Skin lesions
Nevus flammeus (stork bites)
Pink macules on upper eyelids, mid-forehead (also called salmon patch) and nape of the neck (Fig. 21.4). Common. Dilated superficial capillaries. Those on the eyelids and forehead fade over the first year. Those on the neck persist but are covered with hair.
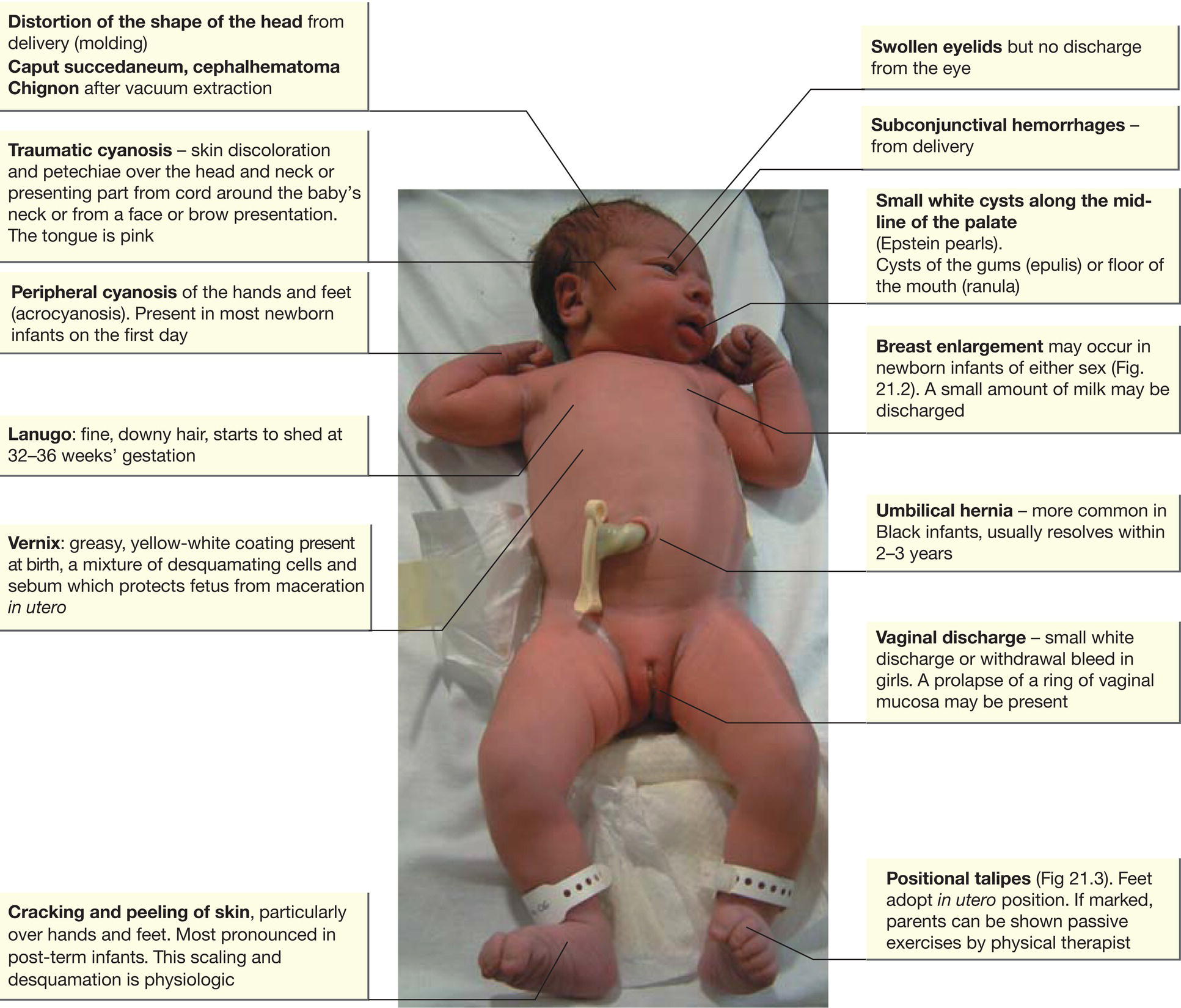
Fig. 21.1 Minor abnormalities noted in the first few days of life.
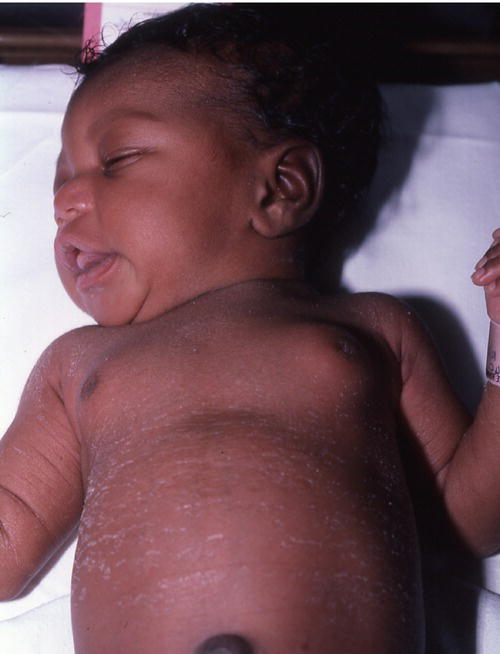
Fig. 21.2 Breast enlargement.
