Chapter 18 What Causes AIDS in Africans? 81
Chapter 19 HIV and AIDS in Health Care Workers
and Scientists 84
Chapter 20 Is AIDS Caused by Some Other Virus? ... 88
Chapter 21 What Causes AIDS? 92
Chapter 22 More on Drug Abuse 96
Chapter 23 'The Terminator' 100
Chapter 24 Anecdotal AIDS Cases from the
General Population 115
Chapter 25 Politics: Consequences of the
Virus/AIDS Hypothesis 118
Chapter 26 Government Funding for
Intimidation and Propaganda 120
Chapter 27 "The Duesberg Phenomenon" 131
Chapter 28 Questions and Answers 135
References 144
Index 183
Chapter 1
The Creation of AIDS by Press Release
Consider the following: we are asked to visit 1000 households and find that in every household where someone is sick in bed, there is medicine on the night table. Do we conclude that the medicine was responsible for the sickness or do we conclude that the medicine is there in response to the sickness? In the following discussion, we plan to show you that HIV is not the cause of AIDS, that HIV is often not even found in AIDS patients, and that even in those cases where HIV is found, the presence of HIV, as determined by the antibody test, is the result (rather than the cause) of a depressed immune system.
In April, 1984, retrovirologist Robert Gallo of the National Institutes of Health in Bethesda, Maryland and Margaret Heckler, United States Secretary of Health and Human Services, announced jointly that the cause of AIDS or Acquired Immune Deficiency Syndrome had been found. They claimed that the cause of AIDS was a retrovirus 1 which we all know now by the name HIV or Human Immunodeficiency Virus (Altaian, 1984).
AIDS, as originally defined , is a syndrome or a group of symptoms attributed to a depressed immune system that is acquired as a result of environmental exposure as opposed to heredity.
AIDS
This announcement was made at a time when not a single American study had been published on HIV. For this reason, the scientific community had no way of judging the merits of Gallo's hypothesis when it was announced to the press. Nevertheless, it essentially received blind acceptance and became national dogma overnight. It is an example of what we would call science by press release.
The evidence that was cited in The New York Times in favor of the HIV/AIDS hypothesis was that Gallo and his collaborators had found antibodies 2 against this virus in 85% of the AIDS patients they examined.
Although antibodies are the ultimate defense in the rejection of a virus and the body's ultimate mechanism for protection against disease, these investigators said in The New York Times article that the presence of these antiviral antibodies proved that HIV was causing AIDS. Although antibodies against HIV, rather than HIV, was all they found in AIDS patients, they nevertheless promised that by artificially inducing more antibodies — with a vaccine they would develop at the latest within two years — they would protect us against this deadly virus and thus eliminate AIDS (Connor, 1987; Adams, 1989; Farber, 1992; Hodgkinson, 1992).
However, the best a vaccine could do would be to induce the body to produce antibodies. But all the patients that tested positive to their so-called 'AIDS test' already had antibodies. Yet, even now, in 1995 they are still trying to make a vaccine.
Furthermore, all the HIV/AIDS proponents can ever detect with their 'AIDS test' is antibody against the virus, not the virus itself. Yet they are talking about developing a vaccine that eliminates a virus which in many cases can't be found. In many HIV antibody-positive persons, there is no detectable HIV.
2 an antibody is a protein produced by the immune system to specifically neutralize foreign agents, such as particular viruses, bacteria, toxins, etc. after these agents have gained entry into the body
Creation of AIDS by Press Release
If you are found positive by the HIV antibody test, this can mean one of three things:
1. You have low levels of the virus which are under control.
2. You don't have any HIV viruses in your body because your immune system has destroyed them all.
3. You were never even exposed to the virus; your immune system produced antibodies to some other infectious agent and these antibodies cross-reacted to give a positive HIV antibody test. This is called a false-positive test..
In the scientific papers that appeared a month later in Science (Gallo, et al., 1984; Popovic, et al. 1984), Gallo explained his hypothesis. He said HIV is a cell-killing virus — a retrovirus that killed T-cells 3 . Once T-cells are gone, a person is no longer protected by an effective immune system and thus is susceptible to all sorts of infection.
So this was science by press release — the press conference that started the virus/AIDS hypothesis. In fact, the virus/ AIDS hypothesis was a political thing from the very beginning. It occurred at the time when Reagan was up for reelection. The gay community had become organized and raised their voices: "Something has to be done about AIDS!" Reagan hadn't said a word about it. So Margaret Heckler, his Secretary of Health and Human Services, and Bob Gallo came to the rescue and announced that they would get AIDS under control with a vaccine that they promised would be ready in two years. Reagan was re-elected, the gays accepted the story, and Gallo became famous.
3 a T-cell is one of the two major types of lymphocytes, i.e. white blood cells, that determine the specificity of the immune system; the other type is referred to as a B- cell
Chapter 2
Changing the Ground Rules to Make the Shoe Fit the Foot
After the original definition of AIDS in 1983 , promoters of the HIV/AIDS theory changed the definition of AIDS and expanded the list of AIDS diseases to about 30 previously known apparently unrelated diseases. In all diseases classified as AIDS after the creation of the HIV/AIDS dogma in 1984, the presence of antibodies against HIV was necessary for the diseases to be classified as AIDS .
So if you have tuberculosis now — or had it in 1987 — and also antibody against HIV, you are an AIDS patient. In the absence of antibody against the virus you are just a tuberculosis patient, just as it used to be a hundred years ago when Robert Koch first discovered the cause of tuberculosis.
The HIV-based AIDS Definition
AIDS is one or a combination of any of 30 old diseases in the presence of antibodies to HIV.
Examples: Tuberculosis + HIV = AIDS
Tuberculosis - HIV = Tuberculosis
Dementia + HIV = AIDS Dementia - HIV = Stupidity
If you have dementia in the presence of HIV, you are an AIDS patient. But if you have dementia without HIV, you are
just stupid and no one is particularly excited about you. This sounds funny but this is not a joke. No, this is the definition of AIDS put forward by the Centers for Disease Control (CDC), and it is good to keep this in mind because we all were led to believe that AIDS was a new disease.
Remember, the Centers of Disease Control, the official national registry for AIDS, does not claim that even one of the AIDS diseases is new. Nobody says that. It only sounds that way in the media. These are all old diseases which now become AIDS, in most cases, because of the presence or the presumed presence of antibody against the virus. If the antibody is there, then HIV is presumed to be responsible for the disease and one has AIDS by definition.
What follows is the 1993 revision of AIDS diseases according to the U.S. Public Health Service (Centers for Disease Control, 1992b).
The original 12 diseases characterizing AIDS
established in 1983 ( none of the following required that the
person be HIV-antibody positive to be classified as AIDS )
Pneumocystis carnii pneumonia 1983
Kaposi's sarcoma 1983
Toxoplasmosis, causing pneumonia, of CNS or brain 1983
Strongyloidosis, pneumonia or central nervous system 1983
Aspergillosis 1983
Cryptococcosis, pulmonary, CNS, and disseminated 1983
Candidiasis, esophageal 1983
Cryptosporidiosis, chronic intestinal 1983
Cytomegalovirus, pulmonary, Gl, and CNS 1983 Herpes simplex, chronic mucocutaneous
infection, pulmonary, Gl, disseminated 1983 Progressive multifocal leukoencephalopathy,
presumably caused by Papova virus 1983
Lymphoma, primary, of the brain 1983
The 7 additional diseases characterizing AIDS established in 1985 ( each of the following requires that the person be HIV-antibody positive to be classified as AIDS ).
Mycobacterium avium complex or M. kansasii
disseminated or extrapulmonary 1985
Histoplasmosis 1985
Isosporiasis, chronic intestinal 1985
Lymphoma, Burkitt's 1985
Lymphoma, immunoblastic 1985
Candidiasis of the bronchi, trachea, lungs 1985
The 8 additional diseases characterizing AIDS established in 1987 ( each of the following requires that the person be HIV-antibody positive to be classified as AIDS ).
Encephalopathy, dementia, HIV-related 1987 Mycobacterium tuberculosis any site (extrapulmonary) 1987
Wasting syndrome, HIV-related 1987
Coccidiomycosis, disseminated or extrapulmonary 1987
Cryptococcosis, extrapulmonary 1987
Cytomegalovirus, other than liver, spleen or nodes 1987
Cytomegalovirus retinitis 1987
Salmonella septicemia, recurrent 1987
The 4 additional diseases and one non-disease characterizing AIDS established in 1993 ( each of the following requires that the person be HIV-antibody positive to be classified as AIDS ).
Recurrent bacterial pneumonia 1993
Invasive cervical cancer 1993
Mycobacterium tuberculosis any site (pulmonary) 1993
Pneumonia, recurrent 1993
CD4 T-cell count is less than 200 cells per microliter
or less than 14% of the expected level 1993
Now a person no longer has to even be sick to have AIDS. As of 1993, persons who are merely HIV-positive and whose CD4 T-cell 4 count is under 200 cells per microliter have AIDS. Persons with a T-cell count under 200 cells per microliter who are not HIV-positive do not have AIDS. By adding just this one group of HIV-positive low T-cell individuals to the AIDS list, the number of new AIDS victims for 1993 increased from about 50,000 to nearly 200,000.
Note that increasing the list of diseases and adding one non-disease to the AIDS list as shown in the previous table, two of the predictions of the HIV/AIDS proponents are artificially fulfilled: (1) the annual AIDS rate will continue to increase and (2) the percentage of AIDS cases that are HIV-positive will increase. This type of'science' ensures that funding for HIV and AIDS will also continue to increase.
4 a CD4 T-cell is one of the two major types of T-cells; the other type is referred to a CD8 T-cell
Chapter 3
Sanctif ication of the Belief that HIV Causes AIDS
Early on, because of the growing AIDS threat, the United States National Academy of Sciences called a blue ribbon committee together. The committee authored a book, Confronting AIDS, which is the bible of orthodoxy on AIDS (Institute of Medicine, 1986). The chairman of the committee was the Nobel Prize winner and retro virologist, Dr. David Baltimore.
The July 3, 1993 issue of the New England Journal of
Medicine had this to say about Dr. Baltimore: "a scientist named Dr. Margot O'Toole was vilified and effectively driven from her profession after she revealed that a paper in Cell [a scientific journal] coauthored by, among others, her supervisor . . . and Dr. David Baltimore relied in large part on data that were falsified. . . Dr. Baltimore . . . admitted that the paper was grossly defective . . . At the end of a lengthy investigation by the Office of Scientific Integrity, Dr. Baltimore retracted the Cell article. He later resigned from the presidency of Rockefeller University. Still later, he announced his intention to retract the retraction . . . [criminal charges against his coworker were dropped in 1992 because of] the difficulty of presenting complex scientific facts to a lay jury, which would have to understand them fully to find guilt beyond a reasonable doubt in a criminal trial. [U.S. Attorney Robert] Bennett emphasized that the declination [dropping of the case] was not an exoneration of David Baltimore or [his coworker] Thereza Imanishi-Kari nor did it reflect doubt on the part of the prosecutors office that the data had been falsified."
Baltimore, Gallo, Duesberg, and others had been chasing retroviruses for thirty years as causes of cancer and had come home from that war empty-handed. We learned a lot about retroviruses, but we did not find a single retrovirus that would cause cancer in humans. With the claim that HIV causes AIDS, retrovirologists now could have something to justify the tremendous amount of time, money, and effort that had been invested into research on retroviruses.
So the committee, in a fairly short time, came out with the following statement: ''The committee believes that the evidence that HIV causes AIDS is scientifically conclusive." The word 'believe' used to be reserved for weekend activities when the committee members went to their respective temples or churches. What they did during the week used to be either 'proven' or 'not proven', or 'scientifically conclusive' or 'not scientifically conclusive', but not what they 'believed'.
But with AIDS, what one believes or what the majority believes — something that used to be considered politics or religion — now became science in this field. So this blue ribbon committee really sealed Gallo's hypothesis into national dogma and with it, sanctified an expenditure of what now amounts to 6 billion taxpayer dollars annually. About $1.5 billion of this goes for HIV research and about $4.5 billion for HIV-related 'health care' and 'education'.
If you study AIDS and want to study the virus or if you want to treat AIDS patients with AZT (which is also referred to as Azidothymidine or 3'-azido 3-deoxythymidine or Zidovudine) to inhibit the virus, then you are eligible to get some of those 6 billion dollars. If you say we may be on the wrong track, that is, that the virus is not the cause, then you get nothing.
So the committee adopted the virus/AIDS hypothesis on the basis of questionable assumptions and circumstantial evidence. And today, this virus hypothesis, which they have sealed into national dogma, is the only approach to the AIDS crisis. It has been a complete failure in terms of public health benefits. The promised vaccine has yet to come. AIDS 'continues to spread'. Moreover, the virus/AIDS hypothesis has
failed completely to predict the course of the epidemic (Institute of Medicine, 1988; Duesberg, 1989c, 1991a, 1992b; Duesberg and Ellison, 1990; Thompson 1990; Savitz, 1991; Waldholz, 1992).
Chapter 4
Can HIV Cause AIDS?
Jrroof that a virus causes a disease depends on showing that
1. in all those who have the disease, the virus is present and that it is present in amounts sufficient to cause the disease,
2. in those who do not have the disease, the virus is not present or at least not present in amounts comparable to those who have the disease,
3. after it is isolated and grown in culture, the virus can induce the disease [These first three criteria of proof are termed Koch's postulates (Merriam-Webster, 1965; Weiss and Jaffe, 1990).],
4. the disease caused by the virus can be prevented through naturally acquired immunity or vaccination,
5. the disease can be cured with antiviral drugs, and/or
6. the disease can be prevented by preventing viral infection.
As a result of research efforts that exceed those on all other viruses combined — research efforts that have resulted in over 75,000 papers on HIV in less than 10 years — it has been found that
1. in many who have AIDS, HIV is not present and in those who have the virus, it is not present in amounts sufficient to cause the disease and
2. in over 12 million persons who do not have AIDS, HIV is present, in many cases, at levels higher than those who have AIDS.
And despite this massive amount of research, no one has been able to
3. induce AIDS by injection of chimpanzees with HIV viruses grown in culture,
4. show that natural immunity to HIV prevents AIDS or develop a vaccine against HIV that can prevent AIDS,
5. cure AIDS with antiviral drugs, or
6. prevent AIDS by preventing HIV infection, despite 'safe sex' and 'clean needle' programs.
HIV is a very weak virus, which is characteristic of retroviruses in general. Unlike the flu virus, which can go through a population in a matter of days or weeks, HIV is very difficult to transmit 5 . Despite knowledge of its existence for 10 years, the number of people testing positive via the HIV antibody test has not increased in the last ten years. In 1984, only 0.4% of the U.S. population was HIV-antibody positive; in 1994, this percentage remains the same, 0.4% (Duesberg, 1992g and 1994a and NIAID, 1994).
5 at least at levels necessary to induce an antibody reaction
Chapter 5
Many AIDS Patients are not 'HIV-Positive'
1 he disturbing reality is that there are no national statistics anywhere in this country or anywhere in the world to document the claim that all AIDS patients are HIV-positive.
It is true the Centers for Disease Control publishes quarterly AIDS statistics in their HIV/AIDS Surveillance Report. Those are the national statistics. But the only mention of HIV was in the title, HIV/AIDS Surveillance Report. In fact, all it reports is AIDS in New York or in San Francisco or in Chicago or in gays or in bisexuals or in scientists or in dentists. It doesn't say one word more about how many of these AIDS cases have HIV and how many don't (Centers for Disease Control, 1992b).
