Mandibular injuries in the growing patient are not uncommon, and the mature patient with permanent dentition can often be treated similarly to the adult patient. However, pediatric patients with primary dentition and mixed dentition can often be treated much more conservatively due to their healing capacity. It is imperative that the surgeon understand proper application of Risdon cables/wires to facilitate conservative treatment in the pediatric patient. Additionally, some fracture patterns are concerning for growth disturbance and require monitoring over ensuing years to ensure that no further intervention is necessary.
Core Messages
Pediatric mandible fractures occur much less frequently as compared to adult mandible fractures.
The majority of pediatric mandible fractures can be treated with closed reduction techniques.
The pediatric mandible heals very quickly and treatment times are much shorter than adults.
The pediatric patient should be observed over time for possible growth disturbances and facial asymmetry.
7.1 Background
Despite the parent’s best efforts and a protective social environment, children will always be involved in maxillofacial trauma. Fortunately, the overall incidence for pediatric facial trauma is much lower than the adult population [1–3]. Common methods of injury include motor vehicle accidents, falls, sport-related injuries, and unfortunately child abuse. The mandible is the most common facial bone to fracture. The definition of pediatric is somewhat variable, depending on who is speaking. Many pediatricians see patients until age 21. Discussing a cohort of 18-year-old patients involved with facial fractures would hardly be considered a pediatric trauma discussion. The focus of this chapter on pediatric mandible fractures will be on patients 12 years old and younger.
When examining the pediatric patient after trauma, one should approach the exam in a systematic and organized approach such as the Advanced Trauma Life Support (ATLS) protocol. Following this protocol approaches the injured patient in a systematic fashion and decreases the chance of missing an injury [4]. Fractures in children equate to a significant amount of force, since children tend to “bounce” and not “break.” Facial fractures are often seen with significant other bodily injuries but can also be seen as isolated injuries.
Many of the same symptoms seen in adult patient facial fractures are seen in the pediatric patient population sustaining facial fractures. Swelling, ecchymosis, and facial deformity are commonly seen. Visible steps in the occlusal plane are seen at the fracture site (Fig. 7.1). The mandible can be mobile at the fracture site. Malocclusion is commonly seen with mandible fractures but can be difficult to verify in the mixed dentition stage when the occlusion is changing [5]. Additionally, the young child or early adolescent may not understand what “malocclusion” means or how their teeth actually come together. This is also true with paresthesia of the inferior alveolar nerve seen with mandible fractures of the parasymphysis, body, and angle regions. The young child may not understand what “numbness” of the lip or chin equates to during the physical exam. Often, in the young patient, the physical exam is very difficult to perform due to the uncooperative child. A basic exam is performed to ascertain injuries and a more detailed exam is performed under anesthesia when the patient is being treated.
Fig. 7.1
Clinical photograph of step in mandibular occlusal plane at the fracture site
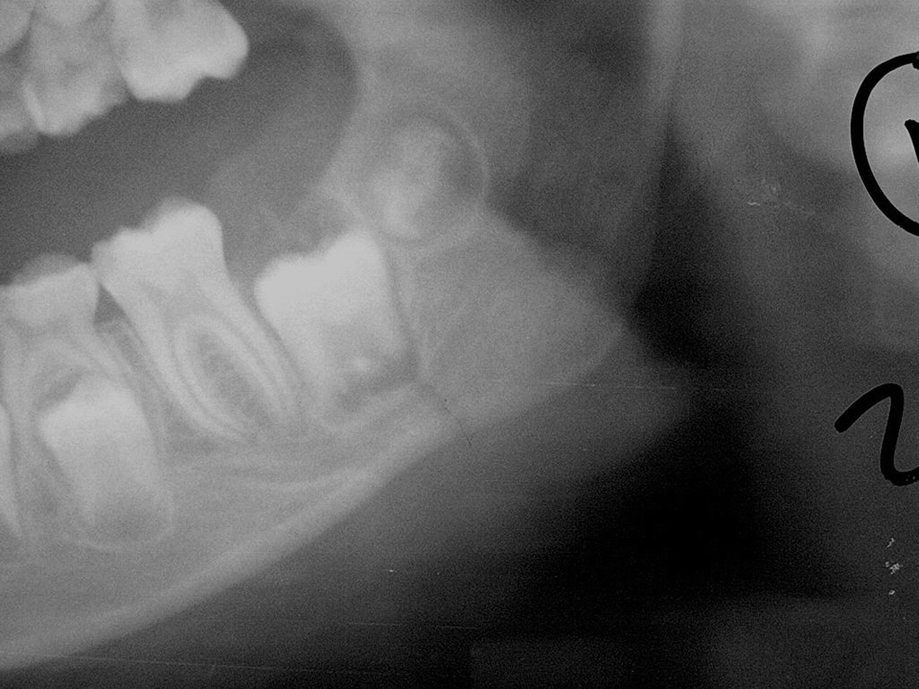
Radiographs are an important aspect in managing the trauma patient. If the patient has suspected bony injuries, radiographs confirm or disprove the injuries. Computerized tomography (CT) scans are commonplace in all hospitals and healthcare facilities. They provide detailed 3-dimensional imaging of facial fractures. The plain films of a “mandible series” have essentially gone by the wayside. Orthopantogram imaging or “Panorex” imaging is still very commonly seen in the office setting and occasionally in the hospital (Figs. 7.2 and 7.3). However, more office practices have realized the value of 3-dimensional imaging and obtained cone beam computerized tomography (CBCT) for daily use in the office (Fig. 7.4). Infants and young children may require hospital-based CT scan imaging if they are not able to sit or stand for office-based imaging (Figs. 7.5, 7.6, 7.7, and 7.8).
