Figure 3.1 (a & b) Schimmelbusch Mask, images showing the mask with/ without a piece of gauze, over which ether would be poured. (Reproduced by kind permission of the Association of Anaesthetists of Great Britain and Ireland)
In the year 2011 a modern anaesthetist would arrive at the equivalent of a casualty clearing station in a war zone armed with a medical degree, several years of clinical experience and probably a Fellowship in Anaesthesia (a postgraduate medical qualification) from the Royal College of Anaesthetists. He or she would have colleagues of similar status and the assistance of specially qualified technicians and nurses. The equipment would be up to date and include not only devices to measure blood pressure and monitor heart beat but also “invasive monitoring” that is plastic tubes inserted into arteries and veins that give a precise and instantaneous indication of the condition of the patient. There would be an array of anaesthetic agents including vapours that are inhaled as well as drugs that are injected along with a pharmacy containing drugs to manipulate and maintain the blood pressure. Vast quantities of fluids would be available to be given intravenously and there would be access to blood transfusion facilities.
There would be support teams that travel into the battle zone by helicopter to initiate resuscitation of the wounded, returning them speedily in good condition to the operating theatre for definitive surgery. Ventilators (machines that breathe for the patient) would be available both in the operating theatre and in the intensive care unit where the most seriously wounded patients would be looked after.
When Major Charles Corfield arrived at a casualty clearing station on the Somme in 1916 as a specially designated anaesthetist, the equipment and agents he found would have been recognizable to a doctor in the mid-19th Century.1 He had at his disposal what he called the usual anaesthetic equipment – chloroform, ether, ethyl chloride and Schimmelbusch masks, which were simple devices made of wire that could hold gauze or lint onto which the anaesthetic agent could be dripped, the inhalation of which resulted in anaesthesia. He asked for another inhalational agent to be made available, the gas nitrous oxide, and was fortunate enough to be able to get some along with the appropriate apparatus.
Despite the passage of some 60 to 70 years between the discovery of anaesthesia and its use during the Great War, very little had changed. A demonstration of anaesthesia using ether took place in 1846 at the Massachusetts General Hospital just twelve months after Horace Wells had failed to produce a state of anaesthesia by using nitrous oxide at the same hospital.2 The age of pain-free surgery had arrived and news quickly spread across the Atlantic to Great Britain and Europe. Keen to find other agents with the same effect James Young Simpson and friends in Edinburgh were experimenting after dinner one evening when they discovered that breathing chloroform rendered them unconscious for a number of minutes. Chloroform acted more quickly than ether, but gradually reports of deaths from chloroform inhalation appeared. Fearing legal action in the event of death, Americans continued to use ether, but chloroform with rapid onset of anaesthesia, became popular in Great Britain. It was not until the early part of the 20th Century that scientific experimentation on animals revealed that the normal beating of the heart could decline into a quivering of the heart muscle known as ventricular fibrillation under the effects of chloroform.
Figure 3.1 (a & b) Schimmelbusch Mask, images showing the mask with/ without a piece of gauze, over which ether would be poured. (Reproduced by kind permission of the Association of Anaesthetists of Great Britain and Ireland)

These very early days of anaesthesia were dogged with arguments about exactly where the first anaesthetics had been given and who had given them, such was the desire to claim responsibility for the discovery. There were occasions when there was failure to produce a state under which surgery could be carried out (surgical anaesthesia) and there were complaints from some members of the medical profession that anaesthesia would be “bad” for patients. They regarded the pain of surgery as a “necessary evil” that kept the patient alive. However, such a welcome relief from suffering could not be suppressed and anaesthesia became an essential part of surgical practice.
However, when Britain went to war in the Crimea the old arguments surfaced once again. Despite the successful use of ether during the Mexican-American war in 1847 the Principal Medical Officer of the British Army, Sir John Hall, cautioned against its use in a memorandum published in the Illustrated London News in 1854:
However barbarous it might appear the smart of the knife is a powerful stimulant and it is much better to hear a man bawl lustily than to see him sink silently into the grave.3
Fortunately his advice was largely ignored and chloroform was given for most operations. Perhaps doctors had been influenced by John Snow, who in 1847 advocated the use of anaesthesia for battle casualties:
The pain endured by the bleeding soldier or sailor wounded in fighting battles of his country is deeply deplored by every feeling mind and a discovery which can prevent so much of it as depends on the operations necessary to save his life, must be hailed as a great blessing.. .4
Snow was a physician of great ability. Famed for his discovery of the spread of cholera through water he dedicated much of his life to the science of anaesthesia. He realized long before many others that good anaesthesia required close observation of the patient, a means of quantifying the dose given and a good bedside manner. Having invented a machine for delivering ether in known amounts which was later modified by another well known 19th Century anaesthetist, Joseph Thomas Clover, to give chloroform, he might well have been surprised to see ether being given from a drop bottle onto a piece of gauze held by a metal mask over the patient’s face in the early days of the Great War.
Further experience was gained in military anaesthesia during the American Civil War and by the time the Boer War started in 1899, the British Army medical services were issued with 10 pounds of chloroform and 5 pounds of ether at every base hospital and doctors on horseback were given a bottle of chloroform in their saddlebag!5
Ethyl chloride gained favour much later on than the other two agents. Its anaesthetic properties were first noticed in 1847 but it wasn’t until 1895 that it came into general use when improvements in manufacture decreased impurities. Like chloroform it induces anaesthesia quickly but there was disagreement among physicians as to whether it was safer than other agents.
Various combinations of those four agents ether, chloroform, nitrous oxide and ethyl chloride had been advocated in order to make induction and maintenance of anaesthesia a safe and pleasant experience and they formed the backbone of inhalational anesthesia well beyond the end of the Great War. Induction of anaesthesia refers to the period between consciousness and the state of surgical anaesthesia which is defined as the state when it is possible to carry out surgery without the patient experiencing pain. Today, injections of drugs directly into a vein produce unconsciousness quickly and pleasantly but the inhalation of gases and vapours takes longer. In particular the use of ether on its own produces first a state of excitement during which the patient struggles before breathing becomes regular and surgical anaesthesia ensues. It takes considerable skill to produce a smooth induction, hence the desire to add other agents which speed up the process and make it more pleasant.
There was however, a form of anaesthesia available to surgeons which did not require the patient to be unconscious, that of local anaesthesia. Coca leaves were used in South America for their pain relieving (analgesic) properties and the active substance cocaine was isolated in 1859. Karl Koller, a German eye surgeon, was the first person to try out cocaine for its anaesthetic properties and in 1884 he used a direct application of it to carry out eye surgery. Hollow needles with syringes had been available since the 1850s and in 1892 Carl Ludwig Schleich infiltrated cocaine under the skin to “freeze” an area that could then be operated upon. Cocaine itself was poisonous but over the course of the next twenty years other local anaesthetic drugs were manufactured which could be used either under the skin or directly applied to a nerve to produce anaesthesia in the area supplied by that nerve. In 1891 the German physician Heinrich Quinke described the technique of lumbar puncture when a needle is inserted into the fluid which surrounds the spinal cord (cerebrospinal fluid).
Seven years later in 1898 one of his former students, August Bier, described the injection of small amounts of cocaine into the cerebrospinal fluid of six patients to produce abolition of sensation sufficient to allow surgery.6 The ability of small amounts of local anaesthetic injected around the spinal cord to render large areas of the body insensitive to pain had been proven, and spinal anaesthesia was born. In order to reach a well-informed opinion, Bier decided that he should personally experience the technique and asked a colleague, Dr Hildebrandt, to carry out a spinal anaesthetic on himself. Inability to get a good fit between the syringe and needle resulted in a loss of local anaesthetic and the procedure was not successful. Hildebrandt then offered himself as a subject and the experiment successfully resulted in surgical anaesthesia, although both physicians suffered from terrible headaches.
Cocaine, however, failed to produce reliable results and the technique was abandoned until stovaine, another local anaesthetic, was discovered a few years later. It was so called because it was synthesized by Furneau, which is the French word for stove, and rapidly gained a place in the operating theatre. Several papers in the medical literature showed spinal anaesthesia to be a safe and reliable technique and Major Houghton of the RAMC (one of the first British Army anaesthetists) recorded its successful use on peace time army recruits in a series of papers carefully recording dosage, effect and side effects in all patients.7 Usually, however, spinal anaesthesia fell under the jurisdiction of the surgeon and a separate anaesthetist was not involved. Many believed it to protect patients from the shock of surgery but in severely wounded battle casualties this was often not the case.
It should be noted that August Bier was not only famous for the introduction of spinal anaesthesia but was also responsible for introducing the distinctive steel helmet worn by German soldiers. Presumably after witnessing the disastrous effects of penetrating head wounds from shrapnel he realized that adequate protection was required.