Nobody has ever published the percentage of AIDS cases that are HIV-positive. It is always assumed to be 100%, but this assumption is based entirely on selected individual studies. The committee of the National Academy of Sciences relied primarily on Gallo's original studies 6 which were the basis of the National Academy of Sciences' claim that HIV causes AIDS.
However, after a three-year investigation by the Office of Scientific Integrity, Gallo's studies were found to be fraudulent and Gallo was cited for scientific misconduct.
A Credibility Problem
On July 3, 1993, the New England Journal of Medicine
reported: "After Dr. Zaki Salahuddin, one of his [Gallo's] long-time laboratory scientists [and a coauthor on one of his 1984 papers in Science explaining the HIV I AIDS theory], was convicted of a felony in connection with his activities at Dr. Gallo's laboratory, Dr. Gallo explained that he had been unaware of Dr. Salahuddin's activities. In short order, Dr. Prem Sarin, Dr. Gallo's deputy laboratory chief, was indicted for activities unrelated to those of Dr. Salahuddin but also stemming from work at the laboratory. Dr. Gallo explained he knew nothing of his deputy chiefs misconduct and that these two separate criminal cases involving his laboratory scientists were unfortunate coincidences."
The New England Journal of Medicine continued: "[T]wo subjects described in an article in the Lancet coau-thored by Dr. Gallo . . . had died, but Dr. Gallo had failed to report the deaths to the NIH [National Institutes of Health] as was required by grant regulations and had erroneously reported in Lancet that he had observed no adverse reactions in the human subjects. He explained that the statement in Lancet was an inadvertent error and that his failure to comply with NIH procedure was a result of unfamiliarity with the regulations — this despite some 20 years of employment at the NIH.
"More recently, in the controversy over the AIDS blood test, Dr. Gallo is under investigation because of, among other things, allegations that statements he made in the patent application and thereafter in the patent dispute were deliberately misleading. Dr. Gallo first stated that the virus he used was definitely different from that used by the competing French team. When genetic sequencing proved that the viruses were identical, he suggested that the French must have taken his virus. When that claim was challenged, Dr. Gallo explained that there must have been an inadvertent contamination in his laboratory.
"Meanwhile, there were also questions about the cell line [a group of cells derived from a single cell] in which Dr. Gallo grew his viruses. Initially, Dr. Gallo seemed to suggest that the cell line was his own development. It eventually emerged that the cell line belonged to Dr. Adi Gazdar, a researcher at another NIH institute . . . the Office of Research Integrity found last December [1992] that Dr. Gallo had intentionally misled the scientific community by claiming that he had not grown the lymphoadenopathy-associated virus [the original name for HIV] obtained from the French investigators in a permanent cell line . . . they found that 'Dr. Gallons actions reflect Dr. Gallo's propensity to misrepresent and mislead in favor of his own research findings and hypotheses'" (Dingell, 1993).
More recently, according to the November 11, 1993 issue of the Washington Post, Dr. Gallo was let off the hook again. According to the Post: "The federal government yesterday dropped its charge of scientific misconduct against Robert C. Gallo. . . . The Office of Research Integrity said it would have been 'extraordinarily difficult' to defend against Gallo's appeal of the office's finding 13 months ago that he was guilty of misconduct" because of a newly adopted policy requiring the Office of Scientific Integrity to show "deliberate intent to deceive". Formerly, they only would have had to show that Gallo "knew or should have known" that the statements he was making were false.
Dr. Baltimore and his National Academy of Sciences committee also accepted, without question, the practice of the proponents of the virus hypothesis, that is, using antibodies as a measure of AIDS instead of using the virus; they used antibodies as an indicator of the pathogenic (or disease-causing) powers of HIV currently acting or yet to come.
But nowhere in the report was there a statistic that in fact proved that all AIDS cases, as originally defined, were close to 100% HIV-positive, or even antibody-positive. Probably more than 50% were antibody-positive, but if you look for
AIDS
Dr. Robert Gallo
cytomegalovirus or hepatitis virus or Epstein-Barr virus or gonococcus or syphilis or spirochetes or any other microbe, you will also find that over 50% of the AIDS patients are antibody-positive for one or more of these microbes as well, you have sexual contacts with lots of people and/or if your body's defense mechanisms are down, you pick up these microbes and they can induce an antibody response.
If
The National Academy of Sciences committee also believed that AIDS is unknown in persons who are free of HIV. That's what they said in 1986 and 1988 (Institute of Medicine, 1986 and 1988). This is also not true. There were, even at that time already, quite a few cases of gays with Pneumocystis pneumonia and Kaposi's sarcoma 7 ; of IV drug users with tuberculosis and weight loss and dementia; and of babies with mental retardation — all AIDS cases by the then current definitions — in the absence of HIV (Duesberg, 1993d).
News of numerous HIV-free AIDS cases reported at the Joint Meeting of the Eighth International Conference on AIDS and the Third Sexually Transmitted Diseases World Congress in Amsterdam in July 1992 was written up in Newsweek. Surprisingly, some of the HIV-free AIDS cases announced at this conference had been studied for years (Altman, 1992a; Cohen, 1992a,b; Laurence, et al., 1992), even by the CDC (Spira and Jones, 1992).
In the meantime, Dr. Anthony Fauci, AIDS chief at the National Institutes of Health and Dr. James Curran, AIDS chief at the Centers for Disease Control, were still in the U.S. When they realized the threat to the HIV/AIDS hypothesis posed by having hundreds of people reporting and talking about HIV-free AIDS, they immediately hopped on Air Force 2 and flew over to Amsterdam for damage control (Bob Garry, Tulane University, personal communication). Two weeks later, they called a meeting in Atlanta, coined the new term, idiopathic CD4 lymphocytopenia or ICL, and claimed that this HIV-free AIDS was a totally different disease. With the help of Newsweek writer Geoffrey Cowley, this message was taken to the public.
7 this is even less surprising in view of the fact that investigators have now found a new herpes-like virus which appears to be associated with Kaposi's sarcoma and is not found in non-AIDS patients or in non-Kaposi's sarcoma tissues from AIDS patients (Y. Chang, et al., 1994)
AIDS
Dr. Anthony Fauci
Many AIDS Patients are not HIV-Positive
19
Dr. James Curran
In the August 1993 issue of Biotechnology , Duesberg published a paper in which he listed all the HIV-free AIDS cases that he could find in the literature (CDC doesn't list them) and came up with 4621 HIV-free AIDS cases in studies that have used the HIV-antibody test as well as tests for HIV virus itself (Duesberg, 1993d). Here's how they were broken down.
HIV-free AIDS-defining diseases and immunodeficiencies
Africa
2555 2555
Most of them, in fact, are in Africa because African health workers, in contrast to those in the U.S., Canada, and Europe, do an unbiased AIDS diagnosis. It's called the clinical diagnosis. They diagnose dementia, tuberculosis, weight loss, fever, and diarrhea — and then occasionally test for HIV. When they do that, they find that half of the AIDS cases turn out to be HIV-negative.
Currently in the United States, we do it the other way around. We look for HIV and then we look for the disease. If the patient has an AIDS-defining disease but is HIV-free, the
HIV/AIDS proponents call it by its old name — tuberculosis, candidiasis, lymphoma, pneumonia, etc. The patient is no longer called an AIDS case, so by definition, we have no HIV-free AIDS.
And now we have gone even further. We have classified HIV-positive persons who have no disease but who have a CD4 T-cell count of under 200 cells per microliter as AIDS patients. If a person has a CD4 T-cell count of under 200 cells per microliter and is HIV-negative, by definition they don't have AIDS, they now have idiopathic CD4 lymphocytopenia or ICL.
Those diagnosed as AIDS patients because of a low T-cell count, together with those diagnosed as AIDS on the basis of the AIDS diseases which have been added since 1983, all of which require the presence of HIV, now make up approximately 90% of the AIDS cases (see Chapter 2, page 6). These AIDS cases must be HIV-positive by definition. This is the way the HIV/AIDS proponents have fabricated a virtual 100 percent correlation between HIV and AIDS.
In Chapter 1, we mentioned that "AIDS, as originally defined, is a syndrome or a group of symptoms attributed to a depressed immune system that is acquired as a result of environmental exposure as opposed to heredity." There is no question that if HIV/AIDS proponents classify HIV-positive individuals with low T-cell counts as AIDS victims, they should also classify HIV-negative individuals with low T-cell counts as AIDS victims. Instead, HIV-negative individuals with low T-cell counts are classified as having idiopathic CD4 lymphocytopenia or ICL. The words "idiopathic" and "acquired" both implied "of unknown cause" (as a matter of fact the term 'AIDS virus' is a contradiction in terms; the "A" of AIDS implying that the cause of the disease is unknown and the "virus" implying that the cause is known and is, in fact, this particular virus). CD4 lymphocytopenia, which means a decrease in the number of CD4 lymphocytes in the blood stream is the "symptom" by which the "immune deficiency" can be determined.
AIDS
So it is obvious, at least in AIDS patients who do not have HIV, that HIV did not cause their AIDS. The question is, "Does HIV cause AIDS in anyone? And if it does, how long does it take for HIV to cause AIDS?"
Chapter 6
Many 'HIV-Positives' have no HIV Virus
"Circumstantial evidence is a very tricky thing. It may seem to point very straight to one thing, but if you shift your point of view a little, you may find it pointing in an equally uncompromising manner to something entirely different"
Sir Arthur Conan Doyle, 1928
1 he primary argument of the HIV/AIDS hypothesis was and is the assumption of a nearly 100% correlation between AIDS and antibody against that virus. According to this argument, an antibody is already equated with the presence of the virus, although that is by no means so.
If you are found positive by the HIV antibody test, this can mean one of three things:
1. You were never even exposed to the virus; your immune system produced antibodies to some other infectious agent and these antibodies cross-reacted to give a positive HIV antibody test.
2. You don't have any virus in your body because your immune system has destroyed them all.
3. You have low levels of the virus which are under control.
In cases 1 and 2, even if you are an AIDS patient, it is obvious that HIV did not cause your AIDS, since there wasn't any HIV in your body. Case 3 is discussed in Chapter 7.
Based on the assumption of a nearly 100% correlation between AIDS and antibody against HIV, the National Academy of Sciences' committee said they believed, quoting again from their book, Confronting AIDS, that "close to 100% of all AIDS patients are harboring the virus." But where is the evidence for that frequently cited claim? Of the hundreds of thousands of cases of AIDS patients that have been diagnosed since 1980, hardly any have been tested directly for HIV. And while others have been tested only for antibodies to the virus, there are some who have not been tested for HIV at all, either directly or indirectly (Duesberg, 1994a).
Chapter 7
HIV is Never Present in Amounts Sufficient to Cause AIDS
Even in AIDS patients who are HIV-antibody-positive and in whom the virus is found, there is typically no infectious HIV 8 . Indeed, the scarcity of infectious HIV in typical AIDS patients is the reason that neutralizing antibodies, rather than virus, have become the diagnostic basis of AIDS. It is also the reason that on average 5 million leukocytes (white blood cells) of HIV-positives must be cultured to activate ('isolate') HIV from AIDS patients. Even under these conditions it may take up to 15 different isolation efforts (!) to get just one infectious virus out of an HIV carrier (Weiss, et al., 1988). The vast majority of the viruses in our bodies have no interest whatsoever in killing us or even making us sick. They let us live as long as we can so they can live along with us. It's a bit like the government taxing a citizen; they tax us as much as they can without rocking the boat rather than taking over completely and taxing us to death. So typically, most viruses do not cause a disease, but just hang around there and tax our body, killing a few cells at a time, taking a few proteins and a few vitamins, whatever they need to keep alive without causing disease. These are the passenger viruses (Duesberg, 1994a).
How do you tell a passenger virus from one that is causing a disease? Here are the criteria for distinguishing a causative virus from one that is just hanging in there for the ride.
Causative Viruses
A causative virus usually causes a disease very soon after infection; then immunity follows and if the immune system works properly, the disease is resolved or rejected within days or weeks after that infection.
This is certainly not the case with HIV. HIV infection is typically followed by little or (in the vast majority of cases) no disease — and antibodies to HIV may be produced. This is the reason that virtually nobody who is antibody-positive can remember a primary HIV disease. After antibodies are formed, the virus is destroyed or remains latent. Oddly enough, it is only after this period of antibody formation that HIV/AIDS believers contend that HIV produces AIDS. Normally, people who have antibodies against viruses, such as measles, mumps, or chicken pox can remember the disease that led to the respective antiviral antibodies and these antibodies do not predispose them to the disease but rather provide immunity to the disease.
However, it can be argued that HIV sits in our cells quietly waiting for a time when the immune system is low to come out and do a sneak attack on our white blood cells (Stewart, 1968; McKeown, 1979; Moberg and Cohn, 1991). Such microbes are referred to as being conditionally pathogenic. This is true for tuberculosis bacillus, cholera, influenza virus, polio virus and many others (Freeman, 1979; Mims and White, 1984; Evans, 1989c).
Thus, HIV could be a causative virus that could hang around in the body in the form of a latent virus like herpes. If you once have a herpes infection, you have it for the rest of your life. The same is true with retroviruses and with many other microbes. They hang in there. Then, when the immune system fails at a later time, 10 years, 20 years later, they can become active, increase in number, infect more cells and cause a disease.
However, when AIDS symptoms begin and start to increase, the levels of HIV typically do not increase. For example, if a person has been found to be HIV-positive and if at some later time, say five, six years later, they come down
with AIDS and die, it is found that the number of HIVs in their body has not increased.
In addition, the levels of HIV among HIV-positive AIDS patients is not significantly different from the HIV levels among HIV-positive individuals without symptoms. In fact, in many asymptomatic HIV carriers, there are more HIV-infected white blood cells than in HIV-positive AIDS patients with fatal AIDS. Simmonds and coworkers report that there are from 1 in 700 to 1 in 83,000 HIV-infected white blood cells in healthy HIV carriers and from 1 in 900 to 1 in 30,000 in AIDS patients (Schnittman, et al., 1989; Simmonds, et al., 1990).
Bagasra and coworkers, using a technique which often gives false-positive results, report that there are from 1 in 30 to 1 in 1000 infected white blood cells in healthy carriers and from 1 in 10 to 1 in 1000 in patients with fatal AIDS (Simmonds, et al., 1990; Bagasra, et al., 1992; Duesberg, 1992g).
If reliable assays are used, HIV is never present in amounts sufficient to cause pathological effects. According to one study, "The most striking feature ... is the extremely low level of HIV provirus 9 present in circulating [white blood cells]" (Simmonds, et al., 1990).
Since on average only about 0.1% (1 out of 500 to 3000) of T-cells are ever infected by HIV in AIDS patients, but at least 3% of all T-cells are regenerated (Sprent, 1977; Guyton, 1987) during the two days it takes a retrovirus to infect a cell (Duesberg, 1989c), HIV could never kill enough T-cells to cause immunodeficiency. Thus even if HIV killed every infected T-cell, it could deplete T-cells only at 1/30 of their normal rate of regeneration.
In terms of HIV infecting white blood cells, it is even more notable that the levels of HIV replication in these cells (as measured by HIV RNA synthesis) in AIDS patients is either extremely low or nonexistent. Only 1 in 10,000 to 100,000 of their white blood cells contain viral RNA which is an indication of viral replication — and only 50% of AIDS patients
9 the genome or genetic makeup of a virus
have even this low rate of HIV replication in white blood cells. In the remaining 50%, no HIV expression is detectable (Duesberg, 1989c; Simmonds, et al., 1990). The very fact that amplification by high-tech procedures (the "polymerase chain reaction") must be used to detect HIV DNA or RNA (Semple, et al., 1991) in AIDS patients indicates that not enough viral RNA can be made or is made in AIDS patients to explain any, much less fatal, pathogenicity based on all conventional precedents of viral disease (Duesberg and Schwartz, 1992).
