Care with Abortion Pills and/or Herbs
Two days after President Donald Trump’s inauguration, an editor from the United Kingdom approached me with an assignment—reporting on the likelihood of DIY (self-induced, “do-it-yourself ”) abortion taking over the country now that the federal government was under Republican control. It didn’t take me long to learn that it was a topic at the front of everyone’s mind. In April 2017 Women Help Women announced the launch of an online support service called Self-Managed Abortion: Safe and Supported (SASS) to offer information and counseling to those trying to end their pregnancies through abortion-inducing medications outside a clinical setting. As SASS’s US spokesperson Susan Yanow told the Guardian, “People are not being advised to use the pills. They’re being advised if they’ve already decided to use the pills. What drives this project is the knowledge that women have been managing this on their own.”34
Those who want to end a pregnancy but either can’t access a clinic or prefer to manage their own abortions have been using herbs and abortion pills since long before Trump’s surprise electoral win. Herbal abortions have existed for as long as there have been midwives, medicine women, and pregnancy. Today’s herbal abortion attempts are often far less effective due to misleading or incorrect information on the Internet and no medically vetted, detailed directions on how to use herbs correctly that the general public can easily access. Herbs also tend to require action as early as possible in the pregnancy and are a long-term commitment since they take time to work.
Using medication (mifepristone plus misoprostol or misoprostol alone) to effectively induce a miscarriage, however, is a much more recent (and effective) option. Mifepristone (RU-486) was approved by the FDA for use in the US in 2000 and offered as a medication-only option for terminating a pregnancy outside an abortion clinic. As part of a protocol developed first by the FDA and later streamlined by medical professionals through their own clinical use and more than a decade of research, patients were now able to obtain medicine in the clinic and take the dose of mifepristone there, then take misoprostol home to finish the termination in private. Current research shows that medication abortion can and is being used to easily and safely end pregnancies independent of a clinic and with minimal risk to a patient—at least, minimal medical risk. The biggest health risk for self-managed abortion care using abortion pills is that those who attempt to induce their own abortions may not seek out medical assistance in the rare case that there is a complication, fearing a doctor or hospital may then report them to law enforcement.
Again, to be clear, multiple studies from mainstream medical journals state that medication abortion conducted independent of a provider is a safe and effective means of ending a pregnancy—as long as the person terminating is not forced to hide their actions out of fear of legal punishment. It is the criminal code—not the medications themselves—that makes self-managed abortion care risky.
The following sections are reprints of information found on the Internet or taken from medical sources, and are simply a compilation of what information has been published regarding herbal and medication abortions in a nonclinical setting. This is not meant to encourage any decisions regarding abortion care. In many states in the US it is illegal to purchase medications online from outside the country, and in some states it is illegal to purposely terminate a pregnancy if you are not a medical provider or if you are doing it outside a hospital or clinic. However, it is not illegal to research or to share scientific and medical information, especially when that information is about health care that may affect more than half of the population.
This is only information, and not legal or medical advice. If a person were seeking information about self-managing an abortion using medications and herbs, this is the type of information that they would find by searching the Internet.
Herbal Abortion
It isn’t easy to find information online about inducing miscarriage with herbs, and googling brings up a lot of nonspecific information (“ingest a lot of Vitamin C” or “insert parsley into your vagina”). Sometimes that information conflicts with other sources and some instructions can be potentially dangerous. According to those with experience in herbal abortions, there are a lot of misconceptions on the Internet, especially when it comes to how and when herbs should be used.
In general best practices, using herbs to try to induce a miscarriage must be done as soon as a person believes they may be pregnant in order to have any potential success, and even then there is no guarantee that it will work. According to Sister Zeus, the reference point for most of the at-home herbal abortion information on the Internet (but again, not a medically vetted or endorsed site), if an abortion hasn’t been successful by about six weeks (two weeks after the period should have arrived), it’s unlikely it will work at all.35
By sorting through multiple websites one does find a few commonalities, usually involving the use of parsley. One site suggests that as soon as a person realizes their period is late, that person should insert fresh parsley into the vagina, removing and replacing it with new sprigs every twelve hours, while also taking a tincture of between two and six tablespoons of a parsley infusion every four hours (a tincture should be made by adding one ounce parsley stems to two and a half cups of boiling water, removing the water from the heat, and then allowing the mixture to steep for one to two hours). In addition, a person should also ingest five hundred milligrams of vitamin C every hour, maxing out at six thousand milligrams a day.
As you can see, even these instructions are still frustratingly imprecise, and the results are only partially guaranteed, which is why so few people manage to successfully induce miscarriages using herbs. Even more alarming is the assumption that just because something is “herbal” rather than medication based, it can’t harm you.
