Your lifestyle choices are incredibly important when you have type 2 diabetes. Eating wholesome, nutritious foods and staying physically active are cornerstones of managing your blood glucose. Some people, particularly soon after diagnosis, can manage their diabetes solely by making changes to their lifestyle like eating healthy foods and exercising regularly. They probably lose a few pounds, too. It’s inspiring that these healthy choices can be so impactful! (You can find out more about eating healthy foods and moving more in Part 4.)
Most people with type 2 diabetes need to take medications, in addition to making lifestyle changes, to manage their blood glucose. If you need to take a diabetes medication, you are certainly not alone.
No single medication is used to treat everyone with type 2 diabetes. Instead, quite a few classes of medications are used to treat diabetes, and each class features different brands. Medications include pills you take by mouth, medications you inject once a day or once a week, and of course, insulin.
New medications for type 2 diabetes are constantly being developed; many more medications are available today than, say, 20 years ago. Some old medications work incredibly well, and others have fallen out of favor because of side effects.
This chapter describes each type of medication — how it works, how you take it, and possible side effects and precautions.
Besides medications specifically targeted at blood glucose, you might take medications for your blood pressure and cholesterol. You also find out about these commonly used pills in this chapter. And don’t forget surgery: It’s now a recommended treatment option for some people with type 2 diabetes.
Why Do I Need to Take Medication?
People with type 2 diabetes have several things going on in their bodies with blood glucose, insulin, and other hormones:
People with type 2 diabetes may not make as much insulin as they used to — or none at all.
People with type 2 diabetes may not be as sensitive to the hormone insulin (called insulin resistance) as people who don’t have diabetes.
Other hormones, called incretins, affect how much insulin the body releases and help control blood glucose. For some people with type 2 diabetes, a hormone called glucagon-like peptide-1 (GLP-1) may not work properly and may not stimulate the pancreas to make enough insulin.
People with type 2 diabetes may release too much glucose from their livers, causing blood glucose to rise.
All these things can cause high blood glucose, which can cause short- and long-term health problems. (Read more about the complications of type 2 diabetes in Chapter 8.) Medication can target these different problems to help lower your blood glucose. In this chapter, we describe how each medication works. Some people with type 2 diabetes may need to take insulin because their bodies are no longer responsive to blood glucose–lowering medications or because their bodies don’t make any insulin at all.
Your diabetes medication regimen can change over time. You may take a drug like metformin at the beginning, but then need to add or change medications to keep your blood glucose in your target range later on. (Remember: Most people are aiming for an A1C of 7 percent or less.) Or you may experience side effects that prompt medication changes. You may also need to take insulin at diagnosis or several years down the road. It totally depends on the individual!
Your healthcare team is your number-one resource for medications. You’ll work with your nurse, doctor, pharmacist, physician assistant, or diabetes educator to troubleshoot problems or adjust doses.
Never stop taking a medication because you think it’s not working or because of annoying side effects (an unintended effect, such as diarrhea or flatulence, of taking a certain drug). Instead, call your provider and tell her what’s going on. Don’t be shy about bringing up concerns like bowel movements, changes in mood, or any other concern. All drugs can have side effects, although some may be more severe than others.
Know the names, doses, and instructions for each medication you take. If you’re like most people, you’ll probably need to write them down. Don’t be afraid to ask your provider or pharmacist for these details each time you see her.
Pills for Type 2 Diabetes
The majority of medications for type 2 diabetes are oral medications, meaning they’re in pill form. Some have been around for decades, and others have recently been approved by the Food and Drug Administration (FDA). Pills for type 2 diabetes fall into nine major classes, which is just a fancy way of saying that these groups of medications work in similar ways. Within each class, there are usually generic and brand-name versions of medications in the class. You’ll also find combination pills that combine two different medications into one dose.
Ask your provider about potential side effects whenever you start taking a new medication. Then keep an eye out for these problems and call your doctor if you notice anything out of the ordinary.
Tell your provider if you’re thinking about becoming pregnant, because some type 2 diabetes medications are not recommended during pregnancy.
Supplements, including vitamins or herbal remedies, and certain foods can interfere with your medications. Over-the-counter medications can also impact prescription drugs. Tell your provider about any supplements or over-the-counter medications you’re currently taking and how you normally take them with meals.
Table 6-1 lists the oral medications for type 2 diabetes. The following sections cover these medications in greater detail.
Improves sensitivity to glucose. Blocks the release of glucose from the liver.
Metformin
Glucophage
Sulfonylureas
Stimulates your body to produce more insulin. Helps to lower your blood glucose after meals.
Glimepiride
Amaryl (and various generics)
Glipizide
Glucotrol, Glucotrol XL (and various generics)
Glyburide
Micronase, DiaBeta, Glynase PresTab (and various generics)
Meglitinides
Stimulates your body to produce more insulin.
Repaglinide
Prandin
Nateglinide
Starlix
Dipeptidyl-peptidase 4 (DPP-4) inhibitors
Keeps the blood glucose–lowering hormone glucagon-like peptide-1 (GLP-1) in your body.
Sitagliptin
Januvia
Saxagliptin
Onglyza
Linagliptin
Tradjenta
Alogliptin
Nesina
Sodium-glucose cotransporter 2 (SGLT2) inhibitors
Blocks glucose from being reabsorbed by the kidneys. Helps your body excrete excess glucose through your urine.
