5
Right-Brain Affect Regulation
An Essential Mechanism of Development, Trauma, Dissociation, and Psychotherapy
Allan N. Schore
THERE IS CURRENTLY AN increasing awareness, indeed a palpable sense, that a number of clinical disciplines are undergoing a significant transformation, a paradigm shift. A powerful engine for the increased energy and growth in the mental health field is our ongoing dialogue with neighboring disciplines, especially developmental science, biology, and neuroscience. This mutually enriching interdisciplinary communication is centered on a common interest in the primacy of affect in the human condition. Psychological studies on the critical role of emotional contact between humans are now being integrated with biological studies on the impact of these relational interactions on brain systems that regulate emotional bodily based survival functions.
By definition, a paradigm shift occurs simultaneously across a number of different fields, and it induces an increased dialogue between the clinical and applied sciences. This transdisciplinary shift is articulated by Richard Ryan in a recent editorial of the journal Motivation and Emotion:
After three decades of the dominance of cognitive approaches, motivational and emotional processes have roared back into the limelight…. More practically, cognitive interventions that do not address motivation and emotion are increasingly proving to be short-lived in their efficacy, and limited in the problems to which they can be applied. (2007, p. 1)
Echoing this perspective, the neuroscientist Jaak Panksepp now boldly asserts:
The cognitive revolution, like radical neuro-behaviorism, intentionally sought to put emotions out of sight and out of mind. Now cognitive science must re-learn that ancient emotional systems have a power that is quite independent of neocortical cognitive processes…. These emotional substrates promote cognitive–object relations, optimally through rich emotional experiences. (2008c, p. 51)
And in the psychotherapy literature Karen Maroda sets forth this challenge:
From my experience there are more therapists who have painfully sat on their emotions, erroneously believing that they were doing the right thing. For these therapists, the prospect of using their emotional responses constructively for the patient is a potentially rewarding and mutually healthy experience…perhaps we can explore the therapeutic nature of affect, freeing both our patients and ourselves. (2005, p. 140)
In contrast to the prevailing privileged status of verbal, conscious cognition, I have suggested that emotional communications between therapist and patient lie at the psychobiological core of the therapeutic alliance, and that right-brain to right-brain emotional processes are essential to development, psychopathology, and psychotherapy (Schore, 1994). Indeed, recent clinical research reports that the more therapists facilitate the affective experience/expression of patients in psychotherapy, the more patients exhibit positive changes; furthermore, therapist affect facilitation is a powerful predictor of treatment success (Diener et al., 2007).
In this chapter, after a brief introduction, I discuss the interpersonal neurobiology of the essential right-brain process of nonconscious affect regulation in development, in psychopathogenesis and trauma dissociation, and finally in the change process of psychotherapy.
Regulation Theory and the Primacy of Affective Structures and Functions
A central theme running throughout all my work is the exploration of the primacy of affective processes in various critical aspects of the human experience. Lane stresses the evolutionary functions of both implicit and explicit affects:
Primary emotional responses have been preserved through phylogenesis because they are adaptive. They provide an immediate assessment of the extent to which goals or needs are being met in interaction with the environment, and they reset the organism behaviorally, physiologically, cognitively, and experientially to adjust to these changing circumstances. (2008, p. 225)
The right brain implicit self represents the biological substrate of the human unconscious mind and is intimately involved in the processing of bodily based affective information associated with various motivational states (Schore, 1994, 2003a, 2003b). The survival functions of the right hemisphere, the locus of the emotional brain, are dominant in relational contexts at all stages of the lifespan, including the intimate context of psychotherapy.
