Chapter 3
3D Bioprinting Techniques
Binil Starly
Rohan Shirwaiker Department of Industrial and Systems Engineering, North Carolina State University, Raleigh, NC, USA
Abstract
3D bioprinting technologies enable the digital fabrication of living constructs encapsulating cells, biomolecules, and biological moieties in spatially patterned structures. Several 3D bioprinting techniques have been developed over the last decade utilizing ink-jet printheads, applied pressure, laser-induced, acoustic wave, and solenoid valve based methods to deposit cells onto substrates. The ability to digitally direct and deliver cells has opened up applications in the fabrication of tissue models for studying disease pathophysiology, as complex multicellular constructs to perform drug screening and as constructs to model cancer growth. Compared to traditional techniques, the single biggest advantage of 3D bioprinting is the ability to digitally define the tissue construct of interest and reproduce the physical 3D structure through automated techniques and at resolutions not possible through any conventional photolithography techniques.
Keywords
3D in vitro tissue models
cell printing
regenerative medicine
tissue constructs
tissue engineering
3.1. Introduction
Critical to the success of tissue engineering and regenerative medicine (TERM) approaches, which require the use of a structural matrix, is the design of the scaffold and ensuing tissue construct. Cells involved in the regeneration process are influenced by the macro- and microarchitecture of the constructs. Two primary approaches have been developed to produce scaffolds and tissue constructs: (1) chemically driven processes, such as gas foaming, solvent casting, salt leaching, and freeze casting; and (2) computer-aided layered manufacturing-based approaches. Scaffolds produced through either of these approaches create structural matrices with defined pore architecture in terms of size, shape, and orientation. The three-dimensional (3D) surface area offered by these scaffolds serves as anchoring surfaces for cell adhesion, proliferation, and differentiation to the desired tissue type and function. In these approaches, scaffolds are produced first and the cells of interest are added in a subsequent processing step. The main drawbacks of this approach are the lack of cellular penetration and highly variable cell distribution within the scaffold matrix, primarily seen in scaffold sizes larger than 5 mm in thickness. These limitations arise from two reasons: (1) low cell seeding efficiency at the initial stages to fully inoculate the scaffold itself; and (2) lack of cellular proliferation deep into the scaffold architecture primarily due to rapid drop-off of nutrient concentration within the scaffold core. Several approaches have been developed by the research community over the last decade to mitigate these disadvantages. One popular approach has been the adoption of perfusion-based bioreactor systems to help improve cell seeding efficiency and the transport of nutrients within the scaffold to promote more uniform cellular adhesion and proliferation. An added benefit is that these bioreactors can be customized to provide mechanical and chemical stimulation to accelerate tissue formation. While generally successful, these methods are often limited to small-size defects and thus cannot be translated to thicker tissue constructs.
A more exciting approach is to directly involve cells within the construct design and fabrication process. This offers the advantage of combining multiple processing steps together through which a cellular construct is directly achieved. This approach helps to overcome the seeding efficiency and cell distribution problem. It opens up newer opportunities to customize and regulate the cellular microenvironment by the controlled placement of cells and other biological molecules in defined spatial orientation. In recent years, this approach has rapidly taken off, with several fabrication processes being developed to build in situ cellular constructs. These processes include photopolymerization-based processes, laser-based patterning, contact stamping, and cellular microencapsulation to form multicellular tissue spheroids and casting-based biocompatible processes to help achieve complex micro- and macroarchitecture (Valerie Liu Tsang, 2004; Derby, 2012). Perhaps one of the more exciting approaches is “3D bioprinting”-based methods due to the advantages they offer over competing methods to fabricate tissue and organ constructs. Among the advantages of this approach are
(1) Capability to build both 2D and 3D structures
(2) Ability to directly incorporate two or more different cell types in a defined spatial architecture in multi-scale patterns
(3) Flexibility to achieve hybrid processes simply by switching out “tool” options as seen in conventional manufacturing machines, such as CNC-based systems. This suggests that multiple nozzle types or print heads can be incorporated to achieve heterogeneous structures.
(4) Digitally enabled processes allow faster clinical translation and eventual approval by regulatory agencies. The control systems accompanying these processes offer the ability to control process parameters to help achieve desired cellular construct characteristics.
3.2. Definition and Principles of 3D Bioprinting
3D bioprinting is the process of automated deposition of biological molecules on a substrate to form a 3D heterogeneous functional structure with data derived from a digital model. The “print” material used in bioprinting techniques, also known as bioinks, often include a judicious combination of living biological cells, polymers, chemical factors, and biomolecules to form a physical and functional 3D living structure. The substrate is typically planar solid surfaces such as those of Petri dishes, glass slides, or wells of culture plates, although the concept can be extended to nonplanar, nonsolid, and flexible substrates. Living biological cells can be mammalian, insect, and plant-based as well as viruses and bacteria. 3D bioprinting has its roots in the conventional “ink-jet” process developed in the early 1950s that reproduces text and images from a computer file through droplets of ink deposited on a substrate such as paper. Much of the 3D bioprinting techniques have also grown from conventional additive manufacturing (AM) or layered manufacturing (LM) approaches. The complexity of the 3D bioprinting techniques, when compared to AM-based methods of scaffold fabrication, is attributed to the direct involvement of biological living materials during the fabrication process.
Hod Lipson in his book “Fabricated: The New World of 3D Printing” highlights 10 principles of 3D printing as guiding beacons to disrupt the current notion of manufacturing by reducing key barriers of time, cost, and skill level (Lipson, 2013). We have highlighted 10 principles of 3D bioprinting that will help shape the future of printing living tissue and organs for applications in regenerative medicine and tissue engineering.
Principle 1: Physical replication of the living construct from a digital blueprint file.
Bioprinting machines receive initial manufacturing process data input from a digital model of the construct. This digital model must serve as a repository of information that informs upstream and drives downstream manufacturing process activities.
Principle 2: Product customization with high degree of feature variety
Decision-makers and end-users of the printed construct must have the freedom to specify feature sets and functionalities of the construct with minimal complexity in manufacturing process activities.