As mentioned before, Gallo said in 1984 that HIV would cause AIDS by killing T-cells (Gallo, et al., 1984; Weiss and Jaffe, 1990). In the same month he published his results that HIV would kill T-cells in his paper in Science, he signed under oath to the U.S. Patent Office that he was the one who could grow HIV better than anybody else in the world. And guess where he was growing his HIV? In human T-cells. T-cells in culture which, after infection, were strong and healthy and had acquired the ability of growing indefinitely, as healthy and as happy as can be. If HIV could kill T-cells, how is it T-cells do so well after being infected — so well in fact that T-cells were patented as a continually growing host for HIV? These very same cells of Gallo are still growing in his laboratory, at Abbott Laboratory, Dupont Laboratory, and many other laboratories. Yet Gallo and others get royalties for the 25 million 'AIDS tests' that are conducted per year in this country (and many more millions abroad) at approximately $50 apiece.
Thus HIV does not kill T-cells in cell culture, in fact these cells grow indefinitely like all other retrovirus-infected cells. The hallmark of the retrovirus is not to kill the cells. That's why we were chasing retroviruses for the last 20 or 30 years as possible carcinogens because a virus that would cause cancer would have to be a virus that doesn't kill a cell (Weiss, et al., 1985; Duesberg, 1987). If the virus kills a cell, it couldn't cause cancer because there would be nothing there to grow into the cancer. If HIV were the cause of AIDS, it would have to cause AIDS by a mechanism that nobody has anticipated and that nobody can explain.
Gallo's first candidate for an AIDS virus, Human T-cell Leukemia Virus-I or HTLV-I (Gallo, et al., 1983), as well as his second, Human T-cell Leukemia Virus-Ill, now referred to as HIV, are little more than renamed cancer viruses (Gallo, et al., 1984; Shaw, et al., 1984; Crewdson, 1989; Rubinstein, 1990; Coffin, et al., 1986). And like cancer viruses, HIV does not kill T-cells. In 1984, even Montagnier, the discoverer of HIV, wrote: "In a search for a direct cytopathic [cell-damaging] effect of the virus on (primary) T-lymphocytes, no gross changes could be seen in virus-producing cultures, with regard to cell lysis [breakage] or impairment of cell growth" (Montagnier, et al., 1984). More recently, Montagnier published another paper showing that T-cells are not killed by HIV (Lemaitre et al., 1990, Herman, 1994).
Others have confirmed that HIV does not kill infected, primary T-cells in culture (Hoxie, et al., 1985; Anand, et al., 1987; Langhoff, et al., 1989; Duesberg, 1989c). Moreover, HIV-infected primary T-cells are considered the natural 'reservoir' of HIV in the body (Schnittman, et al., 1989).
Trying to explain his way out of this, Gallo claimed that T-cell lines in culture have all acquired resistance to being killed by HIV (Gallo, 1991). However, there is no precedent for this, that is, no other virus has ever been observed that kills cells in intact animals, but not in culture. Furthermore, there is not even one T-cell line that is consistently killed by HIV.
So the claim that HIV kills T-cells turned out to be wrong.
Alternatively, HIV/AIDS proponents have proposed that HIV proteins are directly toxic because of structural similarities with scorpion and snake poisons (Gallo, 1991; Garry, et al., 1991; Garry and Koch, 1992). However, no such toxicity has been observed in millions of asymptomatic HIV carriers, and there is no reason that it should occur. Even if it did, supporters of this alternative hypothesis would have to explain why this toxicity would occur only after latent periods of 10-20 years.
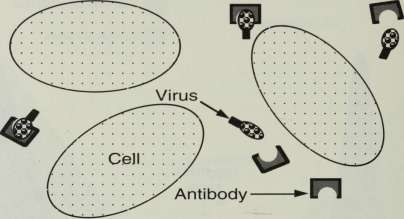
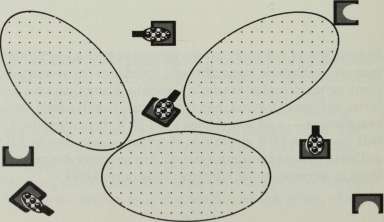
In all conventional viral diseases, the degree of pathogenicity is directly proportional to the number of infected cells.
To produce a disease, viruses must first infect cells, replicate themselves within the cell to produce many virus particles identical to themselves, break out of the cell, and have these virus particles reinfect other cells until the viruses have infected enough cells that the host starts exhibiting the symptoms of a disease. So the disease is initiated and controlled by the action of a causative virus — like the pilot controls the flight of the plane.
In the following graphic representations, the virus is represented by a dark gray area, the disease by a light gray area, and the overlap, where there is both virus and disease present, is represented by a black area. An increase in the concentration of the virus is represented by an increase in the height of the dark gray area. Similarly, an increase in the intensity of the disease is represented by an increase in the height of the light gray area.
Causative Virus
Concentration of virus Intensity of disease
Unpredictable interval
i
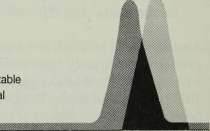
Time
In the above figure, you see the relation between a causative virus and its characteristic disease. This is representative of
what you might see in a herpes infection. The virus becomes active and increases in concentration; soon after, the disease starts. Then the immune system destroys or neutralizes the virus and the virus concentration decreases — and soon after, as a result, the disease passes. In the case of herpes, the virus continues on in the body at low concentrations until the immune system is down due to stress, malnutrition, environmental exposure, and/or lack of sleep. Then the herpes virus flares up again, soon followed by the same disease and the battle starts all over. That's typical for a recurrent causative virus.
Passenger Viruses
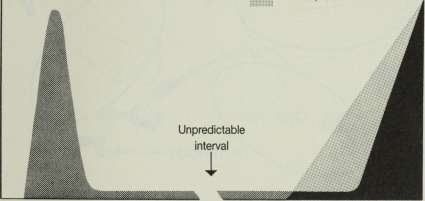
In the following figure, the virus infects, becomes active, and increases in concentration, but no disease follows. It is an opportunistic passenger virus, that's the simple word for it. It infects you today and nothing happens. Then the immune system destroys or neutralizes the virus and the virus concentration decreases to background levels. Then ten years later, for example, you get AIDS. You look for HIV and find that HIV is there at background levels, the same levels found in asymptomatic HIV carriers (illustrated below).
Passenger HIV Virus
111 Concentration of HIV virus Intensity of disease

Unpredictable interval
i
Time
In some cases you can't find any HIV virus there, as is illustrated below
NoHIVVirus
Intensity of AIDS
mmi
Unpredictable interval
i
Time
In some terminal AIDS patients elevated HIV concentrations can be found in the blood; this is referred to as viremia (Baltimore and Feinberg, 1989; Coombs, et al., 1989; Ho, et al., 1989a; Semple, et al., 1991, Piatak, et al., 1993). However some of these investigators also found viremia in 25-50% of the asymptomatic HIV carriers they studied. HIV viremia indicates that the immune system is pretty well shot, whether the patient has AIDS symptoms or not. The increase in HIV in these rare cases is the result, not the cause, of a
HIV Amounts Not Sufficient to Cause AIDS
33
severe immune deficiency occurring after, not before, AIDS symptoms appear, as illustrated below.
ViremicAIDS
Concentration of HIV virus Intensity of disease
Time
Indeed, many normally latent parasites become activated and may cause chronic 'opportunistic infections' in immunodefi-cient persons, as for example Candida, Pneumocystis, herpes virus, cytomegalovirus, hepatitis virus, tuberculosis bacillus, toxoplasma — and sometimes even HIV. It is consistent with this view that HIV viremia is observed more often in AIDS patients (whose immune systems are severely depressed) than in asymptomatic carriers (Duesberg, 1990c).
AIDS
Even at these higher concentrations, the HIVs in the blood, which are neutralized by antibodies, do not infect the white blood cells in the AIDS patient's body (in vivo), because only a negligible fraction of the white blood cells, on average only 1 in 1500 to 8000 in AIDS patients, are infected. Since viruses, as obligatory cellular parasites, can only be pathogenic by infecting cells, these noninfectious viremias cannot be relevant to the cause of AIDS (because so few cells are infected).
HIV Amounts Not Sufficient to Cause AIDS
35
If assayed in the test tube (in vitro), in the absence of free antiviral antibodies, antibodies may dissociate from neutralized viruses and thus render the virus infectious for cells in culture. This explains the discrepancy between the noninfectious 'viremias' in vivo and the relatively high infec-tivity recorded in vitro (Coombs, et al., 1989; Ho, et al. 7 1989a).
In order to explain why in many cases there is no increase in the number of HIV viruses between a person with AIDS and the same person when first found to be HIV-positive, Fauci came out with another report (Pantaleo, G., et al., 1993) in which he proposed that HIV was playing hide-and-seek. But if you get past the puffery, you see that he finds only one virus particle per thousand cells, exactly the same results that Gallo had found ten years earlier (Shaw, et al., 1984, 1985; Duesberg, 1993c; Piatak, et al., 1993). And this despite the fact that Fauci was looking in the lymph nodes which are the dust bin of the immune system. The lymph nodes are where Montagnier first found HIV. That's why it was called lymphadenopathy associated virus at that time. There was one in a thousand infected cells and the virus was neutralized by antibody. It wasn't infecting any other cells. This is exactly what Fauci found. He couldn't find infectious virus. He only found viral nucleic acid. Aside from high-tech procedures, there was nothing new.
He applied high technology to an old question and got the old answers — that's all that has happened. We have technology to see a needle in a haystack now. But you don't die from a needle in a haystack. You could have mercury, uranium, strontium-90, cyanide, and anything combined in one in a thousand T-cells, and, so long as it doesn't cause cancer, you would not even notice it. You'd only notice it if it would get 30% of your T-cells. But you would never notice what happens by contaminating one cell in a thousand, no matter what is in there, from HIV to dynamite.
Therefore, it appears obvious that HIV does not cause AIDS and that it is, instead, a passenger virus. In the case of a passenger virus, the time of the primary infection and the disease with which it 4 s connected, like, say HIV and AIDS, are totally unrelated ihe passenger virus could infect you today and the disease could follow 30 years later. If Dr. Gallo or some other virologist starts using the polymerase chain reaction in a diseased patient to look for "the causative virus", he would find all sorts of passenger viruses, such as HIV, that you have accumulated over the last 10, 20, or 30
years. The time of infection is irrelevant to the cause of the disease because the virus is irrelevant to the cause of the disease. You could be infected by a passenger virus today and get AIDS 10 years from now and the passenger virus may still be around in a latent form. But since it hasn't caused AIDS, the time interval between infection and disease is unpredictable and irrelevant.
Let's look at it this way. Your T-cell is the airplane. The pilot of the plane is the causative virus. With the causative virus, the disease follows the infection very quickly like the plane follows the pilot directing its flight. In contrast, the passenger (passenger virus) can be sitting in the plane for 10 years, but has no control over the plane.
Another telling difference between the two is that the causative virus is always present when the disease occurs, but the passenger may or may not be present — because the flight goes with or without the passenger, but not without the pilot. So if you have poliomyelitis or the flu, the polio virus is there or the influenza virus is there. In their absence, the diseases they cause wouldn't occur. The presence or absence of a passenger virus is irrelevant.
So HIV cannot be a causative virus, because you can very well have AIDS without HIV. As was already pointed out, there are at least 4621 such cases (Duesberg, 1993d). These HIV-free AIDS cases exhibit the same symptoms as AIDS patients with HIV, indicating again that HIV is a passenger virus, not the cause.
HIV acts instead like a passenger virus. The passenger virus can be anything it wants to be during the course of the disease. It can be active, benefitting sometimes or often from the immunodeficiency which typically precedes or accompanies a disease; it could sleep in the back seat of the plane; or it may not be on the plane at all.
In other words. HIV meets every one of the criteria of a harmless passenger virus.
In AIDS risk groups and AIDS patients, HIV is not the only microbe that behaves like a passenger virus. Antibodies against many other passenger viruses and microbes are also found. These include cytomegalovirus, hepatitis virus, Epstein-Barr virus, Human T-cell Leukemia Virus-I (HTLV-I), herpes virus, mycoplasma, amoebae, as well as microbes which can result in gonorrhea, syphilis, tuberculosis, and toxoplasmosis (Gallo et al., 1983; Sonnabend et al., 1983; Blattner et al., 1985; Mathur-Wagh et al., 1985; Darrow et al., 1987; Quinn et al., 1987; Messiah et al., 1988; Stewart, 1989; Goldsmith, 1990; Mills and Masur, 1990; Root-Bernstein, 1990a,c; Duesberg, 1991a; Buimovici-Klein et al., 1988). According to Quinn et al. (1987), "Common to African patients with AIDS and outpatient controls and American patients with AIDS and homosexual men was the finding of extremely high prevalence rates of antibody to cytomegalovirus (range, 92-100%), herpes virus (range, 90-100%), hepatitis B virus (range, 78-82%), hepatitis A virus (range, 82-95%), Epstein-Barr virus capsid antigen (100%), syphilis (11-23%), and Toxoplasma gondii (51-74%). In contrast, the prevalence of antibody to each of these infectious agents was significantly lower among . . . American heterosexual men".
In addition, there are between 100 and 150 chronically latent retroviruses in the human germ line (Martin et al., 1981; Nakamura et al., 1991), of which HIV is only one. These human retroviruses are in every cell, not just in a few like HIV, and have the same basic genetic structure and complexity as HIV and all other retroviruses (Duesberg, 1989c). Thus, the incidence of many human parasites, both rare and common, is high in typical AIDS patients and in typical AIDS risk groups. However, none of these microbes are fatal and nearly all are harmless to those with a normal immune system.
According to the World Health Organization, the CDC, and others, there are about one million Americans infected with HIV whose health status is not clinically different from those not infected either now or since 1985, when some of them were first detected as being HIV-positive. Similarly,
there are 8-10 million Africans who are HIV-positive, half a million Europeans, one and a half million South Americans, one and a half million Asians, altogether about 13 million people (Merson, 1993) who have HIV and whose health is not clinically different from those who do not have HIV.
Originally, estimates were made that HIV would cause AIDS in a matter of months, then later, that it would cause AIDS in one or two years, and now there are estimates that it will take 10 years or more. Could it be that the unreliability of these estimates is based on the fact that HIV doesn't cause AIDS at all?
Chapter 8
Most who have been 'HIV-Positive 5 for Ten Years do not have AIDS
Vv herever viruses are the cause of disease, the disease follows viral infection within a couple of months or weeks or days. But ever since HIV-antibody tests have been done, it was found that about one million Americans were infected. That number hasn't changed since the first test in 1984 to the last one in 1994. One million Americans were infected in 1984 and one million Americans are infected in 1994 (NIAID Backgrounder, 1994) with and without safe sex, no matter what they did, according to the Centers for Disease Control. The number of American HIV-infected persons has not changed during this time.
But the incidence of AIDS diseases has changed significantly from a few hundred cases to fifty thousand cases per year. Thus there is a very poor correlation between the number of HIV-positive Americans and the number of American AIDS cases reported — in fact no correlation whatsoever. The fact that the number of American HIV carriers has remained so consistently at one million was discussed in an article in the February 1993 issue of Spy magazine under the title "The Good News is That the Bad News is the Same". The editors of Spy called the Centers for Disease Control and asked them, "Is it [the number of HIV-positive Americans] still the same?" "Yes" responded the Centers for Disease Control.
