If you have never been sick, never lost so much as a day in bed— then you have missed something! When your turn comes, don't be dismayed. Remind yourself that pain and suffering may teach you something valuable, something that you could not have learned otherwise. Possibly it may change for the better the entire course of your life. You and those around you will be happier if you can look upon any illness as a blessing in disguise, and wisely determine to make the most of it. You can turn your sickness into
an asset. —Louis Bisch
When You Have a Fever
by J. D. Ratdiff
Millions of people each day slip thermometers under their tongues, wait a few minutes, then consult the little arrow. Most laymen believe that the higher the body temperature the graver the illness. Physicians aren't so sure. For upwards of two thousand years medical men have been debating the question: is fever friend or foe? Is it an indicator of how sick a person is—or of how vigorous an effort his body is making to get well?
What is fever? It is simply an indication that the body is generating heat faster than it is losing it. Your body's remarkable heating system is in many respects strikingly like a home heating
system. The food you eat is burned, mainly in muscle tissue. The resultant heat is piped around the body by the blood in blood vessels. Like a well-built home, the body has its insulation—a layer of fat under the skin—to cut down heat loss. The entire system is controlled by cells in the hypothalamus, on the underside of the brain. This is the body thermostat. When it is pushed too high, there is fever. The sweating mechanism slows down and the skin becomes dry and hot.
No real studies of body temperature were made until, in the middle of the last century. Dr. Carl Wunderlich of the University of Leipzig measured temperatures of 100,000 people and concluded that "normal" body temperature was 98.6° Fahrenheit.
Today's research men note that body temperature varies widely during a day—being lowest in the early-morning hours, highest in the late afternoon. Therefore, physicians think it would be better to speak of a normal "zone"—from 97.2° to 99.5°.
Although the blood is highly efficient as a distributor of heat, it doesn't do a perfect job. If the mouth temperature is 98.6°, the rectal temperature is usually a degree higher. The liver, hottest organ in the body, is around 101°. The groin area is usually at least a degree lower than the interior of the body. Survival of the human race depends on its rising no higher. Above this level, male reproductive glands are unable to produce sperm.
What induces fever? A surprising variety of causes. Anxiety is one. Children frightened by going to the hospital often run fevers in the 101° to 103° range. One draft-board physician found that the temperatures of 324 draft examinees, anxious about their status, averaged nearly a degree above normal. Also, injury to the brain thermostat—caused by accidents or by tumors growing into the area—often produces raging fevers.
By far the largest producers of fever are bacterial and viral diseases. The exact means by which these microbes cause fever is not known. But Dr. Paul B. Beeson of Yale believes that under microbial attack white blood cells release fever-producing chemicals called pyrogens which prod the brain thermostat into action.
Are fevers harmful? There is no cut-and-dried answer. Some fevers are clearly dangerous—particularly those caused by brain
injury, tumors, sunstroke. They soar to levels where temperature itself becomes a menace to life. A fever of 109°, for example, does irreparable damage to the brain if not brought under quick control by ice-water enemas or immersion in tubs of ice water.
Fevers following heart attacks are also grave affairs. The danger here is this: in fever the rate of cellular activity in the body (metabolism) may be greatly increased. At this faster clip the cells require more oxygen. Thus there is an added load on an already damaged heart.
These are the exceptional cases. About the more common fevers that accompany colds, sore throats and such, one point should be remembered: fever is not a disease but a symptom — often a valuable and revealing one. Many physicians are today questioning the w^isdom of fighting common fevers with temperature-reducing drugs—such as aspirin. Speaking mainly of childhood diseases, Dr. Alan K. Done of Stanford University school of medicine observes: "Antifever therapy is often employed more for the benefit of parents, or the physician, than the child. It is doubtful whether body temperatures in the range of 104° are harmful, even if prolonged for several days."
Fever may be the best, or the only, available sign for following the course of an illness, as many diseases have readily recognized temperature patterns. In typhus, for example, fever is continuous. Malaria has a relapsing pattern—normal for a few days, followed by an upward swing. In typhoid there is a remittent pattern (marked fluctuations remaining above normal); in bone infections and abdominal abscesses there is an intermittent fever (where normal is approached at some time during the day).
What are safe limits for fever? There is no hard and fast rule. It has been observed that people rarely survive temperatures above 109°. However, temperatures almost never rise above 106°. Apparently, the body has some emergency mechanism that takes over at this point. A chain of lifesaving events gets under way. The patient usually goes into coma, blood flow to the blood vessels near the surface of the body is increased and sweating becomes profuse. These events produce a cooling effect, and the fever begins to fall to safer levels
Fearsome as fever may be to laymen, it has many beneficial effects. It prods the body into greater production of bacteria-fighting white blood cells and bacteria-killing antibodies. Recent evidence indicates that it increases production of the hormone ACTH, which in turn combats the stress placed on the body by disease. It appears to enhance the action of such antibiotics as penicillin.
At certain reasonably safe temperature levels some bacteria are simply cooked to death. Last century, for example, physicians noted that after bouts with certain feverish diseases (malaria, typhus) many patients were cured of syphilis. This led Dr. Julius Wagner-Jauregg, Austrian physician, to infect patients with malaria as a treatment for syphilis, and led later on to production of artificial fevers with high-frequency electric current.
As wider knowledge of fever has accumulated, many old rules have been rewritten. A generation ago it was standard practice to "starve a fever"—which undoubtedly killed many badly debilitated patients. Since fever hoists the metabolic rate, the need for food and fluids is increased. Today's rule: a high-protein, high-vitamin diet, with all the liquid the patient can take.
Another old rule was to cover the feverish patient with blankets and heat up the sickroom—so he could "sweat it out." This was the worst possible treatment. In fever, the body is struggling to get rid of heat. Why make the job more difficult? Today's rule: a comfortably coolish room, light bed covering.
Until recently it has been customary to keep feverish patients in bed. Under certain circumstances this rule, too, may be ready for discard. Not long ago Dr. John P. Gibson, a Texas physician, collected records of 1082 feverish youngsters. Some were confined to bed, some were allowed up and about the home. Temperatures returned to normal at almost exactly the same rate with each group. Concluded Dr. Gibson: "This study seems to indicate that in 'ordinary' or 'self-limiting' illnesses . . . children may rest as they desire, and play quietly in the house."
To sum up: Fever is no longer the frightening thing it once was. According to present-day thinking, the great majority of fevers are more apt to be friends than foes.
Repelling
the
Unseen Invaders
by Ruth and Edward Brecher
"IVTot sickness but health,^^ a famous physician once remarked, jy^ "is the greatest of medical mysteries."
Your own good health is an example. Every day your body is assailed by billions of germs, many of which can produce illness or even death. Tet you stay well. Countless bacteria and viruses gain entry into your body with the food you eat or the air you breathe or through breaks in your skin. Tet you stay well. Some of them establish permanent residence in your mouth, your nose and throat or your intestines, where they may multiply fantastically. Tet you stay well.
What protects you from these ceaseless assaults by bacteria and viruses?
Through decades of study scientists have been slowly finding out. Your health is safeguarded, they report, by an ingenious series of defenses arranged in depth like the successive lines of an army entrenched to ward off invaders.
Suppose, for example, that a germ-laden fleck of dust floats into your eye. In all probability there is nothing to worry about.
Your eye surface is constantly bathed in tears, which contain a bacteria-destroying antiseptic called lysozyme. Lysozyme is so powerful that a single teardrop diluted with half a gallon of water will still destroy at least one species of germs.
Your saliva and the other fluids manufactured by your body also contain antiseptic chemicals. Even your bare skin has considerable germicidal power. For example, virulent-dysentery bacteria in a drop of fluid placed on a glass slide will survive for hours, while those in a drop placed on the clean palm of your hand will be dead within about twenty minutes.
Some kinds of germs can survive these external defenses and even multiply on your skin. Before they can harm you, however, they must gain entry into your body and then run an amazing gantlet of other defenses. Germs entering through your mouth, for instance, are attacked by the antiseptics in your saliva. For those that are swallowed and washed into your stomach, powerful digestive juices lie in wait. Few reach your intestines alive.
Germs which gain entry through your nose must thread the complicated maze of your air-filtering nasal passages. The surfaces of these passages are kept moist by a mucous fluid for catching germs. If the germs cause irritation, they are sneezed out; or your nose starts to run and they are flushed out. Germs which manage to reach the tubes to the lungs are also trapped in a mucous fluid, and are coughed out, or if swallowed, meet their fate in the well-guarded gastrointestinal tract.
When germs get into your body through breaks in your skin or mucous surfaces—breaks so small that they may be unnoticed—the peril is seemingly greater. Let's say that you step on a germ-laden nail. Each germ thus entering your tissues may divide into two after twenty minutes or so, and divide again in another twenty minutes. If this rate were to continue, you would be host to a million descendants within seven hours, and to several quadrillion the next day. By then your entire body would, of course, be overwhelmed. But before this can happen another type of defense will have come to your aid.
One of the most awe-inspiring marvels of life is the ability of the body to renew itself, to repair damage and go forward. Every
time you so much as nick yourself with a razor or paring knife, a construction job far more complex than building a skyscraper gets underway. We take this healing power for granted, yet without it surgery couldn't exist; the slightest injury could lead to death.
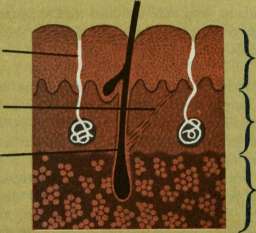
Inflammation begins when various chemicals are released at the site of a germ invasion by the invaders or by the injured cells in your body. These chemicals seep outward in all directions until they reach the nearest blood vessels. There they cause a relaxing of the vessel walls that enables plasma, the watery part of the blood, to seep out. Accompanying the blood plasma are white blood cells called leucocytes, and various chemicals that curb bacterial growth.
Leucocytes are among the most curious and most effective of your body's defenses. In appearance they resemble the one-celled animal called amoeba, and like the amoeba they can propel themselves from place to place within your body. In some way not yet understood, leucocytes are attracted as if by a magnet to the site of a bacterial invasion. When they arrive they gobble up any invading particles they find.
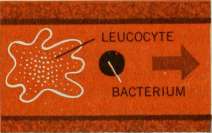
It is fascinating to watch this gobbling-up process through a microscope. A leucocyte slithers up to an invading bacterium, crowds it against a solid surface, then flows its jellylike body around the bacterium to "corner" it. Next it opens a hole-in its skinlike membrane, and the bacterium is completely engulfed. A moment later the leucocyte slithers off after its next quarry. Millions of leucocytes are often mobilized at the site of an infection.
Other factors involved in inflammation help the leucocytes in their work. In the blood plasma is a chemical called fibrinogen, which quickly solidifies into a network of strands and, with other plasma substances and the leucocytes, forms a wall around the battlefield, trapping the germs so that the infection is localized. Boils and abscesses are typical examples of how this walling-oflf process safeguards the rest of your body from germ invaders.
Even though bacteria are thus contained, the resources of your entire body are mobilized to defeat them. Some of the chemicals released during the battle enter your bloodstream and carry the
OUR HUMAN BODY
alarm to storehouses throughout your body where leucocyte reserves are maintained. Within minutes millions of additional leucocytes are released into your blood, which carries them to all your tissues. While this is going on, your bone marrow is also alerted and it speeds up the manufacture of new leucocyte reserves.
Some germs are coated with a repellent which keeps leucocytes away, and some have the power to kill the leucocytes that engulf them. Even in death, however, the leucocytes continue to release chemicals injurious to germs.
If the leucocytes cannot complete the mopping-up operation, they are joined by larger (but still microscopic) cells called macrophages. These can gobble up not only bacteria but also leucocytes that are harboring bacteria.
Usually when a leucocyte or a macrophage engulfs a germ it means death to the germ, but not always. Some bacteria can survive for long periods within cells which have gobbled them up. Indeed, a cell may occasionally prolong the life of a bacterium by protecting it from antiseptic blood substances and from the drugs your physician prescribes to help combat the infection. Your body requires a way to dispose of these germs after they have been engulfed, and to get rid of other waste products.
To provide for this, your body tissues are drained by a network of channels called the lymphatic system. Leucocytes, macrophages and invading particles enter the vessels of this network and are carried by the lymph fluid to "regional lymph nodes," or glands, situated at strategic points throughout your body. Each node
LEUCOCYTE ABSORBING BACTERIUM

THE WISDOM OF THE BODY
93
serves as a filter, holding back bacteria and other particles. The lymph fluid flows on from one node to another until it reaches the ones in the neck, where it is discharged into the bloodstream. By then, generally, all germs have been filtered out of the lymph fluid.
Following an illness, however, disease germs may survive for days or even weeks within the lymph nodes. The glands in your neck are the final barriers which prevent germs from reaching your bloodstream, and the survival of germs in them for long periods explains why these glands sometimes remain swollen and tender long after other symptoms have disappeared.
Even if a few germs reach the bloodstream, another line of defense stands ready. Your bone marrow, liver, spleen and a few smaller organs are equipped with multitudes of macrophages to filter invading particles out of your blood just as the lymph nodes filter your lymph fluid.
How are the leucocytes and macrophages able to distinguish between invading germs or other particles and the cells or molecules of your own body? Your body has a built-in identification system which labels invading particles. These labels, which attach themselves to invaders, are called antibodies. Leucocytes and macrophages will occasionally engulf almost any particle they happen upon, but the ones they search out and devour with the greatest voracity are those which have been labeled as invaders by antibodies.
Most cases of recovery from an infection are traceable in large part to antibody action. If you have never had scarlet fever, your


body lacks antibodies tailored to fit the streptococci which cause that disease. But if streptococci secure a sufficient toehold in your body to multiply, your antibody factories start tooling up. For several days, perhaps, the germs continue to multiply and you get sicker and sicker. By then, however, full-scale antibody production has begun and antibodies are turned out in large amounts. These latch onto the scarlet-fever streptococci, which, as soon as they are labeled, fall prey to the voracious leucocytes and macrophages, and your recovery begins. Other substances in your blood help out by destroying bacteria to which antibodies are attached.
