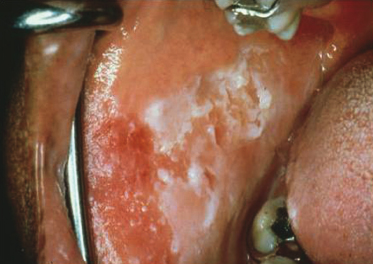
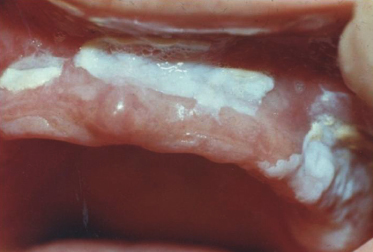
A 38-year-old woman has three children and is in the process of divorce from an abusive husband. She takes Ambien to help her sleep at night and is very concerned about the bilateral, superficial “peeling” of this roughened, ragged, and thickened plaque area of her right cheek. When the patient responded negatively to a series of questions regarding habits and application of materials to the area, a biopsy was done. What is the diagnosis?
Candidiasis
Leukoedema
White sponge nevus
Morsicatio buccarum
Case 2
A 2-month-old bottle-fed baby has had this oral condition since shortly after birth, although she feeds well and is gaining weight normally. She lives in a rural community without access to a pediatrician. These lesions wipe away, leaving an erythematous base. What is the diagnosis?
Candidiasis
Diphtheria
White sponge nevus
Hairy leukoplakia
Case 3
A 29-year-old schizophrenic man is living in a homeless shelter. He presents with severe pain in the lower left mandible and deep recurrent caries in tooth #18. What would not be an appropriate process to list in the differential diagnosis of this lesion?
Chemical trauma
Leukoedema
Morsicatio buccarum
Tobacco pouch keratosis
Case 4
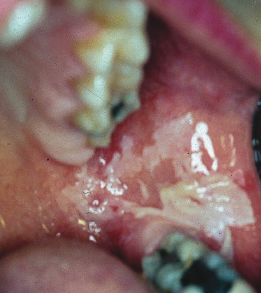
A 57-year-old widower confides to you that he believes he has halitosis. He has recently noticed that the “lining of his cheeks seems to be peeling.” The appearance combined with the history fits what most likely diagnosis?
Leukoedema
Lichen planus
Chemical reaction to mouthwash
Uremic stomatitis
Case 5
This 62-year-old man smokes one pack of cigarettes a day. This lesion was discovered on a routine new patient examination; he had not been aware of it and did not know how long it was present. Based on the information given and the clinical photograph, what is the best diagnosis for this lesion?
Morsicatio
Leukoplakia
Squamous cell carcinoma
Hairy leukoplakia
Case 6
A 55-year-old woman is troubled by a burning sensation on the tip of her tongue. She is convinced that the appearance of her tongue has changed from the previous pink color. What is the white layer seen on the dorsum of this coated tongue?
Desquamated epithelial cells and bacteria
Cells from white sponge nevus
Necrosis from a chemical burn
Hyperkeratosis
Case 7
A 46-year-old man was a professional baseball player in his youth. He admits to drinking a 6-pack of beer and use of tobacco products every day. If the histology from a biopsy of this area showed only excess keratin, what would the clinical diagnosis be?
Leukoedema
Hyperplastic candidiasis
Tobacco pouch keratosis
Lichen planus
Case 8
A 35-year-old man is obese and takes lisinopril for hypertension. The observed changes are bilateral and asymptomatic. What is the likely clinical diagnosis of the lesions seen in this case?
Tobacco pouch keratosis
Pseudomembranous candidiasis
Nicotine stomatitis
Leukoedema
Case 9
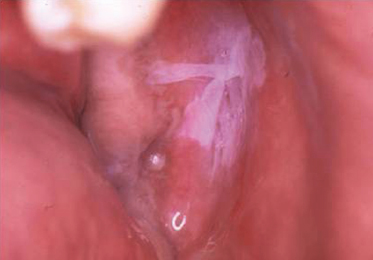
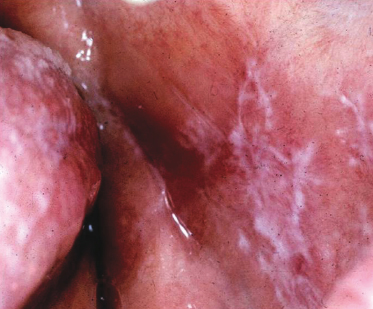
This 48-year-old man complains of roughness on the inside of both of his cheeks. He claims that this has been present for about 6 months although it is asymptomatic. The clinical photograph and history strongly suggest lichen planus; what are the lines on the buccal mucosa called?
Wickham's striae
Lines of Zahn
Lines of Retzius
Koebner's striae
Case 10
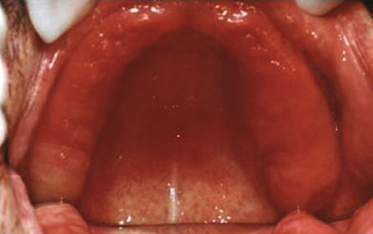
A retired 72-year-old man has smoked three packs of cigarettes a day for 30 years. He has severe periodontal disease but, on questioning, did not know about any changes in his oral tissues. What is the clinical diagnosis given to this condition?
Leukoplakia
Hyperkeratosis with dysplasia
Nicotine stomatitis
Lichen planus
Case 11
A 60-year-old woman has worn complete upper and lower dentures for 20 years. She has chronic obstructive pulmonary disease (COPD) and recently completed a course of antibiotics to treat bacterial pneumonia. This is an example of pseudomembranous candidiasis. What in the history is not a typical factor for the development of the disease?
Age of 60
History of COPD
Denture wear
Antibiotic use
Case 12
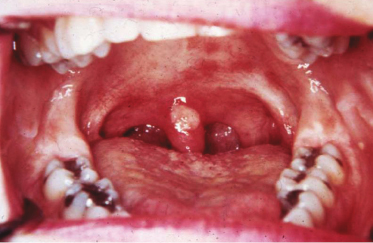
This 39-year-old man exhibits these changes bilaterally. On questioning about his social history he admits to being bisexual although he has never been tested for HIV. If you wanted to evaluate this person for hairy leukoplakia, what would be diagnostic?
HIV testing
Biopsy with stains for Epstein–Barr virus
The lesions should wipe away with gauze
Historical information about other family members with a similar condition
Red, Red-and-White, and Purpuric Lesions
Case 13-1
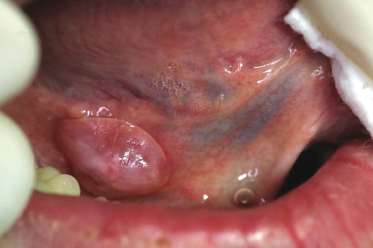
A young adult has been aware of this lesion for years and it has remained the same size. The blanchable and compressible lesion is not painful. What is the most likely provisional diagnosis of this lesion?
Erythema migrans
Erythematous candidiasis
Erythroplakia
Hemangioma
Case 13-2
A hemangioma is considered:
Neoplastic
Developmental
Inflammatory
Reactive
Case 14-1
A 25-year-old woman has noticed this unilateral change for the past few months. The area is asymptomatic and cannot be wiped off. Each of the following would be a reasonable differential diagnosis for this lesion except one. Which one is the exception?
Cinnamon allergic reaction
Acute candidiasis
Lupus erythematosus
Cheek nibbling
Case 14-2
Which of the following is the most likely provisional diagnosis?
Lichen planus
Cinnamon allergic reaction
Thermal burn
White sponge nevus
Case 15-1
A 59-year-old man is noted to have this lower lip appearance during his routine dental cleaning appointment. None of the roughened area is removable. Based on the history and site, morphology, and color of the lesion, its provisional diagnosis is which of the following?
Lichen planus
Verruciform xanthoma
Actinic cheilitis
Candidiasis
Case 15-2
Which is true about actinic cheilitis?
Lesion often oozes a mucous secretion.
Actinic cheilitis is more common on the upper lip.
Precancerous changes are reversible.
A significant percentage of lesions are premalignant.
Case 16-1
A dental student is aware of this lesion that “comes and goes.” When present, the area tends to change shape from day to day. Which of the following is the most likely diagnosis?
Traumatic erythema
Erythema migrans
Erythroleukoplakia
Nicotine stomatitis
Case 16-2
Which condition is statistically associated with geographic tongue?
Candidiasis
Erosive lichen planus
Psoriasis
Fissured tongue
Case 17-1
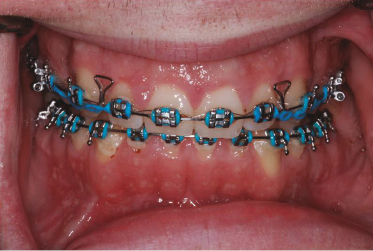
A 16-year-old girl taking phenytoin complains of fatigue, weight loss, low-grade fever, spontaneous gingival hemorrhage, and this gingival change. What part of the history is not consistent with drug-induced gingival hyperplasia?