But what of the training and experience of medical personnel whose duty included the giving of anaesthetics? Major Corfield, who was both a doctor and a barrister, had prior experience of the subject, having been employed as an anaesthetist at the Gordon Throat and Temperance Hospital, London and the Bristol General Hospital. At the outbreak of the war, such experience was the exception rather than the rule.
The idea that training in anaesthesia should be systematic and included in every medical student’s curriculum was advocated in 1892 by Frederick Silk, assistant anaesthetist to Guy’s Medical School.8 Writing in The Lancet he argued that improvements in surgery required improvements in anaesthesia that would only be brought about by properly trained doctors devoting time and energy to the subject. Not only was equipment becoming more complicated but doctors were beginning to realise the importance of understanding the physiological effects of anaesthesia and surgery on the human body. In addition, Silk felt that the medical profession should do all in its powers to make it as safe a process as possible. The fact that having an anaesthetic was safer than a railway journey was not an excuse for the occasional death. Over the course of the next twenty years, specialist anaesthetists were appointed to many hospitals but even in 1901 Dudley Wilmot Buxton, anaesthetist at University College Hospital London, was still trying to get the teaching of anaesthesia included in the curriculum of every medical school.9 A bill proposing that all general anaesthetics be given by medical personnel was put before Parliament in 1909 but it failed. Only in 1912 did the General Medical Council include anaesthetics as the last of 16 subjects to be included in the undergraduate curriculum of all medical schools.10
It is therefore understandable that most of the young men assigned the position of anaesthetist during the Great War had scant training and experience in the subject. They struggled to cope with the demand of two surgeons working between four or even six operating tables. During the Battle of The Somme, the Reverend Leonard Pearson found himself giving anaesthetics at Casualty Clearing Station No 44. Photographs and a scrap album of his were found in a rubbish skip and deposited at the Bodleian Library, Oxford. In Lyn Macdonald’s book The Roses of No Man’s Land he recounts his experience:
I spent most of my time giving anaesthetics. I had no right to be doing this of course but we were so rushed If they had had to wait their turn in the normal way, until the surgeon was able to perform the operation with another doctor giving the anaesthetic, it would have been too … late for many of them. As it happened, many died.11
It is small wonder then that an approach was made to Geoffrey Marshall, a doctor serving on a hospital barge that was used to transport casualties who were too sick to go by train or road. Marshall described his time on the barge as most enchanting but the use of barges was sporadic and there were times of inactivity interspersed with a few days of desperate activity. In an interview in 1966 Marshall is quoted as saying:
A dreadful old man, who was the senior consultant, Sir Anthony Bowlby [see Chapter 2], drove up to my barge one day – lovely day – and said “Marshall we are having an awful lot of deaths in the forward hospitals from shock and you did a lot of work on the physiology of anaesthesia before the war so I want you to come along and see if you can do anything about these chaps.12
“A dreadful old man” he might have been but Sir Anthony Bowlby had gained experience in the Boer War as well as the Great War and he knew exactly who to ask to sort out the problems of the large number of anaesthetic-related deaths. Marshall was a physician and respiratory physiologist who had worked at Guy’s Hospital as a demonstrator in physiology, a recognized training ground for young physicians, and Bowlby remembered him from his pre-war days. The last thing Marshall wanted to be remembered as was an anaesthetist. However, in a carefully controlled study carried out at Casualty Clearing Station No 17 at Remy Siding near Ypres, he cemented the anaesthetist’s role as peri-operative physician able to understand the physiology of shock and how the method of anaesthesia could be tailored to the condition of the patient with a resulting decrease in mortality.13
Patients arriving at casualty clearing stations often required immediate life-saving surgery but were suffering from the effects of shock and haemorrhage (blood loss).
When blood loss occurs, physiological changes take place which are designed to preserve the flow of blood to the most vital organs of the body and keep the person alive. First of all, small blood vessels in the skin constrict and then the blood flow to the kidneys is reduced. The heart rate increases and initially blood pressure is maintained. As the blood loss becomes more pronounced blood pressure falls and finally the patient becomes semi-conscious as the body fails to maintain flow to the most vital organ of all, the brain. Patients with blood loss are pale with a weak and rapid pulse. Many of the wounded had lain on the battlefield for some time and they were wet and cold, and in winter many suffered from bronchitis as well. Australian and Indian soldiers were particularly susceptible to the effects of the European winter. Hence Marshall said at the start of his paper:
A correct choice of anaesthetic is of the first importance: the patient’s life will be as much imperiled by faulty judgment on the part of the anaesthetist as by a wrong decision on the part of the surgeon.
The methods of anaesthesia available to Marshall were:
1. Nitrous oxide and oxygen.
Nitrous oxide differs from ether and chloroform in being a gas not a vapour and as such comes in pressurized metal cylinders. Metal was in short supply during the war as it was required for munitions and gaining a supply of nitrous oxide was difficult.
2. Ether and chloroform by the open method (i.e. a dripped onto a mask)
3. Ether and chloroform by Shipway’s warm vapour apparatus.14 The use of the open method allowed considerable loss of vapour into the operating theatre and loss of body heat from the patient. The evaporation of ether could result in the temperature of the inhaled vapour being 30-40° below that of the room. Shipway’s apparatus allowed the patient to breathe warm vapour at a known concentration which was less irritant to the lungs and this decreased the incidence of post-operative bronchitis. Along with the addition of chloroform, it also improved the smoothness of induction.
4. Intravenous ether. Producing anaesthesia by injecting ether and also by instilling it per rectum (into the bowel) enjoyed a brief period of acceptance in the first twenty years of the 20th Century but it never really caught on, nor was it used to a large extent during the Great War.
5. Spinal anaesthesia with stovaine.
6. Local infiltration with novocaine. This was one of the local anaesthetics synthesised in 1905. It is known today as procaine and is still in use.
The commonest wounds were minor and required a quick anaesthetic with a rapid recovery so that the patient was fit for early evacuation by ambulance train. These patients were given nitrous oxide and oxygen and it suited short operations very well. Anyone who has inhaled entonox (50:50 nitrous oxide and oxygen) as carried by ambulances or on maternity wards will know that although it provides very good pain relief it rarely results in unconsciousness sufficient to allow surgery to proceed. It is no surprise that back in 1845 Horace Wells failed to demonstrate its use for anaesthetic purposes. The only way in which a state suitable for surgery can be produced is either by having a patient who already has a reduced level of consciousness due to blood loss or morphine administration or by giving 100% nitrous oxide. In the latter instance the patient is given nitrous oxide without oxygen and when asleep, sufficient air is allowed into the system so that the patient gets enough oxygen to prevent death from asphyxiation. Corfield described it as a compromise between consciousness and colour (a patient without sufficient oxygen would change from pink to blue), something which would be considered unethical today. When patients were already partly deadened to pain as a result of haemorrhage it would prove invaluable for a quick and definitive procedure such as a guillotine amputation. Marshall found that in patients close to death, a ‘quick whiff’ of nitrous oxide and oxygen would allow an arm or a leg to be amputated and blood vessels to be tied off to prevent further haemorrhage. Other anaesthetics would have killed the patient.
The disadvantage of nitrous oxide and oxygen alone was that while it produced analgesia for short procedures, it was of no use for prolonged operations requiring deeper levels of anaesthesia. These required ether and chloroform.
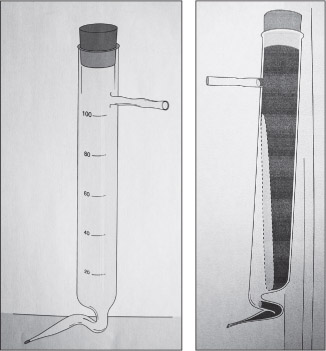
Figure 3.2 (a & b) Shipway’s Warm Ether Apparatus. The purpose of these bottles is to warm the ether before it is administered to the patient, who otherwise may become very cold. Shipway’s apparatus was of particular use in longer operations to help prevent the core temperature of the patient dropping. (Reproduced by kind permission of the Association of Anaesthetists of Great Britain and Ireland)

Giving chloroform at the start of the induction and then proceeding with ether speeded up the time before the patient was ready for the surgeon’s knife. Dripping these agents onto an open mask led to high levels of the vapours in the operating theatre and it must have been a very heavy and soporific atmosphere to work in. The advantages of Shipway’s apparatus were such that one was issued to each hospital unit. Marshall felt it a huge improvement but Corfield was less impressed as he found it cumbersome and very tiring as there were hand bellows that required pumping.