Canagliflozin
Invokana
Dapagliflozin
Farxiga
Empagliflozin
Jardiance
Alpha-glucosidase inhibitors
Slows the digestion of the carbohydrates you eat.
Acarbose
Precose (and various generics)
Miglitol
Glyset (and various generics)
Thiazolidinediones (TZDs)
Improves sensitivity to glucose.
Pioglitazone
Actos
Rosiglitazone
Avandia
Bile acid sequestrants
Binds to bile acids in the intestines to lower blood glucose and cholesterol.
Colesevelam
Welchol
Dopamine-2 agonist
Lowers blood glucose in some people with type 2 diabetes.
Bromocriptine
Cycloset
Biguanides
Biguanides improve the body’s sensitivity to insulin and block the release of glucose from the liver. Biguanides include the most commonly prescribed medication for type 2 diabetes: metformin. Yes, you’ve probably heard this name before. There’s a reason it’s popular: It’s safe, effective, and inexpensive for many people.
Metformin is often the first medication prescribed to patients diagnosed with type 2 diabetes. And it can even be prescribed to prevent diabetes in people at risk for the disease (with a diagnosis of prediabetes).
Metformin was approved in the United States in the 1990s under the brand name Glucophage. Now, the generic form, called metformin, is readily available. You take metformin as a pill, usually two times a day. It’s also available as a liquid. Glucophage XR is an extended-release version that is also available generically.
Metformin doesn’t improve your body’s ability to make insulin, so it’s unlikely to cause episodes of low blood glucose, which is a good thing. It does have some side effects; the most common is diarrhea or loose stools. Other side effects like nausea can occur, too. Tell your healthcare provider about any side effects so she can work with you to adjust the dose or change medications.
A rare but serious side effect of metformin in certain patients is called lactic acidosis, which can cause muscle pain and weakness and other symptoms. People with severe kidney disease should not take metformin.
Ask your provider about vitamin B12 deficiency if you’ve been taking metformin for a long time. He may measure your B12 levels and, if they’re low, recommend taking a vitamin B12 supplement.
Sulfonylureas
Sulfonylureas help you make more insulin and lower your blood glucose after meals. Sulfonylureas include glimepiride (Amaryl and various generics), glipizide (Glucotrol, Gluctorol XL, and various generics), and glyburide (Micronase, DiaBeta, Glynase PresTab, and various generics).
Sulfonylureas were first approved in the 1950s, and they’re often taken once or twice a day.
Each type of sulfonylurea has different dosing, side effects, and interactions with other drugs. Sulfonylureas stimulate your body to produce insulin, so they can cause low blood glucose. Some of the most common side effects across all sulfonylureas are episodes of low blood glucose, weight gain, and skin rashes.
Meglitinides
Meglitinides help you make more insulin and lower your blood glucose. They include repaglinide (Prandin) and nateglinade (Starlix). They’re similar to sulfonylureas but faster acting.
Repaglinide was approved in 1997 and Nateglinide was approved in 2000. Meglitinides work quickly and for about 4 hours. They’re taken three times a day, just before meals.
Meglitinides can cause episodes of low blood glucose, weight gain, nausea or vomiting, and headaches.
Dipeptidyl-peptidase 4 (DPP-4) inhibitors
DPP-4 inhibitors work by keeping the “helpful hormone” GLP-1 around in your body. GLP-1 naturally lowers blood glucose, but your body breaks down GLP-1 quickly. DPP-4 inhibitors stop that breakdown and lower blood glucose. DPP-4 inhibitors include sitagliptin (Januvia), saxagliptin (Onglyza), linagliptin (Tradjenta), and alogliptin (Nesina).
Sitagliptin was the first DPP-4 inhibitor approved in the United States in 2006. DPP-4 inhibitors are usually taken once a day.
DPP-4 inhibitors can cause side effects like upper respiratory infections, sore throats, and headaches. They may also cause joint pain that is severe and disabling. And they may cause inflammation of the pancreas, which can cause gastrointestinal symptoms like pain in the abdomen, nausea, or vomiting. Tell your healthcare provider if you’ve noticed any of these side effects.
Incretins are a group of hormones that signal the body to release insulin after eating. Scientists have developed medications that target these hormones for people with type 2 diabetes. Two medications, DPP-4 inhibitors (pill) and GLP-1 agonists (injectable), work by regulating these hormones.
Sodium-glucose cotransporter 2 (SGLT2) inhibitors
Sodium-glucose cotransporter 2 (SGLT2) inhibitors work differently from the medications covered earlier. They block your kidneys from reabsorbing glucose into your bloodstream and help you excrete excess glucose through your urine. In this way, SGLT2 inhibitors lower blood glucose. They can also help you lose weight. Also, SGLT2 inhibitors could benefit patients at a high risk for cardiovascular disease. These medications include canagliflozin (Invokana), dapagliflozin (Farxiga), and empagliflozin (Jardiance).
Canagliflozin was approved in 2013; dapagliflozin and empagliflozin were approved in 2014. They’re taken once a day.