It is chiefly your antibodies which make you immune to second attacks of many common illnesses. The first time you suffer from a disease such as scarlet fever or measles your antibody factories take several days to learn the right pattern. Once the lesson is learned, however, production can begin much more promptly, and large amounts of antibodies of the desired pattern may be turned out within a few hours after the entry of a few thousand germs. Thus the second invasion and subsequent entries of a particular type of germ are frequently wiped out before you even suspect that you've been infected.
Antibodies are also the agents which make it possible to control infectious diseases through vaccination. A vaccine is a substance which teaches your body in advance how to manufacture antibodies promptly against a disease you have not yet encountered.
A few kinds of germs have learned how to evade our antibody defenses. The influenza virus is the most striking example. Every few years a type of flu virus comes along which is unaffected by the common flu antibodies. When this happens, an influenza "pandemic" sweeps the world, as with the "Asian flu." Within a few years almost everybody gets the new kind of flu and develops antibodies against it—whereupon a different flu virus pops up. Each type of flu requires a separate antibody.
Most of the antibodies circulating in your blood are found in a part of the blood plasma called gamma globulin. This antibody-rich substance can be extracted from the blood of donors and
Stored for considerable periods. Small injections of gamma globulin will provide temporary immunity to measles and infectious hepatitis; the "borrowed antibodies" in the gamma globulin act in just the same way as the antibodies you manufacture yourself.
Newborn babies also stay well on borrowed antibodies. Their antibody factories operate poorly or not at all during the first few weeks of life, but antibodies received from their mothers before birth protect them for a time from most of the diseases to which the mothers themselves are immune. Babies also get protective antibodies in mother's milk, especially in the milk secreted during the first few days of nursing.
Some germs attack only cells in their immediate vicinity; others release poisonous molecules called toxins which may circulate to other parts of your body. Diphtheria and tetanus bacteria are examples of these toxin producers. When attacked by toxins your body manufactures antitoxins—that is, antibodies against toxin molecules. And just as you can be immunized against virus diseases by means of vaccines containing denatured viruses, so you can be immunized against diphtheria and tetanus toxins by injections of denatured toxins called toxoids.
In the economy of the body a wound always gets first priority. Even people starving in World War II concentration camps retained the ability to heal. Whatever materials are needed for the healing process are provided by tearing down tissues elsewhere in the body. Thus, muscle is broken down into amino acids, which build new tissue at the wound site. That is why badly injured people "waste away."
Gradually a wound fills with granulation tissue—a beefy, spongy patching material which will be replaced by firm, fibrous scar tissue.
The construction of new tissue is one of the true wonders of nature. In response to some mysterious directive force, fiber cells arrange themselves in neat geometric patterns, like chemical crystals. Since these more complex tissues need a reliable blood supply, an intricate plumbing system of capillaries must be installed. Researchers can watch this when the ear of a rabbit is
injured: little blood vessels, so delicate that they bleed at the touch, start drilling their way through the new tissue. Their ends remain sealed; otherwise, blood would leak away. Progressing in random fashion, they finally strike another capillary. The ends magically dissolve and the two join, laying down the elements of a new circulatory system. By a process still more complex, nerve tails push their way into the new tissue.
All this has been taking place deep under the scab. Meanwhile directly beneath the scab, new skin is forming. Around the margins of the wound, skin cells start playing their all-important role. They start elongating—reaching their way toward the center of the denuded area, just as bark grows over a blaze on a tree. The first skin to cover the wound is thin, fragile, living. Eventually it will mature, with uppermost cells dying and hardening to form a permanent, inert covering.
A week or so after the injury the wound looks healed. Actually, some of the most remarkable steps in the healing process are to come. In the months following injury, tiny muscle fibers start growing outward from either side of the wound, finally meeting and splicing together. Fat joins to fat, connective tissue to connective tissue. In time, perhaps a year, the scar tissue is replaced by functioning tissue. The reconstruction job is completed.
Could mankind survive without the human body's miraculously coordinated "defense in depth"? It seems unlikely.
Iain makes man think. Thinking makes man wise. Wisdom makes Ufe endurable. —John Patrick, Teahouse of the August Moon
IN EVER does nature say one thing and wisdom another. —^Juvenal, Satires
CHAPTER 4^

l


Giants of the Body
EVEN primitive man sensed that the brain, the heart and the lungs played the most dramatic roles within the human body, though the nature of their functions long remained cloaked in mystery and superstition.
The more medical knowledge advances, the more awe-inspiring does the magnitude of the tasks performed by these great organs become.
^/^
PART I . THE BRAIN
Introducing the Brain
by John Pfeiffer
This vivid account of the human brain in all its aspects is from the most outstanding work written for laymen in the English language on the subject of this organ of the human body. The condensation of the opening chapter of The Human Brain by John Pfeiffer is an exciting invitation to self-under standing.
The human brain is perched like a flower on the top of a slender stalk, which in a six-foot man is not quite a yard long. The top three inches of the stalk, a thick white cable of nerve fibers known as the brain stem, lies entirely within the skull and is partly buried by the bulging halves or hemispheres of the brain. The rest of the long stalk, the spinal cord, is a direct continuation of the cable outside the skull. It runs down through holes in the vertebrae of the spine and ends at the small of the back. Many branches extend from the central stalk, like the roads that feed traflftc in and out of a superhighway. Through their finest fibers they reach into the remotest places, and into every nook and cranny from the roots of hairs and teeth to the tips of the toes.
The brain itself is three pounds of "messy substance shut in a dark warm place"—a pinkish-gray mass, moist and rubbery to the touch, about the size of a softball. Shock-absorbing fluid cushions it against bumps, sharp blows and other impacts. It is wrapped in three membranes, including an extra-tough outer envelope, and is set snugly into its crate of bone.
Under the microscope a single brain cell with its fibers may resemble the crown of a tree. Growing out from each branch are smaller branches, and from each of them comes a succession of smaller and smaller off"shoots down to the most delicate twig. The brain contains some thirteen billion such cells, five times more than the total number of people in the world.
These units form masses of twisted fibers, a tangle which one investigator has called the "cerebral jungle." Until recently most investigators assumed that nerve fibers occupied fixed positions, or at least moved only as they grew, like the roots of plants. But new studies (at the University of Texas) indicate that brain tissue is far more active than this. As you read this sentence, fibers in your head are swaying like seaweed swept by tides. Tentacles of protoplasm are slowly moving forward, retreating, swelling and shrinking, waving from side to side.
What is the brain for? Judging by what we know today, it is the great organ of adjustment. It plays the basic biological role of keeping us adjusted to unpredictable events in the outside world, of preserving our identities in an environment of swift and ceaseless chemical change.
The brain keeps us alive by balancing the processes of birth and decay. These basic reactions have top priority. Everything else either helps in carrying them out, or else waits its turn. We pay a high price when the balance of any vital process is upset. For example, sugar is one of the body's energy-providing substances and we must have just the right amount, no more and no less. We walk a biological tightrope between coma and convulsion, the possible results of relatively slight changes in blood-sugar levels.
But the brain usually receives advance notice of impending trouble. It receives a steady flow of information about current
sugar levels, and makes adjustments as effectively as a pilot guiding an airplane through a storm. If there is too much sugar, the excess is burned up and excreted. If there is too little, the liver is instructed to release the proper amount of reserve sugar. Notice what such control implies. The brain must "know" the desired sugar level, about a sixtieth of an ounce for every pint of blood, on the average. It must go by similar standards in regulating breathing (most of us inhale and exhale eighteen to twenty times a minute) and heartbeat rates (about seventy times a minute), and in holding body temperature at 98.6° Fahrenheit.
The brain must also be in constant communication with all parts of the body. Indeed, it turns out to be the headquarters of the most elaborate communications network ever devised. Its activities are the result of the combined and patterned activities of billions of nerve cells. A nerve ceil is a living wire which produces and conducts rapid electrical impulses. It keeps itself "loaded" and ready for action with the aid of a built-in battery which runs on an oxygen-sugar mixture and recharges automatically. It fires—that is, emits up to several hundred impulses a second— when triggering impulses reach it from sense organs or from other nerve cells.
These outside signals enter the body of the cell through special receiving fibers which are usually short, fine and highly branched. The slenderest fibers, about 1/25,000 of an inch in diameter, have speed limits of a foot a second or two thirds of a mile an hour. But in large-gauge fibers, which measure about ten times thicker, nerve impulses flash along at speeds up to 150 yards a second, a respectable 300 miles an hour. Thick, fast fibers generally connect remote parts of the nervous system; thin, slow fibers connect neighboring regions. Thus, if a cell communicates with several other cells at varying distances, the messages all tend to arrive at about the same time. This means that widely scattered parts of the nervous system can be stimulated, inhibited or alerted at once—a distinct advantage in coordinating very complex behavior.
The brain uses this network to adjust us to the outside world. Generally speaking, its operation can be divided into three parts:
(i) it receives input in the form of messages from the sense organs; (2) it organizes the input on the basis of past experience, current events and future plans; and (3) it selects and produces an appropriate output, an action or series of actions.
The brain keeps in constant touch with the flow of events. It is stirred up by lights, sounds, odors and other disturbances in the environment. Each sensation produces electrical impulses in nerves leading to the brain, "shocks" which stream into higher nerve centers and cause cell after cell to fire in a series of chain reactions.
The sense organs most remote from your brain are those located in your toes. Fibers originating in these outlying stations carry messages concerning heat, cold, muscle tension, touch, pain. They are joined by more and more fibers from your foot, leg, knee and thigh.
By the time the collected fibers reach the lower part of the spinal cord they form a thick cable. The cable continues to thicken as it climbs and is joined by millions of fibers from other organs of the body on the way up to the brain. It subjects the brain to constant proddings. Although its lines are less busy during sleep, even then it is occupied with various duties—keeping your heart and lungs going, dreaming, and listening with a somewhat reduced vigilance. The brain relaxes, but as long as it is alive it finds no rest.
The brain's informers are sense organs, sentinels located at strategic points throughout the body. Imbedded in the skin are some 3,000,000 to 4,000,000 structures sensitive to pain, 500,000 touch or pressure detectors, more than 200,000 temperature detectors. These tiny organs—plus the ears, eyes, nose and tongue— are some of your windows to the outside world. Reports about the state of things inside your body come from other built-in sense organs which give rise to sensations of muscular tension, hunger, thirst, nausea. '
The brain has other sensory maps. On the cortex at the back of the head are visual maps, screens made up of a mosaic of nerve cells. Every pattern you see around you, every tree and building and face, produces patterns on these screens as various cells in the mosaic. Other sensory fibers lead to the smell areas of the
cortex, which are buried deep down in the walls of the chasm between the cerebral hemispheres. Each sense thus has its map on the cortex, its exclusive zone in the highest center of the nervous system. In this way, the brain sorts the information upon which its activities are based.
In nerve messages, as in dot-dash telegraph codes, patterns of pulses stand for the items of information being sent. But the interpretation of nerve signals depends first of all on the place they arrive at. No matter how accurately senses have been coded, no matter how meaningful the signals are, they will be misinterpreted if they arrive at the wrong place. A happy-birthday telegram means just that, even if it should happen to reach the wrong person. But a slip-up in the nervous system is something else again.
Suppose you were listening to fast music—say, the Benny Goodman version of "Sing, Sing, Sing"—and the nerve signals somehow got switched to the wrong line, arriving at the visual areas of the cortex instead of the hearing areas. You'd "see" the music as a mad rush of flashing lights, moving forms, vivid colors. Such mix-ups actually occur, and may result from "cross talk" between nerve fibers. Cross talk is familiar to repair men of your local telephone company. If insulation wears off neighboring wires in a telephone cable, electricity leaks away and you may find yourself listening in on someone else's conversation.
Similar leaks in the nervous system may account for many peculiar sensory disorders. Current escaping from a touch fiber to a nearby sound fiber, for example, might make you hear crashing noises when you bumped your elbow. Somehow certain drugs increase cross talk among sensory fibers, and nerve injuries may produce the same effect. There is no reason to doubt that a certain amount of cross talk takes place in the normal nervous system; the nerve signals traveling through neighboring fibers interact in some way. We do not yet know the significance of this effect. But new evidence indicates that cross talk between fibers of the right and left eyes have something to do with the mechanism whereby we see objects as three-dimensional solids.
The brain is continually adjusting and readjusting the tensions of many muscles so that you maintain your posture and balance.
Simply standing up represents an acrobatic feat which is no less remarkable because it is performed automatically. Everyone naturally sways a bit in an upright position, and a failure in the balance-controlUng centers of the brain would send you sprawling. There is one powerful muscle which, if uncontrolled, would snap your leg back at the knee, pressing your calf hard against your thigh. Another muscle would keep your leg stiff as a ramrod. The brain receives messages specifying the tensions of more than two hundred pairs of opposing muscles, every one of which must be properly adjusted to keep you standing.
Things become more complicated during a walk over uneven ground—and even more complicated when you dive from a high board, lower a sail in a storm or ride a surfboard. Every action, however simple, is made up of many individual muscle contractions and large-scale movements. These movements must follow one another at just the right time and in just the right order. The brain does the timing. It coordinates all sequences of movements so that we move smoothly and not in a series of jerks. When it comes to pursuing the activities of everyday life, we are thus reasonably sure of ourselves and our positions in the world.
The hand, working under the direction of the brain, is capable of an unlimited variety of skilled manipulations. A master pianist can play 120 notes a second, or a dozen notes a second with each finger. One famous surgeon used to put a piece of silk thread in a matchbox and impress reporters with the following trick. Working within the cramped space of the half-closed matchbox, he nonchalantly tied the thread into complicated surgical knots— using only the thumb, index and middle fingers of his left hand.
Every set of coordinated movements, from such highly skilled performances to routines like walking and driving a car, involve the integrating powers of the nervous system. All activities— direct or indirect, successful or unsuccessful—are attempts to keep the fire of life burning steadily and as long as possible. And this includes all our attempts to understand life itself.
Our adjustments are never perfect. Things are too complex and too uncertain for that. Still, we do not and cannot stop trying, and the brain coordinates our continuing efTorts.