Principle 3: Structurally heterogeneous product spanning more than two dimensional scales
Bioprinting processes must enable the realization of constructs with structural properties that vary in more than two dimensions. This is necessary to mimic the complexity of nature’s own tissue and organ architecture. Processes must take advantage of repeating functional units often seen in complex organs, such as the liver and kidney.
Principle 4: Precise spatial patterning of “bio-ink” materials
The drop-on-demand and the continuous print capability combined with robotic automation in bioprinting processes enable the precise spatial patterning of biological entities in two and three dimensions.
Principle 5: Minimal handling and manipulation of living cells
All bioprinting processes will need to ensure minimal mechanical and environmental stress on nonliving biological molecules, chemical factors, and living biological cells. This is to ensure protein and growth factor stability and maximum cellular viability during fabrication.
Principle 6: Conducive microenvironment for functional cells before and after printing
Processes must provide a suitable microenvironment for cells to sustain themselves both prior to and post-printing. Both viability and functionality of cells must be minimally altered during the printing process.
Principle 7: Construct must be functionally stable for downstream operations.
Any printed construct that involves biomaterials and cells must be mechanically, chemically, and/or biologically stable for use in downstream applications. Structurally weak constructs cannot be handled by either humans or automated equipment. Chemically unstable structures will lead to disintegration of properties, while biologically unstable constructs simply cannot be used reliably for downstream processes.
Principle 8: Plug-n-Play bioprinting machines with minimal operator assistance
The machines should be relatively easy to operate with minimal input from operators and should be capable of being installed at any qualified manufacturing facility or hospital. This capability is essential to economically produce the final construct at a price acceptable to the end user. If the machines require very high skilled operation with labor-intensive monitoring, manufacturing costs will be untenable.
Principle 9: Cellular construct, engineered tissue and organs on demand
The digitally enabled technology provides the capability for decision-makers and end-users to custom specify features of the product and request them on-demand, reducing the need for large inventory stock-up of biomaterials and final product storage solutions.
Principle 10: Repeatable and assured functional quality of the bioprinted structure
Bioprinting processes must be accurate to initial design specifications, precise in terms of structural/ biological variability, and repeatable in terms of its operation. This is an essential requirement for any process to be qualified by regulatory agencies for any targeted biomedical application.
Several bioprinting processes have achieved varying degrees of adherence to each of the 10 listed principles. The processes themselves are continually being improved by several research groups through expanded biomaterial selection, improved accuracy of spatial arrangement, degree of automation, and complexity of structures generated. Processes successfully meeting all 10 principles will yield commercially viable fabrication processes for the scale-up manufacturing of engineered tissue and organoid systems. If developed well, processes will also find limited challenges to being integrated into any upstream operation that would define the entire manufacturing process cycle for TERM. In the following sections, we will go through some of the most widely investigated 3D bioprinting processes, their fundamental working principles, their application toward the fabrication of cellular constructs, and differences between each process.
3.3. 3D Bioprinting Technologies
Scaffold-based regenerative medicine therapies involve the fabrication of scaffolds followed by seeding them with cells, preconditioning them inside an incubator, and then conditioning the construct inside a bioreactor to achieve adequate cell proliferation and function. Traditionally, both scaffold fabrication and cell seeding are two mutually separate and distinct steps in the process cycle. 3D Bioprinting techniques essentially combine both the scaffold fabrication and cell placement steps in an in situ layered manufacturing process step. The layer by layer bioprinting process enables the direct realization of scaffolding biomaterials, chemical molecules, and living cells in a desired spatial pattern to form the heterogeneous 3D construct. This feature was previously impossible to achieve with any of the conventionally produced tissue scaffolds or even with biopatterning approaches such as UV photopolymerization. The fundamental ability to “bioprint” essentially means that it is possible to accurately control the amount of “bioink” ejected out of the printhead or delivered on to a substrate. Figure 3.1 gives the generic architecture for a bioprinting machine with information and material flow paths highlighted among the entities contained with any system.
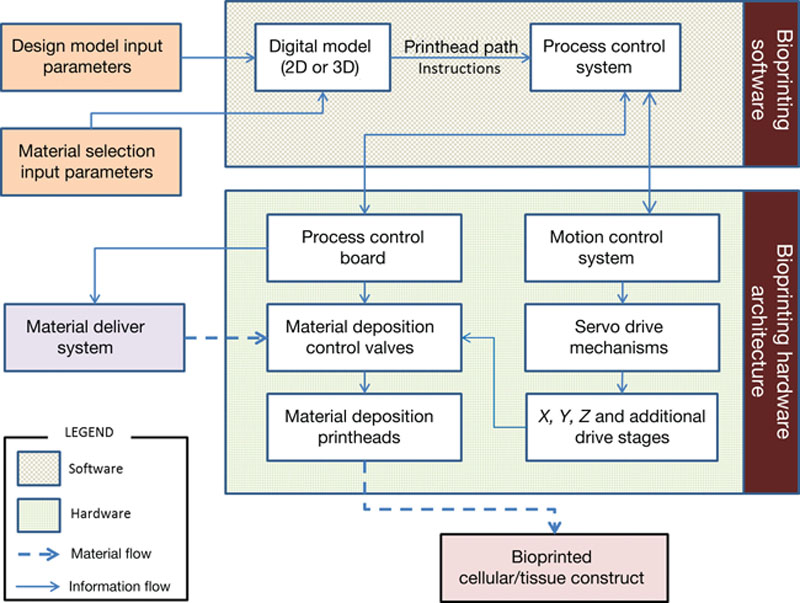
Figure 3.1 General 3D bioprinting hardware and software information and material flow.
3D Bioprinting processes begin with a digital model definition of the cellular and tissue construct architecture to be fabricated. In the case of 2D patterns, the digital files can be directly coded into the process control interface to drive the motion of printheads to help physically reproduce the architecture. This digital modeling of a complex 3D construct is typically performed in a computer-aided design (CAD) software environment. Both the external and internal architecture for the 3D construct can be designed with initial data obtained from CT/MRI images of the patient in need of a tissue replacement strategy. Image-based 3D reconstruction procedures can be carried out to help define the 3D digital model of the tissue replacement construct. Tools available in the software environment can help identify different material regions which specify the placement of the biomaterial matrix, biological molecules, and living cells. Process algorithms are written to convert the digital model to printhead path instructions necessary to drive the hardware systems. The exact format for machine instructions in such computer-aided manufacturing (CAM) depends on the printing technique and hardware configuration utilized. Once the signal for printing is activated, the process control system drives the bioprinting system hardware components for the physical realization of the printed construct.
