CHAPTER 5
![]()
Patterns of Uncertain Diagnostic Significance
A number of waveforms and patterns have not been reported to occur in normal infants, do not fit the criteria of normality, and are not associated with well-defined abnormal clinical correlates. These patterns are of questionable or uncertain diagnostic significance.
FOCAL SHARP WAVES
Currently, little understanding exists of the significance of focal sharp waves in premature and term infants. Various definitions of “normal” spikes and sharp waves have been proposed. For example, sharp waves occurring two or three times in an hour-long recording may have no significance in the newborn. To be considered normal, sharp waves occurring more frequently than this must be truly random and without persistent focality (Monod et al., 1972) and may arise from any scalp location (Engel, 1975; Hagne, 1972; Schulte, 1970). However, no stringent criteria have been developed to separate, unambiguously, abnormal from normal sharp-wave activity in the newborn.
Sharp waves or sharp-and-slow-wave complexes are commonly recorded from the midtemporal region during sleep in apparently normal premature and term infants. The features our group uses to differentiate between normal and abnormal temporal sharp waves are as follows:
Amplitude and Duration
In general, as the amplitude and duration of sharp waves increase, so does the likelihood that they are abnormal. For example, in a premature or term infant, random midtemporal sharp waves having a voltage of less than 75 µV, a duration of less than 100 msec, and occurring only rarely during sleep, would be considered normal (Figure 5.1). Conversely, midtemporal sharp waves with a voltage exceeding 150 µV and a duration greater than 150 msec would be considered abnormal. Unfortunately, numerous temporal sharp waves fall in a “gray zone” by these criteria. The most controversial is that of amplitude, since some sharp waves of greater than 100 µV may be considered normal if they are normal by all other parameters. However, other features, discussed in this section, often aid the neurophysiologist in determining the probability of normality or abnormality.
Incidence and Persistence
Temporal sharp waves that are considered normal occur randomly. They usually occur bilaterally but asynchronously and may be symmetrical or asymmetrical (Figure 5.2). Generally, these sharp waves appear infrequently; thus, temporal sharp waves occurring in quick succession, in series or long runs, and occurring on only one side are likely to be considered abnormal (Figures 5.3–5.5).
Morphology and Complexity of Waveforms
Temporal sharp waves classified as normal are usually mono- or diphasic. The morphology of abnormal temporal sharp waves is more variable. Although they are sometimes mono- or diphasic, abnormal sharp waves more often are polyphasic and followed by a high voltage slow wave (Figures 5.6–5.9).
Polarity
The initial component of a normal temporal sharp wave is surface negative. Temporal sharp waves with an initial or prominent surface-positive component are abnormal (Figure 5.9).
Features Associated With Changes in Wake/Sleep States
In the premature infant, normal temporal sharp waves may occur in any state. In the term infant, however, normal temporal sharp waves are more common during transitional sleep. If temporal sharp waves appear in the waking record of term infants, they probably are abnormal, regardless of other characteristics (Figure 5.10).
Midtemporal sharp waves satisfying the above criteria of normality occur in some healthy-term newborns during sleep. These sharp waves disappear rapidly during the first month of life and are seen in less than 5% of healthy newborns after 6 weeks post-term. Even temporal sharp waves considered clearly abnormal often do not persist beyond this age.
FOCAL RHYTHMIC ACTIVITY
Midline Frontal Rhythmic Activity
Bursts of rhythmic 50 to 200 µV, 5 to 9 Hz activity may occur in the midline frontal regions of neurologically normal infants between 38 and 42 weeks conceptional age (CA) (Hayakawa et al., 1987). The waves may have a sharp appearance and may occur in brief bursts usually lasting less than 1.5 seconds. They may occur in transitional and nonrapid eye movement (NREM) sleep, but typically not in REM sleep. They have been reported to occur in 55% of neurologically normal term infants, only rarely occur in infants with abnormal outcomes (4% of abnormal infants), and are not present in infants with moderate to severely depressed background activity (Hayakawa et al., 1987).
Midline Central Rhythmic Activity
Rhythmic activity similar to the frontal midline activity described earlier may also be present in the midline central in an otherwise normal electroencephalography (EEG) (Hrachovy et al., 1990) (Figures 5.11–5.13). This activity may also accompany other EEG features that are considered abnormal, particularly central sharp waves, in infants who have experienced various central nervous system (CNS) insults.
Occipital Rhythmic Theta Activity
In the term infant’s EEG, an uncommon finding is the occurrence of brief runs of rhythmic 4 to 6 Hz, 50 to 100 µV activity in the occipital regions with a duration of less than 1 second. This activity appears in wakefulness or sleep and usually occurs asynchronously on the two sides (Figure 5.14). In some infants, this activity may be unilateral (Figure 5.15). Occipital rhythmic theta activity can occur as an isolated feature in an otherwise normal EEG, but usually it accompanies other abnormalities such as sharp waves or an abnormal background.
