ON MAY 13, 2015, LAWMAKERS ON THE FLOOR OF THE HOUSE of Representatives in Washington, DC, took turns standing up and boiling down remarkably complex science into quick sound bites. Their topic: whether an unborn child feels pain at specific points of development while in the womb, and whether abortions should be banned after the earliest of these points to avoid any suffering for the fetus.
Here’s Charles Boustany, from Louisiana:
The scientific evidence is clear: unborn babies feel pain.
They feel pain at 20 weeks post-fertilization.
Next up, Dan Benishek, from Michigan:
The Pain-Capable Unborn Child Protection Act will prevent abortions from occurring after the point at which many scientific studies have demonstrated that children in the womb can actually feel pain.
And one more, Ralph Abraham, also from Louisiana:
As a doctor, I know and I can attest that this bill is backed by scientific research showing that babies can feel pain at 20 weeks, if not before.1
Other legislators—all Republicans—made very similar statements. An average listener may have heard these statements and thought, Okay, it sounds like science has found the precise point at which a fetus feels pain. Interestingly, most of the Democrats who stood up and spoke in opposition to the bill did so on grounds unrelated to the science in question, but instead focused on the bill’s attack on women’s rights and government control of one’s body. This could have been a good opportunity, though, to add to that message and simply say: The science on this topic is far from settled.
The problem with researching fetal pain is that pain is a subjective experience. This is why doctors will ask a patient: “On a scale of 1 to 10, what is your pain?” There has been extensive research into pain scales, pain tolerance, and related issues, because pain is complicated. All we can say about pain is what the person in pain can tell us about it, and of course an unborn child is incapable of telling us whether something hurts. As a result, the science on this topic is almost impossible to settle, and we’re certainly not there yet. But if you listened to all those House members, you would think we did a few studies, got a result, and hey, we’re done! Fetal pain at 20 weeks is a certainty.
This is the most basic of the mistakes, misrepresentations, and mangling of science that this book will address: the OVERSIMPLIFICATION. Unlike the science discussed, this idea is straightforward: politicians often make strong, definitive claims about topics that have far more subtlety than those statements allow or acknowledge. They take a complicated scientific issue and strip it down to a sound bite, a pithy turn of phrase that might garner cheers during a speech or build support for a piece of legislation, but would also give anyone listening an incorrect impression of the science in question.
This isn’t to say that there is malicious intent behind any particular OVERSIMPLIFICATION. Sometimes, indeed, it is useful to take complicated issues and make them easier for the public to understand, even if it means leaving out a few details. But politicians aren’t always just trying to help their constituents understand an issue. Sometimes they use the technique to obscure the truth, which—when it comes to science—can be messy, confusing, and unsettled.
So what do we know about fetal pain? Again, we can’t ask a fetus whether anything hurts, so most of the research into this topic involves neuroanatomy and neurodevelopment. Basically, at what point are the connections completed between, say, our limbs and our brain, where the pain is actually processed and experienced? Though we can’t really know just how a fetus perceives something that an adult would consider painful—like a pinprick, which a fetus can experience when a pregnant woman undergoes amniocentesis—we can at least know whether the signal gets from the site of the painful stimulus up to the brain.
And in fact, most published research suggests that the Republicans are wrong; the connections in question likely do not exist prior to about 23 or 24 weeks of gestation, if not even later. The connections needed for pain experience are between a part of the thalamus, which is a sort of relay center in the brain, and the cortex, the big part of the brain where many experts think pain is actually processed. Without connections from nerve endings to the spinal cord, from the spinal cord into the thalamus, and from the thalamus up into the cortex, pain simply may not be possible.
