Selected Letters Between the United States Public Health Service, the Macon County Health Department, and the Tuskegee Institute, 1932–1972
It is almost impossible to capture what it is like to sit in an archive, whether in Tuskegee, Washington, or Atlanta, and sift through all the extant letters and reports of the Tuskegee Syphilis Study. Even for a seasoned historian, the experience can be overwhelming as the assumptions, beliefs, and convoluted reasoning of those involved in the creation and perpetuation of the study are visible.
Since the contemporary reader begins by knowing what happened in the end in this quintessential American tragedy, the inexorable progress of the study, in its seeming banality and scientific neutrality, is painful to read. For the scientist, researcher, historian, or citizen, these documents are humbling reminders of how much medical research and treatment decisions are inextricably intertwined with assumptions about medical uncertainty, scientific progress, racial and gender stereotypes, and class power.
The thousands of pages of primary documents cannot be reprinted here (but they can be found in the collections cited in the Guide to Further Reading). The selections were made with an eye toward capturing a sense of the range of discussion over the course of the study’s history. The sifting was a difficult task and is meant to capture some of the study’s unfolding and complexity.
Taliaferro Clark, Assistant Surgeon General, Public Health Service, to Dr. J. N. Baker, State Health Officer, Montgomery, Alabama, August 29, 1932
August 29, 1932
Doctor J. N. Baker
State Health Officer
Montgomery, Alabama
Dear Doctor Baker:
I have for some time wished to talk over with you a piece of research work that might be carried out on syphilitic Negroes in Macon County, the expense of which is to be borne by the Public Health Service. If you are likely to be in Montgomery about the middle of September I should like to arrange to leave Washington on the afternoon of September 12th en route for Montgomery to talk this matter over with you in person and then proceed to Tuskegee with a view of securing the cooperation of the Andrews Memorial Hospital of Tuskegee Institute.
In working up the data for the final report to the Julius Rosenwald Fund I was particularly impressed with the fact that a negligible number, something less than 35, of the Negroes under treatment in Macon County during the period of the demonstration had ever had any previous treatment. It seems to me that this situation in a very heavily infected population group affords an unparalleled opportunity of studying the effect of untreated syphilis on the human economy. If you think you will be interested in this subject, but nevertheless cannot arrange to be in Montgomery on the date or dates specified above, I shall arrange to visit you on any date that may be mutually satisfactory.
Very sincerely yours,
Taliaferro Clark
Assistant Surgeon General
Division of Venereal Diseases
TC:AMM
United States Public Health Service Division of Venereal Diseases, Record Group 90 (1918–1936), Box 239, Folder 1, Macon County, National Archives.
J. N. Baker to Assistant Surgeon General Taliaferro Clark, September 23, 1932
September 23, 1932
Assistant Surgeon General, Taliaferro Clark
United States Public Health Service
Washington, D.C.
Dear Dr. Clark:
In accordance with our previously discussed plans, Dr. Gill met with the Macon County Board of Health this morning. At this meeting he presented the proposed study in Macon County and asked for their approval. The Board was quite enthusiastic about the previous project, and was quite willing for this new undertaking to proceed along the suggested lines. Accordingly, they passed a motion approving the project, but with the distinct understanding that treatment be provided for these people. The Board approved the idea of internes from Tuskegee Institute giving this treatment under the general supervision of Dr. Smith, County Health Officer.
The County Board of Health speaks for the organized medical profession in Macon County, so with their endorsement it is now possible to proceed with your further plans.
Kindest personal regards, I am
Very sincerely yours,
J. N. Baker, M.D.
State Health Officer
United States Public Health Service Division of Venereal Diseases, Record Group 90 (1918–1936), Box 239, Folder 1, Macon County, National Archives.
Eugene H. Dibble, Jr., Medical Director, Tuskegee Institute, to Dr. R. R. Moton, Principal, Tuskegee Institute, September 17, 1932
September 17, 1932
Dr. R. R. Moton, Principal
Tuskegee Inst., Alabama
My dear Dr. Moton:
Dr. Taliaferro Clark, Assistant Surgeon General, Division of Venereal Diseases, U.S. Public Health Service came to Tuskegee last Tuesday evening and remained over until Wednesday night. He tried to wait until you returned to the Institute, but he had to catch a train out of Montgomery, so I took him to Montgomery about seven o’clock Wednesday evening.
He was very sorry that he was not able to have a conference with you, and asked me to express to you his very best regards and in the meantime to take up with you his mission to Tuskegee.
The U.S. Public Health Service in connection with the Julius Rosenwald Fund and the Alabama State Board of Health conducted in Macon county a survey of the syphilis problem together with its treatment.
This experiment was very successful but was discontinued due to the lack of funds. The U.S. Public Health Service however, is very anxious to extend its research further into this problem, so that they can find out just what effect syphilis is having on people who have been untreated over a period of years. As you know, there are hundreds of people in this section who probably have certain forms of syphilis and have never had any treatment whatever. This would occur of course, in people from 25 to 70 years of age.
The cost of the treatment of this disease is very high, so that it would be of world wide significance to have this study made. The study, of course would have a special attention paid to the effects of this disease on the cardiovascular system and the nervous system.
It is the desire of Surgeon General Cummings and Dr. Clark that this study should be made at our Hospital. There would be no cost, as I understand it from Dr. Clark, to the Institute. This would necessitate of-course, the use of the facilities of the hospital including the use of a section of the clinical building, the use of the minor operating room for the taking of blood wassermans and spinal fluids.
They would furnish the necessary dressings, cotton, X-Ray films and the Neo-Salvarsan for any treatment given. In a conference with Dr. Ward at the U.S. Veterans Hospital, he has consented with the approval of the Veterans Bureau, for the use of the electro-cardiograph for the taking of heart tracings.
The personnel would be supplied from the Public Health Service, and paid from that service also. This would include one of the Specialists in the Venereal Disease Control Work who would be detailed to Tuskegee for the purpose of directing this course. In addition, Dr. Clark has authorized me, if the thing goes thru’ to appoint one of our own nurses to assist in carrying on this work. The salary of the nurse would be approximately $1200.00 per year, plus $50.00 per month for the maintainence of her car.
In thinking over this and especially in connection with the Alabama State Board of Health, we feel that we could give Miss Eunice Rivers leave from her work at the hospital for the purpose of this service. She, as you know has been connected with the State Department for the past ten years, and has personally done more effective Public Health work with that department than any of our group.
Of course, our Internes and Nurses would be greatly benefited by this training. In addition, Dr. Clark has asked that one of our Internes be allowed two afternoons a week to accompany the Nurse during this course, into the country for the further treatment of these cases.
While this would not bring any additional compensation to our hospital, it would certainly not cost us any more and would offer very valuable training for our students as well as for the Internes. As Dr. Clark said, our own hospital and Tuskegee Institute would get credit for this piece of research work. He also predicts that the results of this study will be sought after the world over. Personally, I think we ought to do it and I would be very glad to talk with you personally or to confer with any committee you desire me to meet.
I am quite sure that you will be hearing from Dr. Clark immediately upon his return to Washington further about this. I am taking the liberty to inclose to you a copy of a letter from Dr. Clark to me.
Yours very truly,
Eugene H. Dibble, Jr.
Medical Director
EHD/J
Incl.
R. R. Moton Papers, General Correspondence, Box 180, Folder 1516, Public Health Service, Tuskegee University Archives. Permission granted by Tuskegee University.
H. S. Cumming, Surgeon General, to Dr. R. R. Moton, September 20, 1932
September 20, 1932
Doctor R. R. Moton
Tuskegee Institute
Alabama
Dear Doctor Moton:
I regret your unavoidable absence from Tuskegee that prevented your meeting Assistant Surgeon General Taliaferro Clark at the time of his recent visit to Tuskegee because I wanted him to explain to you at firsthand the proposed study of the effects of untreated syphilis on the human economy with the cooperation of your hospital. It is expected the results of this study may have a marked bearing on the treatment, or conversely the non-necessity for treatment, of cases of latent syphilis. For this reason I shall be grateful if you shall be able to extend the splendid cooperation offered by Doctor Dibble contingent on your approval.
The recent syphilis control demonstration carried out in Macon County, with the financial assistance of the Julius Rosenwald Fund, revealed the presence of an unusually high prevalence rate in this county and, what is still more remarkable, the fact that approximately 99 per cent of this population group was entirely without previous treatment. This combination, together with the expected cooperation of your hospital, offers an unparalleled opportunity for carrying on this piece of scientific research which probably cannot be duplicated anywhere else in the world.
No doubt Doctor Dibble has explained our plan of procedure to you that contemplates, among other things, an intensive physical and serological examination of untreated cases having positive Wassermann, which may not be carried out in the necessary scientific detail except in a hospital. You can readily see, therefore, that the success of this important study really hinges on your cooperation.
Sincerely,
H. S. Cumming
Surgeon General
TC:AMM
R. R. Moton Papers, General Correspondence, Box 180, Folder 1516 Public Health Service, Tuskegee University Archives. Permission granted by Tuskegee University.
Joseph Earle Moore, M.D., Johns Hopkins University Medical School, to Dr. Taliaferro Clark, Assistant Surgeon General, September 28, 1932
Sept. 28, 1932
Doctor Taliaferro Clark, Assistant Surgeon General
United States Public Health Service
Washington, D.C.
Dear Doctor Clark:
I have given considerable thought to the problem which you raise of the investigation of the course of untreated syphilitic infection in the negroes of Macon County, Alabama. You state that there are in this county about 8000 negroes in a rural area far removed from medical care, and that Wassermann surveys have shown about half the adult population to be infected with syphilis. In order to study the effects of treated syphilitic infection with any accuracy, it would be necessary, it seems to me, to survey the entire adult male population of the county without reference to whether or not their blood Wassermanns were positive or negative. This inclusion of all males is essential, because of the fact that the spontaneous evolution of untreated syphilis may lead to the spontaneous production of a negative Wassermann reaction in a considerable proportion, perhaps twenty-five per cent, of cases. If you rely on a Wassermann survey only, you will miss this group entirely when, as a matter of fact, they may prove to be the most important group of the lot.