Even assuming that in 1984, there were, as reported, 1,000,000 HIV-positive individuals and that by 1993, 300,000 of them had come down with AIDS and that all those coming down with AIDS were HIV-positive, that would mean that 700,000 HIV-positive individuals survived for 10 years with-
out getting AIDS. Since we know there are some who get AIDS who are HIV-negative, it could be that as few as 200,000 of the 1,000,000 or 20% who were HIV-positive for ten years got AIDS and the remainder, 80%, did not.
Assuming that 50,000 to 100,000 of the 250,000,000 (or .02%-.04%) of the U.S. population who were HIV-negative in the U.S. got AIDS, it still can be seen that the chance of a person who is HIV-positive has a substantially greater chance of getting AIDS. However, as we have pointed out, antibodies to HIV as well as antibodies to a number of other microbes, are markers for, rather than causes of, a depressed immune system.
The incidence of HIV-positives has also remained fixed at about 10% of the population of Central Africa since 1985. Despite this, only about 1% of the HIV-positive individuals have gotten AIDS in the last 9 years — 99% of the HIV-positives being AIDS-free.
Moreover, HIV is not new. HIV existed in the U.S. long before its fictitious origin in Africa (Gallo, 1987; Gallo and Montagnier, 1988; Anderson and May, 1992) and its fictitious entry into this country in the 1970s (Shilts, 1985). For example, in the U.S. in 1968 an HIV-positive, male homosexual prostitute died from Kaposi's sarcoma and immunodeficiency (Garry, et al., 1988), and 45 out of 1129 American intravenous drug users were found to be HIV-positive in 1971 and 1972 (Moore, et al., 1986). Thus, it is hard to tell how long those 1,000,000 Americans who were found (by figures extrapolated by the U.S. government) to be HIV-positive in 1984 were infected — 20, 30 or 40 years — and yet they're still walking around without AIDS.
Judging from the following incidence curve of HIV infection in the United States, it again appears that HIV and HIV-infected individuals have been around for a long time. A comparison of HIV with the more commonly found long-established microbes in the U.S. population, such as Candida, Pneumocystis (Freeman, 1979; Pifer, 1984; Pifer, et al., 1988), cytomegalovirus, and herpes (Evans, 1989c) indicates that it
AIDS
has probably been around for thousands or millions of years, or for as long as man has walked the surface of the earth.
1985
1990 Year
1995
A microbe entering a population spreads until a susceptible pool is saturated. Subsequently those microbes either develop a coexistence within the population or become incompatible with long-term survival of the host population and are eliminated. If HIV were a new virus, its infection curve would have had to look more like curve A.
Claims that HIV is new are based on the idea that until you find something, it doesn't exist. Thus, before Columbus discovered the New World, can we say it didn't exist? And before the technology became available that made it possible to discover HIV and many other latent retroviruses like HTLV-I (Duesberg and Schwartz, 1992), can we say these viruses didn't exist? Indeed not. The fact that the technology to detect a latent virus like HIV only became available around the time AIDS appeared can hardly be used to prove that HIV causes AIDS.
Chapter 9
Can HIV Grown in Culture Cause AIDS?
Attempts to show that HIV grown in culture is able to induce AIDS have failed miserably. The most ambitious project involved injecting HIV into chimpanzees. Just like their human cousins, chimpanzees make antibodies against HIV. This proves that they are, unlike other primates, susceptible to HIV. Therefore, it was predicted that if chimpanzees were inoculated by HIV, they would get AIDS.
Up to 150 chimpanzees have been inoculated with HIV since 1983 and have been examined year after year since then. The last word received indicated that they were all still healthy (Weiss, 1993; Duesberg, 1992g). Not even one of them had developed AIDS symptoms or died. They've been doing well on HIV for the last ten years at a cost to the taxpayers of $50,000 a piece. They are not getting Kaposi's sarcoma or dementia. (Hilts, 1992; Steinbrook, 1992; Jorg Eichberg, personal communication).
Chapter 10
Anti-HIV Immunity
does not Protect against AIDS
Another prediction that was made is that natural vaccines or artificial vaccines would protect against AIDS. Well the reality is that those who have developed a natural immunity to HIV are now considered prospective AIDS patients and their immunity, as evidenced by antibody against the virus, is being used as a predictor of the disease. In fact, the natural vaccine or immunity they have developed against the virus is so good that the virus is not to be found. Ironically, it is only when you have made this antibody and when it is almost impossible to find the virus — only then, they say, can you get AIDS.
Now if you were infected with a virus like the flu virus and the virus grew rapidly and you failed to make the antibody, the virus concentration would be high. That would be a typical situation where you could get a viral disease. However, according to the HIV/AIDS proponents, it is only when you get antibodies that you can get the disease. And then, for those who have antibodies, they say that they want to make a vaccine. If these people already have antibodies, what good is it to inject them with a vaccine for the purpose of making antibodies? They already have antibodies that are so effective that nobody can find the virus in HIV-positive individuals.
Natural antiviral antibodies, nature's vaccination, against HIV — which completely neutralize HIV to virtually undetectable levels — are consistently found in AIDS patients. Yet these antibodies consistently fail to protect against AIDS diseases (Duesberg, 1989b,c, 1991a; Evans, 1989a,b). This again should give us a clue that HIV does not cause AIDS.
However according to HIV/AIDS proponents: "The dilemma in HIV is that antibody is not protective" (Evans, 1989a). Antibodies against HIV are claimed not to protect against AIDS because proponents claim that they do not neutralize HIV (Institute of Medicine, 1988; Evans, 1989a; Weiss and Jaffe, 1990; Gallo, 1991; Baltimore and Feinberg, 1990).
In fact, antiviral immunity completely neutralizes HIV and restricts it to undetectable levels in healthy HIV-carriers as well as in AIDS patients (Duesberg, 1989b,c). Indeed, three recent studies have just confirmed that HIV activity is 'rapidly and effectively limited' by antiviral immunity (Clark, et al., 1991; Daar, et al., 1991, Piatak, et al., 1993) to less than 1 in 1000 T-cells. By contrast, HIV replicates in the absence of antiviral immunity in human T-cells in culture to concentrations of 30 million virus particles per ounce. Thus, the assumption that HIV causes AIDS because of inadequate antiviral immunity is unconfirmed.
Baltimore's, Feinberg's, and Evans' paradox "that antibody is not protective" (Evans, 1989a) is their failure to recognize that HIV doesn't cause AIDS.
Chapter 11
HIV does not Cause AIDS, but..
Even leading researchers and supporters of the HIV/AIDS hypothesis have acknowledged that (1) in many who have AIDS, HIV is not present; (2) in those who do not have AIDS, HIV is present; and (3) HIV grown in culture has not been found to induce AIDS.
It is also obvious that (4) no anti-HIV vaccine that can prevent AIDS has been found; (5) AIDS has not been prevented or cured with antiviral drugs; and (6) AIDS has not been reduced by preventing HIV infection.
Nevertheless, HIV/AIDS proponents have argued that this does not invalidate their belief that HIV is the cause of AIDS. It only means that the suspected pathogen cannot be proven responsible for a disease by classical means — but perhaps can be proven by new laws of causation (Blattner, et al., 1988; Evans, 1989a,b; Weiss and Jaffe, 1990; Gallo, 1991).
But HIV even fails to meet the new laws of causation. Attempts to show that HIV causes 30 mostly unrelated diseases by destroying the immune system through the destruction of T-cells have also failed (Chapter 7). Even HIV-discoverer Montagnier and others admit that they could find no harmful effect of HIV on T-cells (Montagnier et al., 1984, Lemaitre, et al., 1990).
And even though HIV/AIDS proponents at the CDC have, since 1985, required that most AIDS diseases not be classified as AIDS in the absence of HIV, this does not constitute proof that HIV causes AIDS. Saying that only blind people wearing green shirts can be called blind does not mean that green shirts cause blindness.
There was a time when an informed person could have been led to believe that the association between HIV and AIDS in various age groups, sex groups, or risk groups indicated a causal relationship. As we will show in the following chapters, that time has passed.
Chapter 12
Age Distribution of AIDS
About 98% of all the American AIDS cases occur in persons over the age of 20. If HIV caused AIDS by suppressing the immune system, one would expect it to cause AIDS in those whose immune systems are weakest, people in the 65 and over age group. Quite the contrary, AIDS primarily strikes 20- to 45-year-old males — those whose immune systems are normally strongest (Mims and White, 1984). This is also the group which consumes hard drugs at the highest rate.
Moreover, mortality from drugs and AIDS appear to claim their victims from this same risk group. For instance, the annual mortality in 25- to 44-year-old American males increased about 10% from 1983 to 1987, corresponding to about 10,000 deaths among about 40 million in this group (Buehler, et al., 1990). Annual AIDS deaths had also reached 10,000 by 1987 (Institute of Medicine, 1986; Centers for Disease Control, 1987, 1992b).
Mortality in 25- to 44-year-old males from septicemia, considered an indicator of intravenous drug use, rose almost four-fold from 1980 to 1987, and direct mortality from drug use doubled (National Center for Health Statistics, 1989; Buehler, et al., 1990), indicating that drugs played a significant role in the increased mortality of this group (Buehler, et al., 1990). In addition, death rates from AIDS diseases and non-AIDS pneumonia and septicemia per 1000 intravenous drug users in New York increased at virtually the same pace. From 1984 to 1987, AIDS deaths increased from 3.6 per thousand to 14.7 per thousand drug users. During the same time period, non-AIDS deaths (pneumonia and septicemia) increased from 3.6 to 13.6 per thousand drug users. This strongly suggests that the drugs are the problem and that AIDS is a reflection of that problem.
Age Distribution of AIDS
49
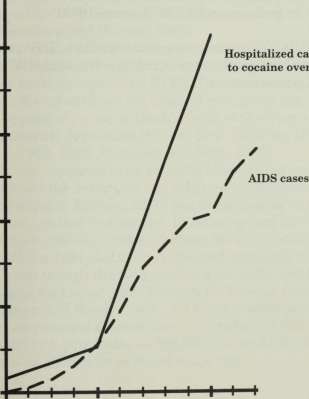
Indeed, cocaine-related hospital emergencies alone could more than account for the American AIDS patients that are intravenous drug users. These emergencies increased from 'a negligible number of people' in 1973 to 10,526 cases in 1985 (Kozel and Adams, 1986), when a total of 10,489 AIDS cases were recorded and to 82,838 cases in 1990 (National Institute on Drug Abuse, 1990a,b), when a total of 41,416 AIDS cases were recorded by the CDC (Centers for Disease Control, 1992a). The following figure shows the association between cocaine overdose and AIDS.
80,000 +
Hospitalized cases due to cocaine overdose
60,000 ■■
40,000 ■
20,000 ■■
1985 1990
Year
Moreover 82% of the cocaine-related and 75% of the morphine-related hospital emergencies were 20-39 years old (National Institute on Drug Abuse, 1990a), the age group typical of AIDS patients.
Another striking coincidence is that over 72% of all American AIDS patients (Centers for Disease Control, 1992b) and about 75% of all Americans who consume 'hard' psychoactive drugs such as cocaine, amphetamines and inhalants (National Institute of Drug Abuse, 1987, 1990a,b; Ginzburg, 1988) or get arrested for possession of such drugs (Bureau of Justice Statistics, 1988) or are treated for such drugs (National Institute on Drug Abuse, 1990a) are 20- to 44-year-old males. Thus there is a substantial correlation between drug abuse and AIDS (Lerner, 1989).
'But', HIV/AIDS proponents might point out, 'HIV attacks this group because they are sexually active and HIV is spread through sexual contact.'
Chapter 13
Sexual Distribution of AIDS and HIV
Another group that would be predicted to fall victim to the 'deadly' HIV, spread sexually of course, would be prostitutes 10 , because it's their business to have sexual intercourse with everybody who can pay for it. Nonetheless, HIV infection among prostitutes is almost exclusively restricted to drug users (Rosenberg and Weiner, 1988).
It was predicted from the very beginning by Gallo, by Heckler, by Surgeon General C. Everett Koop, who are essentially just microphones of the HIV/AIDS proponents, that AIDS would explode from the original risk group into the general population — or as Heckler said at the time — into the heterosexual population (Shilts, 1985; Shorter, 1987; Fumento, 1989, 1993; Anderson and May, 1992).
AIDS was supposed to be sexually transmitted and equilibrate between the sexes like any other venereal disease. But in America and in Europe, AIDS has remained, to this date, in the same original risk groups. In America and Europe, male homosexuals still make up about 50-60% of all AIDS patients. Since 1981, AIDS has remained primarily a male disease, even though the first women with AIDS had been diagnosed in that same year (Centers for Disease Control, 1986; Guinan and Hardy, 1987). No other infectious disease, certainly no venereal disease, has ever remained 90% male for 10 years in a population of 250,000,000 as AIDS has in America — or 86% male as it has in Europe.
10 unless otherwise specified, "prostitute" will be used in this book to refer to a female prostitute
AIDS
Distribution of AIDS cases 1985-1991
AIDS by age (over 20 years old)
Epidemics 11 American European African
98% 1 2
96%
In Africa, the number of AIDS cases is equally distributed among males and females. Since it is postulated that AIDS appeared in America and Africa at about the same time, 10-20 years ago (Institute of Medicine, 1986; Blattner, et al., 1988; Gallo and Montagnier, 1988), AIDS should have reached the same equilibria between the sexes in all countries.
To account for the fact that AIDS is a male disease and predominantly a male homosexual disease in the U.S. and Europe, the promoters of the HIV/AIDS theory assumed that the virus first got its footing in the U.S. in male homosexuals (Booth, 1988) and has remained with male homosexuals because it is transmitted preferentially by anal intercourse (Shilts, 1985; Centers for Disease Control, 1986; Blattner, et al., 1988; Institute of Medicine, 1988; Blattner, 1991; Bardach, 1992; Project Inform, 1992).
11 data from World Health Organization, 1992a; Centers for Disease Control, 1992b.
12 Nearly all American (98%) and European (96%) AIDS patients are over 20 years old; the remaining 2% and 4%, respectively, are mostly infants (World Health Organization, 1992a; Centers for Disease Control, 1992b). There is very little AIDS among teenagers, as only 789 American teenagers have developed AIDS as of 1991, including 160 in 1991 and 170 in 1990 (Centers for Disease Control, 1992b).
L34
ncluding homosexuals
14 includes estimated 10% non-IV recreational drug users
However, this assumption is inconsistent with the following: (1) about 10% of all males and females prefer anal intercourse and thus AIDS should have spread into the heterosexual population (Boiling and Voeller, 1987; Turner, et al., 1989; Seidman and Reider, 1994) and (2) the risk of women for both HIV infection and AIDS is the same for those who practice anal intercourse as for those who practice other types of intercourse (Guinan and Hardy, 1987).
The 10-fold higher incidence of AIDS in American and European males compared to females is assumed to reflect a 10-fold higher incidence of HIV in men (Blattner, et al., 1988; Blattner, 1991; Goudsmit, 1992). However, there is no evidence that the incidence of HIV is 10 times higher in males than in females of the general American and European population.
To the contrary. The U.S. Army (Burke, et al, 1990) and the U.S. Job Corps (St. Louis, et al., 1991) tested the HIV status of millions of individuals. They found that HIV was equally distributed between the sexes among 17- to 21-year-olds of the general population over the last five years. The U.S. Army data predict that among 17- to 24-year-olds, AIDS risks should be distributed equally between the sexes. However, the CDC documents that 85% of the AIDS cases among 17- to 24-year-olds occurred among males (Centers for Disease Control, 1992b).