By the early 20th Century it was realized that the shock of surgery could be very harmful following on from the shock of being wounded. No longer did doctors believe that the stimulating experience of pain could be in any way beneficial. Spinal anaesthesia was thought to minimize the shock of operation and therefore ought to be used for wounds below the level of the umbilicus. Marshall found that if he used it at base hospitals when wounds were a few days old it proved a satisfactory method. It could also be used at casualty clearing stations if the wounds were not less than forty hours old.
However, when the wounds were more recent, spinal anaesthesia could be followed by profound drops in blood pressure. The radial pulse at the wrist might disappear completely and fatalities could result. He observed that it was loss of blood that made spinal anaesthesia particularly dangerous. He tried decreasing the dose of local anaesthetic but this just resulted in incomplete anaesthesia. He set about finding out which patients could be given spinal anaesthesia safely and which could not. He felt that neither the appearance of the patient nor the pulse and blood pressure were helpful in making this decision.
What was of use was the haemoglobin concentration in the blood. Blood consists of many different types of cells and haemoglobin, which gives the red cells their colour, is responsible for carrying oxygen around the body. When a patient bleeds and red cells are lost the haemoglobin falls. If the haemoglobin concentration was low in a recently wounded patient then this meant that they had lost a lot of blood and would collapse if given spinal anaesthesia. The normal range for haemoglobin is 97 to 120% and Marshall found that a safe level was above 100%.
The following chart looks at the pulse and blood pressure in a soldier with a shell splinter wound of the leg, who underwent surgery twenty-one hours after being wounded. The haemoglobin was 85% and the blood pressure fell to 81mms Hg. The patient died of gas gangrene 24 hours after the operation.
This collapse in blood pressure was not understood by Marshall. With the benefit of current knowledge, when a local anaesthetic is injected into the fluid around the spine it blocks not only the sensory nerves that carry the sensations of touch and pain to the brain and the motor fibres which allow the brain to send impulses to move the limb but also the fibres of the sympathetic nervous system. These sympathetic nerves innervate the small blood vessels in the body to alter their caliber in response to changes in blood volume and the outside temperature. When a person is shocked due to blood loss these small vessels constrict to direct blood to the brain and other essential organs in an attempt to preserve their function. Vaso-constriction caused by cold aggravates the problem. If that patient were to have a spinal anaesthetic so that the action of the nerves on the blood vessels is blocked, the effect is like pulling a rug from under someone’s feet. This element of the compensatory mechanism that has been maintaining the blood pressure is withdrawn and the effect is dramatic. The peripheral blood vessels dilate uncontrollably. No amount of increase in the pulse rate will counteract the problem, and the blood pressure crashes. It is perhaps a testament to the fitness of youth that some men did survive this experience.
Figure 3.3 The administration of anaesthetics at the Front. (With permission from the British Medical Journal Publishing Group)
Having solved the problem of to whom not to give spinal anaesthesia Marshall turned his attention to the casualty with severe shock, the patient with a pale face and a very weak pulse. How was such a patient to be managed? He noted that these patients had a very cold skin and could be improved with hot water bottles (see Chapter 2). The blood pressure was taken regularly and if it was improving operation could be delayed for a short time, although too long a delay might result in gas gangrene setting in.
He warned that chloroform would result in death on the table and ether either by inhalation or intravenously would improve the patient initially and then result in profound collapse two hours later. Chloroform tended to depress the pumping of the heart resulting in death during surgery whereas ether stimulated it, resulting in an initial improvement which declined later. The only suitable anaesthetic in profoundly shocked patients was nitrous oxide and oxygen and although so light that there was occasional movement, there was no evidence of deterioration.
Shock due to haemorrhage occurred early on but septic shock took longer to develop. It might be due to infection of dead and damaged tissues that had been inadequately excised or to wounds of the abdomen which had resulted in bowel contents being spread into the peritoneum or bacteria being introduced with the offending weapon. Here the blood pressure is low but the pulse often full and bounding. We now know that toxins produced by bacteria act on the blood vessels to dilate them and on the heart to decrease the power of its pumping action. Although the pulse might not seem too fast and the blood pressure appear to be adequate, insufficient oxygen finds its way to the tissues and starting with the kidneys all the organs of the body fail. Marshall felt these patients were much more favorable subjects for spinal anaesthesia. Injection of stovaine around the spinal cord did not result in the same collapse as in haemorrhagic shock since the blood vessels were already dilated. The dramatic effect seen in the casualty with shock secondary to acute major blood loss did not happen. Ether could also be given without post-operative collapse, intravenous ether seemed to improve the patient’s condition and nitrous oxide and oxygen could be used as well. Only chloroform was to be avoided as it had a direct depressant action on the heart.
Anaesthesia for severe limb wounds
Most of these patients were suffering from shock as a result of blood loss. They were cold and clammy, with pale faces and barely perceptible pulses. Marshall felt that many of their lives could be saved if correct procedures were followed. Morphine should be withheld as this would further depress the blood pressure. The only acceptable anaesthetic was nitrous oxide and oxygen, allowing the shattered limb to be quickly amputated. Anaesthesia might be so light that the patient would move when nerves were divided but the patient would be conscious five minutes after operation and able to “sit up and take nourishment”.
Anaesthesia for penetrating head wounds
Marshall’s opinion for head wounds was that local anaesthesia was far better than chloroform. Any general anaesthesia in a patient whose conscious level was impaired would have resulted in a depression of the patient’s respirations and a rise in the carbon dioxide levels in the blood. This in turn would lead to the blood vessels of the brain dilating and the brain swelling, a condition referred to as cerebral oedema (See Chapter 9 for explanation of this). Without more modern agents and the ability to control the patient’s ventilation any general anaesthetic would have been very dangerous. However if the casualty was completely awake, Marshall felt that if the patient found cutting through the skull too upsetting, then warm ether could be recommended. As a mask would have got in the way of the surgeon he devised a way of passing a catheter down one of the patient’s nostrils through which the anaesthetic vapour was passed.
Anaesthesia for Abdominal Wounds
Warm ether was of particular value, as temperature loss was a real problem when large amounts of the patient’s intestines were exposed to the air. When the abdomen is opened, heat loss from exposed bowel is considerable and anything which counteracts a fall in body temperature is beneficial. Marshall found that when several feet of intestine were laid outside the abdominal cavity, the blood pressure fell. He suggested that surgeons should make large incisions and work within the abdomen. As casualties seemed to be able arrive at casualty clearing stations with several feet of intestine outside the abdominal cavity without any drop in blood pressure he attributed the deterioration in condition to heat loss from exposed blood vessels of the gut. If the casualty wasn’t anaesthetized then the loss of heat was much less.
Ether itself would cause the blood pressure to rise but excessive manipulation of the bowel or pulling on the peritoneum which lines that abdominal cavity would result in a fall. The bowel and peritoneum are supplied by nerves from the sympathetic nervous system and stimulation of these nerves by pulling results in a slowing of the heart rate and fall in blood pressure. In other words the stimulation of the sympathetic nervous system by ether is counteracted by manipulation of the bowel. Bronchitis could be common after abdominal surgery as breathing and coughing are impaired due to the pain of the wound. Marshall found that he could decrease the incidence from 54% to 14.7% by using warm ether instead of open ether.
Operations on abdominal wounds could take a long time and it was important that surgeons proceeded quickly on a decisive course of action. Casualties might have holes in many parts of the intestine and these all had to be dealt with so that soiling of the peritoneal cavity was kept to a minimum. Just as it was important to excise dead tissue in a limb to prevent infection getting a hold so it was important to keep the peritoneal cavity free from intestinal contents. Once infection had set in it was difficult to combat. Even now septic shock from ruptured abdominal viscera may prove difficult to treat although support may be provided on an intensive care unit for every failing organ. When the operations took some time Marshall found that it was inadvisable to turn patients on their side to enable the surgeon to deal with a wound on the back.
The blood pressure in this situation fell markedly and it could be hours before the patient improved. Perhaps this was due to the patient being severely short of fluid. He stated that it was usual to give three pints of normal saline subcutaneously through a needle placed just under the skin during the operation but if the patient was shocked it would not be well absorbed as he showed in post-mortem studies. Three pints would be insufficient to replace the fluid that had evaporated from the surface of the intestines especially when combined with blood loss.
Figure 3.4 Marshall Gas/Oxygen/Ether Apparatus. Curved tubes deliver nitrous oxide and oxygen directly into the bubble bottle on the left. The bubbles of gas can easily be observed and the relative percentage of oxygen estimated. The gases then pass to the ether bottle on the right via a simple on/off valve. (Reproduced by kind permission of the Association of Anaesthetists of Great Britain and Ireland)
Anaesthesia for chest wounds
One operation in which chloroform proved superior to ether was when there was a penetrating chest wound. Ether in this situation provoked haemorrhage, perhaps because it had a tendency to raise the blood pressure.
