Chapter 8
Legs: Muscle Isolation
At last, exercises for the legs. Maybe now you’ll gain the strength for that killer shot, the 60-yard goal kick, or the accurate penetrating pass out of the back that shreds the defense. Soccer is primarily about the legs. All other exercises are for support. Let’s get to the good stuff.
For most sports, the power behind the activity comes from the legs. Even sports that emphasize the arms build momentum from the ground up. Problems in the legs can affect the arms and shoulders. For example, the damaged shoulder of baseball pitching legend Jay Hanna Dean, better known as Dizzy Dean, began with a toe injury. A soccer player who does not have a good foundation may soon find a lack of balance, agility, and more affecting his soccer skills. Ill-timed or poorly executed actions above the legs can be seen as poor skill execution. Players who spend too much time working their legs while neglecting the rest of the body will never be the players others thought they could be.
Players make the greatest gains in developing a stronger shot or a longer goal kick by kicking. Improvements in velocity and distance are due mostly to the coordinated timing of all the complex mechanical actions of kicking with the recruitment of the optimal muscle fibers at the instant of ball contact. Improving strength improves general motor skill performance and prevents injury.
Bones, Ligaments, and Joints of the Legs
The leg is made up of three main bones. The femur (thigh bone) is above the tibia (shin bone), which is parallel to the fibula. The patella (knee cap) has no direct bony connection to the femur or tibia because it is embedded in the back of the tendon of the large thigh muscle, the quadriceps femoris. The foot and ankle are a complex mix of seven tarsals, five metatarsals, and 14 phalanges. Although the actions and dexterity of the foot are less than in the hand, the foot is no less complex.
The hip, knee, and ankle are the three primary joints of the leg, but there are more. The hip is the classic ball-and-socket joint. It is a very strong, sturdy joint whose integrity is supported by three very strong ligaments that begin on the pelvis and wrap around the neck of the femur. The hip has good range of motion, but not as good as the shoulder. The primary actions are flexion (swinging the thigh forward) and extension (swinging the thigh back), abduction (moving the leg sideways away from the body) and adduction (swinging the leg from the side back to the midline), internal rotation (rotating the thigh in toward the midline) and external rotation (rotating the thigh away from the midline), and circumduction (swinging the leg around in a circular motion).
The knee, where the femur sits on top of the flat surface of the tibia, is the definitive hinge joint. There is also the patellofemoral joint, where the patella glides along a smooth surface of the femur. The patella doesn’t attach to the femur per se. Although the knee is a hinge joint like the fingers, it is a very complex joint. The real magic of the knee is in its ligaments. The medial collateral ligament, or MCL, connects the femur and tibia on the medial side of the knee, between the knees. The lateral collateral ligament, or LCL, connects the femur and tibia on the lateral side of the knee, on the outside surface. These ligaments prevent the bones from getting into an extreme bow-legged or knock-kneed arrangement. The classic clip block in American football can damage the MCL.
Within the knee joint are the two cruciate ligaments. Both begin on the tibia and insert within the large notch at the end of the femur. The anterior cruciate ligament (ACL) begins in the front and runs diagonally toward the lateral wall of the notch, while the larger posterior cruciate ligament (PCL) begins in the back and crosses behind the ACL to insert on the medial wall of the notch. These two ligaments prevent the femur and tibia from twisting on each other. The ACL also prevents the tibia from shifting too far forward, and the PCL prevents the tibia from shifting too far backward.
The knee also has a pair of crescent-shaped cups of cartilage called the medial meniscus and lateral meniscus. Another cartilage, called articular cartilage, covers the surfaces of the femur and tibia and the back of the patella. The two menisci and the articular cartilage support the free movement of the knee and are frequently damaged during sports such as soccer. An injury to the meniscus can create a sharp edge that can damage the articular cartilage, and when this happens, you are on the fast track to osteoarthritis. A big problem with an ACL injury and the resulting instability is the risk of early-onset arthritis.