Several reviews of available evidence, conducted by well-respected scientific organizations, have concluded that the insistence on pain at 20 weeks is misplaced. For example, one 2010 synthesis of the evidence by the Royal College of Obstetricians and Gynaecologists in the United Kingdom concluded:
In reviewing the neuroanatomical and physiological evidence in the fetus, it was apparent that connections from the periphery to the cortex are not intact before 24 weeks of gestation and, as most neuroscientists believe that the cortex is necessary for pain perception, it can be concluded that the fetus cannot experience pain in any sense prior to this gestation.2
The Texas branch of that group’s US counterpart, the American Congress of Obstetricians and Gynecologists, agreed with that conclusion and specifically addressed the periodic attempts to pin down 20 weeks in legislation, writing in 2013:
Supporters of fetal pain legislation only present studies which support the claim of fetal pain prior to the third trimester. When weighed together with other available information . . . [the] supporters’ conclusion does not stand.3
And finally, a synthesis of available evidence was published in the prestigious Journal of the American Medical Association (known as JAMA) in 2005, by researchers at UC San Francisco. They concluded, as others have, that “evidence regarding the capacity for fetal pain is limited but indicates that fetal perception of pain is unlikely before the third trimester.”4 The third trimester begins at 27–28 weeks from conception.
The supporters of the 20-week ban point to a few sources of evidence, though they don’t stand up to much scrutiny. In one commonly cited paper from the journal Behavioral and Brain Sciences in 2007, Swedish neuroscientist Bjorn Merker wrote about “evidence that children born missing virtually all of the cerebral cortex nonetheless experience pain.”5 In other words, maybe that fully formed cortex isn’t even necessary to experience pain, which could push that developmental milestone earlier by a few weeks. Merker’s paper, however, wasn’t about fetuses in particular, and the children he wrote of were anencephalic infants (babies born without large parts of the brain, who generally do not survive long after birth)—not quite the same question. In fact, Merker himself told the New York Times in 2013 that his paper had only “marginal bearing” on the question of fetal pain.6
Another common argument goes back to amniocentesis—a procedure to test for certain birth defects or genetic issues, as well as infections, in which a needle is inserted into the amniotic sac. If the needle pricks the fetus’s heel, the fetus may recoil—just as you might pull your hand back from a hot stove. That response certainly may look like the fetus is experiencing pain, but let’s go back to the 2005 JAMA review to explain this phenomenon: “Flexion withdrawal from tactile stimuli is a noncortical spinal reflex exhibited by infants with anencephaly and by individuals in a persistent vegetative state who lack cortical function.”7 In other words, the body is capable of perceiving and responding to harm—a process called nociception—without the brain actually processing it as pain. A reflex can move your limbs even without your knowing it. Pain requires some degree of consciousness, while nociception requires no such thing.
This all may sound like a complicated jumble of conflicting research. Note the language used in the JAMA conclusion quoted earlier: “fetal perception of pain is unlikely.” Even some of the world’s experts on the topic, writing in a journal carefully reviewed by other experts, are unwilling to state conclusions in as concrete terms as the GOP House members did. The lawmakers used words like “clear” and “settled,” aiming to close off any and all debate on the topic. This is a hallmark of the OVERSIMPLIFICATION: science is often far muddier than a politician is willing to admit.
Furthermore, those politicians don’t enjoy being called on their loose use of complicated science. Again, boiling down a complicated issue to a pithy quote makes for good speechifying, but it also often backs the speechifier into a scientific corner:
“Thing X is true!”
“Okay, where is your evidence for thing X?”
“It’s . . . complicated.”
Congressman Ralph Abraham, one of the legislators quoted at the beginning of this chapter, gave a fine illustration of this problem, and of the general disconnect between politics and science, when asked for evidence to support his claims about fetal pain. His spokesman sent an e-mail that, instead of offering up any actual studies as evidence, claimed simply that Abraham’s expertise should not be questioned, given his training as a doctor.
[Congressman Abraham] has read countless medical journals and articles during that career that have led him to the conclusion that babies feel pain at 20 weeks. There’s no single article or fact sheet that led him to this conclusion; he reached it during an entire career of study.8
This is a stunning misunderstanding of how science works, for a doctor or for a lawmaker. “Trust me, I’m a doctor” does not exactly prove one’s point. If you heard it from your own doctor when asking about a particular medication or procedure, you might decide it’s time to switch doctors. It was essentially a Jedi mind trick, a wild hope that “you don’t need to see the evidence” would somehow convince people that they did not, in fact, need to see the evidence. Remember, Abraham said on the House floor that fetal pain at 20 weeks is “backed by scientific research.” If that were the case, it shouldn’t be hard to actually cite that research.
