;18:3–10.
6. Sciubba JJ. Improving detection of precancerous and cancerous oral lesions: computer-assisted analysis of the oral brush biopsy. JADA 199;130:1445–1457.
7. Bhoopathi V, Kabani S, Mascarenhas AK. Low positive predictive value of the oral brush biopsy in detecting dysplastic oral lesions. Cancer 2009;115:1036–1040.
8. Mehotra R, Mishra S, Singh M, Singh M. The efficacy of oral brush biopsy with computer-assisted analysis in identifying precancerous and cancerous lesions. Head and Neck Oncology 2011;3:39.
9. Reddy SG, Kanala S, Chigurupati A, et al. The sensitivity and specificity of computerized brush biopsy and scalpel biopsy in diagnosing oral premalignant lesions: a comparative study. J Oral Maxillofac Pathol 2012;16:349–353.
10. Svirksy JA, Burns JC, Carpenter WM, et al. Comparison of computer-assisted brush biopsy results with follow up scalpel biopsy and histology. Gen Dent 2002;50:500.
11. McIntosh L, McCullough MJ, Farah CS. The assessment of diffused light illumination and acetic acid rinse (Microlux/DL) in the visualization of oral mucosal lesions. Oral Oncology 2009;45:e227–e231.
12. Arwan KH, Yang YH, Morgan PR, Warnakulasuriya S. Utility of toluidine blue as a diagnostic adjunct in the detection of potentially malignant disorders of the oral cavity—a clinical and histological assessment. Oral Diseases 2012;18:728–733.
13. Ujaoney S, Motwani MB, Degwekar S, et al. Evaluation of chemiluminescence, toluidine blue and histopathology for detection of high risk oral precancerous lesions: a cross-sectional study. BMC Clin Pathol 2012;12.
14. Jayaprakash V, Sullivan M, Merzianu M, et al. Autofluorescence-guided surveillance for oral cancer. Cancer Prev Res 2009;2(11):966–974.
15. Lane PM, Whitehead TGP, Zeng H. Simple device for the direct visualization of oral-cavity tissue fluorescence. J Biomedical Optics 2006;11(2):024006-1–7.
16. Poh CF, Ng SP, Williams PM, et al. Direct fluorescence visualization of clinically occult high-risk oral premalignant disease using a simple hand-held device. Head and Neck Pathology 2006:28. Available at: http://www3.interscience.wiley.com/cgi-bin/jissue/89011929 (accessed November 2, 2006).
17. Lingen MW. Can saliva-based HPV tests establish cancer risk and guide patient management? Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol 2010;110:273–274.
19. Franzmann EJ, Reategui EP, Pereira LHM, et al. Salivary protein and solcd44 levels as a potential screening tool for early detection of head and neck squamous cell carcinoma. Head and Neck. DOI: 10.1002jhed.21810.
20. Lee YH, Zhou H, Reiss JK, et al. Direct saliva transcriptome analysis. Clin Chem 2011;57(9):1295–1302.
Recommended Reading
Cawson RA, Binnie WH, Barret AW, Wright JM. Oral Disease, 3rd edition. St. Louis, MO: Mosby; 2001.