As a result of Marshall’s work, the place of nitrous oxide and oxygen became firmly established as a safe choice in difficult circumstances. Used in conjunction with ether for longer procedures an anaesthetic machine to regulate administration was required. Marshall designed such a machine. When home on leave he took his design to Coxeters, a manufacturer of anaesthetic equipment, who produced a machine for him which became the standard RAMC machine later on in the war. Marshall was encouraged to publish his work because “someone had borrowed their blocks”.15
The “someone” in question was Captain Henry Boyle, who had by chance met an American doctor called James Tayloe Gwathmey in 1912 at the Seventeenth International Congress of Medicine in London. Before the war, in 1912, Gwathmey had developed an apparatus for giving nitrous oxide and oxygen which incorporated a device which could measure the flow of gases so that at a glance the relative proportions could be observed.16
Boyle acquired a Gwathmey machine when working in London. He adapted this, introducing reducing valves and used it on war casualties in London. Both Gwathmey and Marshall added bottles for ether or chloroform through which the gases were bubbled. These agents were introduced to enable Marshall to employ longer anaesthetics.
During the war chloroform was shown to lower the blood pressure whereas ether did not and if a small amount of ether was added to the nitrous oxide/oxygen mixture then the anaesthetic was still safe but could be used for more extensive surgery.17
However, it was Boyle who further developed the nitrous/oxide/ether machine and published his work on the new invention in February 1919. It was called a Boyle’s Machine for many decades, the decline in the use of the term being a relatively recent phenomenon. Marshall did not really mind, because he had no wish to be remembered as an anaesthetist anyway.
Gwathmey went on to devise a method for giving nitrous oxide and ether to patients without the lungs collapsing during thoracic surgery. He delivered it through a mask which had an attachment containing an exit valve which had to be forced open before expired gases could escape. Thus the patient was breathing out against resistance and a continuous positive pressure was applied which kept the lungs expanded and allowed a lower percentage of oxygen to be given.18
Gwathmey also devised a simple method for giving analgesia to soldiers who required frequent wound dressings without removing them from their beds. He tried out a variety of mixtures deciding that a combination of paraldehyde, liquid paraffin and ether gave the best results. The smell and taste of paraldehyde was poorly tolerated but this was overcome by giving the soldiers a glass of port wine, an initial mouthful being followed by the ether mixture and then the remainder of the glass!

Figure 3.5 James Tayloe Gwathmey administering nitrous oxide/oxygen from his own apparatus. (from J.T. Gwathmey, Anaesthesia. New York: Appleton, 1914)
Figure 3.6 Sir Geoffrey Marshall. (Photograph originally published in K. Bryn Thomas, The Development of Anaesthetic Apparatus, 1975. Reproduced with permission of Wiley-Blackwell)
One of the hazards of general anaesthesia is the problem of operating on patients with a full stomach. This appears to have been given scant consideration during the Great War. An American anaesthetist called Flagg was one of the few to consider this problem in the emergency surgical patient.19 In modern practice it is usual to fast people before surgery, so that there are no stomach contents that can be regurgitated or vomited, which could enter or obstruct the flow of air to the lungs. However, soldiers arriving at the casualty clearing stations cold and dehydrated were given a pint of hot tea (or coffee) whilst waiting for surgery. It warmed them up and helped to restore their blood volume and as it was liquid would hopefully not obstruct respiration if vomited. This might seem a strange practice to the present-day anaesthetist who would be concerned by the smallest amount of stomach contents entering the trachea (windpipe). The benefits might have outweighed the disadvantages but Flagg doubted this as he had observed that stomach movements ceased during anaesthesia and little would be absorbed. When wounds are suffered, gastric emptying is delayed and the stomach may remain full for many hours and for decades it has been accepted practice to perform maneuvers at induction which prevent regurgitation. This appears not to have been understood during the Great War as Major Corfield recalls one patient who brought up three bowls of bully beef and biscuit that he had consumed 28 hours earlier and been wounded two hours after it!
Largely as a result of Marshall’s work, the need for a specialist anaesthetist as part of a surgical team was acknowledged.20 Such team structure was haphazard to begin with in 1915, but as time went on, became more structured, so that by 1917 a surgical team with an anaesthetist was a well established group.
How Marshall managed to produce such high quality work with attention to detail in a casualty clearing station is remarkable, and careful charting of blood pressure and pulse rate during well given anaesthetics must have saved many thousands of lives. It is not clear how widespread the use of blood pressure measurement was in the hectic environment of a casualty clearing station. It is conjecture, but perhaps a finger on the pulse was the main monitor. Today it is unacceptable to use anything except ‘minimal monitoring’, that is an ECG recording heart beat, an automatic blood pressure measuring device, pulse oximetry (which indicates the amount of oxygen in the blood) and measurement of gases inhaled and expired including oxygen, carbon dioxide and anaesthetic vapours.
The use of a chart during anaesthesia to record blood pressure and pulse rate can be ascribed to an American Harvey Cushing who is best known for his work as a neurosurgeon.21 He appreciated the importance of a meticulously given anaesthetic with routine blood pressure measurement. He had experienced a defining moment, when as a medical student in the 1890s, he gave his first anaesthetic to an elderly man. The patient vomited, inhaled and died. Cushing felt responsible. He was quickly reassured and told that such things happened frequently, and he should forget about it. He did not forget, and decided instead that he should train himself to be a better ‘etherizer’ and introduced charts to record pulse, respiration and temperature. He stated that careful anaesthesia and record taking:
… was undoubtedly a step towards improvement in what had been a very casual administration of a dangerous drug.22
Initially, charts recorded pulse rate, respiration and temperature. The measurement of blood pressure by an inflatable cuff with a mercury column (sphygmomanometer) was described by an Italian, Riva Rocci, in 1896. On a visit to Switzerland in 1901 Harvey Cushing saw a simplified version of Riva Rocci’s devise in use at the bedside at the Ospidale di St Matteo in Pavia. On returning to America the following year he introduced blood pressure measurement and a new anaesthesia chart into his clinical practice. The blood pressure was determined by palpating the pulse at the wrist and observing when it disappeared with the inflation of a cuff around the patient’s upper arm.
In 1906 Korotkoff, a Russian doctor, described the changes in sound that were heard if a stethoscope was placed over the brachial artery at the elbow. In this way, both the systolic and diastolic blood pressures could be measured reflecting the pressure during contraction and relaxation of the heart. Marshall employed a Riva Rocci sphygmomanometer with stethoscope when he carried out his observations at Remy Siding.
Cushing therefore joins the ranks of men who realized the importance of anaesthesia as a subject even before the turn of the century. He served in the war from 1917 as a surgeon in chief at a base hospital in Boulogne where he took to work Gertrude Gerrard, a nurse anaesthetist who had worked with him in Boston. She was later decorated by the British Red Cross for her work at an advanced unit in Belgium. Nurse anaesthetists have a long history in the USA and are still used today. Their first training program was established in 1909, and when a surgeon by the name of Crile from the Lakeside Hospital, Cleveland, Ohio set sail for the American Hospital in Paris he took two nurse anaesthetists with him, Miss Agatha Hodgkins and Miss Mabel Littleton.23
Owing to a shortage of British anaesthetists the question of training British nurses was taken up by the DGMS in 1917.24 A course was set up, and commenced in January 1918. It was open to all nursing sisters and VADs and lasted for three months, the first two months in selected base hospitals and the third month in a casualty clearing station. The nurses were taught to assess patients before surgery so that the correct choice of anaesthetic could be made, and they were taught how to manage an emergency. Two courses were held and 159 nurses trained although the use of VADs was not sanctioned and neither would the Australians allow their nurses to practice. The result appears to have been very successful but the withdrawal of experienced nurses from other duties was unfortunate.
The importance of the quality and training of personnel at casualty clearing stations became the concern of an American anaesthetist, Arthur Guedel, who was of the opinion that young medical officers could not become proficient and safe learning on the job. He set up training schools in Chaumont and Contrexville. He realized that they needed instruction in basic principles of airway control and depth of anaesthesia. He devised a chart which demonstrated the changes in the reaction of the pupils and certain reflexes under ether anaesthesia so that medical officers could recognize when they had achieved a suitable plane of anaesthesia.25 To cement this training he became a well-known figure travelling between casualty clearing stations on a motorbike.