Fig. 7.2
Orthopantogram “Panorex” radiograph showing left mandibular angle fracture in pediatric patient
Fig. 7.3
Close-up showing left mandibular angle fracture
Fig. 7.4
CT scan showing right mandibular condyle fracture on the same patient that was not visible on “Panorex” imaging
Once the mandible fracture has been confirmed, the next step is to develop the appropriate treatment plan for management. Treatment can be very variable, ranging from observation and soft diet to open reduction and internal fixation (ORIF) [5–7]. The treatment plan is based on the location of the fracture(s), patient’s dentition, and patient age. Overall, the pediatric patient with a mandible fracture can be treated more conservatively when compared to the same fracture in adults. The pediatric patient has a thick, robust periosteum which allows for rapid healing and remodeling of the fracture site. The majority of pediatric mandible fractures can be managed with closed techniques. Treatment times are also much shorter in the pediatric patient when compared to similar fractures in adults. Treatment times are primarily based on the patient age and fracture pattern/anatomic location. For example, a mandibular body or angle fracture in a 7-year-old may only require 10–14 days of MMF or elastics as compared to 4 weeks of MMF in the adult patient with a similar fracture.
Closed reduction techniques can include arch bars, Risdon cables, circum-mandibular wires, and splints [8, 9]. Innovative techniques such as using silk sutures around primary teeth for short-term maxillomandibular fixation (MMF) have been described [10]. Most surgeons are familiar with arch bars as they are common in the management of mandible fractures in adults. However, the pediatric dentition has some unique features which occasionally make conventional arch bar techniques very difficult or impossible. The primary teeth have short, squat crowns with a different height of contour as compared to adult teeth (Fig. 7.9). Occlusal schemes with anterior teeth occluding tightly can preclude the use of arch bars. Standard arch bars can easily become dislodged from the primary teeth which can require an additional surgical procedure (Fig. 7.10). Occasionally the arch bar is taller than the crown of the primary tooth. One helpful technique for closed reduction treatment in the pediatric mandible fracture patient is the use of Risdon cables [11]. Risdon cables are low profile and easy to place. They only require wire to fabricate, which can be found in any hospital. A 24-gauge wire is braided after anchoring it to a molar tooth. The braided wire is anchored to the molar on the opposite of the dental arch. The braided wire acts like a conventional arch bar. Wires are then passed above and below the braided wire and around the teeth, similar to anchoring an arch bar to teeth in a conventional situation. In the pediatric patient, this author prefers the use of elastics over wires for postoperative maxillomandibular fixation. The Risdon cable is a valuable fixation technique which can be used in areas where resources are limited and is applicable for adult patients also (Figs. 7.11, 7.12, 7.13, and 7.14).
Fig. 7.9
Primary dentition in pediatric patient
Fig. 7.10
Wire fixation failure with arch bars in pediatric patient with primary dentition
Fig. 7.11
Risdon cable application. Braided wire acts as arch bar
Fig. 7.12
Risdon cable technique completed
Fig. 7.13
Risdon cable with postoperative training elastics
Fig. 7.14
Panorex with Risdon cables in place
Splints can also be used in pediatric mandible fracture management techniques. A lingual splint can provide adequate stability to allow a pediatric mandible fracture to heal and avoid open reduction techniques (Fig. 7.15). The fractures must be amenable to treatment with a lingual splint by being body fractures or anteriorly located. If the fracture is located posteriorly, such as posterior body or angle/ramus, the splint cannot reach that region and provide lingual support. Surgeons must have the laboratory support to fabricate the appliance and sometimes a separate anesthetic is required to take dental impressions to fabricate the splint. Occlusal splints can also be used with circum-mandibular wires to stabilize the pediatric mandible fracture [8, 9].