Complex engineered tissue and cellular construct-based products will be made from spatially patterned cellular layers which ultimately will become large aggregates for a specialized tissue function. The entire operation must take place in sterile conditions to limit contamination of both source raw material and the final construct. If cells are involved in the fabrication process, the total time needed to produce a construct can be critical. The amount of time available is dependent on the cell type used. Unless printing conditions are well suited for cell maintenance, time to fabricate constructs should not exceed an hour. Longer times will result in reduced cellular viability and abnormally higher cellular stress, which will lead to degraded function.
We describe the main bioprinting techniques used by the research community to print biomaterials including cells and biomolecules to form 3D constructs. These 3D constructs can be used as tissue models for drug screening, as disease models to study cancer, and as constructs meant for animal or human implantation. Due to the size scale of cells, which are generally in the 5–20 μm size range, all bioprinting processes work at dimensional scale levels larger than the cell type utilized.
3.3.1. Ink-Jet-Based Bioprinting
Ink-jet bioprinting is a noncontact printing process involving the precise deposition of picoliter to nanoliter droplets of “bioink” (a low-viscosity suspension of living cells, biomolecules, growth factors, etc.) onto a “biopaper” (a hydrogel substrate, culture dish, etc.) in a digitally controlled pattern. It is a direct adaptation of the conventional ink-jet printing process, and a majority of current ink-jet bioprinting activities continue to be conducted using partially modified commercially available desktop ink-jet printers. There are two fundamental approaches to ink-jet printing: continuous (CIJ) and drop-on-demand (DOD). In the CIJ approach, an uninterrupted stream of droplets is produced by forcing the ink through a microscopic nozzle orifice under pressure and deflecting it onto the substrate using an electrostatic field. Where droplet deposition is not required in the digital pattern, the droplets are steered into a gutter and collected for reuse. In the DOD approach, the ink droplets are ejected through the nozzle orifice by creating a pressure pulse inside a microfluidic chamber only when required. The DOD approach is of primary interest in bioprinting due to the pulsed nature of printing. The CIJ approach is not well suited to bioprinting due to the need for conductive ink formulations and the risk of contamination due to ink recirculation, among other reasons.
The DOD approach can be further categorized into thermal (heat) or piezoelectric (mechanical compression) based on the droplet actuation mechanism. A schematic of DOD ink-jet printing based on both mechanisms is presented in Figure 3.2. In thermal DOD, an electric current pulse applied to the heating element (thin film resistor) rapidly vaporizes a small pocket of ink in the microfluidic chamber. The resulting vapor bubble creates the pressure pulse that propels the ink droplet through the nozzle orifice and onto the substrate. In piezoelectric DOD, a microfluidic chamber above the nozzle contains a piezoelectric transducer for droplet actuation instead of a heating element. A voltage pulse applied to the transducer causes it to expand, creating the transient pressure that results in droplet ejection. For both forms of DOD, the rheological and surface tension properties of the ink govern their ability to be printed. The ink viscosity requirements vary from system to system, but a typical threshold is around 30 mPa/s (Reis et al., 2005; Seerden et al., 2001; Derby, 2008). In addition to the ink characteristics, the orifice size, the distance between nozzle and substrate, the frequency of the current pulse and resulting temperature gradient (thermal DOD), and the frequency of the voltage pulse and piezo-deformation characteristics of the transducer (piezoelectric DOD) have an effect on the ejected droplet size and spatial resolution in ink-jet printing.
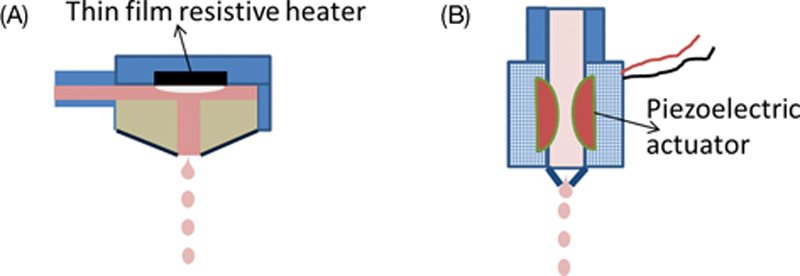
Figure 3.2 Inkjet printing mechanisms. (A) Thin film resistive heater generating a vapor bubble that ejects the bio-ink material; (B) A piezoelectric driven actuator that squeezes out a defined quantity of the bio-ink upon pulsed activation. Both mechanisms can either work in continuous or drop-on-demand jetting mode.
In addition to creating structures of nonliving biomolecules, such as DNA (Okamoto et al., 2000) and proteins (Delaney et al., 2009), DOD ink-jet bioprinters have been successfully used to print and pattern live mammalian cells, opening up new and exciting avenues in the field of tissue engineering and regenerative medicine. Ink-jet printing also offers the capability to print multiple cell types, biomaterials, or their combinations from different printheads in a single fabrication operation, allowing for complex multicellular patterns and constructs. The concept of tissue and organ 3D printing, which is being widely explored today, has evolved over years starting with ink-jet bioprinting. Both thermal and piezoelectric DOD printers have been explored for cell bioprinting, but the use of thermal ones has been more prevalent (Cui et al., 2012). In thermal ink-jet printing, while the localized temperature around the heating element can reach between 200–300°C, it lasts for only a few microseconds, and the ejected cells are subjected to a temperature rise of only a couple of degrees above ambient for 2 μs (Cui et al., 2012; Roth et al., 2004; Cui et al., 2010).