Anterior facial involvement
Erythema
Excess attached gingiva
Spontaneous gingival hemorrhage
Case 17-2
Which is the most likely provisional diagnosis?
Leukemia
Infectious mononucleosis
Scarlet fever
Hereditary hemorrhagic telangiectasia
Case 18-1
A 50-year-old man has had this chronic sore for the past year. It occasionally bleeds and is intermittently sore. What is the most likely provisional diagnosis?
Hemangioma
Lichen planus
Actinic cheilitis (cheilosis)
Angular cheilitis
Case 18-2
In addition to candidiasis, what is another cause of angular cheilitis?
Vitamin deficiency
Developmental defect
Viral infection
Protozoan infection
Case 19
A 55-year-old woman has had asymptomatic bilateral and symmetrical lesions for the past several years. Recently, some focal pain has occurred. The areas “feel rough” to the patient when rubbed with the tip of her tongue. Once a provisional diagnosis is made based on this lesion's site, morphology, color, and history what is the next step in management of this condition?
Topical steroid application
Biopsy of left and right lesions
Cytology to rule out malignancy
Antifungal medication
Case 20
A denture patient is unaware of this lesion. What is the proper management of this condition?
Treat both the denture and oral mucosa with antifungal agents.
Leave the denture out at night, clean it, and rinse it in an antifungal solution.
Use laser ablation followed by new denture construction.
Apply antifungal cream to the affected oral soft tissues.
Acute Oral Ulcerations
Case 21
A 36-year-old woman has an asymptomatic lesion of 1 week's duration; no other signs or symptoms were seen. Spontaneous healing occurred after 2 weeks. The patient has a history of recurrent aphthous ulcers but does not recall having lip lesions. What finding in the history suggests that this lesion is not an aphthous ulcer?
Patient's age
Asymptomatic lesion
Healed spontaneously in 2 weeks
Site
Case 22
A 20-year-old woman has an acute onset of painful ragged ulcerations of the movable mucosa accompanied by fever and malaise. The patient also gives a history of “cold sores” that occur several times per year on her lip. The history of painful acute-onset ulcers of the movable mucosa favors what diagnosis?
Erythema multiforme
Aphthous ulcers
Herpes simplex
Varicella
Case 23
A patient has had recurrent painful bouts of oral mucosal ulcerations of greater than 1 year's duration. Each episode of lesions resolves in approximately 10 days. Similar cutaneous lesions were seen at one time and were treated with steroids and antibiotics, resulting in resolution. What is the triad of signs and symptoms seen in Behcet's syndrome?
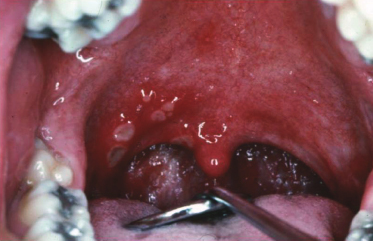
A 16-year-old boy had soft palate ulcerations derived from ruptured vesicles. The ulcers were mildly tender and accompanied by a sore throat. The lesions resolved in 1 week. No prior history of a blistering or ulcerative disease was given. What is the most likely diagnosis for these lesions?
Herpangina
Herpes simplex
Recurrent aphthae
Syphilis
Case 25
Painful, often multiple, deep ulcerations of a cyclical nature, corresponding to her menstrual cycle, began in this 16-year-old girl. No treatment has been effective. Behcet's disease, cyclic neutropenia, Crohn's disease, and Sweet's syndrome all have oral lesions that can be identical to what?
Herpangina
Recurrent aphthous ulcers
Erythema multiforme
Pemphigus vulgaris
Case 26
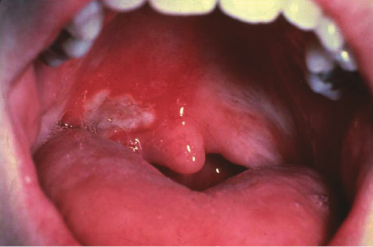
An 8-year-old girl was seen by her physician for a complaint of fever, malaise, and sore throat. During the exam this ulceration was found. The lesion was asymptomatic and thus the patient was unaware of its presence. If this lesion were an initial finding for primary varicella zoster (i.e., chicken pox) what is likely to follow?
Painful ocular inflammation
Gingivostomatitis
Necrosis of the interdental papillae
Vesicular skin lesions
Case 27
A 38-year-old woman complains of almost constant painful crops of small ulcerations of the oral mucosa not preceded by vesicles. Individual ulcers heal within 2 weeks but are almost immediately replaced by new similar-appearing lesions. She reports that she is in otherwise good health with no concurrent skin lesions. What is the likely diagnosis for these lesions?
Herpetiform aphthae
Herpes simplex
Herpes zoster
Chicken pox
Case 28
A 25-year-old man is seen because of a painful swelling on his hard palate. It has been present for about a week and the pain worsens when eating rough foods such as potato chips. Upon intraoral examination, ulceration is seen in the area of the swelling. Which would not be part of a reasonable differential diagnosis?
Recurrent aphthous ulcer
Necrotizing sialometaplasia
Superficial mucocele
Wegener's granulomatosis
Chronic Vesiculoerosive and Ulcerative Lesions
Case 29
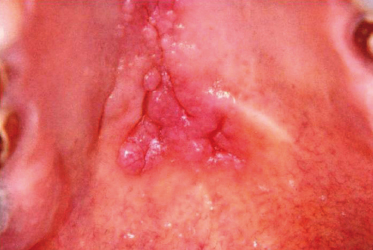
An 18-year-old boy with mandibular alveolar mucosa papules has similar lesions on the buccal mucosa and palate. His medical and social histories are noncontributory; however, on the review of systems he mentions some recent episodes of intestinal cramping and diarrhea. Although these lesions do not look ulcerative, the history should make you suspect what condition?
Wegener's granulomatosis
Noma
Erosive lichen planus
Pyostomatitis vegetans
Case 30
A 62-year-old woman complains that for the last 2 years she has been unable to eat spicy foods and finds it painful to perform good oral hygiene. Upon head and neck examination, it is noticed that she has conjunctival inflammation. The clinical appearance is that of desquamative gingivitis. The presence of eye involvement should make you suspect what disease?
Mucous membrane pemphigoid
Erosive lichen planus
Erythema multiforme (Stevens–Johnson syndrome)
Herpes zoster
Case 31
A 54-year-old man presents with an area that has been tender for 3 months. He is in good health, drinks red wine with dinner about 3 times per week, and has never used tobacco. A nonhealing ulcer on the lateral tongue should make you think of all of these choices except which one?
Squamous cell carcinoma
Deep fungal infection
Mucous membrane pemphigoid
Traumatic granuloma
Case 32
This 62-year-old man emigrated from Guatemala 10 years ago. He has no health insurance and resisted going to the hospital until he began feeling deep fatigue and episodes of epistaxis. The patient in this case eventually died of his disease despite aggressive chemotherapy. He had no other known risk factors such as diabetes mellitus, and his immune status was intact. What is the likely diagnosis?
Behcet's syndrome
Midline lethal granuloma
Tertiary syphilis
Wegener's granulomatosis
Case 33
A 61-year-old man experiences tenderness of the buccal mucosa that comes and goes. He changed to a mild children's dentifrice and stopped using mouthwash, but the lesions persisted. These lesions of lichen planus can easily be confused with a lichenoid hypersensitivity response. What clinical sign does not help to distinguish that this is lichen planus?
Lesions are bilateral
Lesions come and go
White striae
Ulceration
Case 34
A 54-year old man has had continuous, very painful mouth sores for approximately 7 months. The only time the sores remitted was when he was given high dose methylprednisolone for a bowel condition 2 months ago. The patient has pemphigus vulgaris. What will help to confirm the disease besides histopathology?
Presence of rheumatoid factor
Presence of antinuclear antibodies
Positive Nikolsky sign
Direct and indirect immunofluorescence studies
Case 35
A 38-year-old man bit his tongue 4 weeks ago and is concerned because it has not healed. Since most oral ulcerations resolve in 2 weeks a biopsy was taken from this patient. When the patient returned for a follow-up visit the next week the lesion was almost completely resolved. What is the likely diagnosis?
Traumatic ulcerative granuloma
Deep fungal infection
Squamous cell carcinoma
Erythema multiforme
Case 36
This 72-year-old edentulous man does not wear dentures. He has smoked cigarettes and used alcohol his entire adult life. He complained of a “raised” lesion on the left lateral tongue. This asymptomatic lesion was found on oral examination. The site and lack of symptoms should make what diagnosis the primary consideration in your differential diagnosis?
Recurrent herpes
Traumatic ulcer
Noma
Squamous cell carcinoma
Papillary Lesions
Case 37-1
An HIV-positive male is unaware of this tongue lesion and, thus, duration is unknown. What is the most likely provisional diagnosis of this lesion?