TRANSIENT UNILATERAL ATTENUATION OF BACKGROUND ACTIVITY DURING SLEEP
Transient unilateral attenuation of background EEG activity occurring during NREM sleep is an unusual finding reported to occur in about 3% to 4% of all newborns (Challamel et al., 1984; O’Brien et al., 1987) (Figures 5.16 and 5.17). The attenuation episodes usually last about 1 minute and begin and end abruptly. The background EEG activity is normal in many infants. In our experience, these episodes usually occur only once during a recording session and usually within minutes of the time the infant first enters NREM sleep.
The significance of this finding, which occurs in apparently normal as well as in abnormal infants, has not been determined. Such episodes of unilateral attenuation of background activity should not be confused with the more common finding of marked generalized and/or lateralized voltage attenuation seen in the EEGs of infants who have experienced a variety of CNS insults. The latter attenuation episodes are short in duration (2–15 sec), occur repeatedly during the recording session, and may be present in all wake/sleep states. The isolated transient unilateral attenuation episodes seen in NREM sleep, and the generalized and/or lateralized attenuation episodes associated with various CNS insults, must also be distinguished from the generalized attenuation of background EEG activity that is seen when transient arousal occurs from NREM sleep.
LIST OF FIGURES
Temporal Sharp Waves
Figure 5.1 Randomly occurring right temporal sharp wave.
Figure 5.2 Independent, symmetrical, bilateral temporal sharp waves.
Figure 5.3 Repetitive left temporal sharp waves.
Figure 5.4 Repetitive right temporal sharp waves.
Figure 5.5 Repetitive, independent, bilateral temporal sharp waves.
Figure 5.6 Sharp- and slow-wave morphology.
Figure 5.7 Complex morphology of left temporal sharp waves.
Figure 5.8 Complex and variable morphology in bilateral, independent temporal sharp waves.
Figure 5.9 Complex morphology and varying polarity of temporal sharp waves.
Focal Rhythmic Activity
Figure 5.11 Brief burst of rhythmic theta activity in the midline central region.
Figure 5.12 Sustained burst of rhythmic theta activity in the midline central region.
Figure 5.13 Rhythmic midline central theta bursts and midline central sharp waves.
Figure 5.14 Brief, rhythmic occipital theta activity on the left and right.
Figure 5.15 Brief, rhythmic occipital theta activity on the left.
Transient Unilateral Attenuation of Background Activity During Sleep
Figure 5.16 Transient unilateral attenuation of background activity during sleep.
Figure 5.17 Transient unilateral voltage attenuation.
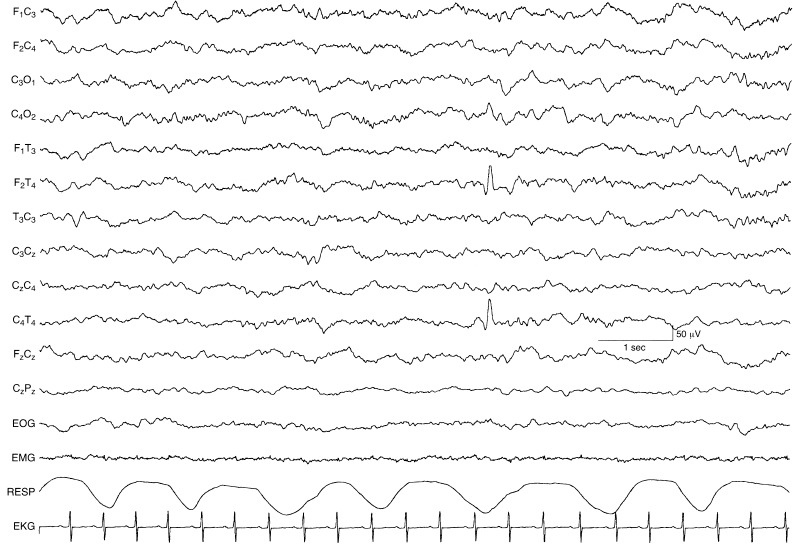
Figure 5.1 Randomly occurring right temporal sharp wave. An isolated diphasic sharp wave is present in the right temporal region with features that suggest it is a normal phenomenon. The background EEG of this sleeping 40-week CA infant is normal.
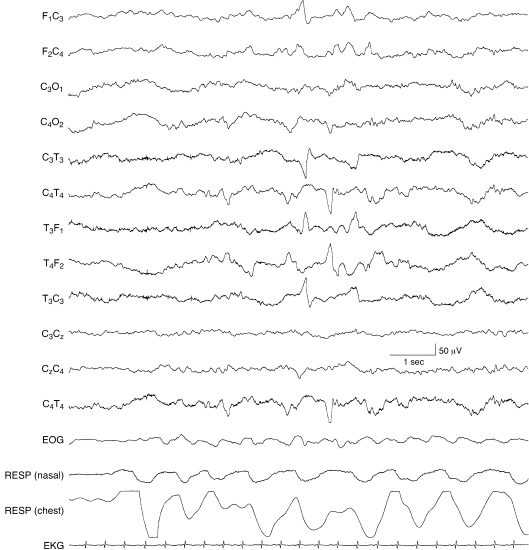
Figure 5.2 Independent, symmetrical, bilateral temporal sharp waves. Sharp waves are present in the left and right temporal regions appearing asynchronously, but symmetrically. The bilateral and asynchronous nature of the sharp waves is a normal finding. However, their amplitudes are near or greater than 150 µV and their durations are relatively long suggesting abnormality. The background activity is normal in this 40-week CA infant.