The Memory-
REMARKABLE STORAGE BATTERY
b}> Bruce Bliven
How are we able at will to summon up mental images of places seen years ago? What is the mysterious process involved? Because of brilliant laboratory work carried on in several countries in recent years we are beginning to find the answers to such questions. In essence, the physical process is electrical.
The human nervous system—brain, spinal cord and nerves— contains what is substantially a wet-cell electric battery, generating a direct current of about a tenth of a volt—roughly one twentieth as much as a flashlight battery. The electric charge is created by two body chemicals, sodium and potassium, operating on nerve tissues bathed in a fluid that is chiefly water. As each section of nerve fiber receives an electrical impulse, it triggers a reaction in the next section, so that impulses travel instantly to and from the marvelously intricate message centers of the brain.
To get a faint idea of what is going on continuously in the brain and the spinal cord, think of a thousand telephone switchboards, each big enough for a city like New York, going full tilt receiving
and transmitting requests, questions, orders. Through its incredible ability to hook together thousands of reverberating circuits in a fraction of a second—each representing a memory or an idea— the brain is able to bring together into one grand circuit the data needed to think and make decisions.
Many scientists beheve that every experience of our lives is recorded and preserved by these electrical circuits, including millions that we seem to have completely forgotten. Psychiatrists have found that when a patient tries day after day he can recall buried incidents of his childhood, even though he invariably begins by saying, "I don't remember a thing."
How the brain stores its memories is still not fully known. Some scientists believe that each item of memory is contained in a loop of cells connected by tiny tendrils with an electrical current going around and around the loop, which might be hundreds or thousands of cells in length. Other theories suggest that the memory is somehow impressed, or "etched" on the cell, or exists on a chain of cells like knots in a string. We do know that for the first thirty to sixty minutes after being received, any sensory impression is "floating around," so to speak, in the brain, not yet firmly registered. This may be why, after a sharp blow on the head, people often permanently forget what happened to them during the previous fifteen or twenty minutes.
Be that as it may, the number of items that can be remembered is far greater than the total number of brain cells. Dr. Ralph W. Gerard, a neurophysiologist at the University of Michigan, estimated that after seventy years of activity the brain may contain as many as fifteen trillion separate bits of information. Thus your memory is a treasure house whose size and strength are almost beyond human comprehension. It is a pity that so many of us store up so much less learning and experience than is possible.
Since our senses report, automatically and continuously, everything that we see, touch, hear, smell or taste, the avalanche of impressions would be overwhelming if there were not ways to screen them out. Fortunately at many points in the nervous system there are tiny gaps, called synapses, which prevent millions of minor signals, such as a one-degree change in temperature, from
OUR HUMAN BODY
getting through. The electrical impression from any one nerve fiber is not strong enough to jump across one of these breaks, but the impression from a large bundle of fibers transmitting simultaneously can do so.
A good example of this protective mechanism is the retina of the eye, which has about 100,000,000 light-sensitive cells capable of transmitting an impression. But there are only about 1,000,000 nerve fibers leading back into the brain. Thus, before it can reach the brain, an impression has to be strong enough to command the response of at least 100 cells.
There are three main message centers in the brain. Each part receives and acts upon messages appropriate to its special functions. The medulla oblongata (see illustration) takes care of automatic functions like breathing and the pumping of the heart. The cerebrum with its covering of gray matter in turn is the seat of consciousness, memory, reason—in short, the human personality. The cerebellum controls the voluntary action of the muscles, partly on orders from the cerebrum. A reflex action, like with-
THE BRAIN
LEG CONTROL BODY CONTROL
ARM CONTROL HAND CONTROL FACE CONTROL
SPEECH
CEREBRUM
MEDULLA OBLONGATA
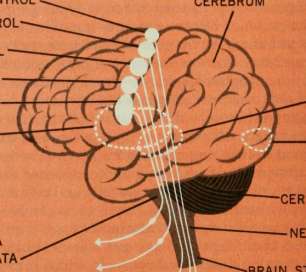
HEARING SIGHT
CEREBELLUM NERVE FIBERS
BRAIN STEM

drawing your foot when it is tickled, might be handled by the spinal cord alone.
The size of the brain area used by each part of the body is governed by the amount of conscious control the member requires—the more control, the larger the brain area. For example, the hands and fingers, which can perform highly complicated maneuvers, require a brain area much larger than that set aside for the legs. (The tongue and lips also require a proportionately big brain area.)
How are light, sound, temperature and the other aspects of the external world translated into seeing, hearing, feeling? All we know is that certain physical conditions cause our sense organs to transmit electrical messages to the appropriate receiving area in the brain, and that the quality of the sensation is determined by the pattern of impulses received.
While the brain is exposed during an operation, a small electrical charge applied to the nervous tissues where sight and hearing are recorded can make a patient see flashes of light or hear buzzing, ringing or knocking. Stimulation to a speech center will cause the individual to cry out like a baby but not to indulge in articulate speech, which is too complicated for such stimulation.
When these experiments are performed on individuals who are conscious (brain tissue is not sensitive to pain) they report that they do not feel as though some external force were causing the baby like cries to be uttered. On the contrary, they feel a strong but inward compulsion to cry out.
In many cases messages go simultaneously to more than one of the four main parts of the nervous system. Sometimes these centers are required to cooperate, sometimes not. You huddle deeper under a blanket on a cold night on orders from the cerebellum, but the message might also go up as high as the cerebrum and cause you to dream of the Arctic. But these are "low-priority" messages. An important signal, such as the smell of smoke in the night, alerts all the message centers, sets the electrical circuits flashing at a furious rate and leads to conscious action.
Many actions that require a great deal of conscious attention
the first time they are performed can afterward be shunted down into a part of the brain functioning at a lower, less conscious level. Riding a bicycle, swimming and other skills which initially demand thought (cerebration) gradually become automatic or reflex actions. We also learn to discard from consciousness unwanted messages that are many times repeated. Thus a city dweller sleeps through the sound of traffic but is awakened in the country by the crowing of a distant rooster.
What causes mental disturbance? In both retarded mentality and certain types of insanity there is damage either to the brain cells themselves or to their electrical processes.
Excessive anxiety, ungovernable rage and other unreasonable states of mind evidently result from electrical circuits that get out of control. Some mental illnesses seem associated with the inability to bring together a sufficiently large number of the reverberating electrical circuits of the brain. The deluded individual who thinks he is Napoleon is able to use the circuits that contain the name of Napoleon and the fact that he was a general. But he is unable to connect with these circuits the ones that should tell him that Napoleon was somebody else who died many years ago.
What constitutes genius? Presumably the highly gifted person has some inborn capacity to coordinate his electrical circuits unusually well. The more we learn, the greater the store of memories on which we will be able to draw. The more we exercise the function of combining hundreds of circuits into larger ones, the easier it becomes and the more extensive these circuits will grow to be.
The late Sir Charles Sherrington, the great authority on the brain, after pointing out that man's brain is, in proportion to his weight, far larger than that of any of the animals, suggests that its evolution is still continuing: "Nor is the brain's present state, we may suppose, more than an interim phase, on the way to something else, something better, we may hope."
Can any more exciting prospect be held out to mankind?
Your Brain's Unrealized Powers
by Bruce Bliven
Here are seven important facts, some turned up by recent re-. search, which can help you to use your brain more efficiently:
I.There is no such thing as '''brain fag.^^ Laymen often speak of "mental fatigue" or "brain fag," thinking that long, concentrated mental effort produces tiredness in the brain itself. Yet scientists believe that this state cannot exist. Your brain is not like your muscles. Its operations are not muscular but electrochemical in character.
When your brain appears tired after hours of mental work, the fatigue is almost certainly located in other parts of the body, your eyes or the muscles of your neck and back. The brain itself can go almost indefinitely.
A young woman undertook as an experiment to multiply in her head a series of two four-digit numbers, one after the other, as rapidly as possible. She went on doing this for twelve hours. During that time there was only a slight decrease in her efficiency, measured by speed and accuracy. At the end of twelve hours she stopped only because of bodily fatigue and hunger.
What seems like mental fatigue is often merely boredom. In
reading a difficult book, for example, you are torn between the desire to go on and the impulse to stop. According to Edgar J. Swift, psychologist of Washington University, it often is not fatigue that you feel but inattention and the inability to ignore distracting thoughts.
2. The brain''s capacity is almost inexhaustible. That part of your brain involved in thinking and memory, and all your conscious activities, has as its most important part ten or twelve billion minute cells. Each of these has a set of tiny tendrils by means of which an electrochemical message can pass from one cell to another. Thinking and memory are associated with the passage of these electrical currents. The wisest man who ever lived came nowhere near using the full capacity of his wonderful mental storehouse. (Quite possibly, people in general employ only lo to 15 percent of the capabilities of their brains.)
3. Tour IQ^ is less important than you probably think. Many of us have an unnecessary inferiority complex about our IQs—the figure that represents native intelligence as compared to that of the average individual. It is easy to score lower in such a test than you deserve. This might result from temporary ill health or emotional disturbance. So, if you have ever seen your score on an IQ test, you can be reasonably sure that your IQ, is at least that high.
What is the physical basis of high intelligence? Contrary to a common belief, it does not require an unusually large skull. It is likely to be associated with especially large numbers of surface convolutions in the cerebral cortex, the great top part of the brain. Highly intelligent people also have good blood circulation to the brain, bearing oxygen, glucose and certain other important chemicals. It is possible that a person with some very special talent—a mathematical or musical genius, for example—may have an unusually thick bundle of nerve fibers in one particular place in the brain.
But the physical endowment of your brain is far less important than what you do with it. The number of brain cells in an individual with an IQ of 100 (which is average) is large enough so
that, used to the full, it could far exceed the record, so far as memory is concerned, of the greatest genius who ever lived. A person of average IQ who industriously stores up knowledge and skills year after year is better off than a person with a very high IQ who refuses to study. Research by the noted Yale psychologist, Dr. Catharine Cox Miles, indicated that some of the most important men in history had no more than ordinary IQ,s.
Among them, for example, are statesmen such as Cromwell, John Adams and Lincoln; military heroes like Drake, Napoleon and Nelson; writers like Goldsmith, Thackeray and Emerson. All these men, to be sure, were above the average in intelligence; yet they ranked far below the most brilliant of the individuals studied. What they possessed in high degree was character, and the ability to keep plodding ahead until they achieved what they had set out to do.
4. Age need not prevent your learning. One of the commonest misconceptions about the brain is that as you grow older something happens to it causing the learning process to become more difficult. This is true only to such a minute extent that for most of us it is of no practical importance.
Learning is associated with ability to create new reverberating electric circuits in the brain, and as long as that power remains you can continue to acquire new knowledge and skills—even at ninety.
It is true that all old people suffer impairment of their physical powers, and that some experience a decline of mental power. The best current medical opinion is that, in both cases, what happens is a series of minor "accidents" to various parts of our marvelously complicated physiological mechanism. None of these may be serious by itself, but the total effect can be severe.
Impairment of the brain in the aged is associated with decreased circulation of the blood and the precious substances it carries, especially oxygen and glucose. This is probably why old people remember happenings of their youth more vividly than those of the recent past; the youthful memories were implanted when blood circulation was better.
Yet severe mental impairment occurs only in some elderly people. Everyone knows of men and women who are vigorous and alert mentally into the ninth or even tenth decade of life. Their existence proves that impaired mental powers are not an inevitable accompaniment of passing years, but a result of disease processes.
Science knows of no reason why the average person cannot continue to learn with at least 85 to 90 percent efficiency through the seventh decade and beyond. It would be a fine thing if retired people went back to school or college or began to learn new skills and subjects. On the false notion that they are "too old to learn" millions of elderly people cut themselves off from exhilarating intellectual adventures.
5. Tour mental powers grow with use. Like the muscular system of the body, the brain tends to atrophy with disuse, and to become better with exercise. This is proved by the fact that if the optic nerve is destroyed early in life, the brain cells in the corresponding visual area of the brain stay undeveloped.
As your brain matures, the nerve fibers arc surrounded with a fatty substance called myelin, and they do not function properly until this has taken place. A newborn baby lacks most of its myelin, which is one reason why we cannot remember much that happened before we are two or three years old. Many physiologists believe that intensive exercise of any part of the brain encourages the growth of additional all-important myelin.
Anything you do with your brain exercises it, though obviously there is more exercise in doing something difficult than something easy. The more reasoning you do, the easier it is to go on to new reasoning. The ability to memorize also improves with practice. Robert S. Wood worth, professor emeritus of Columbia University, estimated that the time required to memorize anything can, with practice, be reduced as much as two thirds.
Every aspect of your personality is stored in your brain. This includes your willpower, which is also developed by practice. Each time you exert your will to drive yourself to the completion of an unpleasant or irksome task you make it a little easier next time to do what you need to do.
6. The unconscious mind is a marvelous storehouse. The most wonderful part of your mind is undoubtedly the unconscious, which lies below the recoverable memory and is thousands of times larger. We don't yet know very much about the unconscious mind, but we are learning fast and someday may know how to tap its great powers.
Your unconscious mind contains many millions of past experiences that, so far as your conscious mind knows, are lost forever. By means of several devices we now know how to bring back lost memories. One method is "free association," used by psychiatrists. If a patient lets his conscious mind wander at will, it can give him clues to forgotten things which, skillfully pursued by the doctor, will bring up whole networks of lost ideas and forgotten terrors. There are certain drugs which also help in this process; hypnotism, too, can be of tremendous value in exploring a patient's unconscious.
Many psychologists believe that we can make more use of our unconscious minds. Innumerable people have found that they can profitably "talk to" their unconscious. Some people find that they can bid themselves to wake up at a certain time in the morning. You can sometimes even improve your tomorrow's mood if you will say to yourself when you go to bed—and believe it— that you will be more cheerful in the morning.