In Argentina, where an August 2018 attempt to legalize abortion in the first trimester failed to pass the senate, a woman died just days after attempting to induce her own miscarriage using herbs. According to reports, the thirty-four-year-old woman named Elizabeth already had a two-year-old and, unable to obtain an abortion in Argentina, attempted to induce labor by inserting parsley into her vagina. When an infection developed, she was afraid to go to a hospital out of fear of jail for attempting her own abortion, waiting until she developed sepsis before seeking care. Her uterus was removed, but she died anyway, another victim of the country’s abortion ban.36
Remember—herbal doesn’t automatically mean safe, either in miscarriage induction or in any other setting.
Medcation Abortion
Unlike herbal abortion methods, which can be unreliable, long, labor intensive, and potentially ineffective or dangerous, medication abortion has been extensively studied. Misoprostol alone is effective in ending a pregnancy before twelve weeks 80 to 85 percent of the time. Mifepristone plus misoprostol is effective in ending a pregnancy before ten weeks 95 to 98 percent of the time.
Medication abortion as it is conducted in a clinic is actually a combination of the two medications—two hundred milligrams of mifepristone and eight hundred micrograms of misoprostol. Mifepristone will reduce the progesterone in a person’s body by blocking progesterone receptors, ending the pregnancy. Misoprostol causes contractions, expelling from the womb the products of conception. Misoprostol is taken after the mifepristone, with the time interval depending on whether people place the tablets vaginally or buccally (between the cheek and gums).
People have also learned that miscarriage can be induced by using Misoprostol alone, although that is a bit less effective than the combination of the two medications. Those who research abortion-inducing medications often find that accessing misoprostol is easier than locating mifepristone and using the two medications together.
Where People Find Medications
Many people are likely to look online in order to find websites where they can either purchase misoprostol or mifepristone plus misoprostol in a “combipack,” or find information on where to purchase those medicines. The website www.abortionpillinfo.org is one place where information can be found. If a person were to click on “Information about abortion pills” and then the question “How can I find abortion pills?” they would learn the following:
- That abortion in the first twelve weeks of pregnancy can be done safely using misoprostol alone (80 to 85 percent effective) or mifepristone plus misoprostol (95 to 98 percent effective). Abortion pills cause a miscarriage if used correctly.
- Misoprostol is available in pharmacies, with a prescription. Misoprostol is used to prevent ulcers in people with conditions like arthritis that require them to take nonsteroidal anti-inflammatory (NSAID) medication long-term.
- Misoprostol is available from some Internet veterinary supply stores and veterinarians, as it is used to treat ulcers and arthritis in dogs.
- Misoprostol is available over the counter in many Latin American countries.
- Online pharmacies in Canada sell misoprostol inexpensively, and it has been reported that some may not require a prescription.
- Combination packs of mifepristone and misoprostol together are also available on the Internet.
In October 2017 a study was conducted to determine how reliable it was to get abortion pills from online pharmacies outside the US. A report on which websites were found to sell authentic medicines can be found on the Plan C website at https://plancpills.org/need-pills#options at the link “Report Card” and is also printed later in this chapter. The average cost of mifepristone plus misoprostol from these sites was reported to be $85–$200.
According to the Plan C site:
Online pharmacies—A Google search for “buy abortion pills online” will give many options for purchasing products. In early 2017, we ordered from sixteen different sites and received pills from fourteen of them . . .
. . . All of the pills we received contained the labeled active ingredients. Some of these sites accept credit cards, others require wiring money from a bank account or Western Union. The cost of the pills, including shipping, averages about $200 for an abortion “kit” containing both mifepristone and misoprostol. Buying misoprostol (Cytotec) alone may be less expensive (but is less effective than using both mifepristone and misoprostol). None of the websites we ordered from asked for a prescription.