Fig. 7.15
Lingual splint used to treat pediatric mandible fracture
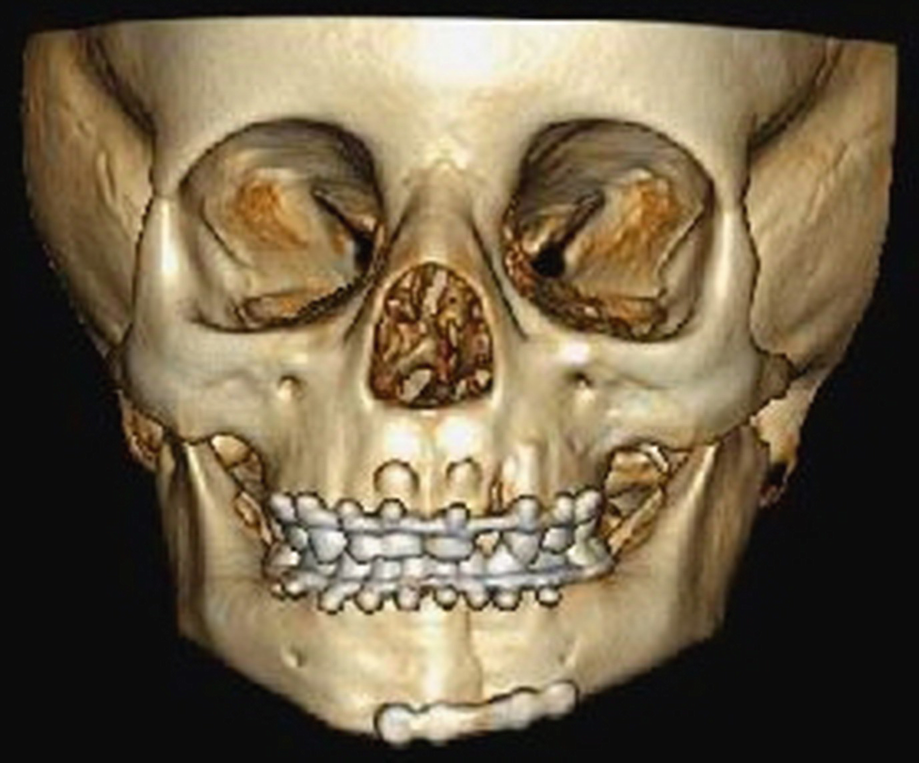
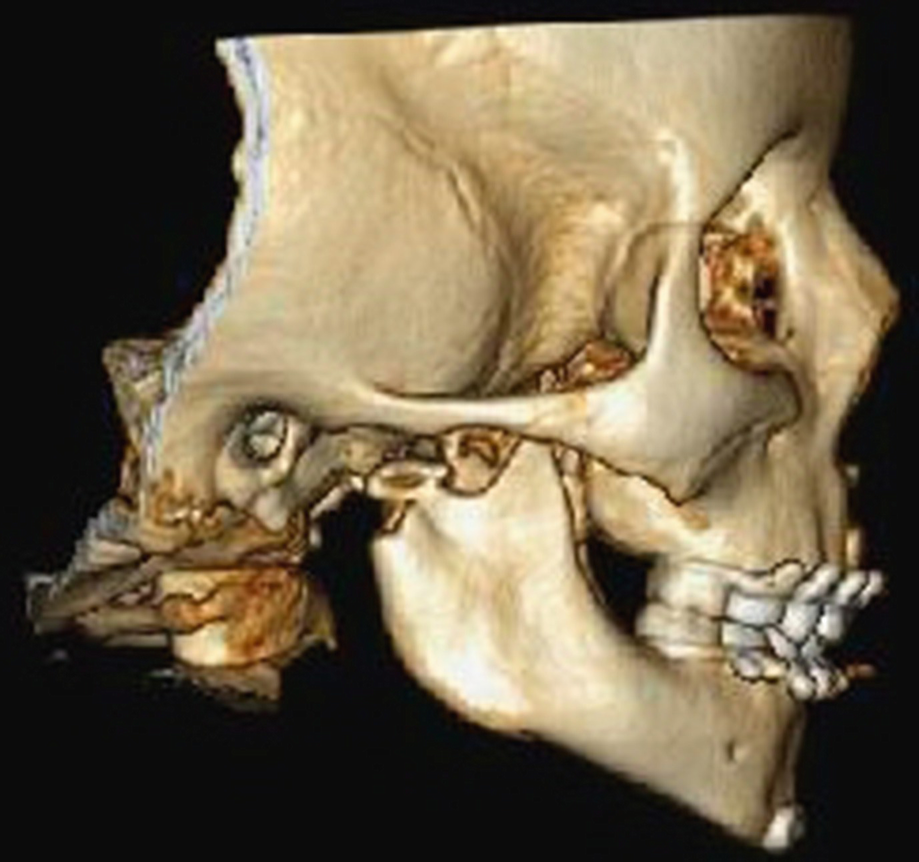
There will be pediatric mandible fractures that are grossly displaced or unstable that will require open reduction techniques (Figs. 7.16 and 7.17). Additionally, the pediatric mandible fracture pattern may involve the condyle with other fractures and postoperative function is desired to prevent TMJ ankylosis, which can be very difficult to treat. Open reduction and internal fixation techniques allow the other mandible fractures to be stabilized and permit functioning of the condyle fracture during the healing phase [12, 13]. Great care must be taken when using plate and screw fixation in the pediatric mandible fracture. The pediatric mandible houses the developing permanent dentition which can complicate conventional plate placement seen in the adult patient population. To avoid damaging the developing permanent dentition, plates and screws must be placed very low, at the inferior border of the mandible. There is very limited space to place plates and screws and avoid damaging the developing permanent tooth bud. Additionally, consideration should be given to the use of monocortical screws to avoid damaging the permanent tooth buds. The majority of the time, the plates and screws can be placed in a transoral fashion to avoid external scars (Figs. 7.18, 7.19, 7.20, 7.21, 7.22, 7.23, 7.24, 7.25, and 7.26). There is controversy over the use of resorbable fixation versus titanium fixation. Many surgeons advocate removal of the titanium fixation plates used in pediatric mandible fracture fixation. This requires an additional surgical procedure and anesthetic. Resorbable fixation has the advantage that a second surgical procedure is not required for removal [14, 15]. However, resorbable fixation is currently not approved for mandibular fracture fixation by the Food and Drug Administration in the United States and must be used off label. Surgeons have reported good results with using resorbable fixation in treating pediatric mandible fractures [16, 17].
