Your new baby will need about 16 hours of sleep a day. However, his tiny stomach means that he won’t be able to sleep for more than a few hours at a time before crying to eat again. While he was inside you, his needs for fluid and nourishment were supplied continually by his placenta through the umbilical cord. But now that your baby’s a land creature, he has to demand to be fed. At first, sleeping times will seem random rather than predictable. But eating and sleeping patterns will gradually become more predictable and, between 8 and 12 weeks of age, when the baby’s stomach grows larger, feedings will start to become more frequent in the daytime and less so at night.
All babies should be placed on their backs for sleep. Recent research has shown that doing so can lessen the risk of your baby dying from sudden infant death syndrome (SIDS). You should also keep sheets and blankets away from his face, since these may become loose and could suffocate him. (For more information on SIDS, see in 1. Your Baby’s First Half-Year.)
Tip
If diaper rash bumps don’t go away in a week, or they turn bright red, weepy, or form a bright red ring around your baby’s anus, then it’s time to ask your baby’s health-care provider about treatment options. The rash may have turned into a yeast infection or be the result of the same strep infection that causes family members to have sore throats.
If you haven’t already figured it out, you need to learn to “let sleeping dogs lie,” that is: Don’t wake up your baby because you’re afraid he’s got a wet diaper, that he’s too cold, or because you think he needs to eat. Your baby will teach you in no uncertain terms, with a whimper or a scream, that he’s uncomfortable; otherwise, it’s best to just let well enough alone.
Tip
Your newborn will seldom remain awake for more than 2 hours at a time, and usually will sleep for periods of 4 to 5 hours throughout the day and night, waking up to feed. He will normally spend between 16 to 17 hours cycling in and out of sleep every 24 hours.
Basic sleep strategies
As you will very soon realize, no amount of wishing, hoping, or begging can make a baby go to sleep. Although there are plenty of products out there that claim to help babies sleep faster (teddy bears with heartbeats, crib vibrators, and so on), usually they aren’t very effective, at least not for very long.
What should I put in my diaper bag?
If you haven’t known many babies, you may be wondering what’s in a diaper bag besides diapers. The following is a list of items you may wish to pack when you leave the house with your baby. It’s a good idea to keep your diaper bag stocked and by your front door in case you need to leave the house in a hurry. Also, if you drive, it can be helpful to have a backup supply of essentials in your car.
• Diapers (2 or 3, minimum).
• Portable changing pad or a small towel (something to protect the baby’s bottom from surfaces and vice versa).
• Premoistened baby wipes. (Use travel-sized packages, or carry individual wipes in a plastic sandwich bag that seals shut.)
• Diaper rash cream or ointment, if your baby has a rash.
• Plastic bag to hold any dirty clothes until you get home.
• Change of clothes for your baby.
• Tissues, washcloth, or cloth diaper in case you encounter spit-up or a leaky diaper.
• If you’re bottle feeding, pure water for mixing formula.
• If you’re breastfeeding or weaning, spare nursing pads.
• Seasonal outerwear for your baby (hat in summer; jacket, blanket, or bunting in winter).
• Sunscreen for you and your baby, if you’re going to be outside.
• Pacifiers, if your baby uses them.
• Antibacterial hand gel for yourself.
• Be kind. Don’t try to make baby “cry it out” during the first six months. Your baby is just asking to have his basic needs met, and you’re the person to do the job.
• Be flexible. Be open to whatever works. You probably made a decision before your baby was born about where you planned to put him to sleep. But babies are different: Some sleep best in a crib; others in the family bed or a bedside bassinet. If your baby doesn’t seem to sleep well where he is, try a new location.
• Monitor comfort. Make sure your baby is dressed comfortably so he won’t wake up because he’s uncomfortably hot or cold or his sleeper is scratchy.
• Be consistent. Try a consistent, early bedtime, and naps during the day. There is such a thing as a baby getting too tired and having a hard time settling down.