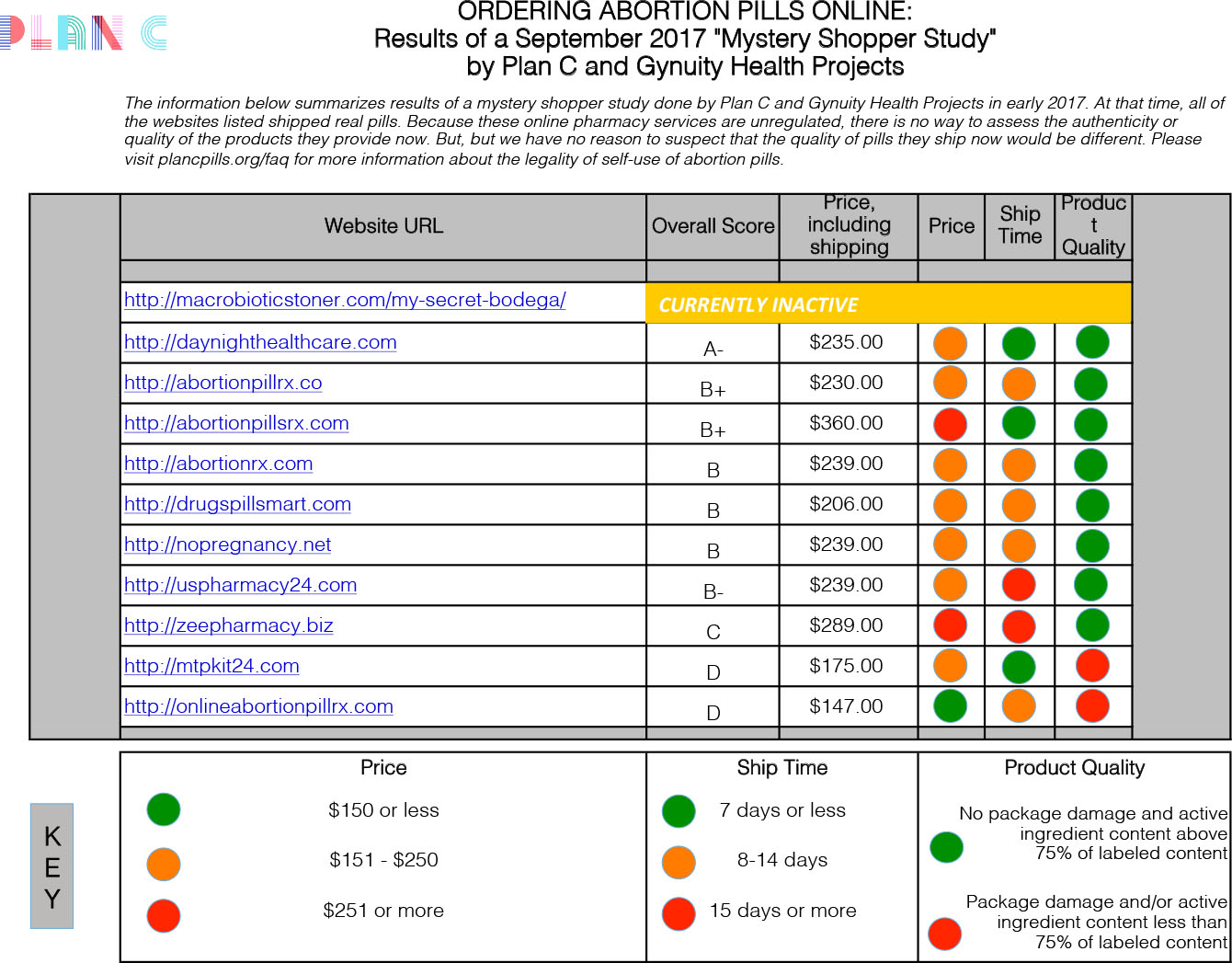
Source: Murtagh C, Wells E, Raymond EG, Coeytaux F, Winikoff B. Exploring the Feasibility of Obtaining Mifepristone and Misoprostol from the Internet. Contraception. Published online October 11, 2017. http://www.sciencedirect.com/science/article/pii/S0010782417304754
Please note that our findings reflect purchases made in early 2017. Because these online pharmacy services are unregulated, there is no way to assess the authenticity or quality of the products they are providing currently, but we have no reason to suspect that the quality of pills they ship now would be different.
Also, be aware that certain states—Hawaii, Maine, New York, Oregon, and Washington State—are currently allowing abortion pills by mail through the TelAbortion Study. Please visit www.telabortion.org for further information if you live in one of those states.
How Are Mifepristone and Misoprostol Used to End a Pregnancy?
These instructions are replicated from the Women Help Women website, an open-sourced information-sharing site about World Health Organization protocols ((http://consult.womenhelp.org/en/page/401/how-should-i-take-the-pills):
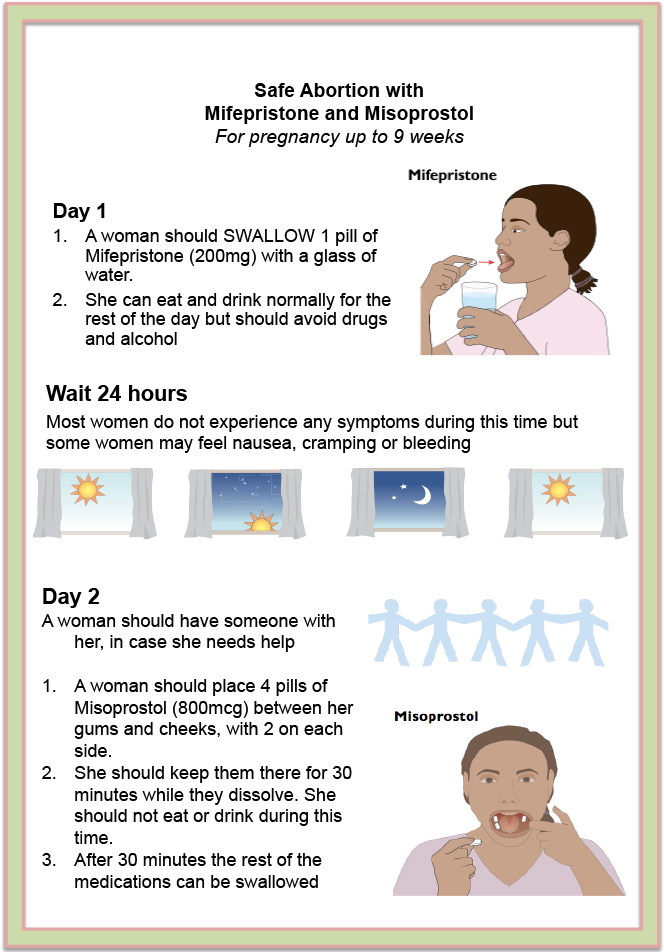
These instructions are for a pregnancy that is up to ten weeks (seventy days). The evidence suggests that mifepristone plus misoprostol is very safe and effective to ten weeks. After twelve weeks, there is a higher chance of a complication and the medicines are used differently.