The main actions of a hinge joint are flexion (bending the knee) and extension (extending the knee). But the knee is more than a hinge joint because of smaller but no less important movements such as rotation of the femur and tibia with each other. Another frequently mentioned movement is a valgus (knock-kneed) or varus (bow-legged) motion that usually occurs in response to some force exerted from the opposite side. A physician can test the varus and valgus instability of a knee by prying open the medial or lateral side of the joint, which sounds worse than it is. When you hear that someone tore an ACL when her knee went into an apparent valgus, the knee looks knock-kneed, but the actual motion is a combination of knee flexion and internal rotation of the femur at the hip. The knee is far more complex in its structure and function than we yet understand. Orthopedic surgeons who specialize in the knee learn something new nearly every day.
The fibula is a thin bone that runs parallel to the tibia. The bony connection between the tibia and fibula up near the knee is quite strong, but it is not as strong down at the ankle. Those large knots on the inside and outside of your ankle (each is called a malleolus) are actually the ends of each bone. They form a sort of pincer-like grasp on the top tarsal, the talus. Ligaments connect the ends of each bone with nearby tarsals to add stability to the ankle. The primary actions of the ankle are inversion and eversion plus plantar flexion and dorsiflexion. Inversion is rolling the sole of your foot inward, and eversion is rolling the sole outward. Flexion and extension of the foot are more properly called dorsiflexion (pointing your toes up) and plantar flexion (pointing your toes down). The powerful kicking motion is done with a plantar-flexed ankle. The anatomy of the ankle makes it likely that you will sprain the outside of your ankle (an inversion sprain) far more often than the inside of your ankle (an eversion sprain). With sufficient force, the talus can force the tibia and fibula out of parallel, resulting in what is often called a high ankle sprain.
Just like the hand and wrist, the ankle and foot have a dizzying array of ligaments for proper bony alignment. The same naming conventions for the bones of the hand and wrist apply, only with metatarsals instead of metacarpals.
Muscles of the Legs
Some of the muscles that originate on the pelvis, insert on the femur, and act to move the leg are described in chapter 6. The muscles that act on the knee, foot, and ankle are the topic of this chapter.
The thigh muscles are in three primary groups. The quadriceps femoris (the four-headed muscle in the thigh, or femoral, region) has four distinct originations. The three vasti muscles—the vastus medialis, vastus lateralis, and vastus intermedius—all begin along the long shaft of the femur (figure 8.1). (Vastus is Latin for huge.) The fourth head is the rectus femoris, which begins on the pelvis around the socket where the femur articulates with the pelvis. You can easily see three of the quads, but the vastus intermedius is underneath the other three. These four muscles come together to form the common quadriceps tendon that passes over the patella and down to insert on the knot on the tibia just beyond the knee. In one of those anatomical naming quirks, once the quadriceps tendon goes past the patella, its name changes to the patellar ligament. Since a muscle pulls its insertion toward its origin, when the quadriceps contracts, the knee extends. The rectus femoris begins on the pelvis and also assists in hip flexion.
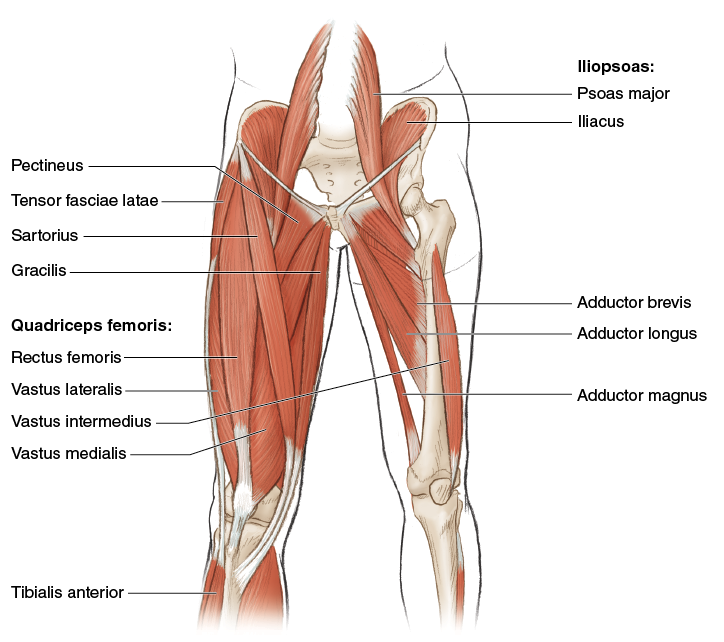
Figure 8.1 Muscles of the front of the leg.