Verruca vulgaris
Hairy tongue
Squamous papilloma
Hairy leukoplakia
Case 37-2
If a biopsy of suspected hairy leukoplakia is taken, the confirmatory microscopic features should demonstrate evidence of the following:
Human papillomavirus
Epstein–Barr virus (EBV)
Human immunodeficiency virus
Herpes simplex virus
Case 38-1
A 41-year-old man has this firm, nonpainful, pedunculated palatal lesion of 1 year's duration. What is the least likely clinical diagnosis?
Verruca vulgaris
Squamous papilloma
Verrucous carcinoma
Verruciform xanthoma
Case 38-2
What clinical clue is not present in the current history that could aid in a provisional diagnosis of verrucous carcinoma?
Rapid onset
Pain
Smokeless tobacco habit
Compressible
Case 39-1
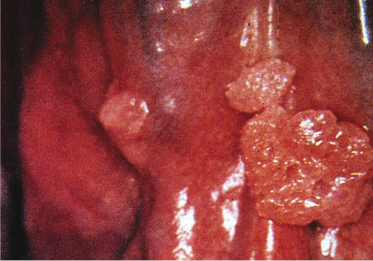
A 51-year-old man is seen in the emergency clinic with this large gingival mass of 8 months' duration. According to the patient the nonpainful lesion has slowly increased in size. Based on the history, site, morphology, and color of the lesion its provisional diagnosis is which of the following?
Verrucous carcinoma
Condyloma acuminatum
Inflammatory papillary hyperplasia
Giant cell fibroma
Case 39-2
What is the proper treatment for verrucous carcinoma?
Cessation of tobacco habit followed by chemical cauterization
Complete surgical removal
Biopsy; antiviral treatment; then surgical removal
Surgical removal followed by radiation therapy
Case 40
A 14-year-old boy is seen at the pediatric dentist for a fluoride treatment. The patient and his mother report that this firm lesion has been present less than a month. What is this lesion's morphology?
Sessile macule
Pedunculated vesicle
Sessile plaque
Pedunculated papule
Case 41
An adult patient is embarrassed by this extensive tongue lesion. Although the lesion will not wipe off, the tongue does not have a burning sensation. What abnormality causes this appearance?
Increased spongiosis of the stratum spinosum layer
Elongated hyperkeratotic filiform papillae
Excess melanin deposition in the basal cell layer
Interruption in the normal maturation sequence of the epithelium
Case 42-1
A partial denture wearer has this asymptomatic palatal lesion. What is the provisional diagnosis?
Denture stomatitis
Inflammatory papillary hyperplasia
Squamous cell carcinoma
Papilloma
Case 42-2
What disease is often associated with inflammatory papillary hyperplasia (IPH)?
Giant cell fibroma
Verruca vulgaris
Condyloma acuminatum
Candidiasis
Case 43
A 52-year-old cigarette smoker is aware of this nonwipeable tongue lesion. The lesion has been present for several years and is believed to have slowly enlarged. What is the diagnosis?
Acute pseudomembranous candidiasis
Geographic tongue
Leukoplakia
White sponge nevus
Case 44
These asymptomatic ventral tongue lesions are also noted on the patient's anterior facial gingiva. What is the likely provisional diagnosis?
Condyloma acuminatum
Squamous papilloma
Verruciform xanthoma
Verrucous carcinoma
Pigmented Lesions
Case 45
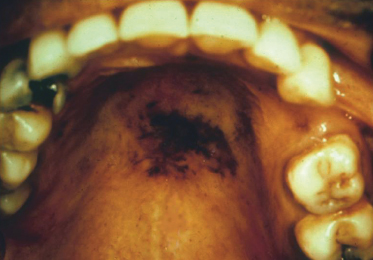
A 29-year-old man with AIDS complains of fatigue, weakness, and depression. There has been a recent onset of oral pigmentation. The patient takes a regimen of antiviral medications. Why would a person with AIDS have the described symptoms and pigmentation as in this case?
AZT treatment
Opportunistic infection that has destroyed the adrenal cortex
Low lymphocyte counts
Increased melanocytic nevi in HIV-positive populations
Case 46
What structure in the area could form a fluid-filled cystic lesion that might appear blue?
Incisive canal
Mucocele
Dentigerous cyst
Cyst from a nonvital tooth
Case 47
What is the best treatment for this lesion?
Observation
Wide excision
Brush cytology for diagnosis
Biopsy
Case 48
What is the likely diagnosis of this lesion given its rapid appearance following trauma?
Melanoma
Melanoacanthoma
Peutz–Jeghers syndrome
Blue nevus
Case 49
When biopsied this lesion showed increased melanin pigment in the basal layer. What is the diagnosis?
Pigmented nevus
Melanoma
Amalgam tattoo
Melanotic macule
Case 50
This person is being treated with an antimalarial drug that is known to cause oral pigmentation. What disease listed would be commonly treated so?
Mucous membrane pemphigoid
Lupus erythematosus
Cat scratch disease
Diabetes mellitus
Case 51
A 12-year-old boy with congenital pigmentation of the orofacial area has multiple medical problems, including hyperthyroidism and multiple bone lesions resulting in several fractures. What is the most likely diagnosis?
Peutz–Jeghers syndrome
Addison's disease
Melanotic neuroectodermal tumor of infancy
McCune–Albright syndrome
Case 52
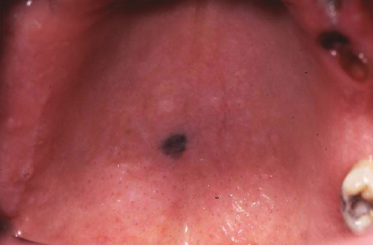
An 8-year-old boy has had this asymptomatic lesion for “a long time.” Considering the history what is the most likely diagnosis?
Mucocele
Foreign body
Peutz–Jeghers syndrome
Albright's disease
Soft Tissue Masses
Case 53
Through an interpreter, this 59-year-old woman gives a 13-year history of a slowly expanding swelling. The lesion is nontender and firm upon palpation. Based on the site, morphology, color, and history of this lesion, what would be the best provisional diagnosis?
Mucocele
Fibroma
Nasolabial cyst
Monomorphic adenoma
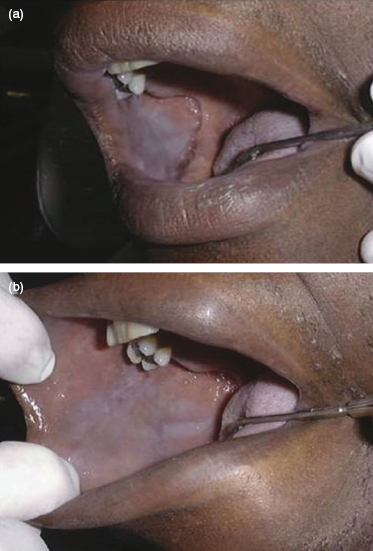
Case 54
A 16-year-old girl had a history of delayed eruption of her permanent teeth. Photo a uses a mirror to show the changes on the left side; photo b shows labial and lingual views of the anterior maxilla. Based on the information and pictures provided, the provisional diagnosis should be which of the following?
Gingival fibromatosis
Amyloidosis
Gingival cyst of the adult
Neurofibromatosis type 1
Case 55-1
A 33-year-old amateur hockey player has a history of facial trauma a few years ago. This fluctuant, asymptomatic swelling has been present for about 3 weeks. The soft tissue lesion illustrated is yellow because of which of the following?
Fat
Lymphoid tissue
Pus
Sebum
Case 55-2
If the morphology of this lesion is a vesicle, then the correct provisional diagnosis would be which of the following?
Mucocele
Parulis
Fistula
Pyogenic granuloma
Case 56-1
A 45-year-old man with a past medical history of colon carcinoma developed this nontender, compressible swelling approximately 2 weeks ago. He is concerned and scheduled an emergency appointment with his dentist. If the patient is not seen by the dentist for several more weeks, what is likely to become of the lesion?
Regress and regrow
Spontaneously involute
Continue to enlarge indefinitely
Remain the same size
Case 56-2
What is the best treatment of this lesion?
Inject sclerosing agent and then completely remove
Incisional biopsy
Excisional biopsy
Excisional biopsy of the mucin and involved minor salivary gland
Case 57
A healthy 18-year-old boy has not traumatized this nonpainful lesion. Which of the following would not be a reasonable differential diagnosis?
Peripheral ossifying fibroma
Peripheral giant cell granuloma
Granular cell tumor
Pyogenic granuloma
Case 58
An obese 40-year-old woman presented with this lesion at a new patient examination. She was not aware of this swelling, although her last appointment with her previous dentist was 2 years ago and he had not mentioned it then. What is a possible etiology of this lesion if when biopsied a central large mass of adipose tissue is discovered?
Infection
Physical trauma
Herniation of the buccal fat pad
Excessive fat metabolism
Case 59
This healthy 25-year-old woman admitted to a habit of sometimes sucking on this soft nonpainful lesion. What is a very likely provisional diagnosis?