1. Mifepristone should be swallowed with a glass of water.
2. Twenty-four hours later the woman should put four pills of misoprostol buccally (between the gum and the cheek).
She should put two tablets into her mouth, between her gum and cheek, on the left side and two more tablets between the gum and cheek, on the right side.
All four pills should be left in the mouth for approximately thirty minutes to dissolve. Women shouldn’t eat or drink anything while the pills are dissolving. Anything left in the mouth after thirty minutes should be swallowed. Before and after using the misoprostol she can eat and drink normally, but should not use drugs or alcohol; she needs to pay attention to her body.
How Is Misoprostol Alone Used to End a Pregnancy?
Again, according to Women Help Women (https://consult.women-help.org/en/page/434/how-should-i-take-the-misoprostol-pills):
These instructions are for a pregnancy that is up to twelve weeks (eighty-four days). These instructions are based on the recommendations of the World Health Organization. After twelve weeks, there is a higher chance of a complication and the medicines are used differently.
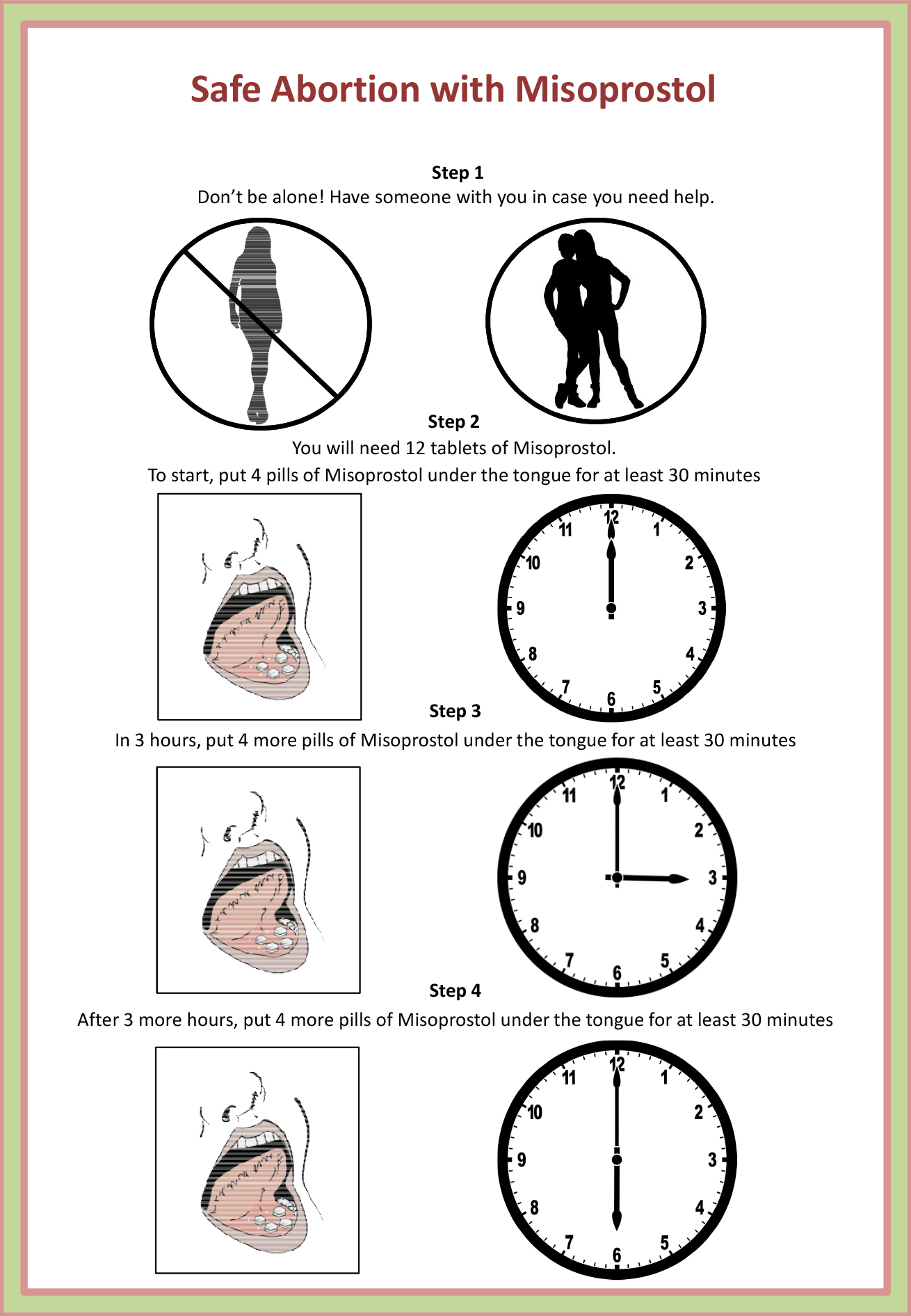
A woman will need a total of twelve pills of two hundred micrograms each.