Our attempts to get further information on the distribution of HIV in males and females has been frustrated by the public health establishment. For example, when asked for information regarding the percentage of HlV-positives that are male and female, Leslie Ann Helmut of the Ohio Department of Health refused to supply the data which she admitted she had in her possession and replied: "We cannot release data that can be severely misinterpreted."
Examination of the previous table (page 52) indicates that the best explanation of the difference between the sex distributions of AIDS in America and Europe on the one hand and Africa on the other is that we are looking at two different groups of diseases with different causes. In America and Europe, we should look at peculiarities in the life-styles of males and particularly male homosexuals and in Africa we should look at peculiarities in the life-style of the general population to determine the cause of their respective diseases.
The male bias for AIDS in America and Europe reflects male-specific behavior. Over 75% of all intravenous drug users are males. Long-term consumption of sexual stimulants, like amyl nitrite and butyl nitrite inhalants (both of which are carcinogenic and immunosuppressive agents (Haverkos, 1988b)) is almost entirely restricted to male homosexuals. HIV is just a marker of the many AIDS risks of men, but not women , in America and Europe (namely drugs). In Africa, malnutrition, parasitic infections and poor sanitary conditions, but not sex-specific risk factors, are causing AIDS diseases. This is the reason that in Africa, AIDS occurs with equal frequency in both men and women. Drug usage resolves the paradox between the different sexual distributions of AIDS in these countries.
According to Rosenberg and Weiner, "HIV infection in non-drug using prostitutes tends to be low or absent, implying that sexual activity alone does not place them at high risk" (Rosenberg and Weiner, 1988).
It is virtually impossible to find non-neutralized HIV anywhere in the semen of HIV-antibody-positive men. In a group of 25 antibody-positive men, only one single provirus of HIV could be found in over 1 million cells of semen in one of the men and no HIV at all was found in the semen of the other 24 (Van Voorhis, et al., 1991). Likewise, HIV could only be isolated or reactivated from ejaculates of 9 out of 95 antibody-positive men (Anderson, et al., 1992).
These findings seriously question the significance of the sexual transmission of HIV as a causative factor in AIDS.
Chapter 14
The Incidence of Diseases Attributed to HIV
In the previous chapters, we have seen that HIV is not biologically capable of causing AIDS. In the following chapters we will see that even if it were, the HIV/AIDS hypothesis could not explain the prevalence of diseases that its fans would like to attribute to it.
Now within Europe and the United States, we have HIV-infected risk groups which have totally different annual risks of getting AIDS, and have, in fact, different group-specific diseases.
Prevalence of AIDS and Specific Diseases of various HIV-positive at-risk groups
Risk group
HIV-positives who get AIDS after the 1st year Characteristic Diseases
American recipients of transfusions
American babies
Male homosexuals using sexual stimulants 15
Intravenous drug users 15 4-6%
Hemophiliacs 15
50% pneumonia,
opportunistic infections
25% dementia,
bacterial infections
4-6% Kaposi's sarcoma
tuberculosis, wasting disease
1-2% pneumonia,
opportunistic infections
The above table (derived from Morgan, et al., 1990; Centers for Disease Control 1992a,b) clearly shows the differences between the characteristic diseases attributed to HIV that are experienced by various risk groups. You can see that the rates at which HIV carriers get AIDS annually varies greatly depending on the risk group. For example, HIV-positive non-hemophiliac transfusion recipients have 25 or more times the risk of getting AIDS than HIV-positive hemophiliacs receiving blood products. Yet the characteristic diseases of these two groups (which are similar) differ greatly from the characteristic diseases of HIV-positive babies, homosexuals, and drug users.
Kaposi's sarcoma is prevalent among male homosexuals. As a matter of fact, 92% of the AIDS-related Kaposi's sarcoma cases occur among male homosexuals which make up only about 5% of the population. This means that the rate of Kaposi's sarcoma of male homosexuals is over 200 times higher than the rate of the general population. If HIV caused Kaposi's sarcoma, why would Kaposi's sarcoma be so predominant among male homosexuals and why wouldn't it occur equally in other AIDS groups?
In America 99% of the hemophiliacs with AIDS have opportunistic infections, of which about 70% are fungal and viral pneumonias (Evatt, et al., 1984; Selik, et al., 1987; Stehr-Green, et al., 1988; Goedert, et al., 1989; Koerper, 1989; Becherer, et al., 1990). Only one study has ever mentioned a Kaposi's sarcoma in a hemophiliac. There are no reports of wasting disease and dementia in hemophiliacs.
Why would HIV cause a series of 30 or so diverse diseases? Why would HIV cause Kaposi's sarcoma in male homosexuals but not in non-homosexual male hemophiliacs? Why would it cause dementia in babies and almost exclusively opportunistic infectious diseases in hemophiliacs and transfusion recipients? Why would it cause one set of these diseases in the United States and Europe primarily among males over the age of 20 — and another set of diseases in Africa among both sexes and at all ages. In the following chapters, we will see that these diseases that are now attrib-
uted to HIV all existed before HIV was ever considered a threat and that the AIDS diseases in the U.S. and Europe are the result of unsafe or ill-advised medical treatments and 'recreational' drug abuse.
Chapter 15
What Causes AIDS
in Hemophiliacs and
Other Transfusion Recipients?
About 15,000, or 75% of the 20,000 American hemophiliacs are HIV-positive as a result of transfusions received before the 'AIDS test' was developed in 1984 (Tsoukas, et al., 1984; Hardy, et al., 1985; Institute of Medicine, 1986, 1988; Stehr-Green, et al., 1988; Goedert, et al., 1989; Koerper, 1989). Based on limited data, it is generally estimated that most of these infections occurred between 1978 and 1984 (Evatt, et al., 1985; Johnson, et al., 1985; McGrady, et al., 1987; Goedert, et al., 1989). This high rate of HIV infection reflects the practice, developed in the 1960s and 1970s, of preparing Factor VIII (a protein clotting factor given to hemophiliacs to prevent internal bleeding) from blood pools collected from large numbers of donors (Johnson, et al., 1985; Aronson, 1988; Koerper, 1989).
The annual AIDS risk of HIV-infected American hemophiliacs is about 2% and for German hemophiliacs, it is about 1% (Bundesgesundheitsamt (Germany), 1991; Leonhard, 1992). According to the virus/AIDS hypothesis, one would have expected that by now (10-16 years after infection) most of the 15,000 HIV-positive hemophiliacs would have developed AIDS or died from AIDS. However this is not the case.
What causes AIDS in hemophiliacs?
During transfusions, foreign proteins 16 or protein fragments from the cell wall of white blood cells (including T-cells) of pooled donors are injected into the blood of hemophiliacs (as well as other transfusion recipients). This can lead to the
lfi injected proteins that are not from the person who was injected
production of antibodies which attack these foreign proteins or protein fragments. However, these same antibodies can also attach to the same protein or protein fragment on the surface of the individual's own white blood cells and can lead to the destruction of these cells as well. Destruction of white blood cells results in the immune deficiency and opportunistic infections resulting therefrom which we currently call AIDS. This process (by which an individual's own white blood cells are destroyed by their own immune system) is called an autoimmune response.
Support for this has come from studies showing that uninfected monkeys injected with white blood cells (including T-cells) produced antibodies, whether or not the cells they were injected with were infected with simian immunodeficiency virus, which is also referred to as SIV. As a result of these experiments, others have proposed that AIDS is the result of an induced autoimmunity (Hoffmann, 1990; Maddox, 1991a; Mathe, 1992).
Alternatively, an abundance of foreign protein may be able to paralyze immunity by blocking cell division of the very cells that are able to recognize it. This process is used in practice to prevent graft rejection. For example, a surgeon will transfuse a prospective organ recipient with the blood of the donor before the transplant to prevent rejection of the transplanted organ.
(Similarly, those who receive transfusions of whole blood or plasma have foreign proteins or protein fragments injected into their blood and can be expected to be subjected to the same disease risks, in addition to any underlying disease that they may have had to cause them to get a transfusion.)
According to hematologist Pollack and coworkers (1985) "derangement of immune function in hemophiliacs results from transfusion of foreign proteins or a ubiquitous [non-HIV] virus rather than contracting an AIDS infectious agent". Madhok and coworkers (1986) reported that ''clotting factor concentrate impairs the cell mediated immune response to a new antigen in the absence of infection with HIV". Aledort observed that "chronic recipients . . . of Factor VIII, Factor IX and pooled products . . . demonstrated significant T-cell
abnormalities regardless of the presence of HIV antibody" (Aledort, 1988).
Two controlled studies showed directly that protein impurities (of commercial clotting Factor VIII), rather than Factor VIII itself or HIV, were immunosuppressive among Factor VHI-treated, HIV-positive hemophiliacs. Over a period of two years the T-cells of HIV-positive hemophiliacs treated with commercial Factor VIII declined by 50%, while those of matched HIV-positive hemophiliacs treated with purified Factor VIII remained unchanged (de Biasi, et al., 1991, Seremetis, 1993).
Isn't there any evidence showing that HIV in blood products cause AIDS?
The National Academy of Sciences committee on AIDS accepted the hypothesis that so-called 'AIDS-causing' viruses could be transmitted by transfusion (Institute of Medicine, 1986). However this hypothesis was not based on controlled studies. For example, it was hypothesized that hemophiliacs (or other recipients of transfusions) would get AIDS from HIV transmitted along with a blood transfusion. It is true that a few hemophiliacs have developed pneumonia subsequent to a transfusion containing HIV, but the question was never answered as to whether it was HIV or some other contaminants in the blood that caused AIDS.
Several investigators comparing HIV-negative to HIV-positive hemophiliacs have noted that the more transfusions one gets, the more likely they are to be HIV-positive (see table below derived from Cohen, 1994). This is not surprising because HIV is a rare contaminant of blood and blood products. The more transfusions a person receives, the more likely they are to be HIV-positive.
According to Yiamouyiannis, the number of transfusions a person receives is not the only factor determining whether a hemophilia patient will become HIV-positive. The state of a hemophiliac's immune system can also determine whether HIV-antibodies are produced. This can explain why, in the previous table, some receiving moderate doses of Factor VIII are not HIV-positive and most receiving low doses of Factor VIII are HIV-positive. As pointed out in the introduction, if a hemophiliac's immune system is so poor that its nonspecific immune system is unable to cope with a virus, such as an HIV, and it has to call in the specific immune system to make antibodies to control the infection, that individual will be recorded as HIV-positive. However, if their immune system is in good shape, they can be exposed to HIV through transfusions and still remain HIV-negative according to the antibody test. Again, the HIV-positive response is an indication of a pre-existing immune deficiency and one would expect that an HIV-positive hemophilia patient would be more likely to come down with AIDS than one who is HIV-negative, even if they both received the same doses of Factor VIII.
In fact, investigators comparing HIV-negative to HIV-positive hemophiliacs have observed that immunodeficiency is more often affiliated with HIV-positives (Tsoukas, et al., 1984; Kreiss, et al., 1986; Sullivan, et al., 1986; Koerper, et al., 1989; Becherer, et al., 1990; see the following table). This is not surprising. As pointed out in the previous table, being HIV-positive as a hemophiliac is an indication that an individual has received more clotting factor concentrates, leading to a greater risk of inducing an autoimmune response to their own immune system. In addition, Kreiss and his coworkers (1986) point out that "seropositive [HIV-positive] hemophiliac subjects, on average, had been exposed to twice as much concentrate . . . as seronegativefs]."
Immunosuppression (T4/T8 about or less than 1)
Study HIV-negative HIV-positive
Tsoukas, et al. (1984) 43% 6/14 60% 9/15
Kreiss, et al. (1986) 35% 6/17 92% 22/24
Gill, etal. (1986) 33% 8/24 94% 30/32
Nonetheless, as can be seen in the above table, immunodeficiency, as determined by depressed ratios of two types of T-lymphocytes, T4 and T8, were observed in some HIV-negative hemophiliacs. Kreiss and coworkers (1986) even document AIDS-defining diseases in an HIV-free hemophiliac. Other controlled studies show that immunodeficiency in hemophiliacs occurs in the absence of HIV, and that the lifetime dosage of transfusions is the cause of AIDS-defining diseases of hemophiliacs (Duesberg, 1995b). Hemophiliacs with AIDS-defining diseases have exactly the same diseases and death rates whether or not they are HIV-positive.
Age and sex of hemophiliacs dying from 'HIV-related diseases'
Chorba, et al. (1994) reported that from 1987 to 1989, 815 male hemophilia A patients died and that 469 or 58% of them died from 'HIV-related diseases'. During the same period, 38 female hemophilia A patients died and only 1 or 2.6% of them died from 'HIV-related diseases'. If HIV obtained from transfusions was the cause, there should be no difference in the percentage of men and women dying from 'HIV-related diseases' among hemophiliacs. But there is — over a 20-fold difference.
In the same study, deaths from non-HIV infectious diseases increased from 15 in 1979-1981 to 67 in 1983-1985 to 139 in 1987-1989. How could HIV be responsible for the rise in deaths due to non-HIV diseases? This again shows that something else, Factor VIII impurities maybe, but certainly not HIV, is causing an increase in diseases resulting from weakened immune systems.
Chorba and his coworkers (1994) point out that "A low HTV-1 seroprevalence in the pediatric hemophilia population and an increasingly greater seroprevalence among older persons with hemophilia was expected and observed/' Nonetheless, the percentage of those hemophilia A patients dying from 'HIV-related diseases' did not increase with increasing age, a measure of increasing prevalence of HIV, as can be seen from the following table.
Instead as is observed with members of the general population, what is referred to as deaths from 'HIV-related diseases' occur predominantly among males and predominantly among those between the ages of 20 and 49, not among those groups that had a high rate of HIV-positives.
Other transfusion recipients
Half of the American transfusion recipients are said to die within a year after being transfused with blood containing HIV. What HIV/AIDS proponents don't tell you is that half of the American transfusion recipients without HIV also die within a year after being transfused — exactly the same. (Hardy, et al., 1985; Ward, et al., 1989).
The reason is because the average American transfusion recipient is not a 19-year-old kid falling from a motorcycle, but a 77-year-old like the California tax reformer, Paul Gann. What HIV/AIDS proponents don't tell you is that when he
died, Gann was 77 years old, that he had a 5-fold bypass operation (as well as a threefold bypass operation 8 or 9 years earlier), then fell in his home and busted his hip, was immobilized in a hospital in Los Angeles for 2 weeks, and developed pneumonia, when he then became of course, by definition, an AIDS patient (Duesberg, 1992g).
That's what the majority of transfusion recipients are, and half of them simply die within a year of the transfusion because of the underlying diseases that led them to get a transfusion. Like hemophiliacs, they get pneumonia and opportunistic infections. The diseases they get are significantly different from the diseases of other risk groups. Hemophiliacs and transfusion recipients almost never get Kaposi's sarcoma or dementia.
A properly designed study to determine whether HIV causes AIDS in transfusion recipients would have been conducted as follows. The study would have examined ten Paul Ganns or ten HIV-positive men or women of that age group who had bypass operations and broken hips and were hospitalized and immobilized for two weeks. It would have compared this group with ten men or ten women without HIV, but with similar medical histories and determined how many of them developed pneumonia. It would have found out whether or not those with HIV were dying from pneumonia while the others, those without HIV, were jogging on the beaches of Los Angeles.
There is actually one controlled study in the New England Journal of Medicine which examined 400 transfusion recipients in San Francisco: 200 with HIV and 200 without. In this study, Ward and coworkers (1989) found exactly the same mortality in both groups. Half of the 200 with the HIV and half of those without HIV were dead within the year after receiving the transfusions.