Text books of anaesthesia had been written from the 1890s but had to be rewritten after the war. Boyle and Hewer’s Practical Anaesthesia, first published in 1907 and again in 1911, required an extra chapter on blood pressure and pulse reactions during anaesthesia when it was reprinted in 1923, presumably at least in part due to advances made during the Great War. It recommended regular charting of these parameters to detect changes from the patient’s norm which would indicate the development of shock and result in prompt treatment with intravenous saline.26
From a 21st Century perspective the areas of research which will be described appeared to be leading physicians down blind alleys and sidetracking them. The fundamental problem which nobody fully appreciated was that many wounded soldiers had lost massive amounts of blood. The clinical problem was aggravated by a lack of fluid intake both before being wounded and on the long transfer back to casualty clearing stations. Extreme cold also made things worse. If they continued to bleed either from a femoral fracture, if it was inadequately splinted, or internally from chest or abdominal wounds, then what might appear manageable at the beginning was life-threatening by the time they reached surgical help.
A healthy young man can lose up to 30% of his blood volume without a change in blood pressure and only a modest rise in pulse rate. He can compensate for even larger amounts of blood loss. He does this by constricting the blood flow to the skin and other organs. Deprived of blood flow and oxygen these tissues continue to function and survive by changing to what is called anaerobic (without oxygen) metabolism. The consequence of this is to produce an excess of acid. Cold makes matters worse. The flow of blood to the periphery is reduced to decrease heat loss and conserve core temperature. However, before measures were taken to keep casualties warm their core temperature must have fallen and we now know that cardiac output (the amount of blood pumped with every contraction of the heart muscle) falls directly with a decrease in body temperature.
When the compensatory mechanisms are inadequate for the blood loss the ability to preserve the blood pressure is lost and the shock worsens. These wounded soldiers needed fluid, blood, warming and early surgical intervention. Furthermore tissues deprived of oxygen provided an ideal environment for the bacteria responsible for gas gangrene to proliferate. These bacteria are classified as anaerobic as they flourish in an oxygen free environment.
The relationship between the amount of fluid in the vascular system and the alteration of the caliber of the blood vessels to compensate for the lack of fluid and blood is fundamental to understanding the mechanisms of shock. In order to direct blood to the vital organs of the body primarily the brain and heart, blood vessels constrict to reduce the blood flow to the skin and the kidneys. In this way the blood pressure is maintained. If the blood pressure falls much below 60mm Hg then the brain is no longer perfused and vital centres of the brain that maintain life cease to function. If a patient survives for any length of time with a very low blood pressure, it may be difficult to reverse, and kidney damage ensues. It should be noted that whenever a figure is given for blood pressure it refers to systolic pressure i.e. the pressure reached when the heart is contracting.
In retrospect it is frustrating to read about the attempts to understand shock when what the soldiers needed were massive amounts of intravenous fluids and pints of blood.
The different theories of shock are outlined below.
Before the war Crile, an American surgeon, became interested in the nature and treatment of shock whilst working in Cleveland, Ohio where a large proportion of his practice was trauma cases due to industrial accidents. After serving in the Spanish-American War he returned to civilian practice in 1901 and developed the kinetic theory of shock. He believed that the brain became bombarded with stimuli from the wound and from the operation, and as a result of fear. It was proposed that the continuation of such stimulation led to exhaustion of the part of the brain that controls the peripheral blood vessels (vasomotor centre) with subsequent dilatation of vessels and a fall in blood pressure. He advocated that the painful stimuli should be abolished by the injection of local anaesthetic and that nitrous oxide be given to eliminate fear. He called this technique anoci-association. As he was using an appropriate anaesthetic along with pain relief that didn’t worsen shock his technique had some value.
Another theory, the acapnia theory, was put forward by Yandell Henderson, an American physiologist. He suggested that the deep and rapid breathing seen after the infliction of a painful stimulus which results in a decrease of carbon dioxide in the blood results in a failure of the centre in the brain that is responsible for maintaining blood pressure. He claimed that when abdominal surgery was performed even more carbon dioxide was lost from the surface of the intestines which exacerbated the problem. In order to counteract this he suggested slow breathing or breathing through a long tube so that expired air was re-breathed. Furthermore warm saline saturated with carbon dioxide could be instilled into the abdominal cavity.
These are just two of the theories that were devised to explain the state of shock which could be defined as a “depression of all the vital functions of the body, the state being primarily induced by the infliction of injury on the body tissues and being characterized by a progressive fall of the blood pressure”.27
During the Great War large numbers of patients suffering from wound shock were seen and their associated high death rate troubled doctors. If the survival rate was to improve then understanding of this condition had to advance. Marshall had solved the problem of which anaesthetics to use but the prevention and treatment of wound shock required the combined talents of a number of physicians and scientists.
In order to co-ordinate research and clinical observation on wound shock the Medical Research Committee (MRC) in 1917 appointed a Special Investigative Committee. This consisted of surgeons who were working at casualty clearing stations supported by physiologists in Britain carrying out research and laboratory doctors at base hospitals. In France a research group was organized in the First Army area. Professor Cannon, an American physiologist from Harvard and John Fraser, a Scottish surgeon who also did a lot of work on abdominal wounds (see Chapter 7), worked in the laboratory and surgical wards of a casualty clearing station in Béthune whilst Captain Ernest Cowell of the RAMC worked further forward.
Cowell established parameters for the normal limits of blood pressure found in fighting men by observing them when there was no active fighting.28 29 Knowing that the release of adrenaline in the body prepared the soldier for battle by increasing heart rate and blood pressure and releasing glucose from the body he wondered whether over a period of time this prolonged exposure to the effects of adrenaline might be harmful. He measured the blood pressure of men in the front line and found it to be raised compared to that of soldiers further back. During a full moon he measured the blood pressures of a garrison of a detached outpost in a part of the line that was exposed. He noted how their blood pressures became raised when danger increased and questioned whether outpouring of adrenaline contributed to the later development of shock if they were wounded.
He studied the onset of shock by making observations on casualties before they were evacuated to the casualty clearing stations. In early 1917, working at “Lone Farm” Advanced Dressing Station, he measured the blood pressure of casualties soon after wounding and observed what happened on the journey from the advanced dressing station to the casualty clearing station.
He was able to demonstrate to surgeons in the field how shock could develop and by now the terms primary and secondary shock were coming into common usage. Primary shock occurred when, after being wounded, a soldier’s blood pressure would be low, but secondary shock didn’t present until a few hours later. Some soldiers appeared in reasonable condition to begin with but after a journey back to the casualty clearing station with little attention paid to food, water and warmth the blood pressure might fall uncontrollably.
Looking back on this term in 1928 Cowell stated that several points stood out:
• The effect of the cold wasn’t appreciated in the early months of the war,
• A correlation between the amount of shock and the extent of muscle injury was noted,
• The slowness of onset of shock was observed,
• Where the blood pressure was low and the patients survived it was beginning to look as if the low pressure predisposed to gas gangrene.
By the summer of 1917 Cowell worked at Casualty Clearing Station No 23 at Lozinghem, which received cases from around Loos. Here he was joined by Professor Cannon and together, at the suggestion of Professor Bayliss, another member of the Shock Committee, they looked at the effects of various intravenous solutions for improving blood pressure.30
Cowell’s contribution to the investigation of shock was a very practical one and although a general surgeon in London during peacetime he became a senior army surgeon during the Second World War.
Cannon, however, had entered the war largely to research the problem of wound shock and he was a scientist. Realising that there was decreased circulation of blood and believing that it was pooling somewhere within the body, he was prompted to look at the use of a substance extracted from the pituitary gland of the brain (pituitrin) which if injected abdominally would constrict the vessels of the splanchnic bed and return the circulation to normal. Crile had already proposed that exhaustion of the vasomotor centre led to dilatation of blood vessels but it was a matter of which vessels the blood was hiding in. As the skin was pale in patients with shock he thought that the blood couldn’t be here but must be in the huge area of blood vessels supplying the bowel (splanchnic circulation). Determined to investigate this at the front, when soldiers from the Battle for Hill 70 came into Casualty Clearing Station 23 he persuaded Cowell to let him inject pituitrin, however it did not work.
From autopsy studies Cannon learnt that there was no pooling of blood in the splanchnic circulation. In so doing, he effectively disproved the theory of splanchnic pooling as an explanation for shock. However, he was determined to solve the mystery of the missing blood and working with Fraser and Hooper in Béthune, Cannon then thought that pooling must occur in capillaries, tiny blood vessels connecting the arteries and veins.31 He found that blood taken from capillaries was more concentrated than blood from larger veins. The greater the degree of shock the greater the discrepancy between the two figures
He concluded that blood was stagnating in the capillaries and that if this blood could be returned to the circulation then the blood pressure would improve. In other words, having disproved splanchnic pooling, he persisted in the mistaken belief that blood must be pooling somewhere else within the body, and he was determined to find out where.