The three muscles that make up the hamstrings (figure 8.2) are the opposite, antagonistic muscles to the quadriceps. They all begin on the pelvis. The biceps femoris is the lateral and largest of the three; it inserts down near the top of the fibula. The semitendinosus and semimembranosus run down the medial side of the thigh and insert behind the medial side of the knee. Most people can find at least two if not all three of these tendons. The main action of the hamstrings is knee flexion, but because all the muscles originate on the hip, they also perform hip extension. The hamstrings also play an important role in protecting the ACL from injury.
The muscles commonly referred to as the groin muscles all begin on the pelvis near the midline and run diagonally down and laterally to insert on the femur. Most are referred to as adductors, muscles that move the thigh toward the midline of the body. They range from quite small (pectineus) to progressively bigger (adductor brevis, adductor longus) to very large (adductor magnus) or very long (gracilis). The adductor longus is particularly susceptible to a strain injury in soccer players. All of these muscles assist in external rotation of the femur and more. You can’t appreciate all these muscles do until you strain a groin and feel pain with nearly every step.
One final muscle of the thigh, sort of, is the tensor fasciae latae. The tensor fasciae latae is more tendon than muscle. This short, flat muscle originates on the crest of the hip, and the short fibers run down the outside of the thigh, ending roughly in the area of that knot felt on the side of your hip. Depending on your height, the fleshy portion might be 4 to 6 inches (10 to 15 cm) in length. From here, the tensor fasciae latae is mostly tendon all the way down the outside of the thigh, and it inserts on the mass of soft tissue that surrounds the knee. It abducts, medially (internally) rotates, and helps flex the hip.
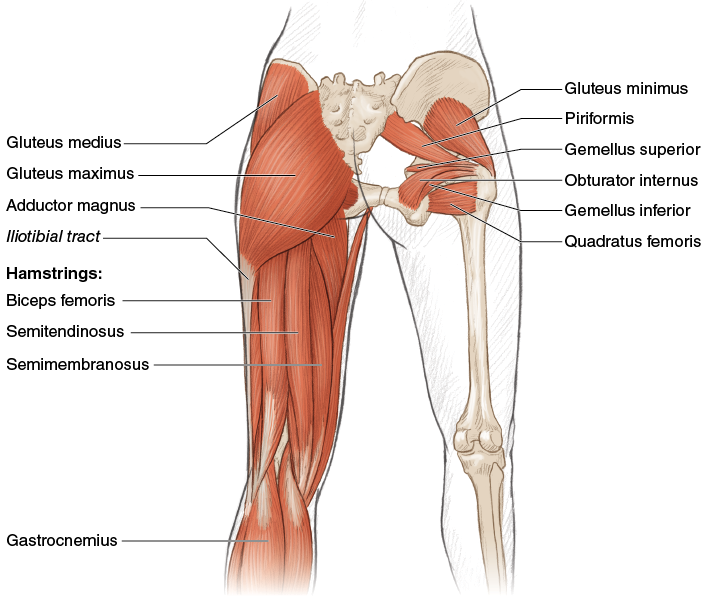
Figure 8.2 Muscles of the back of the leg.
