CHAPTER 12
Your Fertility Planner
OF COURSE YOU CAN GET PREGNANT the old-fashioned way—stop using birth control, have sex whenever, wherever, in whatever position, and wait for that missed period. Or the even more old-fashioned way—dispense with the birth control altogether, and take an “oops” approach to conception. But there’s definitely an upside to planning your conception—actually many upsides. Taking charge of your fertility planning gives you the opportunity to get your body, your spouse’s body, and your life in tip-top baby-making shape before your conception campaign begins—and gives you a chance to stack the cards in favor of a speedier conception, a safer and more comfortable pregnancy, and a healthier baby. Plus, it gives you an opportunity to put that multitasking control freak in you (yes, you) to work on one of life’s most satisfying projects: baby making. Let the planning begin.
Countdown to Conception
You can never be fully prepared for becoming a parent, or even for becoming pregnant. But when time is on your side (you’re just starting to think about taking the baby plunge), it makes sense to put those pre-baby-making months to the most productive possible use.
The following schedule is a general guide to conception prep (there may be other items you’ll have to add to your specific plan). Don’t stress too much about the exact time frame—more important right now is getting most (if not all) of the items on the agenda crossed off your to-do list before you get cracking on conception.
Another consideration as you count down to conception—just how much to-doing you’ve got to get done (for instance, if you have a hefty number of pounds to lose, you’ll want to get an earlier start on weight loss; if you know that you’ll never be able to quit cigarettes in 3 months, make 6 months your goal). Yet another consideration: your own time frame for getting pregnant. If you want to get busier sooner rather than later, skip right to the 3-month plan.
Six to Twelve Months Out
FOR HER:
 Evaluate your weight and BMI. If you have a lot to lose, start a healthy balanced weight loss program now. If you’re significantly underweight, start eating with an eye on moving those numbers up (and if you have an eating disorder, get treatment now).
Evaluate your weight and BMI. If you have a lot to lose, start a healthy balanced weight loss program now. If you’re significantly underweight, start eating with an eye on moving those numbers up (and if you have an eating disorder, get treatment now).
Start taking a daily prenatal vitamin, if you want. It’s not considered a must-do until 3 months out, but it’s never too early to start catching up on any nutritional deficits. Plus, some research indicates that taking prenatals for a year before conception may reduce the risk for preterm delivery.
If you have substantial problems with your gums and/or teeth, or you suspect you might, get busy having any necessary dental work done.
If you have any chronic medical conditions, take steps to get them under control.
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
FOR HIM:
Evaluate your BMI. If you have a lot of weight to lose, start a healthy balanced weight-loss program now.
If you have any chronic medical conditions, take steps to get them under control.
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
Three Months Out
FOR HER:
Evaluate your weight and BMI. If it needs a little adjusting (up or down), start a healthy balanced weight-loss (or -gain) program now.
Take a look at your eating habits and if they’re not up to prepregnancy par, ease into a healthy eating plan with baby making in mind.
Start taking a daily prenatal vitamin, if you haven’t already.
Cut out smoking. If quitting cold turkey will be too tough, use the next 3 months to cut back slowly until you’re nicotine free.
Begin weaning yourself off prescription and over-the-counter medications (under your doctor’s guidance) that are not conception compatible and substituting those that are.
Ditch hormonal birth control (the Pill, patch, ring) and use only barrier methods for now (condom, diaphragm, spermicides).
Stop using recreational drugs. If you need help quitting, seek it now.
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
FOR HIM:
Evaluate your weight and BMI. If you could drop a few pounds, now’s the time to start a healthy balanced weight-loss program. If you’re too thin, consider beefing up a bit.
Take a look at your eating habits. If there’s room for improvement, now’s a great time to start eating with fertility optimizing in mind.
Take a multivitamin to make sure your body is well stocked for optimal sperm production.
Cut out smoking. If quitting cold turkey will be too tough, use the next 3 months to cut back slowly until you’re nicotine free.
Take stock of your medicine cabinet. With your doctor’s help, begin substituting medications that are compatible with baby making for those that aren’t.
Stop using recreational drugs. If you need help quitting, seek it now.