Xu et al. (2005) have highlighted the initial challenges in adapting the piezoelectric mechanism for ink-jet cell printing, which revolve around their higher ink viscosity. Primarily, the frequencies and power employed by commercial piezoelectric printers lie within the same range of vibrating frequencies (15–25 kHz) and power (10–375 W) that are known to disrupt cell membrane and cause cell lysis during sonification (Cui et al., 2012; Xu et al., 2005; Simons et al., 1989; Hopkins, 1991). Adapting piezoelectric printers for less viscous ink to lower the frequency and power would be challenging, since the resulting ink leakage and mist formation during printing would affect the spatial and feature resolution (Cui et al., 2012; Xu et al., 2005). However, it should be noted that in recent years, other research groups have successfully demonstrated more than 90% viability for piezoelectrically deposited mammalian cells including human osteoblasts, fibroblasts, and bovine chondrocyte cells (Saunders et al., 2005; Saunders et al., 2008; Saunders et al., 2004). Nonetheless, the original investigations into the feasibility of ink-jet bioprinting of live cells were performed on a piezoelectric system. (Wilson and Boland, 2003) used a bioprinter derived from commercially available HP 660C piezoelectric ink-jet printer and custom designed piezoelectric printheads to print viable line patterns (2D) of bovine aortal endothelial cells (BAEC) and smooth muscle cells. In a subsequent study, they printed BAEC aggregates layer-by-layer (3D) in thermosensitive gels with the same printer, and demonstrated that the closely placed cell aggregates could fuse together, which is critical for tissue formation (Boland et al., 2003). Later, they also became the first to use a commercial thermal ink-jet printer (HP 550C and a modified HP 51626a ink cartridge) to create viable patterns of mammalian cells (Chinese Hamster Ovary (CHO) and embryonic motoneuron cells) onto gel substrates (Cui et al., 2010). The viability of printed mammalian cells was found to be in the range of 85–95% for different cell concentrations. The difference in apoptosis ratio and heat shock protein expression level between printed and nonprinted cells was reported to be not statistically significant. Other studies have further investigated the fundamental effects of ink-jet process parameters on viability of different types of cells, and also developed multimaterial composite strategies that combine cells with other biomaterials including proteins, growth factors, and scaffolding polymers (Pepper et al., 2012a; Pepper et al., 2012b; Cui and Boland, 2009; Xu et al., 2006; Chahal et al., 2012). Binder et al. (2011) have provided a primer on DOD ink-jet bioprinting for the research community. Cui et al. (2012) have discussed thermal ink-jet printing from the tissue engineering and regenerative medicine perspective. Derby (2008) has provided a detailed review of ink-jet bioprinting of proteins and hybrid cell-based biomaterials.
3.3.2. Pressure-Assisted Bioprinting
Pressure-assisted bioprinting (PAB) refers to a set of extrusion-based layered manufacturing processes capable of creating digitally controlled 3D patterns and constructs. Biomaterials including polymers and ceramics, proteins and biomolecules, living cells, and growth factors as well as their hybrid structures can be printed using PAB. For printing cells, the bioink is essentially a cell-laden hydrogel of the appropriate viscosity capable of being extruded under pressure through a microscale nozzle orifice or a microneedle at temperatures around 37°C to maintain cell viability. The mechanical integrity of the extruded structures can be controlled through thermal or chemical cross-linking, or multimaterial channel approaches postdeposition. During the process, the biomaterial is contained in a temperature controlled cartridge inside a three axis robotic printhead with a nozzle or microneedle. Deposition takes place by pneumatic pressure, plunger or screw-based extrusion of the material as a continuous filament through the nozzle or microneedle orifice onto a substrate. The substrate can be solid (e.g. culture dish), liquid (e.g. growth media) or a gel based substrate material. The substrate as well as the deposition setup can be contained within a sterile and climate-controlled environment further enabling the use of temperature-sensitive cells and biomaterials. The printhead trajectory is guided by layered data obtained from the digital model of the construct to be laid out. A schematic of the PAB setup is presented in Figure 3.3. The rheological properties of the biomaterial, extrusion temperature, nozzle type used, and applied pressure are the critical parameters that affect the physical and biological characteristics of the printed construct.
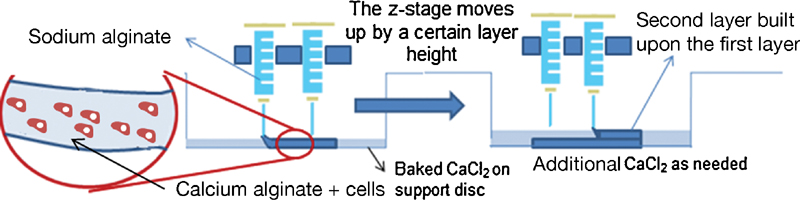
Figure 3.3 Pressure-assisted bioprinting using sodium alginate and calcium chloride as the cross-linking agent to fabricate calcium alginate-based hydrogels. The hydrogels can encapsulate or immobilize any desired cell type within the gel. The precursor solution of sodium alginate and water can be modified to include collagen or other peptides to enhance cellular attachment to promote growth within the gel.
Multiple commercially available multinozzle systems that can be used to deposit biopolymers, cells, and growth factors are currently being marketed by Envisiontec GmbH, Germany (3D Bioplotter) and nScyrpt, Florida, USA. Other low-cost 3D printing systems, such as those available from Fab@Home, are being modified to fabricate cellular constructs. Traditionally, pressure-assisted deposition processes were being utilized for the fabrication of tissue-engineered scaffolds, since the controlled pore architecture due to the CAD/CAM-controlled layer-by-layer approach was not achievable by traditional scaffold fabrication processes, such as salt leaching and solvent casting. Several studies have focused on the design and optimization of scaffolds using polymers, such as PCL, PLGA, PLLA, PEG, and their blends, and their composites with ceramics, such as hydroxyapatite (HA) and tricalcium phosphate (TCP), have been reported (Vozzi et al., 2002; Wang et al., 2004; Xiong et al., 2001; Landers and Mulhaupt, 2000; Park et al., 2011).