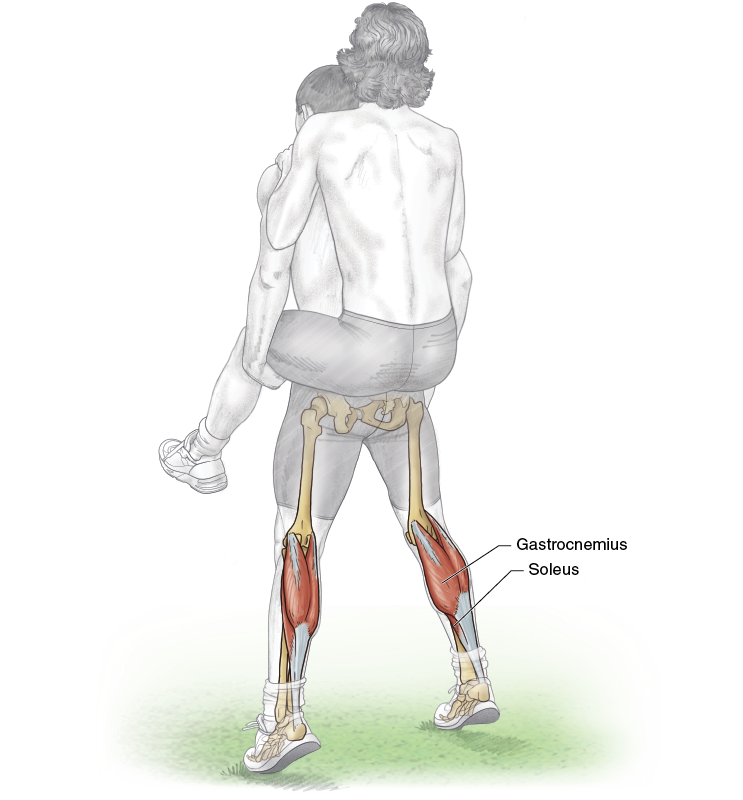
Beyond the knee is a series of muscles that move the ankle, foot, and toes (figure 8.3). Originating along the front of the tibia are muscles that dorsiflex the ankle and others that go all the way to the toes for extension. On the lateral (outside) of the leg is a group of three peroneal muscles that originate on the fibula and mostly evert the foot but also assist in other actions. On the back of the leg are two major muscles. The gastrocnemius, which originates on the back of the femur and often is called the calf muscle, lies over the soleus, which originates on the tibia. The tendons of these two muscles join to become the Achilles tendon, which inserts on the heel (calcaneus). When these muscles contract, you rise up on your toes. They also contribute to your ability to jump and push off the ground during walking and running. These muscles are organized as distinct groups in the anterior, lateral, and posterior compartments of the leg. No muscles are considered medial.

Figure 8.3 Muscles of the lower leg and foot: (a) back and (b) front.
Toe Raise Carrying Partner
Execution
1. Find a partner who is about the same height and weight as you.
2. Have your partner climb onto your back in a piggyback fashion.
3. Perform slow, controlled toe raises by rising as high as possible with each attempt. Swap positions and repeat.
Muscles Involved
Primary: Gastrocnemius, soleus
Secondary: Erector spinae and other accessory back muscles (such as latissimus dorsi and external oblique)
Soccer Focus
Jumping power comes from the coordinated contribution of hip extension, knee extension, and plantar flexion (rising up on the toes). All these muscle groups need to be trained so that each can contribute appropriately during a jump. The calf muscles are also involved in running because much of the power in the push-off portion of the gait cycle comes from the gastrocnemius and soleus. This is especially true during the initial takeoff and acceleration in sprinting. The increase in stride length with faster speeds is in large part due to a stronger push-off from the gastrocnemius and the soleus. In addition, the calf muscles are strong contributors to the rigid locking of the ankle when striking the ball. Much of the power built up in the leg during the swing phase of kicking can be lost if the foot and ankle are not rigid at ball contact.
Variation
Machine Toe Raise
This exercise, also known as the standing calf raise, really isolates the gastrocnemius and soleus, with the gastrocnemius producing the more force of the two. The muscles can be further challenged by standing on a board or step to add an additional stretch over a greater range of motion. The demand on the soleus muscle increases if the knees are slightly bent during toe raises.