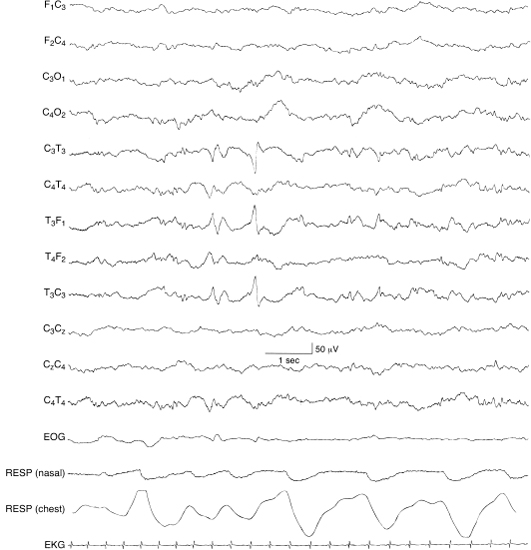
Figure 5.3 Repetitive left temporal sharp waves. Recurring sharp waves are present in the left temporal region in this 40-week CA infant with normal EEG background activity. Only two sharp waves are present in this sample. Thus, although repetitive, the degree of repetition is marginal, suggesting normality.
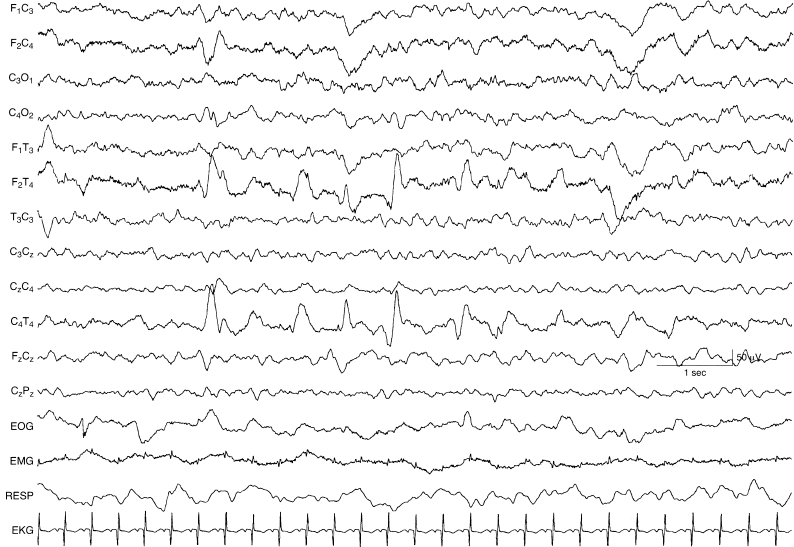
Figure 5.4 Repetitive right temporal sharp waves. The temporal sharp waves on the right are repetitive. They are also high in amplitude. These features suggest abnormality. The background EEG activity is normal in this 40-week CA infant (low frequency filter, 0.16 Hz).
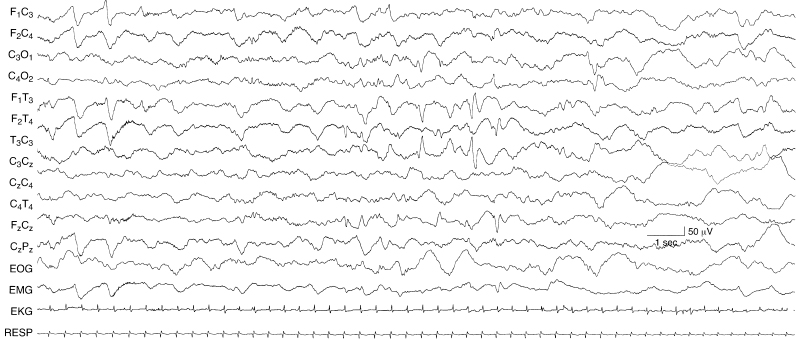
Figure 5.5 Repetitive, independent, bilateral temporal sharp waves. Runs of sharp waves are present in the left and right temporal regions, more prominently on the left where the sharp waves are more frequent and higher in amplitude than those on the right. Their repetitive occurrence and the high amplitude of some of the waves and their association with slow waves on the left suggest abnormality. Note the frontal sharp transients in the early portion of the sample; their occurrence is a normal phenomenon at this CA. This sleeping infant is 40-week CA and there is normal background EEG activity.

Figure 5.6 Sharp- and slow-wave morphology. A temporal sharp wave is present on the left that is normal in morphology and marginal in amplitude. However, the high-voltage slow wave that follows the sharp wave—creating a sharp- and slow-wave complex—suggests that this is an abnormal finding. This 42-week CA infant is in nonrapid eye movement (NREM) (quiet) sleep. The background activity is normal.