1. A woman should put four pills of two hundred micrograms (in total eight hundred micrograms) misoprostol under the tongue. Do not swallow the pills for at least thirty minutes until the tablets are dissolved! (She can swallow her saliva, but NOT the pills. After thirty minutes it is okay to swallow what remains of the pills.)
2. After three hours she should put another four pills of misoprostol under the tongue. Do not swallow the pills for at least thirty minutes, until the tablets are dissolved.
3. After three hours she should put another four pills of misoprostol under the tongue again for a third time. Do not swallow the pills for at least thirty minutes, until the tablets are dissolved.
In between the doses of misoprostol, a woman can eat and drink normally.
The success rate is approximately 84 percent.
This means that eight to nine women of every ten women who use misoprostol correctly will have a safe abortion after this procedure.
Can People Share Information About Using Abortion Pills?
While conducting an abortion outside a clinic setting may not be legal in all circumstances, sharing open-sourced information is always legal. Please be aware that this is publicly available information based on the World Health Organization (WHO) protocol, and is not meant to encourage a person to induce a termination of pregnancy.
These graphics are available for reprint and can be shared online, as printouts or handouts, posters, pamphlets, or in any other form. Feel free to copy and distribute them on campuses, on bulletin boards, at political marches or demonstrations, or any place you think it would be good to get the information out to the general public.
The originals can be found at the Women Help Women website: https://consult.womenhelp.org/en/page/434/how-should-i-take-the-misoprostol-pills
https://consult.womenhelp.org/en/page/117640/whw-safe-abortion-with-misoprostol-english2-pdf
Stickers encouraging people to learn more about safe use of abortion pills can be found at https://abortionpillinfo.org/en/page/352/want-to-help. These can also be reprinted and circulated.
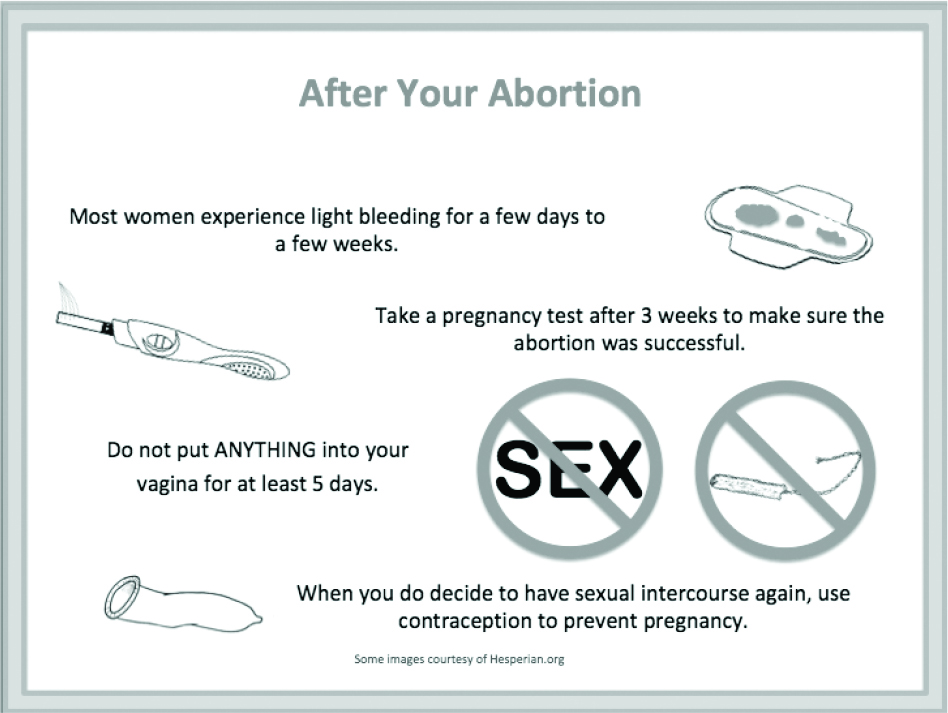
Aftercare
Information on post-abortion care is also available online. A very simple protocol can be found at Women Help Women (womenhelp.org):
Medical Risks
According to an article published in the BMJ in a study of one thousand women in Ireland who accessed medication abortion via Women on Web (www.womenonweb.org/en/i-need-an-abortion) because abortion was illegal in their country, nearly 95 percent of them were successful in ending their pregnancies without surgical intervention. Less than 10 percent of the patients reported symptoms that were alarming enough to suggest they should seek out medical advice, and there were no deaths.37
Public information about potential medical risks and symptoms of a possible complication can be found at the Women Help Women site at https://consult.womenhelp.org/en/page/417/what-to-do-in-case-of-emergency.