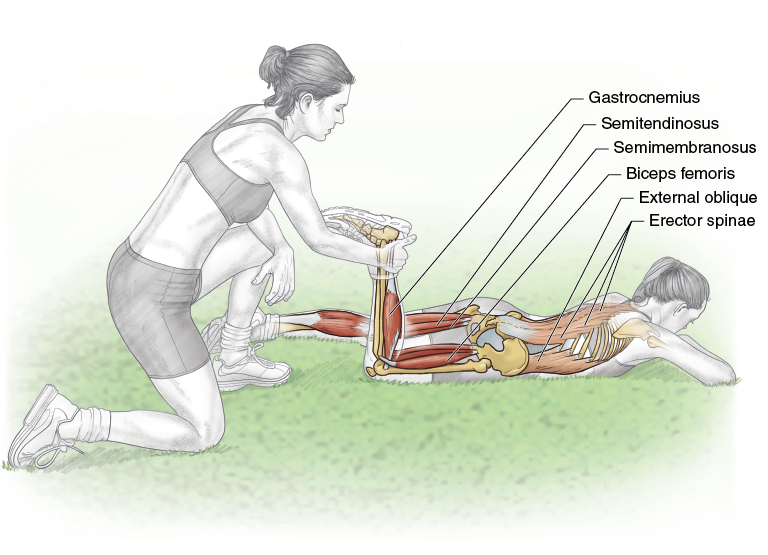
Partner Prone Leg Curl
Execution
1. Lie prone on the ground, with one knee extended and the other knee flexed.
2. Your partner kneels at your feet and holds the ankle of your flexed leg.
3. Perform knee flexion, curling the leg, while your partner resists the motion, allowing the flexion through the range of motion.
4. Switch legs and repeat with the other leg. After exercising both legs, switch places with your partner.
Muscles Involved
Primary: Hamstrings (biceps femoris, semitendinosus, semimembranosus), gastrocnemius
Secondary: Abdominal core (external oblique, internal oblique, transversus abdominis, rectus abdominis), erector spinae for core stabilization and posture
Soccer Focus
For earlier generations of soccer players, a hamstring strain was a rare injury. The pace and ballistic nature of the modern game have made this previously rare injury the number one soccer injury, according to some studies. Some studies show that professional teams see six or more hamstring strains a year. And these take awhile to heal, which means a team could be without a number of core players for an extended period of time. There are three risk factors for a hamstring strain. The strongest predictor of a strain, or almost any injury, is a history of a previous strain injury. Next, the older the player, the more likely he is to suffer a strain. Finally, poor hamstring strength increases the risk of a strain. Notice that of these three factors, the only one that can be modified is strength. Thus, it is wise to improve hamstring strength to prevent this serious strain injury.

Variation
Machine Knee Flexion
Hamstring strength can be improved by using a machine designed for standing, prone, or seated leg curls. Regardless of the positioning, the knee flexion isolates the motion to the hamstrings and will effectively increase strength. The greatest strength gain and reduction in strain injury come from performing the hamstrings exercise, sometimes called the Nordic curl, in the FIFA warm-up (page 30).