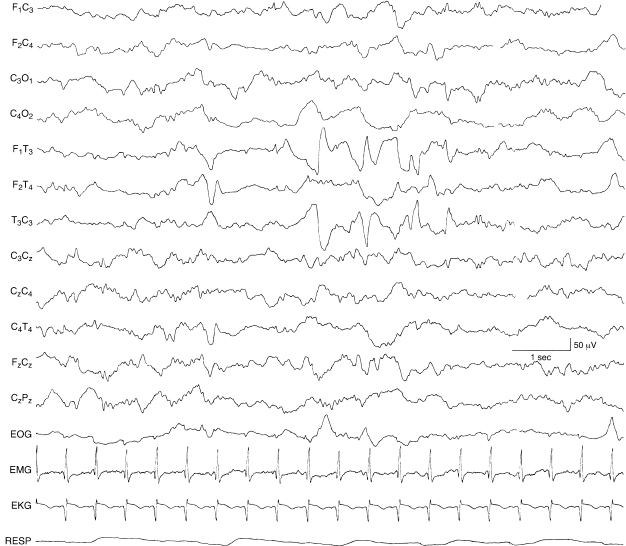
Figure 5.7 Complex morphology of left temporal sharp waves. The morphology of the sharp wave activity in the left temporal region is relatively complex, with slow and fast components and some waveforms that are sharper than others, suggesting abnormality. The background EEG activity is normal in this 38-week CA infant.
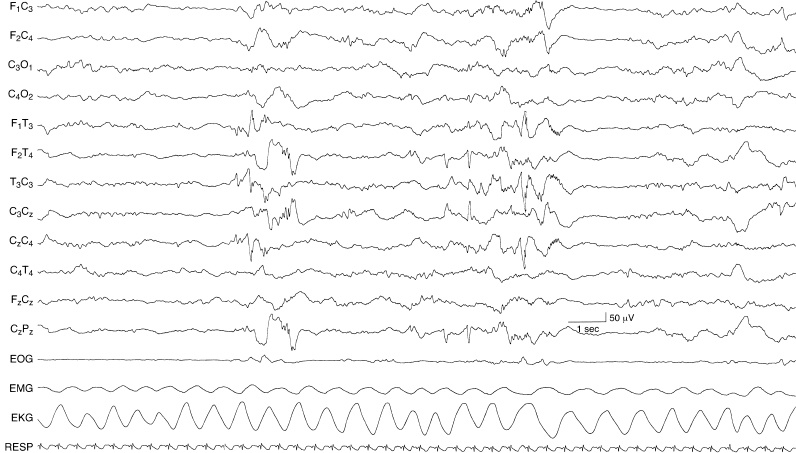
Figure 5.8 Complex and variable morphology in bilateral, independent temporal sharp waves. Repetitive temporal sharp waves appear independently in the left and right temporal regions with complex morphology, including spike-like waveforms. These features suggest that these temporal sharp waves are abnormal. The background EEG activity is abnormal with brief episodes of generalized voltage attenuation in this 40-week CA infant.
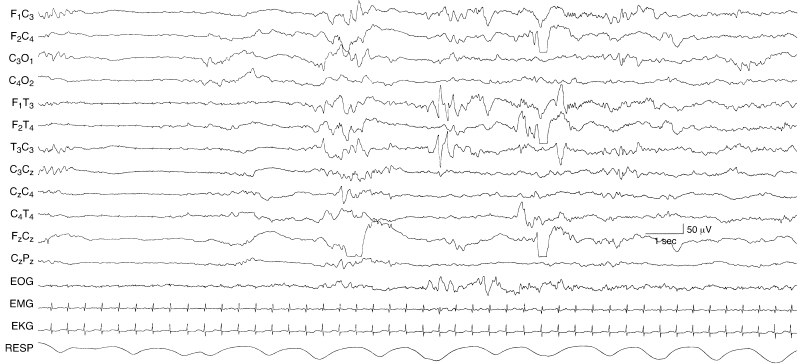
Figure 5.9 Complex morphology and varying polarity of temporal sharp waves. The sharp wave activity appears independently in the left and right temporal regions. There is variable and complex morphology in both regions with waveform components that are both surface negative and surface positive in polarity. The EEG background is abnormal with brief periods of generalized voltage attenuation in this 40-week CA infant.