SGLT2 inhibitors can cause urinary tract and genital yeast infections and increased urination leading to dehydration. Canagliflozin and dapagliflozin carry a risk for kidney injury. In rare cases, canagliflozin causes an increased risk of leg and foot amputations, according to two large clinical trials.
Alpha-glucosidase inhibitors
Alpha-glucosidase inhibitors also work a little differently from other medications. They slow down your digestion of carbohydrates during meals and lower blood glucose. They include acarbose (Precose and various generics) and miglitol (Glyset and various generics).
Alpha-glucosidase inhibitors were approved in the mid-1990s. They’re taken three times a day at the beginning of each meal.
Side effects include gas, stomach pain, and diarrhea. They can also contribute to episodes of low blood glucose, and because these medications can slow the breakdown of sugars such as fruit juice, always use a glucose product such as glucose gel to treat symptoms of hypoglycemia.
Thiazolidinediones (TZDs)
Thiazolidinediones (TZDs) make you more sensitive to insulin and lower blood glucose. They include pioglitazone (Actos) and rosiglitazone (Avandia).
TZDs were approved in the late 1990s. They’re taken once or twice a day.
Side effects of TZDs have made them less commonly prescribed, particularly rosiglitazone. In 2010, the FDA imposed restrictions for prescribing rosiglitazone because of concern over increased cardiovascular risk, although those restrictions were lifted in 2013. Rosiglitazone may also increase the risk of bone fractures. Pioglitazone may increase the risk of bladder cancer; people with a history of bladder cancer should not use it. Other side effects include headache, sore throat, and back pain.
Bile acid sequestrants
Bile acid sequestrants bind to bile acids in the intestinal tract and lower blood glucose and cholesterol. There is one with FDA approval called colesevelam (Welchol).
Side effects include gas, constipation, nausea, diarrhea, stomach pain, and weakness or muscle pain.
Dopamine-2 agonists
Dopamine-2 agonists lower blood glucose in some people with type 2 diabetes, although how they work is unclear. One medication, bromocriptine (Cycloset), is FDA approved for this use.
Side effects include dizziness, nausea, and fatigue.
Combination pills for type 2 diabetes
Your provider may recommend a combination pill if your body needs more help lowering blood glucose. A combination pill is handy because you only need to take one, versus two or more pills, at a time. Some common examples of combination pills include
Metformin and glipizide (Metaglip)
Metformin and glyburide (Glucovance)
Metformin and sitagliptin (Janumet and Janumet XR)
Metformin and linagliptin (Jentadueto and Jentadueto XR)
Metformin and repaglinide (Prandimet)
Metformin, extended release, and saxagliptin (Kombiglyze XR)
Metformin and alogliptin (Kazano)
Metformin, extended release, and dapagliflozin (Xigduo XR)
Metformin and canagliflozin (Invokamet and Invokamet XR)
Metformin and empagliflozin (Synjardy and Synjardy XR)
Metformin and pioglitazone (ActosPlus Met and ActosPlus Met XR)
Metformin and rosiglitazone (Avandamet)
Dapagliflozin and saxagliptin (Qtern)
Empagliflozin and linagliptin (Glyxambi)
Glimepiride and pioglitazone (Duetact)
Glimepiride and rosiglitazone (Avandaryl)
Alogliptin and pioglitazone (Oseni)
Injected Medications for Type 2 Diabetes (Besides Insulin)
Pills aren’t the only option for people to lower their blood glucose (see the preceding section). Now patients have access to injected medications (other than insulin), which are injected under the skin with a needle. This is different from a pill that you pop in your mouth.
There are two non-insulin classes of injected medication for type 2 diabetes: GLP-1 agonists and amylin analogs.
Table 6-2 lists the injected medications for type 2 diabetes. The following sections cover these medications in greater detail.
TABLE 6-2 Injected Medications for Type 2 Diabetes
Drug Class
How It Works
Generic Name
Brand Name
Glucagon-like peptide-1 (GLP-1) receptor agonists
Mimics the action of the incretin hormone GLP-1. Stimulates your body to produce more insulin. Slows down how quickly your stomach empties.
Exenatide
Byetta
Extended Release Exenatide
Bydureon
Liraglutide
Victoza
Dulaglutide
Trulicity
Lixisenatide
Adlyxin
Amylin analogs
Mimics the action of the hormone amylin. Slows down how quickly your stomach empties. Suppresses your liver from releasing glucagon, a hormone that moves glucose into your bloodstream.
Pramlintide
Symlin
GLP-1 agonists
Glucagon-like peptide-1 receptor agonists (wow, that’s a mouthful) are otherwise know as GLP-1 agonists. They’re also sometimes called incretin mimetics because they mimic the action of the incretin hormone GLP-1, which helps lower blood glucose. GLP-1 agonists help your body make more insulin and slow down how quickly your stomach empties so your blood glucose doesn’t rise as rapidly. They may also make you less hungry and encourage some weight loss. GLP-1 agonists include exenatide (Byetta), liraglutide (Victoza), extended-release exenatide (Bydureon), dulaglutide (Trulicity), and lixisenatide (Adlyxin). Victoza can be used to reduce the risk of heart attack, stroke, and other cardiovascular events in adults with type 2 diabetes and at high risk for cardiovascular disease.