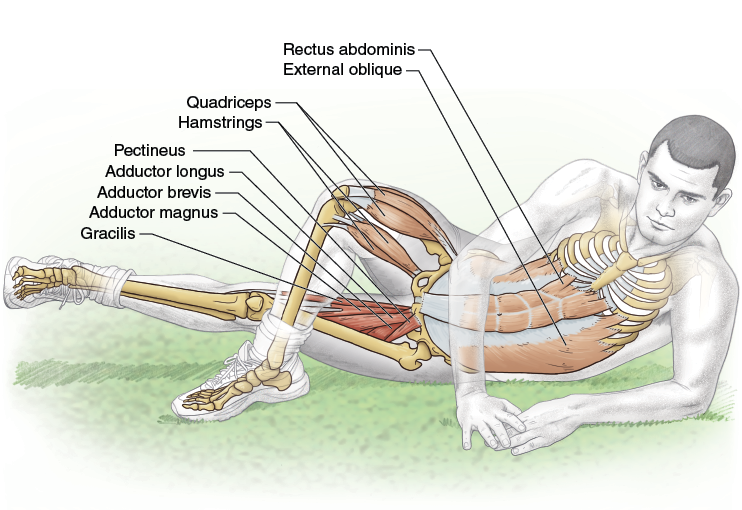
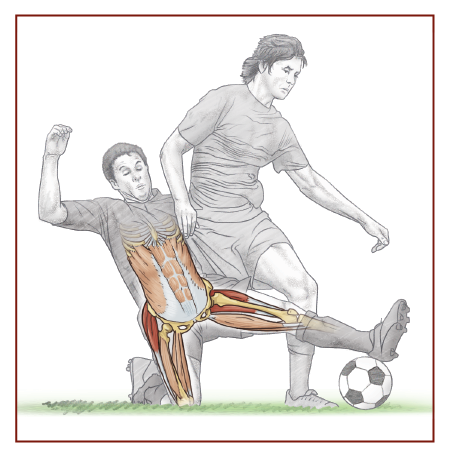
Lying Adduction
Execution
1. Lie on the ground on your side.
2. Flex your upper leg, and place the foot flat on the ground in front of the thigh of the lower leg. The lower leg is fully extended.
3. Slowly raise the lower leg off the ground. Hold briefly at the highest position, and then return to the starting position.
4. Switch sides and repeat on the other leg.
Muscles Involved
Primary: Adductors (adductor longus, adductor brevis, adductor magnus, pectineus, gracilis)
Secondary: Abdominal core for posture, quadriceps (vastus medialis, vastus lateralis, vastus intermedius, rectus femoris) and hamstrings to maintain an extended knee
Soccer Focus
A sport’s pattern of activity can lead to some particular deficiencies. Soccer players are famous for poor flexibility about the knee, groin, and ankle. Are these weaknesses due to the nature of the sport or the lack of attention to improving flexibility? Poor flexibility is considered a risk factor for a variety of injuries including groin strains, which can happen while defending or blocking a pass or shot; while taking a very hard shot; or during a rapid reactive change of direction. The most commonly injured groin muscle is the adductor longus. Most people don’t realize how much the groin muscles are used during normal daily activities until one is injured. The leg is attached to the pelvis through a ball-and-socket joint (the hip) that allows the leg to pivot around the joint. During flexion and extension, the leg can move through a rather large cone-shaped range of motion, but the action of the adductors helps minimize the sideways motion of the leg as it moves through hip flexion and extension. Those who have suffered groin strains usually are receptive to supplemental exercises that help strengthen the adductors to prevent or delay the next strain. Another pesky groin injury is a sports hernia, sometimes called athletic pubalgia (see chapter 2, page 16). Although the pain is situated in the groin, the actual problem can lie elsewhere, and the player may not be able to recall exactly when the injury occurred. See a sports medicine physician for an accurate diagnosis because the treatments for a groin strain and a sports hernia are quite different.
Variation
Cable Hip Adduction
The lying adduction exercise can be performed on the field. But the only way to continue to train the adductors on the field is to do more repetitions, increasing local muscle endurance more than pure strength of the adductors. (I have even seen some teams bring ankle weights to the field.) To really increase adductor strength, go to the weight room and use the cable machine so you can add resistance.
Fire Hydrant
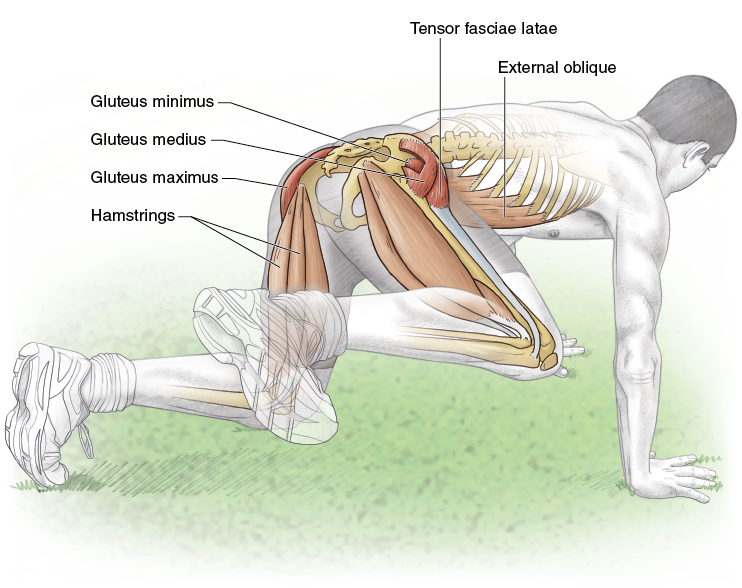
Execution
1. Get on all fours on the ground.
2. Raise one flexed leg to the side until the leg is parallel to the ground. Pause briefly and then lower the leg back to the starting position.