• Establish routine. Make a routine (but stay flexible). Doing the same thing every night will help give baby the cue that it’s time to settle down. Try dimming the lights and turning off the television for a half hour before bedtime. Consider incorporating a warm bath or a massage. (For more information on baby massage, see in 1. Your Baby’s First Half-Year.) Make sure that your baby is well fed, then try any combination of rocking, singing, reading, or telling a story.
The co-sleeping debate
Whether newborns should be in a crib or in bed with their parents is a hotly debated topic, and a personal decision. For a long time, U.S. pediatricians have discouraged parents from sleeping with their babies, even though the vast majority of parents worldwide do so. Today, many parents opt to share the “family bed” as a way of nurturing emotional and physical closeness with their babies while getting more rest at the same time. But other parents prefer to have their own personal space in bed and feel they sleep less deeply and have less privacy when a baby is there with them.
In recent years, the U.S. Consumer Product Safety Commission (CPSC) has issued an advisory warning parents that co-sleeping can be dangerous for babies. The Commission points to a survey of baby deaths showing that 515 babies died from accidents linked to sleeping in adult beds between 1990 and 1997.
However, most of the deaths were linked not to the babies’ sleeping with their parents per se but to suffocation or strangulation when the babies became trapped between the mattress and another object, such as between gaps in the headboard or between the mattress and the bedside table; or suffocation occurred when a baby was placed facedown on a waterbed.
At least one group of studies appears to show that placing a baby close to a parent during sleep can help to entrain the baby’s sleep patterns, lowering the risk of SIDS.
WARNING! Cribs Can Kill
Although studies appear to prove that it is more risky for babies to sleep in their parents’ beds, they fail to acknowledge the hazards of the alternative: crib sleeping. While an average of 64 babies die each year in accidents associated with sleeping in adult beds, 50 babies also die each year in cribrelated accidents. Most crib deaths are caused by old, malfunctioning models that allow babies to get entrapped in widely spaced bars, have their necks compressed on the edges of poorly fitting mattresses, or who are strangled when their bodies slide through loose or missing bars, leaving their heads behind. Babies also get entangled in loose crib sheets, suffocate in puffy, decorative crib quilts, or hang themselves when their clothing or pacifier strings get captured on ledges that protrude from the tops of headboards when their parents aren’t nearby to protect them.
Keeping Baby Safe in Your Bed
If you do decide to bring your baby into your bed, a few simple precautions can help to make things safer:
Monitor soft and suffocating objects. Keep pillows, quilts, sheets, and blankets away from the baby’s face.
Back and side sleeping. Keep the baby on his back or on his side, attached to your breast, so that you’re aware of his breathing and motions. Avoid placing baby to sleep on his stomach, and don’t co-sleep on a waterbed.
Avoid bed frame and furniture hazards. Consider removing your bed’s mattress from the springs and frame, placing it on the floor, and wedging it tightly against one corner of the room to remove the dangers of the baby getting entrapped between hard furniture surfaces.
Keep aware. Don’t sleep with the baby if you’ve been drinking or taking any kind of sedating medication.
Be there. Don’t allow your baby to sleep on your bed unless you are with him.
How baby teeth erupt
In rare cases, a baby may already have a tooth or two at birth. But, typically, a baby’s teeth break through in a rather predictable fashion. First, you will notice a small, whitish bump under the baby’s gum that signals a tooth is about to erupt.
Tip
If your baby’s gums become red, hot, and swollen, or he has an ongoing fever of 101° F, or higher, then the issue may not just be teething, and it’s time to contact your baby’s doctor or dentist. If your baby is over six months of age, a mild painkiller, such as liquid acetaminophen (Infant’s Tylenol®) or ibuprofen may be recommended.
Baby teeth are called “primary” teeth. They’re usually whiter and smaller than lifelong teeth. Molars resemble little white flower buds and appear smoother with fewer ridges and dents than fully formed adult teeth.
At the same time as your baby’s primary teeth are erupting, permanent teeth are also forming underneath in the jaw. It will take several years before the larger permanent teeth—the wisdom teeth, canines, and other back teeth—begin to take shape. The roots for these teeth don’t grow and take hold until the teeth actually start to break through the gums.