7. The ''''old''' brain and the ^^nevu'^ can he kept in proper proportion. Your brain may be described (with severe oversimplification) as having three parts: the upper, the middle and the lower. The lower section is where the automatic functions of the brain are performed—keeping the blood and lungs functioning, for instance. The midbrain participates in these operations but also serves as a bridge, to pass messages on to the upper brain or cerebral cortex. This top part of the brain is the single characteristic which most strongly separates man from animal.
The earliest living organisms on the earth had only a trace of the upper brain, or none at all; as we come down through evolution, the proportion steadily increases, which is why the upper is called the "new" brain. Even the highest of the primates, the
chimpanzee and the gorilla, have at most only one third as much upper brain as a human being.
While we have been developing the new brain, we have, of course, retained all the characteristics of the "old" one. When certain areas inside your skull are electrically stimulated, you will bite and scratch like an animal. To some extent, the old brain represents ruthless egotism, while the new is the seat of elaborate abstract concepts like honor, esprit de corps and beauty. Growing up represents the triumph of the new brain over the old.
Deep emotion in the old brain can blot out the circuits in the new brain which represent reason and foresight. The man who commits a murder in a sudden rage knows, with his new brain, that he is likely to be caught and punished, but he does not think of these things until his passion has subsided.
We must not, of course, try to live by the intellect alone or reject the legitimate and important demands of the emotions. Pushing down into the unconscious a legitimate emotional impulse can only cause it to fester there. We must, however, try to keep the old brain and the new in proper proportion to each other, remembering that when either gets the upper hand too completely the human being cannot properly fulfill his destiny.
Suppose there should suddenly be dumped into man's conscious mind a small part of what he had forgotten: Out of all his past, ten million faces would surge up from darkness into a dreadful glare;.a vast murmur of voices would gather out of silence and grow until it built pandemonium in his skull. In that sea of faces he would not find the few that had been dear to him; voices he had loved would be drowned in rapid chatter. The few good books he had read would be smothered under the ten thousand bad. Worst of all, he would search in vain among the trivialities, the broken purposes and the weak surrenders of his own past for that ideal self of which his weak memory had allowed him complacently to dream.
—Odell Shepard
Why Strokes Occur
Adapted from "Why Strokes Occur" by Irvine H. Page, M.D., and "What You Should Know about Strokes" by Tom Mahoney
The stroke which President Eisenhower suffered was not caused, as some news stories suggested, by worries over Sputnik. It was a so-called "little stroke," one of the commonest ailments of men in their sixties the world over. In all likelihood the stroke would have occurred even if the President had been living a calm, uneventful existence on his Gettysburg farm.
The word "stroke"—literally a striking down—has frightening overtones for most people. A stroke can be very serious, even fatal. But it can also be quite mild. A "little stroke" does not necessarily shorten a person's life and may impair his faculties only temporarily. It most certainly should not be looked upon as the end of a man's productive life.
Strokes, which doctors term "cerebrovascular accidents," or apoplexy, have advanced from seventh to third place among the natural causes of death, and are now behind only heart disease and cancer. More than 140,000 people in the United States are killed by strokes each year, and at least four times this number suffer nonfatal strokes. Yet stroke receives less attention than many maladies that affect fewer persons.
Often called apoplexy, a stroke occurs when the blood supply to the brain, or to some portion of it, is cut off. To perform its
vital functions the brain needs an enormous quantity of oxygen— 20 percent of the total amount consumed by the body. It gets this oxygen directly from the bloodstream. More than a pint and a half of blood must be circulated through the brain every minute. If brain cells are denied their quota of oxygen for even five minutes, they die. Once killed, they cannot grow back. Though this damage is irreparable, the brain's ability to perform all functions is often recovered. The area affected may be large or small.
A stroke usually takes place in the cerebrum, that part of the brain where nerve centers controlling sight, hearing, speech and bodily movements are located. These zones of nerve cells are on the surface of the cerebrum, and nerve fibers run from them deep into the brain and on down the spinal cord, carrying impulses between the zones and the parts of the body they afTect. If a blockage stops blood flow to one of these control zones, or to nerve fibers leading from the zones, then the activity controlled by the zone will be impaired. For example, if the nerve center controlling speech is damaged, the ability of .the zone to coordinate ideas and words and to send correct signals through the nerves to tongue and vocal cords is afTected. The victim will find his ability to speak impaired.
There are at least four ways in which a stroke can take place:
I. Clotting. In atherosclerosis, fatty substances like cholesterol accumulate on the walls of the blood vessels, narrowing the space through which the blood can pass. (Atherosclerosis is the most serious form of hardening of the arteries.) As the blood flow slows down, it may begin to stagnate. Tiny "platelets"—specks of chemical "dust" in the bloodstream—may begin to cluster on rough spots caused by atherosclerosis. Thus coagulation may form the core of a clot, or thrombus, which blocks the further flow of blood and produces a condition known as thrombosis.
Sometimes the artery seems to be closed by a nervous spasm. Occasionally the spasm relaxes or the brain manages to establish some circulation around the obstruction. When this happens, many of the impaired brain abilities return and much of the paralysis disappears.
Another form of clotting is called embolism. After surgery and under some other conditions, a blood clot, or embolus, may break away in the body and be carried through arteries to the brain, where it blocks a blood vessel. Embolus is from the Greek word meaning "a plug." When strokes occur in young persons, a cerebral embolism usually is responsible.
Once lodged in the brain, little can be done about an embolus. But administration of one of the "anticoagulant" drugs may prevent the formation of additional emboli or growth of the one already present. Anticoagulants also slow coagulation of the blood and prevent formation of emboli during surgery.
2. Hemorrhage. A brain artery may rupture. The blood escapes, damaging the surrounding tissue. Since the brain floats in cerebrospinal fluid and is encased by unyielding bone, much bleeding may also cause serious pressure on the brain. Cerebral hemorrhage—usually detectable by blood in the spinal fluid—is harder to recover from than any other type of stroke.
If the hemorrhage is massive, death may come swiftly. But most hemorrhages are small. There may be only a slow leakage of blood, only a few tiny arteries and capillaries broken down. The damage may not be enough to cause the patient to lose consciousness.
Some clots resulting from cerebral hemorrhage may be removed by surgery. Where the clot has not hardened, the surgeon may drill a small hole in the skull and drain the liquid clot through a hollow needle.
3. Compression. A tumor, swollen brain tissue or a large clot from a cerebral blood vessel may press hard enough upon an adjoining blood vessel to stop its flow.
4. Spasm. An artery of the brain may constrict and thus reduce or pinch off" the blood passage, the damage depending upon how long it takes the aff"ected artery to relax again. The specific role of spasms of the cerebral vessels and whether they actually occur in stroke are subjects of medical controversy.
The seriousness of a stroke depends upon which blood vessel is affected, the kind of blockage, how long the brain areas involved go without oxygen, plus a number of other considerations. In many cases, especially among younger persons, other blood vessels may take over the functions of the one blocked. Sometimes, even when certain brain centers have died, other areas of the brain are able gradually to take over.
On rare occasions the victim of a stroke may be a young person, even a child. In such cases the stroke results from some illness like rheumatic fever or extremely high blood pressure. It might also result from an aneurysm (a blood-filled pouch) of a blood vessel, which the child was born with. Surgery can often remove this difficulty and, if the rest of the circulatory system is healthy, the child can look forward to a normal life span.
The average age of a stroke victim is sixty-four. There has been a steady increase in the number of strokes among our people in recent years, because the number of elderly persons has been increasing. Elderly males seem to succumb more easily than elderly females. No reliable statistics are available on the frequency of recurrence of strokes, but it is generally agreed that, in most cases, a stroke victim is sooner or later stricken again.
If the stroke victim does not die—and he usually does not—a variety of things may happen to him. He may feel tired, numb, weak, stuporous or confused. He may show emotional or personality changes. He may have headaches and suffer disturbances of vision, speech or memory. He may lose sensation in certain parts of his body. He may not be able to walk. He may be stricken paralytically and have to lie in bed for years. There are about two million such incapacitated or handicapped stroke victims in the U.S.A. today. Many of them could be at least partially rehabilitated by properly supervised nursing care, adequate diet, massage and exercise.
What can you do to avoid a stroke? You can, first of all, have a thorough annual physical examination that will include checking your blood pressure and your heart action. Strokes usually do not come without warning signs.
Approximately one out of every four individuals with a blood
pressure of over 200 eventually may have a stroke, reported Dr. Harry J. Johnson, medical director of the Life Extension Examiners, an organization of doctors which has made nearly three million health examinations. Early detection of high blood pressure gives you the opportunity to reduce it. In doing so, you reduce your chance of having heart attacks as well as strokes.
Additional premonitory symptoms of stroke include: severe aches in the back of the head and neck, dizziness or fainting, motor or sensory nerve disturbances, nosebleeds and certain hemorrhages in the retina of the eye. These symptoms, however, can be found with other diseases and are not necessarily indicative of high blood pressure or pending stroke.
The causes of high blood pressure remain in dispute, but doctors have come up with several methods of controlling it: (i) avoidance of overweight and strain of all kinds; (2) various diets;
(3) surgery—the severing of nerves which constrict the arteries;
(4) drugs which temporarily relax the blood vessels. Happily the body is often capable of making its own repairs.
Some physicians advocate anticoagulants as a preventive measure. But there is no unanimity about the worth of this treatment; there is no certain evidence that it might not in some cases be harmful. Going on a low-fat diet in the hope of preventing a stroke is futile once atherosclerosis has made its subversive inroads.
A stroke is obviously not to be brushed aside lightly. On the other hand, one should not get panicky when one occurs. A little stroke might do no more than make the victim feel a bit ill and cause some slight, momentary disturbance of his faculties. Even a more severe stroke is seldom as severe as it seems at first. In the shock of the initial impact a victim and his family may feel that he is hopelessly paralyzed or has gone out of his mind. This is hardly ever the case. And it does no one any good, least of all the victim, if everyone acts as though the funeral notices had gone out. Even the severest cases can recover with astonishing rapidity.
A stroke does not necessarily mean the end of a career. Louis Pasteur, the great French scientist who fathered microbiology,
lived twenty-seven years and did his greatest work after suffering a stroke at forty-six. Sir Joshua Reynolds produced a hundred canvases after a stroke at fifty-nine. George Frederick Handel composed his immortal Messiah and lived for many years after a stroke.
Great advances have been made in the treatment and retraining of stroke patients by a number of hospitals, including those caring for war veterans. Special exercises, water therapy and electric devices are employed to restore function to limbs and teach undamaged brain centers to take over the tasks from those that have been injured.
Much, of course, depends on the patient's own courage and desire to regain his skills. It is humiliating for a man to have to learn to speak again, to have to teach his left hand to do what his right did, to have to learn to tie his shoes. He needs all the understanding that his friends and family can give him.
When Pasteur was stricken with a cerebral thrombosis, his condition seemed so hopeless that construction was stopped on a laboratory the government was building for him. Pasteur learned of this, and declined rapidly. His friends appealed to Emperor Napoleon HI, who ordered construction resumed. Pasteur then began to recover and in the new laboratory conquered rabies and half a dozen other diseases.
l>|o ROBOT could come even close to duplicating the human brain. A machine even remotely like it would have to be about the size of Rockefeller Center, and it would take several lifetimes to wire it up. The electrical-power requirements would be about equal to the power used now to supply the greater part of New York City. And the necessary cooling system would be so enormous that you'd probably have to divert the Hudson to supply it. —Dr. Norbert Wiener
121 PART 2 • THE HEART
Knowledge of the heart has become a very necessary part of our daily living. In a sense, each man has now become his own doctor, for it is not the wonders of heart surgery — marvelous though they are — but practicing good sense that preserves the human heart.
It is a wonderful machine. The following section reveals not only how it works but how you should keep it in working order.
The Heart-
WONDROUS, COURAGEOUS ORGAN
by Henry Morton Robinson
Don't worry too much about your heart, as so many healthy people seem to be doing nowadays; rejoice, rather, that nature has placed in your breast one of her most delicate yet durable marvels, an organ of surpassing patience, flexibility and strength. Rejoice, and try to understand how it works. It will work all the better for being understood.
Borrow a doctor's stethoscope, and listen to the beating of your own heart. In its steady rhythm— hihh-dup, hihh-dup —you will hear the sound of life itself as blood courses through the valves
and chambers of this inimitable pump. For the heart, mechanically speaking, is just that—a pressure pump which forces the blood, with its freight of oxygen, food or waste, through the vessels of the body.
Driven by the heart, the approximately six quarts of blood in the average human body make a round trip about once every minute. In twenty-four hours the heart receives and pumps out again between seven and nine thousand quarts of blood. In a life span of the Biblical three score years and ten, the heart \uhh-dups some two and a half billion times, without a single shutdown for repairs. And—so it seems to one listening through the stethoscope—without a rest.
Yet, without rest no muscle can endure, and the heart is a muscle. Though brief, the pauses between dup and the next lubb are rest enough. The normal heart, like man himself, spends twice as much time relaxing as it does at work. Besides, the heart draws extra rations. Though it weighs but 1/200 of the body's weight, it requires i /20 of the blood in circulation for itself.
Your heart is about the size of your fist and is snugly enclosed in a tough protective covering called the pericardium. Attached to the body only by the great blood vessels stemming from its base, it hangs within your chest, pointing diagonally downward toward your left breast. It is divided into two parts, right and left, by a blood-tight wall. Each part forms a separate pump.
And each of these two pumps, in turn, has two interacting chambers: the auricle, which receives blood into the heart from the veins, and the ventricle, which forces it out again into the body through the arteries. The heart's specialized muscles are so cunningly layered and interwoven that they can squeeze, twist and literally wring out the contents of their chambers at every lubb—in other words, at every contraction of the pump.
What causes the heart to beat? This question, asked seventeen hundred years ago by the anatomist Galen, was not answered until about 1890, when investigators began to suspect electrochemical energy. They were right. We now know that a kind of electrical timing apparatus called the pacemaker normally gen-
GIANTS OF THE BODY
123
erates, about seventy times a minute, a tiny electrical impulse which sweeps down and across the muscle fibers, causing them to contract.