3. Switch legs, raising the other leg to the side until it is parallel to the ground. Alternate legs.
Muscles Involved
Primary: Gluteals (gluteus maximus, medius, and minimus), tensor fasciae latae
Secondary: Vastus lateralis, hamstrings, abdominal core for posture and balance
Soccer Focus
The hip is a curious joint when it comes to sports injury. Not many players remember a specific inciting event, one they can pinpoint as causing the hip injury. But a substantial number of retired players have undergone total hip replacements at an age most would consider too young for new hips. It seems the lack of control of the femur within the pelvis causes minor defects in the socket portion of the joint that, over time, will wear down and eventually need to be replaced. Because strength is important in joint stability, look for exercises such as this one that can be used to improve the muscles around the hip joint. This exercise works the various muscles involved in hip abduction. At the same time, when done properly by taking the thigh through a wide range of motion, the fire hydrant is also a great dynamic stretch of the adductors. It should be easy to see where this exercise gets its name.
Variation
Machine Abduction
Most activities have both a field and a machine-based version. This machine exercise is done in a seated posture. Place your knees between the padded arms of the machine, and spread your legs as much as possible. Varying the angle of the seat is said to change the primary location of the muscle fibers being recruited.
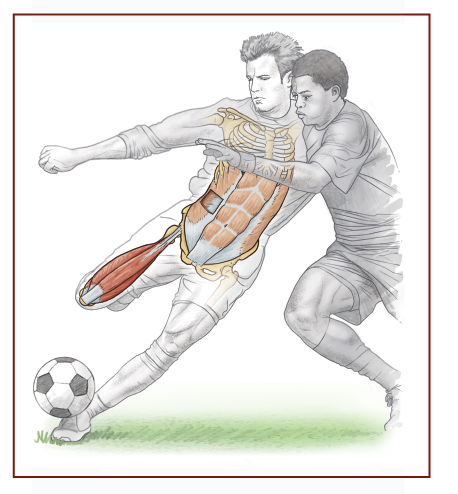
Cable Kickback

Execution
1. Stand and face a cable machine or other stable object. Loop the rope or strap or a resistance band around one ankle.
2. Keeping the leg as straight as possible, extend the leg at the hip (move it backward) as far as possible. Pause briefly and then return to the starting position. If necessary, hold onto the machine for balance.
3. Switch legs and repeat with the other leg.
Muscles Involved
Primary: Gluteus maximus, hamstrings
Secondary: Abdominal core for posture, muscles of the balancing leg (such as quadriceps, gastrocnemius, soleus, peroneus longus, peroneus brevis, and peroneus tertius)
Soccer Focus
Any movement that results in a ball being thrown or kicked requires some sort of a windup. The longer the windup, the farther or faster the ball will go. The anatomy of the hip joint as well as a specific ligament of the hip (the iliofemoral, or Y ligament) limits the backswing of a kick. Kicking is not just about the forward swing of the kicking leg. You can increase your power by increasing the strength of the hip extensors so that you use as much of the motion available for the windup as possible.

Variation
Stability Ball Hip Extension
A hip extension variation can be performed with a stability ball. Lie on the floor with one foot high up on the ball. Cross the other leg over the leg on the ball. Push against the floor and ball to extend the hip. The stability ball increases the difficulty by adding a balance component to the task.