That’s where the OVERSIMPLIFICATION tends to break down. When you start to ask for and examine the evidence behind a scientific claim, you often see that science doesn’t quite cooperate with political sound bites.
A KEY STRATEGY for spotting this type of error is to look at the underlying policy position behind the science in question. With regard to fetal pain, the claim regarding 20 weeks is part of the ongoing effort by Republicans to limit and restrict abortions. When placed in that context, it’s not difficult to understand why “settled” science on fetal pain could help the political cause, and why the more nuanced take on the issue would undermine the legislative effort.
Here’s another example of how the OVERSIMPLIFICATION is used to serve a specific policy position: in April 2015, New Jersey governor and GOP presidential candidate Chris Christie appeared on a radio show and said definitively, “Marijuana is a gateway drug.”9
That sounds bad! The term “gateway drug” is likely familiar to most people. What Christie was saying was, essentially, if you smoke pot, you’re well on your way to a needle sticking out of your arm. He made this clear, definitive claim—it is a gateway drug, not that evidence suggests it might be, or that it could be considered, or anything of the sort—as a way to support a policy position: his belief that states that had recently legalized recreational marijuana should not be exempt from federal laws that still considered marijuana an illegal and dangerous drug. Christie said that, as president, he would still prosecute marijuana offenses, even in Washington and Colorado, where pot was legal at the time of his comments. Why? Because gateway drug, that’s why.
But once again, this is a fairly drastic OVERSIMPLIFICATION. Scientifically speaking, it is not accurate to say that marijuana is a gateway drug. It would also be inaccurate to claim the opposite, that marijuana is definitively not a gateway drug. The science, once again, is complicated.
The gateway hypothesis essentially says that the use of one substance can lead to—or at least increase the likelihood of—the use of another. If you ask hardcore antidrug folks—like Governor Christie, apparently—the gateway effect for marijuana is real and important. If you ask pro-legalization folks, of whom there are a growing number around the country, you’ll find the opposite claim: marijuana is definitively not a gateway substance. The reality, as is often the case, lies somewhere in the middle.
“The scientific community is still arguing about it,” said Susan Weiss, an expert with the National Institute on Drug Abuse (NIDA), which is part of the National Institutes of Health. “It’s a really complicated thing to tease out. It has been very contentious over the years.”10
Responsible scientists are not afraid to admit this lack of definitive conclusion. “We don’t know the answer” is not an admission of defeat, but just an acknowledgment that science is hard, that biology and chemistry and physics don’t always offer a single, easy answer. Politicians don’t like that sort of uncertainty.
There are two distinct ways a gateway effect could occur: (1) biologically, meaning that using one drug actually changes your brain or body in ways that make use of another drug more likely; (2) socially or culturally, meaning that the context in which you use or abuse the first substance might make the second more readily available, or more likely to be used as well. Some evidence suggests that both of these mechanisms do function with marijuana, though there is also evidence that suggests otherwise, or that other legal drugs, including nicotine and alcohol, have similar or even more dramatic gateway effects.
In 1999, the Institute of Medicine, which is part of the National Academy of Sciences (and has since changed its name to the National Academy of Medicine), released a report entitled Marijuana and Medicine, which addressed the gateway hypothesis and laid out a remarkably common problem when it comes to science and health in particular:
In the sense that marijuana use typically precedes rather than follows initiation into the use of other illicit drugs, it is indeed a gateway drug. However, it does not appear to be a gateway drug to the extent that it is the cause or even that it is the most significant predictor of serious drug abuse; that is, care must be taken not to attribute cause to association.11
Correlation does not equal causation! This truism should ring out in classrooms, in newsrooms, in the halls of Congress and the White House—anywhere that science is discussed and acted upon. Just because one circumstance is connected to another, or follows another, does not mean that one caused the other.