The heart, then, is a kind of electromuscular pump, contrived by millions of years of evolution, for the purpose of keeping the blood circulating in two main circuits. One, starting from the left chamber of the heart, is the great systemic circuit, which the blood makes through the entire body for the purpose of maintaining its tissues. A shorter, independent circuit goes from the right chamber of the heart to the lungs, to let the blood discharge its freight of carbon dioxide and pick up life-renewing oxygen. This is the pulmonary circulation.
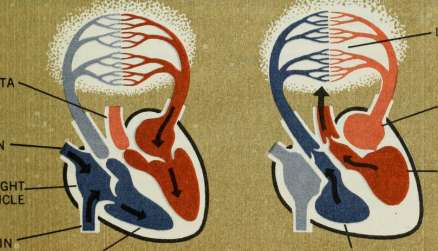
In order fully to understand the action of the heart, let us trace more precisely the course of the blood. Dark venous blood, laden with carbon dioxide and waste matter picked up in its progress through the body's veins, is drawn into the right auricle as the auricle lies momentarily relaxed. When the auricle is filled, the valve in its floor opens and the blood pours into the ventricle below.
When the ventricle is full, its smooth pumping pressure closes the valve, which bellies out like a parachute. This same pressure
THE HEART
COURSE OF BLOOD THROUGH THE HEART
AORTA
VEIN
RIGHT AURICLE
LUNGS
LEFT I AURICLE
LEFT ^
VENTRICLE
(contracted)
RIGHT VENTRICLE (expanded)
RIGHT VENTRICLE (contracted)
simultaneously opens another set of valves (half-moon-shaped) and forces blood out of the ventricle into the artery that leads directly to the lungs. In the thin-walled network of the lungs the dark blood is purified by exchanging its load of carbon dioxide for oxygen from the outer air. Thus freshened, the blood returns bright crimson to the heart—and the marvel of pulmonary circulation has been accomplished in less than ten seconds.
Meanwhile, the left chamber of the heart, more powerful than the right, carries on the next phase in rhythmic unison with the first. Fresh from the lungs, the blood enters the left auricle. When the auricle is full, the valve opens and the ventricle begins to fill. A fraction of a second later the ventricle contracts, pushing its cupful of blood into the aorta, the huge artery that leads out from the base of the heart. When the pressure in the aorta exceeds that from the ventricle, the half-moon valves between them close. The brisk dup that you hear is the sound of the valves as they slam shut.
From the aorta, widest of the rivers of life, the red flood branches out, ever more slowly, through arteries and arterioles and tiny capillaries, to every cell in the body.
The heart repeats this process of contracting and relaxing, of systole and diastole, \\ihh-dup, \nhh-diip, day after day, year in, year out, in disease and health, through sleep, love and battle, with the enduring constancy of time itself, with an efficiency not equaled by any of man's inventions, and a courage that passes all understanding.
In i8i6 in Paris, a physician, Rene Laennec, was consulted by a young and buxom female suffering from a heart ailment. Being too modest to put his ear against her bosom to listen to her heart, he tried a roUed-up piece of paper and found it conveyed the sound distinctly. This led to his famous invention—the stethoscope. —Freling Foster
Steady Pace or Heartbreak f
Adapted from "The World's Most Efficient Pump" by G. A. Skinner and "Stop Breaking Your Heart" by Howard Whitman
There is no man-made pump that compares in efficiency with the human heart. It is able to run a hundred years and more without the loss of even a few minutes for repairs.
Even this efficient machine needs care, for the causes operating to induce heart trouble are many. Probably among the first is rheumatic fever, found often among young people. This is very likely to leave the heart damaged, although the patient may seem completely recovered and may even indulge in quite heavy athletics for some years. But trouble develops in the thirties, as a rule, and in the fifties or earlier the person with this sort of heart may break down.
Then there is the rapid pace of present-day life, to which some ascribe much of the increase in the death rate from heart disease of recent years. Hearts today are as good as those of yesterday, except for the changed conditions under which they are forced to labor. Years of constant tension may lead to high blood pressure, increasing materially the burden on the heart. In time permanent damage is done which, if nothing more, restricts considerably the physical activities of the possessor.
Certain methods of exercise use up the reserves of the heart with undue rapidity. One of the most serious is the common custom, indulged in by many men who spend most of their time at desks, of trying to get a month's exercise, very strenuously, in a single day. Especially dangerous is it for such a man on a fishing or hunting trip to go into competition with guides and others who are physically active much of the time. His pride insists that he keep up with them and he does—but often at the cost of a serious heart strain. Youth withstands much more of this sort of strain than do middle or late life, as the elastic limit of the circulatory system is in youth much higher.
The same sort of strain takes place in comparatively young men who, splendidly trained athletes in college, have then let all training go. In the course of ten years or so they acquire a fine income, a family and probably thirty or forty pounds of surplus weight. They decide that something must be done. If exercise is taken in moderation and gradually increased as the body becomes accustomed to it, the results usually will be excellent. Often, however, the same vigor is used right at the start that was the habit of college days, and trouble is almost certain.
In order to remain at the greatest efficiency, the heart, like all other muscles, should be used not only reasonably, but regularly. Otherwise, the reserve built up in active days is gradually lost, and the heart gets "soft," unable to withstand sudden or prolonged strains. If, however, the individual takes a fair amount of exercise daily he is always in training and the heart will withstand astonishing loads, even in late life. It is the man playing often for short periods throughout his career who can play tennis in the late sixties, apparently without harm.
There is no set time that a man becomes old, but long observation has set fifty as the age to commence to slow down in every way, particularly in strenuous physical exertions, A man may boast that he is as good as he was at twenty-five, but he is not, no matter how much he may feel that way.
The greatest protection against heart attack, suggests Dr. Irvine H. Page, famed heart specialist of the Cleveland Clinic, is the "achievement of equanimity," "Some men can achieve this
intellectually," he comments. "They ask themselves, 'What kind of philosophy do I intend to live by?' And they find one which nurtures life instead of destroying it. Others achieve equanimity emotionally, through a belief in beauty, in ideals, in unselfishness. They let the annoyances of life pass in one side and out the other."
This does not mean that you should deliberately repress your emotions, however. When you get angry—and all of us do, at times—most doctors believe there is greater danger in holding your anger back than in expressing it. Dr. Henry I. Russek comments, "That's why we need 'gripe sessions' in our daily lives. Easy release of angry feelings not only lessens the danger of continuing inner pressure but makes violent blow-offs less necessary."
The Why and How of Heart Attacks
Adapted from "Stop Breaking Your Heart!" by Howard Whitman and "Candidates for Heart Attack" by George Dock
Many people have thanked God for their heart attacks. They have recovered to find a new life with greater satisfactions, more peace. But why do so many of us have to wait until we come within an inch of death to learn this lesson? Can't we learn how to live before the heart attack?
I put the question to a famous coronary victim, Kentucky author and poet Jesse Stuart, who suffered a heart attack some years ago. "People just won't listen," he said. "I wouldn't listen myself until the good Lord gave me a heart attack."
Just what is the lesson life is trying to teach? What is the truth to which people won't listen? It is this: A person's attitudes toward life, his emotions, are strongly linked to heart attacks. There are indications that they may be as important as such better-defined factors as overweight, diet and heredity.
The heart and the emotions are tied together in language we use daily: heartbroken^ heavy hear ted, heartfelt, heartache. Physicians in ancient times considered the heart the seat of the emotions but could not prove it. Modern physicians are at last proving the effect that emotions have on the heart's behavior.
A study by Dr. Henry I. Russek, U.S. Public Health Service consultant in cardiovascular research, and Professor Burton L. Zohman, of the State University of New York College of Medicine, found emotional stress four and a half times more prevalent in coronary victims than in people with healthy hearts. The coronary victim, they report, "commonly possesses an ambitious, driving nature and exhibits a consistent tendency toward compulsive striving, self-discipline and hard work. He frequently sets herculean tasks for himself, exceeding his normal capacity and tempo, minimizing warning signals and neglecting prudent rules of health."
Drs. Meyer Friedman and Ray H. Rosenman, of San Francisco, made a study of two specially selected groups of men. Group A consisted of highly competitive, ambitious men who were constantly fighting deadlines. Group B men were easygoing, with far less drive. Seven hundred percent more heart disease was discovered in Group A!
In a study of coronary patients at Temple University Hospital, Philadelphia, Dr. Edward Weiss and his colleagues found "gradually mounting tension" prior to the attack in 49 percent of the cases and "acute emotional stress" just before the attack in 37 percent. They checked an equal number of noncoronary patients
and found no instances of gradually mounting tension, and acute emotional stress in only 9 percent.
One of the patients was a forty-three-year-old machinist in charge of a number of machines in a large shop, who took pride in keeping them in perfect working order. Here's how he described his own "gradually mounting tension": "Everything was okay until the last few weeks. Then the boss started a speedup. The equipment broke down, and as fast as we could rebuild it something else would break. Work used to be enjoyable, but now I hated to get up in the morning. All the knocks I've had in life couldn't add up to this. When I saw my work being smashed to pieces, it broke my heart."
How can emotions break the heart?
"Under stress of emotion, adrenalin is poured into the bloodstream from the adrenal glands," explains Dr. Herbert Pollack of New York University Postgraduate Medical School. "This causes the smaller arteries to contract. The heart, in an effort to maintain full circulation in the face of this resistance, steps up the pulse rate and blood pressure. When the adrenalin secretion causes the coronary blood vessels to contract, the heart muscle is deprived of its full blood supply and the result is pain which we call angina pectoris. This type of adrenalin response may predispose an individual to actual permanent blocking of a coronary blood vessel—coronary occlusion."
Nature intends that shot of adrenalin to provide extra strength and alertness to meet whatever threat brought on the emotional surge. Primitive man found it useful in encounters with wild beasts. So does modern man when he fights a fire in his basement or snatches his child from the path of a car. But continual tension, repeated emotional emergencies—as though all of life were a crisis—is more than nature bargained for.
The damage usually begins long before a heart attack—in the narrowing of the arteries by the formation of fatty deposits in their linings. The process (atherosclerosis) which thickens the inner arterial wall also roughens it, and blood clots form more readily in contact with the rough surface.
Today there is evidence that emotional tension, in addition to
its direct effect on the blood vessels as described above, hastens the process of narrowing the coronary blood vessels by interfering with the metabolism of fats and overloading the bloodstream with the fatty substance—cholesterol—which thickens the arteries.
Cholesterol is an essential element of the blood. It is manufactured within the liver and is also absorbed from the cholesterol contained in certain foods—including animal fats, egg yolk, butter, cream and milk—the most valuable of all foods for infants, growing children and undernourished adults. Cholesterol is not found in fruit, vegetables, cereals or nuts. Lean meat and fish contain a little of it, and provide large amounts of protein, which seems to give the body the power to bum up some of the excess cholesterol in our blood.
Postmortems made upon thousands of Chinese revealed astonishingly few cases of coronary illness or the atheromata (fatty deposits in the walls of arteries) which are its forerunners. In China, rice and protein-rich millet and soybeans are the mainstay of millions. Eggs, milk and animal fats are almost unknown luxuries to them. The blood-cholesterol level of the average Chinese is little more than half as high as that of most Americans.
U.S. Army medical officers have been disturbed by the high death rate from coronary disease among American troops (especially in the lower age brackets) in training camps in the United States, where the per capita consumption of eggs, milk and fatty foods was far above the average peacetime intake.
British troops, who drank more tea than milk, and ate more bread and beef than ice cream and eggs, incurred a considerably lower death rate from coronary attack. So there seems to be a definite relationship between high-cholesterol diet and high coronary mortality.
Resistance to coronary disease is very much a matter of heredity, because of the importance of the inborn thickness of the arterial lining, which varies so widely among people of any age group. But the rate at which that lining takes on greater thickness and a rough surface is the deadliest factor in laying the individual open to coronary attack. Some experts believe it can be slowed down through dietary measures.
People vary in their ability to deal with cholesterol. Many persons keep their blood cholesterol at safe levels even on food containing a great deal of that substance. Others develop fatally high cholesterol on diets practically free from it.
It is well to remember that the problem of human diet is complex, that individuals vary greatly in their needs. We all know families whose members live to a vigorous old age on diets that fairly sag with cream and eggs and fats. But they may owe their long lives to a rare combination of congenitally thin coronary linings, some inherited mechanism for burning up surplus cholesterol and a healthy supply of protein in their fare.
A U.S. Air Force doctor, Colonel Marshall E. Groover, tested the blood-cholesterol levels in a group of Air Force officers under emotionally placid conditions and later under stressful circumstances. In some, emotional stress caused a remarkable rise. One officer had a cholesterol level, when calm, of 190 (milligrams per 100 milliliters of blood serum). After he got news that his son had quit school to be married, it spurted to 380.
Drs. Friedman and Rosenman checked the cholesterol levels of a group of accountants: the average was 210. But just before April 15, when the emotional stress of a tax deadline was upon them, their cholesterol level averaged 252.
What are the outward signs of the man who is building toward a heart attack? (It is most frequently a man. Statistics indicate that the death rate from heart disease in middle age is almost three times as high in men as in women.) Can we identify him in advance? Some doctors think we can select the men among whom coronary disease may develop.
"When one has studied 'younger' patients with coronary disease, one knows that they exhibit rather telltale characteristics," say Dr. Friedman and Dr. Rosenman, who have encountered many such ■ individuals at Mount Zion Hospital and Medical Center. "For example, these men frequently use emphatic gestures, particularly the clenched fist, to accompany their talking. They scan each day in advance to see how much activity they can squeeze into it, and how they can accelerate any project's pace. They hate to waste time.
"When you talk to the coronary-prone man, he often believes he knows what you're going to say before you've actually said it. He will sometimes finish your sentence for you, or his lips will silently finish it, or he may urge you on by saying 'Yes, yes,' at intervals."
In addition to the usually recommended regime of low-fat diet and moderate exercise, Drs. Friedman and Rosenman try to put such patients on a deceleration program. "Get up early enough so you won't have to rush," they say. "Cut out unnecessary activities, delegate duties that you don't have to do yourself."