Second, the study should be limited to males since only males as compared with females can usually give a definite history of infection.
Third, it should be limited to males who can give a definite history of infection so that the duration of syphilitic infection can be dated with at least approximate accuracy.
Fourth, it should be limited to males over the age of 30 so as to obtain the clinical material composed of patients who have had syphilis for 10 years or longer.
I visualize the selection of this material somewhat as follows: It may be necessary to do a Wassermann survey on the entire population of the county, men, women and children. At the time this Wassermann survey is made, males over the age of 30 should be carefully questioned for a history of syphilitic infection. A history should be accepted as positive only if it includes a story of the lesions of secondary syphilis following at an appropriate interval after a genital sore. A mere history of a penile sore only would not be adequate, inasmuch as the average negro has had as many penile sores as rabbits have offspring. Furthermore, the patient should be able to date, at least with approximate accuracy, the onset of his syphilitic infection. And finally, there must be a definite history of the absence of antisyphilitic treatment. Patients who have been previously treated should be excluded from the detailed survey. I should imagine that in going over the entire 8000 population you might find perhaps two or three hundred males in whom such an adequate history could be obtained. These patients should be selected for special study and the remainder completely disregarded.
In the patients selected for special study, a complete medical history should be taken and a complete physical examination carried out. The history should lay particular stress on the possible occurrence of bone or cardiovascular symptoms, since involvement of these two systems is especially common in the negro. Under the head of the symptoms of cardiovascular syphilis, each patient should be specifically questioned for the presence of dyspnea on exertion, paroxysmal dyspnea, nocturnal or otherwise, and substernal pain.
From the physical standpoint, particular emphasis should be laid by the examiner on the following features of the examination:
• The pupils
• The fundus of the eye
• Simple hearing tests for air and bone conduction (Watch and tuning fork).
• The reflexes
• Deep pain sense in Achilles’ tendons and testes
• Generalized enlargement of the lymph nodes
• Inspection and palpation of all accessible long bones and the skull
• Complete examination of the skin and mucous membranes of the stripped body for lesions or scars (note particularly the palms and soles)
• The presence or absence of retrosternal dulness
• The presence or absence of an accentuated tympanitic, bell-like aortic second sound, especially in patients without hypertension or peripheral arteriosclerosis.
• The presence or absence of visible or palpable pulsation in the episternal notch.
• The presence or absence of cardiac murmurs, particularly in a systolic murmur in the aortic area or a diastolic murmur down the left sternal border.
• The blood pressure
• Palpation and percussion of the abdomen with particular reference to the size of the liver
• Inspection of the genitalia for scar and palpation of the scrotal contents.
In addition to these physical investigations, which should be specifically noted, both in positive and negative form, the following laboratory tests should be carried out:
• Urine
• blood Wassermann
• spinal fluid
• teleroentgenographic and fluoroscopic examination of the chest.
It is understood that this very detailed study will be applicable only to a very small group of the inhabitants and that the remainder may be dismissed with a Wassermann survey and subsequent anti-syphilitic treatment when the Wassermann is found to be positive. It is also understood that where such outspoken lesions as tabes, paresis, aortic insufficiency, aortic aneurysm, etc., exist, it will not be necessary to provide the details of all of the physical findings suggested above. Positive or negative statements as to such a minute examination are intended to pick up particularly those patients with minor abnormalities in the central nervous system and those with syphilitic aortitis uncomplicated by aortic regurgitation or aneurysm.
I think that such a study as you have contemplated would be of immense value. It will be necessary of course in a consideration of results to evaluate the special factors introduced by a selection of the material from negro males. Syphilis in the negro is in many respects almost a different disease from syphilis in the white.
If I or any of the members of my staff can be of any further service to you with reference to this proposed investigation, I should be only too glad to have you call upon me, either for advice or for more concrete assistance.
Respectfully yours,
JEM:G
United States Public Health Service Division of Venereal Diseases, Record Group 90 (1918–1936), Box 239, Folder 1, Macon County, National Archives.
R. A. Vonderlehr, Passed Assistant Surgeon, Public Health Service, to Assistant Surgeon General Taliaferro Clark, January 22, 1933
Tuskegee, Jan. 22, 1933
Dear Dr. Clark:
For some time I have been planning to take up with you the matter of supply of anti-syphilitic drugs and the present scarcity of mercury forces the problem rather acutely upon us. We have received none of the oleate of mercury as yet but I believe that this shipment will be somewhat inadequate except for immediate demands. A recent inventory of our neoarsphenamine shows that this supply also is rapidly becoming exhausted.
The need for the strictest economy in this project is and has been fully appreciated from its inception, but, as you know, unusual and unexpected conditions have complicated the problem and made it much more expensive than originally anticipated. The positive Wassermann prevalence is perhaps the most outstanding example but the number of individuals receiving previous treatment is higher than we believed it to be.
At the present time it is probably that the number of patients under antisyphilitic treatment approximates 500. I have completed about 1175 physical examinations on negro men in the desired group, and experience has taught us that these men constitute about 33.3% of the syphilitic individuals uncovered. I do not believe that the number of negroes under treatment will go much above the present peak but if we are to continue the study the number will remain at about that figure. The completion of the course of arsenic will automatically eliminate large numbers of patients each month, equalizing the new numbers acquired. It is desirable and essential if the study is to be a success to maintain the interest of each of the cases examined by me through to the time when the spinal puncture can be completed. Expenditure of several hundred dollars for drugs for these men would be well worth the while if their interest and cooperation could be maintained in so doing. Our serious mistake made in the beginning was that patients receiving neoarsphenamine were given heavy metal treatment concomitantly instead of following the course of arsenic with mercury treatment and prolonging the therapeutic period without any additional cost. I only learned of this concomitant treatment a few days ago from Dr. Smith and have given him strict instructions to give treatment with both drugs simultaneously in the early communicable cases of syphilis only. This will lengthen the treatment period in late syphilis 50% without extra cost and decrease the probability of injury to vital organs already discussed. We are also cutting the dose of neoarsphenamine in all late cases of syphilis from 0.6 grams to 0.4 grams, any action which I feel will not be detrimental to the welfare of those under treatment. It would be a great economic aid if the number of women applying for treatment could be decreased and Smith and myself have under consideration various methods to accomplish this end without injury to the project. We are at present endeavoring to bring in the husbands of the infected women, and already show special consideration to such female patients. Any drastic attempt to separate the sexes would be productive of more harm than good as I informed you in my December report.
I should like to give you some idea of the amount of antisyphilitic drugs which we will need if 400 cases are to be examined. I previously estimated that it would take until March 15th to complete 300 examinations, and, if the tilling of the soil does not offer too many difficulties, we should finish the 400 by May 1st. The spinal punctures should be carried out in one month and treatment could be stopped about June 1st. This gives us a period of four months—about 18 weeks—during which we must treat an average of 500 patients once a week. We shall, therefore, need for the 300 patients on mercury about 75,000 doses (300 patients X 18 weeks X 14 doses per week for mercury administered per [unclear]=75,600 doses). If mercury inunctions are given in the oleate, a 1/4 lb. jar lasts a pt. with a belt one month, and one would need approximately 300 lbs. of oleate of mercury in 1/4 lb. (300 patients X 4 months=1200 one fourth pound jars). Two hundred of the weekly patients receive neoarsphenamine, and without committing myself as to the amount of treatment we would administer I have the promise of Dr. Gill, after a visit to Montgomery yesterday, for a supply of neoarsphenamine sufficient to treat 100 cases weekly. We have at present 300 grams of the first arsenic sent or enough with Dr. Gills supply to last six weeks to carry on treatment until June first—12 additional weeks—we shall need 50 grams per week or 600 more grams. Recapitulating then we shall need the following drugs to carry the study to completion on approximately June 1st:
600 grams neoarsphenamine
150—3.0 gram ampules
150—0.6 ″ ″
75000 pill of protiodide of mercury or 300 lbs. oleate of mercury in 1/4 lb. jars. I realize that this request is very much greater than we originally thought it would be, but am certain that our experiment cannot be carried out without treatment. If we are to retain the services of Dr. Smith after Jan. 31st the question of the administration of these drugs is settled, and without Smith or someone of his ability we could not carry on. In making the request for these drugs I believe that the added expense is justifiable for the great amount of good, which they will do per se to the negroes of the county, irrespective of the effect their administration will have on the study of untreated syphilis.
Sincerely yours,
R. A. Vonderlehr
P.A. Surgeon
United States Public Health Service Division of Venereal Diseases, Record Group 90 (1918–1936), Box 239, Folder 2, Macon County, National Archives.
R. A. Vonderlehr to Dr. Clark, April 8, 1933
Tuskegee, Ala, April 8, 1933
Dear Doctor Clark:
For some I have been thinking of an aspect of the study of untreated syphilis being conducted here, which may not have occurred to you. I do not submit this idea with the desire that it even be considered a suggestion but rather that you keep it [in] mind until I return to my work in Washington.
At the end of this project we shall have a considerable number of cases presenting various complications of syphilis who have received only mercury and may still be considered untreated in the modern sense of therapy. Should these cases be followed over a period of from five to ten years many interesting facts could be learned regarding the course of complications [of] untreated syphilis. The longevity of these syphilitics could be ascertained, and if properly administered I believe that many necropsies could be arranged through the hospital at the Institute with the cooperation of the National Institute of Health. A part time social worker should be able to see the cases as often as necessary and the whole scheme could be supervised by one of our officers occasionally. Undoubtedly other interesting points for study could be worked out should this follow-up work be considered seriously. I realize, of course, the difficulties in the way of the projection of such a plan in view of the unsettled conditions and the urgent need for economy. However, it seems a pity to me to lose such an unusual opportunity.
Sincerely yours,
R. A. Vonderlehr
P.A. Surgeon
United States Public Health Service Division of Venereal Diseases, Record Group 90 (1918–1936), Box 239, Folder 2, Macon County, National Archives.