Fig. 7.16
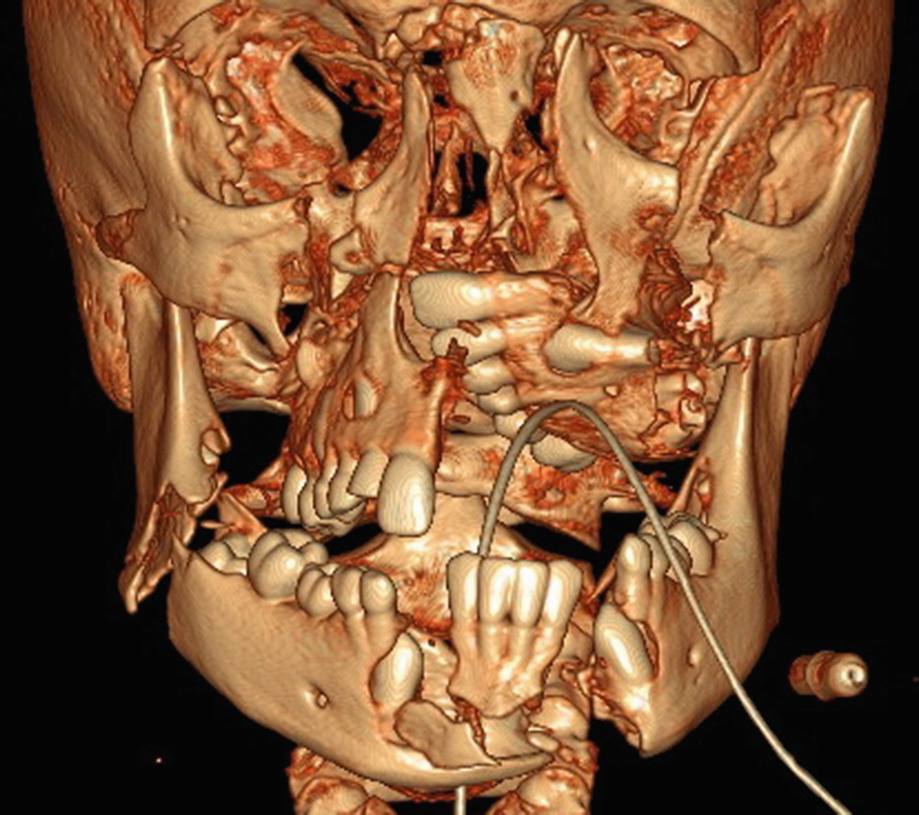
Grossly displaced, complex pediatric facial fractures planned for ORIF
Fig. 7.17
Grossly displaced, complex pediatric facial fractures planned for ORIF
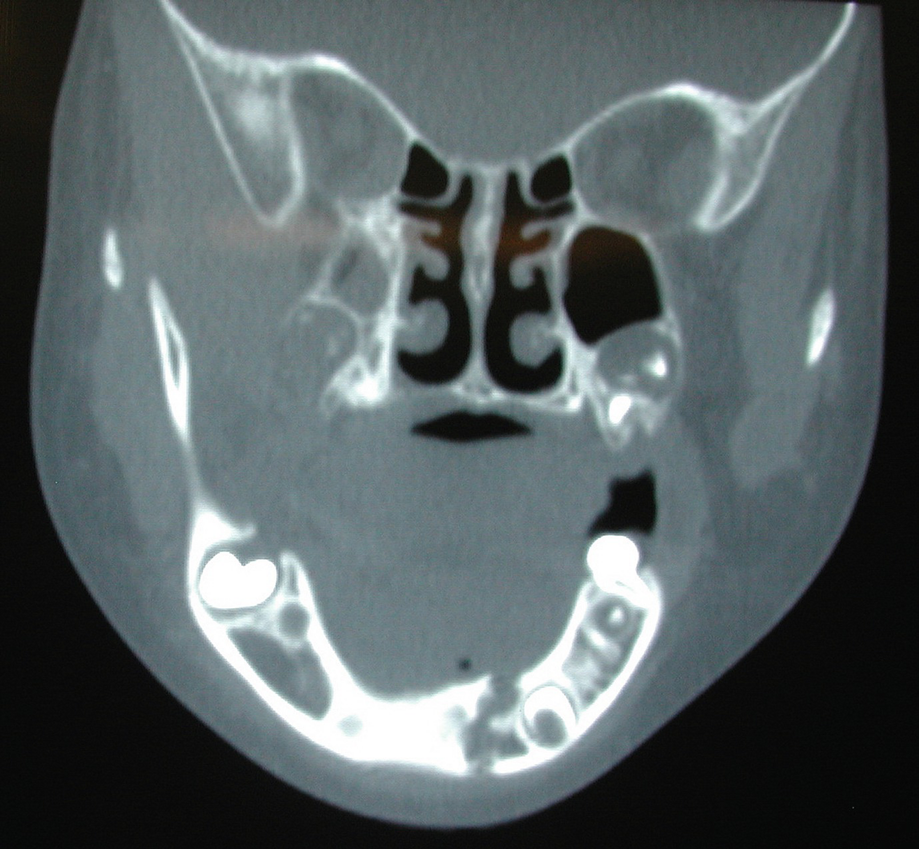
Fig. 7.18
Coronal CT scan showing fracture of anterior mandible
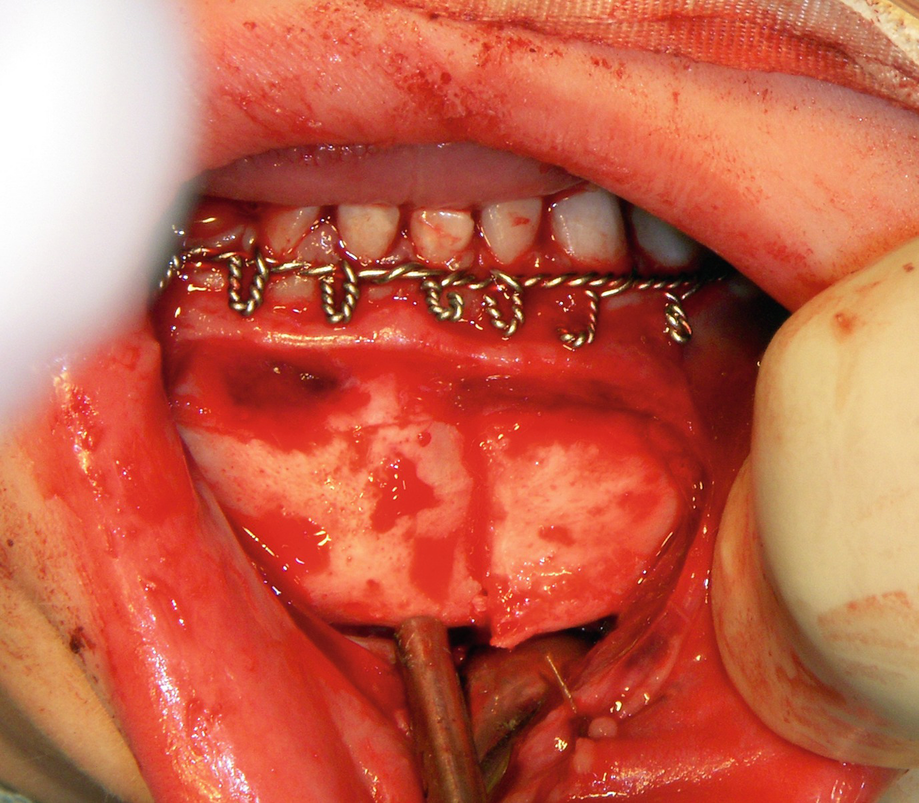
Exposure of anterior mandibular fracture via transoral route
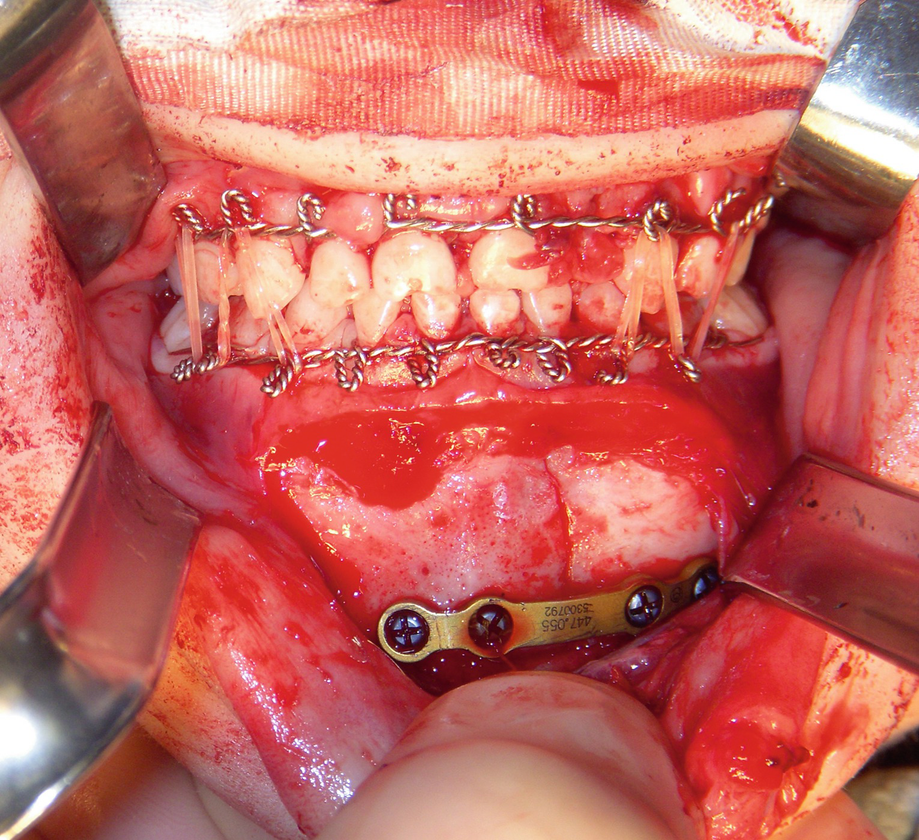
Fig. 7.21
Fracture reduced and plate placement at inferior border to avoid damaging permanent teeth
Fig. 7.22
Plate placed at inferior border, Risdon cables and elastics in place to manage condylar fractures in a closed method
Fig. 7.23
Post-op CT scan, 3D reconstruction in AP view
Fig. 7.24
Post-op CT scan, 3D reconstruction in left lateral view
Fig. 7.25
Post-op CT scan, 3D reconstruction in right lateral view
Fig. 7.26
Post-op CT scan, 3D reconstruction in “worms-eye” view to see mandible reduction
The surgeon must always weigh the risks and benefits of surgery in children and keep in mind the wonderful healing capacity of children.