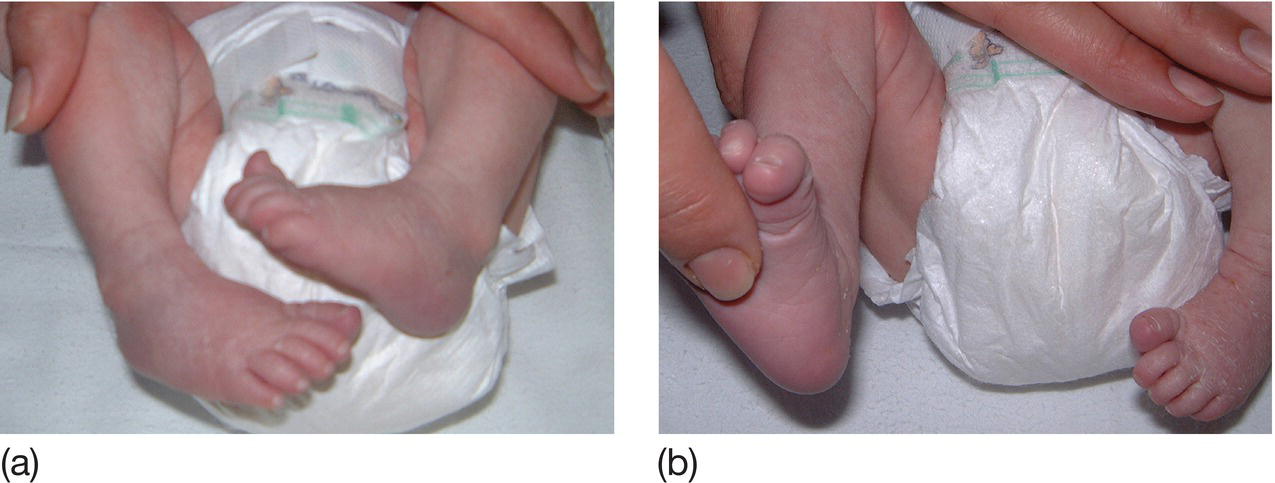
Fig. 21.3 Positional talipes. (a) Position of the feet. (b) The foot can be fully dorsiflexed to touch the front of the lower leg. In true talipes equinovarus this is not possible.

Fig. 21.4 Stork bite (nevus flammeus, salmon patch).
Milia
White, pinhead-sized pimples on the nose and cheeks and fore-head. Resolve during first month of life. Are from retention of keratin and sebaceous material in the pilosebaceous follicles.
Miliaria
Pin-sized vesicles, particularly over the neck and chest. Usually develop at 2–3 weeks. Caused by sweat that is retained due to obstructed eccrine glands. Avoid excessive clothing and heating.
Erythema toxicum
Small, firm, white or yellow pustules on erythematous base (Fig. 21.5). It is the most common transient lesion, usually appears at 1–3 days but up to 2 weeks of age; primarily on trunk, extremities and perineum. Moves to different sites within hours. Contains eosinophils. May be present at birth.
Mongolian spots
Blue–black macular discoloration at base of the spine and on the buttocks (Fig. 21.6). Usually but not invariably in Black or Asian infants. Sometimes also on the legs and other parts of the body. Fade slowly over the first few years. Of no significance unless misdiagnosed as bruises.
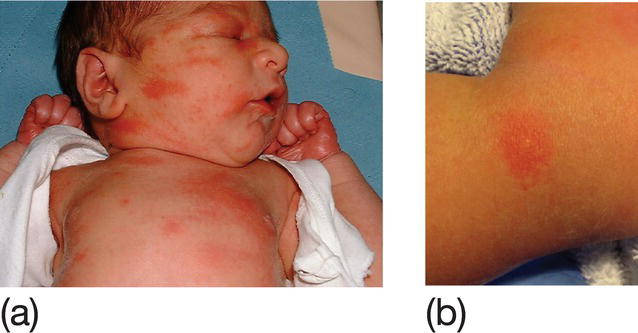
Fig. 21.5 (a) Erythema toxicum showing patchy pustules on erythematous base. (b) Close-up of skin lesion.
(Courtesy of Dr Nim Subhedar.)

Fig. 21.6 Mongolian spot.
Transient pustular melanosis (transient neonatal pustulosis)
Resembles miliaria, but present at birth and may continue to appear for several weeks. Superficial vesiculo-pustular lesions rupture within 48 hours to leave small pigmented macules with white surround. More common in Black infants, in whom the lesions are often hyperpigmented.
Harlequin color change
Sharply demarcated blanching down one half of the body – one side of the body red while the other is pale. Lasts a few minutes. Thought to be due to vasomotor instability. It is benign.
Sucking blisters
Vesicles on hand, fingers or lips, from vigorous sucking in utero.