R. A. Vonderlehr to Surgeon O. C. Wenger, July 18, 1933
July 18, 1933
PERSONAL AND CONFIDENTIAL
Dear Doc:
During the past 6 weeks I have been busily engaged in reviewing the literature in connection with our recent study of untreated syphilis in Alabama. I have also discussed the matter with a number of the officers here in Washington and everyone is agreed that the proper procedure is the continuance of the observation of the Negro men used in the study with the idea of eventually bringing them to autopsy. I realize that this may be impracticable in connection with some of the younger cases, but those more advanced in age with serious complications of the vital organs should have to be followed for only a period of a few years.
Some time ago I submitted a memorandum to the Surgeon General outlining the activities in which I believed the Division should take part and one of these activities was the continued observation of our untreated syphilis cases. I have reason to believe that this program will be approved by the Surgeon General. I am taking this matter up with you primarily to ascertain whether or not you have any member of your staff whose services could be dispensed with without serious harm to the work at Hot Springs. Here in Washington the Division has lost (including Doctor Clark) 3 of the 15 former members of the personnel and there is also a possibility that 2 of our statistical workers, whose salaries are at present being paid by a philanthropic organization, may be discontinued on January first. While it might be possible to drop one of the clerks in the statistical section, this work would be greatly handicapped if we lost the support of the philanthropic organization.
Briefly my plan in Tuskegee is to obtain the cooperation of the state and local health departments and, most important of all, the Tuskegee Institute Hospital. Doctor Dibble would probably accept the appointment of Acting Assistant Surgeon and act in an advisory capacity as far as the nurse was concerned. As you know, the nurse I plan to use was the previous one employed during the untreated syphilis project last winter, and I feel that we could employ her on a two-thirds time basis, having her furnish transportation, for $1,000 a year. I believe that $200 per month additional would furnish incidental needs, such as small amounts of medicines, et cetera.
I would like for you to give this matter your careful attention and let me hear from you in the next few days.
Doctor Pierce has promised to detail an Assistant Surgeon in the regular corps to Hot Springs for a period of 8 months in order to familiarize him with work in the venereal diseases. It is my aim, if possible, to keep a young Service officer at all times stationed with you.
With best wishes from all in Washington,
Sincerely yours,
(Sgd) R. A. Vonderlehr
R. A. Vonderlehr
Passed Assistant Surgeon
RAV:AMM
Surgeon O. C. Wenger
U.S. Public Health Service
Hot Springs, Arkansas
United States Public Health Service Division of Venereal Diseases, Record Group 90 (1918–1936), Box 239, Folder 2, Macon County, National Archives.
O. C. Wenger to R. A. Vonderlehr, July 21, 1933
July 21, 1933
Personal and Confidential
Dear Von:
In reply to your personal letter of the 18th., let me explain the duties of our staff so you will understand how understaffed we are.
My own time is taken up as the executive officer and filling in where ever needed. [Letter continues to list the staff and their duties at the Public Health Service Venereal Disease Clinic in Hot Springs, Arkansas]
You can readily see that we are understaffed. Further more, none of the staff, with the exception of myself, has had any experience in the field. We certainly could not spare any of the doctors for the work in Macon County and no other member of the staff, even if available could handle this field work.
I remember we discussed this matter when together in Tuskegee and I agreed with you it would be a good plan. I believed at that time and still do that you can carry out your program without the aid of the nurse at $1,000 per annum. I don’t see that she can do anything else than use up gasoline making weekly calls on these patients, which does not seem to me to be necessary.
As I see it, we have no further interest in these patients until they die [underlining in the original]. To secure the post-mortems two plans present themselves. When these patients die, some one of the dozen or more physicians in Macon County must sign a death certificate, which goes to the County Health Officer, Doctor Murray Smith. Doctor Smith could then notify Doctor Dibble who could make arrangements for the post-mortem. Or, thru the cooperation of Doctor Dibble, we could arrange with the doctors in Macon County to turn over to Doctor Dibble any of our demonstration cases applying to them for treatment. This would enable Doctor Dibble to keep more complete notes on these cases and in the event of a death he would have more time to persuade the family to have a post-mortem performed. I know the doctors of Macon County well enough to believe they will cooperate.
There is one danger in the latter plan and that is if the colored population becomes aware that accepting free hospital care means a post-mortem, every darkey will leave Macon county and it will hurt Dibble’s hospital. This can be prevented, however, if the doctors of Macon County are brought into our confidence and requested to be very careful not to let the objective of the plan be known.
It may be several months or longer before any of these cases need medical attention and I cannot see how the nurse would be profitably employed all of the time. In fact it seems to me that nurse might do more harm than good by making weekly visits to these families in the hope of finding them in extremis and ready for a postmortem. If the nurse continues to call and give these patients medicines, some of the local doctors might object and embarrass the State Board of Health and local health unit.
I am sure that Doctor Dibble will cooperate and that he will accept a position as Acting Assistant Surgeon at $1.00 per annum as you suggest.
Now there is something else. Who will do the post-mortems? Certainly not Dibble or any of his internes because their findings would be of no more scientific value than if you or I did the post-mortem. So why not bring into the picture the pathologist at the U.S. Veterans Bureau Hospital? Then we will have a postmortem record that is worth while.
summarize:
We have no personnel available at this clinic.
A nurse does not seem necessary to this program.
Doctor Dibble and the Macon County doctors will cooperate.
Patients decease may either be reported thru the County Health Officer when death certificate is filed, or the local physicians may refer patients to Doctor Dibble when they report to him for treatment.
Now let me have your reaction to this. Perhaps you can run to Montgomery and Tuskegee yourself and see Baker, Gill, Dibble and the local men. If you can’t go yourself and want me to go down there for a few days I can arrange to do so. I do wish, however, you would go yourself and then come on to Hot Springs for a few days visit.
The best news I have heard is that Doctor Pierce and you are planning on sending a young regular officer here for training.
Best regards to everybody, including Lady Vonderlehr.
Sincerely,
O. D. Wenger, Surgeon
Acting Medical Officer in Charge
OW/CR
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 5, Folder Correspondence, National Archives–Southeast Region, East Point, Georgia.
R. A. Vonderlehr to Dr. H. T. Jones, Tallassee, Alabama, November 20, 1933
November 20, 1933
Doctor H. T. Jones
Tallassee, Alabama
Dear Doctor Jones:
A week or two ago I paid a visit to Tallassee for the purpose of contacting you in connection with the study of untreated syphilis in the Negro, which the Public Health Service is conducting in Macon County with the cooperation of the Alabama State Health Department, the Macon County Health Unit, and the Tuskegee Institute. About 400 cases of syphilis in Negro males 25 years of age and over have been found and subjected to thorough clinical and roentgenological examinations. Preliminary analysis of the records of this group shows that cardiovascular disease is extremely frequent although it is impossible to say just how much syphilis is responsible for the cardiovascular disease. Hypertension and arteriosclerosis were frequent complications and a control group of 200 Negroes is now being examined with the idea of noting the prevalence of arteriosclerosis and hypertension in this nonsyphilitic group.
This study should give valuable information to the scientific world in indicating the efficacy of present-day antisyphilitic treatment. The Public Health Service already has on hand records of a fairly large number of Negroes who have been both adequately and inadequately treated for syphilis and it is our desire to use the untreated group now being examined in Macon County as a comparison to indicate the value of treatment.
In order that the observation of this untreated group may be completed, it has been decided to attempt to follow the clinical course in the 600 syphilitic and nonsyphilitic Negroes and in case of death attempt to obtain a necropsy. Arrangements for the necropsy have been made with the Tuskegee Institute but if the attempt is to be most successful it is believed that it will be necessary to hospitalize those cases in the event of a terminal illness. The Tuskegee Institute has agreed to furnish free hospitalization to each one of these patients should he become seriously ill, and your cooperation is sought in reporting the serious illness of any one of these Negroes who may consult you. This can probably be best worked out if you will ask Negroes past the age of 25, in the neighborhood of Realtown on the Macon-Tallapoosa County border who consult you for a serious illness, whether they were examined for bad blood by the “Government doctor” at Tuskegee Institute. Your alertness in detecting these cases and immediately notifying Doctor Eugene H. Dibble, Jr., Tuskegee Institute, Alabama, will do much to make this study a success. It is doubtful whether a great deal can be accomplished without your cooperation.
By direction of the Surgeon General:
Respectfully,
(Sgd) R. A. Vonderlehr
R. A. Vonderlehr
Passed Assistant Surgeon for Division of Venereal Diseases
RAV:AMM
United States Public Health Service Division of Venereal Diseases, Record Group 90 (1918–1936), Box 239, Folder 3, Macon County, National Archives.
Patient X, Auburn, Alabama, to The Public Health Service, June 4, 1934
Auburn, Ala
June 4, 1934
The Public Health Service
Dear Sirs your answer to my letter of May 12 Stating that you would try to arrange to have Doctor Dibble of the John A hospital to give my wife some treatment it was suggested that I take her to Doctor Dibble in the near future that he would tell me whether he would be able to treat her or not so I have been to see him and he said that he could and would Just as soon as you sent the Medicines and was to let me know as soon as he got it but have fail to here from him so if you have not sent it please send it because my wife is haves a lot of trouble with blood. [I told] Doctor Dibble said they come [here] that bad blood Please let me hear from you but at once and if you all send the medicines tell Doctor Dibble to notify me my wife is [blanked out in original]
Your
[subject name blanked out in original]
United States Public Health Service Division of Venereal Diseases, Record Group 90 (1918–1936), Box 239, Folder 3, Macon County, National Archives.
R. A. Vonderlehr to Patient X, June 7, 1934
June 7, 1934
R.F.D. 2, Box 76
Auburn, Alabama
Dear Rubin:
Your letter of June 4, making further request that treatment be given your wife, has been received. The medicine which Doctor Dibble required for the treatment of your wife’s bad blood has been furnished him and if you will take her to John A. Andrew Hospital I am sure treatment will be started immediately. On the day that you take her go in the morning and tell her not to eat any breakfast before she leaves home.