7.3 Complications in Managing Pediatric Mandible Fractures
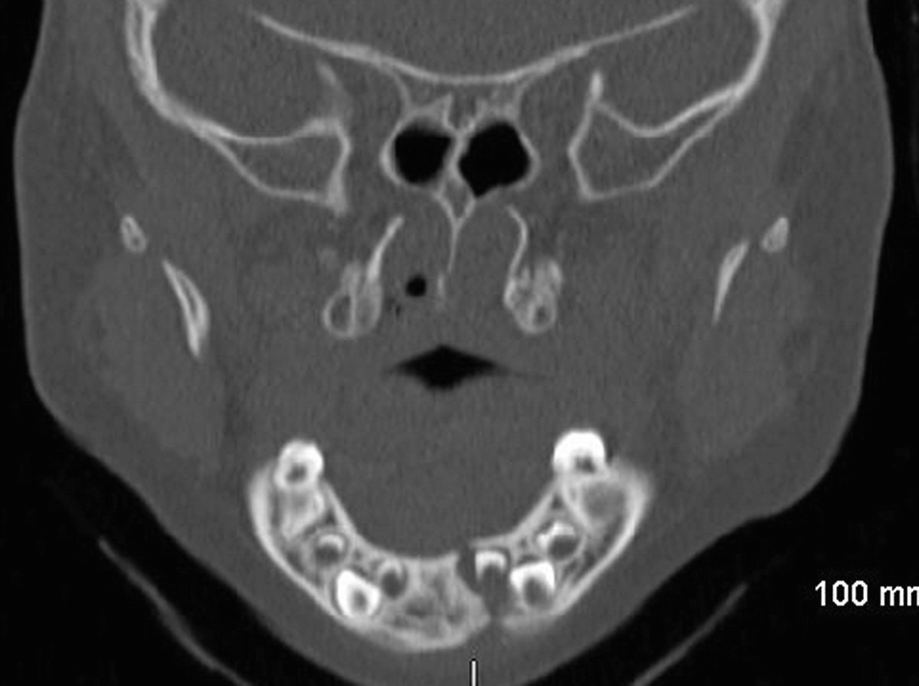
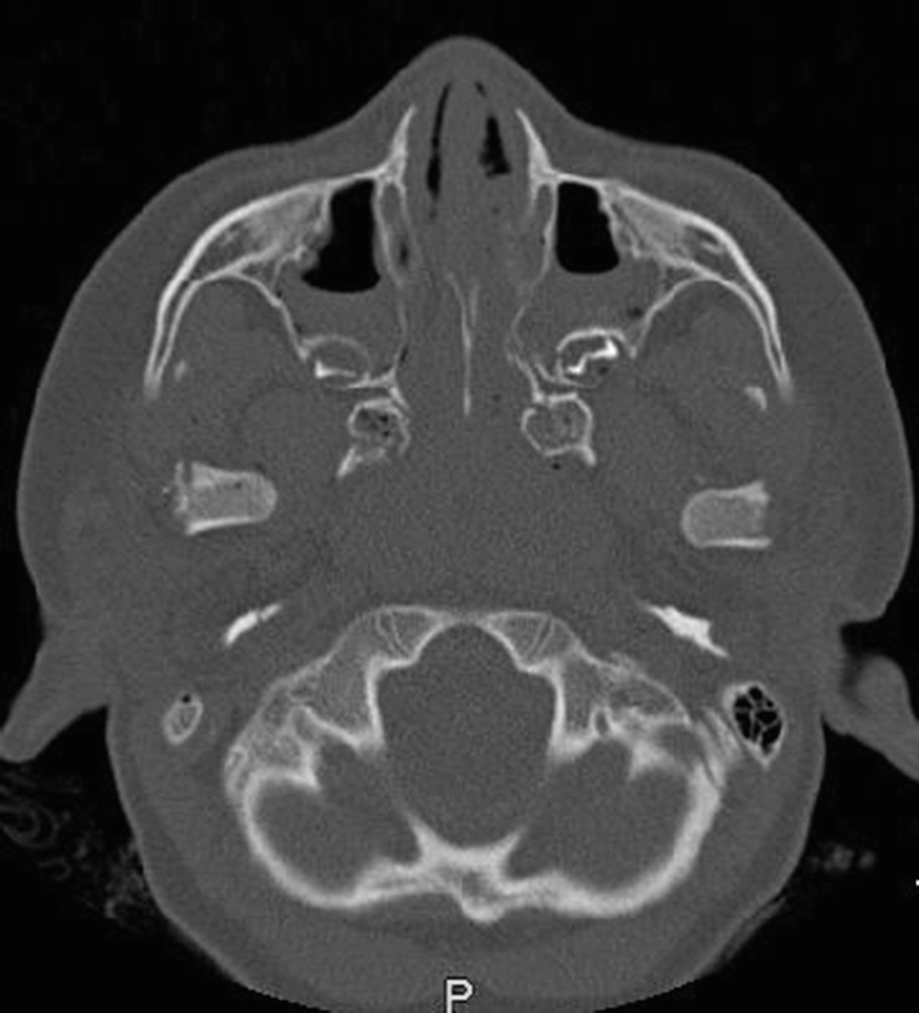
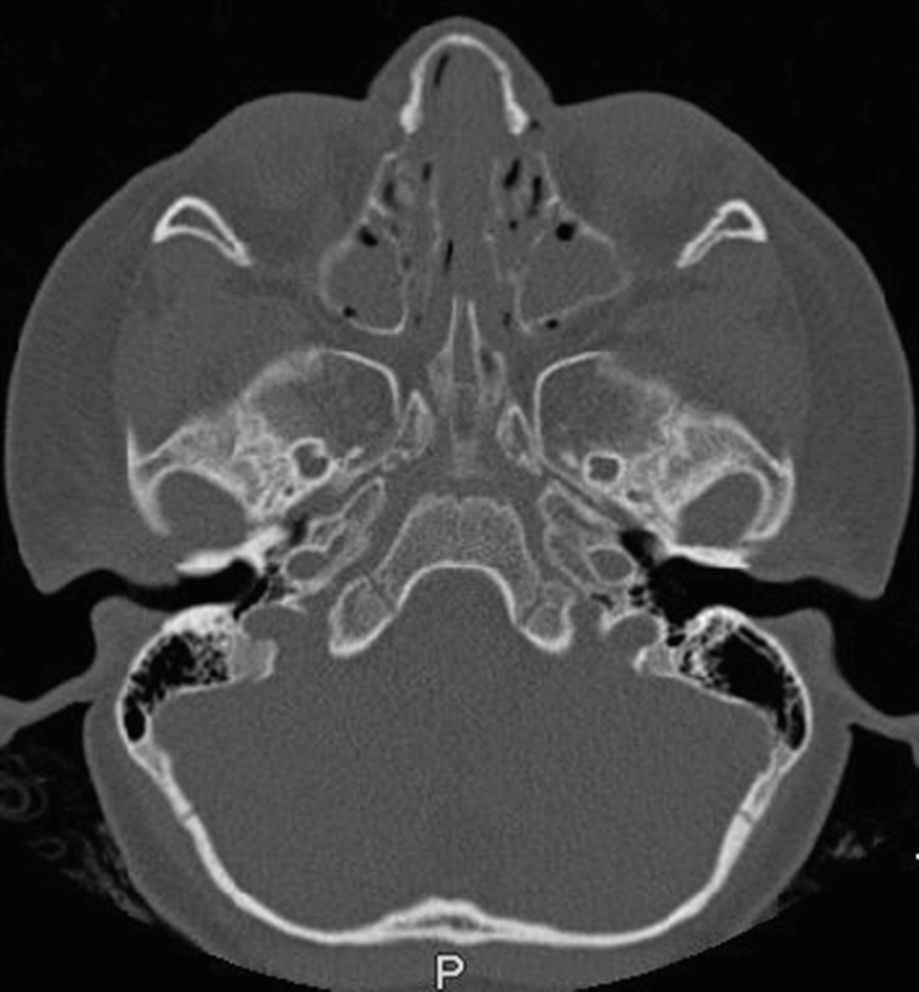
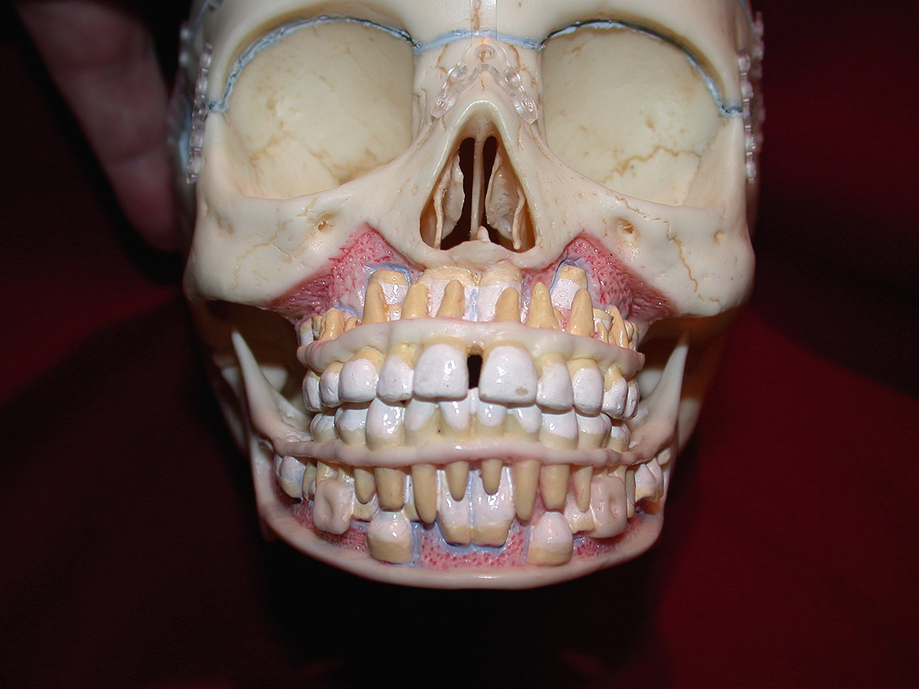
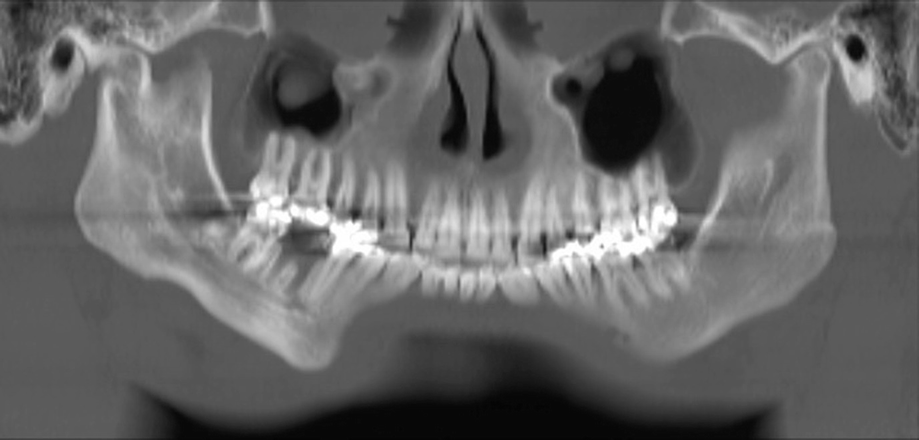
Fortunately, complications encountered when treating pediatric mandible fractures are much lower than adults [18]. Nonunion of fractures is virtually not seen. The pediatric mandible has a tremendous healing capacity in a short time period. Malocclusions are also rare and much better tolerated in the primary dentition which will exfoliate and be replaced with the adult dentition. Orthodontic treatment can easily manage the majority of malocclusions. Damage to permanent tooth buds near the fracture site and from placement of plates and screws is always a possibility. The surgeon must always be aware of the position of developing permanent tooth buds (Figs. 7.27 and 7.28). TMJ ankylosis is a potentially devastating complication seen in pediatric condylar fractures. TMJ ankylosis can be very difficult to treat and require multiple surgeries. This is usually seen with prolonged periods of maxillomandibular