The information on the page reads as follows:
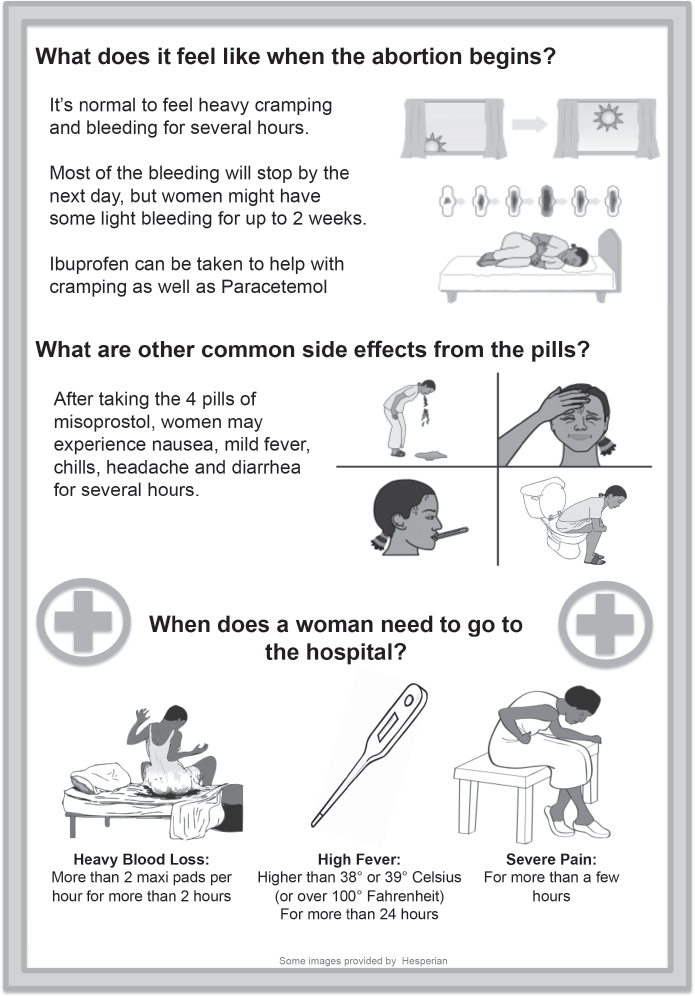
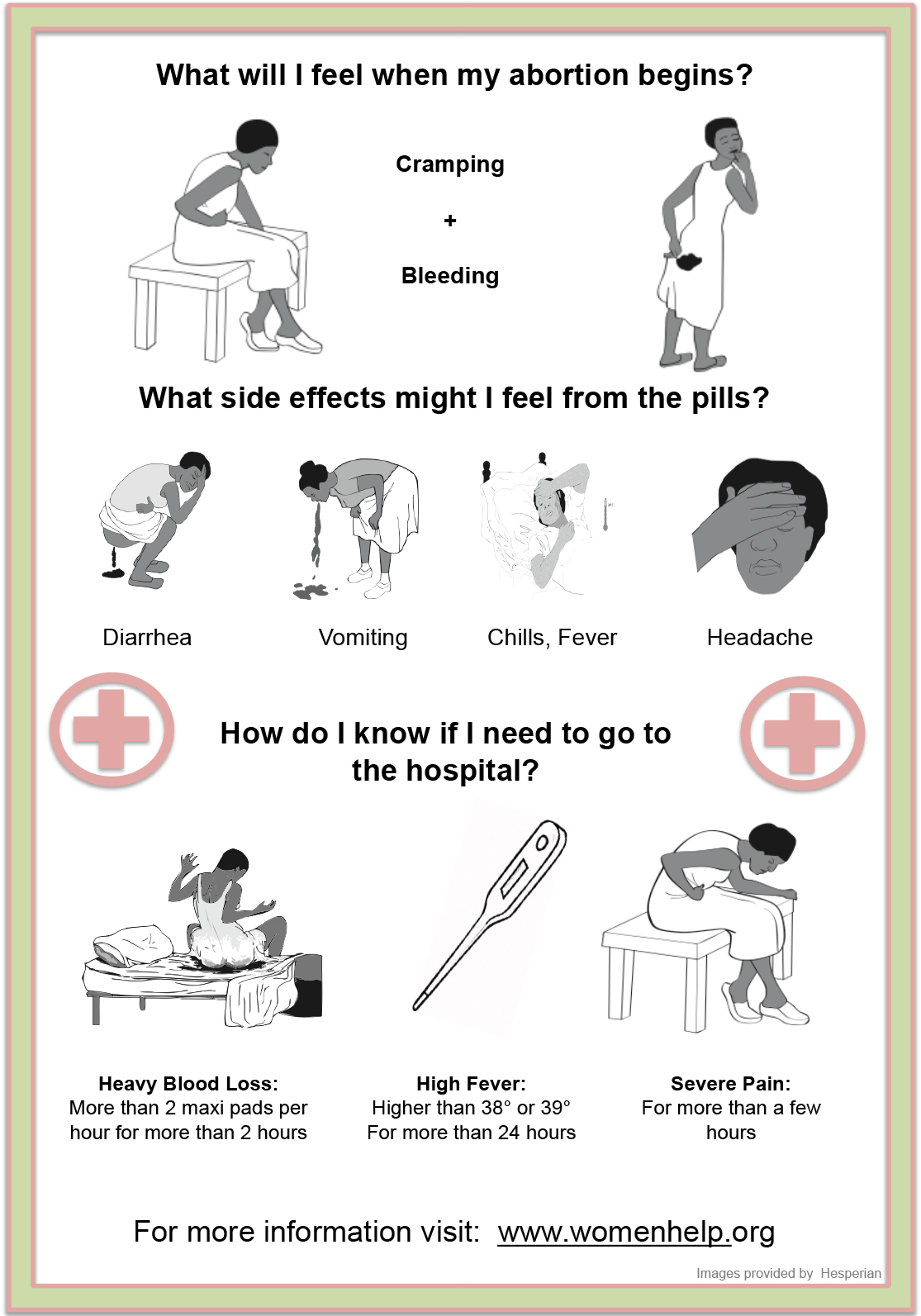
Complications after medical abortion are rare, and include severe bleeding and infection. You should go to the doctor or hospital if you have any of the signs of complication below:
- Severe bleeding (more than two or three pads used every hour for more than two or three hours)
- Severe abdominal pain that isn’t relieved with painkillers or continues for two to three days after taking the pills
- Fever over 39º or 38º for more than twenty-four hours (over 101º F)
- Abnormal vaginal discharge
The risk of a complication is low (two to five women in every one hundred), and the need for emergency care (that might be needed in case the woman suffers from heavy bleeding) is extremely low (one in every two thousand women). However, to make the process as safe as possible, it is important to be near medical care in case of an emergency or a complication throughout the process of abortion. If a woman lives far from medical care, she should use the medicines where she can access medical care, preferably within one or two hours. She should also plan how she would get to medical care (by car, taxi, or in case of emergency by ambulance).
If possible, the woman should choose a hospital or doctor where she knows that women having miscarriages are treated respectfully.
If a woman seeks medical attention, she does not have to say she used medicines. She can say she is having a miscarriage. The symptoms and treatment of a complication of miscarriage are exactly the same as those of abortion.
Misoprostol cannot be detected in the blood or any bodily fluids within a few hours after use. Even if a hospital claims that they can check to see if a woman took medicines to cause the miscarriage, it is not true.
How Can Medical Risks Be Minimized?
If a person has begun a self-managed abortion outside a clinical setting and has questions but doesn’t want to seek out medical help at this point, there are other options available to them. If they are in the US and need assistance, they should go to SASS and fill out the contact form at https://consult.womenhelp.org/en/contact-sass. This is a secure portal and there will be no electronic trail after the Q and A session. All questions are answered by skilled counselors from Women Help Women (womenhelp.org) who speak English and Spanish and are located outside the US.
Legal Risks
There are multiple legal risks that can come with self-inducing an abortion, and not just for the person who is terminating the pregnancy. Even with Roe in place, nearly two dozen people have been jailed for various crimes associated with allegedly inducing abortions, ranging from murder, homicide, and feticide to failure to report a death or properly dispose of remains, child endangerment or negligence, and being in possession of a drug without a prescription.
Unsurprisingly, it is people of color who tend to get the most severe punishments. Because prosecutors and other law enforcement officials typically pursue the “crime” of self-induced abortion at their discretion, racial bias becomes a large factor in deciding who should be investigated and to what extent they should be charged.