It has been possible for the Public Health Service to give your wife this treatment because we are cooperating with the Tuskegee Institute and the Macon County Board of Health.
Very truly yours,
(Sgd) R. A. Vonderlehr
R. A. Vonderlehr
Passed Assistant Surgeon
Division of Venereal Diseases
RAV:KNV
United States Public Health Service Division of Venereal Diseases, Record Group 90 (1918–1936), Box 239, Folder 3, Macon County, National Archives.
Austin V. Deibert, Passed Assistant Surgeon, to Dr. R. A. Vonderlehr, November 26, 1938
Nov. 28, 1938
Doctor R. A. Vonderlehr
Assistant Surgeon General
Division Venereal Disease
United States Public Health Service
Washington, D.C.
Dear Doctor Vonderlehr:
In the two months which have passed since I began the resurvey of our untreated syphilis study, I noticed the increasing incidence of cases who received some arsenical therapy on their admission to the study. Recently I analyzed statistically from the files that I have here, and according to age groups, the amount of treatment they received. I was quite amazed to discover that fully 40% of the group had received some treatment, even though inadequate. The grouping is as follows:
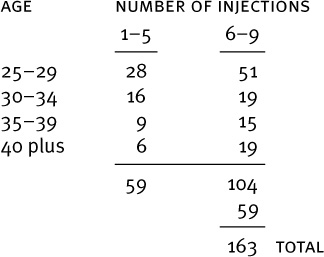
I understand that our study is, in spirit, an introspective one in contradistinction to the retrospective study of Bruusgaard. I firmly believe that we cannot obtain a true reflection of the course of untreated syphilis in view of 40% of the cases having had some treatment.
I have made no attempt to divide the 163 cases into early and late syphilis as inadequate treatment reacts in various ways. Apparently in early syphilis a few injections of an arsenical suffices to greatly lower, if not prevent, late syphilitic cardiovascular disease. Again, inadequate treatment in early syphilis greatly increases the incidence of neurorecurrence and other forms of relapse. The effect of inadequate treatment on late syphilis is problematical. In view of the foregoing statements I acutely fear that adverse criticism of the study would be justifiable, viewing it as an “untreated group.”
With your approval, and if reasonably statistically sound, I would like very much to supplement the present study with the following plan, believing that it would not cause an appreciable increase in expenditure of time or money: 1) Maintain the syphilitic cases who have received some treatment as a study group of inadequately treated cases and on whom subsequent periodic observations can be made. 2) Replace these cases with strictly new untreated men of comparable ages and infection dates.
I am assured here that little trouble would be encountered in finding suitable cases as numbers have stated they would like very much to get on the “government list,” and Dr. Smith advises that I could, with comparative ease, locate many cases in his files with positive blood tests who have never received any therapy.
Hoping that such a plan as this will meet with your approval, I am,
Sincerely yours,
Austin V. Deibert
Passed Assistant Surgeon
Tuskegee, Ala.
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 7, Folder 1938, National Archives–Southeast Region, East Point, Georgia.
R. A. Vonderlehr to Austin V. Deibert, December 5, 1938
December 5, 1938
P.A. Surgeon Austin V. Deibert
U.S. Public Health Service
c/o County Health Department
Tuskegee, Alabama
Dear Doctor Deibert:
Your letter of November 28th has been received and I am sorry that you were surprised to learn that a considerable group of the individuals included in the untreated syphilis study in Macon County had actually received treatment. I had the impression that we had discussed this matter with you before you went to Alabama. The reason treatment was given to many of these individuals was twofold: First, when the study was started in the fall of 1932, no plans had been made for its continuation and a few patients were treated before we fully realized the need for continuing the project on a permanent basis. Second, it was difficult to hold the interest of the group of Negroes in Macon County unless some treatment was given. This was particularly true in the patients with early syphilis. In consequence, we treated practically all of the patients with early manifestations and many of the patients with latent syphilis.
I have discussed with Miss Usilton your plans for examining additional Negro males in the proper age groups to replace those who were previously treated. If you can find the Negro males in these age groups who have been untreated without a great deal of additional work, I see no reason why they should not be carefully examined. It is desirable to increase the number of individuals included in this study because the number is already small for the purpose of statistical analysis.
If it is not possible to add to the number of untreated syphilitic Negro males included in the study, it will, of course, be necessary to exclude all of those who were treated some years ago in the future. I doubt the wisdom of bothering to examine the treated individuals carefully because we already have in the clinics of the Cooperative Clinical Group a considerable number of Negro males in the proper age groups who have received inadequate treatment and who are under observation.
Sincerely yours,
(Sgd) R. A. Vonderlehr
R. A. Vonderlehr
Assistant Surgeon General
Division of Venereal Diseases
RAV:MCK
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 7, Folder 1938, National Archives–Southeast Region, East Point, Georgia.
Austin V. Deibert to R. A. Vonderlehr, March 20, 1939
March 20, 1939
Asst. Surgeon General R. A. Vonderlehr
Division of Venereal Disease
U.S. Public Health Service
Washington, D.C.
Dear Doctor Vonderlehr:
I was very much disappointed that your trip South was cancelled but realize how necessary was your presence in Washington at that time.
My chief reason for wanting to talk to you was regarding spinal punctures on the group. I know now that if I had not deferred obtaining spinal taps, we wouldn’t have examined half the cases we have to date. They simply do not like spinal punctures. A few of those who were tapped are enthusiastic over the results but to most, the suggestion of another causes violent shaking of the head; others claim they were robbed of their procreative powers (regardless of the fact that I claim it stimulates them); some experienced memorable headaches. All in all and with no attempt at humor, it is a headache to me.
As a consequence of those primary taps, Nurse Rivers has had some difficulty getting patients in when breaking into a new community. After the word passes along sufficiently that we are not giving “back shots” they come out of the canebrakes. I hope I know something of the psychology of the negro but at any rate I try my best to send them forth happily shouting the praises of the clinic to their friends at home.
If we repuncture, or try to, I gravely fear that they will not be persuaded to come in a third time and the study would collapse. Those cases who have not had punctures and those whose fluids were positive, I think should be punctured.
I don’t believe that any information relative to neurosyphilis on this group would be of much value as it would be open to criticism in that malaria is so widespread here. Doctor Smith tells me a survey here last year of 1,600 people revealed the presence of parasites in 20%. No one can say how many have had or will be infected with malaria before the study is over. Malaria probably is the best treatment for neurosyphilis and nearly every patient I have seen so far gives a good history of having had it. So far in the study I have found only a few neurosyphilitics and they were vascular affairs and optic atrophies with not a case of tabes or paresis.
With the exception of new patients, those old ones who have not been punctured and in cases who had positive fluids, I personally feel that repuncture is inadvisable. The danger of jeopardizing the future of the study by lack of cooperation of the patients far outweighs the importance of obtaining information about the spinal fluid, which information at best would be open to adverse criticism. I would like very much to have your reaction to this.
Sincerely yours,
Austin V. Deibert
P.A. Surgeon
Tuskegee, Ala.
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 7, Folder 1939, National Archives–Southeast Region, East Point, Georgia.
R. A. Vonderlehr to Special Consultant C. A. Walwyn, John Andrew Memorial Hospital, June 13, 1939
June 13, 1939
Special Consultant C. A. Walwyn
U.S. Public Health Service
c/o John Andrew Memorial Hospital
Tuskegee, Alabama
Dear Doctor Walwyn:
Within the next month or two the Public Health Service proposes to make available on loan to the Macon County Health Department a mobile treatment unit for the control of syphilis in this area. If the usefulness of the mobile unit is demonstrated, it may be extended to include one or two counties adjacent to Macon County.
Some time ago Doctor J. N. Baker requested that Nurse Eunice Rivers be assigned to duty on this unit, and because I feel that it will facilitate the follow-up of patients included in our study of untreated syphilis, I have recommended to the Surgeon General that this assignment be made. Consequently, official orders have been requested assigning Nurse Rivers to duty with the Macon County Health Department. I trust that this action meets with your approval.
Sincerely yours,
(Sgd) R. A. Vonderlehr
R. A. Vonderlehr
Assistant Surgeon General
Division of Venereal Diseases
RAV:MCK
cc: Dr. Deibert
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 12, Folder Personnel 1938–39, National Archives–Southeast Region, East Point, Georgia.
Murray Smith, M.D., to R. A. Vonderlehr, November 27, 1941
Tuskegee, Alabama
November 27, 1941
Dr. R. A. Vonderlehr
U.S. Public Health Service
Washington, D.C.
Dear Doctor Vonderlehr:
When it comes time for you to renew the Milbank appropriation for taking care of autopsies in the untreated syphilis study, I wish that you would give some consideration to placing the Fund with the Macon County Health Department instead of the Tuskegee Institute. The officials at Tuskegee Institute are not the same ones that you and I had such fine cooperation with a few years ago. They know nothing about the study, they do nothing for the patients, and for two years autopsies have been done in undertaker parlors. This proved to be more convenient for undertakers, and for us. The Institute will pay no bills that Dr. J. A. Kenny does not approve. Dr. Kenney knows nothing of what is going on, is always hard to find and is out of town a good deal of the time.
If you will allow us to disburse the fees, it will give us a closer tie-in with the families and undertakers, whereas at present, they feel that Tuskegee Institute is giving them this help. They have lost sight of the fact that the Health Department is still doing its part in keeping the study going along according to plans.
Please advise me of your reaction to this proposition. Its sole aim is to place the Health Department more in the “spot light” than Tuskegee Institute.
Sincerely yours,
Murray Smith, M.D.
Special Expert, V.D.
Tuskegee Syphilis Study, HEW Report Documents, Bound Book II, Tuskegee University Archives.
D. G. Gill, Bureau of Preventable Diseases, Department of Public Health, State of Alabama, to R. A. Vonderlehr, July 3, 1942
July 3, 1942
Dr. R. A. Vonderlehr
Assistant Surgeon General
U.S. Public Health Service
Washington, D.C.