In recent years, with the emergence of the concept of organ printing, the focus has shifted toward direct printing of cell-encapsulated hydrogels. (Yan et al., 2005a; Yan et al., 2005b; Wang et al., 2006; Cheng et al., 2008), and (Xu et al., 2007) used pressure-assisted multisyringe deposition systems to fabricate liver constructs by encapsulating rat hepatocytes in hydrogels including gelatin in conjunction with chitosan, alginate, and fibrinogen. The initial structural support was achieved by thermal cross-linking of gelatin extruded from a low-temperature syringe onto a warmer stage, and the constructs were further strengthened by chemical cross-linking. Favorable cell viability and function results were obtained based on liver tissue markers (urea and albumin production). Although there was difficulty in stabilizing the 3D structure due to enzymatic degradation of the gelatin/chitosan constructs, the process allowed simultaneous deposition of living cells within a biomaterial. Furthermore, (Xu et al., 2009) and (Li et al., 2009) fabricated biomimetic 3D constructs by simultaneous deposition of adipose-derived stem cells and hepatocytes encapsulated in gelatin-based hydrogels. Similarly, Fedorovich et al. have demonstrated the feasibility of multicellular bioprinted constructs incorporating goat multipotent stromal cells (MPSCs), endothelial progenitor cells in Matrigel®, alginate-based materials for bone grafts (Fedorovich et al., 2001), human mesenchymal stem cells (MSCs), and articular chondrocytes for osteochondral grafts (Fedorovich et al., 2011).
Most recent approaches with pressure-assisted deposition have focused on creating multimaterial multifunctional constructs. For example, (Schuurman et al., 2011) have demonstrated fabrication of hybrid constructs of polycaprolactone (PCL) and chondrocytes-laden alginate. The alginate was cross-linked with calcium chloride postdeposition, but showed relatively good cell viability. Using the same strategy, (Shim et al., 2011) successfully fabricated hybrid constructs containing a PCL/PLGA blend as the structural polymer alongside collagen containing preosteoblast cells. Using the same polymer and cell-laden hydrogel composite strategy, (Lee et al., 2014a) fabricated a viable auricle using PCL for the structural framework, water-soluble poly-ethylene-glycol (PEG) as a sacrificial material, and chondrocytes/ adipocytes differentiated from adipose-derived stromal cells encapsulated in alginate hydrogel as the biological component. Quantitative analyses showed that the auricular cartilage and earlobe fat can be regenerated while maintaining their inherent functions in different regions of the same structure at the same time by printing chondrocytes and adipocytes separately. (Mannoor et al., 2013) fabricated a bionic ear in the anatomic geometry of a human auricle using silicone as the structural component, bovine chondrocytes-laden alginate as the biological component, and silver nanoparticles infused silicone for electronics. They were able to demonstrate structural integrity and shape retention, >90% viability of the printed chondrocytes, and enhanced auditory sensing for radio frequency reception, all within a single simultaneously printed 3D construct.
3.3.3. Laser-Assisted Bioprinting
Laser-assisted bioprinting (LAB) is a set of noncontact direct writing processes that utilize a pulsed laser beam to deposit biological materials using cells onto a substrate. Three components are central to most LAB systems—a pulsed laser source, a bioink-coated “ribbon,” and a receiving substrate. Nanosecond lasers with UV or near UV wavelengths are used as the energy source. The “ribbon” is a glass or quartz target plate that is transparent to the laser radiation wavelength and has one side coated with a heat-sensitive bioink consisting of cells either adhered to a biological polymer or uniformly encapsulated within a thin layer of hydrogel. Depending on the optical characteristics of the bioink and the laser wavelength, the system may also contain a laser-absorbing interlayer between the target plate and the bioink to allow viable cell transfer. The receiving substrate positioned below the bioink-coated side of the ribbon is coated with a biopolymer or cell culture medium to maintain cellular adhesion and sustained growth after cell transfer from the ribbon. The pulse of laser causes rapid volatilization at the ribbon’s plate-bioink interface and propels a high-speed jet of the cell-laden bioink onto the receiving substrate.
A schematic of the LAB approach is presented in Figure 3.4. Commonly used LAB processes based on this fundamental working principle include absorbing film-assisted laser-induced forward transfer (AFA-LIFT) or biological laser processing (BioLP) (Hopp et al., 2004; Barron et al., 2005) and matrix-assisted pulsed laser evaporation direct writing (MAPLEDW) (Barron et al., 2004; Patz et al., 2006). The AFA-LIFT and BioLP are bioprinting versions of the laser-induced forward transfer (LIFT) technique which was originally developed for the direct writing of metal features using a high-energy pulsed laser to deposit a metal film on an optically transparent substrate and has also been employed for direct writing of biomolecules (Duocastella et al., 2007). In AFA-LIFT and BioLP, a high-powered pulsed laser is used to vaporize and deposit the bioink onto the substrate. To protect cells from direct exposure to the high-energy laser beam, a sacrificial metal or metal oxide (e.g. Au, Ag, Ti, and TiO2) thin film (∼100 nm) is included at the interface between the target plate and the bioink. The rapid thermal expansion of this interfacial layer due to the high-energy laser pulse propels a small volume of bioink onto the substrate, but with minimal heating of the bioink to prevent cell damage. The BioLP process also utilizes computer-controlled motorized stages and a CCD camera to visualize and focus the laser. Unlike AFA-LIFT and BioLP, the MAPLE-DW process uses a low-power pulsed laser and an interfacial layer of a sacrificial hydrogel such as Matrigel® instead of a metal thin film to accomplish cell transfer. This interfacial layer that acts as an attachment layer for the cells also absorbs the laser energy to prevent it from affecting them. Similar to BioLP, computer-controlled manipulation of the stages coupled with a CCD camera allows for selective cell patterning. Laser-guided direct writing (LGDW) is another commonly used LAB process, but unlike other LAB processes, it does not use a pulsed laser or a print ribbon (Nahmias et al., 2005). Instead, the optical energy of a weakly focused continuous laser is directly used to target and manipulate individual cells from liquid cell suspension onto the substrate. Several parameters related to the laser source, bioink, substrate, interfacial ribbon layer, among others, affect the resolution and performance of LAB processes, and have been described by (Guillemot et al., 2010).