Lichtenberg observes a central focus of the psychotherapeutic encounter:
To appreciate the patient’s motivation, we need to…discern the emotional experience he or she seeks. At times, the goal sought will be self-evident to patient and [therapist]. At other times, the goal will lie out of awareness and will be difficult to ascertain…. The golden thread in assessing motivation lies in discovering the affect being sought in conjunction with the behavior being investigated. (2001, p. 440, emphasis added)
Relevant to the renewed interest in emotion in models of the change process in both development and psychotherapy, there is now a growing body of evidence which indicating that “in most people, the verbal, conscious and serial information processing takes place in the left hemisphere, while the unconscious, nonverbal and emotional information processing mainly takes place in the right hemisphere” (Larsen et al., 2003, p. 534). The right hemisphere is dominant for the recognition of emotions, the expression of spontaneous and intense emotions, and the nonverbal communication of emotions (see Schore, 2003a, 2003b for references). The central role of this hemisphere in survival functions is outlined by Schutz:
The right hemisphere operates a distributed network for rapid responding to danger and other urgent problems. It preferentially processes environmental challenge, stress and pain and manages self-protective responses such as avoidance and escape…. Emotionality is thus the right brain’s “red phone,” compelling the mind to handle urgent matters without delay. (2005, p. 15)
Furthermore, an important ongoing trend in interdisciplinary studies is a focus on not just emotion but unconscious, implicit emotion. At the beginning of the last century Freud speculated, “Unconscious ideas continue to exist after repression as actual structures in the system Ucs, whereas all that corresponds in that system to unconscious affects is a potential beginning which is prevented from developing” (1915/1957, p. 178). In my own work on unconscious affect, I have suggested that bodily based affects are the center of empathic communication, and that the regulation of conscious and unconscious feelings is placed in the center of the clinical stage (Schore, 1994, emphasis added). Maroda (2005) challenges therapists to ponder an essential clinical problem: “How do you relate empathically to an unexpressed emotion?” (p. 136). I argue here that unconscious affects can best be understood not as repressed but as dissociated affects. Later-forming repression is associated with left-hemispheric inhibition of affects generated by the right brain, whereas early-forming dissociation reflects a dysregulation of affects resulting from the dis-integration of the right brain itself.
Although this topic has been controversial, neuroscience now demonstrates a right hemispheric dominance in processing of unconscious negative emotion (Sato & Aoki, 2006). Other studies document a cortical response to subjectively unconscious danger (Carretie, 2005). For example, basic research on the neurobiology of survival mechanisms clearly shows that the emotion of fear “is not necessarily conscious; a fearful response may be evoked even when one is not fully aware of being ‘afraid.’…As with emotion itself, the enhanced memory for emotional experiences may proceed at a relatively subconscious level, without clear awareness” (Price, 2005, p. 135).
Neurobiological studies also demonstrate that the right cortical hemisphere is centrally involved in “the processing of self-images, at least when self-images are not consciously perceived” (Theoret et al., 2004, p. 57). Deep psychotherapeutic changes alter not only conscious but unconscious self-image associated with nonconscious internal working models of attachment. Both unconscious negative emotions and unconscious self-images are important elements of the psychotherapy process, especially with the more severe self pathologies.
Thus, the essential roles of the right brain in the unconscious processing of emotional stimuli and in emotional communication are directly relevant to recent clinical models of an affective unconscious and a relational unconscious, whereby one unconscious mind communicates with another unconscious mind (Schore, 2003a). In a number of writings I have described in some detail the fundamental role of right-brain to right-brain communications across an intersubjective field embedded within the therapeutic alliance (Schore, 1994, 2002a, 2005b, 2007). This dialogue of ultrarapid bodily based affective communications in patient–therapist (and infant–mother) attachment transactions occurs beneath levels of conscious awareness in both members of the dyad.
Another area of common intense interdisciplinary interest is the self-regulation of emotion. Affect regulation is usually defined as the set of control processes by which we influence, consciously and voluntarily, our emotions, and how we experience and behaviorally express them. However, “Most of moment to moment psychological life occurs through nonconscious means…. Various nonconscious mental systems perform the lion’s share of the self-regulating burden, beneficently keeping the individual grounded in his or her environment” (Bargh & Chartrand, 1999, p. 462). Greenberg now asserts, “The field has yet to pay adequate attention to implicit and relational processes of regulation” (2008, p. 414). Applying this principle to psychotherapy, Ryan notes, “Both researchers and practitioners have come to appreciate the limits of exclusively cognitive approaches for understanding the initiation and regulation of human behavior” (2007, p. 1).