Dear Doctor Vonderlehr:
Dr. Murray Smith has called my attention to the fact that in our program of getting all selectees who are rejected for syphilis under treatment we are encroaching on some of your study material. Apparently a few of the untreated cases of syphilis have been called for army duty and rejected on account of a positive blood. In conjunction with the draft boards we are insisting on all these men taking treatment. I am wondering if we should make an exception of these few individuals. There should not be many of them involved since most of your group are beyond draft age by this time. I would appreciate your advice on this matter.
Very sincerely yours,
D. G. Gill, M.D., Director
Bureau of Preventable Diseases
DGG/h
Tuskegee Syphilis Study, HEW Report Documents, Bound Book II, Tuskegee University Archives.
Vonderlehr to Gill, July 10, 1942
Bethesda Station
July 10, 1942
Dr. D. G. Gill
Director
Bureau of Preventable Diseases
Department of Public Health
Montgomery, Alabama
Dear Doctor Gill:
Receipt is acknowledged of your letter of July 3rd regarding the treatment of some of the men included in the study of untreated syphilis in Macon County under the provisions which have been set up for the treatment of selectees in connection with the current mobilization program.
Some time ago Doctor Murray Smith wrote to me about this matter. I suggested to him that he confer with the chairman of the local Selective Service Board, Mr. J. F. Segrest, and explain to him that this study of untreated syphilis is of great importance from a scientific standpoint. It represents one of the last opportunities which the science of medicine will have to conduct an investigation of this kind.
Doctor Smith replied that he had furnished the local board a list containing 256 names of men under 45 years of age and asked that these men be excluded from the list of draftees needing treatment. During his conference with the board they agreed to this arrangement in order to make it possible to continue this study on an effective basis.
Sincerely yours,
(Sgd.) R. A. Vonderlehr
R. A. Vonderlehr
Assistant Surgeon General
Division of Venereal Diseases
RAV:LR
Tuskegee Syphilis Study, HEW Report Documents, Bound Book II, Tuskegee University Archives.
Murray Smith to R. A. Vonderlehr, August 6, 1942
Tuskegee, Alabama
August 6, 1942
Dr. R. A. Vonderlehr
U.S. Public Health Service
Washington, D.C.
Dear Doctor Vonderlehr:
A new situation has arisen with reference to the untreated syphilis study patients. Some of the Control cases who have developed syphilis, are getting notices from the draft boards to take treatment. So far, we are keeping the known positive patients from getting treatment. Is a control case of any value to the study, if he has contracted syphilis? Shall we withhold treatment from a control case who has developed syphilis? Please let me have your wishes with reference to handling this type patient and I shall carry them out as best I can.
Sincerely yours,
Murray Smith, M.D.
Special Expert, V.D.
MS/s
Tuskegee Syphilis Study, HEW Report Documents, Bound Book II, Tuskegee University Archives.
R. A. Vonderlehr to Dr. Murray Smith, August 11, 1942
Bethesda Station
August 11, 1942
Dr. Murray Smith
Macon County Health Dept.
Tuskegee, Alabama
Dear Doctor Smith:
Replying to your letter of August 6th, it seems to me that the non-syphilitic control cases in the study of untreated syphilis in the Negro who have acquired syphilis since the time the study began have lost their value to the study.
There is no reason why these patients should not be given appropriate treatment unless you hear from Doctor Austin V. Deibert who is in direct charge of this study and who may foresee some objection with which I am not familiar.
Sincerely yours,
(Sgd) R. A. Vonderlehr
R. A. Vonderlehr
Assistant Surgeon General
Division of Venereal Diseases
RAV:LR
CC: Dr. Deibert
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 17, Folder Vonderlehr, National Archives–Southeast Region, East Point, Georgia.
Dr. Wenger, “Untreated Syphilis in Negro Male,” September 18, 1950
Dr. Wenger
Hot Springs Seminar
In this series of meetings there has been much discussion about finding people with syphilis, how to treat them and how to evaluate the results of that treatment. This is good and it is proper. But in the few minutes I have, I wish to focus your attention on another aspect of the broad study of syphilis, that of its effect on those you don’t find, don’t treat and don’t follow.
This subject of untreated syphilis is not something new. The study of it was started some twenty years ago and has been plodding quietly along ever since, with parts of the findings coming to print sporadically. I would like briefly to review the matter.
Among the many interests of the late Julius Rosenwald was the health and welfare of the American Negro. From the Fund that now carries his name came money which was used in cooperation with Federal, State and local health departments for a survey of the prevalence of syphilis among negroes. One county in each of six southern states was chosen for study. The highest rate was found in Macon County, Alabama. Not only was the prevalence higher, but it was found that only one out of 25 had received treatment. With this as a start, Drs. Vonderlehr, Heller, Taliaferro Clark, Austen Diebert and myself, along with others, got together to organize a study of the syphilitic process when uninfluenced by treatment and to compare those findings with results after treatment had been given.
We decided to limit the study to negro males 25 years old or more. In the winter months of 1931–32 and 32–33 a group of 399 negro males with untreated syphilis was selected together with a group of 201 negro males who were presumably nonsyphilitic to be used as a control. The age distributions in the two groups were comparable.
I won’t bother you with minor details of how the study was to operate except to say that all were to have regular blood tests, and physical examinations. In addition it was planned to secure autopsies at death whenever possible. The Milbank Memorial Fund agreed to contribute money for necropsy. Part of the money goes to the physician doing the work and part of it goes to the family to aid in burial expenses.
The first physical examinations were made in 1932–33 with the findings published in September 1936. In 1938–39, a second physical examination was made at which time it was found that a considerable proportion of the younger men had received some but inadequate treatment.
From the second examination came two papers in 1946—one covering mortality, in February and one on cardiovascular abnormalities and other forms of morbidity, in December.
A third physical examination was made in the fall of 1948. In May of this year, 1950, the findings were published, covering abnormalities observed under 16 years.
Now, what have these findings been, in terms of generalities? First, that untreated syphilis apparently shortens the life expectancy by 20 percent. Second, that there is a greater involvement of the cardiovascular system and third, that syphilitics without treatment appear to be subject to a higher rate of other types of morbidity. Thus there are more potentially disabling defects among them and they die earlier. This is probably what most people might expect from general knowledge or assumption, but it is important to have the facts documented.
I heartily support the work that has been done, but it does not go far enough. When the third examinations were done in 1948–49, 26 percent of the syphilitics had been lost from observation and 35 percent of the controls. This is not counting known deaths. One of the reasons for selecting Macon county as a study area, aside from its high prevalence rate, was that it seemed remarkably suitable for the study purposes. It had the broad extremes of development of the Negro race, from those connected with Tuskegee Institute to those with the lowest of living standards. Health facilities ranged from a Veterans hospital to nothing, transportation from 3 railway centers and a main highway to inaccessible winter roads. But most of all, the county’s principal industry is agriculture of a type which tends to provide a stable population for a long term study such as this. What became of this third or so that dropped from observation? Were they in the county but just didn’t respond to a written notice? Would they have responded if they could read? Did they stay away because they were no longer interested or were they too ill to come in? Perhaps they had moved out of the county. Some have, I am sure. But if they’ve moved—are they living and well? If they are dead, what was the cause?
These questions are important to the value of the study. There is a nurse in the county whose salary is paid to keep track of these patients but I think more is necessary. Remember, these patients wherever they are, received no treatment on our recommendation. We know now, where we could only surmise before, that we have contributed to their ailments and shortened their lives. I think the least we can say is that we have a high moral obligation to those that have died to make this the best study possible.
This is the last chance in our country to make an investigation of this sort. You may say, if that’s so isn’t the point rather academic. I don’t think so. It may be academic so far as the patient who is treated, but you know even better than I, that you are not yet finding and treating all of the cases. Your casefinding publicity makes a point for the public to “Know for Sure” whether the disease has been contracted. I say it behooves the medical profession to “Know for Sure” what happens if the disease is not treated.
I urge in the strongest possible way that the Public Health Service place a full time male investigator in Macon county whose sole job is to locate those persons who were first selected and examined. Sure, they may have moved, perhaps moved and died, but arrangements can be made for them to be examined wherever they may be, if living. If they’ve died, let’s trace them through vital statistics to see when, where and why. And if humanly possible, arrange for autopsy of those who die in the future.
This matter of autopsies is of tremendous importance. There are, as you know, only two other studies that even remotely resemble this—the one started by Bruusgaard in Norway and the study of Rosahn at Yale. So far, of the 173 deaths recorded for the Alabama group 67 percent have come to autopsy. The correlation of postmortem findings with periodic clinical findings can be done only in the Alabama group. What other way will we ever be able to learn the meaning of our clinical findings?
Once again let me emphasize the importance of this quiet undertaking and urge that steps be taken so that it doesn’t slip through our fingers.
9-18-50
KHJ/mrb
Tuskegee Syphilis Study, HEW Report Documents, Bound Book II, Tuskegee University Archives.
Sidney Olansky, Sr. Surgeon, Public Health Service, Venereal Disease Research Laboratory, Chamblee, Georgia, to Dr. John C. Cutler, Washington, D.C., November 6, 1951
November 6, 1951
Chief, Division of Venereal Disease
U.S. Public Health Service
Federal Security Building (South)
Washington 25, D.C.
Attn: Dr. John C. Cutler
Dear John:
I received your letter of October 22, 1951. Stanley and I have both studied and discussed your outline. We agree wholeheartedly with your premises for the validity of the study, your arguments for the importance of this follow-up, and your recommendations for the clinical examination.
Enclosed is our outline of the Tuskegee project which you have requested, in as much detail as possible at this time. Much of this will merely be repetition of what Dr. Bauer has already received in our progress reports. (Reference is made to letters dated September 24, 1951 and October 18, 1951, especially.)
Please pardon the length of the outline. Some of the details may be more useful than superfluous to any future investigators on this project.
Yours sincerely,
SIDNEY OLANSKY
Sr. Surgeon, USPHS
Director
Encl.—1
CC: Dr. Bauer
Outline of Problems to Be Considered in Tuskegee Study
A. Even though there is real and reasonable doubt as to the original diagnosis of many of the patients, it seems to me that it may be necessary to consider the diagnosis as probably correct and to work on. While malaria may have played a role in false positivity and while other factors may have been operative, the same factor was working in all groups of patients considered—untreated, treated, and controls. Furthermore, the lower level of sensitivity of tests of those days gives good reason to assume that the level of false reactivity was lower than would be expected today.