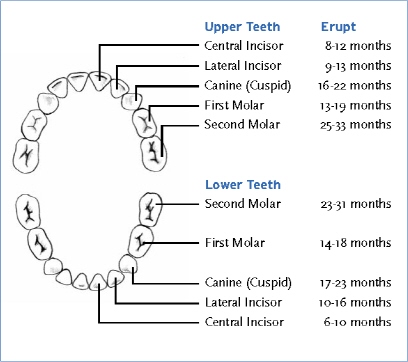
Front teeth on the lower jaw are usually the first primary teeth to emerge—at about six to ten months of age, but that’s not always the case. A first tooth may not show up for nearly a year for some babies.
Typical teething symptoms
Signs of teething discomfort:
• Changing feeding habits.
• Awakening more in the night.
• Getting a runny nose with clear mucus.
• Uncharacteristic loose stools.
• Red bumps on the gums.
After the first, lower teeth come in, next come the top front primary teeth—usually between eight and twelve months. Next, the teeth on either side of the front teeth emerge—first on the top (nine to thirteen months), followed by teeth on the bottom sides of the jaw (10 to 16 months).
The remaining teeth, including the canines and molars, erupt between 14 and 31 months in an orderly progression—starting from the front of the mouth, and moving toward the back, often alternating between top and bottom jaws.
The larger, stronger permanent teeth don’t start showing up until your child is getting ready for first grade. Again, different children have different schedules. (For a good chart that helps to predict tooth eruption, see: www.thekidsdds.com/chart.htm.)
Teething and pain
A baby’s first teeth usually emerge without a lot of fuss. But when the larger teeth, especially the molars, start erupting at about one year of age, your baby may show signs of discomfort.
Signs of teething: A baby will drool more than usual and want to gnaw on fingers, toys, or anything he can clamp his jaws onto. The teething process may take several weeks, and each time a tooth is coming in, your baby may seem uncomfortable, perhaps batting his ears as if to say, “This HURTS.”
If you’re breastfeeding, there will be that undeniable signal that something’s up in the jaw department when baby chomps down the first time with the sharp edge of a tiny tooth. Most moms know instinctively what to do about biting: Just temporarily remove the baby from the breast (don’t forget to break the suction first!) and say, “No!” Your baby may be shocked and whimper, but one or two removals should deliver the message.
Home remedies for teething troubles
• Your finger. Use the pad of your finger or a cold piece of damp gauze to gently massage the sore area. Do this only briefly.
• Washcloth. With careful supervision, let your baby gnaw on a dampened, frozen washcloth.
• Carrot. Let your baby gum the thick end of a cold carrot, but take it away immediately if he succeeds in breaking off any particles.
• Cold spoon. Give your baby a cold, smooth-edged spoon, such as a soup spoon, to hold in his lips.
• Teething tools. Try teething beads or a teething bracelet made either from tough, spongy material or filled with a liquid that can be safely refrigerated. Don’t freeze teethers that contain gels, since the cold can burn tender gums.
Baby dental care
Dental care for your baby’s teeth should begin even before your baby’s born! A baby’s teeth begin to form at about the sixth week of pregnancy, and permanent teeth at about the twelfth week—growth that will take about eight years to complete.
WARNING! Chewing Babies Choke
Your baby has a built-in drive to gnaw on things. Babies accidentally choke on pieces of pacifiers and small toy parts that they manage to chew off or halfway swallow. Any object that is small enough to slip through the hole in the center of a toilet roll is small enough for your baby to choke on.
Tip
Some children have allergic reactions to toothpastes. The symptoms are reddening inside the mouth or a red rash around the mouth that may also cover the chin.
Although it’s not true that the baby absorbs calcium from the mother’s teeth during pregnancy, your developing baby is dependent on your diet to provide the calcium, phosphorous, and other vitamins and minerals necessary for the formation of healthy teeth. Certain drugs you take during pregnancy may affect your baby’s teeth. For example, drugs in the tetracycline family can cause brown or gray discoloration of your baby’s tooth enamel.
Basic tooth cleaning
Most pediatric dental specialists recommend that parents gently wipe down a baby’s gums once or twice a day using fresh gauze or a clean baby washcloth. This is because the bacteria that cause tooth decay are present in a baby’s mouth even before the first teeth emerge.