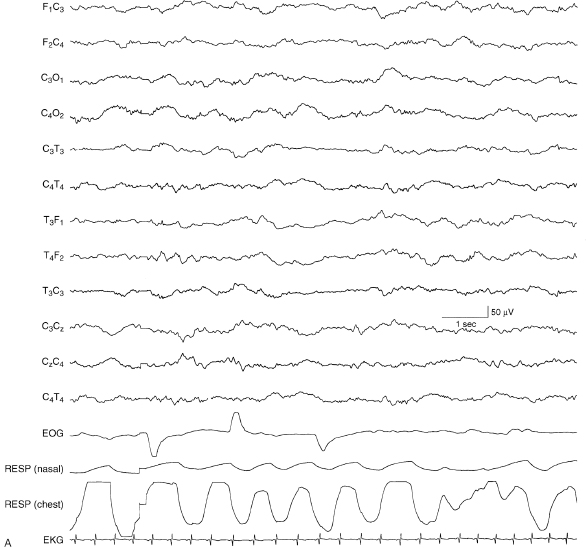
Figure 5.10 (A) and (B) Influence of wake/sleep state on the occurrence of temporal sharp waves: activation of sharp waves during sleep. (A) The awake recording in this 40-week CA infant is normal with continuous polyfrequency activity and no sharp waves.
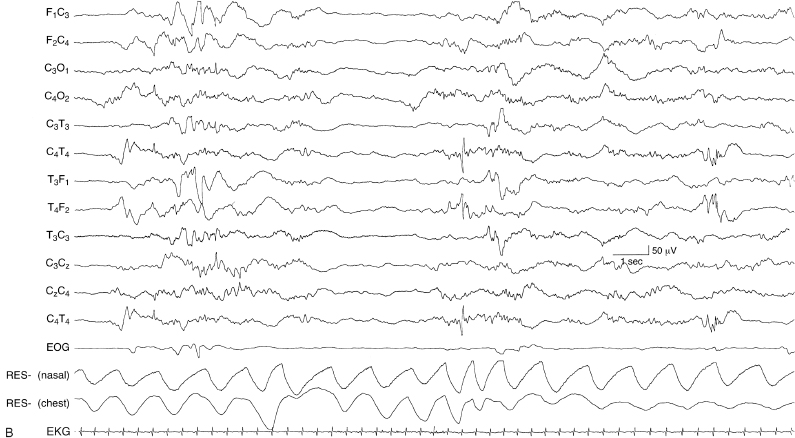
Figure 5.10 (B) In NREM (quiet) sleep there are independent, bilateral temporal sharp waves with variable and complex morphology. The background activity is characterized by abnormal periods of generalized voltage attenuation.
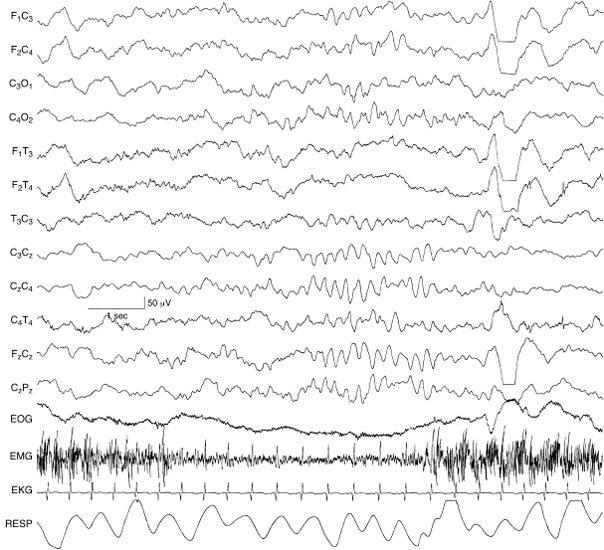
Figure 5.11 Brief burst of rhythmic theta activity in the midline central region. There is a brief burst of rhythmic theta activity in the midline central (Cz) region in this sample from a 40-week CA infant with normal background EEG activity.
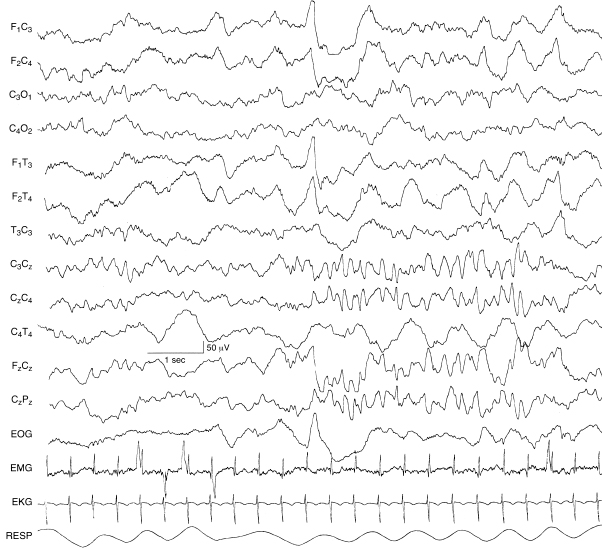
Figure 5.12 Sustained burst of rhythmic theta activity in the midline central region. There is a sustained burst of rhythmic theta activity in the midline central (Cz) region. Normal frontal sharp transients are present. The background EEG activity is normal in this 40-week CA infant.