Figure 3.7 Photograph of Walter Cannon, John Fraser and A.N. Hooper, 1917. (Reproduced by kind permission of Harvard Medical Library in the Francis A. Countway Library of Medicine).
He was going from one blind alley (splanchnic pooling) to another (capillary pooling). The reality seems obvious to us now. The blood had been spilled onto the fields of France and Flanders.
Subsequently, Cannon turned his attention to measuring the amount of acid in the blood of shocked patients and he found it to be increased.32 This is called acidosis or acidaemia. In cases of gas gangrene it appeared to be particularly severe and when operated upon it worsened still further. The acidosis was now thought to be a cause of shock and all that would be needed was baking soda! A method of giving sodium bicarbonate intravenously was devised and used with some success to improve the survival of shock.
In June 1918 Colonel Sir Almroth Wright wrote in The Lancet setting out to explain the acidosis seen in shock.33 Work had already been done showing that muscles working without oxygen produced lactic acid and Wright concluded quite rightly that this was the same process as occurred in shock when arrest of the circulation cut off the supply of oxygen to the tissues and metabolism resulted in the production of acid.
As regards treatment of shock he paid particular attention to the warming of patients. Ideally he said prevention of heat loss was better than cure and the giving of hot drinks and application of warmth as early as possible was advisable. However once shock was established then too rapid resuscitation by warmth would convey large amounts of acid to the blood stream once the circulation was re-established. He suggested treating with sodium bicarbonate before resuscitation began and not subjecting the patient to anaesthesia and surgery before the blood alkalinity had returned to normal.
It seems to me that Almroth Wright, a laboratory physician, was beginning to understand the process. Firstly, he recognized that the acid blood was the result of a decrease in circulation to the tissues. In other words, acidosis was the result, and not the cause of shock. From this he concluded that trench foot and chilblains were also produced from the same process i.e. extreme cold decreased blood flow to the foot in such a way that metabolism changed to the anaerobic form and acid was produced in the tissues. He stated that:
The pathology of trench foot and anaesthesia would seem to lie poles apart, but in reality they would seem to have in common the factor of a shutting off of the circulation and the resultant cutting down of oxygen supply to the muscles.34
He recognized that prolonged and severe operations in cold operating theatres would be particularly likely to result in an acidosis and acknowledged Cannon’s warning that it was very important not to superimpose an anaesthetic acidosis upon a wound acidosis. This was an important fact to have recognised not only during wartime but for future surgical practice. Long and difficult operations can only be carried out if the patient is kept warm and fluid and blood losses are replaced in a timely manner.
By the time Gray had written his book The Early Treatment of War Wounds in 1919, the priorities in the treatment of shock had been worked out.35 Gray concluded that most cases of shock were due to haemorrhage and that the extent of blood loss was difficult to estimate and that the total amount lost was greater than generally supposed. In practical terms he stated:
Every effort should be made at the earliest opportunity to replenish the depleted fluid reserves of the wounded soldier by the administration of large amounts of fluid.
As drinking water was limited at the front line, soldiers were already short of fluid, and when wounded any reserves were further depleted by perspiration. The preferred method of giving fluid was by mouth or by rectum, and for it to be preferably warm.
The recognition of the need to actively warm and rehydrate the wounded led to the introduction of resuscitation wards at casualty clearing stations. Special efforts were made to keep wounded men warm on the journey from the front. Blankets, hot water bottles, and better warming of advanced dressing stations all played their part. This reduced secondary shock and the period of resuscitation was shortened. A sister and orderlies acted under a special experienced medical officer who supervised the care of the wounded and prepared them for surgery. If oral and rectal fluids were not tolerated then intravenous fluids were required.
Professor W.M. Bayliss, who was a physiologist and a member of the Shock Committee, delivered a lecture to the Royal College of Physicians of London on 30 April 1918 on intravenous injections in wound shock.36 He recognized that restoring the blood pressure so that oxygen could be delivered to the tissues was the single most important factor to reduce secondary shock. Although it would be thought that blood itself would be the best way to achieve this, he felt that it didn’t show itself to be as superior to other solutions as might be expected. A dilute blood at high pressure was found to be more effective than normal blood under a low pressure. To some extent anaemia could be tolerated if the blood pressure was maintained.
The transfusion of normal saline or Ringer’s solution (basically saline with a few other electrolytes) had been used for some years but as it leaked out of the blood vessels it provided only a transient improvement. The use of hypertonic saline, which is saline that is more concentrated than the surrounding tissues and should therefore hold the fluid within the blood vessels wasn’t much better.
In order to achieve an increase in blood volume Bayliss introduced the use of Gum Arabica into clinical practice. A solution could be made of 6% or 3% in saline and the large molecules of galactose and arabinose present in gum were inert and stayed in the circulation. He found that it was useful in severe haemorrhage and in cases where haemorrhage and shock were not excessive but blood pressure fell after anaesthesia. In one case of gas gangrene where there was neither shock nor haemorrhage but a low blood pressure of 70mm Hg a transfusion of Gum Arabica restored the blood pressure. Gray was less impressed and felt that if the time interval between haemorrhage and the giving of Gum Arabica was prolonged then it was less effective. Therefore the use of this fluid was pushed forward to the field ambulances where it allowed a casualty to arrive at a casualty clearing station in a better condition where, if necessary, blood transfusion could be started.
The introduction of blood transfusion during the Great War can rightly be ascribed to doctors from Canada and America where the subject had been given much more consideration in the first decade of the 20th Century than in Britain. However, the first person-to-person transfusions for acute haemorrhage were carried out in 1818 by James Blundell, a London obstetrician who had seen women dying of post-partum bleeding. Four of the ten transfusions that he carried out were successful, which is remarkable given that he didn’t understand the presence of different blood groups or how to stop blood clotting on its route from one person to another. This meant that blood transfusion remained on rocky ground until 1900, when Landsteiner recognized the existence of three blood groups. The fourth group was recognized two years later in 1902. However the cross-matching of blood didn’t become a practical proposition until almost a decade later when Moss, working at the John Hopkins Hospital, developed a technique at the same time as Jansky, who was working independently in Bohemia.
George Washington Crile, who has already been mentioned in connection with his work on shock, was one of the earliest users of blood transfusion in the field of surgery.37 His first transfusions were carried out without cross-matching or anti-coagulation (to stop the blood clotting) and he regarded it as an adjunct to the treatment of shock rather than a first line measure. He connected an artery in the donor’s wrist to a vein on the inside of the patients elbow. By using a very short tube to connect the two he managed to overlap the two vessels and thus prevent clotting. A letter from Berkeley Moynihan, a surgeon in Leeds, appeared in The Lancet in June 1918, strongly rebuffing the idea that transfusion hadn’t been used in Britain before the war. He had visited Crile in Cleveland, had learned the technique and used it to good effect.38
Blood transfusion during the Great War was first reported in the British Medical Journal in July 1916 by L. Bruce Robertson, a captain in the Canadian Army Medical Corps.39 In cases of primary haemorrhage when initial wounding produced the blood loss, benefit would not be in doubt. However Robertson’s first wartime transfusions were given at a base hospital in cases of secondary haemorrhage where infection had eroded into blood vessels resulting in major bleeding. Blood transfusion made the patient well enough to undergo further surgical intervention to stop bleeding, or boosted the patient’s own condition, thus enabling him to combat the infection.
There were two problems with blood transfusion. The first was the possible introduction of infection from donor to patient, and it was important to establish as far as possible that the donor did not carry syphilis. Healthy donors could withstand the loss of 600 to 1000 ml of blood, which could be replaced by saline. There were also a few convalescent patients with minor fractures and sprains who were relatively healthy but unfit for duty who were ideal donors.
Rifleman Charlie Shepherd’s experience as a donor is quoted in The Roses of No Man’s Land. Finding himself in an American base hospital where a volunteer donor was requested, and seeing that most of the other casualties had both legs blown off, he offered his services. He was rolled into the operating theatre head to tail with the recipient and watched whilst his blood returned the colour to the face of the badly wounded soldier. This made him something of a hero and he was given champagne on his return to the ward. The best part was to be sent back to England for convalescence, when his own wound necessitated no more than two weeks out of the front line.