Experts suggest wiping the gums after feeding and before bed—but most parents prefer to do it when the baby’s fully awake rather than risk arousing a nap-ready baby.
Start regular teeth cleaning when the first tooth erupts.
Toothpastes containing fluoride and abrasive cleaners aren’t recommended for children under two. Toddlers aren’t ready to brush their own teeth until they are three or four years old.
Choosing the right dentist
Your baby’s first visit to the dentist should be either before his first birthday or before his first tooth emerges, whichever comes first (preferably not at eight months, when babies usually have strong stranger anxiety!).
There are two types of dentists who can care for your child’s oral health: general dentists; or pediatric dentists, called pedodontists, who specialize in treating children. (Check the Web site of the American Academy of Pediatric Dentistry, www.aapd.org, for help with finding the pediatric dentist nearest you.)
A pedodontist brings extra training to the job, along with an understanding of child psychology. Most have offices that appeal to kids, and there is a strong effort from both these dentists and their staffs to ensure your child has a positive experience the first time around. This could prove helpful later if your child is fearful of strangers or novel experiences, or if your child turns out to need extensive dental work.
During your baby’s first exam, the dentist will examine your baby’s oral cavity and answer any questions you may have about future dental care. He may suggest fluoride treatments, and will show you how to clean your baby’s gums and emerging teeth.
Small concessions from a dentist can mean a lot, such as allowing your tot to sit in your lap during an exam instead of insisting that your child be “independent,” which can be frightening. Taking time to explain everything at a child’s level of understanding is important, too, and so is working with you if you are hesitant about having X-rays or other procedures carried out on your child when there’s no serious problem being presented.
Tooth decay
Primary teeth, or baby teeth, are vulnerable to decay. Typically, decay can progress from a small dot on the outer enamel covering of a tooth and grow into the deeper layers, sometimes in less than six months.
Whether a decay spot needs treatment is up to your child’s dentist. If it’s shallow and your child will be losing the tooth soon, it may be left alone. But if there’s a danger that the tooth will disintegrate or become painful, then the cavity may need to be filled. Healthy baby teeth hold the place for emerging permanent teeth, and cavities can migrate to permanent teeth from baby teeth.
There are basically three bacteria related to dental decay: Streptococcus mutans, Lactobacillus species, and Actinomyces species. These bacteria play a part in forming plaque, the soft, clear, white, or sometimes yellow buildup on the teeth that is removed through brushing, flossing, or wiping.
Tartar is the hardened form of plaque and is usually white, yellow, or brown. Once tartar has formed, it cannot be brushed away. It must be scraped off by a dentist or hygenist.
Tooth decay isn’t a direct result of the bacteria, plaque, and tartar that are present in all mouths. It comes from a complex interaction of factors: the level of bacteria, a child’s diet, cleaning habits, saliva characteristics, genetics, and whether the child’s teeth are protected by fluoride. But, researchers predict that someday children will be immunized against tooth decay.
Protecting your baby’s teeth
There is some thought that the dental decay process can be transmitted from one person to another. And some specialists recommend that parents try to avoid saliva-to-saliva contact with their babies by not sharing spoons, chewing food for the baby, or putting a baby’s pacifier in their mouths.
Once your child is in daycare or nursery school, you’ll learn to be careful about saliva transfer for your own sake! Being “sanitary” will help protect you from catching all the colds and infections that children pass between one another like wildfire.
Once your child’s permanent teeth erupt, a protective sealant can be applied to your child’s teeth, especially in the nooks and crannies on the tops of molars, to prevent cavities from forming.
Tip
Primary teeth help to keep the place in the jaw so permanent teeth underneath have the space they need when they emerge. If one of your baby’s primary teeth gets knocked out, it may change the way his permanent teeth erupt, and other teeth may tip or move over into the vacant space. Don’t wash the tooth if it’s knocked out, but wrap it in a moist piece of gauze or tissue and contact your baby’s dentist about what to do. He or she will tell you whether the tooth should be saved and may recommend that your child be fitted with a space maintainer to ensure that adequate room is held open for the permanent tooth.