Nowhere have we been able to find any evidence whatsoever that transfusion of HIV ever caused any diseases.
AIDS-type diseases in hemophiliacs and transfusion recipients prevalent before HIV became the rage
Before HIV and AIDS came on the scene, a multicenter study investigated the immune systems of 1551 hemophiliacs treated with Factor VIII from 1975 to 1979. This study documented a decrease in the number of lymphocytes in 9.3% and a decrease in the number of thrombocytes in 5% of all hemophiliacs treated with Factor VIII (Eyster, et al., 1985). This is consistent with destruction of lymphocytes, of which T-cells are a type, via an autoimmune response set off by factor VIII. It also explains why the resulting opportunistic infections occur in both HIV-positive and HIV-negative hemophiliacs.
Accordingly, AIDS-defining opportunistic infections, including 60% pneumonias and 20% tuberculosis, have been recorded in hemophiliacs between 1968 and 1979 (Johnson, et al., 1985). These transfusion-acquired immunodeficiencies could more than account for the 2% annual incidence of AIDS-defining diseases in HIV-positive hemophiliacs recorded now (Centers for Disease Control, 1992b). In 1983, an American hematologist who recorded opportunistic infections in hemophiliacs occurring between 1968 and 1979, including 2 candidiasis and 66 pneumonia deaths, commented "... it seems possible that many of the unspecified pneumonias in hemophiliacs in the past would be classified today as AIDS" (Aronson, 1983).
Immune deficiency in hemophiliacs is a function of the life-time dosage of blood units that they have received as well as the prior immune status of the individual, not whether or not they are HIV-positive. The more transfusions they have received, the more foreign proteins they get and the more likely they are to have a suppressed immune system. That theory was very popular before HIV and in fact continued to be published for several years thereafter, but it was not widely publicized. Once the virus hypothesis became totally dominant in 1988, new studies describing HIV-free immunod-eficient hemophiliacs and the question whether HIV-free
immunodeficient hemophiliacs ever developed AIDS-defining diseases became taboo.
In summary, HIV is merely a marker for the number of transfusions and Factor VIII treatments received. Immune suppression in hemophiliacs is the price they have to pay for the prolongation of their life. They depend on regular transfusions, or Factor VIII. However most currently available commercial Factor VIII is contaminated with foreign protein which makes up more than 99% of the product. Factor VIII makes up less than 1% of the product. While contamination of Factor VIII presents a real and serious problem, prior to the advent of Factor VIII therapy, most hemophiliacs died as adolescents from internal bleeding (Koerper, 1989). This is now being prevented by treatment with Factor VIII. Recent findings that uncontaminated Factor VIII does not suppress the immune system proves this foreign-protein hypothesis correct (de Biasi, et al., 1991; Seremetis, et al., 1993). Indeed about a third of the HIV-positive hemophiliacs treated with purified Factor VIII not only maintained their immune systems in the state it was prior to therapy, but even recovered lost immunity — despite the presence of HIV (Seremetis,et al., 1993).
Chapter 16
What Causes AIDS in 'at risk' Homosexuals and Other Intravenous Drug Users?
While they comprise only about 5% of the population, male homosexuals account for approximately 60% of AIDS cases and at least 92% of the AIDS-related Kaposi sarcoma cases in the U.S (CDC, personal communication, 1993). Male homosexuals who get AIDS are virtually confined to groups that engage in homosexual activities with large numbers of partners (Centers for Disease Control, 1982; Jaffe, et al., 1983b; Darrow, et al., 1987; Oppenheimer, 1992) that often average over 100 per year and have exceeded 1000 over a period of several years (Mathur-Wagh, et al., 1984; Newell, et al., 1985a; Turner, et al., 1989; Callen, 1990). This is undoubtedly one of the main reasons why some have come up with the idea that AIDS was a disease that was passed on through homosexual activities.
This group of highly active homosexual men are long-term users of not only injected drugs, but also other drugs that are used mainly, or partly at least, as aphrodisiacs and facilitators of anal intercourse — specifically, nitrite inhalants that were designed a hundred years ago as vasodilators (agents used to open up blood vessels) against angina. They are psychoactive drugs that give a 'high' and also facilitate anal intercourse by relaxing smooth muscles. Their use in enhancing homosexual activities was accidentally discovered in the sixties and has since become a banner of 'gay' liberation.
(CH3)2CHCH2CH2-0-N=0 CH3CH2CH2CH2-0-N=0
amyl nitrite butyl nitrite
Indeed, Kaposi's sarcoma and other AIDS-defining diseases were observed in male homosexuals who took drugs before HIV was discovered. The first five AIDS cases, diagnosed in 1981 before HIV was known, were male homosexuals each of whom had consumed nitrite inhalants (Centers for Disease Control, 1981; Gottlieb, et al., 1981; Jaffe, et al., 1983a). AIDS has since been observed in HIV-free homosexuals consuming nitrites and other 'recreational drugs'. These cases include 153 immunodeficient HIV-free homosexuals (Drew, et al., 1985; Weber, et al., 1986; Novick, et al., 1986; Collier, et al., 1987; Bartholomew, et al., 1987; Buimovici-Klein, et al., 1988) and 23 HIV-free Kaposi's sarcomas (Afrasiabi, et al., 1986; Ho, et al., 1989b; Friedman-Kien, et al., 1990; Bowden, et al., 1991; Safai, et al., 1991; Castro, et al., 1992; Huang, et al., 1992).
Among a group of homosexuals that have been using nitrite inhalants or 'poppers', six had Kaposi's sarcoma, yet not one of them was HIV-positive (Friedman-Kien, 1990).
Kaposi's sarcoma frequently has been diagnosed in male homosexuals in the absence not only of HIV, but also in the absence of immunodeficiency as determined by the standard immunodeficiency tests used by AIDS researchers. For example, the immune systems of 20 out of 37 HIV-positive homosexuals with Kaposi's sarcoma were normal when their disease was first diagnosed (Spornraft, et al., 1988). Another study also describes 19 male homosexual Kaposi's sarcoma patients with normal immune systems (Murray, et al., 1988). Likewise, Kaposi's sarcomas have been diagnosed in HIV-free male homosexuals with normal immune systems (Afrasiabi, et al., 1986; Archer, et al., 1989; Friedman-Kien, et al., 1990; Marquart, et al., 1991). This indicates that cancer-causing agents like nitrites can result in Kaposi's sarcoma before any immunodeficiency could be determined by the tests currently being used.
Just before the virus hypothesis was announced in 1984, the Centers for Disease Control still studied what was then called the 'Life-style Hypothesis' — a euphemism for drug-users and homosexuals at that time.
Drug use among homosexuals in 1983 and 1987
Percentage Using Drug Drug Used 1983 1987
The above table lists the drugs used and the incidence of drug usage among 170 homosexuals in 1983, including 50 with AIDS (Kaposi's sarcoma and pneumonia) and 120 without AIDS. The study was done by Henry Jaffe, the director of HIV/AIDS at the CDC (Jaffee, et al., 1983). You can see 96 percent of them self-reported regular use of nitrite inhalant, as well as the use of ethyl chloride inhalants, cocaine, amphetamines, phenylcyclidine, Quaaludes, barbituates, marijuana, and heroin. So these fellows were walking pharmacies, but they were told that HIV — and not these drugs — did all the damage. In 1987 and 1990, similar studies were again conducted by the CDC on homosexuals in San Francisco (Darrow, et al., 1987; Wilson, et al., 1990; Lifson, et al., 1990). Overall drug use was high among homosexuals in 1987 (see the above table) and it is still high.
In 1993, two epidemiological studies from San Francisco and Vancouver again confirmed that every one of several hundred men with AIDS had been on "recreational drugs" such as nitrite inhalants, amphetamines, and cocaine or on AZT (Ascher, et al., 1993; Schechter, et al. 1993; Duesberg, 1993b).
Part of the reason that drug use is still high is because the medical orthodoxy essentially tells the American consumer and the homosexuals 'Don't worry about drugs.' What they say in their AIDS prevention program is: 'Make sure you wear a condom and use a clean needle. We are not the police. We are not bigots. You can use your drugs. They don't hurt you. They may be against the law, but they have nothing to do with AIDS. HIV causes AIDS'.
That is the message of the medical orthodoxy. Former Surgeon General Koop, Fauci, and others — they print it, it's on television, it's in The New York Times, everywhere. Drugs are harmless as long as your needle is clean and your condom is of Michelin quality. What they don't tell you is that it's not what's on the needle but what's in the needle that counts.
Nitrite Inhalants
Nitrite inhalants in the amounts used by the homosexuals are toxic and depress the immune system (Newell, et al., 1985b; Schwartz, 1988; Osterloh and Olson, 1986; Maikel, 1988; Newell, et al., 1985b, 1988; Wood, 1988; Goedert, et al., 1982; Haverkos, 1988a). They cause genetic damage and cancer. They have been shown to transform normal cells into cancer cells in tissue cultures, and to cause cancer in animals (Jorgensen and Lawesson, 1982; Hersh, et al., 1983; Mirvish et al., 1987, 1988, 1993; Newell, et al., 1988, Winter, 1989; Lewis, 1989). The Food and Drug Administration limits the concentration of nitrites to less than ten parts per million. You cannot sell your lox, or your meat, or your Polish sausage or German sausage with more than ten parts per million nitrite.
But the amount that is consumed as a recreational 'hit' by homosexuals, in a gay bar, is far more — up to a milliliter per person, per night, or even more. Those guys couldn't be sold on the meat market for at least two or three days! — according to the FDA's guidelines on nitrite contamination. But if you point out that this may be toxic you're immediately labeled — you're a homophobe, you're a bigot, you're a fascist,
you're a communist. But when it comes to lox, everyone agrees, you can't sell the lox anymore! But, your homosexual partner with a milliliter of nitrite in him is fine.
There seemed to be some ray of hope amidst mostly dark clouds. From 1984 to 1991, the use of nitrite inhalants among male homosexuals decreased by 50% (Lesbian and Gay Substance Abuse Planning Group, 1991b). In parallel, the incidence of Kaposi's sarcoma among American AIDS patients decreased from a high of 50% in 1981 (Haverkos, 1988b) to a low of 10% in 1991 (Centers for Disease Control, 1992b). However, according to the National Institute on Drug Abuse and the Centers for Disease Control, use among homosexuals has increased in the 1990s (Haverkos and Drotman, unpublished).
Because of their toxicity, a prescription requirement was instated for the sale of nitrite inhalants by the Food and Drug Administration in 1969 (Newell, et al., 1985b). Because of an 'AIDS link' (Cox, 1986), the sale of nitrites was banned by the U.S. Congress in 1988 (Public Law 100-690) (Haverkos, 1990) and by the 'Crime Control Act of 1990' (January 23, 1990).
There is certainly more than enough information showing a link between AIDS in the form of Kaposi's sarcoma and nitrite inhalants.
Before HIV was known, three controlled studies compared (1) 20 homosexual AIDS patients to 40 AIDS-free controls (Marmor, et al., 1982), (2) 50 patients to 120 controls (Jaffe, et al., 1983b) and (3) 31 patients to 29 controls (Newell, et al., 1985a) to determine AIDS risk factors. Each study reported that multiple 'street drugs' were used as sexual stimulants. These studies concluded that the consistent use of nitrites provided a 94% to 100% association with AIDS.
A 4.5-year tracking study of 42 homosexual men with lymphadenopathy (abnormal swelling of the lymph glands) but not AIDS report that 8 had developed AIDS within 2.5 years (Mathur-Wagh, et al., 1984) and 12 within 4.5 years of observation (Mathur-Wagh, et al., 1985). All of these men had used nitrite inhalants and other inhalants and other recreational drugs including amphetamines and cocaine, but they were not tested for HIV. The authors concluded that "a
history of heavy or moderate use of nitrite inhalant before study entry was predictive of ultimate progression to AIDS" (Mathur-Wagh, et al., 1984).
The National Institute on Drug Abuse reports correlations from 69% (Lange, et al., 1988) to virtually 100% (Haverkos, 1988a; Newell, et al., 1988) between nitrite inhalants and other drugs and subsequent Kaposi's sarcoma and pneumonia.
In 1985, and again in 1988, Haverkos analyzed the AIDS risks of 87 male homosexual AIDS patients with Kaposi's sarcoma (47), Kaposi's sarcoma plus pneumonia (20) and pneumonia only (20) (Haverkos, et al., 1985; Haverkos, 1988b). All men had used several sexual stimulants, 98% had used nitrites. Those with Kaposi's sarcomas reported double the amount of sexual partners and 4.4-times more receptive anal intercourse than those with only pneumonia. The median number of sexual partners in the year prior to the illness was 120 for those with Kaposi's and 22 for those with pneumonia only. The Kaposi's cases report 6-times more amyl nitrite and ethyl chloride use, 4-times more barbituate use, and twice the methaqualone, lysergic acid and cocaine use than those with pneumonia only. Since no statistically significant differences were found for sexually transmitted diseases among the patients, the authors concluded that the drugs had caused Kaposi's sarcoma.
A 27- to 58-fold higher consumption of nitrites by male homosexuals compared to heterosexuals and lesbians (Lesbian and Gay Substance Abuse Planning Group, 1991) correlates with a 20-fold higher incidence of Kaposi's sarcoma (Selik, et al., 1987; Beral, et al., 1990) and a higher incidence of all other AIDS diseases in male homosexuals compared to most other risk groups.
A study investigating AIDS risk factors among French homosexuals reported that 31% of those with AIDS, but only 12% of those without AIDS, had achieved "over 100 nitrite inhalations' (Messiah, et al., 1988). The study included 53, or 45%, of all homosexual AIDS patients recorded in France by 1987.
A survey of homosexual men from Boston, conducted between 1985 and 1988, documented that drug abuse was more prevalent among HIV-positives than HIV-negatives: among 206 HIV-positives 92% had used nitrite inhalants, 73% cocaine, 39% amphetamines, 29% lysergic acid in addition to six other psychoactive drugs as sexual stimulants; among 275 HIV-negative controls, 71% had used nitrites 57% cocaine, 21% amphetamines, and 17% lysergic acid in addition to six other psychoactive drugs (Seage et al., 1992).
Drug-abusing heterosexuals
With the exception of Kaposi's sarcoma, the incidence and the types of AIDS diseases of intravenous drug users and homosexuals is virtually identical. If found to be HIV-positive, each group has about a five percent annual risk of developing AIDS.
About a third of all American and European AIDS patients are heterosexuals, but most of them are intravenous drug users (National Commission on AIDS, 1991; Centers for Disease Control, 1992b; Brenner, et al., 1990; World Health Organization, 1992a).
In an article titled "AIDS and intravenous drug use: the real heterosexual epidemic", AIDS researcher Moss (1987) points out that "90% of HIV-infected prostitutes reported in Florida, Seattle, New York and San Francisco have been intravenous drug users". Indeed, studies of American and European prostitutes indicate that AIDS is almost exclusively restricted to drug users (Rosenberg and Weiner, 1988), although all prostitutes should have the same risks of HIV infection if HIV were sexually transmitted.
So do we have any evidence that these 'recreational drugs' are immunotoxic? Or that drug use is toxic? Indeed, when you check the literature there is a lot of it starting in 1909. At the time, cocaine use was common.