Indeed, a large body of data suggests that unconscious affect regulation is more essential than conscious emotion regulation in human survival functions (Schore, 1994, 2003a, 2003b, 2007). There is agreement among both scientists and clinicians that this essential adaptive capacity evolves in early attachment experiences:
The developmental achievement of a sense of self that is simultaneously fluid and robust depends on how well the capacity for affect regulation and affective competency has been achieved…. When these early patterns of interpersonal interaction are relatively successful, they create a stable foundation for relational affect regulation that is internalized as nonverbal and unconscious. Thus, further successful negotiation of interpersonal transactions at increasingly higher levels of self-development and interpersonal maturity is made possible. (Bromberg, 2006, p. 32)
Right-Brain Processes in Development: The Interpersonal Neurobiology of Secure Attachment
As summarized in a recent contribution on modern attachment theory (Schore & Schore, 2008), the essential task of the first year of human life is the creation of a secure attachment bond between the infant and his or her primary caregiver. Secure attachment depends upon the mother’s sensitive psychobiological attunement to the infant’s dynamically shifting internal states of arousal. Through visual–facial, auditory–prosodic, and tactile–gestural communication, caregiver and infant learn the rhythmic structure of the other and modify their behavior to fit that structure, thereby cocreating a specifically fitted interaction. Developmental researchers now describe this nonverbal intersubjective communication in a way that is congruent with the models of nonconscious communication discussed above.
Preverbal communication…is the realm of non-consciously regulated intuitive behavior and implicit relational knowledge. Whether information is transferred or shared, which information gets across, and on which level it is “understood,” does not necessarily depend on the sender’s intention or conscious awareness. (Papoušek, 2007, p. 258)
During these bodily based affective communications the attuned mother synchronizes the spatiotemporal patterning of her exogenous sensory stimulation with the infant’s spontaneous expressions of his or her endogenous organismic rhythms. Via this contingent responsivity, the mother appraises the nonverbal expressions of the infant’s internal arousal and affective states, regulates them, and communicates them back to the infant. To accomplish this regulation, the mother must successfully modulate nonoptimal high or nonoptimal low levels of stimulation that would induce supraheightened or extremely low levels of arousal in the infant.
In play episodes of affective synchrony, the pair experience a condition of resonance, and in such, an amplification of vitality affects and a positive state occurs. In moments of interactive repair, the “good-enough” caregiver who has misattuned can regulate the infant’s negative state by accurately reattuning in a timely manner. The regulatory processes of affective synchrony that create states of positive arousal and of interactive repair that modulates negative arousal are the fundamental building blocks of attachment and its associated emotions. Resilience in the face of stress and novelty is an ultimate indicator of attachment security (Schore, 2005a).
These adaptive capacities are central to the dual processes of self-regulation: interactive regulation—the ability to flexibly regulate psychobiological states of emotions with other humans in interconnected contexts; and autoregulation—which occurs apart from other humans in autonomous contexts. According to Pipp and Harmon, “It may be that…we are biologically connected to those with whom we have close relationships…. Homeostatic regulation between members of a dyad is a stable aspect of all intimate relationships throughout the lifespan” (1987, p. 651). The evolutionary mechanism of attachment—the interactive regulation of emotion—thus represents the regulation of biological synchronicity between and within organisms (Bradshaw & Schore, 2007).
In line with earlier proposals that emotional attachment experiences during early critical periods of development facilitate the experience-dependent maturation of emotion regulatory brain circuits (Schore, 1994), neuroscientists now assert:
The mother functions as a regulator of the socio-emotional environment during early stages of postnatal development…. subtle emotional regulatory interactions, which obviously can transiently or permanently alter brain activity levels…may play a critical role during the establishment and maintenance of limbic system circuits. (Ziabreva et al., 2003, p. 5,334)
It is well established that the human central nervous system (CNS) limbic system extensively myelinates in the first year and a half and that the early-maturing right hemisphere—which is deeply connected into the limbic system—undergoes a growth spurt at this time (Gupta et al., 2005; Howard & Reggia, 2007; Moskal et al., 2006; Schore, 2003a; Sun et al., 2005).