Here are some tips to help you protect your baby’s teeth:
• Nix sweets. Sugar, corn syrup, and other sweeteners in your baby’s diet can promote early tooth decay. Don’t give your baby bottles filled with sweetened drinks, teas, sodas, or flavored mineral water to use like a pacifier.
• Wipe off starches. Starches from cookies, cereals, and crackers can promote tooth decay if particles remain on the teeth. Wipe down your baby’s teeth after snacks.
• No bottle in the crib. Don’t put your baby to bed with a bottle of formula or breastmilk. (Put water into the bottle instead.)
• No snoozing while nursing. Avoid prolonged bottle or breastfeeding at night when your baby sleeps and then awakens with a bottle or your nipple in his mouth. That allows milk acids to pool around his teeth.
• No sugar or honey on the “passy.” Don’t dip your baby’s pacifier in sugar or honey to make it more appealing. Apart from causing tooth decay, honey presents a botulism poisoning danger for babies under a year of age.
• Shift your baby to a cup. After your baby’s first birthday, teach him how to suck liquid through a straw or drink from a sippy cup rather than using a bottle.
FLASH FACT: Juice, Candy, and Cavities
A 2001 study published in Dentistry and Oral Epidemiology found that toddlers who drank lots of juice or who ate candy more than once a week were nearly twice as likely as their peers to have a mouth full of cavities by kindergarten. The tooth-brushing habits for the candy eaters and juice drinkers were no different between those who had cavities and those who were cavity-free. Even though teaching your toddler how to brush his teeth is an important skill to learn, tots are not very good at doing it. Keeping sugary drinks and candies away from your child is more important for making sure his teeth stay healthy.
Fluoride issues
There is continuing controversy in the dental world over whether babies and children need fluoride to protect their teeth from decay. It’s commonly considered vital for protecting healthy teeth, but there are still some questions about the dangers and side effects of the chemical.
Too much fluoride intake in children can cause fluorosis, the discoloration of teeth. Although many cities add fluoride to drinking water, such excessive amounts usually do not result from municipal water treatment but are more common in regions where fluoride appears naturally in the water.
If you use well or bottled water that contains less than 0.3ppm (parts per million) of fluoride, you may want to discuss giving your baby under six months of age prescription fluoride drops. But exercise caution when following dosage directions. Teach your children not to swallow fluoridated toothpaste or mouthwash.
Crying is the thread of connection that draws a parent to a baby to care for him. It’s a powerful signal designed by nature to bring parents running. Crying can be fearsome for babies, and may feel to the baby like the sound is coming from somewhere outside of himself. In fact, cries of other babies can cause babies to break out crying without even knowing why. Your baby won’t have any tears when he cries until he reaches about a year of age.
Crying, although it may start mildly, intensifies in depth as the baby becomes more involved and his emotions build. In the midst of a crying jag, a baby’s oxygen level plummets rapidly. He turns blue around the lips. His voice strains to the limits of its capacity. Like a frightened, running horse, the more your baby cries, the more fear builds, until the only answer is to shut down, exhausted.
Research has shown that when parents respond immediately to a baby’s cries, rather than making him cry a long time before getting a response, their babies rapidly learn other ways to express their needs and feelings. On the other hand, babies who must cry long and hard for attention become frozen in only one communication mode: crying.
Soothing swaddling
It appears that this new, strange, gravity-heavy world, where legs and arms may be left to flail helplessly, can be upsetting to a baby who has only known the confines of his tiny bedroom inside his mom. Swaddling is an age-old practice of wrapping up a baby into a tight little bundle to make him feel secure, as though he were back in his familiar, tight quarters again. It’s as though having something to press against feels a lot more secure than the prospect of endless space. Besides being a great soother, swaddling your baby transforms him into a neat little bundle that is easier for other children to hold, and which will also allow you to shampoo his hair.
For swaddling, choose a generoussized, baby-soft, absorbent blanket that is square in shape. Choose an all-cotton, lightweight fabric rather than something that will be cumbersome or hot.