Seated Leg Extension

Execution
1. Adjust the seat height of the leg extension machine as needed and take a seat. Hook your ankles underneath the pads.
2. Extend the knees. Pause at the top of the movement, and then slowly return to the starting position. Repeat.
Muscles Involved
Primary: Quadriceps
Secondary: Abdominal core for seated posture
Soccer Focus
Knee extension is one of the more obvious movements of kicking. Once the backswing ceases, the hip flexes while the knee remains flexed. As the knee gets close to the ball, hip extension slows and knee extension accelerates rapidly until ball contact. (Actually, the leg starts to slow just before ball contact.) The rapid acceleration of knee extension is what imparts a large fraction of the power for a shot or a long pass. Many studies have attempted to show what weight training does for kicking ability and, while it helps, it’s not as much as you might think. If you want to kick the ball harder or farther, you will gain the most by kicking and a little from lifting. Be realistic about the goals of strength training. For the knee, strength training is about increasing strength to prevent injury, not necessarily to improve kicking performance.
Variation
Single-Leg Extension
This exercise can be done with one leg at a time. For some athletes, the stronger leg will do the bulk of the work during a bilateral exercise, and the weaker leg will go along for the ride. The single-leg extension works one leg at a time, ensuring both legs receive the optimal training stimulus. Also, this and other lifts can be modified by taking twice the time to lower the weight as it takes to raise the weight.
Stability Ball Leg Curl
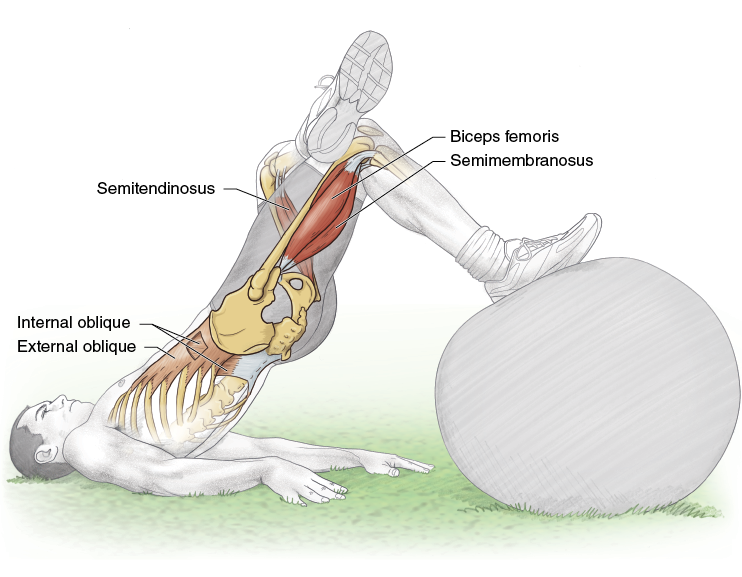
Execution
1. Lie on the ground, and place the heel of one foot high up on the stability ball. Cross the other leg over the knee. Raise your trunk off the ground, and put the weight on your shoulders.
2. Flex the knee, and roll the ball from under the heel to the sole of the foot as far as possible. Pause and then slowly return to the starting position. Switch legs and repeat.
Muscles Involved
Primary: Hamstrings
Secondary: Abdominal core for balance
Soccer Focus
The Soccer Focus section for the partner prone leg curl (page 155) covers the importance of strengthening the hamstrings to protect them from a muscle strain injury. The hamstrings also figure into anterior cruciate ligament tears. Remember, the ACL begins on the front portion of the flat surface of the tibia (leg bone) and courses back to the lateral surface within a big notch at the end of the femur (thigh bone), so it goes in sort of a diagonal direction. Think about its configuration. If you twist your right tibia in a clockwise direction, the ligament gets looser, but if you twist the right tibia in a counterclockwise direction, the ligament tightens. That’s not all. If the tibia slides backward under the femur, the ligament loosens, but if the tibia slides forward, the ligament tightens. The tibia slides forward every time you land from a jump or plant a foot to make a cut. Imagine if the hamstrings contracted just as the tibia started to slide forward. What would happen? The tibia wouldn’t slide forward as far, and you would have protected the ACL from being stretched through the contraction of the strong hamstrings and by calling on the hamstrings at the right time after learning how to land and cut. Strong hamstrings are very important in team sports such as soccer.