One famous example is particularly illustrative: when ice cream sales increase, so do violent crime and murder rates; therefore, delicious summer treats are to blame for homicides, right? Obviously not; this is just coincidence. There is ample evidence that violence peaks in summer months12 (why that happens is another unanswered question), when ice cream happens to become a lot more desirable than in January. Ice cream does not, in fact, send all of us into a murderous rage.
With regard to a gateway effect, just because the use of drugs like cocaine or heroin or methamphetamines tends to follow chronologically behind the use of marijuana does not mean that use of that first drug caused use of the latter.
To a politician, that fundamental tenet of science can get in the way of a good narrative. Wanting to appear hard on drugs and on crime, Christie made use of the sequential nature of drug use to make pot seem worse than it is.
However, he’s not 100 percent wrong: some evidence does actually support gateway effects of marijuana; it’s just not definitive, as Weiss of NIDA said. Some studies, done in rats and other rodents, have made intriguing findings. For example, in one study published in the journal Neuropsychopharmacology in 2007, researchers treated adolescent rats with THC (tetrahydrocannabinol), the main active compound in marijuana.13 Those rats, when they reached adulthood, were given a way to self-administer heroin. The rats treated with THC used more heroin than other rats that had not been treated with THC. Another study, in 2014, published in the journal European Neuropsychopharmacology, similarly found that THC exposure in adolescence seemed to engender lasting changes to the rat brains.14 One more, published in 2004 in Biological Psychiatry, found that THC exposure increased rodent tolerance for other drugs, meaning it could increase the use of cocaine, morphine, and others later in life.15
These studies, though, were all done in animals, meaning extrapolation to humans is difficult. Furthermore, the findings are not at all unique to marijuana. Nicotine and alcohol have shown very similar effects in other animal studies—drugs that, of course, are perfectly legal.
There is some limited evidence of a gateway effect in humans, using studies of twins. For example, a study published in JAMA in 2003 followed sets of twins that were “discordant” for marijuana use: one twin had used the drug by the age of seventeen, and the other had not.16 This is a way to tease out any genetic underpinnings for a given effect, since identical twins share a genetic code: if genetics is responsible rather than a gateway effect, the discordant twins should have similar rates of drug use later. But they didn’t. In that study, the pot-user twin had a 2.1- to 5.2-times higher risk of using other drugs, becoming dependent on alcohol, and overall drug abuse or dependence than the pot-naïve twin. In other words, according to that study at least, genetics cannot explain the drug use, and thus the gateway effect gains support.
But that’s not the whole story—not remotely, as it turns out. As Susan Weiss, of NIDA, said: “Did marijuana change that twin and make them more likely to use other drugs? What was it about that one twin that made them use marijuana while the other twin didn’t? We don’t know the answer to that. Did he happen to have friends that were more deviant? It’s very difficult to completely interpret these things; most likely there is probably some convergence of factors.”17
Indeed, other studies have questioned that twin study’s conclusion. One published in Development and Psychopathology a few years later found the same link as the first—but only in nonidentical twins. This is remarkable: nonidentical (fraternal) twins don’t share DNA the way identical twins do, meaning that contrary to the first study, genetics apparently do play a role in drug use patterns. Put another way, the genetically identical siblings seemed to follow similar drug use patterns regardless of early exposure, but those who had different genes seemed to experience a gateway effect from early use. The authors of this second twin study concluded that “the ‘gateway effect’ might be better conceptualized as a genetically influenced developmental trajectory.”18
Would Christie’s point have sounded as strong, as presidential even, if he had said: “Marijuana likely plays a role in a genetically influenced developmental trajectory, similar in fact to nicotine and alcohol, and therefore I will prosecute pot offenses even in states that have legalized it”? That’s not as straightforward as, simply, pot is bad and you should go to jail if you use it.