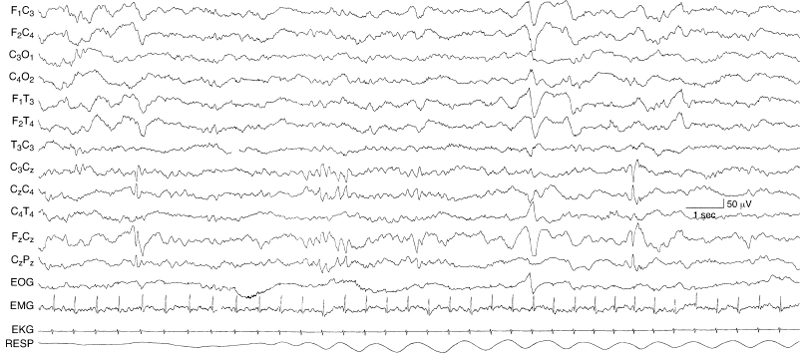
Figure 5.13 Rhythmic midline central theta bursts and midline central sharp waves. There is a brief run of rhythmic theta activity in the midline central region in the middle portion of this sample. Earlier and later there are sharp waves or spikes in the same region that are more abnormal features. Frontal sharp transients, normal waveforms, are present and the EEG background activity is normal in this 40-week CA infant.

Figure 5.14 (A) and (B) Brief, rhythmic occipital theta activity on the left and right. There are brief bursts of rhythmic theta activity in the left (A) and right (B) occipital regions on two samples from one EEG recording in this 34-week CA infant.
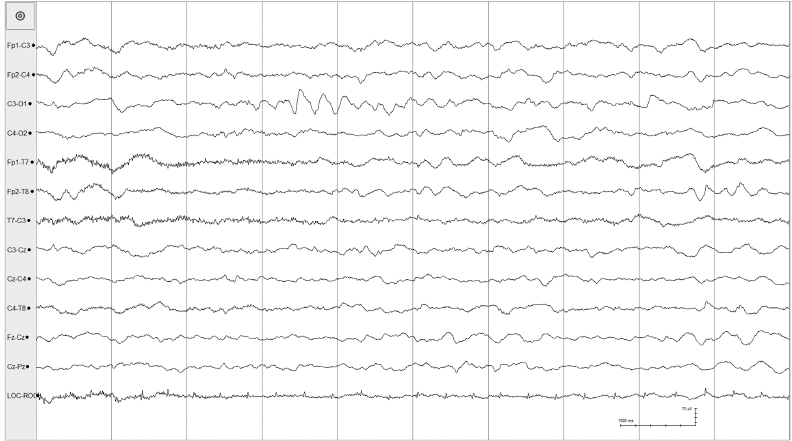
Figure 5.15 Brief, rhythmic occipital theta activity on the left. A brief burst of rhythmic theta activity is present in the left occipital region in the recording from this 40-week CA infant with a normal background EEG.
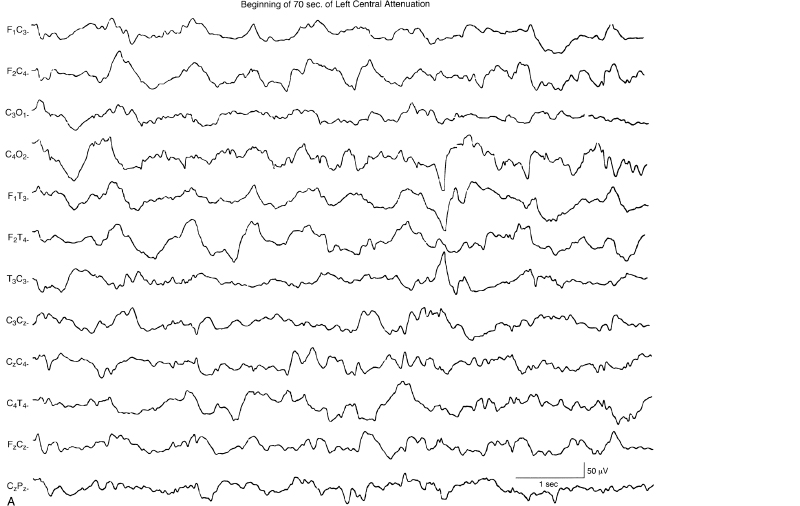
Figure 5.16 (A)–(D) Transient unilateral attenuation of background activity during sleep. Selected segments are shown of an episode of transient unilateral attenuation of background activity during sleep lasting 70 sec. (A) Initially, there is voltage attenuation of activity in leads from the left hemisphere.
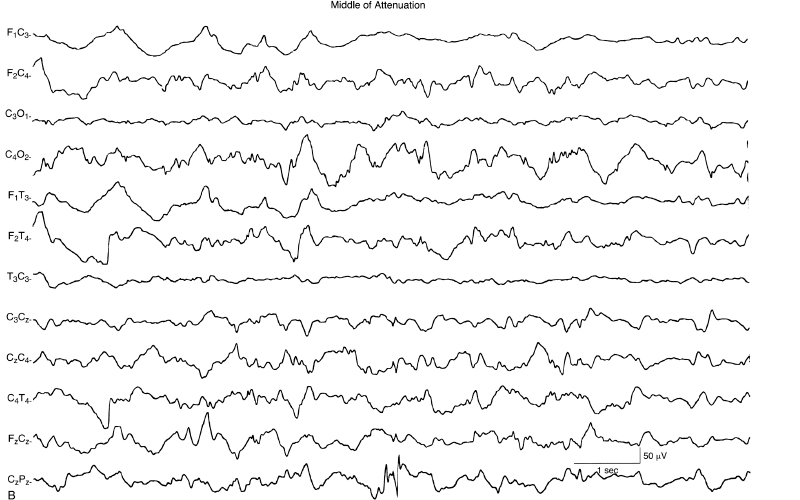
Figure 5.16 (B) The attenuation persists for several seconds.