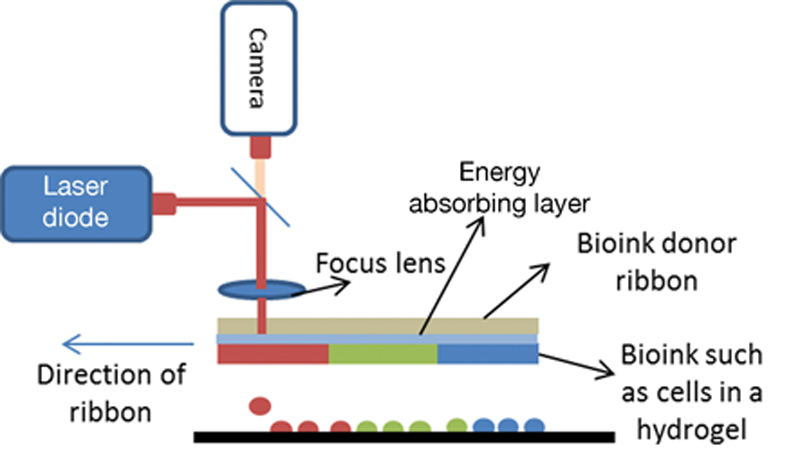
Figure 3.4 Laser-assisted bioprinting
MAPLEDW was one of the first processes used to successfully demonstrate the feasibility of laser-based printing of mammalian cells. Bu et al. (2001) first demonstrated the patterning of Chinese hamster ovary (CHO) cells using the process. Later, Ringeisen et al. (2004) and Barron et al. (2005) printed mouse carcinoma cells (P19), human osteosarcoma (MG-63), and rat cardiac cells with the same process with viability greater than 95%. Recently, (Schiele et al., 2010) have used the MAPLEDW to create viable patterns of human dermal fibroblasts, mouse C2C12 myoblasts, bovine pulmonary artery endothelial (BPAEC), breast cancer (MCF-7), and rat neural stem cells. The AFA-LIFT and BioLP processes have also been successfully used to print various cell types including human osteosarcoma (MG-63), rat Schwann and astroglial and pig lens epithelial cells, BAEC, human umbilical vein endothelial cells (HUVECs), and human umbilical vascular smooth muscle cells (HUVSMC). Invalid source specified. Schiele et al. (2010b) have recently provided a thorough topical review of LAB processes and their applications.
3.3.4. Solenoid Valve-Based Printing
Microdispensing using solenoid valves has seen applications in depositing solder and adhesives onto electronic boards, deposition of optical and electrical polymers, and deposition of biomolecules such as DNA, proteins, and diagnostic reagents. The system has shown itself capable of printing live biological cells for dermal repair, printing mesenchymal stem cells onto tissue well plates, and printing of constructs within a controlled environment. A complete system consists of a fluid reservoir, a solenoid-based dispensing device with droplet volumes ranging from 5 pl to 1 nl droplet quantities, heating elements to control the nozzle head temperature, connections to the pneumatic controller, and an inert gas source. Multiple print head assemblies can be fitted together to improve the throughput of the system. Figure 3.5 shows the schematic of a solenoid-based jetting nozzle. The droplet volume of the printed materials can be controlled by the applied air pressure and the frequency of the solenoid valve open time. Electrical pulse signals sent from the computer can engage or disengage the solenoid leading to droplet ejection from the nozzle. Different nozzle diameters can be attached to the print head to deliver precise quantities of the fluid. The solenoid valve system does not involve heat and is capable of accepting viscous polymers such as collagen and 1–2% sodium alginate. Multiple nozzles can be fitted to the robotic stage to print multiple materials to form a complex heterogeneous construct.
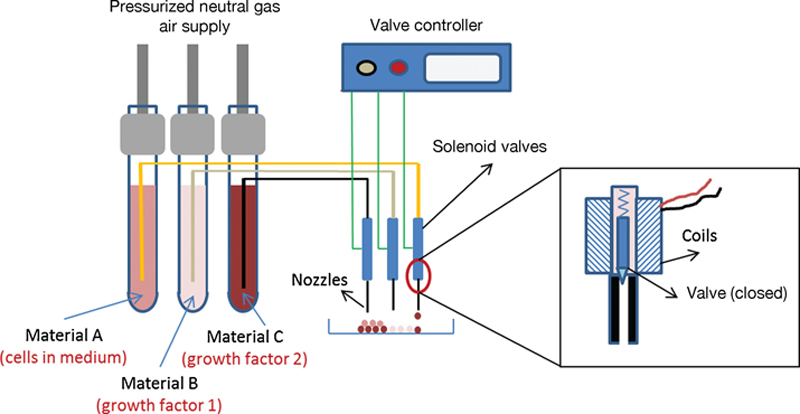
Figure 3.5 Solenoid valve-based bioprinting capable of depositing 20 pl or higher droplets of living cells and biological molecules.
Yoo and coworkers (Lee et al., 2010) reported using this technique for the on-demand fabrication of cellular constructs containing a neural cell line, a fibrin matrix containing a vascular endothelial growth factor (VEGF), and a collagen hydrogel. Since fibrin gel cannot be preloaded into the cartridge, its constituents—fibrinogen, thrombin, and heparin—were separated into two different material cartridges. A third cartridge contained the neural cells to be printed and a fourth cartridge contained a sodium bicarbonate to help in the cross-linking of the collagen gel. With an initial cell density of 1 × 106 cells/ml, each printed droplet of volume 11 ± 0.6nl contained about 56 ± 9 cells. Reported viability of cells within the 500 μm thick collagen construct was greater than 93% soon after printing. This work demonstrates the feasibility of precisely placing desired concentrations of VEGF within spatial locations inside the construct to affect cellular behavior, namely proliferation and differentiation, by controlling the time release behavior of these growth factors. In another study using a similar technique, Karande and his team demonstrated the solenoid-based printing technique to engineer human skin. Fibroblasts and keratinocytes representing the epidermis and dermis respectively, along with collagen were bioprinted to showcase the capability of fabricating a complex living system. The printed skin tissue provides applications in topical drug formulation discovery and screening along with designing autologous grafts for wound healing (Lee et al., 2014b).