All that conflicting evidence touches on only the biological mechanisms that could underlie a gateway effect; the cultural and social side comprises another set of research altogether.
The argument here is much easier to understand: if you are someone who uses marijuana habitually, you are likely going to be exposed to other types of drugs as well, just by being around other drug users and dealers. That concept actually makes a gateway effect hard to tease out—the direction from pot to, say, cocaine, likely reflects the easy access to marijuana in the United States as compared to the harder-to-find drugs like cocaine or heroin.
Some sociocultural studies have actually suggested a causal link between marijuana and harder drugs. One example is an ongoing study in New Zealand looking at 1,265 individuals born in 1977, whom researchers have followed for more than three decades, measuring various health and developmental parameters. The study’s lead author, David Fergusson of the University of Otago, has said that at least some of the data from this cohort of people “clearly suggest the existence of some kind of causative association in which the use of cannabis increases the likelihood that the user will go on to use other illicit drugs.”19
If that sounds convincing, don’t get too excited. He went on: “Where things get murky is in the area of the nature of the causal process.” We think pot leads to other drugs! But we have no idea how or why.
The availability of a given drug certainly does seem to play a role. One 2010 study comparing drug use patterns across countries found that “early-sequence” drugs including marijuana, alcohol, and nicotine did predict the use of other drugs—but the availability of each of those early drugs made a difference as to the strength of the gateway effect. For example, Japan has very low rates of marijuana use—in that study, only 1.6 percent of people tried it by the age of twenty-nine—and it also has higher rates of harder illicit drug use before using those in the alcohol/pot/nicotine group. These findings suggest that limiting access to marijuana—which, of course, was the policy position that led to this lengthy we-don’t-know-much-of-anything discussion—may not have much effect on limiting other drug use.
Since Governor Christie’s point was that he would enforce federal marijuana laws even over the state laws that made it legal, here is another interesting factor to chew on: the illegal status of the drug may, in fact, contribute to its gateway effects.
This makes rational sense: accessing one illegal drug probably opens doors toward accessing others. In contrast, going into a store to buy some beer or a pack of cigarettes doesn’t do much of anything to improve one’s access to meth.
There is evidence that legal status does matter—from everyone’s favorite legal-pot paradise, the Netherlands. In that country, 15 of every 100 cannabis users have tried cocaine at least once. That’s a lower rate than in countries where marijuana remains illegal, including Scotland, Italy, and Norway.20
Again, the lesson here, and through much of this book, is simple: science is hard. When a politician makes it sound easy, settled, definitive—look closer.
LET’S EXAMINE ONE MORE example of the OVERSIMPLIFICATION. This example illustrates another danger when it comes to dumbing down—even slightly!—a complicated scientific topic. Here’s President Barack Obama with a simple declarative statement:
2014 was the planet’s warmest year on record.21
Obama said this a number of times over the course of 2015, as he launched an aggressive, multifaceted campaign aimed at staving off some of the worst effects of climate change. And it sounds convincing, definitive: of all the years for which we have temperature data, 2014 (at the time he said it; 2015 subsequently obliterated the record, and 2016 is likely to do so once more) was the absolute warmest of the bunch.
Simple, right? Well, actually, no. Sort of. Somewhat? This is likely the most subtle and, honestly, nitpicky claim that this book will address. The president was almost correct, but not entirely—and the other lesson of the OVERSIMPLIFICATION is that even that tiny bit of wrongness can leave a politician open to far more misleading attacks by his opponents.