Mucocele
Fibroma
Congenital epulis
Pleomorphic adenoma
Case 60
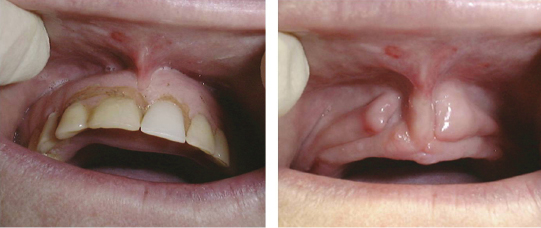
A 64-year-old woman has worn the maxillary denture in the photograph (left) for 30 years. These bilateral soft swellings (right) are visible when the denture is removed. What is the clinical diagnosis term?
Traumatic neuroma
Fibromas
Epulis fissuratum
Peripheral odontogenic tumor
Case 61-1
This soft and compressible lesion is associated with a subtle fluctuant swelling of the ipsilateral floor of mouth. Based on this lesion's site, morphology, and history provided, what would be the best provisional diagnosis?
Plunging ranula
Dermoid cyst
Cat scratch disease
Infectious mononucleosis
Case 61-2
What floor-of-mouth pierced muscle results in this neck swelling?
Genioglossus
Geniohyoid
Omohyoid
Mylohyoid
Case 62
A 10-year-old boy has this firm, unilateral neck swelling as well as a low-grade fever and night sweats. Based on the patient's age, signs and symptoms, and site of involvement the most likely provisional diagnosis is which of the following?
Cervical lymphoepithelial cyst
Abscess
Lipoma
Hodgkin's disease
Case 63-1
A 31-year-old woman has several facial and thoracic lesions similar to this neck lesion. In addition to the pigmentation noted on the neck, there is also axillary pigmentation. What is the likely diagnosis?
Sarcoidosis
Neurofibromatosis type 1
Multiple endocrine neoplasia syndrome type 2b
Amyloidosis
Case 63-2
What is the name of the smaller, flat brown pigmentations higher up on the neck?
Café au lait spots
Snail track lesions
Ash leaf spots
Purpura
Case 64
This floor-of-mouth, nonpainful, compressible bulla has been present for several weeks in a 12-year-old girl. What is the clinical name for this lesion?
Dermoid cyst
Ranula
Mucoepidermoid carcinoma
Nevus
Case 65
A patient accidentally bit his tongue a few weeks ago. Lately, he has noticed this firm “bump.” What is the most likely tissue that has proliferated to result in this clinically apparent lesion?
Connective tissue
Neurofibroma
Granular cell tumor
Hemangioma
Case 66
A 57-year-old man is aware of this boggy, edematous swelling of the palate. Each of the following is a reasonable clinical differential diagnosis for this lesion except one. Which one is the exception?
Kaposi's sarcoma
Mucoepidermoid carcinoma
Non-Hodgkin's lymphoma
Mucocele
Case 67
This tender neck mass arose following a severe sore throat and flulike symptoms. Which of the following neck swellings best fits the clinical history and appearance provided?
Cervical lymphoepithelial cyst
Thyroglossal duct cyst
Reactive lymphadenopathy
Pleomorphic adenoma
Case 68
A patient requests a head and neck examination to evaluate a very firm, nonpainful swelling of his left neck. The patient recently quit smoking cigarettes after a 30-year, pack-a-day habit.
If, upon biopsy of this lymph node swelling, squamous cell carcinoma were found, where would the occult primary most likely be?
Prostate
Hard palate
Floor of mouth
Posterior lateral tongue
Answers to Case Study Questions
Discussion
White Lesions
Case 1
Candidiasis—wrong. The lesion does not have a roughened, ragged appearance and the entire white component is removable (i.e., the Candida albicans hyphae/spores).
Leukoedema—wrong. The lesion disappears when stretched; it is not partially removable; it is bilateral.
White sponge nevus—wrong. The lesion has been present from an early age and is bilateral; it is not partially removable.
Morsicatio buccarum—correct. The ragged white clinical appearance is typical; tissue tags are “peelable” but frictional-induced white keratin component is not; patients are often not aware of their nibbling habit and/or deny it.
Case 2
Candidiasis—correct. The age, history, and clinical information are diagnostic for a typical case of pseudomembranous candidiasis.
Diphtheria—wrong. Similar-appearing lesions of necrotic debris may be seen but are in the oropharynx with diphtheria.
White sponge nevus—wrong. The patient's age is correct but white sponge nevus lesions do not wipe away.
Hairy leukoplakia—wrong. The patient's age and immune status and the lesion's wipeability and site are not correct.
Case 3
Chemical trauma—wrong. This is an aspirin burn and the white areas represent necrotic tissue. This should be part of your differential diagnosis.
Leukoedema—correct. Leukoedema lesions should be bilateral and disappear with stretching.
Morsicatio buccarum—wrong. Morsicatio may appear this way and be unilateral. This should be part of your differential diagnosis.
Tobacco pouch keratosis—wrong. The history would provide more details. Tobacco pouch keratosis is a type of keratotic reaction to the irritant chemicals in tobacco. This should be part of your differential diagnosis.
Case 4
Leukoedema—wrong. The lesion should be bilateral and disappear when stretched; leukoedema does not peel.
Lichen planus—wrong. The lesion should be bilateral and more linear; lichen planus does not peel.
Chemical reaction to mouthwash—correct. This is especially seen with mouthwash having a high alcohol content; coagulative necrosis portion peels off.
Uremic stomatitis—wrong. It has similar lesions but more widespread and there is a history of kidney failure; uremic stomatitis does not peel.
Case 5
Morsicatio—wrong. This diagnosis needs clinical corroboration or biopsy results.
Leukoplakia—correct. This is purely a clinical diagnosis; there is not enough information to diagnose it further.
Squamous cell carcinoma—wrong. Biopsy is necessary for diagnosis.
Hairy leukoplakia—wrong. The lesion is at an atypical site and there is no history of HIV. Biopsy is necessary for diagnosis.
Case 6
Desquamated epithelial cells and bacteria—correct. The bacteria likely cause the burning sensation.
Cells from white sponge nevus—wrong. The patient's age is too great, and there is no family history.
Necrosis from a chemical burn—wrong. The pattern is too generalized, and there is no history of caustic chemical use.
Hyperkeratosis—wrong. The pattern is distinct enough to allow a clinical diagnosis of coated tongue, and hyperkeratosis is not the cause of the coloring.
Case 7
Leukoedema—wrong. Leukoedema would have a different histology and is usually seen on the buccal mucosa.
Hyperplastic candidiasis—wrong. Histopathology would show fungal hyphae.
Tobacco pouch keratosis—correct. This is a hyperkeratosis from the irritation of chemicals in snuff.
Lichen planus—wrong. This is an unusual site and the histopathology is not consistent with lichen planus.
Case 8
Tobacco pouch keratosis—wrong. Lesion would not disappear upon stretching.
Pseudomembranous candidiasis—wrong. Lesion would wipe off, leaving a red base, and would not disappear if stretched.
Nicotine stomatitis—wrong. The location is incorrect, and the lesion would not disappear with stretching.
Leukoedema—correct. Leukoedema is clinically diagnosable from history, appearance, and behavior.
Case 9
Wickham's striae—correct. These are typical for lichen planus but similar lesions are seen with hypersensitivity reactions and lupus erythematosus.
Lines of Zahn—wrong. They are fibrin and platelet lines separating coagulated blood in a thrombus.
Lines of Retzius—wrong. They are the incremental deposition of enamel.
Koebner's striae—wrong. Koebnerization leads to Wickham's striae.
Case 10
Leukoplakia—wrong. There is enough information given along with the clinical presentation to make a diagnosis.
Hyperkeratosis with dysplasia—wrong. Diagnosis requires microscopic analysis.
Nicotine stomatitis—correct. Heat-induced changes cause inflammation of the salivary ducts.
Lichen planus—wrong. The red papules seen are not typical for lichen planus.
Case 11
Age of 60—correct. People of all ages get candidiasis.
History of chronic obstructive pulmonary disease (COPD)—wrong. People with COPD often take steroids, which may predispose to candidiasis.
Denture wear—wrong. Wearing dentures day and night, improper cleaning, and so on enhance the development of candidiasis.
Antibiotic use—wrong. Antibiotic may kill other organisms, resulting in an imbalance where yeast may overgrow.
Case 12
HIV testing—wrong. People without HIV can have hairy leukoplakia.
Biopsy with stains for Epstein–Barr virus—correct. The only way to confirm a diagnosis of hairy leukoplakia is to show the presence of Epstein–Barr virus.
The lesions should wipe away with gauze—wrong. That is true for some types of candidiasis.
Historical information about other family members with a similar condition—wrong. Hairy leukoplakia is not an inheritable disease such as white sponge nevus.
Red, Red-and-White, and Purpuric Lesions
Case 13-1
Erythema migrans—wrong. The lesion has the wrong morphology; there is usually a white raised rim and the lesion changes size.
Erythematous candidiasis—wrong. The lesion has the wrong color (blue) component; the history is not supportive.
Erythroplakia—wrong. The lesion has the wrong color (blue) component and wrong morphology.
Hemangioma—correct. The lesions may be blue besides red; they are compressible and blanchable.