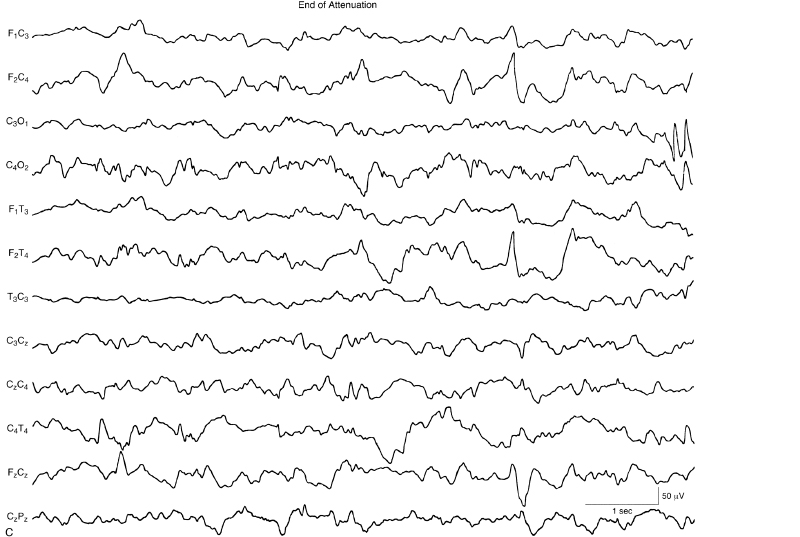
Figure 5.16 (C) There is gradual resolution of the attenuation.
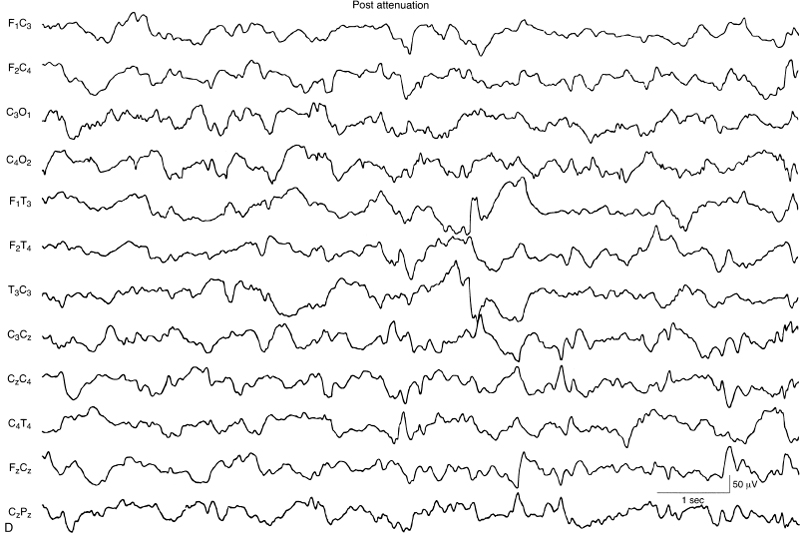
Figure 5.16 (D) The EEG eventually returns to baseline. The background EEG activity is normal in this 40-week CA infant.
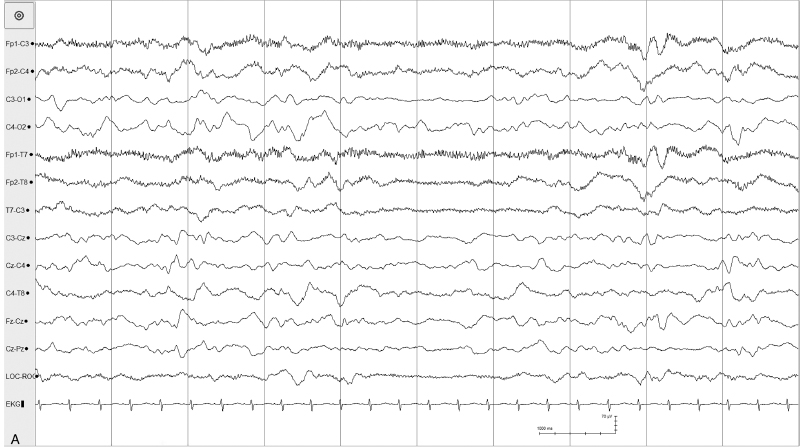
Figure 5.17 (A)–(E) Transient unilateral voltage attenuation. (A) Onset of voltage attenuation in the left posterior central region.