Exenatide received FDA approval in 2005. You inject GLP-1 agonists using a pre-dosed pen. Depending on the medication, you may inject twice a day, once a day, or once a week.
Side effects include weight loss, nausea and vomiting (and resulting dehydration), episodes of low blood glucose, kidney problems, and inflammation of the pancreas. Tell your healthcare provider if you’ve had pancreatitis, gallstones, a history of alcoholism, high triglycerides, or kidney problems.
Whether you’re starting a new medication or just can’t remember, don’t be afraid to ask your healthcare provider why you’re taking it. Knowing the reasons why you take a specific medication may help you remember to take it — or just feel more empowered about your actions.
Amylin analogs
Amylin analogs mimic a hormone called amylin that the body naturally produces along with insulin. Pramlintide (Symlin) is a manufactured version of this hormone. Some people with type 2 diabetes don’t make enough insulin or enough amylin. Pramlintide lowers blood glucose by slowing how fast your stomach empties and suppressing your liver from releasing a hormone called glucagon, which puts glucose into your bloodstream. It may also encourage you to eat less because you feel more full at meals.
Pramlintide received FDA approval in 2005 for people with type 1 or type 2 diabetes who use insulin. You inject pramlintide using a disposable pen during meals. It does not replace insulin. It’s helpful for people who need something beyond insulin to help control their blood glucose.
Side effects include episodes of low blood glucose, nausea, vomiting, stomach pain, and headache.
All About Insulin
Insulin is that all-important hormone that helps us get energy from the foods we eat. Insulin does that by letting glucose into cells. Without insulin, glucose stays in the bloodstream and leads to high blood glucose. High blood glucose can make you feel crummy in the short term, but it can also lead to long-term complications like heart disease, stroke, and kidney disease.
Insulin is also a medication for type 2 diabetes. We’ve put the topic of insulin into its own section in this chapter because there is a lot of information to cover. You find out the basics of insulin therapy, types of insulin, and how it’s delivered and stored.
There is not one single reason why people with type 2 diabetes take insulin. Some people need to take insulin because changes to their foods, physical activity, or medications cannot lower their blood glucose. Some people need to take insulin because they’re allergic to other medications. Some people may take insulin when they become pregnant.
There also is not one single time when people with type 2 diabetes take insulin. Some people take insulin when they’re first diagnosed with type 2 diabetes. Some people take insulin after they’ve had diabetes for years or decades. Some people with type 2 diabetes may never need to take insulin.
Never look at starting insulin as a failure. It is not a judgment. It is not good or bad. Instead, taking insulin is just doing what you need to take care of your body.
Insulin 101
Insulin is a naturally occurring hormone in your body. However, insulin also refers to the man-made, manufactured medication that people with diabetes use in order to survive and live healthy lives.
For a person without diabetes, the body produces insulin naturally. It releases a low, background level throughout the day and night, as well as bursts of insulin during meals to manage those carbs! A person without diabetes doesn’t feel or experience a thing related to insulin. It just happens as part of the body’s everyday workings. The body naturally releases insulin to keep blood glucose within a range of about 60–100 mg/dL while fasting and 140 mg/dL or less after eating.
Insulin therapy
People with diabetes who take insulin are trying to mimic the body’s natural way of releasing insulin. However, it’s not as straightforward as you might expect. It takes special formulations, delivery, and timing of insulin to get close.
Insulin therapy is a fancy name for giving yourself insulin. Insulin therapy may require one or several different forms of insulin to simulate the background release and bursts of insulin that naturally occur in the body of people without diabetes. Insulin comes in different types, mixtures, and strengths. You inject this insulin at different times too. The way you inject insulin can also vary; you may need to use a needle, pen, pump, or inhaler.
Basal (background) and bolus insulin therapy
Basal insulin mimics the background level of insulin in the body. It’s the steady, low stream that occurs between eating during the day and while you’re sleeping at night. Basal insulin is an intermediate- or long-acting insulin that is absorbed slowly.
Bolus insulin mimics the bursts of insulin that occur in your body. You’ll need bolus insulin when you eat something and you need to process those carbohydrates for energy. This is called a mealtime bolus. It is an extra amount of insulin taken to cover an expected rise in blood glucose.
Some people with type 2 diabetes need just basal insulin, or that steady, low background level. For example, you may take basal insulin in the morning or at night or both. Some people with type 2 diabetes need just bolus insulin, or those short bursts. Still others need both basal and bolus insulin therapy.
Types of insulin
People with diabetes have been able to inject insulin since the 1920s when scientists began extracting insulin from the pancreases of cows and pigs. Phew, we’ve come a long way in the last century! Since the 1980s, pharmaceutical companies have been able to manufacture synthetic human insulin.
Nowadays, two groups of injected insulin are available: synthetic human insulin and analog insulin. Within these two groups of insulin, there are different types that have varying characteristics regarding when they start to work, when they peak, and how long they last.
Hopefully, your eyes haven’t started to glaze over yet, because there is plenty more information to cover about insulin. It may seem like a lot to digest at first, but you’ll soon get the hang of it. Remember: Your healthcare team is your best source for questions about insulin. No one is going to just give you a needle and a bottle of insulin and say, “Good luck.”