Case 13-2
Neoplastic—wrong. Hemangiomas are not neoplastic but rather developmental hamartomas.
Developmental—correct. Hemangiomas are hamartomatous.
Inflammatory—wrong. Hemangiomas are not inflammatory but rather developmental hamartomas.
Reactive—wrong. Hemangiomas are not reactive lesions but rather developmental hamartomas.
Case 14-1
Cinnamon allergic reaction—wrong. Topical mucosal allergic reaction can be a mixture of red and white, and lesions do not wipe off.
Acute candidiasis—correct. The acute form is the pseudomembranous type and the white mixture of fungal hyphae, epithelial cells, keratin, and bacterial colonies can be wiped off.
Lupus erythematosus—wrong. The age, gender, and lack of wipeability fit, although the lesions are often painful since the red component is erosive in nature.
Cheek nibbling—wrong. The site is good for this and sometimes there is a lack of wipeable tissue shreds so that none of the white portion can be wiped off; the reddened area could be secondary inflammation and the habit can be unilateral.
Case 14-2
Lichen planus—wrong. Although the age and gender are good, the red component of the lesions would be painful erosions.
Cinnamon allergic reaction—correct. Although the history does not mention the use of cinnamon-flavored gum or candy, the color, site, morphology, and lack of wipeability all fit.
Thermal burn—wrong. The white component is wipeable.
White sponge nevus—wrong. The site is good but onset is in childhood for this autosomal dominant inherited condition, which is more extensive, bilaterally on the buccal mucosa.
Case 15-1
Lichen planus—wrong. There is no evidence of papules or striae; the red component is not erosive.
Verruciform xanthoma—wrong. This is not a typical site and verruciform xanthoma does not account for the diffuse, mottled reddened vermilion.
Actinic cheilosis—correct. The mottled red-and-white changes are typical of a sun-damaged lip; furthermore, the lesion has a rough, sandpaper surface texture.
Candidiasis—wrong. Candidiasis lesions are wipeable and more extensive.
Case 15-2
Lesion often oozes a mucous secretion—wrong. That condition is cheilitis glandularis.
Actinic cheilitis is more common on the upper lip—wrong. It is much more common on the lower lip.
Precancerous changes are reversible—wrong. The elastic and collagen fibers are permanently damaged as well as the surface epithelium.
A significant percentage of lesions are premalignant—correct. Approximately 20% will develop squamous cell carcinoma.
Case 16-1
Traumatic erythema—wrong. The lesion is not an ulcer and there is no mention of pain.
Erythema migrans—correct. The lesion is a flat reddened area encircled by a raised border; this condition comes and goes and the lesion frequently changes shape as different areas of the tongue undergo depapillation and then repappilation.
Erythroleukoplakia—wrong. This potentially malignant lesion is seen in middle-aged to elderly adults and does not have a cyclical appearance.
Nicotine stomatitis—wrong. This smoking-tobacco-related condition is not premalignant despite its leukoplakic component; the red component comprises inflamed minor salivary glands.
Case 16-2
Candidiasis—wrong. Neither the chronic erythematous nor the acute pseudomembranous form of this superficial fungal condition is associated with geographic tongue.
Erosive lichen planus—wrong. This condition is an immune-mediated condition in which there is a blistering process of the epithelium resulting in ulceration and erosion.
Psoriasis—wrong. Even though geographic tongue has histopathology similar to psoriasis, there is no evidence that it is related to psoriasis.
Fissured tongue—correct. This harmless developmental disorder is associated with geographic tongue in a relationship that is not understood.
Case 17-1
Anterior facial involvement—wrong. That is the most common site of involvement.
Erythema—wrong. Although the tissue may be firm and pink it is often secondarily inflamed.
Excess attached gingiva—wrong. In dentate areas the attached gingival hyperplasia creates areas of anatomical crown coverage.
Spontaneous gingival hemorrhage—correct. For this condition to be occurring, some inherited or disease-associated blood diathesis must be present.
Case 17-2
Leukemia—correct. The constitutional symptoms are seen along with an elevated white blood cell count; anemia and infections, in addition to decreased platelets with resultant spontaneous hemorrhage, are seen due to a bone marrow myelophthesic anemia (all three major blood cell lines are affected).
Infectious mononucleosis—wrong. Mononucleosis lesions are petechiae on the soft palate, 1–2 mm of extravasated blood due to capillary fragility; there usually is an associated pharyngitis/tonsillitis.
Scarlet fever—wrong. The oral site involved is the tongue (i.e., strawberry or raspberry tongue).
Hereditary hemorrhagic telangiectasia—wrong. The vascular lesions are pinpoint areas of extravasated blood due to a developmental defect in the blood vessel wall; no gingival hyperplasia is seen, nor are constitutional symptoms.
Case 18-1
Hemangioma—wrong. They are flat or raised, are compressible, and do not bleed or cause soreness.
Lichen planus—wrong. It is a chronic mucosal or cutaneous disorder that can be found in this age group and in men nearly as often as in women, but there should be a blister (vesicle); additionally, this would be a rare site of involvement.
Actinic cheilitis (cheilosis)—wrong. This lesion is related to sun damage and would not be sore, and it involves other areas of the lower lip more than the commissure.
Angular cheilitis—correct. The site, morphology, and color are correct as is the painful chronic nature.
Case 18-2
Vitamin deficiency—correct. Nutritional deficiencies such as vitamin B complex and iron can cause this condition, also known as perleche, besides certain infectious bacterial organisms.
Developmental defect—wrong. Developmental blind-ended epithelial lined pouches called commissural lip pits can be seen at this site but they are depressed areas that are asymptomatic and normal color.
Viral infection—wrong. Viral infections cause vesicle (blister) formation such as recurrent herpes labialis, which secondarily breaks down into clusters of small ulcers that then scab. Unless the patient is severely immunocompromised the lesions should be acutely painful for 7–10 days and then resolve; furthermore, there should not be bleeding.
Protozoan infection—wrong. Angular cheilitis is typically caused by the fungal organism Candida albicans and rarely by the bacterium Staphylococcus aureus.
Case 19
Topical steroid application—wrong. Although the lesion is likely lichen planus, which often positively responds to topical or systemic steroid treatment, the provisional diagnosis should be confirmed by biopsy.
Biopsy of left and right lesions—correct. The only way to know the diagnosis with absolute certainty is to perform incisional, perilesional biopsies of both sites of involvement; never assume that the diagnosis is the same for each side.
Cytology to rule out malignancy—wrong. Cytology is a screening procedure not a diagnostic procedure.
Antifungal medication—wrong. The provisional diagnosis is lichen planus with areas of erosion beginning; steroid medication is usually most effective.
Case 20
Treat both the denture and oral mucosa with antifungal agents—correct. The denture should be soaked nightly for 2 weeks in a nystatin rinse mixed with water; the oral mucosa should be treated with either clotrimazole troches (10 mg, five times daily; dissolved) or clotrimazole cream applied to the inner aspect of the denture.
Leave the denture out at night, clean it, and rinse it in an antifungal solution—wrong.
Use laser ablation followed by new denture construction—wrong. The diagnosis is chronic erythematous candidiasis, and laser ablation will not address the organisms that are within the denture's acrylic resin.
Apply antifungal cream to the affected oral soft tissues—wrong. In addition to managing the oral mucosa, the denture should be soaked in an antifungal solution (e.g., nystatin 100,000 I.U.; use several drops in a small container of water).
Acute Oral Ulcerations
Case 21
Patient's age—wrong. People of all ages get aphthae.
Asymptomatic lesion—correct. Aphthae are painful.
Healed spontaneously in 2 weeks—wrong. Aphthae usually resolve in 2 weeks.
Site—wrong. Although aphthae usually do not begin on the dry lip (i.e., vermilion), they start on the labial mucosa and can expand to the dry lip.
Case 22
Erythema multiforme—correct. Erosions of explosive onset are the typical finding.
Aphthous ulcers—wrong. Aphthae are a chronic recurrent problem with a recognizable prodrome.
Herpes simplex—wrong. Primary herpes would have a gingivostomatitis. Secondary lesions would begin as ulcers on nonmovable mucosa bound to bone.
Varicella—wrong. Oral lesions of chicken pox are usually nonpainful.
Herpangina—correct. Site, age, morphology, and mild symptoms are all correct.
Herpes simplex—wrong. Site is wrong and symptoms are too mild.
Recurrent aphthae—wrong. Aphthae do not begin with blisters.
Syphilis—wrong. Recurrent oral lesions are mucous patches and not ulcerative.
Case 25
Herpangina—wrong. The lesions are not vesicular.
Recurrent aphthous ulcers—correct. The only way to tell the difference is to search for systemic signs and symptoms.
Erythema multiforme—wrong. Chronicity and recurrence are different than the signs of erythema multiforme.
Pemphigus vulgaris—wrong. Pemphigus lesions begin as blisters and spread until the disease is controlled.
Case 26
Painful ocular inflammation—wrong. This occurs in Behcet's disease.