Obama’s warmest-year claim came from the agencies responsible for actually measuring the world’s temperature: the National Oceanic and Atmospheric Administration (NOAA) and the National Aeronautics and Space Administration, better known as NASA. NOAA’s monthly report on climate for December 2014 included this statement:
The average combined global land and ocean surface temperature for January–December 2014 was the highest on record among all years in the 135-year period of record, at 0.69°C (1.24°F) above the 20th century average.22
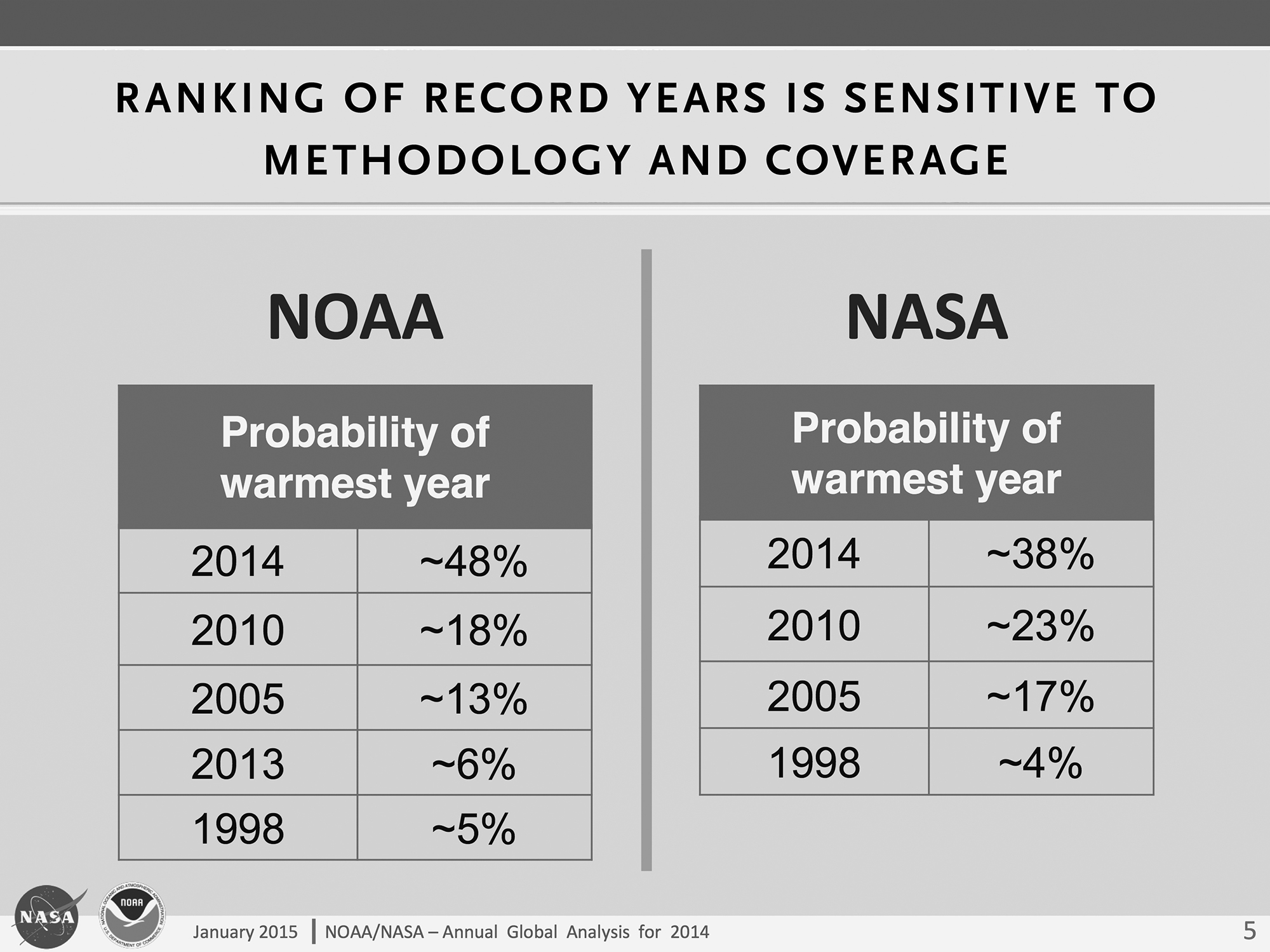
Again, pretty definitive! But that wasn’t the only publication NOAA and NASA offered regarding 2014’s place in the record books. They also put together a joint presentation, which included this slide:23
Credit: NOAA/NASA
Navigate past the bit of jargon at the top, and you can see 2014 atop a list of other years, with a “probability of warmest year” number next to it. What this means is that, according to NOAA’s calculations, 2014 had approximately a 48 percent chance of being the warmest year ever recorded; NASA gave it even less of a chance, about 38 percent. Measuring average temperatures across the entire globe is complicated and comes with a degree of uncertainty; these percentages reflect that uncertainty. In fact, according to NOAA, that 1.24°F above the twentieth-century average mentioned in its December 2014 statement had a range of uncertainty of 0.16 degrees in either direction. So, it could have been only 1.08 degrees above the twentieth-century average, which might move it down the list of warm years.