The very large differences in morbidity of syphilitic and control groups suggests a real difference in the two “universes” with possible economic and social differences which, however, cannot be resolved now.
So regardless of our present feeling, I feel that we must utilize the material available with knowledge that the diagnoses were made by very competent syphilologists, utilizing the best information available at the time.
B. Assuming the diagnostic validity of the material, it is felt advisable to get all the information possible from the material. We have an investment of almost 20 years of Division interest, funds, and personnel; a responsibility to the survivors both for their care and really to prove that their willingness to serve, even at risk of shortening of life, as experimental subjects. And finally, a responsibility to add what further we can to the natural history of syphilis.
Out of what we have, the following avenues of exploration remain:
1. It is assumed that complete studies will be done, i.e., physical and history, with attention to intercurrent illness, administration of penicillin, etc. In other words, a medical school type work-up.
2. When the follow-up worker is assigned, one of the first bits of information obtained may be further study of the progression in the observed and non-observed groups. Compare with Iskrant hypothesis that both are same.
Knowing the type of cardiovascular studies done earlier, it is felt that the same techniques of measurements, etc. should be repeated to observe changes. For the cardiovascular work-up, it is felt that the services of a cardiologist should be secured and that full advantage should be taken of the technical diagnostic measures.
Careful studies of spinal fluid and neuromuscular system are advised. For this the type of work-up to fill the new CNS evaluation forms are recommended so as to get material comparable with that from the research participants.
From this type of work-up it is anticipated that data comparable with the Bruusgaard material may be obtained.
3. Serologic studies relative to spontaneous cure, correlation between STS and clinical, and pathological findings may be productive of much valuable information.
4. The pathologic studies made to date must be gathered together and worked up. Shall Rosahn’s protocol for tabulation be followed.
5. There is much valuable material here for aid in evaluation of the TPI procedure.
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 7, Folder 1951, National Archives–Southeast Region, East Point, Georgia.
Eleanor N. Walker to Dr. John C. Cutler, December 4, 1952
TO: Dr. John C. Cutler
DATE: December 4, 1952
FROM: Eleanor N. Walker
SUBJECT: Study of Untreated Syphilis in the Male Negro, Macon County,
Alabama
It seems to me that after 20 years we have too much of a stake in this study to let it slide now for the sake of a few more dollars. I have never felt that Nurse Rivers was an adequate “policeman” for these people. I know the colored people in the South and one shouldn’t expect 100% effort from any of them unless they are under constant supervision. In a community of this type where everyone knows everybody’s business I can’t see how we could have lost from contact so many of the group if Nurse Rivers had been even moderately interested in perpetuating this study.
I would like to spend several weeks with her and prepare from the records and from whatever other source available, an informative list of the “lost” study individuals and try to locate some of them through a series of letters to the various local health departments. In the case of those residing in Alabama it should be simple to have them located and examined.
The assignment of a young investigator to the County Health Department to absorb some of Nurse Rivers duties doesn’t appear to be the answer, because he is here today and gone tomorrow. Would it be possible to think about tying in more closely with the Institute staff in some way. Certainly something should be done right now to put this study on a firmer foundation if it is determined it should be continued.
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 7, Folder 1952, National Archives–Southeast Region, East Point, Georgia.
Public Health Service to Dear Sir, October 18, 1955
Tuskegee, Alabama
October 18, 1955
Dear Sir:
The Government doctor will be here next week. Be sure to meet him at the time and place listed below that is nearest your home.
Tuesday, November 1, 1955 |
|
Cooper’s Chapel |
8:30 A.M. |
Creek Stand |
9:30 A.M. |
Cross Roads |
10:45 A.M. |
Swanson |
11:30 A.M. |
Hannon |
12:00 NOON |
Robe |
12:30 P.M. |
Armstrong |
12:45 P.M. |
Ft. Davis |
1:15 P.M. |
Cotton Valley |
2:00 P.M. |
Mt. Nebo |
2:30 P.M. |
Wednesday, November 2, 1955 |
|
Nebraska |
8:45 A.M. |
Chesson |
9:45 A.M. |
Prairie Farm Clinic |
10:15 A.M. |
Pinkston’s Store |
10:45 A.M. |
Milstead |
11:30 A.M. |
Bethal Grove |
12:45 P.M. |
Walker’s Chapel |
1:00 P.M. |
Thursday, November 3, 1955 |
|
Simmons’ Chapel |
8:30 A.M. |
Mt. Zion |
9:00 A.M. |
Shiloh |
9:30 A.M. |
McCray’s Chapel |
10:00 A.M. |
Brown Hill |
10:30 A.M. |
Oak Grove |
11:00 A.M. |
Brownville #2 |
11:45 A.M. |
Brownville #1 |
12:30 P.M. |
Pine Grove |
1:15 P.M. |
Mt. Pleasant |
1:45 P.M. |
Friday, November 4, 1955 |
|
Macon County Health Office |
8:30–12:00 |
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 16, Folder Alabama-Miscellaneous, National Archives–Southeast Region, East Point, Georgia.
Eunice Rivers Laurie to Dear Sir, July 16, 1963
July 16, 1963
Dear Sir:
The Public Health Service doctor who was here last fall plans to return to Tuskegee about the 23rd of July for a visit of several weeks. During that time he would like to see you at the Veterans Administration Hospital, if you are able, if not, he will visit you at your home.
I will notify you 2 or 3 days in advance of the exact day on which the doctor will expect you and I will let you know at that time when and where I will meet you to take you to the hospital. Since the examination will take a little time, lunch will be provided at the hospital before you are returned home.
In appreciation of your cooperation during the last 30 years and for your valuable contribution to medical research, you will be presented a cash award. I sincerely hope, therefore, that you will make every effort to see the doctor when you are notified.
Sincerely yours,
Eunice Rivers Laurie, R.N.
Public Health Service
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 16, Folder Alabama-Miscellaneous, National Archives–Southeast Region, East Point, Georgia.
Irwin J. Schatz, M.D., Henry Ford Hospital, Detroit, Michigan, to Donald H. Rockwell, Venereal Disease Research Laboratory, Public Health Service, Atlanta, Georgia, June 11, 1965
June 11, 1965
Donald H. Rockwell, M.D.
Venereal Disease Research Laboratory
Communicable Disease Center
United States Public Health Service
Atlanta, Georgia 30333
Dear Dr. Rockwell:
I have recently read your paper on the Tuskegee Study of Untreated Syphillis appearing in the Archives of Internal Medicine in December, 1964.
I am utterly astounded by the fact that physicians allow patients with potentially fatal disease to remain untreated when effective therapy is available. I assume you feel that the information which is extracted from observation of this untreated group is worth their sacrifice. If this is the case, then I suggest that the United States Public Health Service and those physicians associated with it in this study need to re-evaluate their moral judgements in this regard.
Yours sincerely,
IRWIN J. SCHATZ, M.D.
Head, Section of Peripheral Vascular Disease
IJS:cao
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 8, Folder 1965, National Archives–Southeast Region, East Point, Georgia.
Anne R. Yobs, M.D., to Dr. E. J. Gillespie, June 15, 1965
NOTE—DO NOT USE THIS ROUTE SLIP TO SHOW FORMAL CLEARANCES OR APPROVALS
DATE: 6/15/65
TO: AGENCY BLDG. ROOM
Dr. E. J. Gillespie Buckhead 500
APPROVAL REVIEW PER CONVERSATION
SIGNATURE NOTE AND SEE ME AS REQUESTED
COMMENT NOTE AND RETURN NECESSARY ACTION
FOR YOUR INFORMATION
PREPARE REPLY FOR SIGNATURE OF_____________
REMARKS: This is the first letter of this type we have received. I do not plan to answer this letter.
(Fold here for return)
To
From Anne R. Yobs, M.D.
PHONE BUILDING ROOM
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 8, Folder 1965, National Archives–Southeast Region, East Point, Georgia.
Peter J. Buxtun to Dr. William J. Brown, Chief, Venereal Disease Branch, Communicable Disease Center, November 24, 1968
11/24/68
Dr. William J. Brown
Chief, Venereal Disease Branch
Communicable Disease Center
Atlanta, Georgia
Dear Dr. Brown:
I again am writing you with regard to the study of untreated Syphilis in the male negro. It has been well over a year since I last communicated with you in this regard. In that period of time, I have left the USPHS, and so am no longer informed as to CDC projects.
When we discussed the matter in Atlanta, I told you that I had grave moral doubts as to the propriety of this study. While I could see the justification and propriety of the study at its inception, and even up to the time of the widespread use of penicillin, I could not condone the continuation of this study up to the present day. While I must grant the danger of treating aged syphilitics, and while I am sure medical science has benefitted by the study, I still must advocate the following points:
1.) The group is 100% negro. This in itself is political dynamite and subject to wild journalistic misinterpretation. It also follows the thinking of negro militants that negros have long been used for “medical experiments” and “teaching cases” in the emergency wards of county hospitals.
2.) The group is not composed of “volunteers with social motives.” They are largely uneducated, unsophisticated, and quite ignorant of the effects of untreated syphilis.
3.) Today it would be morally unethical to begin such a study with such a group. Probably not even the suasion of belonging to the “Nurse Rivers Burial Society” would be sufficient inducement.
I earnestly hope that you will inform me that the study group has been, or soon will be, treated.
Very truly yours,
Peter J. Buxtun
1730 Kearny St.
San Francisco
CC:DI
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 6, Folder Buxtun, National Archives–Southeast Region, East Point, Georgia.
Ira L. Myers, M.D., State Health Officer, State of Alabama, to William J. Brown, M.D., Chief Venereal Disease Branch, Public Health Service, March 13, 1969
March 13, 1969
William J. Brown, M.D.