Instead, you’ll come up with an insulin plan — with the help of your healthcare provider, of course — for your type(s) of insulin, including when, how much, and how often to use insulin. This section is meant to be a primer so you know the scope of options available.
Table 6-3 lists the commonly used types of insulin. The following sections cover these medications in greater detail.
TABLE 6-3 Commonly Used Insulin Types and Action Profiles
Type of Insulin
Generic Name
Brand Name
Onset
Peak
Duration
Fast-acting insulin
Insulin glulisine
Apidra
15 minutes
1–2 hours
3–5 hours
Insulin lispro
Humalog
Insulin aspart
Novolog
Inhaled insulin
Afrezza
Regular/short-acting insulin
Regular insulin
Humulin R
30 minutes
2–3 hours
5–8 hours
Novolin R
Intermediate-acting insulin
NPH insulin
Humulin N
2–4 hours
4–10 hours
10–16 hours
Novolin N
Long-acting insulin
Insulin detemir
Levemir
1–2 hours
No peak
Up to 24+ hours (up to 42 hours for insulin degludec)
Insulin glargine
Lantus
Basaglar
Insulin degludec
Tresiba
Premixed insulin
70% NPH/30% regular
Humulin 70/30
30 minutes
2–12 hours
18–24 hours
Novolin 70/30
30 minutes
2–12 hours
18–24 hours
50% lispro protamine (NPL)/50% lispro
Humalog Mix 50/50
15–30 minutes
1–5 hours
14–24 hours
75% lispro protamine (NPL)/25% lispro
Humalog Mix 75/25
15–30 minutes
1–6.5 hours
14–24 hours
70% aspart protamine/30% aspart
Novolog Mix 70/30
10–20 minutes
1–4 hours
18–24 hours
Human insulin
Synthetic human insulin is manufactured to be the same chemical structure as the insulin that your body naturally produces. However, its action is not the same as your body’s insulin because it clumps up when you inject it under the skin and it takes longer to absorb.
There are three types of human insulin:
Short-acting human insulin (also called regular insulin) starts to work in 30 minutes, peaks at 2–3 hours, and lasts for 5–8 hours.
Intermediate-acting insulin (also called NPH) starts to work in 2–4 hours, peaks at 4–10 hours, and lasts for 10–16 hours.
Premixed combinations of short- and intermediate-acting insulin are also available.
How is human insulin made? Scientists put the human gene for insulin into bacteria or yeast, causing them to churn out insulin. The insulin is then extracted and purified. Voilá! It’s human insulin, without the humans (or perhaps a little help from humans).
Analog insulin
Analog insulin is manufactured to be similar to human insulin, but it has certain more desirable traits such as working more quickly or more slowly. Analog insulin is newer than human insulin — and it’s also more expensive.
There are three types of analog insulin:
Fast-acting insulin starts to work in 15 minutes, peaks in 1–2 hours, and lasts for 3–5 hours.
Long-acting insulin starts to work in 1–2 hours and can last up to 24 hours.
Premixed analog insulin starts to work in 5–15 minutes and lasts up to 24 hours.
Whether you take human or analog insulin depends on many factors such as cost (in general, human insulin is cheaper), insurance coverage, convenience (analogs can provide more flexibility), and your blood glucose goals.
Inhaled insulin
Afrezza is the only FDA-approved inhaled insulin. Adults without chronic lung problems may be eligible to use Afrezza. You use an inhaler to breathe in Afrezza during mealtimes. It’s a fast-acting insulin that starts working within 15 minutes, peaks at about 1 hour, and last for 3 hours.
Buying and storing insulin
Your healthcare provider will give you a prescription for insulin, which will usually come in a vial. Read the package instructions about the best way to store insulin once you get it from the pharmacy. Usually, insulin can be kept at room temperature for up to a month. And that’s the preferred way to do it because injecting insulin at room temperature is more comfortable than injecting cold insulin. Unopened vials of insulin can be stored in the refrigerator.
Never expose insulin to extreme temperatures like the freezer or the hot sun (or inside your car on a summer day). These changes in temperature could affect its potency. Also check the expiration date just like you would with any other medication. Don’t use insulin if it’s expired. Instead, return it to your pharmacy.
Also, inspect the insulin before you inject it. Visual cues are helpful. Rapid-acting, long-acting, and regular insulin should be clear without floating pieces. Intermediate-acting and premixed insulin should be cloudy, but also without floating pieces or crystals. If you suspect anything funky, don’t use the insulin, and take it back to your pharmacist for concerns or a refund or exchange.
Insulin prices have been steadily increasing, making it difficult for some people without health insurance (or with limited health insurance) to afford medications. Insulin manufacturers have special programs to help lower-income individuals obtain insulin. Insulin affordability is a major advocacy issue for the American Diabetes Association.
Injecting insulin: Syringes, pens, and more
You can inject insulin using a syringe or an insulin pen. We cover insulin infusion in the following section on insulin pumps. Whether you choose a syringe or pen for your insulin is a matter of personal preference.