The right hemisphere also has tight connections with the involuntary autonomic nervous system (ANS) that controls visceral organs, effectors in the skin, and the cardiovascular system, and is responsible for the generation of vitality affects. Via a right lateralized vagal circuit of emotion regulation, “the right hemisphere—including the right cortical and subcortical structures—would promote the efficient regulation of autonomic function via the source nuclei of the brain stem” (Porges, Doussard-Roosevelt, & Maiti, 1994, p. 175). Affect-regulating attachment experiences specifically impact cortical and limbic–autonomic circuits of the developing right cerebral hemisphere (Cozolino, 2002; Henry, 1993; Schore, 1994, 2005a; Siegel, 1999). For the rest of the lifespan, internal working models of the attachment relationship with the primary caregiver, stored in the right brain, encode strategies of affect regulation that nonconsciously guide the individual through interpersonal contexts.
Earlier speculations (Schore, 1994) are now supported by current studies which observe that right lateralized limbic areas responsible for the regulation of autonomic functions and higher cognitive processes are involved in the “formation of social bonds” and are “part of the circuitry supporting human social networks,” and that the “the strong and consistent predominance for the right hemisphere emerges postnatally” (Allman et al., 2005, p. 367). In very recent work on mother–infant emotional communication Lenzi et al. (in press) offer data from a functional magnetic resonance imaging (MRI) study “supporting the theory that the right hemisphere is more involved than the left hemisphere in emotional processing and thus, mothering.” Also confirming this model Minagawa-Kawai et al. (2009, p. 289) report a near-infrared spectroscopy study of infant–mother attachment at 12 months and conclude, “our results are in agreement with that of Schore (2000) who addressed the importance of the right hemisphere in the attachment system.” Summarizing this data, Rotenberg asserts:
The main functions of the right hemisphere…the ability to grasp the reality as a whole; the emotional attachment to the mother (Schore, 2003a); the regulation of withdrawal behavior in the appropriate conditions (Davidson et al., 1990); the integration of affect, behavior and autonomic activity (Schore, 2003a) are the basic functions of survival (Saugstad, 1998) and for this reason are the first to appear. (2004, p. 864)
The Interpersonal Neurobiology of Attachment Trauma
During the brain growth spurt (last trimester of pregnancy through second year), relational trauma-induced arousal dysregulation precludes the forementioned visual–facial, auditory–prosodic, and tactile–gestural attachment communications and alters the development of essential right brain functions. In contrast to an optimal attachment scenario, in a relational growth-inhibiting early environment, the primary caregiver induces traumatic states of enduring negative affect in the child. This caregiver is inaccessible and reacts to the infant’s expressions of emotions and stress inappropriately and/or rejectingly, and therefore shows minimal or unpredictable participation in the various types of arousal-regulating processes. Instead of modulating stimulation, the caregiver induces extreme levels of arousal, very high in abuse and/or very low in neglect. And because the caregiver provides no interactive repair, the infant’s intense negative affective states last for long periods of time. These deficits in maternal function outwardly reflect the mother’s own internal stressful states of dysregulated arousal.
Psychophysiological studies of human maternal behavior directed toward infants clearly indicate that
stress is an important factor that may affect social interactions, especially the mother–child interaction. Mothers during stressful life episodes were less sensitive, more irritable, critical and punitive…. Moreover, stressed mothers showed less warmth and flexibility in interactions with their children…. Overall, stress seems to be a factor that has the power to disrupt parenting practices seriously and results in a lower quality of the mother–child interaction. (Suter et al., 2007, p. 46)
These authors demonstrate that stress impacts the female’s autonomic nervous system and specifically disrupts her right hemisphere.
On the other side of the mother–infant dyad, interdisciplinary evidence indicates that the infant’s psychobiological reaction to traumatic stress is comprised of two separate response patterns: hyperarousal and dissociation. In the initial hyperarousal stage, the maternal haven of safety suddenly becomes a source of threat, triggering an alarm or startle reaction in the infant’s right hemisphere, the locus of both the attachment system and the fear motivational system. This maternal stressor activates the infant’s hypothalamic–pituitary–adrenal (HPA) stress axis, thereby eliciting a sudden increase of the energy-expending sympathetic component of the infant’s ANS, resulting in significantly elevated heart rate, blood pressure, and respiration—the somatic expressions of a dysregulated hypermetabolic psychobiological state of fear/terror.