Gingivostomatitis—wrong. This occurs in primary herpes simplex.
Necrosis of the interdental papillae—wrong. This occurs in ANUG.
Vesicular skin lesions—correct. These lesions are typical for chicken pox.
Case 27
Herpetiform aphthae—correct.
Herpes simplex—wrong. This is an incorrect site for recurrent lesions.
Herpes zoster—wrong. Zoster does not cross the midline.
Chicken pox—wrong. Age, recurrence, and pain are not typical for chicken pox.
Case 28
Recurrent aphthous ulcer—correct. Aphthae occur on movable mucosa.
Necrotizing sialometaplasia—wrong. This is a likely diagnosis. Extranodal non-Hodgkin's lymphoma and salivary gland tumors should also be considered.
Superficial mucocele—wrong. This is a good site and they often have periodic rupture with painful ulceration.
Wegener's granulomatosis—wrong. This is a good site and presentation for this disease; however, lung and kidney involvement should also be present.
Chronic Vesiculoerosive and Ulcerative Lesions
Case 29
Wegener's granulomatosis—wrong. Lesions usually occur on palate with lung and kidney involvement.
Noma—wrong. Necrotic ulcerations are seen in immunocompromised patients.
Erosive lichen planus—wrong. Usually Wickham's striae are seen along with erythema and ulceration.
Pyostomatitis vegetans—correct. The peculiar lesions in conjunction with the history are indicative of inflammatory bowel disease (Crohn's, ulcerative colitis, etc.).
Case 30
Mucous membrane pemphigoid—correct. About 30% of cases have ocular involvement that can lead to scarring and blindness.
Erosive lichen planus—wrong. The oral lesions are similar but eye lesions are not present.
Erythema multiforme (Stevens–Johnson syndrome)—wrong. This disease can have oral and eye lesions but it is an acute rather than a chronic process.
Herpes zoster—wrong. Zoster stops at the midline; this patient's distribution is wrong.
Case 31
Squamous cell carcinoma—wrong. This should be the first choice in the differential diagnosis.
Deep fungal infection—wrong. This is a lesion of histoplasmosis. Deep fungal infections closely resemble carcinoma.
Mucous membrane pemphigoid—correct. Lesions of pemphigoid are usually multiple and shallow, and they heal.
Traumatic granuloma—wrong. These nonhealing ulcers are very similar to carcinomas in appearance.
Case 32
Behcet's syndrome—wrong. The ulcers seen in Behcet's are mucosal and there should also be cutaneous and ocular signs.
Midline lethal granuloma—correct. This is a T-cell lymphoma that occurs on the palate.
Tertiary syphilis—wrong. A gumma presents with a similar lesion but does not cause death by malignant spread.
Wegener's granulomatosis—wrong. A very similar presentation may be seen and it may prove fatal, but death is usually from kidney failure. It is not a malignancy.
Case 33
Lesions are bilateral—wrong. This is a typical sign of lichen planus.
Lesions come and go—correct. Lichen planus is a chronic disease with exacerbation and remission. Hypersensitivity reactions will remain as long as the allergen is in contact with the area.
White striae—wrong. White striations (striae) can be seen in lichenoid hypersensitivity reactions as well as lupus erythematosus.
Ulceration—wrong. Ulceration can be seen in erosive lichen planus as well as in a hypersensitivity reaction.
Case 34
Presence of rheumatoid factor—wrong. Rheumatoid factor is common in the serum of people with many autoimmune diseases.
Presence of antinuclear antibodies—wrong. This is seen in lupus erythematosus.
Positive Nikolsky sign—wrong. A Nikolsky sign will be present but it is seen in many blistering diseases.
Direct and indirect immunofluorescence studies—correct. Direct (tissue) and indirect (serum) immunofluorescence should be positive in pemphigus.
Case 35
Traumatic ulcerative granuloma—correct. These lesions are typically long-standing and are suspicious for carcinoma or deep fungal infection. They often spontaneously resolve after biopsy.
Deep fungal infection—wrong. Healing does not occur without treatment.
Squamous cell carcinoma—wrong. Lesion would not resolve without treatment.
Erythema multiforme—wrong. This is an acute disease and would not present as a long-standing single ulcer.
Case 36
Recurrent herpes—wrong. Herpes lesions will be on intraoral mucosa bound to bone and will be painful.
Traumatic ulcer—wrong. The ulcer is usually painful and has a history of injury.
Noma—wrong. Necrotic ulcerations occur in severely immunocompromised children, especially those who are malnourished.
Squamous cell carcinoma—correct. The leading site for intraoral carcinoma is the lateral ventral tongue and floor of mouth. The lesions are often asymptomatic.
Papillary Lesions
Case 37-1
Verruca vulgaris—wrong. The site, morphology, and color of the lesion all fit and so a reasonable clinical provisional diagnosis would include this lesion; however, the history of HIV-positivity does not make this choice the most likely diagnosis.
Hairy tongue—wrong. The site, but not the morphology or color, of the lesion does not fit and so this is not a reasonable clinical provisional diagnosis. The “hairs” of the dorsal tongue are elongated filiform papillae with excess keratin that is extrinsically stained, usually brown or black.
Squamous papilloma—wrong. The site, morphology, and color of the lesion all fit and so a reasonable clinical provisional diagnosis would include this lesion; however, the history of HIV-positivity does not make this choice the most likely diagnosis.
Hairy leukoplakia—correct. The site, morphology, and color of the lesion all fit and so a reasonable clinical provisional diagnosis would include this lesion; furthermore, the history of HIV-positivity makes this choice the most likely provisional diagnosis.
Case 37-2
Human papillomavirus—wrong. This family of DNA viruses, of which there are more than 130 types, cause some oral squamous papillomas and warts (verruca vulgaris) besides genital ones; 15 or so types are oncogenic, including cervical carcinoma.
Epstein–Barr virus—correct. When the immune system in an HIV-positive patient becomes increasingly inefficient (i.e., full-blown AIDS onset is imminent), then the Epstein–Barr virus for unknown reasons congregates especially on the lateral border of the tongue, invades the epithelial cells, and creates this benign neoplastic growth.
Human immunodeficiency virus—wrong. Although hairy leukoplakia is associated with the transformation of HIV-positivity to AIDS by severe immunodeficiency onset, it is another virus that then is able to infect and cause hairy leukoplakia.
Herpes simplex virus—wrong. Herpes simplex type 1 causes recurrent herpes labialis and intraoral lesions involving nonmovable mucosa in immunocompetent persons; the epithelial cells are invaded by the virus, the destroyed cells resulting in clusters of vesicles that then de-roof into coalescing shallow, irregular ulcers.
Case 38-1
Verruca vulgaris—wrong. Site, color, and morphology are all as expected for this lesion.
Squamous papilloma—wrong. Site, color, and morphology are all as expected for this lesion.
Verrucous carcinoma—correct. Although the surface texture, lack of pain, and color (some are red or a mixture of white and red) are acceptable, the size is much too small and the location is not particularly common; also the age of occurrence is generally patients in their 50s and older.
Verruciform xanthoma—wrong. Site, color, and morphology are all as expected for this lesion.
Case 38-2
Rapid onset—wrong. Verrucous carcinoma has a very slow, chronic onset.
Pain—wrong. Verrucous carcinoma is not a painful condition.
Smokeless tobacco habit—correct. Many elderly patients use this type of tobacco (snuff, chewing) and in 1–9% of users it forms where the tobacco is held against the mucosa.
Compressible—wrong. Verrucous carcinoma is not fluid-filled (vesicle–bulla).
Case 39-1
Verrucous carcinoma—correct. Typically seen in the vestibule, particularly with smokeless tobacco users; white intermixed with red and hemorrhage; slowly enlarges with a marked verrucous surface and advancing sessile borders.
Condyloma acuminatum—wrong. Usually multiple lesions with blunt projections; no bleeding.
Inflammatory papillary hyperplasia—wrong. Typically seen beneath a denture base, particularly in the palatal vault; multiple small pink papules often with erythema (red) but no hemorrhage.
Giant cell fibroma—wrong. Typically a smooth or papillated surface papule/nodule with no bleeding.
Case 39-2
Cessation of tobacco habit followed by chemical cauterization—wrong. Even those cases caused by smokeless tobacco use will not reverse the diagnosis once this well-differentiated form of squamous cell carcinoma has arisen; chemical cauterization can be helpful for painful conditions in which nerves are exposed to the oral cavity.
Complete surgical removal—correct. Once a diagnosis is established by a small biopsy of a representative area of the lesion, then its complete removal is necessary to ensure no recurrence.
Biopsy; antiviral treatment; then surgical removal—wrong. The intermediate step of antiviral treatment is not helpful and only delays completion of treatment.
Surgical removal followed by radiation therapy—wrong. Surgical removal is appropriate after an incisional biopsy diagnosis; however, controversy exists if radiation treatment can be used as primary or adjuvant treatment. Prior studies have shown radiation causes increased grade of tumor but more recent reports point to success with radiation as a primary therapy.