Chief, Venereal Disease Branch
Department of Health, Education and Welfare
Public Health Service
National Communicable Disease Center
Atlanta, Georgia 30333
Dear Dr. Brown:
I have discussed the Macon County Untreated Syphilis Project with Dr. Ruth R. Berrey, the County Health Officer, and she knows of no opposition to the project at this time. She feels that it is not generally known or publicized. She doubts if the Medical Society is aware of its existence but hopes they will be sympathetic with the desires of the Public Health Service.
This matter has been discussed with the State Board of Health and as we discussed at the Advisory Meeting, the Alabama State Board of Health refers this matter to the Macon County Medical Society for its decision regarding continuity. The present officers of the Society are as follows:
Luther Curtis McRae, Jr., M.D., President
Henry Wendell Foster, M.D., Vice-President
Sheridan Howard Settler, Jr., M.D., Secretary Treasurer
I shall attempt to discuss this matter and this action with Dr. McRae later today. You may proceed to make your contacts directly with local officers. Please keep us informed and if a visit is made we will provide someone to go along or meet you there, if possible.
Dr. W. H. Y. Smith is improving and out of intensive care. We are encouraged by his progress.
With kindest personal regards, I am
Sincerely yours,
Ira L. Myers, M.D.
State Health Officer
ILM:fs
[handwritten addendum]
4/16 - Dr. Sencer was advised that Dr. Myers had talked to Dr. McRae and that Dr. McRae was receptive to the idea of bringing the Med. Society “on board” and suggested Mon May 19th for appearance before the Society. WJB
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 1, Folder Ad Hoc, National Archives–Southeast Region, East Point, Georgia.
James B. Lucas, M.D., Assistant Chief, Venereal Disease Branch, Public Health Service, to William J. Brown, M.D., Chief, Venereal Disease Branch, September 10, 1970
Date: September 10, 1970
Subject: An analysis of the current status of the Tuskegee Study
To: William J. Brown, M.D.
Chief, Venereal Disease Branch
1. In recent years the Tuskegee Study has become an increasingly emotionally charged subject. This aura has in large measure prevented a rational appraisal of the situation. It is hoped that these remarks will aid in restoring our prospectives and lead to a reasonable course of future action.
2. Priority—Resources must follow priorities. While some medical knowledge has been gained from this study its volume and quality has been less than gleaned from the preceding Boeck-Bruusgaard study. This is largely because effective and undocumented treatment has been given to the vast majority of patients in the syphilitic group. Most received this therapy in the “happenstance” manner while under treatment for other conditions. The impact of this inadvertent treatment will be almost impossible to assess, but without question the course of untreated syphilis (which the study was supposed to have delineated) has been radically altered. This is not to suggest that some contributions to medical knowledge do not yet lurk in the information gathered to date. However, it must be fully realized that the remaining contribution from this study will be largely of historical interest. Nothing learned will prevent, find, or cure a single case of infectious syphilis or bring us closer to our basic mission of controlling venereal disease in the United States.
3. Probably the greatest contribution that the Tuskegee Study has made and can continue to provide has been documented sera for study in our laboratory. Without those sera the problem of evaluating new serologic tests becomes much more difficult and the results less certain. In a great measure the development and our endorsement, of the FTA-ABS test rested on Tuskegee sera. The collection of future specimens hardly requires a special unit for that purpose.
4. To point up how obtunded the medical findings are currently one must only look to the special study carried out in 1967 by Dr. J. Lawton Smith. We permitted him to study these patients, but insisted on a “blind” study so he would not know who were syphilitic and who were controls. All available patients were rather elaborately studied for neurologic and ophthalmologic defects. When Dr. Smith presented his clinical findings we broke the code. Absolutely no correlation was discovered between the pathology uncovered in his study and the status of the patients.
5. All of this simply serves to point out that neither major medical revelations nor program benefits are likely to be forthcoming irregardless of who supervises the study, and thus the overall priority of the Tuskegee Study from these viewpoints is relatively low.
6. Moral Obligation—Any question of termination hinges upon an obligation to the remaining syphilitic patients. This is both an implied and expressed obligation. The long continued assignment of Mrs. Laurie and now Mrs. Kennebrew to Tuskegee demonstrates our good faith and sincerity. The annual examination of survivors and referral of those with significant physical findings also clearly demonstrates our position and good will. Several recent pieces of correspondence indicate that termination is now desirable since many of the patients are now dead or that the deaths of those remaining will bring the study to a natural termination within the next few years. Certainly we are obligated to maintain our present level of observation as long as a significant number of patients remain alive.
7. A point may be reached where the number of survivors no longer justifies continued surveillance, but this might expose the program to justifiable criticism on grounds of the moral issue. What number of survivors would justify such a decision?
8. A more definite answer can be made concerning natural termination. One merely needs to know the current number of survivors, their average age, and have access to a life table for non-white males to definitely determine the number who will be living for any future year. Currently 149 syphilitics are alive and their average age is 71. In five years, 101 can be expected to still be alive. In 1980, sixty-eight of the syphilitics will still be living. In the years that follow the annual mortality will probably be no greater than 9–10 percent so that approximately 25 individuals may reasonably be expected to survive yet another decade (1990). This exercise simply points out that natural termination in the forseeable future is an unlikely event.
9. It is also suggested that a lack of continuity on the part of VD personnel is a valid excuse for termination. I would like to point out that this study has not had a fulltime person (other than Nurse Laurie) handling this study for a great many years. Periodically medical officers have become interested or were assigned for short periods to the project, but there has been very little medical continuity since the inception of the study. It is true that Mrs. Price has handled the record keeping for many years, but this was only a small part of her duties. She is still readily available as a consultant should questions concerning the records arise. In essence then, there has long been a lack of medical continuity and the need for this now is debatable at best.
10. Due to our present financial duress it hardly seems feasible to commit $150,000 over a three or four-year period or even hire a GS-14 pathologist to oversee the study. It has also been suggested that a summary monograph obstensively authored by appropriate experts be prepared. This raises several questions. Why outside experts, who have not been involved in the study? Such experts may very well prefer not to be associated with this study because of its sensitive nature. In any event there remains very little expertise on late syphilis.
11. More importantly, what would be the value of an elaborate and expensive monograph? The “green book” certainly adequately covers the pertinent aspects of late syphilis. Distribution of such a monograph might well cause more harm than good to the program.
12. A much more realistic approach would involve the preparation of a series of “in-house reports.” Any findings of special interest or importance might then be published in appropriate journals as has been done in the past.
13. In summary, three distinct courses of action appear to be open:
(1) The study may be terminated. This is clearly not justified from the foregoing discussion. In fact the assignment of a new nurse already indicates our dedication to this study and its subjects.
(2) The study may be continued along its present lines with periodic clinical observation and serologic surveillance. On occasion the publication of any new significant finding may be considered. This can be handled by the present staff in clinical research with occasional supplementation by VDRL or VD Branch medical officers.
(3) A special unit with a fulltime director may be created. The costs, value and long term nature of this option have been discussed.
14. In my opinion, when all factors are considered, the second option appears to be the wisest course of action.
James B. Lucas, M.D.
Assistant Chief
Venereal Disease Branch
State and Community Services Division
U.S. Department of Health, Education and Welfare, Tuskegee Syphilis Study Ad Hoc Advisory Panel, Box 2, Ad Hoc Committee Folder, MSC 264, National Library of Medicine, History of Medicine Division, Bethesda, Maryland.
Don W. Printz, M.D., Chief, Clinical Research Activity, Venereal Disease Branch, Center for Disease Control, to Mrs. Elizabeth M. Kennebrew, Macon County Health Department
April 27, 1972
Mrs. Elizabeth M. Kennebrew
Macon County Health Department
Tuskegee, Alabama 36083
Dear Mrs. Kennebrew:
From time to time it is customary to review the duties and responsibilities of our field assignees who serve principally with state and local health departments. I notice I have not corresponded with you about this since I assumed the position of Chief, Clinical Research Activity.
My predecessor, Dr. Arnold L. Schroeter, was especially pleased with your new system of record keeping for patients being followed in Tuskegee. I too feel it is imperative with the average age of the patients involved well in excess of 70 years that we maintain as close contact with them as possible. Therefore, I suggest you make personal contact with every patient being followed in the Tuskegee area at least once every 2 months. The excellent rapport which Mrs. Laurie had with these patients cannot be achieved overnight, but I believe a regular system of visitation will aid you in doing this. In addition, patients who are hospitalized for any reason should be followed daily with visits. Because of the great age of the patients now in the study, the regular physical examination, with good patient participation, will loom even more important in the future.
I envision at least 80 percent of your working time, that is 4 out of 5 working days, should be spent working exclusively with the Tuskegee patients. It may be that from time to time during illness of other nurses or during exceptional circumstances, such as epidemics, you may have some duties assigned to you by the Macon County Health Department. However, these should be the exception rather than the rule. I feel to justify the Federal Government paying 100 percent of your salary we should expect you to devote 80 percent of your time exclusively to work with the Tuskegee patients on our Venereal Disease Branch sponsored program. The remaining 20 percent of your time should be devoted to venereal disease control programs in the Macon County area in cooperation with and with direction from VD control officials of the State of Alabama.
Sincerely yours,
Don W. Printz, M.D.
Chief, Clinical Research Activity
Venereal Disease Branch
State and Community Services Division
JOB DESCRIPTION OF “PROGRAM REPRESENTATIVE” WITH TUSKEGEE STUDY
The “Tuskegee Study” is a research study of Negro males, all of whom resided in the Macon County, Alabama area when the study began in 1933. Participants of the project fall in one of two categories: (1) untreated, acquired syphilitics; (2) nonsyphilitic controls. Average age of participants is approximately 74. This project is being conducted by the Venereal Disease Program, Division of Special Health Services, United States Public Health Service.
The public health nurse, or “program representative,” is to provide specialized nursing services to a group of study patients, most of whom reside in Macon County and surrounding Bullock, Lee, Russell and Tallapoosa Counties.