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
Two Months Out
FOR HER:
See your doctor and/or ob-gyn or midwife for a top-to-bottom checkup to make sure all systems are ready for baby making.
Get a dental checkup and cleaning, if you haven’t recently.
Begin (or continue) a moderate exercise program (aim for 30 minutes each day).
Start to limit the amount of caffeine you get each day (goal: no more than 200 mg, or 2 cups, a day).
Stop dieting for weight loss and continue eating balanced healthy foods that will maintain your loss.
Take a good look at your environment at work. If any occupational hazards might be a problem when trying to conceive (or during pregnancy), find ways to limit your exposure.
Begin charting your basal body temperature (BBT) and your cervical mucus (CM) changes. Mark down any other cycle changes and ovulation signs you notice so you’ll be able to pinpoint ovulation.
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
FOR HIM:
See your doctor for a full-body checkup. Be sure to let him or her know you’re about to start trying for a family and ask if any special tests or exams might be important now.
Evaluate your work environment. If you’re exposed to any hazards that may harm your fertility or the health of your sperm, find ways to limit exposure for now.
Keep cool by staying out of hot tubs, hot baths, and saunas. Treat your laptop as a desktop and keep your cell phone out of your pants pocket.
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
One Month Out
FOR HER:
Start reducing your alcohol intake with the aim of cutting it out altogether once you start trying to conceive.
Make sure your finances are in order, including your insurance policies and will.
Learn ways to relax and try to avoid stressful situations starting now
(as best you can).
Continue tracking your BBT, your CM changes, and other ovulation signs.
Don’t forget that daily vitamin.
Think happy baby thoughts!
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
FOR HIM:
Cut back on alcohol for now to keep your sperm production high and in good baby-making shape.
Cut back on overly strenuous exercise routines (especially heavy-duty bicycling).
Make sure your finances are in order, including your insurance policies and will.
Learn ways to relax and try to avoid stressful situations starting now (as best you can).
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
GO! Now that you’re ready to go, make sure to have sex around ovulation each month, keeping in mind that it could take as long as a year of trying before the right sperm and egg get together.
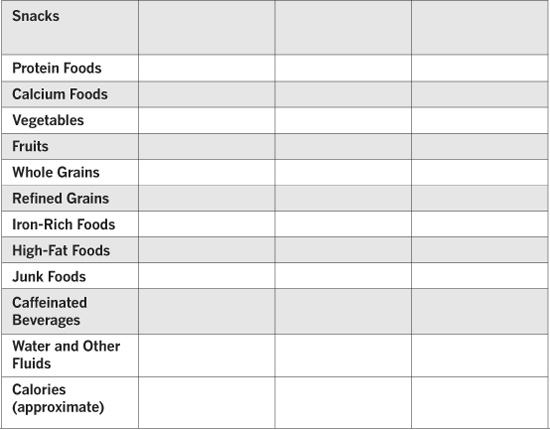
Food Diary
Keep track of your meals and snacks for one week so you can get a clear picture of how you eat and whether you need to do a little preconception diet tweaking.



Health History
When you go for your preconception checkup (which you definitely should), your practitioner will ask you lots of questions about your medical and gynecological health, and will also do some digging into your lifestyle (and your partner’s health and lifestyle, too). To be sure you’re armed with all the info you’ll be asked for, do your homework before the appointment and bring the answers to these routine questions with you.
Your General Health
Age _______ Weight _______ BMI _______ Blood type _______
Chronic conditions
______________________________________________
______________________________________________
______________________________________________
Medications you take regularly (prescription and over-the-counter)
______________________________________________
______________________________________________
______________________________________________
Allergies (including food allergies)
______________________________________________
______________________________________________
______________________________________________
Previous surgeries
______________________________________________
______________________________________________
______________________________________________
Have you had or been vaccinated for:
Measles _____ Mumps _____ Rubella _____ Chicken Pox _____
Date of your last Td or Tdap booster _________________________
Do you have a history of depression?
______________________________________________
______________________________________________
______________________________________________
Are you currently being treated for depression? How?