A second, later-forming reaction to relational trauma is dissociation, in which the child disengages from stimuli in the external world—traumatized infants are observed to be staring off into space with a glazed look. This parasympathetic dominant state of conservation/withdrawal occurs in helpless and hopeless stressful situations in which the individual becomes inhibited and strives to avoid attention in order to become “unseen” (Schore, 1994, 2001). The dissociative metabolic shutdown state is a primary regulatory process, used throughout the lifespan, in which the stressed individual passively disengages in order to conserve energies, foster survival by the risky posture of feigning death, and allow restitution of depleted resources by immobility. In this passive hypometabolic state heart rate, blood pressure, and respiration are decreased, whereas pain-numbing and blunting endogenous opiates are elevated. It is this energy-conserving parasympathetic (vagal) mechanism that mediates the profound detachment of dissociation.
In fact, there are two parasympathetic vagal systems in the brainstem medulla. The ventral vagal complex rapidly regulates cardiac output to foster fluid engagement and disengagement with the social environment, and it exhibits rapid and transitory patterns associated with perceptive pain and unpleasantness—all aspects of a secure attachment bond of emotional communication. On the other hand, activity of the dorsal vagal complex is associated with intense emotional states and immobilization, and is responsible for the severe hypoarousal and pain blunting of dissociation (see Figure 5.1). The traumatized infant’s sudden state switch from sympathetic hyperarousal into parasympathetic dissociation is described by Porges as “the sudden and rapid transition from an unsuccessful strategy of struggling requiring massive sympathetic activation to the metabolically conservative immobilized state mimicking death associated with the dorsal vagal complex” (1997, p. 75).
FIGURE 5.1
Dynamic patterns of regulated and dysregulated autonomic arousal (J. Wheatley-Crosbie, based on Porges, 1997).
Porges (1997) describes the involuntary and often prolonged characteristic pattern of vagal outflow from the dorsal vagal nucleus. This long-lasting state of dorsal vagal parasympathetic activation accounts for the extensive duration of “void” states associated with pathological dissociative detachment (Allen, Console, & Lewis, 1999), and for what Bromberg (2006) calls dissociative “gaps” in subjective reality—“spaces” that surround self states and thereby disrupt coherence among highly affectively charged states. These gaps are also discussed in the developmental psychoanalytic literature. Winnicott (1958) notes that a particular failure of the maternal holding environment causes a discontinuity in the baby’s need for “going-on-being,” and Kestenberg (1985) refers to as “dead spots” in the infant’s subjective experience, an operational definition of the restriction of consciousness of dissociation. At all points of the lifespan, dissociation is conceptualized as “a basic part of the psychobiology of the human trauma response: a protective activation of altered states of consciousness in reaction to overwhelming psychological trauma” (Loewenstein, 1996, p. 312).
Dissociation in infants has been studied with the still-face procedure, an experimental paradigm of traumatic neglect. In the still face, the infant is exposed to a severe relational stressor: The mother maintains eye contact with the infant, but she suddenly totally inhibits all vocalization and suspends all emotionally-expressive facial expressions and gestures. This intense relational stressor triggers an initial increase of interactive behavior and arousal in the infant. According to Tronick (2004), the infant’s confusion and fearfulness at the break in connection is accompanied by the subjective response, “this is threatening.” This stress response is then followed by bodily collapse, loss of postural control, withdrawal, gaze aversion, sad facial expression, and self-comforting behavior.
Most interestingly, this behavior is accompanied by a dissipation of the infant’s state of consciousness and a diminishment of self-organizing abilities that reflect disorganization of many of the lower level psychobiological states, such as metabolic systems. Tronick (2004) suggests that infants who have a history of chronic breaks of connections exhibit an “extremely pathological state” of emotional apathy. He equates this state with Spitz’s cases of hospital-ism, Harlow’s isolated monkeys, Bowlby’s withdrawn children, and Romanian orphans who fail to grow and develop. Such infants ultimately adopt a communication style of “stay away, don’t connect.” This defensive stance is a very-early-forming, yet already chronic, pathological dissociation that is associated with loss of ventral vagal activation and dominance of dorsal vagal parasympathetic states.