The second problem with blood transfusion was that of compatibility, where it was important that the donor and recipient blood when mixed together didn’t result in destruction (haemolysis) or sticking together of the red blood cells. Establishment of the scientific basis of grouping and transfusing only compatible blood resolved this problem.40
Other factors that had to be overcome were how to prevent blood clotting whilst it travelled from donor to patient and how to measure the volume of blood transfused. The connection of a vein to a vein or an artery to a vein had the obvious disadvantage of not being able to observe and therefore measure the amount of blood that was transfusing. Initially this was overcome by using a syringe to extract blood from a cannula placed in the donor’s vein, and then injecting it into a cannula in a vein in the recipient. Saline was injected through the cannulae after withdrawing or injecting blood to keep them patent. This process required two skilled operators and an orderly to run between them. Unger of New York devised a piece of equipment with stopcocks that allowed blood to be withdrawn from the donor and injected into the recipient without disconnecting. A saline flush was also incorporated which prevented the cannulae clotting up.41
Another ingenious method was Kimpton’s tubes as shown in Figure 3.8.42
These consisted of a glass tube with a cannula drawn out at one end. This could be inserted into the donor’s vein and placed in such a position that blood would run into it and then lain so that the blood would not escape. When inserted into the recipient’s vein and held upright the blood would then enter the circulation. The tubes could be autoclaved for sterility and liquid paraffin was used to lubricate the inside of the tube and prevent blood from clotting.
Figure 3.8 (a & b) Diagramatic representations of Kimpton’s Tubes (Gordon Stables, Department of Medical Illustration, University of Aberdeen)
Having successfully carried out blood transfusion in base hospitals, there was a desire to carry it forward to the casualty clearing stations and beyond, where primary haemorrhage was killing men. Saline infusions gave only a temporary improvement and Gum Arabica could be used with effect to tide casualties over if the haemorrhage was not too great, but for more seriously wounded soldiers it was insufficient. L. Bruce Robertson reported in 1917 his results of 36 transfusions in primary haemorrhage.43 His results show that cases considered previously hopeless could be improved sufficiently to allow surgery to take place. Also, some patients who had undergone surgery and who then deteriorated due to the combined effect of wound and surgical haemorrhage could be saved by blood transfusion, which prevented them from sliding into irreversible shock. Blood was obviously a precious commodity and it was important to time the giving of a transfusion for maximum effect. Early transfusion would prevent the degenerative change seen if the exsanguinated situation (almost complete loss of blood) was allowed to persist.
By this stage it was realized that the best way of judging how much blood was lost was by measuring the blood pressure.44 Haemoglobin measurements and blood counts didn’t help, and the pulse rate could vary widely, although the danger of a rising pulse rate was recognized. If morphia had been given the pulse rate might be little over a 100 beats per minute. With a blood pressure less than 70mm Hg the patient was precarious and needed transfusion to save his life and if his pressure was less than 90 mm Hg he was not in a good state for operation. Blood pressures of less than 60mm Hg were rarely seen and it was acknowledged that this was only compatible with life for a short period. As shock without haemorrhage could also result in a low blood pressure it was important to realize that other anti-shock measures should be carried out at the same time as considering transfusion.
In his book The Early Treatment of War Wounds Gray suggested successive blood pressure readings while warmth, rest and rectal saline were given. If the pressure failed to rise then transfusion would be required.
The results of Robertson’s 57 transfusions in cases of primary haemorrhage are summarized in Table 3.1.
Table 3.1
The results of Robertson’s 57 transfusions in cases of primary haemorrhage
| Effects of transfusion | Casualties |
| Life-saving (evacuated to base hospital in good condition) | 36+ |
| Immediately beneficial but died from shock | 8 |
| No benefit | 4 |
| Harmful (haemolysis) | 2 |
+ 3 of these patients subsequently died from a combination of pneumonia, tetanus and sepsis.
The problem of donors in a casualty clearing station could be partially overcome by grouping all possible donors ahead of time and then having simple equipment available to type recipients. However the whole process of transfusion occupied two or three members of trained staff and in times of high numbers of casualties it was difficult to keep pace with the demand.
The idea of having a bank of preserved blood available for these situations which could be administered by one medical officer offered a solution. Oswald Robertson of the US Army tested out this possibility at the casualty clearing stations of the British 3rd Army.45 Rous and Turner, working at the Rockefeller Institute in New York, found that blood could be taken into a solution of dextrose and sodium citrate and preserved in the cold for several weeks. Robertson took volunteer donors from among the lightly wounded. Those with a history of malaria, trench fever or syphilis were excluded. The blood was collected and stored in heavy glass bottles called Winchester Bottles, which were kept in ice boxes until required.
Robertson carried out 22 transfusions in 20 individuals, 11 of whom were discharged to the base and nine died. All of them showed an improvement whether the blood had been stored for 3 or 26 days and the effect was as good as fresh blood. The transfusions were given in the resuscitation ward by one medical officer, thus leaving the operating room free for surgical procedures.
Blood was also transported in ambulance wagons over rough roads without suffering damage. Having introduced transfusion to casualty clearing stations there then came a desire to use it further forward in the field ambulances. Norman Guiou of the Canadian Army Medical Corps showed that it was possible to group patients in a field ambulance, find a suitable donor and transfuse them so that they could reach the casualty clearing station.46 Clearly blood transfusions with either fresh or preserved blood could be carried out as far forward as the regimental aid post if the number of casualties was not overwhelming, and this ability to try to save even the desperately wounded had an important effect on the morale of the men. It should be noted that the amount of blood given, 1000ml at maximum, is small compared to the many litres which might be given to a road traffic victim in a modern emergency centre. Blood transfusion would allow a few lucky individuals to move from an unsalvageable situation to one which allowed life-saving surgery to be carried out.
Towards the end of the war resuscitation teams were formed, which were able to advance as far forward as possible to treat the severely wounded. The first was probably established by Dr Holmes à Court of the 4th Australian Field Ambulance.47 A shock centre had been established in early 1918 at No 3 British Casualty Clearing Station at Gezaincourt. As this was in easy reach of the Australian sector it may have been where Holmes a’Court conceived the idea of a field ambulance resuscitation team. They were ready for action at the Battle of Hamel on July 4 1918, which was a limited combined Australian and American offensive near Amiens. Such was their success that they were instituted as permanent establishments in each of the 5 Australian divisions. They consisted of two medical officers, one of whom was expert in rapid urgent surgery and blood transfusion while the other was experienced in anaesthesia, resuscitation and classification of blood donors. Supported by 4 others, 1 non-commissioned officer and 3 orderlies, they were attached to a main or advanced dressing station and had the use of a motor ambulance vehicle. On finding a casualty they would institute warming methods, infuse gum acacia, ligate any large bleeding vessels and amputate shattered limbs. This enabled the wounded to reach casualty clearing stations in a much better state than they would otherwise have been and saved many limbs by the early removal of tourniquets.

This account of the practice of anaesthesia and resuscitation starts well before the Great War. The anaesthetic agents used during the war were the same ones as had been used before. It was the pioneering work of Geoffrey Marshall and others that led to a better understanding of the applicability of the various agents to the seriously wounded. As a result of this work, there was great improvement in survival. It also became clear that there was a definite need for specialist anaesthetists in military service whose role extended to preparing the wounded for surgery pre-operatively.
Figure 3.9 Sir Ivan Magill. (Photograph published in K. Bryn Thomas, The Development of Anaesthetic Apparatus, 1975. Reproduced with permission of Wiley-Blackwell)
These pioneering individuals not only brought the benefits of improved understanding of the use of agents leading to safer anaesthesia, but also the need for a scientific basis of practice, development of equipment and proper training of anaesthetists. They were responsible for making the specialty what it is today. The influence of the Great War on practice continued beyond 1918 and led to one of the most important anaesthetic developments of the 20th Century, introduced by one of the most able anaesthetists of the time, Sir Ivan Magill.48
Magill worked with the plastic surgeon Harold Gillies at the Queen’s Hospital for Facial and Jaw injuries at Sidcup in Kent. Born in Northern Ireland he qualified from Belfast in 1913 when he was issued with a certificate confirming that he had in his training administered one anaesthetic. During the war he joined the Royal Army Medical Corps as a captain and acted as medical officer to the Irish Guards at the Battle of Loos in September 1915. He also worked in a base hospital near Rouen. After the war he worked originally in Barnet before moving to work with Gillies at Sidcup. The anaesthetics were very challenging. It wasn’t possible to hold a face mask on the patient because of where the surgeon was operating, and the patients often required many operations.