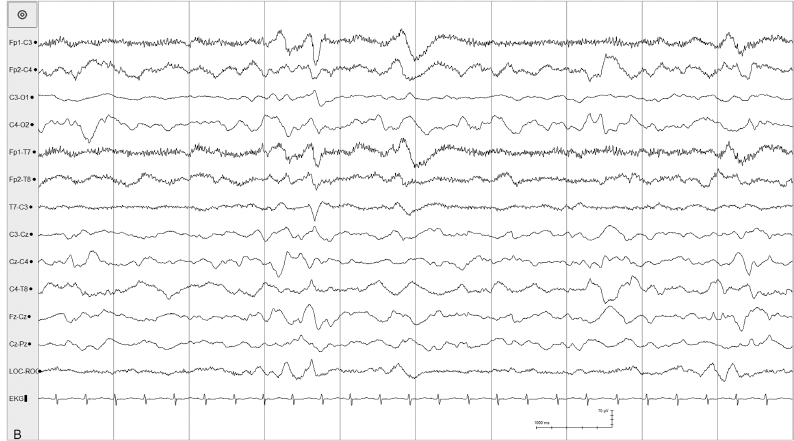
Figure 5.17 (B) The voltage attenuation is sustained.
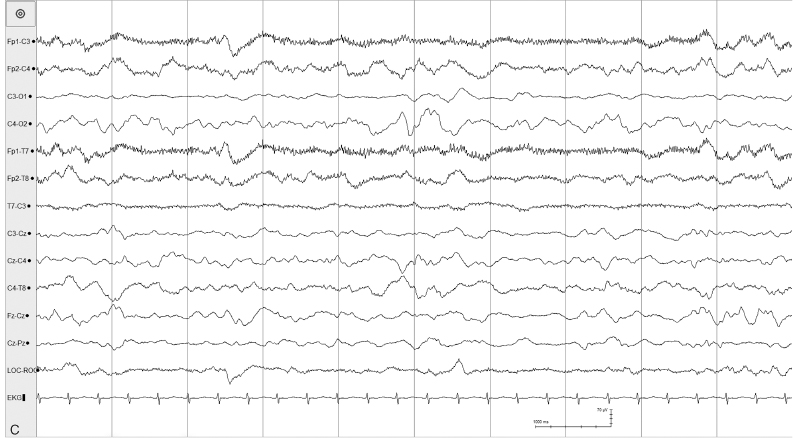
Figure 5.17 (C) The voltage attenuation persists.
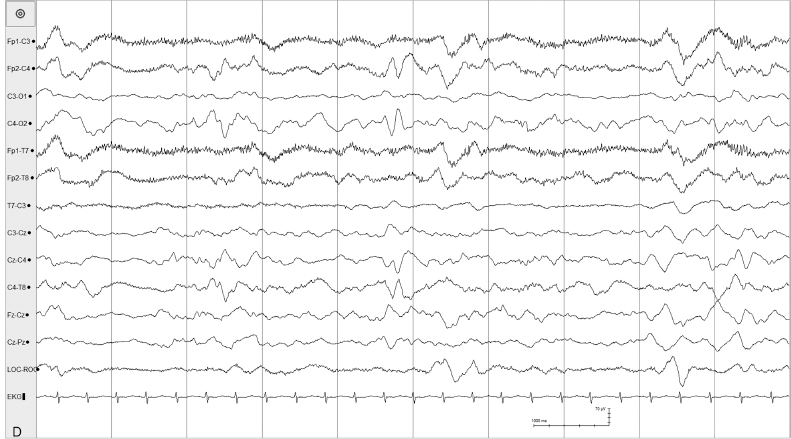
Figure 5.17 (D) The voltage attenuation persists.
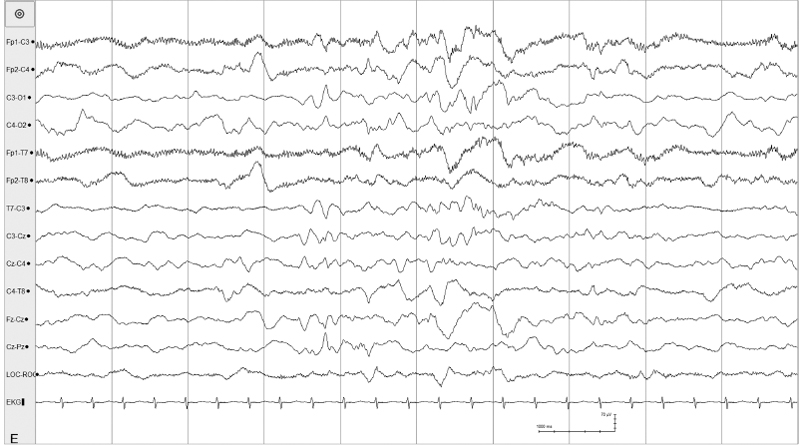
Figure 5.17 (E) The unilateral attenuation resolves spontaneously approximately 90 seconds after onset. This occurred in a 40-week CA, 10-day old infant with an otherwise normal background EEG.