The doctors use a timepiece as a symbol of their patients' trouble. Dr. Rosenman keeps track of the number of times his patients look at their watches during an interview—it may be as many as sixteen times in an hour. When he brings this to their attention, they get the point.
Most men can reduce the emotional stress in their lives without sacrificing mental creativeness and the enjoyment of full living. In my home town, for example, forty-nine-year-old Bill Torno runs a lumberyard. He had a heart attack on March 28. Now he calls it his "birthday." "That's when I learned how to live for the first time," he says. "Before the coronary I was always on the go. I felt that I had to be on top of every detail in the business—and every aggravation, too. Now I get to the yard at 8:30 instead of 7:30. If I see an aggravating argument building up, I just walk away from it. And you know something? The business runs better! I have time to think of the really important things."
Bill Leonard, CBS television and radio broadcaster, who had a heart attack at forty, observed: "Before it happened, I thought there was no excuse for not taking on more work. When a fellow got older, okay; but up to forty-five or fifty he ought to take on anything. Being tired certainly was no excuse."
When Leonard's coronary struck, he was doing nineteen radio and TV programs a week. The industry knew him as indefatigable. After the attack he said: "I simply don't try as hard, as much or as often. I'm lazier—and it doesn't bother me. I spend more time just doing things I like to do—playing bridge, taking long walks, playing golf."
Life is almost always sweeter for the man who has survived a heart attack. There are now many "Coronary Clubs" of happy men, but unfortunately thousands don't live to join them.
Can't we have a "JVo Coronary Club" for those who are smart enough to understand their peril before death makes them forever ineligible?
How to Live After An Attack
by Peter F. Steincrohn, M.D.
Many a man might be saved after a heart attack if he were - fortunate enough to break a leg also. The enforced rest would give his heart the opportunity to recover. But that isn't the whole story. Treating the heart properly doesn't depend entirely upon what you do for it those first few weeks after the attack. It's how you live forever after that matters.
Most people do not realize that the heart patient often lives with his disease for many years. Many cardiacs who have dreaded being shuffled off in a matter of days have lived twenty, thirty or forty years longer than they thought possible. Much needless illness and suffering can be avoided when the patient knows what the doctor is trying to accomplish.
All heart trouble isn't serious. Three out of four fearful persons who walk into the doctor's office have normal hearts. A fleeting pain in the left chest ("It's right over my heart"); the recent loss of a relative or friend ("Why, I saw Jack only yesterday and he looked perfectly healthy"); the desire for reassurance ("There's so much heart trouble around, Doctor")—these are only a few of the things that strike fear into healthy people.
On the other hand, many people who actually have heart disease don't visit their physicians for a checkup. John Jones refuses to chance "hearing the bad news." John Brown uses these excuses: "It's just because I'm slowing up," or "It's only indigestion." Yet the "acute indigestion" reported in former years was often heart disease.
Here is a simple formula, for the healthy as well as for the heartsick, that guarantees a smoother trip along the road to longevity:
First. Visit your doctor for a physical checkup if you have any of the following symptoms: chronic cough, spitting up of blood, fainting spells, asthmatic attacks, swelling of the ankles, gas pressure, tiredness, indigestion, palpitation, rapid pulse, shortness of breath, chest pain, dizziness or the inability to lie flat in bed.
Second. Listen only to what the doctor says. Specific advice for the individual should not come from sympathetic but untrained friends, from papers, periodicals or books.
Third. Get plenty of rest—rest—and more rest. This is the prescription par excellence for the tired heart. In no other disease is it so true that he who knows how to rest lives longest.
There are many kinds of heart disease: congenital, rheumatic, syphilitic, atherosclerotic, bacterial, among others. They are in many ways similar, but in more ways different. Medicine has appropriate drugs for each, but there is only one basic treatment. Call it a Way of Life. Without it most other treatment is useless.
Some years ago Dr. Charles Miner Cooper, a well-known San Francisco physician, wrote the following letter to a patient who had suffered a heart attack. Now practically a West Coast classic through wide circulation and reprinting, it contains sound advice even for those who are in good health.
Dear Mr. Blank:
You have evidently made an excellent recovery from your recent heart attack. That attack should have warned you to live a life which would lessen the work of your heart. However, you have continued to be overweight; you have been eating and drinking as much as you desire. You have carried on strenuous business activities, working long hours and often at top speed. You have not curbed your quick and, at times, rather violent emotional reactions. The load on your heart has been too heavy. Hence you now are incommoded by shortness of breath and other disturbing symptoms.
You come to me for advice, as you have gone to other doctors, perhaps hoping that I can give you a drug which will enable you to carry on as you have been doing. Unfortunately there is no such drug. But let me outline a regime which will help you immensely if, after a period of almost complete physical, mental and emotional rest, you will follow it very conscientiously:
1. You should bring your weight down to what is normal for your height, build and age. This reduction must be brought about slowly, by modifying your diet and by graduated exercises—not by reducing drugs. Refrain permanently from overloading your stomach on any occasion.
2. You must cut down the extent and speed of your physical activities. Do not run to catch a train, hurry up stairs, attempt to park an automobile in a closed-in space, or use any set of muscles to the limit of your vigor. Refrain from physical effort immediately after eating, and do nothing that will make you short of breath. If at any time you begin to breathe fast, or experience a constricting chest pain, lie down and rest.
3. You must indulge in mental tasks only when your mind is fresh, and cease them when you become weary. Thus you will be able to give your best consideration to business problems with the least strain to yourself.
4. You must curb your emotional reactions. When I tell you that I have known a patient's blood pressure to jump 60 points
almost instantaneously in response to an outburst of anger, you can understand what strain such reactions can throw upon the heart. I realize that you are quick on the trigger and inclined to blame those whose behavior incites you, rather than to consider yourself foolish for letting them disturb you. Such a viewpoint is not uncommon. The great Scottish surgeon John Hunter, suffering from much the same condition as you, and appreciating the effect of such emotional reactions upon his heart, said his life was in the hands of any rascal who chose to annoy him. Even he forgot that he should discipline himself, and he had a fatal attack during a fit of anger.
Whenever a business problem starts to vex you, or you begin to get angry, let yourself go limp all over. This will dissipate your mounting inner turmoil.
5. Try to be cheerful under all circumstances. Unfortunately, you are a moody man, given at times to considerable sadness. Such a state does not lend itself to the proper energization of the heart and blood vessels. It may seem to you that to be cheerful when you are inclined to sadness is easier said than done. Let me make a suggestion: Whenever you are feeling down in the dumps, think of some particularly pleasing worthwhile experience you have had. Your mood will often respond to the thought.
If you were a smoker, I should have to tell you to refrain entirely, as I believe tobacco to be injurious to those afflicted with degenerative cardiovascular lesions.
Your heart is calling for a complete change in your ways. It is further asking that it be permanently housed in a lean, cheerful, placid man who will intelligently curb his physical, mental and emotional activities.
I have a number of patients who years ago had the same thing happen to their hearts as has happened to yours. Today they are still enjoying a sense of well-being and are doing valuable work. You may similarly respond if you will seriously follow the foregoing regime.
137 PART 3 • THE BREATH OF LIFE
Magic in Breathing
by W. P. Knowles
During the past thirty years Captain William P. Knowles has been consulted by more than 60,000 sufferers from respiratory complaints. At the Institute of Breathing in London, which he founded, some §00 persons a year study correct breathing practice. In World War II Captain Knowles instructed RAF and Army personnel on ways to achieve physical fitness.
I have a theory that famous work songs, ranging from those of the Volga boatmen to the cadent melodies of the Negro, offered more than just a rhythmic beat to help in hauling that barge, or toting that bale. It's my belief that the songs encourage men to breathe out while they worked, to release air from the lungs in a moderate and orderly manner. You can't sing without exhaling gradually, and when you exhale you expel impurities and empty the lungs for a fresh and involuntary intake of air. Real breath control means learning to control the way we exhale, not the way we inhale. Energy is best renewed by the orderly release of breath, not by strenuously pumping the lungs full of air. Thus in sustained physical exertion—carrying a heavy bag, walking rapidly, wielding a garden shovel—your power is
enhanced when you concentrate on the slow expulsion of air from the lungs.
Speakers, singers, swimmers and runners know this. The rest of us can find it out by simple tests. When you step into a cold shower, for example, the tendency is to gasp and tense the muscles. This only increases the torture. If, instead, you try breathing out in a steady purring breath, you will be amazed at how slightly the temperature of the water affects you. Exhaling helps the body accommodate itself to change.
The next time you have something heavy to lift—whether it be a large pot of soup, a typewriter or a suitcase—try taking a full, deep breath and holding the breath while you lift. Much of the weight oddly disappears. The effect is like picking up a box expecting it to be full, only to find it empty.
Those who have played the game of levitation have found that a person or a table can be hoisted by the mere finger action of a group if all present breathe deeply and simultaneously as they lift. This illustrates the mysterious aid that comes from conscious and calculated use of breathing.
Careful breath control, with emphasis on exhaling, helps us to relax under any kind of tension or stress. Most of us are only half-breathers: we breathe in because we can't help it but we fail to breathe out completely. The result is that we sigh a lot— a sign of our need to exhale. The sigh is nature's way of deflating the lungs when we have neglected the breathing apparatus long enough. The sensible thing is to learn to sigh in a systematic and organized fashion. We know that any interference with breathing causes acute distress. It follows, as common sense and science show, that any improvement in our breathing can bring exhilaration to mind and body.
Normally we do breathe without apparent effort—about i8 times a minute, 1080 times an hour, 25,920 times a day. The more air we exhale, the more we can breathe in. The amount we take in, which can be measured by a watch-size instrument called a spirometer, is known as our vital capacity.
A thoughtful management and husbanding of breath can be
of practical daily aid, can tone us up and contribute visibly to our health and vitality. To increase our vital capacity is the object of all breath discipline. Thus consciousness of breathing out becomes the most important factor of all.
But the main thing is to cultivate the habit. Breathe out before you begin any task. Once you grasp the idea of correct breathing you will find rewards in a dozen different ways. Even in a day of escalators and elevators there are still stairs to climb—usually by puffing and panting. But try this: As you climb the first two steps, keeping the shoulder blades in position, breathe in. On the next two, breathe out. With a rhythm of two in and two out, two in and two out, you can glide up flights of stairs and arrive at the top without gasping for breath.
What happens is this: By quickening the breath rhythmically as we climb we expel a greater amount of carbon dioxide and take in a greater supply of oxygen.
The principle can be illustrated and confirmed further if we shorten our rhythm when we walk up a hill or long slope. In this case, breathe in while you take three paces and breathe out as you take the next three—three in, three out, keeping the shoulder blades in position. A hill that otherwise would leave you clutching for breath can be easily accomplished by this simple change in breathing tempo.
If some strenuous exertion without the right alteration in your breathing leaves you "out of breath," there is a simple way to get your breath back. Breathe faster. Pant like a dog for a few seconds. Then take a couple of full, easy breaths. Again pant and follow with a few full breaths. This will quiet your breathing much more rapidly than the forced effort to breathe naturally.
When a runner gets what we call his "second wind" it means that, at a certain point, he has unconsciously assessed his increased needs and countered the faster accumulation of carbon dioxide by a deeper and steadier intake of oxygen.
During World War II, I was asked to suggest a series of exercises for early-morning use by the Royal Air Force. Hangars and mess hall were cold; fuel was short. To warm up the men, I
prescribed the following routine: they were to inhale and exhale through the nostrils, rapidly at first, then slowly; quick, short breathing for thirty seconds, then slow and full breathing for thirty seconds. Repeated several times, the exercise makes the body glow with warmth.
What the unfortunate majority of us need these days is a breathing program that can help us at our desks or stoves or machines. Tenseness and even depression may be overcome by the following exercise: Place the shoulder blades as nearly together as you can without strain, then breathe out gently and fully. Pause, then inhale with a deep, slow, gentle breath until the lungs are comfortably filled. Breathe out slowly through the nose with a long sigh and without altering the position of the shoulder blades. Do this a dozen times and your depression should disappear. Why? Because you have stimulated and inspired your brain and eased the nerve tension with a fuller supply of life-giving oxygen.
In what is known as stage fright a person often seems to suffer from a mild form of suffocation. Actors and experienced public speakers know the benefits of breath control. Any of us can profit from the actor's practice of stopping in the wings and fortifying himself with several full breaths before entering a scene.
One of the best exercises to establish the habit of proper exhaling involves reading aloud. From a newspaper, read aloud on one breath as many words as you can without effort. Now count the number of words you covered. Tomorrow try again. See how much you can increase the length of your exhalation.
Practice with some favorite passage of literature or Scripture which you have memorized, such as the First Psalm. You probably won't get beyond "the seat of the scornful" on the first attempt, but after a dozen daily efforts you may get through the whole psalm on one breath.
Another effective way to practice controlled outbreathing is counting. Sit down comfortably in an upright position, breathe in gently and steadily to the count of 4. Pause a second and then breathe out to the count of 12. Next time breathe in to the count of 5 and out to the count of 15. Continue this practice until you
see notable progress. By the time you are able to breathe out to the count of 21 you will find that humming helps immensely to limit the amount of air you release. Humming as you breathe out gives you your own form of work song.
Many are the by-products of breathing out consistently, but the greatest of these is awareness. It introduces a sharp change in our regular habits and, in a sense, makes us repossess our bodies. Conscious breathing brings with it a consciousness of posture. You begin to realize that you cannot sit all hunched up and breathe well either in or out.
The average person goes around with his shoulder blades wide apart. By drawing the shoulder blades close together he accomplishes the incidental result of squaring his shoulders. But he also accomplishes far more: he frees the whole abdominal region of unnecessary weight and pressure and sets up arrangements for proper movement of the diaphragm. He is relieved immediately of some of the burden of breathing, for ordinarily we use part of our breath intake to lift the weight of our ribs and chest. Pulling the shoulder blades close together gives us a feeling of lightness in the abdominal region and prompts us to breathe deeply.
By practice we can make our breathing involuntarily good just as it is likely now to be involuntarily bad. The body responds to wise treatment, and a consistent effort to enlarge vital capacity by learning to breathe out will pay off. Good habits will take over and in turn become second nature.