All about insulin syringes
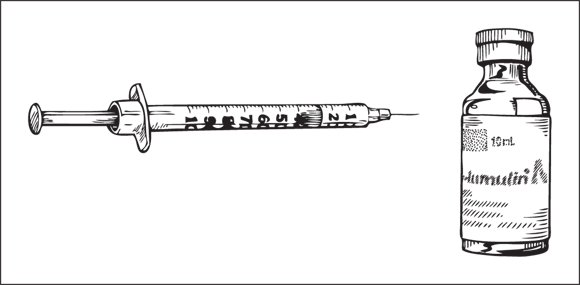
Many people use syringes to inject insulin. They’ve been around for ages! Syringes are made of a disposable plastic tube with a needle on the end. You insert the needle into a vial of insulin and draw up the insulin into the syringe (see Figure 6-1). Syringes hold a variety of insulin amounts or doses, so choose a syringe that holds your entire dose of insulin. For example, if you take a 40-unit dose, don’t choose a 30-unit syringe.
Illustration by Kathryn Born, MA
FIGURE 6-1: An insulin syringe and vial of insulin.
Your syringe will also come with a needle. Needles can vary in length and diameter (also called gauge). Your healthcare provider can help you choose the optimal needle based on comfort and efficacy.
After you’re done with your syringe, dispose of it properly as medical waste. Don’t just throw it in your kitchen trash (ick) because it could poke someone carrying out the garbage or your garbage collector and spread disease. Instead, use a puncture-proof container like an old liquid detergent bottle at home or buy a convenient travel container for disposing of syringes when you’re on the go.
Fear of needles is a common concern among people starting insulin. You’re not the only one who gets the heebie-jeebies when looking at a sharp needle. Don’t keep these feelings inside. Tell someone on your healthcare team, such as a diabetes educator, nurse, or pharmacist, who can offer specific tips for overcoming this fear.
All about insulin pens
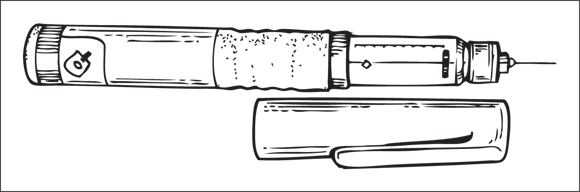
Most people who choose insulin pens do so for the convenience. You don’t have to carry around a vial of insulin, and you don’t have to draw up the insulin on the spot. You can also easily toss them in your bag or purse. However, insulin pens may be more expensive than using a syringe and vial, so do your homework.
Insulin pens (like the one shown in Figure 6-2) come in two styles: disposable (one-time use) and reusable (many times). Also, each pen is specially designed and manufactured to hold a particular type or mixture of insulin.
Pen needles come in varying lengths and diameters, just like syringe needles. Screw on a new needle each time you inject insulin with your pen (needles can carry viruses or bacteria). Follow the instructions on your insulin pen to prime it. Then follow the dosing instructions from your healthcare provider, as well the instructions included with your pen.
Just like storing a vial of insulin, protect your insulin pen from extreme temperatures. You can keep pens you’re currently using at room temperature and store unused pens in the refrigerator. Dispose of used needles in a safe container according to the package instructions.
Tips for injecting insulin
You don’t just inject insulin anywhere you want on your body. That’s not safe. Instead, there are techniques and tips for properly injecting insulin and making it as smooth and pain-free as possible. Ask your diabetes educator, nurse, or another provider for step-by-step instructions on injecting insulin.
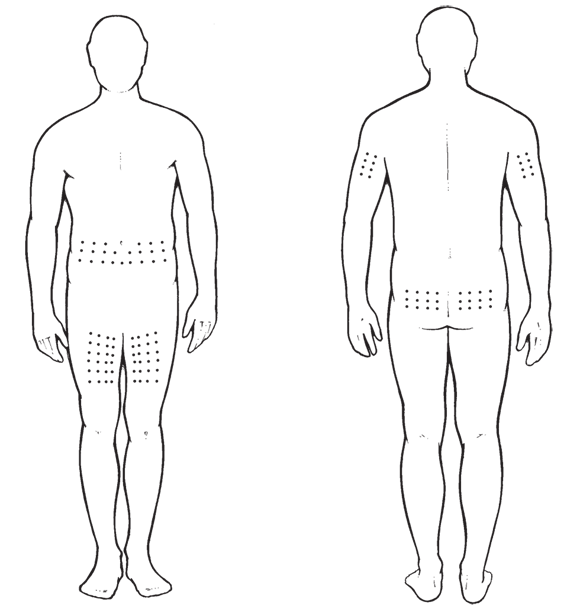
Insulin is injected, using a syringe or pen, into the layer of fat that lies directly under your skin. The fancy name for this fat is subcutaneous tissue. Some of the best places to do that are your abdomen, thighs, and the backs of your upper arms. Your healthcare provider can instruct you on the best places to inject insulin and how to do it.
You can rotate the exact site of the injection so you don’t get lumps or buildup of scar tissue. One technique is to think of the injection site as a 1-inch diameter circle. Choose a different, non-overlapping circle each time you inject and rotate within that part of your body, such as your abdomen. For site rotation techniques see Figure 6-3.
Injecting insulin isn’t easy for some people. Those with dexterity or vision problems, for example, may need a little extra help. There are lots of devices on the market that can help you overcome pain, anxiety, vision impairment, and dexterity challenges. Check out the latest issue of Diabetes Forecast’s annual consumer guide for details on injection aids or search the web for injection aids and look for highly rated and popular injection aids.