Case 40
Sessile macule—wrong. A macule is a flat lesion of abnormal color; sessile indicates a broad base with the base's size exceeding the length of any portion of the lesion superior to it.
Pedunculated vesicle—wrong. A vesicle is an elevated lesion filled with fluid so it is not firm but rather soft and compressible.
Sessile plaque—wrong. A plaque is a very slightly elevated lesion unlike the more marked elevated lesion seen.
Pedunculated papule—correct. The elevated lesion is firm and less than 5 mm in diameter and thus by definition is a papule and upon palpation will be firm; the base involves growth over unattached tooth surface and thus is pedunculated, with the base possessing less length in greatest dimension than the superior aspect of the lesion.
Case 41
Increased spongiosis of the stratum spinosum layer—wrong. Increased intracellular edema (i.e., spongiosis) results in leukoedema or white sponge nevus, which are whitish areas and in the case of white sponge nevus exhibit a thickened folded tissue.
Elongated hyperkeratotic filiform papillae—correct. The excess surface keratin in conjunction with the increased length of the dorsal papillae increase secondary extrinsic staining (often tea, coffee, cigarettes), resulting in a brown or black discoloration.
Excess melanin deposition in the basal cell layer—wrong. Focal melanosis results in a brown discoloration but the morphology is a macule; also, the pigmentation on the tongue generally only involves the tip of the papillae.
Interruption in the normal maturation sequence of the epithelium—wrong. By definition, this is dysplasia, which is a potentially malignant change; the morphology would be white or red plaques (i.e., leukoplakia, erythroplakia).
Case 42-1
Denture stomatitis—wrong. Erythematous form of candidiasis that can be asymptomatic or have a burning sensation, and it has a macular morphology.
Inflammatory papillary hyperplasia—correct. The reddish coloration is from chronic inflammation mixed with numerous individual papules that are coalescing; it is typically seen under a denture base.
Squamous cell carcinoma—wrong. Rare site for this type of cancer; the lesion is typically a white or red plaque that then breaks down into ulceration; verrucous carcinoma would be white and not necessarily associated with a denture.
Papilloma—wrong. Papilloma is usually more discreet and pink to white; it is not associated with a denture.
Case 42-2
Giant cell fibroma—wrong. Lesion is a solitary pink papule/nodule with smooth or rough surface; site is typically gingiva.
Verruca vulgaris—wrong. Lesion is a solitary white papule/nodule with a very rough, spiky surface.
Condyloma acuminatum—wrong. Lesions are usually multiple pink to white-pink papules/nodules lacking any erythematous (inflammatory) component.
Candidiasis—correct. Investigators are not sure if chronic erythematous candidiasis is always secondary to the onset of IPH.
Case 43
Acute pseudomembranous candidiasis—wrong. This type of fungal infection is wipeable; with the information provided, a provisional diagnosis can be made but a diagnosis would require microscopic information.
Geographic tongue—wrong. Although the site is appropriate, the color is incorrect (irregular, red flat area surrounded by a thin, elevated white rim); with the information provided a provisional diagnosis can be made but a diagnosis would require microscopic information.
Leukoplakia—correct. This is purely a clinical term for unwipeable white plaques that do not resolve in 2 weeks. When biopsied this lesion possessed premalignant changes; the tobacco habit is likely the chief etiologic factor.
White sponge nevus—wrong. Although this lesion is white and unwipeable, white sponge nevus is most often seen bilaterally on the buccal mucosa beginning early in life, unlike this patient's history; it is autosomal dominant inherited; it would not slowly enlarge as this lesion has.
Case 44
Condyloma acuminatum—correct. The lesion's site, color, morphology, and multifocal, multicentric distribution are all indicative of this venereal wart condition.
Squamous papilloma—wrong. Lesion is white to pink white and is not multifocal.
Verruciform xanthoma—wrong. Lesion is not multifocal and not common on ventral tongue.
Verrucous carcinoma—wrong. Lesion is red and/or white and is not multifocal.
Pigmented Lesions
Case 45
AZT treatment—wrong. AZT can cause pigmentation but it does not cause the other symptoms listed.
Opportunistic infection that has destroyed the adrenal cortex—correct. Adrenocortical insufficiency (Addison's disease) due to uncontrolled tuberculosis infection is a likely cause in AIDS patients.
Low lymphocyte counts—wrong. This may lead to infection but not pigmentation.
Increased melanocytic nevi in HIV-positive populations—wrong. No reported incidence.
Case 46
Incisive canal—correct. Incisive canal cysts may have a soft tissue component.
Mucocele—wrong. Salivary glands in the rugae area as well as mucoceles not seen.
Dentigerous cyst—wrong. All teeth are erupted; however, this may be an eruption cyst associated with a supernumerary tooth.
Cyst from a nonvital tooth—wrong. An intrabony lesion would not be seen clinically.
Case 47
Observation—wrong. Observation will not give a diagnosis.
Wide excision—wrong. Definitive treatment is not appropriate without a diagnosis.
Brush cytology for diagnosis—wrong. Cytology only looks at superficial cells confined to the epithelium; it is not appropriate for pigmented lesions.
Biopsy—correct. This is a melanoma; real pigmented lesions can rarely be diagnosed by clinical signs and need tissue for microscopic analysis.
Case 48
Melanoma—wrong. Wrong site, wrong age; rapid growth of a new lesion of melanoma is not typical.
Melanoacanthoma—correct. Trauma, buccal mucosa, and rapid growth are the usual findings.
Peutz–Jeghers syndrome—wrong. Pigmentation should be present from early childhood.
Blue nevus—wrong. Lesion usually occurs on palate and is not rapidly spreading.
Case 49
Pigmented nevus—wrong. Nevi are composed of a proliferation of benign melanocytes.
Melanoma—wrong. Melanomas are composed of a proliferation of malignant melanocytes.
Amalgam tattoo—wrong. Amalgam tattoo should have deposits of foreign material in the lamina propria.
Melanotic macule—correct. Lesion is most commonly seen on the lower lip.
Case 50
Mucous membrane pemphigoid—wrong. It is usually treated with topical steroids.
Lupus erythematosus—correct. Chloroquine acts as a steroid sparing anti-inflammatory.
Cat scratch disease—wrong. Disease is usually self-limited.
Diabetes mellitus—wrong. Antimalarials are not indicated for this use.
Case 51
Peutz–Jeghers syndrome—wrong. The pigmentation is similar but Peutz–Jeghers has colon polyposis, not bone lesions.
Addison's disease—wrong. Adrenal insufficiency will show bronzing of the skin but no bone lesions.
Melanotic neuroectodermal tumor of infancy—wrong. Pigmented intrabony lesions are in the anterior maxilla and are solitary; skin pigmentation is absent.
McCune–Albright syndrome—correct. Endocrine disorders, polyostotic fibrous dysplasia, and skin pigmentation are typical of Albright's syndrome.
Case 52
Mucocele—wrong. Good location and age but the lesion should have a history of size increase with fluctuance.
Foreign body—correct. This is a traumatic implantation of pencil “lead.”
Peutz–Jeghers syndrome—wrong. Age is correct but there should be multiple lesions and the patient should have other signs of the disease (colon polyps).
Albright's disease—wrong. There should be multiple lesions.
Soft Tissue Masses
Case 53
Mucocele—wrong. These occur almost exclusively on the lower lip rather than the upper lip.
Fibroma—wrong. Almost always there is a history of trauma, and fibromas rapidly enlarge in a few weeks to months and then remain the same size thereafter.
Nasolabial cyst—wrong. The site is incorrect and this cyst would have fluid in it and be fluctuant, not firm.
Monomorphic adenoma—correct. Over the age of 40 this benign salivary gland is more likely than a pleomorphic adenoma; both are common on the upper lip.
Case 54
Gingival fibromatosis—correct. The age, site, and eruption-pattern disruption are classic for this inherited overgrowth of gingiva caused by excess fibroblastic collagen production; the entire clinical crown can be covered.
Amyloidosis—wrong. The tongue is the most common intraoral site for this peculiar type of protein product that is most often seen at multiple sites in the elderly, associated with multiple myeloma.
Gingival cyst of the adult—wrong. Although it occurs at this site, it is a solitary lesion, often with a translucent bluish appearance; it would not delay the eruption of any tooth.
Neurofibromatosis type 1—wrong. Although the neurofibromas can be on the skin and in the mouth at multiple sites, the patient should also have brown, flat skin pigmentation (café au lait spot) and several other stigmata of the autosomal dominant inherited disorder. The tongue is overwhelmingly the most common oral site.
Case 55-1
Fat—wrong. If this lesion were firm and thus the morphology were a papule/nodule, then it could be a lipoma due to the proliferation of adipose tissue.
Lymphoid tissue—wrong. Although lymphoid tissue can cause soft tissue lesions to appear yellow, the site (not in Waldeyer's ring of lymphoid tissue) is not logical.
Pus—correct. The lesion's morphology is a vesicle and the contents a sea of neutrophils resulting in a focal abscess (i.e., pus).