In the strained circumstances of modern life automatic breathing is not sufficient for our needs. Sedentary or monotonous work habits call for new and consciously controlled rhythms. It will pay to test daily some of the suggestions offered here. Experience will demonstrate the constructive use we can make of a power we now overlook.
Our Lungs-
THOSE WONDERFUL WINDBAGS
by J. D. RaUliff
TTTe cramp them with poor posture and subject them to smog, V Y dust and industrial fumes. We inflate them half a billion times in an average lifetime—wear and tear that would destroy any man-made material. Despite such punishment these remarkable organs—our lungs—give most of us long and trouble-free service.
Wherever we live—frigid North, arid desert, sooty city—our lungs require air much like that found in a tropical swamp: hot, moist, dirt-free. If the smoke and dust we breathe ever reached the lungs' minute air passages, they would be clogged within hours. If bacteria gained admittance freely, we would die of flaming infections. To guard against such disasters, nature has devised an incredibly complex air-conditioning system.
Its wonders begin with the nose, whose special construction is a measure of its importance. Made mostly of pliable cartilage, it can be mashed and pummeled and still continue to function. Hairs in the lining of the nose screen out large dust particles, and its passages help warm the air. Most of this warming task, however, is accomplished in deeper nasal passages, where the bones are covered by tissues with an enormously rich blood supply. Air
passing over these tissues is warmed like air passing over a radiator. On cold days the blood vessels dilate to produce more heat; on warm days they shrink.
As part of the elaborate humidifying system, glands leak fluid into the nasal passages—as much as a quart a day. Added moisture comes from tears that constantly bathe the eyes and spill over into the nasal passages through tear ducts. Here, too, the war on bacteria, which we breathe by the millions each day, gets underway. A remarkable enzyme called lysozyme, one of the most powerful bacteria-destroyers known, turns up in tears and mucous secretions.
The inspired air still contains a potentially lethal burden of dust particles. To help get rid of them, airways are lined with glands which secrete a sticky film of mucus. It acts much like flypaper in trapping dust particles. This "flypaper" would be hopelessly clogged with dirt in a short time but for another remarkable mechanism: air passages have their own sweeping system. Microscopic cilia—hairs—cover the entire route, and flail back and forth twelve times a second. Moving faster in one direction than the other, they sweep debris upward —toward the throat. Swallowed, it will be harmless in the digestive tract.
The incredible energy of the cilia can be demonstrated by snipping a bit of tissue from a frog's throat. If placed on a table, the cilia will "walk" the tissue off the table. If placed in a bottle, the tissue will climb out!
At times we tax the capacity of these cleaning mechanisms— for example, when we smoke too much. In a futile effort to trap countless millions of smoke particles, the throat secretes excess mucus. The mucus itself becomes an irritant and must be coughed up. In a cough, air is trapped in the lungs by the glottis, the valve at the upper end of the windpipe, or trachea, which carries air to the lungs. When the valve opens suddenly, air rushes out with explosive force. Thus the cough, which we may consider a nuisance, is actually essential to life—as an emergency cleaning measure.
Normally we take eighteen to twenty breaths a minute, using
OUR HUMAN BODY
only about one eighth of our lung capacity. With each breath we inhale about a pint of air. Since resting lungs hold six pints, only a sixth of the air is changed at a time. During violent exercise, when cells are hungry for oxygen, deeper and more rapid breathing can bring into the lungs ten or more times the oxygen supplied during rest.
The lungs are not simply inflatable bladders; they are among the most complex structures in the body. Cut through, they look something like the cross section of a rubber bath sponge. Each lung has its own duct from the windpipe; it enters near the top and starts branching like a tree. The branches are the bronchial tubes. Their job: to deliver air to the functioning part of the lung, those 750,000,000 microscopic air sacs called alveoli. All together
GLOTTIS
NOSE
BLOOD VESSELS
ALVEOLUS
LUNG
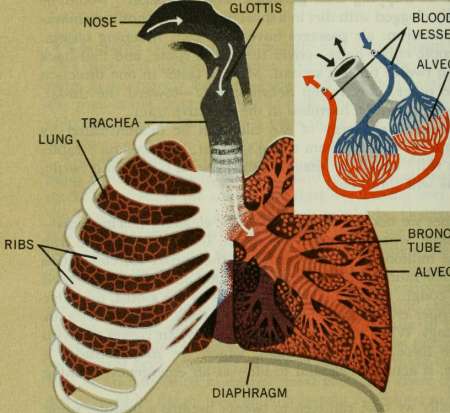
RIBS
BRONCHIAL TUBE
ALVEOLI
THE RESPIRATORY SYSTEM
they have a surface area 25 times that of the skin; spread flat, they would cover 600 square feet.
Each alveolus has a cobwebby covering of capillaries, so tiny that red blood cells must pass through them single file. Through their gossamer walls the blood gives up waste carbon dioxide and takes on refreshing oxygen. Every few minutes the body's entire supply of blood must pass through these minute blood vessels— in one end a dark blue-black, out the other a bright cherry-red. Day and night this all-important work must proceed without interruption.
Breathing itself is an intricate process. The lungs hang loosely in the chest, each in a separate compartment. (The heart is between them, in its own compartment.) Around them is a partial vacuum. Therefore, when the chest is enlarged, the vacuum tugs the lungs outward, thus sucking in air. Expansion of the chest is brought about by either—or both—of two methods. The diaphragm, the sheet of muscular tissue which divides chest from abdomen, may drop downward. Or the ribs, which are hinged to the spine, may swing outward. Expiration is simply a recoil mechanism.
Until the 1930s the chest was generally taboo territory for the surgeon, for once it was opened the lungs, no longer in a partial vacuum, would collapse and breathing would cease. Then came improvements in anesthesiology—chiefly the increased use of tubes which can be slipped down the windpipe so that the anesthetist can rhythmically force air and oxygen into the lungs. With this innovation a brilliant new day dawned for chest surgery.
Omoking two cigarettes is enough to impair a person's night vision, according to Dr. Charles Sheard of the Mayo Clinic. A vasoconstrictor, the nicotine cuts the flow of blood to the retina, causing a 15- to 30-minute delay in the time eyes require to adjust themselves to dim light. It is because of this that Army Air Forces training manuals advise against smoking before night flights. —Science Digest
How Harmful Is
Smoking f
Adapted from "How Harmful are Cigarettes?" by Roger William Riis and "Lung Cancer and Cigarettes" Lois Mattox Miller
In all the history of human habit, there have been few changes . so remarkable as the tidal-wave increase in cigarette smoking. Within our lifetime a new habit has taken hold to an extent we do not begin to realize, and with effects that we certainly do not understand.
In the United States, in 1961, 61 million people consumed 488 billion cigarettes. Two out of three men, two out of every five women, one out of every five boys at the end of their freshman year in high school smoke cigarettes. The average consumption is eleven cigarettes a day. Some 7.1 billion dollars a year are spent on tobacco products, considerably more than are paid to all the public-school teachers in the United States.
Up and up runs the graph at a towering angle, with no sign of leveling off. Americans are, at a lively pace, being engulfed in one giant nationwide cloud of cigarette smoke.
What is this substance which we breathe into our mouths and lungs in such stupendous clouds? It contains a number of ominous-sounding chemicals. Two of the chemicals are under
grave suspicion: benzopyrene, which chiefly affects the respiratory tract, and nicotine.
Nicotine
Nicotine is the essential ingredient of tobacco. It is what makes tobacco tobacco and not just another weed. When one smokes, most of the nicotine escapes into the air. About a third gets into the mouth, where a little is absorbed. Of what goes into the lungs, perhaps a fifth is absorbed. A pipe gives one a trifle more nicotine than does a cigar.
The hotter the burning surface, the more nicotine is taken into the system. Thus, the faster one smokes, the more nicotine one gets; smoking twice as fast results in ten times as much nicotine. And the closer to the end of a cigarette one smokes, the more nicotine also, because the butt, having filtered the first part of the cigarette, has more than its share of nicotine.
In pure form nicotine is a violent poison. One drop on a rabbit's skin throws the rabbit into instant shock. The nicotine content of a trifle more than two cigarettes, if injected into the bloodstream, would kill a smoker swiftly. If you smoke a pack a day, you inhale 400 milligrams of nicotine a week, which in a single injection would kill you quick as a bullet.
In factories which make nicotine insecticides, cases of acute poisoning occur now and then. One worker sat on a stool the concave seat of which held a little spilled nicotine. In less than two minutes he fell to the floor, blue in the face, apparently dead. Rushed to the hospital, he recovered quickly, as one does from light nicotine poisoning. But when he returned to the shop and put on those nicotine-soaked trousers again, again he fell headlong on the ground, and had to be revived a second time.
In the 488 billion cigarettes we smoke each year there are nearly twenty-eight million gallons of nicotine. Administered with precision, this is enough to kill a thousand times the population of the United States—a wild idea, of course, but nevertheless suggestive of nicotine's lethal power.
If nicotine is such a poison, then why doesn't smoking kill us?
Partly because the remarkably adjustable human body can gradually build up a tolerance for larger and larger doses of poison; partly because, in smoke, it is not accumulated in sufficient quantities. Just what the harmful effects of smoking are, the reader will judge for himself from the following evidence.
Smoking and Health
First, no doctor claims that smoking soothes the throat. The argument, as an editorial in The Journal of the American Medical Association put it, hinges on "the extent to which cigarettes irritate the throat." If you smoke a pack a day, you take in 840 cubic centimeters of tobacco tar in a year. That means that you have drenched your throat and lungs with 27 fluid ounces, or 15 full cocktail glasses, of tobacco tar containing benzopyrene.
The brown stain in filters or on your handkerchief when you blow smoke through it is not nicotine, for nicotine is colorless; it is incompletely burned tar products, like the soot in a chimney. Many physicians suspect that its main constituent, benzopyrene, though an irritant rather than a poison, is a greater threat to heavy smokers than nicotine.
In the matter of irritation, it is far more important how you smoke than what you smoke, whether you puff briskly or gently, how far down the butt you smoke, how long you hold the smoke in the mouth and lungs. Rapid smoking increases the irritation because it brings the smoke into the mouth at temperatures up to 135° Fahrenheit.
Do cigarettes affect the stomach and digestion? Every smoker has noticed that a cigarette seems able to still the pangs of hunger for a while. This is not a delusion. The sensation of hunger is caused by contractions of the stomach walls, and smoking can suppress these contractions. By the same process, smoking interferes with the appetite and thereby with good nutrition. Excessive smoking may also cause gastritis. By favoring an accumulation of acid secretions, it brings about heartburn. Relief comes in a matter of hours after the smoking stops.
Excess acidity of the stomach provides the kind of climate
ulcers like. The most recent work in this field, done by New York University, showed that patients who continued to smoke during treatment for their peptic ulcers had more relapses than those who did not, or those who had never smoked at all. In Boston, doctors had an interesting case some years ago, a man who had all the symptoms of duodenal ulcer. Even the X ray showed it. But an operation found no ulcer at all. The patient stopped smoking, under orders, and his "ulcer" left him. Three months later, feeling quite well, he took up smoking again, and back came the "ulcer." This time the doctors ordered him off cigarettes completely. Since he stopped smoking, he has had no more "ulcers."
Antitobacco crusaders assert that pregnant women should never smoke. Doctors have worked on this point for years and are clearer about it than about almost any other aspect of smoking. The conclusion: Smoking does not do pregnant women any more harm, or any different harm, than it does anyone else.
Two pediatricians in Philadelphia analyzed mothers' milk for nicotine content. They found 1.4 parts in ten miUion among moderate smokers, 4.7 parts among heavy smokers. But they could detect no effect whatsoever on the babies.
Where staying power is demanded, tobacco lowers athletic performance. At the Aldershot Army School in England a three-mile cross-country run is a required event. Over seven years the performance of almost 2000 men was analyzed, in groups of heavy smokers, moderate smokers, nonsmokers.
The heavy smokers, 8 percent of the total, drew 9 percent of the last ten places, but only 5 percent of the first ten. The moderate smokers, 73 percent of the total, got 62 percent of the first places and 83 percent of the last places. The nonsmokers, 18 percent of the total, took 32 percent of the firsts and only 7 percent of the lasts.
Nonsmokers, in four years at Yale and at Amherst, grew more in height and weight and lung capacity than did their smoking colleagues. At Yale the increase in chest development of the abstainers was 77 percent better, their increase in height 24 percent greater.
At Wisconsin students were asked to hold a small metal point
in a small hole, trying not to let it touch the sides. Electrical connections registered the number of times it did touch. Regular smokers were 60 percent more unsteady than nonsmokers.
Coaches are almost unanimous in saying that muscular power is lowered and fatigue begins earlier in smokers. Nowhere is there any medical evidence—despite the advertisements—that smoking improves an athlete's abilities.
What does tobacco do to the heart? As to the long-run effects, medical opinions differ. As to the immediate effects of cigarette smoking upon the mechanism of the heart and upon the arteries and veins, there is no difference of opinion, for these effects are easy to observe and measure.
Smoking speeds the pulse by as much as 28 beats per minute. In this respect individuals vary, and the same individual varies at different times. The average increase in pulse due to smoking is ten beats. Smoking can produce arrhythmia, an irregular stop and jump of the heart which often thoroughly frightens its owner. Habitual smokers have a 50 percent higher incidence of palpitation of the heart than nonsmokers.
Smoking raises the blood pressure, markedly and quickly. The higher your blood pressure is, the more sharply does tobacco lift it. Apparently the blood pressure does not develop any tolerance for tobacco, as does the digestive system. Nevertheless, smoking does not cause permanent high blood pressure. When the smoking stops, the pressure falls slowly to normal.
Smoking constricts the blood vessels, especially those of the feet and hands. The smaller the blood vessel the tighter is it constricted, and often smoking closes the tiny vessels under the fingernails entirely. As soon as one starts a cigarette, the rate of blood flow in the hands decreases to less than half normal, and it stays down for about an hour. The temperature of hands and feet drops.