Long-range nursing care planning will include following the patients for life; establishing and maintaining good rapport with patients and their families; promoting optimal health; maintaining present caseload and continuing caseholding efforts of “lost” patients; making preparations and assisting (Communicable Disease Control) public health physicians with routine physical examinations; and obtaining permission for autopsy from family when death occurs.
Regular home visits should be made at least every three months on each patient; more often, if necessary.
Advice and assistance should be provided in Venereal Disease other health problems and problems not related to health, if possible and guidance patient’s condition should be kept for information of Communicable Disease Control physicians.
Families are requested to inform nurse when serious illness or death occurs; follow-up care, as deemed necessary is initiated.
When necessary, patients are to be taken by automobile to private physicians for medication and/or examination.
Inquiries should be made of friends, relatives and older citizens of the communities as to lead where abouts of inactive participants as caseholding efforts.
When not needed on the V-D project the nurse will assist with the general Public Health Nursing program of Macon County.
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 12, Folder Personnel Arrangements, National Archives–Southeast Region, East Point, Georgia.
SDS Leaflet
SYPHILIS STUDY “DEFENSIBLE”?
DAVID SENCER, DIRECTOR OF CDC (Center for Disease Control) SAYS “YES!!”
SDS (Students for a Democratic Society) SAYS “NO!!”
A 40-year-old syphilis research program, otherwise known as the “Tuskegee Study,” has taken the lives of 150 black men in Alabama. These men could have been spared their sufferings from the dreaded disease, syphilis: however, they were among over 400 men who were denied treatment by the government “in the interest of science.” These men were told only that they had “bad blood”—but the real nature of the disease was not explained.
Such acts of racist genocide must be stopped NOW !”
DEMONSTRATE: Saturday, August 12, 1:00 PM, outside the Public Health Service Building at 60 Eighth St. NE.
PICKET the CENTER FOR DISEASE CONTROL: Thursday, August 17 at 3:00 PM. If you need a ride, or for more information, call 373-0713 or 875-5350.
WE INVITE ALL GROUPS AND INDIVIDUALS TO JOIN US IN DEMANDING (1) $600,000 REPARATIONS FOR FAMILIES OF VICTIMS, AND (2) SENCER RETRACT HIS STATEMENT THAT THE STUDY WAS “DEFENSIBLE.”
Join us—TO PROTEST this RACIST STUDY—and BUILD a LASTING MOVEMENT against RACISM
(See other side for the Anti-Racism Bill, sponsored by sds, which we want to bring to Miami to present to the Republicans).
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 8, Folder 1972, National Archives–Southeast Region, East Point, Georgia.
Robert H. Huffaker, Biohazards Control Officer, Memorandum for the Record, August 24, 1972
TO: Memorandum for the Record
DATE: August 24, 1972
FROM: Biohazards Control Officer
SUBJECT: Implementation of Emergency Plans; Picketing by SDS
Late on Thursday, August 10, 1972, the CDC Executive Office received copies of a handbill (exhibit 1) printed by the Students for a Democratic Society (SDS) which announced plans to “Demonstrate August 12, 1972, in front of the PHS building at 60 Eighth Street N.E.” (this houses FDA) and to “Picket CDC on Thursday, August 17, at 3:00 p.m.”
What followed provided a test of CDC disaster preparedness emergency plans. (The formal plans were never referred to during the “exercise”; probably because it was felt that decisions and actions had to be applicable to the specific situation and “cook-book” guides would not be valuable. Probably the greatest value of the formal plan was in preparing the people who compiled them to make decisions during an actual emergency situation).
Friday, August 11, 1972—The following were notified of the planned picketing:
FBI Atlanta Office |
Mr. Stan Maurio |
DeKalb County Police |
Sgt. Roderick |
HEW—Washington |
Mr. Don Dick |
U.S. Attorney’s Atlanta Office |
Mr. Gene Madori |
U.S. Magistrate’s Atlanta Office |
Mr. Al Chancey |
FDA—Atlanta Office |
Mr. Dawson (to warn them that they were scheduled to have a “demonstration.”) |
All chiefs of programs, offices, etc. of CDC. Each was contacted by telephone and told:
1. That SDS was planning to picket, and the date and time.
2. That the information was provided to counteract rumors and enable them to answer questions.
3. That the information was not an invitation from management for employees to participate and that it was expected there would be business as usual.
Later on, the question of employee participation in the demonstration was raised, and it was decided that each inquirer should be sent to personnel (Dr. George Glover) where they would be shown the applicable rules and regulations. The decision to participate would have to be made by each individual. This information should have been given in the initial contact with the supervisors but was not. No written statement was made by CDC to our personnel regarding the picketing. NMAV should have been contacted but was not.
Monday, August 14 - Reports from FDA were that seven people had come to demonstrate on Saturday; these went into the hippy area and got four recruits and returned. The eleven presented demands to a closed building and hung Dr. Sencer in effigy. (The body was cut down for reuse.)
Plans were made to secure the Clifton Road facility. Buckhead and Lawrenceville were informed but were to take no special action. Atlanta City Police were asked to “look in” on Buckhead. Because of the proximity of the Chamblee facility to IRS (known to be demonstration prone), it was decided to close and lock gates in the perimeter fence on Thursday afternoon. One of these gates is card controlled, and an Engineering Branch man was to operate the gate for non-cardholders.
Tuesday, August 15 - Atlanta Police Intelligence said that an appeal to help picket had been placed in the “Great Speckled Bird.” According to the Atlanta Police, the FBI felt there might be a large gathering at CDC on Thursday, August 17.
Wednesday, August 16
Messrs. Gunn and Paine stated that CDC has “proprietorial interest” in the facility and that DeKalb Police have jurisdiction on and in the grounds and buildings. (This point had been researched earlier for another reason.)
Sgt. Brooks (DeKalb County Police) came to Clifton Road and went over the buildings and security plans.
Thursday, August 17
All gates to the parking area were locked just after 1:00 p.m. A guard remained at the upper gate with the key and to admit cars with CDC stickers and also to let traffic out. All building doors were locked at this time with the exception of the doors on the basement level of B (Clinic entrance) and the main front entrance of Building 1. These doors were attended by guards. All other doors “above” the fence that could be opened from the inside were attended by personnel from Engineering Services. Signs were made asking people to use the front door, and these were posted on locked doors.
Captain James Stanley, in charge of the DeKalb County Police, made his headquarters in the front lobby.
Dr. Rafe Henderson invited SDS representatives to come to CDC and discuss the Tuskegee Study. Four people came and talked with him for 21/2 hours, and when they left they appeared to be satisfied with the information. This discussion was probably very important in aborting the picketing.
CDC people behaved very well; there was extra traffic to the cafeteria during the time scheduled for picketing but little loitering and no interference with guards, etc.
NO PICKETS CAME.
A complaint was received that the basement door of Building 4 could not be opened from the inside when locked. This will be changed by installing a crash bar.
Increased security will be continued at night; two of the three outside doors which have often been blocked open will be secured as it is impossible to control access to the facility while these doors are unlocked. The third back door of CDC is open until midnight. Further evaluation of building security must be made and deficiencies corrected as soon as possible.
Friday, August 18
The Information Office had reports of picketing of the Regional Office in Chicago by SDS. In addition, the syphilis study in Chicago is getting very bad press. None of this has appeared on the wire service as yet.
Robert H. Huffaker, D.V.M.
Centers for Disease Control Papers, Tuskegee Syphilis Study Administrative Records, 1930–80, Box 8, Folder 1972, National Archives–Southeast Region, East Point, Georgia.
Charles G. Gomillion to Susan M. Reverby, October 12, 1994
September 20 1994
Dear Dr. Reverby:
I was in Tuskegee during the period of the “Tuskegee Syphilis Experiment,” and I was aware that Miss Eunice Rivers was a nurse employed in the program, but, like many other citizen in Macon County, I thought that the persons being treated by the physicians and nurses were being treated in order to cure them of their ailment. We did not know that the program was a scientific/medical experiment until we read about it in the newspapers. So, we made no inquiries about it. We were glad that those affected with syphilis were being treated.
Miss Rivers might have been a dues-paying member of the Tuskegee Civic Association, but I do not remember her as having been an active participant on any program, or a member of any committee.
I regret that I was very ignorant of what was actually being done to the syphilitic persons in the program. After the suit was filed by Mr. Fred D. Gray, I was informed that a Mr. Pollard, who was an officer in the Macon County Democratic Club, of which I was president, was one of the syphilitic participants. For several years, he and I had worked together in a program of civic and political education. He was the precinct leader for Notasulga [just outside Tuskegee]. At the time, I did not know Mr. Pollard was a participant in the “health” program. He never mentioned it to me. I have not talked with him about it.
Sincerely,
Charles G. Gomillion
October 12, 1994
Dear Ms. Reverby:
Before the newspapers reported that the Federal health project on which Miss Eunice Rivers worked was a research project, I had heard that those who were being “treated” for “bad blood” had syphilis. I think that few persons in the TCA [Tuskegee Civic Association] who talked with me about the project thought as I did, namely, that the project was one to improve the health of the participants, and reduce the mortality rate.
In the ’30s, ’40s, and 50s, the TCA was almost as active in doing what it could to improve the public health and educational opportunities and services as it was in increasing voter registration and voting. If any of the officials in the TCA had known that the syphilitic persons did not know that the project was a research project, and that some (half) of those were not being treated to improve their health, we (the TCA) would have engaged in some kind of action. There might have been some persons in the community, in addition to Miss Rivers, who knew that the project was a research project, but they did not talk with me about it.
I do not know how Miss Rivers was treated in the community by those who knew that the project was a research one, after the newspapers reported the nature of the project, and after Mr. Fred D. Gray became involved, I heard that some blamed Miss Rivers for having participated in the project, if she knew that some of the syphilitic patients did not know that they were not being given health-improving drugs.
Sincerely,
Charles G. Gomillion
Charles Gomillion was a sociology professor at Tuskegee University and the longtime head of the Tuskegee Civic Association which led the struggle for voting and other civil rights in Tuskegee. Permission granted by Lawrence A. Sims, grandson and executor of the Estate of Charles G. Gomillion.