______________________________________________
______________________________________________
______________________________________________
Other general health issues
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
Your Gynecological History
Date of your last menstrual period ___________________________
Average length of your cycles ______________________________
Date of last Pap smear and results ___________________________
Date(s) of any abnormal Pap smears and treatment you have received
______________________________________________
______________________________________________
Birth control use _________________________________________
Do you know if you have fibroids? __________________________
What symptoms, if any, do you have? ________________________
______________________________________________
______________________________________________
Do you know if you have endometriosis? ______________________
What symptoms do you have? ______________________________
______________________________________________
______________________________________________
Do you have any other gynecological conditions? _______________
______________________________________________
______________________________________________
Have you ever had a sexually transmitted disease? ______________
______________________________________________
______________________________________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
Your Reproductive History
Have you ever had any fertility issues? ________________________
Number of previous pregnancies ______ Ages of children ________
Have you ever had a miscarriage?____________________________
How many? _________________ When? _____________________
How far along was the pregnancy? ___________________________
______________________________________________
Have you ever had an ectopic pregnancy? _______ When? ________
______________________________________________
Have you ever had an abortion? _________ How many? __________
______________________________________________
Have you ever had a stillbirth? ______________________________
______________________________________________
Were there any complications during your pregnancies? __________
______________________________________________
______________________________________________
______________________________________________
Were there any delivery complications? _______________________
______________________________________________
______________________________________________
______________________________________________
Were the deliveries vaginal or via C-section? ___________________
Did you ever have any postpartum complications? _______________
______________________________________________
______________________________________________
______________________________________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
Your Lifestyle
Do you smoke? _____ How much? __________________________
Do you drink alcohol? _______ How much? ___________________
Do you use any recreational drugs (cocaine, marijuana)? _________
How much caffeinated coffee, tea, or soda do you drink? _________
______________________________________________
How would you describe your eating habits? ___________________
______________________________________________
Typical breakfast: ________________________________________
______________________________________________
Typical lunch: ___________________________________________
______________________________________________
Typical dinner: __________________________________________
______________________________________________
Typical snacks: __________________________________________
______________________________________________
Do you exercise? ____ What type(s) of exercise, and how often? ___
______________________________________________
Do you take vitamins or any herbal preparations? __ If so, what kinds? __
______________________________________________
______________________________________________
Do you use acne medications? ______ If yes, what kind? _________
______________________________________________
Are you exposed to any environmental hazards at work or at home? _
______________________________________________
Are you under any excessive emotional stress? _________________
______________________________________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
Your Partner’s Health and Lifestyle
Age ____ Height ____ Weight ____ BMI ____ Blood type ____
Chronic conditions _______________________________________
______________________________________________
______________________________________________
Other general health issues _______________________________________________________
______________________________________________
______________________________________________
Medications he takes regularly _______________________________________________________
______________________________________________
Vitamins and supplements he takes regularly ___________________
______________________________________________
Does he smoke? ________________ How much? _______________
Does he drink alcohol? ____________ How much? _____________
Does he use recreational drugs? _____________________________
Does he exercise? _______ What type(s) and how often? _________
______________________________________________
______________________________________________
Is he exposed to environmental hazards at work or at home? _______
______________________________________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
Your Family History
Your ethnicity _______________________________
Your partner’s ethnicity _____________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
Have you, your partner, or anyone in your family or your partner’s family had:


Questions You May Have
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
Additional Questions or Notes
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
Tracking Your Cycle
Ready to keep an eye on the calendar? Using this month-at-a-glance calendar (or any calendar you choose), fill in the appropriate dates and then circle the first day of each monthly period. After a few months, you’ll be able to determine your natural cycle length. Count back 12 to 16 days each month to get an idea of when you likely ovulated during the previous cycle. This will help narrow down when you’ll likely be ovulating next cycle, and when you should schedule in sex. Shade those fertile days to keep track.