When Magill joined the hospital the usual method of giving ether was through the back passage but this resulted in inadequate anaesthesia at the beginning of surgery progressing to unnecessary depth during surgery and a prolonged recovery. Magill introduced the use of tubes which could be passed into the windpipe through the nose through which ether from Shipway’s warm ether apparatus was passed. The ether was insufflated into the windpipe by a motorized pump that drove air through the ether. However it had to come back out of the patient when he exhaled and any obstruction in the throat or mouth would prevent this happening, leading to laboured breathing and increased haemorrhage. Harold Gillies once remarked:
Maggi – you seem to get this anaesthetic into the patient alright, don’t you think you could devise a method of getting it out again so I am not anaesthetized?49
The answer came in one particular case when the patient’s breathing became so laboured that it was necessary for Magill to put another tube down the patient’s other nostril to allow the gases to escape. The back of the throat was then packed with gauze. This eventually led to Magill developing a single endotracheal tube which was passed into the windpipe from the nose and allowed to and fro breathing. At first his invention was treated with scepticism but by the 1970s most anaesthetics were given through an endotracheal tube. Necessity is the mother of invention, and the difficulties anaesthetizing facio-maxillary wounds led directly to the invention of one of the most important pieces of anaesthetic equipment still in use today.50 51
It is unfortunate that it required the large number of casualties of the Great War to launch advances in the practice of anaesthesia. The agents available had hardly changed, but the training of anaesthetists, development of equipment, the preparation of the patient for surgery and post-operative care were revolutionized. The mystery of wound shock began to be unravelled and the lessons learnt applied to civilian practice, enabling more complicated and extensive surgery to be carried out than could have been imagined before 1914.
Above all the advance of anaesthesia owes everything to the clear thinking men and women who felt the subject worthy of their full attention both in peacetime and in war.
1 Corfield, C., “Six months experience at a C.C.S. on the Somme”, Practitioner 1917; 24: pp.251-254.
2 Snow, S.J., Blessed Days of Anaesthesia. New York: Oxford University Press, 1978.
3 Connor, H., “The use of chloroform by British Army surgeons during the Crimean War”, Medical History 1998; 42: pp.161-193.
4 Snow, J., “On the inhalation of vapour of ether in surgical operations”, The Lancet 1847; 50: pp.551-554.
5 Metcalfe, N.H., “Military influence upon the development of anaesthesia from the American Civil War (1861-1865) to the outbreak of the First World War”, Anaesthesia 2005; 60: pp.1213-1217.
6 Wulf, H.F.W., “The centennial of spinal anaesthesia”, Anaesthesiology 1998; 89, No 2: pp.500-506.
7 Houghton, J.W.H. & C.G. Spencer, “Spinal anaelgesia with notes of fifty cases”, Journal of the Royal Army Medical Corps 1905; 4: pp.447-449.
8 Silk, J.F.W., “Anaesthetics a necessary part of the curriculum”, The Lancet 1892; 139: pp.1178-1180.
9 Buxton, D.W., “On the advisability of the inclusion of the study of anaesthetics as a compulsory subject in the medical curriculum”, British Medical Journal 1901; 1: pp.1007-1009.
10 General Medical Council, British Medical Journal 1912; 2: pp.536-538.
11 Macdonald, L., The Roses of No Man’s Land. London: Papermac, 1984.
12 Evans B., “A doctor in the Great War – an interview with Sir Geoffrey Marshall”, British Medical Journal 1982; 285: pp.1780-1783.
13 Marshall G., “Anaesthetics at a casualty clearing station”, Proceedings of the Royal Society of Medicine 1917; 10: pp.17-36.
14 Shipway, F.E., “The advantages of warm anaesthetic vapours and an apparatus for their administration”, The Lancet 1916; 1: pp.70-74.
15 Metcalfe, N.H., “The effect of the First World War (1914-1918) on the development of British anaesthesia”, European Journal of Anaesthesiology 2007; 24: pp.649-657.
16 Thomas, K.B., The Development of Anaesthetic Apparatus. Oxford: Blackwell Scientific Publications, 1975.
17 Marshall, Geoffrey, “Two Types of Portable Gas-Oxygen Apparatus”, Proceedings of the Royal Society of Medicine 1920 (Section Anaestheology); 13: pp.16-19.
18 Gwathmey, J.T., Anaesthesia. London: Churchill, 1925, 2nd ed.
19 Flagg, P.J., “Anaesthesia in Europe on the Western Battle Front”, International Clincs 1918; 3: pp.210-228.
20 MacPherson, W.G. (ed.), History of the Great War based on Official Documents. Medical Services. General History. London: HMSO, 1924, Volume 2, pp.44-45.
21 Hirsch, N.P., “Harvey Cushing: his contribution to anaesthesia”, Anaesthesia and Analgesia 1986; 65: 288-293
22 Beecher, H.K., “The first anaesthesia records (Codman, Cushing)”, Surgery, Gynaecology & Obstetrics 1940; 71: pp.689-693.
23 Bennet, J.A., “War of Ideas”, Proceedings of the History of Anaesthesia Society 1994; 15: pp.59-64.
24 MacPherson, op.cit., Volume 2, pp.165-166.
25 Guedel, A.E., “Third Stage Ether: A sub-classification regarding the significance of the position and movements of the eyeball”, American Journal of Surgery 1920; 34: pp.53-57.
26 Boyle, H.E.G. & C.L. Hewer, Practical Anaesthetics. London: Hodder & Stoughton, 1923, 3rd ed.
27 Fraser J., “Operation shock”, British Journal of Surgery 1923; 11: pp.410-425.
28 Cowell, E.M., “The initiation of wound shock”, Journal of the American Medical Association 1918; 70: pp.607-610.
29 Cowell, E.M., “The pathology and treatment of traumatic wound shock”, Journal of the Royal Army Medical Corps 1928: 51; pp.81-102.
30 Benison, S., A.C. Barger & E.L. Wolfe, “Walter B. Cannon and the mystery of shock: A study of Anglo-American co-operation in World War I”, Medical History 1991; 35: pp.217-249.
31 Cannon, W.B., J. Fraser & A.N. Hooper, “Some alterations in distribution and character of blood in shock and haemorrhage”, Journal of the American Medical Association 1918; 70: pp.526-531.
32 Cannon, W.B., “Acidosis in cases of shock, haemorrhage and gas infection”, Journal of the American Medical Association 1918; 708: pp.531-535.
33 Wright, A.E. & L. Colebrook, The Lancet 1 1918; 191: pp.763-765.
34 Ibid.
35 Gray, Col. H.M.W., The Early Treatment of War Wounds. London: Henry Frowde, 1919.
36 Bayliss, W.M., “Intravenous injection in wound shock”, British Medical Journal 1918; 1: pp.553-556.
37 Boulton, T.B., “The role of George Washington Crile in the development of anaesthesia”, Proceedings of the History of Anaesthesia Society 1991; 9B: pp.54-59.
38 Moynihan, B., “The operation of blood transfusion – letter to the editor”, The Lancet 1918; 191: p.826.
39 Robertson, L. Bruce, “The transfusion of whole blood”, British Medical Journal 1916; 2: pp.38-40.
40 Moss, W.L., “A simplified version for determining the iso-agglutinin group in the selection of donors for blood transfusion”, Journal of the American Medical Association 1917; 68: p.1905.
41 Unger, L.J., “A new method of syringe transfusion”, Journal of the American Medical Association 1915; 64: pp.582-584.
42 Kimpton, A.R. & J.H. Brown, “A new and simple method of transfusion”, Journal of the American Medical Association 1913; 61: pp.117-118.
43 Robertson, L.B. & C. Gordon Watson, “Further observations on the results of blood transfusion in war surgery”, British Medical Journal 1917; 2: pp.679-683.
44 Robertson, L.B., “Blood transfusion in war surgery”, The Lancet 1918; 191: pp.759-762.
45 Robertson, O.H., “Transfusion with preserved red blood cells”, British Medical Journal 1918; 1: pp.691-695.
46 Guiou, N.M., “Blood transfusion in a field ambulance”, British Medical Journal 1918; 1: pp.695-696.
47 Westhorpe, R., “The introduction of a mobile resuscitation service – 1918”, in: Fink, B.R., L.E. Morris & C.R. Stephen (eds.), The History of Anaesthesia: Third International Symposium Illinois: Wood Library, Museum of Anesthesiology, 1992: pp.435-438.
48 McLachlan, G., “Sir Ivan Magill KCVO, DSc, MB, ChB, BAO, FRCS, FFARCS (Hon), FFARCSI (Hon), DA, (1888-1986)”, Ulster Medical Journal, 2008; 77(3): pp.146-152.
49 Pallister, W.K., “Sir Ivan Whiteside Magill (1888-1986)”, in: Atkinson, R.S. & T.B. Boulton (eds.) The History of Anaesthesia; Proceedings of the Second International Symposium. London: Royal Society of Medicine, 1989: pp.605-609.
50 Rowbotham, S., “Ivan Magill”, British Journal of Anaesthesia 1951; 23(1): pp.49-55.
51 Rowbotham, E.S. & I. Magill, “Anaesthetics in the plastic surgery of the face and jaw”, Proceedings of the Royal Society of Medicine 1921; 14: pp.19-27.