Insulin pumps
An insulin pump is another option for people with type 2 diabetes who need to give themselves multiple injections of insulin each day. People choose insulin pumps because they might help them better manage their blood glucose. Pumps can be convenient and can offer more flexibility to your insulin routine.
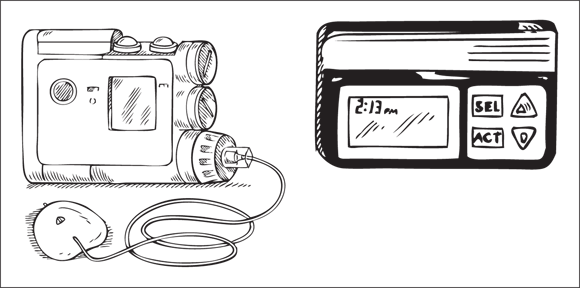
An insulin pump (shown in Figure 6-4) is a small device that you wear on your body that holds and delivers insulin. It’s attached to a thin needle, called a cannula, that you insert under your skin. Some pumps are directly attached to the needle, and others are connected through tubing (called an insertion set) to deliver the insulin.
Illustration by Kathryn Born, MA
FIGURE 6-4: An insulin pump with its insertion set.
Basal rate is the steady trickle of low levels of rapid-acting insulin in an insulin pump.
Most pumps deliver frequent, tiny doses of insulin at a steady background (basal) rate throughout the day and night and short bursts of insulin (bolus) before meals. You can program the pump to deliver insulin ahead of time, based on your expected needs. You can also push a button to deliver an extra bolus of insulin at mealtimes or snacks. This could also be used to treat episodes of high blood glucose.
An insulin pump on the market, called V-GO, is specifically used by people with type 2 diabetes. The pump is simple in that it attaches with a sticky patch to your skin and includes a built-in needle (no tubing required).
Most pumps fit inside a pump case that you wear on your waistband, bra, pocket, or similar spots that you find convenient. Your pump holds and dispenses your insulin, but that’s not all. Pumps have a screen to display information and electronics to keep them running, and they can store data. Some pumps have special features like connecting wirelessly with blood glucose monitors or even integrating with a continuous glucose monitor (CGM).
Being Cautious with Other Medications
People with type 2 diabetes often also have high blood pressure and high cholesterol, so you may take medication for these conditions as well. High blood pressure and cholesterol increase your risk for cardiovascular disease, stroke, and other complications, so it’s important to keep these in check. It’s particularly important for people with diabetes because they are about two to three times more likely to die from heart disease than people without diabetes.
Eating healthier foods like those with less sodium or saturated fat, exercising more often, losing weight, and stopping smoking will help lower blood pressure and cholesterol. You may also need to take medication to achieve your goals.
Medication to lower blood pressure
Your body delivers blood and essential nutrients through its network of blood vessels. Blood pressure is the force at which blood pumps through your vessels. It’s measured as a ratio of two numbers: systolic blood pressure (the pressure of blood in your vessels when your heart beats and pushes blood out) and diastolic blood pressure (the pressure in your vessels between heartbeats). Systolic is the first number; diastolic is the second number.
Your provider should measure your blood pressure at each visit. Most people with diabetes have a blood pressure goal of less than 140/90 mmHg.
Four classes of drugs are often used to lower blood pressure in people with diabetes including ACE inhibitors, angiotensin II receptor blockers (ARBs), thiazide-like diuretics, or dihydropyridine calcium channel blockers. Sometimes people will take more than one blood pressure medication to achieve their goals.
Remembering to take your medications can be difficult, especially if you take a lot of them every day. Pill organizers can help you organize your pills by day and time of day. You can buy them at a pharmacy or online. Noting that you’ve taken a medication by writing it down on a paper calendar or setting an alarm on your phone can also help. Put your medications in a hard-to-forget place like the kitchen table or next to your toothbrush.
Medication to treat cholesterol
High triglycerides, high LDL cholesterol (bad cholesterol), and low HDL cholesterol (good cholesterol) increase your risk of cardiovascular disease and stroke.
Your provider should measure these blood lipids, called a lipid profile, when you’re first diagnosed with diabetes and then periodically thereafter. Statins, including atorvastatin (Lipitor) and simvastatin (Zocor), are medications that reduce the level of bad cholesterol and may increase good cholesterol. The American Diabetes Association recommends that most adults with diabetes take a statin. Other cholesterol-lowering drugs are also used in some patients with specific cardiovascular risks.
LDL cholesterol stands for low-density lipoprotein; it’s the “bad” cholesterol because it narrows and blocks arteries, which can lead to heart disease and stroke. Try to lower your LDL cholesterol. HDL cholesterol stands for high-density lipoprotein; it’s the “good” cholesterol because it helps keep your blood vessels clear. Try to boost your HDL.
Eating healthy foods low in saturated fats, losing weight, exercising, and quitting smoking can have the beneficial effects of lowering LDL cholesterol and raising HDL cholesterol. It’s a double bonus!
Aspirin and other medications
Ask your provider whether it makes sense for you to take a low dose of aspirin (81 mg) daily. People with diabetes who are 50 years old or older and who also have at least one additional risk factor for heart disease (such as high blood pressure, smoking, or high blood fats) may take a daily low-dose aspirin.