In parallel to still-face studies, ongoing attachment research underscores a link between frightening maternal behavior, dissociation, and disorganized infant attachment (Schuengel, Bakersmans-Kranenburg, & van IJzendoorn, 1999). Hesse and Main (1999) point out that the disorganization and disorientation of type “D” attachment associated with abuse and neglect pheno-typically resembles dissociative states. In recent work, Hesse and Main observe that when the mother enters a dissociative state, a fear alarm state is triggered in the infant. The caregiver’s entrance into the dissociative state is expressed as “parent suddenly completely ‘freezes’ with eyes unmoving, half-lidded, despite nearby movement; parent addresses infant in an ‘altered’ tone with simultaneous voicing and devoicing” (2006, p. 320). In describing the mother as she submits to the freeze state, they note:
Here the parent appears to have become completely unresponsive to, or even aware of, the external surround, including the physical and verbal behavior of their infant…. We observed one mother who remained seated in an immobilized and uncomfortable position with her hand in the air, blankly staring into space for 50 sec. (p. 321)
In an electroencephalograph (EEG) study of 5-month-old infants looking at a “blank face,” Bazhenova, Stroganova, Doussard-Roosevelt et al. (2007) report increases in vagal activity “over the right posterior temporal scalp area and over anterior scalp areas…. This observation suggests greater right hemisphere involvement in face processing during blank face” (p. 73).
During these episodes of the intergenerational transmission of attachment trauma the infant is matching the rhythmic structures of the mother’s dysregulated arousal states. This synchronization is registered in the firing patterns of the stress-sensitive corticolimbic regions of the right brain, dominant for survival and the human stress response (Schore, 1994; Wittling, 1995). Adamec, Blundell, and Burton (2003) report findings that “implicate neuroplasticity in right hemispheric limbic circuitry in mediating long-lasting changes in negative affect following brief but severe stress” (p. 1,264). Gadea et al. conclude that an intense experience “might interfere with right hemisphere processing, with eventual damage if some critical point is reached” (2005, p. 136). Recall that right cortical areas and their connections with right subcortical structures are in a critical period of growth during the early stages of human development. The massive ongoing psychobiological stress associated with dysregulated attachment trauma sets the stage for the characterological use of right-brain unconscious pathological dissociation over all subsequent periods of human development.
Right-Brain Processes in Psychopathogenesis: The Neurobiology of Pathological Dissociation
In the neuropsychoanalytic literature Watt contends: “If children grow up with dominant experiences of separation, distress, fear and rage, then they will go down a bad pathogenic developmental pathway, and it’s not just a bad psychological pathway but a bad neurological pathway” (2003, p. 109). Neurobiological research on patients with a history of relational trauma also demonstrates continuity over the course of the lifespan in the expression of this primitive autoregulation defense. It is commonly accepted that early childhood abuse specifically alters limbic system maturation, producing neurobiological alterations that act as a biological substrate for a variety of psychiatric consequences, including affective instability, inefficient stress tolerance, memory impairment, psychosomatic disorders, and dissociative disturbances (Schore, 2001, 2002b).
In a transcranial magnetic stimulation study of adults Spitzer et al. report: “In dissociation-prone individuals, a trauma that is perceived and processed by the right hemisphere will lead to a ‘disruption in the usually integrated functions of consciousness’” (2004, p. 168). And in fMRI research Lanius et al. (2005) show predominantly right-hemispheric activation in posttraumatic stress disorder (PTSD) patients while they are dissociating.
These and other studies are presently exploring the evolution of a developmentally impaired regulatory system over all stages of life. They provide evidence that orbitofrontal (ventromedial) cortical and limbic areas (anterior cingulate, insula, periacqueductal gray, amygdala) of particularly the right hemisphere are centrally involved in the deficits in mind and body associated with a pathological dissociative response (Schore, 2003a, 2003b, in press). This hemisphere, more so than the left, is densely interconnected reciprocally with emotion-processing limbic regions, as well as with subcortical areas that generate both the arousal and autonomic (sympathetic and parasympathetic) bodily based aspect of emotions (see Figure 5.2). Sympathetic nervous system activity is manifest in tight engagement with the external environment and high levels of energy mobilization and utilization, whereas the parasympathetic component drives disengagement from the external environment and utilizes low levels of internal energy (Recordati, 2003). These components of the ANS are uncoupled in traumatic states of pathological dissociation.