fixation (MMF) when treating condylar fractures (Figs. 7.29, 7.30, and 7.31). This is why many surgeons favor functioning the mandible with elastics to control the occlusion and no MMF when treating condylar fractures. Lastly, growth disturbances are always a possibility when the mandible is fractured. Growth and development of the jaws is a complex process and occasionally growth disturbances are seen after fractures, regardless of the treatment used. The growth disturbances often present as a facial asymmetry [19]. This can manifest itself with the need for corrective jaw surgery or orthognathic surgery. Surgeons must be aware and vigilant and the parents should be informed of this possibility. Long-term follow-up of the pediatric maxillofacial trauma is ideal but very often very difficult to accomplish for a variety of reasons. Mobility of families, insurance provider panels, referral to specialists by primary care physicians, and the sense that “nothing is wrong” by parents may contribute to the difficulty in long-term follow-up.
Fig. 7.27
Model showing developing permanent tooth buds in pediatric facial skeleton
Fig. 7.28
Lateral view of model showing developing permanent tooth buds in place in pediatric facial skeleton
Fig. 7.29
CT scan-generated Panorex showing right TMJ ankylosis after treatment of a pediatric condyle fracture
Fig. 7.30
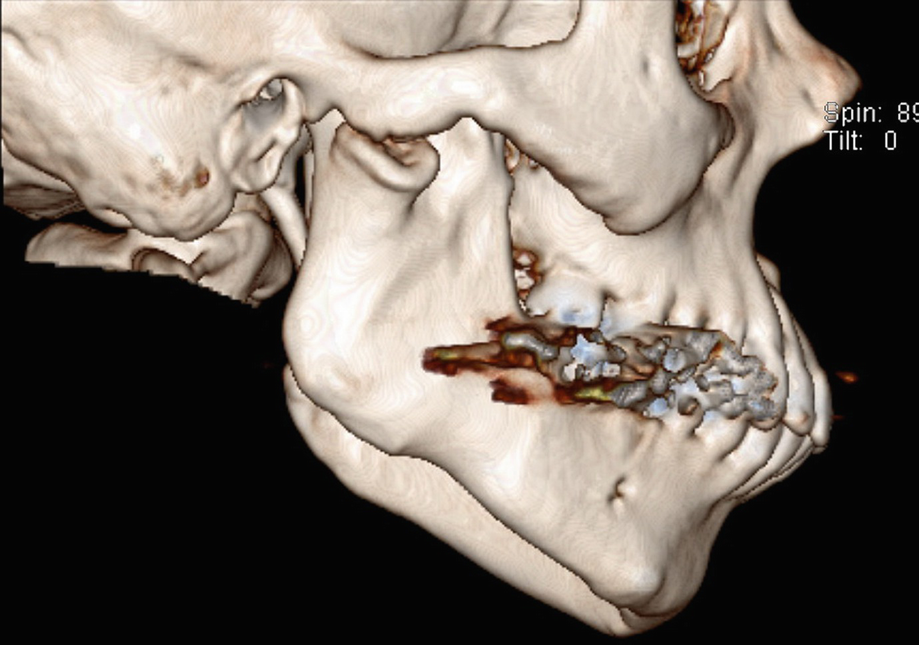
CT scan, coronal view of right TMJ ankylosis
Fig. 7.31
CT scan, 3D reconstruction of right TMJ ankylosis
7.4 Conclusion
Despite everyone’s best efforts, pediatric facial fractures will always occur. Children will always be involved in rough play, sports, and bicycle and motor vehicle accidents. Practitioners must always be wary of potential child abuse and neglect. Most mandible fractures can be managed conservatively with closed reduction techniques. However, there are clearly clinical situations which require open reduction and internal fixation techniques.
Treatment times are much shorter than adults due to the rapid healing of the pediatric mandible and it is robust periosteum. Ideally, the pediatric facial trauma patient should be followed over time to monitor possible growth disturbances which can lead to facial asymmetry. With a mobile population and changing financial situations/insurance coverage this can be a very challenging task.