Sebum—wrong. Sebum can appear yellow as, for example, in the small papules and coalesced plaque areas of Fordyce granules seen most often on the labial and buccal mucosa; Fordyce granules are not typically seen on the gingiva and the morphology is an elevated blisterform (i.e., vesicle and bulla).
Case 55-2
Mucocele—wrong. Mucoceles can occur on the gingiva very rarely but they will appear pink to blue depending on the depth of the pool of inspissated mucin; the history does not agree with this as a provisional diagnosis.
Parulis—correct. The periapical abscess has spread via a fistula to the surface, where a “gum boil” appears (the collection of pus).
Fistula—wrong. A fistula is the epithelial-lined tract extending from an intrabony abscess to the mucosal site.
Pyogenic granuloma—wrong. These are bright red due to the collection of granulation tissue and are more typically found in the interdental papilla area where an inciting etiologic factor is present (e.g., restorative overhang, calculus, retained cement or impression material, hormonal changes as in pregnancy).
Case 56-1
Regress and regrow—correct. The lesion is a mucocele that typically changes sizes due to macrophage involvement with the spilled (extravasated) mucin due to the injured duct of the minor salivary gland lobule.
Spontaneously involute—wrong. The lesion is a mucocele.
Continue to enlarge indefinitely—wrong. The lesion is a mucocele.
Remain the same size—wrong. The lesion is a mucocele.
Case 56-2
Inject sclerosing agent and then completely remove—wrong. Sclerosing agents are only used at times for vascular lesions such as hemangiomas.
Incisional biopsy—wrong. The lesion does not have a worrisome (i.e., malignant) diagnosis and is small enough for complete removal.
Excisional biopsy—wrong. If the damaged gland is not also removed, then the lesion will recur.
Excisional biopsy of the mucin and involved minor salivary gland—correct. If the damaged gland is not also removed, then the lesion will recur.
Case 57
Peripheral ossifying fibroma—wrong. This is a classic site and morphology for this lesion.
Peripheral giant cell granuloma—wrong. This is a classic site and morphology for this lesion.
Granular cell tumor—correct. This lesion is very common on the dorsum of the tongue but very rare at this site.
Pyogenic granuloma—wrong. This is a classic site and morphology for this lesion.
Case 58
Infection—wrong. Fat is not a source of infection and no other signs or symptoms of infection are mentioned or observed.
Physical trauma—wrong. This is a lipoma, which is a true neoplasm (no initiating traumatic event as seen in reactive lesions such as pyogenic granuloma and fibroma or fibrous nodule).
Herniation of the buccal fat pad—correct. At times rather than a neoplastic event (e.g., lipoma) there is an outpouching of normal fat at this site.
Excessive fat metabolism—wrong. There is no relationship between a lipoma and fat metabolism or weight.
Case 59
Mucocele—wrong. Although the site and color fit, the morphology does not; the lesion is stated to be firm whereas a mucocele is a vesicle filled with mucin and thus is soft and compressible.
Fibroma—correct. This is a classic site for accidental biting (as are the tongue and buccal mucosa); firmness indicates an elevated, nonblisterform papule rather than a vesicle.
Congenital epulis—wrong. It occurs in infants (>females) on the alveolar ridge (>anterior maxilla).
Pleomorphic adenoma—wrong. It is much more common on the upper lip than lower lip.
Case 60
Traumatic neuroma—wrong. This is a histological diagnosis; lesion is most often seen as a solitary mass in the mental nerve foramen area of mandibular denture wearers following ridge resorption; it is often painful.
Fibromas—wrong. This is a histological diagnosis of a reactive lesion (typically solitary) subsequent to acute trauma. The history is wrong although site and color fit.
Epulis fissuratum—correct. Low-grade chronic trauma of ill-fitting dentures (due to gradual ridge resorption) often creates a reactive exuberant growth of excess tissue in the denture flange area that is clinically referred to as epulis fissuratum.
Peripheral odontogenic tumor—wrong. This is a histological diagnosis even though the gingiva is the correct site.
Case 61-1
Plunging ranula—correct. This lesion occurs in the lateral or midline of the neck as a soft compressible and fluctuant swelling in which floor-of-mouth extravasated mucin spreads inferiorly.
Dermoid cyst—wrong. It is a soft and fluctuant swelling of the midline (not lateral) neck.
Cat scratch disease—wrong. Although the lateral neck is a typical site, there must be a history of a cat scratch that then subsequently leads to significant infection in a draining lymph node.
Infectious mononucleosis—wrong. Although there is a lateral neck swelling, the patient should be experiencing a sore throat, swollen and tender lymph nodes, and fatigue.
Case 61-2
Genioglossus—wrong.
Geniohyoid—wrong.
Omohyoid—wrong.
Mylohyoid—correct.
Case 62
Cervical lymphoepithelial cyst—wrong. The cyst would be soft and fluctuant; it is typically seen in somewhat older patients (young adults).
Abscess—wrong. The swelling would be painful with or without drainage, and there would not be night sweats.
Lipoma—wrong. The mass would be soft and there would not be a fever or night sweats.
Hodgkin's disease—correct. Classic location, signs, and symptoms; malignant nodes are not painful. Also, age is good since there is a bimodal age distribution with two mean peaks: young people and the elderly.
Case 63-1
Sarcoidosis—wrong. Although multiple lesions of the head and neck occur with this condition, they are usually associated with the eyes, ears, and mouth; the lesions are flat and violaceous; they do not involve the axilla.
Neurofibromatosis type 1—correct. The sites of involvement as well as the color and morphology are classic for this condition, which is autosomally inherited; each lesion is a neurofibroma.
Multiple endocrine neoplasia syndrome type 2b—wrong.
Amyloidosis—wrong. Pale areas are seen and most commonly on the skin near the eyes.
Case 63-2
Café au lait spots—correct.
Snail track lesions—wrong. These are seen in Crohn's disease
Ash leaf spots—wrong. These areas of hypopigmentation are seen in tuberous sclerosis.
Purpura—wrong. These are areas of extravasated blood seen in bleeding disorders and sites of trauma.
Case 64
Dermoid cyst—wrong. This is a microscopic diagnosis of a developmental disorder.
Ranula—correct. This term is a clinical descriptor that means the area appears like a frog's swollen belly.
Mucoepidermoid carcinoma—wrong. This malignant salivary gland tumor can occur in the floor of mouth and have a bluish hue; however, the name is a microscopic diagnosis, not a clinical term.
Nevus—wrong. The term nevus means a “spot” and is typically reserved for cutaneous lesions such as congenital and acquired melanocytic nevi.
Case 65
Connective tissue—correct. This patient's lesion is likely a reactive fibroma due to the trauma, with fibroblasts stimulated to produce extra collagen.
Neurofibroma—wrong. This nerve sheath tumor consists of proliferating neuritis and axonal tissue and is a true, nonreactive neoplasm.
Granular cell tumor—wrong. Although this is the most likely morphology, color, and site for this lesion, a granular cell tumor is not caused by trauma but rather is a true proliferation of Schwann cell origin.
Hemangioma—wrong. Hemangiomas are compressible and blanchable and usually more red and/or blue; they are not caused by trauma but rather are developmental hamartomas.
Case 66
Kaposi's sarcoma—wrong. This vascular neoplasm is frequently found in the palate of HIV-positive males and, although this patient's HIV status is not reported, the site, morphology, and color fit well.
Mucoepidermoid carcinoma—wrong. The palate is the most common intraoral site for this malignant salivary gland tumor; often it has a bluish hue as seen here.
Non-Hodgkin's lymphoma—wrong. The palate is the most common extranodal oral site for this kind of lymphoma, especially B-cell type; it often has a boggy consistency.
Mucocele—correct. Although superficial mucoceles are often seen associated with palatal minor salivary glands, they are small vesicles filled with mucin that are compressible instead of boggy and would not attain the size or color of this lesion.
Case 67
Cervical lymphoepithelial cyst—wrong. Although lateral in position, the cyst would be soft, fluctuant, and nontender.
Thyroglossal duct cyst—wrong. The cyst would be in a midline position, not lateral, and would be fluctuant and nontender.
Reactive lymphadenopathy—correct. This cyst is in a lateral position with tender reactive nodes subsequent to an infection.
Pleomorphic adenoma—wrong. Although the tail of the parotid may involve this benign salivary gland tumor, it would be nonpainful and unrelated to the constitutional symptoms mentioned.
Case 68
Prostate—wrong. Although distant metastasis from the prostate can spread to bone, brain, and soft tissues, including the oral cavity, it does not spread to cervical lymph nodes.
Hard palate—wrong. The hard palate is an infrequent site of primary squamous cell carcinoma and does not typically drain to the anterior triangle lymph nodes.
Floor of mouth—wrong. Although the floor of mouth is second in frequency to the posterior lateral tongue as a primary site of squamous cell carcinoma, it typically drains to the submental nodes rather than to the cervical lymph node chain seen in this patient.
Posterior lateral tongue—correct. This is the most common site of typical squamous cell carcinoma that arises due to the etiologic factor of long-term cigarette use.