At that time, there was a mild epidemic in Europe and it was found that cocaine addicts had the same diseases that
are called AIDS now. Immune deficiency, weight loss, fever, mouth infections, endocarditis, pneumonia, tuberculosis, all the 'good old AIDS diseases' were observed as early as 1909 in long-term recreational drug users. We are not talking about one party per month or parties on weekends; these diseases occurred among serious long-term addicts (Archard, et al., 1909; Terry and Pellens, 1928; Briggset al., 1967; Dismukes, et al., 1968; Sapira, 1968; Harris and Garret, 1972; Geller and Stimmel, 1973; Brown, et al., 1974; Louria, 1974; McDonough, et al., 1980; Cox, et al., 1983; Kozel and Adams, 1986; Selwyn, et al., 1989; Kreek, 1991; Pillai, et al., 1991; Bryant, et al., 1992).
Intravenous drugs can be toxic directly and indirectly. Indirect toxicity can be due to malnutrition, because of the enormous expense of illicit drugs, or to septicemia because most illicit drugs are not sterile (Cox, et al., 1983; Stoneburner, et al., 1988; Lerner, 1989; Buehler, et al., 1990; Pillai, et al., 1991; Luca-Moretti, 1992). Typically, intravenous drug users develop pneumonia, tuberculosis, endocarditis and wasting diseases (Layon, et al., 1984; Stoneburner, et al., 1988; Braun, et al., 1989; Brudney and Dobkin, 1991). Oral consumption of cocaine and other psychoactive drugs has been reported to cause pneumonitis, bronchitis, edema (Ettinger and Albin, 1989), and tuberculosis (Brudney and Dobkin, 1991). According to the National Institute on Drug Abuse, "Cocaine is currently the drug of greatest national concern, from a public health point of view . . . " (Schuster, 1984).
Since the early 1980s, when T-cell ratios became measurable, low T4 to T8-cell ratios averaging 1 or less and thus indicating immunodeficiency were reported in addicts who had injected drugs for an average of 10 years (Layon, et al., 1984).
In a group of 21 long-term heroin addicts, the ratio of T4 to T8 cells declined during 13 years from a normal of 2 to less than 1, again indicating immunodeficiency (Centers for Disease Control, 1987; Institute of Medicine, 1988), but only 2 of the 21 were infected by HIV (Donahoe, et al., 1987).
In New York, 65 intravenous drug users were introduced into a methadone drug-withdrawing program. Some chose to work in the methadone program and gave up drugs. Others continued to use street drugs. Those who continued to use street drugs continued to lose 35 percent of their T-cells per year. Those who stopped didn't lose any further T-cells. Their T-cell levels stabilized (Des Jarlais, et al., 1987).
Another similar study from Zurich, Switzerland followed three hundred asymptomatic HIV-positive intravenous drug users. Some continued to use drugs. Some stopped. Those who continued to use street drugs had three times as many AIDS-defining diseases per year as those who stopped (Weber, et al., 1990).
HIV-positive and HIV-negative drug users have the same diseases and similar mortality rates.
Lymphadenopathy (abnormal swelling of the lymph glands), weight loss, fever, night sweats, diarrhea, and mouth infections were observed in 49 out of 82 HIV-free, and 89 out of 136 HIV-positive, long-term intravenous drug users in New York (Des Jarlais, et al., 1988).
Among intravenous drug users in France, lymphadenopathy was observed in 41 of 69 HIV-positives, and in 12 out of 44 HIV-negatives; in addition, a weight loss of over 10% was observed in 15 of 69 HIV-positives, and in 8 out of 44 HIV-negatives (Espinoza, et al., 1987). Individuals in these groups had used drugs for an average of 5 years, but the HIV-positives had injected drugs about 50% longer than the negatives.
In a group of 510 HIV-positive intravenous drug users in Baltimore, 29% reported one and 19% reported two or more of the following diseases: oral thrush, fatigue, chronic diarrhea, weight loss, and shortness of breath. In a control group of 160 HIV-negative intravenous drug users matched with the HIV-positives for "current drug use", again 29% reported one and 13% reported two or more of these symptoms (Munoz, et al., 1992).
In 1989, the annual mortality of 197 HIV-positive, injectable drug users from Amsterdam with an average age of 29 years was 4% and that of 193 age-matched HIV-negatives was 3% (Mientjes, et al., 1992). The annual incidence of pneumonia was 29% in the HIV-positives and 9% in the negatives. The HIV-positive drug users had injected more drugs for a longer time, 84% of the positives as opposed to 64% of the negatives had injected over the last 5 years.
The annual mortality of 108 HIV-free Swedish heroin addicts was similar to that of 39 HIV-positive addicts, i.e. 3-5%, over several years (Annell, et al., 1991).
A survey of over a thousand intravenous drug addicts from Germany (Puschel and Mohsenian, 1991) and another study from Berlin (Bschor, et al., 1991) showed that the mortality rates of HIV-positive and HIV-negative drug users were similar. 18
Among intravenous drug users in New York who had died from a 'spectrum of HIV-related diseases', 22 out of 50 pneumonia deaths, 7 out of 22 endocarditis deaths, and 11 out of 16 tuberculosis deaths (Stoneburner, et al., 1988) were HIV-antibody positive, and thus AIDS patients.
Among 54 prisoners with tuberculosis in New York state, 47 were street-drug users, but only 24 were infected with HIV and therefore classified as AIDS patients (Braun, et al., 1989).
Thrombocytopenia and immunodeficiency were diagnosed in 15 intravenous drug users on average 10 years after they became addicted, but 2 were not infected with HIV (Savona, et al., 1985).
18 these studies showed that the percentage of HIV-positives among drug deaths (10% and 20-30%, respectively) were exactly the same as or similar to that of HIV-positives among living intravenous drug users . Let us assume that 1000 drug addicts were examined and 200 died; 800 would still be alive. Then, in the first of these two studies, for the HIV-positive group, 10% of 200 or 20 died and 10% of 800 or 80 were still alive. This gives a mortality rate of 20%. Similarly, for the HIV-negative group, 90% of 200 or 180 died and 90% of 800 or 720 were still alive. This also gives a mortality rate of 20%.
Among 97 intravenous drug users in New York with active tuberculosis, 88 were HIV-positive and 9 were HIV-negative; among 6 'crack' (cocaine) smokers with tuberculosis, 3 were HIV-negative and 3 were positive (Brudney and Dobkin, 1991).
While immune-deficiency diseases are generally more prevalent among HIV-positive individuals, the above studies show that HIV is not necessary for the production of immune-deficiency diseases in drug addicts.
According to Duesberg, the presence of HIV antibodies is the result of frequent exposures to possibly infected sources due to frequent drug use and sexual contacts, which are sources of exposure to HIV.
According to Yiamouyiannis, since the presence of HIV antibodies is the result (rather than the cause) of a depressed immune system, HIV serves as a marker of a depressed immune system in those exposed to HIV whether or not the immune system is depressed as a result of drug abuse, other immunosuppressive drugs or chemicals, and/or inherent weaknesses in an individual's immune system. Persons with a depressed immune system can still be HIV-negative so long as they have not been exposed to HIV.
Chapter 17
What Causes AIDS in Babies?
American babies have a high annual incidence of AIDS when they're born with HIV (25% of the HIV-positive babies get AIDS after the first year), but in contrast to other risk groups, AIDS babies get dementia and bacterial infections.
Eighty percent of all American and European AIDS babies are born to mothers who are intravenous drug users (Amaro, et al., 1989; Mok, et al., 1987; European Collaborative Study, 1991). When you look at mothers who are drug users during pregnancy and are HIV-negative, you find that their babies also get dementia and bacterial infections. Thus it is drug use, not HIV, that is associated with these diseases in children.
It is obvious that the drug habits of pregnant women influence the immune status of the children they subsequently bear. Many 'crack babies' will never live a full life because of the damage these drugs can do to their mental competence. Physiological and neurological deficiencies, including mental retardation, are observed in children born to mothers addicted to cocaine and other narcotic drugs (Fricker and Segal, 1978; Lifschitz, et al., 1983; Alroomi, et al., 1988; Blanche, et al., 1989; Root-Bernstein, 1990a; Toufexis, 1991; Finnegan, et al., 1992; Luca-Moretti, 1992). Thus, it is not surprising that maternal drug consumption has been blamed for the new epidemic of immunological and neurological deficiencies, including dementias, of American children (Toufexis, 1991).
The CDC acknowledges, "We cannot discern, however, to what extent the upward trend in death rates from drug abuse reflects trends in illicit drug use independent of the HIV epidemic" (Buehler, et al., 1990). This is especially true when
you consider that an HIV-antibody-positive response (and certainly AIDS) is most likely in a person with a weakened immune system and that drug abuse weakens the immune system. While drug abuse can cause immunodeficiencies and dementias in the children of HIV-free mothers, unfortunately, the studies that have been done have not compared the mental health of drug-abusing and drug-free HIV mothers to see if what appears to be HIV-mediated AIDS is actually due to drug abuse. However, the studies that have been done again indicate that maternal drug abuse, not HIV, results in the AIDS defining diseases. Consider the following studies.
One HIV-positive and 18 HIV-free infants born to intravenous drug-addicted mothers had only half as many white blood cells at birth as normal infants. Twelve months after birth, the capacity of their lymphocytes to proliferate was 50-70% lower than normal (Culver, et al., 1987).
Ten HIV-free infants born to intravenous drug-addicted mothers had the following AIDS-defining diseases, "failure to thrive, persistent generalized lymphadenopathy, persistent oral candidiasis, and developmental delay ..." (Rogers, et al., 1989).
According to a European Collaborative Study performed in 1991, "Children with drug withdrawal symptoms" were most likely to develop diseases; those of former drug users did not significantly differ from those born to women who had no history of IV drug use; whereas children with no withdrawal symptoms but "whose mothers had used recreational drugs in the final 6 months of pregnancy were intermediate" in their susceptibility to disease.
While it is obvious that the drug habits of the mother can lead to immune deficiency and the diseases associated with AIDS in HIV-free children, when these children are additionally exposed to HIV, they will also become HIV-positive and thus classifiable as AIDS patients.
Perinatal transmission of HIV
Perinatal transmission of HIV is the only efficient natural transmission of HIV — and is thus essential for the survival of the virus, just as it is essential for the survival of other animal and human retroviruses. Based on HIV-tracking via the HIV-antibody test, perinatal transmission from the mother is estimated to be 13-50% efficient (Blattner, et al., 1988; Blattner, 1991; Duesberg, 1991a; Institute of Medicine, 1988; European Collaborative Study, 1991).
The real efficiency of perinatal transmission must be even higher than the antibody tests suggest, because in a fraction of the infants receiving HIV from their mothers, HIV only becomes immunogenic, and thus detectable by the HIV-antibody tests, when its hosts pass through infancy (Quinn, et al., 1986; St Louis, et al., 1991). We know that this is the case because, during the antibody-negative phase in these infants, latent HIV can be detected by the polymerase chain reaction (Rogers, et al., 1989, European Collaborative Study, 1991). This is also true for other perinatally transmitted human (Blattner, 1990; Duesberg, 1991a) and animal retroviruses (Rowe, 1973; Duesberg, 1987).
However, if a virus is perinatally transmitted in nature, it cannot at the same time be deadly as HIV is claimed to be, because it would destroy the host before it could be passed on. Hence, HIV must be a harmless passenger virus, just like most other retroviruses.
HIV by itself does not pose a risk to infants
The risk for AIDS-defining diseases for HIV-positive babies, in the absence of other risk factors, is the same as that of HIV-free controls. A controlled study from Africa compared 218 newborns from HIV-positive mothers with 218 from HIV-negative mothers. The "rates of prematurity, low birth weight, congenital malformations and neonatal mortality were comparable in the two groups" (Lepage, et al., 1991). In Central Africa, 1-2% of healthy children are HIV-positive (Quinn, et al., 1986).
Chapter 18
What Causes AIDS in Africans?
We have two entirely different AIDS epidemics: the American-European epidemic and the African epidemic. In the American-European epidemic, ninety percent of the AIDS cases are male; in the African epidemic, AIDS cases are equally distributed between the sexes.
The epidemics also differ with regard to where the AIDS patients come from. In Europe and America, the vast majority of all AIDS patients are either IV drug users, homosexuals, or hemophiliacs. In Africa, the AIDS patients are merely poor.
Clinically, the prevalence of the various diseases in the American-European epidemic and the African epidemic are also very different.
Most AIDS diseases in America and Europe are pneumonia, candidiasis, mycobacterial infections, Kaposi's sarcoma, and dementia. In Africa, fever, diarrhea, and tuberculosis comprise a major portion of the AIDS diseases. Africans develop Africa-specific AIDS diseases 10 times more often than Americans. Americans or Europeans develop Kaposi's sarcoma 10 times more often than Africans. We have been unable to find a single report of a death from Pneumocystis pneumonia (a major cause of death from AIDS in America) in Africa.
And here's something else to consider. A high percentage of the African population is HIV-positive — over 10 million according to the latest estimate — but the number of AIDS cases is relatively low. As a result, an HIV-positive person in Africa has an extremely low annual risk of getting AIDS. If you are HIV-positive in Africa, you have only a 0.2 percent chance of getting AIDS each year. So, if you believe in the
AIDS
HIV/AIDS hypothesis and live in the U.S. or Europe, your best bet is go to Africa and lower your odds of getting AIDS by 90%.
Geographic group
Americans Europeans Africans
HIV-positives
who get AIDS
each year
Characteristic diseases
3% opportunistic infections
3% opportunistic infections
0.2% fever, diarrhea, tuberculosis
(from Morgan, et al., 1990; Centers for Disease Control 1992a,b)
Instead of a new virus, malnutrition, parasitic infections and poor sanitary conditions have all been proposed as causes of African AIDS-defining diseases (Editorial, 1987; Konotey-Ahulu, 1987, 1989; Rappoport, 1988; Adams, 1989). Further, it has been proposed that the incidence of tuberculosis, diarrhea, fever, and other African AIDS-defining diseases may be the same in Africans with and without HIV (Editorial, 1987). And prior to the discovery of HIV, protein malnutrition was identified by the AIDS researchers such as Fauci and his coworkers as the world's leading cause of immunodeficiency, particularly in underdeveloped countries (Seligmann, et al., 1984).
Indeed, recent studies document that only 2168 out of 4383 (49.5%) African AIDS patients with slim disease, tuberculosis and other Africa-specific diseases, who all met the World Health Organization (WHO) definition of AIDS, were infected by HIV. These patients were from Abidjan, Ivory Coast (DeCock, et al., 1991; Taelman, et al., 1991), Lusaka, Zambia and Kinshasa, Zaire (Taelman, et al., 1991). Another study reports 135 (59%) HIV-free AIDS patients from Ghana out of 227 diagnosed by the clinical criteria of the WHO. These patients suffered from weight loss, diarrhea, chronic fever, tuberculosis, and neurological diseases (Hishida, et al., 1992). An earlier study documents 116 HIV-negatives among
424 African patients who meet the WHO definition of AIDS (Widy-Wirski, et al., 1988).
So clinically and epidemiologically, the epidemic in Africa is totally different from the epidemics in America and Europe. The reason they are different is that their causes are different. In America and Europe, AIDS is mainly caused by illicit recreational drug use and misuse of medically administered drugs such as AZT. In Africa, AIDS is due mainly to malnutrition, parasitic infections, and poor sanitary conditions.
Again, according to Yiamouyiannis, in Africa, HIV is little more than a marker of an immune system depressed by malnutrition, parasites, environmental exposures and other factors (see Chapter 21).
Chapter 19
HIV and AIDS in Health Care Workers and Scientists
If HIV caused AIDS, then health care workers, those essential 'soldiers' confronting AIDS in the front line, would be the first ones that would contract AIDS from their patients. They would contract AIDS by treating patients, by washing them, by performing surgery on them, by filling their cavities, and by putting them in their coffins.