“Whether they are choosing to end a pregnancy or continue one, low-income women and women of color are more likely to be the target of investigations and prosecutions, as they are less likely to be able to access private medical care and more likely to regularly encounter police and other government officials in their day-to-day lives. In the post-Roe world, women themselves, and low-income women and women of color in particular, are at more risk of criminal prosecution for abortion and other pregnancy outcomes than at any other point in history,” explains the National Institute for Reproductive Health in their report, When Self-Abortion is a Crime: Laws That Put Women at Risk.38
Those who may be seen as “assisting” in a self-induced abortion could face charges as well. One Pennsylvania mother was jailed for providing abortion-inducing medications to her daughter because there was no nearby clinic.39 Other potential charges could include “unlawful termination of pregnancy” for someone who may live at the same address or whose computer or phone was used to purchase medicines, or “accessory” charges if they are found to have helped cover up an illegal abortion during an investigation.
According to the Self-Induced Abortion (SIA) Legal Team report Roe’s Unfinished Promise, “There are seven states with laws directly criminalizing self-induced abortions, ten states with laws criminalizing harm to fetuses that lack adequate exemptions for the pregnant person, and fifteen states with criminal abortion laws that have been and could be misapplied to people who self-induce. There are also a number of laws deployed when no other legal authorization to punish can be found (obscure laws like disposal of human remains or concealing a birth), which have led to at least twenty arrests for [self-induced abortion] and criminal investigations in twenty states for alleged self-induced abortions since 1973.”40
There is little doubt that as abortion becomes more illegal and inaccessible, more people will go to jail if they are discovered conducting or assisting in a self-managed abortion. If you need legal help or wish to support those who will assist in legal defense for these cases, consider reaching out to the Self-Induced Abortion (SIA) Legal Team:
SIA LEGAL TEAM
844-868-2812 (legal help line)
https://www.sialegalteam.org
info@SIALegalTeam.org
What People Self-Managing Their Abortion Care Need to Know
While the laws differ from state to state and will get even more extreme as Roe is dismantled and potentially overturned, none of this will change the fact that being able to determine your own medical care—including if and when you want to carry a pregnancy to term—is a human right. That also includes a person’s right to health care for whatever that person’s circumstances warrant. No person should ever feel the need to avoid follow-up care because of fear of an arrest. According to a video on the SIA website:
- A person has the right to talk to a health care provider before, during, and after a self-managed abortion—but they also have the right to provide as much or as little detail as they choose.
- That includes hospital staff, emergency room doctors, and anyone else who may ask questions about recent medical actions.
- Doctors state that there is no difference between how they treat complications from a miscarriage and how they treat complications from an abortion, meaning there is no need for a person to clarify which may be occurring.
- Doctors admit there is no actual test that can show if a person has ingested medications meant to induce a miscarriage.
- There are no laws that require hospitals to report suspected abortions to law enforcement.
- Some states even impose penalties on health care providers who violate a person’s privacy by releasing personal health information without patient consent.
- However, because not all medical professionals are clear on the laws, or on the importance of maintaining doctor/patient confidentiality, a patient should always only provide the information they feel comfortable with sharing.
We will discuss how to minimize other potential legal risks in greater detail in chapter 10.
Why Can’t We Just Have Abortion Pills Online in the US?
With the current laws and political climate, at this point it is almost impossible to successfully create a central, telemedicine-style self-managed abortion care network in the US for a number of reasons. While it isn’t illegal to share information about abortion protocols, and in many cases it isn’t illegal to self-induce an abortion, the two being offered together without legal backing offers much greater risk. The multi-state TelAbortion Study mentioned earlier in this chapter is an example of how medication abortion could easily be done remotely, but because of state restrictions it has been impossible so far to extend nationally. But that doesn’t mean people aren’t trying to see if such a network can be created, and how long it can stay active.
In 2018, a new website went live called Aid Access, which claims to offer consultation for pregnant people who either cannot or choose not to go to an abortion clinic to end a pregnancy. After the consultation, according to the site, “A licensed doctor will use the information provided by you and his/her best clinical judgment to determine whether you can use abortion pills without risk.” If the provider approves the request, a package containing mifepristone and misoprostol will be mailed to the address you provide within ten days.
Aid Access is run by Rebecca Gomperts of Women on Waves/Women on Web. Gomperts is a reproductive rights activist who is already supplying medications in countries where abortion is completely illegal. She believes her actions remain legal because the FDA allows medication to be imported for personal use. Still there are some concerns beyond just the legality, such as the possibility that the medication will not get to a user in a timely manner and before the person is too far along gestationally to use it properly, or that the private information being gathered will somehow be leaked, hacked, or otherwise confiscated and turned over to law enforcement, published online, or in any other way used nefariously. It also must be stressed that in some states, using these medications outside a clinic setting continues to be against the law, even if the importing of the drugs is not.
Gomperts claims more than six hundred people have been assisted by the site as of October 2018, but it is unclear if—now that it is more publicly known—it will even still exist by the time you read this book. If not, you can be certain another one will pop up to replace it.
AidAccess as of August 2018 can be reached at www.aidaccess.org.