If you’re overweight and struggling to lose those necessary pounds, you may consider asking your healthcare provider whether weight loss medications could help. Five weight loss medications are available for people with a body mass index (BMI) of more than 27 kg/m2 and type 2 diabetes (or another medical condition).
They include orlistat (Alli, Xenical), lorcaserin (Belviq), phentermine/topiramate ER (Qsymia), Naltrexone/buproprion (Contrave), and liraglutide (Saxenda). All have common and more serious side effects. None of them should be used by pregnant women or those considering pregnancy.
BMI is a measurement of your weight (in kilograms) divided by height (in meters squared). It is used to tell whether you’re underweight, normal weight, overweight, or obese. You can calculate your BMI at www.nhlbi.nih.gov/health/educational/lose_wt/BMI/bmicalc.htm (or just search online for BMI calculator).
Surgery for Type 2 Diabetes
Eating healthy foods, exercising, losing weight, and of course, taking necessary medications like pills or insulin are all proven strategies to manage your blood glucose and prevent complications. But now, some people with diabetes have another effective option: surgery.
Surgery to treat diabetes is called metabolic surgery. It is also sometimes called bariatric surgery or weight-loss surgery. The goal of metabolic surgery is to treat diabetes while helping patients lose weight and reduce the risk of cardiovascular disease. Some patients don’t have to take diabetes medications anymore after surgery.
Several studies have shown that surgery can help people with type 2 diabetes improve their blood glucose and reduce their risk for cardiovascular disease. What’s incredible is that these surgeries improve blood glucose in ways that extend beyond just losing weight. Scientists are still investigating this phenomenon.
Who is eligible for surgery? You must be a good candidate for surgery in order to get metabolic surgery, so ask your healthcare provider whether this might be a good option for you. For example, people with substance abuse problems or mental health conditions might not be the best candidates for surgery.
Then you and your doctor will consider your BMI and blood glucose control. The American Diabetes Association has very specific guidelines on who is an appropriate candidate for metabolic surgery. Recently, the Association recommended metabolic surgery for people with type 2 diabetes who are morbidly obese (BMI greater than 40 kg/m2) and in people with type 2 diabetes with uncontrolled blood glucose and a BMI between 35–39.9 kg/m2. The Association also said that metabolic surgery can be considered in people with type 2 diabetes with a BMI of 30–34.9 kg/m2 if their blood glucose is not adequately controlled.
Consider and weigh the adverse affects: Surgery is expensive and can cause long-term side effects such as a dumping syndrome (nausea, colic, and diarrhea), risk for depression, vitamin and mineral deficiencies, and other issues.
The four most commonly performed metabolic surgeries are: roux-en Y gastric bypass, vertical sleeve gastrectomy, laparoscopic adjustable gastric banding, and biliopancreatic diversion.
Health insurance companies require different criteria for coverage of surgery, so do your homework. If you’re considering metabolic surgery, call your insurance carrier to find out more about your coverage and limits.
 Knowing the need for medicine
Knowing the need for medicine Your diabetes medication regimen can change over time. You may take a drug like metformin at the beginning, but then need to add or change medications to keep your blood glucose in your target range later on. (Remember: Most people are aiming for an A1C of 7 percent or less.) Or you may experience side effects that prompt medication changes. You may also need to take insulin at diagnosis or several years down the road. It totally depends on the individual!
Your diabetes medication regimen can change over time. You may take a drug like metformin at the beginning, but then need to add or change medications to keep your blood glucose in your target range later on. (Remember: Most people are aiming for an A1C of 7 percent or less.) Or you may experience side effects that prompt medication changes. You may also need to take insulin at diagnosis or several years down the road. It totally depends on the individual! Never stop taking a medication because you think it’s not working or because of annoying side effects (an unintended effect, such as diarrhea or flatulence, of taking a certain drug). Instead, call your provider and tell her what’s going on. Don’t be shy about bringing up concerns like bowel movements, changes in mood, or any other concern. All drugs can have side effects, although some may be more severe than others.
Never stop taking a medication because you think it’s not working or because of annoying side effects (an unintended effect, such as diarrhea or flatulence, of taking a certain drug). Instead, call your provider and tell her what’s going on. Don’t be shy about bringing up concerns like bowel movements, changes in mood, or any other concern. All drugs can have side effects, although some may be more severe than others. Know the names, doses, and instructions for each medication you take. If you’re like most people, you’ll probably need to write them down. Don’t be afraid to ask your provider or pharmacist for these details each time you see her.
Know the names, doses, and instructions for each medication you take. If you’re like most people, you’ll probably need to write them down. Don’t be afraid to ask your provider or pharmacist for these details each time you see her. Incretins are a group of hormones that signal the body to release insulin after eating. Scientists have developed medications that target these hormones for people with type 2 diabetes. Two medications, DPP-4 inhibitors (pill) and GLP-1 agonists (injectable), work by regulating these hormones.
Incretins are a group of hormones that signal the body to release insulin after eating. Scientists have developed medications that target these hormones for people with type 2 diabetes. Two medications, DPP-4 inhibitors (pill) and GLP-1 agonists (injectable), work by regulating these hormones.