Was Obama flat-out wrong about 2014’s spot on the temperature leaderboard? Not quite. What those tables tell us is that 2014 was, at the time, more likely than any other individual year to have been the warmest ever. In fact, it was more than twice as likely, according to NOAA, as the second-most probable option, 2010, which clocked in at an 18 percent chance. But if the question was which is more likely to have been warmer—2014 or any other year (in other words, 2014 versus the field)—then the scales actually tip slightly in favor of the field, at 52 percent over 48 percent.
Nonetheless, Obama was just about as right as he could be, without quite getting there. Again, no other individual year had remotely as good a shot as 2014.
A NOAA climate scientist named Deke Arndt explained it to Andy Revkin of the New York Times this way:
This may seem pedantic, but it’s an important point: there is a warmest year on record. One of the 135 years in that history is the warmest. 2014 is clearly, and by a very large margin, the most likely warmest year. Not only is its central estimate relatively distant from (warmer than) the prior record, but even accounting for known uncertainties, and their known shapes, it still emerges as easily the most likely warmest year on record.24
So President Obama was essentially correct, but somewhat imprecise—a largely forgivable version of the OVERSIMPLIFICATION type of error. Though forgivable, here’s why it still matters: it gave climate change skeptics and deniers something to jump on. NOAA’s 48 percent mark doesn’t sound like “warmest ever” to the untrained ear, and NASA’s calculation actually pinned the number a bit lower. Those percentages led to headlines like this, from the Daily Mail in the United Kingdom: “NASA Climate Scientists: We Said 2014 Was the Warmest Year on Record . . . but We’re Only 38% Sure We Were Right.”25
Clunkiness of headline writing aside, this sort of triumphant cackling from climate deniers only fed the confusion that many in the general public likely have regarding climate change and climate science. Many such articles came from a certain corner of the media, and one could sympathize with a confused reader who might simply throw up his hands and say: “The scientists don’t even know what’s happening to the climate. Why should we do anything?”
By adding “probably” to his talking point, the president might have staved off some of the criticism, but he also could have simply skipped the “warmest year” line and used only his follow-up talking point: “Now, one year doesn’t make a trend, but this does: 14 of the 15 warmest years on record have all fallen in the first 15 years of this century.”26
In NOAA’s list of possible record years, you might have noticed that all were recent. This is the far more important point than simply which year squeaks out the statistical victory for warmest ever: the world has warmed dramatically in recent years, and regardless of which specific year wins out, all of the warmest years have come since 1998. After Obama’s claim, 2015 beat out 2014 for warmest year again—by a remarkably large margin, with a 94 percent certainty27—and 2016 is projected to reset the record yet again; though there will again be some degree of uncertainty, it will only further confirm the disturbing trend in rising temperatures.
As we’ve seen, the OVERSIMPLIFICATION can cheapen the magnificent complexity of science in pursuit of the perfect sound bite. Even just the examples in this chapter show that this technique has some very real impacts: abortion restrictions limit women’s access to reproductive health services, misinformation on drugs could contribute to overcrowded prisons and ruined lives, and feeding the climate deniers can only hurt attempts to save the planet. Don’t be seduced by simplified versions of science; they may sound convincing, but odds are they’re not entirely true.