But in the scientific literature, there's not one case of a doctor in America who has contracted AIDS from his or her patients. And remember, this is supposed to be the infectious disease of the century. Despite the over four hundred thousand American AIDS patients who have either died with AIDS in hospitals or have been seen by doctors or by health care workers since 1981, not one single case has ever been confirmed in the literature where a doctor got AIDS from his or her patients. That's indeed remarkable for a presumably infectious disease.
If HIV caused AIDS, one would also expect that scientists who mass-produce HIV for the 'AIDS tests' at good commercial benefits to themselves would immediately be subject to HIV infection and AIDS. They would be dying like flies in the laboratories: rich, but dead from the so-called 'deadly' virus.
In reality, only one of over 10,000 HIV researchers has ever been alleged to have contracted AIDS from growing HIV in his or her laboratory (Cohen, 1994). Yet they grow virus at titers (concentrations) that have never been observed in AIDS patients. In AIDS patients, you would be lucky if you found
one infectious unit per milliliter 18 ; AIDS researchers grow it at a million infectious units per milliliter in their laboratories. Those laboratories may be operated at a very, very high level of security, but accidents still happen, even in the best labs. (For example, when Robert Gallo claimed to have isolated what was later to be called the HIV virus, it was never quite clear whether he had isolated his own virus or had just had his culture medium contaminated by a virus sent to him from Montagnier's lab.) However, to our knowledge, none of these researchers have gotten AIDS from HIV yet.
HIV also fails to cause AIDS when accidentally introduced into humans (Duesberg, 1992g). However the CDC claimed that seven health care workers have developed AIDS from occupational infection (Centers for Disease Control, 1992c). But the CDC failed to report the AIDS diseases of these seven workers or the diseases of those they allegedly got their AIDS from; they failed to report the sex of the workers and failed to report whether they developed AIDS only after AZT treatment (Centers for Disease Control, 1992c) (see Chapter 23). The CDC also failed to provide any evidence that these AIDS cases were not due to nonoccupational exposures, such as drug addiction. Indeed thousands of health care workers, e.g. 2586 by 1988 (Centers for Disease Control, 1988) have developed AIDS from nonprofessional causes.
AIDS is likewise not contagious to family members living with AIDS patients for at least 100 days in the same household (Friedland, et al., 1986; Sande, 1986; Hearst and Hulley, 1988; Peterman, et al., 1988). Contrary to the expectations of HIV/AIDS proponents that health care workers would be the first to be affected by infectious AIDS, the CDC reports that the incidence of AIDS among health care workers is about the same as that in the general population.
18 a milliliter is a measure of volume equal to the amount contained in a cube that is one centimeter by one centimeter by one centimeter; a centimeter is about 4/10ths of an inch. Most rulers have centimeters on the edge opposite the inch calibrations
AIDS
By 1988, 2586 out of 5 million health care workers had developed AIDS. During the same period 110,000 out of the 250 million Americans had developed AIDS (Centers for Disease Control, 1992b). The CDC reports that about 75% (or about 3.75 million) of the American health care workers are females, but that 92% (or about 2379) of the AIDS patients among health care workers occurred in (approximately 1.25 million) males (Centers for Disease Control, 1988). From these figures, a rough approximation of the relative AIDS risk of health care workers as compared to the general population can be calculated. These data appear on the following table:
AIDS incidence among health care workers as compared to the general population in the United States in 1988
U.S. general population
AIDS cases
males
females
both
99,000 11,000
Population Incidence rate (per 100,000)
125,000,000 79
125,000,000 9
110,000 250,000,000
44
U.S. general population (age 20-64)
An approximate age-matched comparison actually indicates that health care workers may have a slightly lower risk (52 AIDS cases per 100,000) than the general population aged 20-64 (74 AIDS cases per 100,000). If AIDS were a contagious disease, this would be very difficult to explain.
Chapter 20
Is AIDS excused by Some Other Virus?
In view of the fact that 30 mostly unrelated diseases have been classified as AIDS and because of the difficulties in attributing them to a common, active microbe, several investigators have proposed that AIDS is caused by a multiplicity of infectious agents such as viruses and microbes, or combinations of HIV with other microbes (Sonnabend, et al., 1983; Konotey-Ahulu, 1987, 1989; Stewart, 1989; Cotton, 1990; Goldsmith, 1990; Lemaitre, et al., 1990; Root-Bernstein, 1990a,c; Baiter, 1991; Lo, et al., 1991).
Typically, these investigators blame AIDS on viruses and microbes that are widespread and either harmless or not life-threatening to a normal immune system, such as Pneumocystis, cytomegalovirus, herpes virus, hepatitis virus, tuberculosis bacillus, Candida, mycoplasma, treponema, gonococci, toxoplasma and cryptosporidiae (Freeman, 1979; Mims and White, 1984; Pifer, 1984; Evans, 1989c; Mills and Masur, 1990; Bardach, 1992). Since such microbes are more commonly active in AIDS patients than in others, they argue that either chronic or repeated infections by these microbes would generate fatal AIDS (Sonnabend, et al., 1983; Stewart, 1989; Mills and Masur, 1990; Root-Bernstein, 1990a,c).
Yet all of these microbes also infect people with normal immune systems either chronically or repeatedly without causing AIDS (Freeman, 1979; Mims and White, 1984; Evans, 1989c; Mills and Masur, 1990). It follows that the ability of these microbes to produce disease in AIDS patients is a consequence of immunodeficiency acquired by other causes (Duesberg, 1990c, 1991a). This is why most of these infections are termed opportunistic.
To explain the cases of HIV-negative AIDS, some virus/AIDS matchmakers reached the consensus that an as yet undiscovered 'new AIDS virus', that "doesn't appear any more contagious than HIV" (Cowley, 1992), was to blame (Bowden, et al., 1991; Castro, et al., 1992; Huang, et al., 1992; Altman, 1992a,b; Cohen, 1992a,b; Laurence, et al., 1992).
AIDS is not compatible with infectious disease
The long and unpredictable intervals between infection and 'acquiring' primary AIDS symptoms — averaging two years in infants and 10 years in adults, and termed 'latent periods' — stand in sharp contrast to the short intervals of days or weeks between infection and primary disease observed with all other viruses, including retroviruses (Duesberg, 1987; Duesberg and Schwartz, 1992). These short intervals reflect the time periods that all microbes with generation times of half-hours and viruses including HIV (Clark, et al., 1991; Daar, et al., 1991) with generation times of 8-48 hours need to reach immunogenic and thus potentially pathogenic concentrations (Fenner, et al., 1974; Freeman, 1979; Mims and White, 1984). Once stopped by the immune system, conventional viruses and microbes are no longer pathogenic. Although HIV/AIDS proponents claim that HIV is a 'slow' virus and thus can cause disease long after neutralization by antiviral immunity (Evans, 1989c), there are, in fact no 'slow viruses'. There are slow virologists, but there are no slow viruses.
Is it true that AIDS is an infectious disease? Proponents of the virus hypothesis, orthodox AIDS researchers, acknowledge that AIDS is not an orthodox infectious disease. In 1992, Jaap Goudsmit, one of the leading AIDS researchers in Amsterdam, who collaborates closely with the NIH, acknowledged in the journal, Lancet, that "AIDS does not have the characteristics of an ordinary infectious disease. This view is incontrovertible." Eggers and Weyer (1990, 1991), two epidemiologists and statisticians from Germany, presented papers at the International AIDS conference in San Francisco in 1990. They concluded that AIDS does not spread like a nor-
mal infectious disease. They had to conjure up some reasons to explain why the AIDS distribution data did not fit the criteria of an infectious agent. They had to come up with some factor or factors to reconcile the fact that AIDS stays primarily in men, in male homosexuals, and in drug users, and yet is supposed to be an infectious disease.
And likewise, Anderson and May (1992), currently the leading AIDS epidemiologists in Great Britain (they frequently write for Science, Nature, and Scientific American) offered a different type of explanation. They said the disease follows 'assortative scenarios'. But what their claims boil down to is that when you are bad, if you don't use condoms and are a promiscuous homosexual, God punishes you with a bad virus and you get dementia and diarrhea. But if you use a condom and are a good person, then the virus won't hurt you so much and you live on for 10-20 years.
Gallo himself claims that he could live with HIV for as many as 20-30 years or more before getting AIDS, because he's free of other 'cofactors' that would lead to AIDS. In a personal interview, he pointed out that if he became HIV-positive, he could avoid AIDS by avoiding contact with people who are infected with opportunistic microbes that could result in one of the AIDS-defining diseases. Secondly, he would improve his diet. When pressed, he also admitted that he would avoid exposure to toxic or immunosuppresive chemicals (even admitting that he might not take AZT), that he would make sure he got an adequate amount of sleep, and that he would recommend exercise for the positive psychological effects it would have and the possible beneficial physiological effects it might have (Gallo, 1994).
A final contrast between AIDS and all other infectious diseases is that despite enormous efforts, no common active microbe has ever been found in AIDS patients. What is claimed to be found is HIV, but when it is found, it is by no
means active. It is only detected as a latent virus in one in a thousand T-cells. The reason for the notorious difficulties of leading AIDS researchers like Bob Gallo and Robin Weiss in England in isolating 'the active virus that causes AIDS' is that it isn't there. If HIV is found, it is not found in the active form.
Furthermore, the virus hypothesis has not made one single valid prediction, not even one. The failure to make valid predictions or produce results is usually the end of a hypothesis in science. Of course, if you get 6 billion dollars for it, then maybe you would study it a little more carefully too — and it doesn't hurt to study it very slowly and very carefully — for 6 billion dollars a year.
So, AIDS then, fails all criteria of a conventional infectious disease. It doesn't even meet one. It is very likely, therefore, that AIDS may not even be an infectious disease. Now, in the face of the problems that the virus hypothesis doesn't produce any results and that AIDS fails all criteria of an infectious disease and that HIV is a passenger virus, it is high time to come back to what we used to call the scientific method. That is, you observe the subject from all possible angles, make a hypothesis that makes testable predictions, test these predictions experimentally, and see whether you can come up with a hypothesis that works. And if it does, then you make patents and royalties and become famous. But if it doesn't work, then you have to come up with another hypothesis.
Chapter 21
What Causes AIDS?
We propose that AIDS in the U.S. and in Europe is caused by the long-term consumption of immunosuppressive recreational drugs, such as cocaine, heroin, and poppers or nitrite inhalants (Chapters 15 and 16) and by protein contaminants in blood and blood product transfusions (Chapter 14). We propose that AIDS in the U.S. and in Europe is also caused by immunosuppressive drugs such as, AZT, ddC, ddl, hydroxyurea, and chemotherapeutic drugs that are prescribed as anti-HIV drugs to HIV-positive persons with or without AIDS.
In addition, Yiamouyiannis proposes that AIDS in the U.S. and in Europe is caused in part, and in some cases, wholly, by immunosuppressive drugs that are sold over the counter or by prescription, such as ibuprofen (sold under the brand names of Motrin or Rufen), imipramine (also sold as Janimine, SK-pramine, and Tofranil), indomethacin, chloramphenicol, cortisone, prednisone, anabolic steroids, Premarin, methyldopa or Aldochlor, Valium, Opren, Darvon (propoxaphene), amoxicillin (Amoxil), and Procardia, as well as chemotherapeutic drugs used in the treatment of cancer.
Indeed, young rats treated for several weeks simultaneously with antibiotics and immunosuppressive cortisone all developed Pneumocystis pneumonia spontaneously (Weller, 1955). The Physicians 9 Desk Reference (PDR) lists "secondary infection" and "decreased resistance to infection' as side effects of cortisone therapy. (1983 PDR, p. 1384, 1407, 1601).
Before listing the immunosuppressive effects of some of the other commonly used drugs, it might be helpful to define some of the terms used. The immune system is composed of white blood cells and the tissues, such as the thymus and bone marrow, associated with them. Another term for white blood cell is leukocyte, "leuko" meaning white and "cyte" meaning cell.
granulocyte - a white blood cell containing granules.
agranulocytosis - a depressed level of granulocytes in the blood.
granulocytopenia - same as agranulocytosis.
phagocyte - cell which engulfs and destroys foreign materials.
neutrophil - a phagocytic granulocyte which does not stain with the
dyes normally used to stain cells.
neutropenia - a depressed level of neutrophils in the blood.
eosinophil - a granulocyte which stains with a dye called eosin.
eosinophilia - an abnormal increase in eosinophils in the blood.
thrombocyte - a white blood cell involved in clotting.
-penia - deficiency.
thrombocytopenia - a depressed level of thrombocytes in the blood.
Coombs positive - antibody-coated red blood cells suggestive of
autoimmune destruction of red blood cells.
purpura - purplish discoloration in the skin due to hemorrhaging.
hemolytic anemia - depression in red blood cell and/or hemoglobin.
aplastic anemia - depression in red blood cell and/or hemoglobin
due to bone marrow depression.
leukopenia - a depressed level of white blood cells in the blood.
Ibuprofen, which is also sold under the brand names of Motrin or Rufen, can result in neutropenia, agranulocytosis, aplastic anemia, hemolytic anemia (sometimes Coombs positive), thrombocytopenia (with or without purpura), eosinophilia, and decreases in hemoglobin and hematocrit (measure of red blood cells in the blood) (1983 PDR, p. 2062).
Imipramine also sold as Janimine, SK-pramine, and
Tofranil can result in bone marrow depression, agranulocytosis, eosinophilia, purpura, and thrombocytopenia (1983 PDR, p. 973).
Indomethacin can result in leukopenia, aplastic anemia, bone marrow depression, hemolytic anemia, agranulocytosis, thrombocytopenia, and purpura (1983 PDR, p. 1308).
Chloramphenicol can result in aplastic anemia, thrombocytopenia, granulocytopenia, bone marrow depression, and pancytopenia.
Anabolic steroids such as testosterone sold as Depo-testerone, Vigorex, Delatestryl, Ditate-DS, and Testaval can result in a depressed level of white blood cells in the blood (1983 PDR, p. 1928).
Methyldopa or Aldochlor can result in a positive Coombs Test, hemolytic anemia, reduction of white blood cell count, granulocytopenia, and thrombocytopenia.
Valium can result in a depressed level of neutrophils in the blood.
Opren can result in a depressed level of thrombocytes in the blood.
Darvon (propoxaphene) can result in skin rashes.
Amoxicillin or Amoxil can result in anemia (depression in red blood cell and/or hemoglobin level), thrombocytopenic purpura (a depressed level of thrombocytes in the blood accompanied by purplish discoloration in the skin due to hemorrhaging), eosinophilia, leukopenia, and agranulocytosis (1983 PDR, p. 665).
Premarin can result in vaginal candidiasis (1983 PDR, p. 647).
Procardia (nifedipine) can result in dermatitis, pruritis, and urticaria (allergic or autoimmune reactions).
Yiamouyiannis insisted in keeping the above potential causes for AIDS in for the following reasons. Though recreational drug use and medical treatments like AZT may be able to account for over 90% of the AIDS cases, some recreational drug users don't get AIDS. The use of other drug and environmental exposures that depress the immune system may be serious contributory factors, along with nutrition, exercise, mental attitude, and sleeping habits, which could predispose high-risk persons to AIDS and may be sufficient in themselves to cause the remaining AIDS cases observed in the U.S.
The African epidemic, we propose, is the consequence of malnutrition, parasitic infections, and poor sanitation — diseases of poverty as they have always existed which are becoming more severe as a result of a rapidly growing population and a declining food supply.
The African epidemic has little in common with the European and American epidemic. The European and American epidemics are primarily the clinical manifestations of the epidemic in the use of illegal drugs, which started in America during the Vietnam War and spread into Europe very soon after.