3.3.5. Acoustic-Jet Printing
For applications that require precise placement of single cells, acoustic-based bioprinting is a viable method to deposit picoliter quantities of the medium or hydrogel encapsulating a single cell in a droplet. The ejection of the fluid medium is by focused surface acoustic waves generated by a piezoelectric actuator (such as quartz, lithium tantalite, and lithium niobate) on interdigitated and periodically spaced gold rings. Upon activation by a sinusoidal electrical signal at the same resonant frequency of the device, surface acoustic waves are generated (Figure 3.6). With specially designed printheads, these waves pass through the fluidic environment, in this case, a biomaterial with cells, and are focused to a single point at the fluid-air interface. At the focal point, the waves interfere constructively at the point and the forces exerted by the acoustic radiation will be larger than the surface tension of the fluid leading to the ejection of a droplet from the printhead. The higher the applied frequency, the smaller the droplets generated from a single nozzle. The droplet diameter also depends on the viscosity of the solution contained within the device. For example, a sucrose-dextrose solution can generate droplets ranging from 200 to 3 μm with a respective frequency range of 10 to 100 MHz at a prescribed operational wavelength. The droplet diameter can be customized to the biomolecule being printed. The drop-on-demand feature of the actuation makes for fast deposition speeds of up to 100,000 droplets per second, making it one of the fastest printing methods available. Multiple nozzles and associated acoustic wave generators can be placed periodically to improve throughput rates of fluid ejection. Hence, this method can enable high-throughput studies by patterning a range of biomolecules including RNA, DNA, extracellular matrix proteins, drugs, growth factors, and living cells in microwells (Moon et al., 2010; Gurkan et al., 2014).
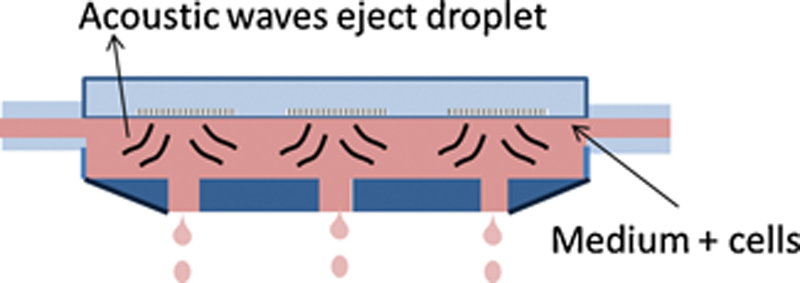
Figure 3.6 Acoustic wave-based bioprinting.
3.4. Challenges and Future Development of 3D Bioprinting
The eventual goal of all biomedical technologies is to make them clinically available so that patients can benefit from them. All bioprinting processes discussed in this chapter are at different stages of development along that path, but none of them have been translated to FDA-approved clinical applications yet (Table 3.1). By allowing the integration of living and nonliving biomaterials in hybrid structures, bioprinting overcomes several drawbacks associated with previous approaches to tissue fabrication. But despite the significant effort in developing and improving process principles and demonstrating their feasibility for viable cell printing, several supplementary and complementary challenges will need to be addressed to accelerate the successful clinical translation of bioprinting technology, first in vitro, and then in vivo. As several researchers and experts have noted, thorough characterization of the underlying process mechanisms, their inputs and their outputs will help in the development of machines and systems with low output variability, eventually leading to lower processing costs and improved commercial and clinical potential.
Table 3.1
Comparison between bioprinting processes
| Process | Common subprocesses/mechanisms | Mammalian cell/tissue types | Typical hydrogels/bioinks/biopaper | Suitability for applications | Salient features | ||||
| Therapeutic | Drug-testing and disease modeling | Cell interaction studies | Spatial resolution | Single cell control | Throughput | ||||
| Ink-jet Bioprinting | • Thermal • Piezoelectric | • Motoneurons (Cui et al., 2012) • Endothelial cells (Saunders et al., 2005) • Smooth muscle cells | • Soy agar (Cui et al., 2012) • Matrigel (Saunders et al., 2005) • Alginate | L | H | M | M | L | H |
| Pressure-assisted Bioprinting | • Air-pressure • Screw-extrusion | • Hepatocytes (Xiong et al., 2001; Landers and Mulhaupt, 2000; Park et al., 2011; Yan et al., 2005a; Yan et al., 2005b; Cheng et al., 2008; Fedorovich et al., 2001) • Endothelial progenitor cells (Xu et al., 2007) • Pre-osteoblasts (Fedorovich et al., 2001) • Adipocytes (Fedorovich et al., 2001) • Ovary cells • Smooth muscle cells • Fibroblasts | • Gelatin (Xiong et al., 2001; Landers and Mulhaupt, 2000; Park et al., 2011; Yan et al., 2005a; Yan et al., 2005b; Wang et al., 2006; Cheng et al., 2008; Fedorovich et al., 2001) • Alginate (Xiong et al., 2001; Landers and Mulhaupt, 2000; Park et al., 2011; Xu et al., 2007; Xu et al., 2009; Li et al., 2009; Fedorovich et al., 2011; Schuurman et al., 2011) • Matrigel Xu et al., 2007 • Collagen (Fedorovich et al., 2001) • Hyaluronic acid (Fedorovich et al., 2001) • Agarose | H | H | L | L | L | H |
| Laser-assisted Bioprinting | • MAPLE-DW • AFA-LIFT/BioLP • LG-DW | • Epithelial cells (Lee et al., 2014a) • Cardiac cells (Barron et al., 2005) • Neurons (Barron et al., 2004) • Spinal cord cells (Ringeisen et al., 2004) • Hepatocytes (Schiele et al., 2010a) • Ovary cells (Lee et al., 2010) • Carcinoma (Lee et al., 2014b) • Myoblasts (Moon et al., 2010) • Neural stem cells (Moon et al., 2010) • Smooth muscle cells | L | H | H | M | M | M | |
| Solenoid-based Printing | N/A | • Neural cells (Lee et al., 2010) • Fibroblasts (Lee et al., 2014b) • Keratinocytes (Lee et al., 2014b) | • Fibrin (Lee et al., 2010) | H | H | L | M | M | M |
| Acoustic-jet Printing | N/A | • Embryonic stem cells (Moon et al., 2010) • Fibroblasts (Moon et al., 2010) • Cardiomyocytes (Moon et al., 2010) • Raji cells (Moon et al., 2010) • Breast cancer cells (Gurkan et al., 2014) • Embryonic kidney cells [B] | • Agarose (Moon et al., 2010) • PBS (Moon et al., 2010) • Dextran (Gurkan et al., 2014) | L | M | H | M | H | H |


L: Low; M: Medium; H: High.
We have highlighted here several issues that must be addressed by the 3D bioprinting research community for the wide-scale adoption of this base technology for several therapeutic and nontherapeutic applications.