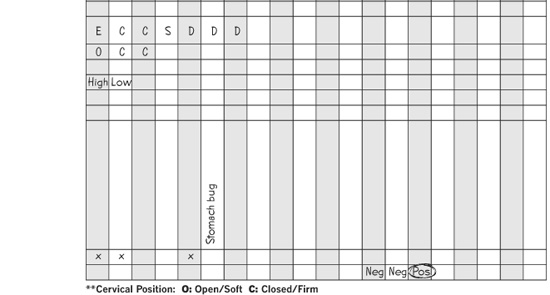
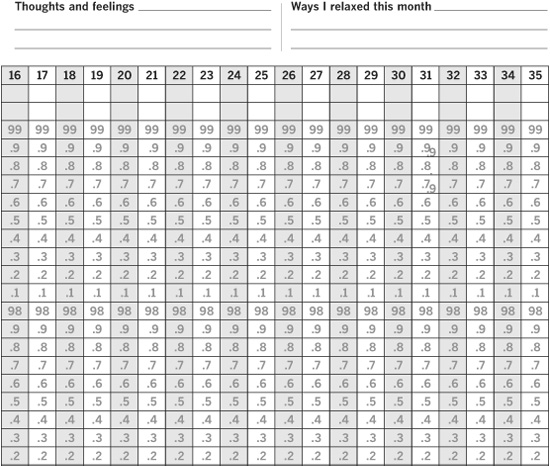
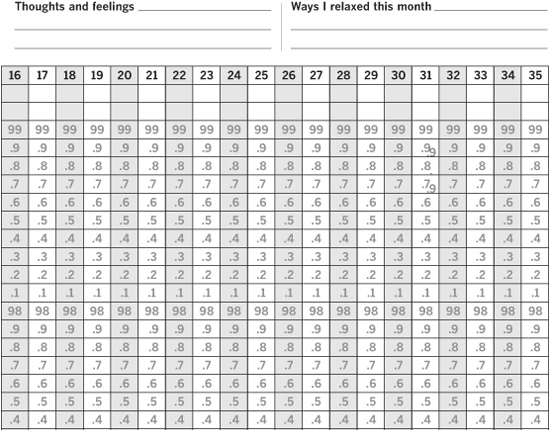
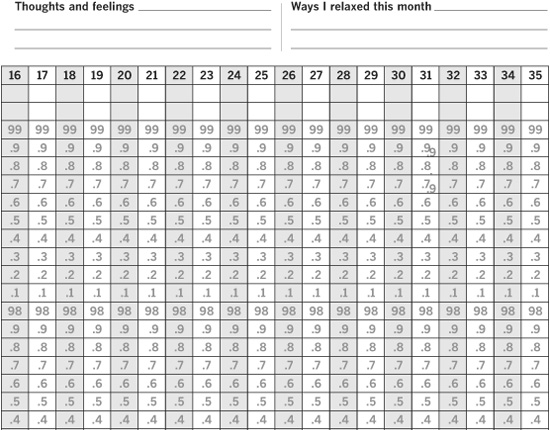
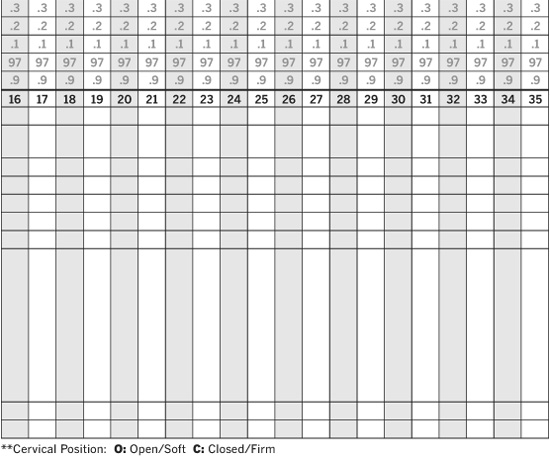
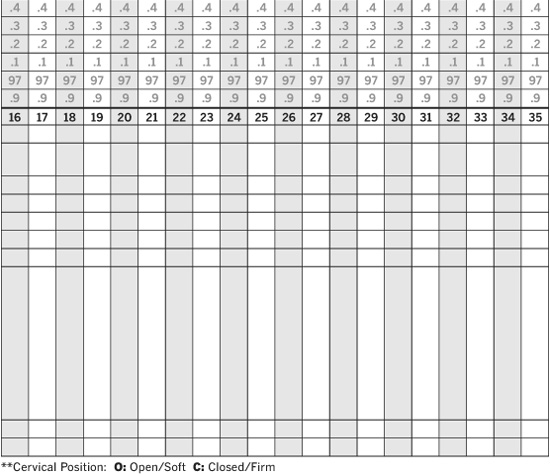
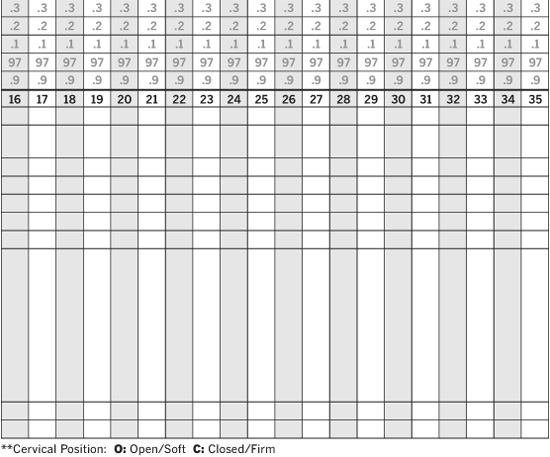
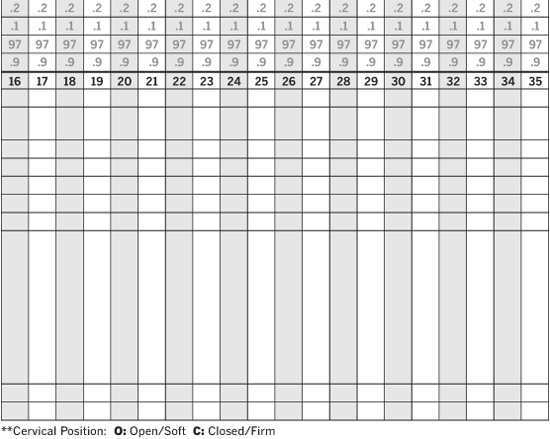
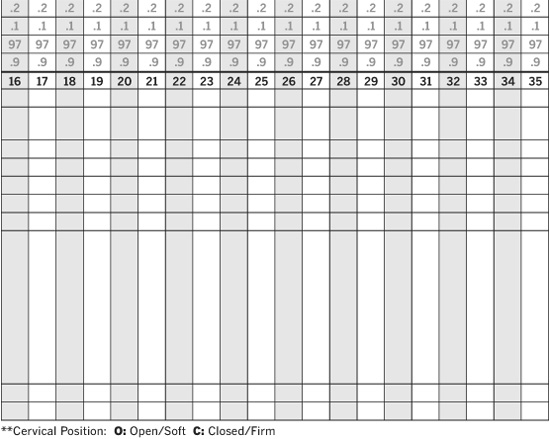
Your Fertility Charts
This all-in-one fertility chart will let you keep track of all your ovulation and fertility signs, enabling you to better pinpoint when ovulation is happening (and when you should start getting busy in bed). Begin a few months before you start TTC so you can get a head start. Here’s how to put it all together:
- Using a digital basal thermometer, take your temperature each morning before you get out of bed and mark each daily reading on the graph. Connect the dots to help pinpoint ovulation.
- In the row marked “Cervical Mucus Consistency,” note the consistency of your CM (dry, sticky, creamy, or slippery) as detailed on page 88 to help identify when you’re most fertile.
- You can mark down whether your cervix is opened or closed in the row marked “Cervical Position.”
- Fill in the appropriate boxes and corresponding dates in the rows marked “Period/Spotting,” “Miscellaneous,” and “Intercourse.”
- Finally, if you’re using any fertility monitors, OPKs, saliva tests, or chloride ion (fertility watch) tests, you can input the results on this chart as well in the appropriate spaces.
- If you’ve figured out your ovulation day, circle it.
- If you’re taking a home pregnancy test (HPT) this month, input the results in the appropriate boxes.
- Record your thoughts and feelings during the charting cycle, and keep track of the time you spend each month relaxing (important when you’re in the baby-making mode).
Fertility Treatment Planner
Do your conception plans need a little push in the right direction from reproductive science? If so, you’re probably going to have a lot more doctor appointments, medications, tests, and other treatments to keep track of. Use this fertility treatment planner to stay on top of it all.