Nicotine constricts the veins; alcohol dilates them. When we drink and smoke at the same time, we are in effect prodding ourselves with a pitchfork to get a lift and beating ourselves on the head with a club to offset it. Hence the popular belief that taking a highball offsets the effect of taking a cigarette. Doctors at
Rochester, Minnesota, went into this interesting possibility, making 121 tests on 65 persons. The winner was nicotine; it was more potent than alcohol: "the constricting effects of smoking cannot be prevented by alcohol."
, There is no proof that smoking causes heart disease. But there is evidence that heart disease is more prevalent among smokers than among nonsmokers, and that smoking may intensify existing heart disease. Virginia doctors, in an article on angina pectoris, point out that "coronary disease develops before the seventh decade significantly more often in smokers than in nonsmokers." The chief difference of opinion among doctors is as to how much damage smoking does to the heart. All doctors agree it can damage sick hearts. It is, in short, never a help and often a menace. It seems reasonable at present to agree with the recent statement of the committee on smoking and cardiovascular disease of the American Heart Association, that present evidence "strongly suggests that heavy cigarette smoking may contribute to or accelerate the development of coronary disease or its complications, at least in men under the age of fifty-five."
Lung Cancer: The Royal College Report
Will cigarettes induce cancer? The increase in lung-cancer mortality shows a suspicious parallel to the enormous increase in cigarette consumption in the United States. From 1930 to 1959, lung-cancer death rates increased nine times. At the present time cancer of the mouth and respiratory tract kills 37,000 men and 7000 women annually in the United States.
"It is probable that lung cancer soon will become more frequent than any other cancer of the body unless something is done to prevent its increase," declares Dr. Alton Ochsner, former president of the American Cancer Society and director of the famous Ochsner Clinic in New Orleans. "It is frightening to speculate on the possible number of [lung] cancers that might develop as a result of the tremendous number of cigarettes consumed in the decades from 1930 to i960."
Out of London in March, 1962, came a chill blast which
sobered cigarette smokers and jolted the tobacco industry on both sides of the Atlantic. The venerable 444-year-old Royal College of Physicians, which never deals with trivia or sensationalism, completed an exhaustive study and published a fact-filled report, Smoking and Health, "intended to give, to doctors and others, evidence on the hazards of smoking so that they may decide what should be done." The Royal College report stated unequivocally:
• "Cigarette smoking is a cause of lung cancer and bronchitis, and probably contributes to the development of coronary heart disease and various less common diseases."
• "Cigarette smokers have the greatest risk of dying from these diseases, and the risk is greater for the heavier smokers."
• "The many deaths from these diseases present a challenge to medicine; insofar as they are due to smoking they should be preventable."
• "The harmful effects of cigarette smoking might be reduced by efficient filters, by leaving longer cigarette stubs, or by changing from cigarette to pipe or cigar smoking."
The report had immediate repercussions in Parliament. It also stirred some nervous activity in Washington, where bureaucrats and Congressmen had dodged or pigeonholed the smoking-health issue for the past ten years. Tobacco-industry spokesmen issued the standard rejoinder that the evidence was merely "old data without new research findings," but the statement sounded weaker and more pathetic than ever.
Sir Robert Piatt, president of the Royal College of Physicians, commented: "Naturally every possible opposition has been raised to the idea that these diseases are due to cigarette smoking. But not one of the opposing theories will hold water, whereas everything confirms the evidence against cigarettes."
"During the past forty-five years," the report explained, "lung cancer has changed from an infrequent to a major cause of death in many countries. To account for this increase, it is necessary to postulate some causative agent to which human lungs have been newly and increasingly exposed during the present century. Cigarette smoke is such an agent and there is now a great deal of evidence that it is an important cause of this disease."
Since 1953 at least twenty-three investigations in nine different countries have reported on the relationship between lung cancer and smoking. "All these studies," the report states, "have shown that death rates from lung cancer increase steeply with increasing consumption of cigarettes. Heavy cigarette .smokers may have thirty times the death rate of non-smokers. They also have shown that cigarette smokers are much more affected than pipe or cigar smokers (who do not inhale) and that the group which had given up smoking at the start of the survey had a lower death rate than those who had continued to smoke."
This strong statistical association between cigarette smoking and lung cancer "is supported by compatible, though not conclusive, laboratory and pathological evidence." Some sixteen substances capable of initiating cancer in animals have been identified in tobacco smoke. In addition to these carcinogens, the smoke contains a variety of irritants which cause "precancerous" changes. These have been noted in the lungs and bronchial tissues of smokers who have died of causes other than lung cancer.
The Royal College report devotes a full section to the theories advanced by those who doubt the cause-and-effect relationship. "None of these explanations fits all the facts as well as the obvious one that smoking is a cause of lung cancer."
How about air pollution, onto which the tobacco propagandists try desperately to shift the blame? In Smoking and Health, the investigators point to the lung-cancer death rates of smokers and nonsmokers who live in cities, in rural areas and even in countries where air pollution is virtually unknown.
Finland, for example, which has the second highest lung-cancer death rate in Europe is essentially a rural country which has little air pollution but a population of heavy smokers. "This suggests that smoking is more important than air pollution," the report concludes. Moreover, "it is clear that at all levels of air pollution cigarette smokers suffer a risk of lung cancer which increases with the number of cigarettes smoked, and even in the most rural areas of the United Kingdom heavy cigarette smokers develop lung cancer fifteen to twenty times as frequently as non-smokers."
"Patients with bronchitis, peptic ulcer and arterial disease should be advised to stop smoking," the Royal College suggests to doctors. "Even a smoker's cough may be an indication that the habit should be given up."
The report observed that the proportion of nonsmoking British doctors has doubled in recent years from 24 percent in 1951 to 50 percent in 1961. "The doctor who smokes cigarettes must, like any other individual, balance these risks against the pleasures he derives from smoking and make his choice. But the doctor who smokes will lessen the effect of public education concerning the consequences of the habit and will find it harder to help his patients who need to stop smoking."
The Royal College report is not the first comprehensive analysis to be made of the smoking-health problem. But it is probably the best factual statement, buttressed by over 200 citations of scientific sources, to be written in the plain English which the average layman can understand. (Besides being widely summarized in the British press, the first 15,000 copies of Smoking and Health were sold out on publication and it since has become a best seller.)
Smoking and Health is also the first report to spell out a practical program of preventive measures for the individual and the government. Some specific recommendations:
More public education, and especially of school children, concerning the hazards of smoking. "The Central Council for Health Education and local authorities spent less than £5000 [Si 4,000] in 1956-60, while the Tobacco Manufacturers spent £38 million [Si07 million] on advertising their goods during this period. Such public education might advise safer smoking habits (filter tips, longer stubs, preference for pipes or cigars) for those whose addiction is too strong to be broken."
More effective restrictions on the sale of tobacco to children ("cigarettes are freely available in slot machines"). Wider restrictions on smoking in public places.
Raising the tax on cigarettes, and perhaps lowering taxes on pipe tobacco and cigars. ("Pipe smokers incur a considerably smaller risk than cigarette smokers. The risk in those who smoke
only cigars is even smaller and may be no greater than that for non-smokers.")
•"Since filters vary in efficiency, it would be desirable to have them tested by some official agency and have the results indicated on the packet."
The Royal College report was immediately subjected to full Parliamentary discussion, and Enoch Powell, the Minister of Health, informed the House of Commons: "The Government certainly does accept that this demonstrates authoritatively and unquestionably the causal connection between smoking and lung cancer and the more general hazards to health of smoking." The report's recommendations, he said, "are under consideration by the Government."
Whither Washington?
The forthright British approach was in sharp contrast to the timidity with which the health services, regulatory agencies and legislators in Washington, D.C., had up to then shied away from the clearly defined issue of smoking and health. In 1959 the Surgeon General of the U.S. Public Health Service published in the Journal of the American Medical Association a lengthy report which covered much the same ground as the current Royal College report, and accepted the causative role of cigarettes in lung cancer. But, unfortunately, some of the Surgeon General's colleagues had written into the report a brief paragraph which downgraded and dismissed filter tips even as partial health protection, and the Federal Trade Commission seized upon this convenient excuse to sweep the whole issue of the tar and nicotine content of American cigarettes under the carpet.
There have recently been, however, encouraging signs of a change of heart. Dr. Michael B. Shimkin of the National Cancer Institute has come out publicly in support of the American Cancer Society's proposal for a federal ruling that packages be clearly labeled with the tar and nicotine content of the cigarettes.
Following the publication of the Royal College report (but
only then), it was disclosed that a House Appropriations subcommittee had heard the testimony, in closed sessions a month earlier, of physicians from the National Institutes of Health. They stressed the overwhelming evidence linking cigarette smoking with lung cancer and other diseases, and urged an educational campaign on the hazards of smoking.
The FTC, apparently, has been holding its own closed-door meetings to find some way out of its quandary. The trade paper Advertising Age quoted Byron H. Jacques, head of the FTC bureau of trade-practice conferences and industry guides, as admitting: "If there is really a significant difference in the health hazards involved in filter tips compared with nonfilters, some change in our attitude might be necessary."
The FTC has long argued that it needs scientific authority and new legislation to handle the job properly. But many well-informed Washington lawyers maintain that the federal government (Food and Drug Administration, FTC, or USPHS) has all the authority it needs under present laws, including the broad Federal Hazardous Substances Act, which went into effect in July, i960. Many cigarette manufacturers state, privately, that they would welcome package labeling and standardized testing— but (for sound legal reasons) only if the government takes the initiative and tells them what to do.
On June 7, 1962, the U.S. Government at last took a significant step—but a first step only—when Surgeon General Luther Terry announced that he was about to appoint an advisory committee of experts to study the effect of cigarette smoking on health. The committee's study, said President Kennedy, would take several months and "go into '63." Meanwhile, this observation in a well-known British medical journal. The Lancet, should be pondered in Washington: "Future historians will have views on our failure to find even a partial solution to the problem of smoking during the first ten years after its dangers were revealed. The enormous and increasing number of deaths from smoker's cancer may go down in history as a strong indictment of our political and economic ways of life."
CHAPTER



Our
Sentinels
STANDING by, night and day, the remarkable sentinels of the body—eyes, ears, nose, throat and skin— keep us in constant contact with the world around us, introduce us to its delights, protect us from its dangers. To know the structure and function of these amazing organs is to marvel anew at the complexity and precision of nature's master plan.

What Your Skin Does for You
by Ruth and Edward Brecher
Have you ever wondered, after bruising or cutting yourself, why nature didn't supply you with a tougher hide? Scientists have an answer. Your tender skin, they report, is far more than a protective covering: it is an organ ranking with the brain, heart and lungs in its importance to human life. It performs services of which you are hardly aware—services which would be hampered if it were a tough, thick hide.
Consider what happens when you cut your finger. At once blood gushes from the tiny blood vessels in the skin, washing out dirt and germs. Then the blood vessels constrict so that the flow diminishes, and soon a clot of rapidly hardening blood fills the gash. Like glue it attaches itself firmly to the two sides of the cut, then gradually shrinks, drawing the sides closer together.
As the hours pass, threadlike connective-tissue cells called fibroblasts invade the clot from all sides, gradually building up new tissues. Once the gap has been solidly filled in, surface skin cells begin to grow from the two edges until they meet in the center, leaving only a hairline scar or none at all.
Each step in this process occurs at just the right time. Remember this when next you cut or burn yourself, and don't try to
scrape off the scab. You might interrupt important steps in the healing process, and be left with an unnecessary scar.
Your skin is a storehouse—and a remarkably roomy one, too. If you weigh 150 pounds, you are carrying about 25 of those pounds in your skin, mostly as fats and water. When your body takes in more of these than it requires, some of the excess is deposited in your skin. Later on, the skin can return stored materials to the bloodstream for transportation to organs which need them. Salts, sugars and other essentials are similarly deposited in your skin.
Your skin can also provide emergency blood rations to vital organs. Suppose that while walking down the street you are unexpectedly assaulted. Your muscles and internal organs immediately demand more blood for fight or flight. It comes partly from your skin, where small blood vessels shrink or collapse and bigger emergency channels open up to provide a rapid shortcut for blood hurrying to the regions of need. As this blood leaves your skin you "turn pale with fear," or with anger.
The blood vessels of the skin help keep your temperature normal. When your body gets too hot, they expand so that more blood flows to the surface of the skin and is cooled. When you go out in the cold, the skin's blood vessels contract, less blood enters the skin and internal heat is conserved.
The sweat glands in your skin are also temperature-regulating devices. When you get too hot, these glands secrete sweat, which evaporates and cools you.
Your skin is studded with nerve endings, some of which respond to warmth, some to cold, some to pressure, some to pain, itching or tickling. The nerve endings provide your "sense of touch," which works in a remarkable way. From early infancy until your skin becomes wrinkled in old age, it is generally a bit too small for you, and is therefore gently stretched. If the degree to which it is stretched changes, you feel that you have been "touched."
Thus when you rub a pencil gently along your skin, it is not really the pencil you feel but the change in stretch which the
OUR HUMAN BODY
pencil produces in your skin. You may "feel" the pencil even when it only touches the hairs of your forearm, for each hair touched disturbs some nerve endings ever so slightly.
The skin you wear today isn't the same skin you wore last year; invisible shedding goes on from hour to hour. Your skin has three major levels: an outer collection of layers (the epidermis), a middle layer (the dermis) and an inner (or subdermal) layer. In the lower part of the epidermis is a thin sheet of cells where most skin growth occurs. Each cell in this sheet divides from time to time, forming new cells which are crowded slowly upward to the surface. The trip may take weeks. On the way, each cell dies, and its exterior disintegrates into microscopic specks of scale.
Some twenty or more layers of scale form the surface of your skin. These invisible fragments of dead cells are constantly being rubbed off and replaced. If the skin surface is scraped so that it loses its tiny scales more rapidly than is normal, the rate at which new cells are formed is trebled or quadrupled.
The outer layer of scales is thickest on the fingertips, palms
CROSS SECTION OF THE SKIN
SWEAT GLAND
ERECTOR MUSCLE OF HAIR
HAIR