Lack of digital models: Data drive the bioprinting machines. Currently there is a lack of software architecture with necessary design tools to engineer tissue and organ systems. New data structures must be developed to capture the heterogeneous information necessary to define such living products. Virtually defining the placement of cells, biomaterials, and biological molecules will lead to designs that are robust. The digital definition can also translate to drive all downstream manufacturing operations. Conventional design software revolutionized methods through which automobiles, airplanes, and consumer and medical products are designed and manufactured. Similar software design platforms must be available if the benefits of bioprinting are to be widely adopted by the research and industrial communities. On a similar note, designers should also be presented with tools to simulate engineered tissue/organoids to pursue what-if analysis scenarios. Tissue systems constantly remodel and change over time. Tools to help predict end function, stability, and efficacy will be necessary for the wide-spread adoption of bioprinting technologies.
Biomaterials are limited, proprietary, and expensive: Another key limitation is the limited class of biomaterials in which the cells are encapsulated. While cell-free scaffolds are printed in a variety of biomaterials, there has not been much development into designing newer biomaterials able to accommodate the encapsulated cells and the printing process in general. While it is generally understood the cells will secrete their own extracellular matrix over time, the initial biomaterial plays an important role in producing the right microenvironment for cells to be accommodated in their new engineered environment. Polymers such as calcium alginate, poly-lactic-glycolic acid (PLGA), and poly-ethylene glycol-diacrylate (PEGDA) are some of the most common polymers used in the 3D bioprinting process. Most polymers used for bioprinting are synthesized in laboratories or are available in commercial quantities that can be cost-prohibitive. There is a need to expand the library of biomaterials to be used for the several bioprinting machines available. Similar to established metals and polymers with their defined properties, new classes of printable biomaterials must be developed to produce engineered tissue and organs.
Lack of adequate cell loading and uniform cell distribution: Engineered constructs of the heart or liver will require millions of cells packed in given volume of a printed construct if they are to function in a physiological manner. Current bioprinting techniques are limited to less than 10 M cells/ml. Improving cell density to reach greater than 50 to 100 M cells/ml will be necessary for proper tissue and organ function. Long fabrication times can lead to settling down of the cells in the printhead chamber. This will lead to nonuniform distribution of cells resulting in inconsistent results. For bioprinting technologies that specify one or two cells per droplet, improving the reliability of cells contained within a droplet is necessary for improving the robustness of the process.
Material development and standardization: Bio-inks are an integral part of the bioprinting technology. It is not the bioprinting process parameters alone, but the material–process interactions that govern the viability and success of the resultant constructs. Hence, developing appropriate bioinks and comprehensively characterizing their rheological, mechanical, and biological characteristics is critical to the success of bioprinting. It is accepted that this development and characterization will have to be cell/tissue- and process-specific. Standardization of the living as well as nonliving bioink components and their sources is also of equal importance, not only from the final production perspective, but also during the process development stage, since any variability in the bioink characteristics ultimately affects the variability of the bioprinting process output. For example, lot-to-lot variability in the growth media can affect the viability of living and biomolecular components of the bioink post printing. Similarly, the viability of fabricated structures can be affected by the source of cells and their storage method prior to printing, even when the bioprinting process parameters are held constant. During the development and characterization of a bioprinting process for allogenic applications, it is critical that the appropriateness of the selected cell source be determined from an application perspective, and its characteristics be thoroughly analyzed and documented. Concepts such as crowd sourcing can be used during the research and development phase to eliminate variability caused by the bioink material.
Measurement and in-process monitoring technologies: A key technology gap to advance bioprinting technologies for engineered tissue is the ability to monitor in real time the process of printing cells and biological moieties. While optical methods are being utilized to monitor droplets and printed constructs, currently there are limited options available to nondestructively evaluate the “living” components within the printed constructs. For example, in the scale-up production of printed cellular constructs, how do we monitor both the placement and functionality of cells within the biomaterial? The problem is even more challenging when encapsulated in 3D hydrogel. Real-time label-free monitoring methods must be developed to advance the scalability and integration of the bioprinting process to economically viable production. The data generated can also help to identify critical process parameters and help implement statistical process control for the bioprinting processes. Ultimately these technologies will be needed to help scale-up or scale-out the process to help meet the demand for customized tissue- and organs-on-demand.
3.5. Conclusion
Undoubtedly, the ability to accurately place cells and cellular constructs to form engineered tissue and organoid systems by the definition of a digital model is powerful. The technologies presented offer viable and high-throughput approaches to printing cells and hydrogels in a biocompatible and cell-friendly environment. Spatial control, precise placement of multiple cell types, and high-throughput speed when compared to manual methods are clearly the biggest advantages of the 3D bioprinting technology. When compared to microfabrication techniques such as microstamping and micromolding, the biggest advantage of 3D bioprinting is the ability to define complex interior architecture in true three-dimensions due to the layer by layer additive manufacturing approach taken by most bioprinting technologies. This bottom-up technology bridges microscale and mesoscale definition of engineered tissue, thereby offering the possibility of addressing the challenge of building thick tissues and organ systems.
An immediate application of 3D bioprinting are the use of these systems to create disease models to study pathophysiology, as complex in vitro tissue models to screen for new therapeutic drugs and as systems to help achieve engineered meat and leather products. Maturation of these applications of bioprinting will see some of the groundwork being laid to address the challenges highlighted in the previous section. Lab-grown organs and functional tissue intended for human implantation will likely see another decade of fundamental research activity before they have the possibility to become real application scenarios. The future success and commercial viability of the process will depend on efforts to address the challenges to adoption of bioprinting. The systems have the potential to be widely adopted and integrated within conventional cell culture laboratories. They provide a new avenue for researchers to ask research questions in the third dimension, thereby replicating the dynamics of in vivo cellular physiology and microenvironment. Bioprinting also has clear applications in regenerative medicine with the ability of these machines to be used in clinical room settings for achieving personalized tissue-on-demand and replacement organs. There are challenges to achieving this vision, but as advancements are made in hardware and software technology coupled with an increased understanding of cellular behavior in the engineered environment, bioprinting will be a viable new biomanufacturing technology.