Fertility Tests
Test ___________________________________________________
Date/Place ______________________________________________
______________________________________________
Doctor _________________________________________________
When/Where to call for results ______________________________
______________________________________________
Results _________________________________________________
______________________________________________
______________________________________________
Follow-up tests needed, if any _______________________________
______________________________________________
______________________________________________
Test ___________________________________________________
Date/Place ______________________________________________
______________________________________________
Doctor _________________________________________________
When/Where to call for results ______________________________
______________________________________________
Results _________________________________________________
______________________________________________
______________________________________________
Follow-up tests needed, if any _______________________________
______________________________________________
Test ___________________________________________________
Date/Place ______________________________________________
______________________________________________
Doctor _________________________________________________
When/Where to call for results ______________________________
______________________________________________
Results _________________________________________________
______________________________________________
______________________________________________
Follow-up tests needed, if any _______________________________
______________________________________________
______________________________________________
Test ___________________________________________________
Date/Place ______________________________________________
______________________________________________
Doctor _________________________________________________
When/Where to call for results ______________________________
______________________________________________
Results _________________________________________________
______________________________________________
______________________________________________
Follow-up tests needed, if any _______________________________
______________________________________________
______________________________________________
Test ___________________________________________________
Date/Place ______________________________________________
______________________________________________
Doctor _________________________________________________
When/Where to call for results ______________________________
______________________________________________
Results _________________________________________________
______________________________________________
______________________________________________
Follow-up tests needed, if any _______________________________
______________________________________________
Fertility Specialist Visits
Date ___________________________________________________
Doctor seen _____________________________________________
Doctor’s recommendations _________________________________
______________________________________________
______________________________________________
______________________________________________
Date ___________________________________________________
Doctor seen _____________________________________________
Doctor’s recommendations _________________________________
______________________________________________
______________________________________________
______________________________________________
Date ___________________________________________________
Doctor seen _____________________________________________
Doctor’s recommendations _________________________________
______________________________________________
______________________________________________
______________________________________________
Date ___________________________________________________
Doctor seen _____________________________________________
Doctor’s recommendations _________________________________
______________________________________________
______________________________________________
______________________________________________
Date ___________________________________________________
Doctor seen _____________________________________________
Doctor’s recommendations _________________________________
______________________________________________
______________________________________________
Date ___________________________________________________
Doctor seen _____________________________________________
Doctor’s recommendations _________________________________
______________________________________________
______________________________________________
______________________________________________
Date ___________________________________________________
Doctor seen _____________________________________________
Doctor’s recommendations _________________________________
______________________________________________
______________________________________________
______________________________________________
Date ___________________________________________________
Doctor seen _____________________________________________
Doctor’s recommendations _________________________________
______________________________________________
______________________________________________
______________________________________________
Date ___________________________________________________
Doctor seen _____________________________________________
Doctor’s recommendations _________________________________
______________________________________________
______________________________________________
______________________________________________
Date ___________________________________________________
Doctor seen _____________________________________________
Doctor’s recommendations _________________________________
______________________________________________
______________________________________________
Fertility Medications
Name of medication/injection _______________________________
______________________________________________
Amount to take ________________ How to take ________________
Time of day _________________ For this long _________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Name of medication/injection _______________________________
Amount to take ________________ How to take ________________
Time of day _________________ For this long _________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Name of medication/injection _______________________________
Amount to take ________________ How to take ________________
Time of day _________________ For this long _________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Name of medication/injection _______________________________
Amount to take ________________ How to take ________________
Time of day _________________ For this long _________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Name of medication/injection _______________________________
Amount to take ________________ How to take ________________
Time of day _________________ For this long _________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Name of medication/injection _______________________________
Amount to take ________________ How to take ________________
Time of day _________________ For this long _________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Name of medication/injection _______________________________
Amount to take ________________ How to take ________________
Time of day _________________ For this long _________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Name of medication/injection _______________________________
Amount to take ________________ How to take ________________
Time of day _________________ For this long _________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Fertility Procedures
Procedure ______________________________________________
Date/Place ______________________________________________
Doctor _________________________________________________
Follow-up needed, if any __________________________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Procedure ______________________________________________
Date/Place ______________________________________________
Doctor _________________________________________________
Follow-up needed, if any __________________________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Procedure ______________________________________________
Date/Place ______________________________________________
Doctor _________________________________________________
Follow-up needed, if any __________________________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Procedure ______________________________________________
Date/Place ______________________________________________
Doctor _________________________________________________
Follow-up needed, if any __________________________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Procedure ______________________________________________
Date/Place ______________________________________________
Doctor _________________________________________________
Follow-up needed, if any __________________________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Procedure ______________________________________________
Date/Place ______________________________________________
Doctor _________________________________________________
Follow-up needed, if any __________________________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Procedure ______________________________________________
Date/Place ______________________________________________
Doctor _________________________________________________
Follow-up needed, if any __________________________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Procedure ______________________________________________
Date/Place ______________________________________________
Doctor _________________________________________________
Follow-up needed, if any __________________________________
NOTES: _______________________________________
______________________________________________
______________________________________________
______________________________________________
Contacts
______________________________________________
General Health Physician
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
E-mail __________________________________________
Gynecologist (GYN)
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
E-mail __________________________________________
Obstetrician/Gynecologist (OB/GYN) or Midwife
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
E-mail __________________________________________
Reproductive Endocrinologist (RE)
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
E-mail __________________________________________
Ultrasound Center
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
CAM Therapist
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
E-mail __________________________________________
CAM Therapist
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
E-mail __________________________________________
Therapist
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
E-mail __________________________________________
NOTES: _________________________________
________________________________________
________________________________________
__________________________________________
Other Specialist
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
E-mail __________________________________________
Lab
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
Hours ___________________________________________
Pharmacy
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
Hours ___________________________________________
Insurance Company
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
Website
NOTES: _________________________________
________________________________________
________________________________________
__________________________________________
Other Contacts
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
E-mail __________________________________________
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
E-mail __________________________________________
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
E-mail __________________________________________
Name ___________________________________________
Address _________________________________________
Telephone _______________________________________
Fax ____________________________________________
E-mail __________________________________________
NOTES: _________________________________
________________________________________
________________________________________
__________________________________________
TTC Glossary
Spend a little time on those TTC message boards, and you’ll soon discover that “TTC” is far from the only acronym used by those who are trying to conceive. Here’s a short—though still pretty long—list of some of the acronyms you may encounter during your conception adventure. You may well come across others–and if you do, you can jot them down here so you can keep them straight:
2WW |
Two-Week Wait (until you can take a pregnancy test) |
AF |
Aunt Flo(w), your period |
BBT |
Basal Body Temperature |
BD |
Baby Dance, sex |
BFN |
Big Fat Negative (pregnancy test result) |
BFP |
Big Fat Positive (pregnancy test result) |
BMS |
Baby-Making Sex |
CD |
Cycle Day |
CF |
Cervical Fluid |
CL |
Corpus Luteum |
CM |
Cervical Mucus |
CP |
Cervical Position |
CY |
Cycle |
DI |
Donor Insemination |
DP |
“Dancing” Partner; spouse or significant other |
DPO |
Days Past Ovulation |
DTD |
Doing The Dance, Sex |
EW |
Egg White (re: consistency of cervical mucus) |
FTTA |
Fertile Thoughts To All |
FMU |
First Morning Urine |
hCG |
Human Chorionic Gonadotropin (pregnancy hormone) |
HPT |
Home Pregnancy Test |
IF |
Infertility |
IUI |
Intrauterine Insemination |
IVF |
In Vitro Fertilization |
LH |
Luteinizing Hormone |
LMP |
Last Menstrual Period |
LP |
Luteal Phase |
O |
Ovulation |
OPK |
Ovulation Predictor Kit |
PCOS |
Polycystic Ovarian Syndrome |
PG |
Pregnancy, pregnant |
S/A |
Sperm/semen analysis |
TTC |
Trying To Conceive |
Other TTC Terms
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
Your TTC Journal
Your feelings may be all over the emotional map while you’re on your TTC journey—excited, hopeful, sometimes frustrated, often a little nervous. Whether you’ve just started out, or you’ve been on the road-to-baby for a while, use these pages to keep track of everything you’re feeling, thinking, stressing about, and dreaming of.
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________
______________________________________________