In line with the current shift from “cold cognition” to the primacy of bodily based “hot affects,” clinical research on dissociation is focusing on “somatoform dissociation,” an outcome of early-onset traumatization, expressed as a lack of integration of sensorimotor experiences, reactions, and functions of the individual and his or her self-representation (Nijenhuis, 2000). Thus, “dissociatively detached individuals are not only detached from the environment, but also from the self—their body, their own actions, and their sense of identity” (Allen et al., 1999, p. 165). This observation describes impaired functions of the right hemisphere, the locus of the “emotional” or “corporeal self.” Crucian et al. describes “a dissociation between the emotional evaluation of an event and the physiological reaction to that event, with the process being dependent on intact right hemisphere function” (2000, p. 643).
I have offered interdisciplinary evidence indicating that the implicit self, the human unconscious mind, is located in the right brain (Schore, 1994, 2003b, 2005b). The lower subcortical levels of the right brain (the deep unconscious) contain all the major motivational systems (including attachment, fear, sexuality, aggression, disgust, etc.) and generate the somatic autonomic expressions and arousal intensities of all emotional states. When optimally functioning, higher orbito-frontal limbic levels of the right hemisphere generate a conscious emotional state that expresses the affective output of these motivational systems (Schore, 1994). This right lateralized hierarchical prefrontal system performs an essential adaptive motivational function: the relatively fluid switching of internal bodily based states in response to changes in the external environment that are nonconsciously appraised to be personally meaningful (Schore, 1994).
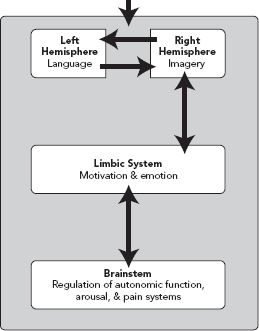
FIGURE 5.2
Vertical axis of right-brain cortical–subcortical limbic–autonomic circuits and subsequent connections into the left brain. Adapted from Kirmayer (2004).
On the other hand, pathological dissociation, an enduring outcome of early relational trauma, is manifest in a maladaptive, highly defensive, rigid and closed system, one that responds to even low levels of intersubjective stress with parasympathetic dorsal vagal hypoarousal and heart rate deceleration. This fragile unconscious system is susceptible to mind–body metabolic collapse and thereby a loss of energy-dependent synaptic connectivity within the right brain, expressed in a sudden implosion of the implicit self and a rupture of self-continuity. This dis-integration of the right brain and collapse of the implicit self is signaled by the amplification of the parasympathetic affects of shame and disgust, and by the cognitions of hopelessness and helplessness. Because the right hemisphere mediates the communication and regulation of emotional states, the rupture of intersubjectivity is accompanied by an instant dissipation of safety and trust.
Dissociation thus reflects the inability of the vertical axis of the right brain cortical–subcortical implicit self system (see right side of Figure 5.2) to recognize and process external stimuli (exteroceptive information coming from the relational environment) and on a moment-to-moment basis integrate them with internal stimuli (interoceptive information from the body, somatic markers, the “felt experience”). This failure of integration of the higher right hemisphere with the lower right brain induces an instant collapse of both subjectivity and intersubjectivity. Stressful and painful emotional states associated with intensely high or low levels of arousal are not experienced in consciousness, but remain in implicit memory as dysregulated dissociated unconscious affects (Schore, in press).
This developmental model of relational trauma describes the psychoneurobiological mechanisms that underlie Janet’s conceptualization of dissociation. As described by van der Kolk et al.:
Janet proposed that when people experience “vehement emotions,” their minds may become incapable of matching their frightening experiences with existing cognitive schemes. As a result the memories of the experience cannot be integrated into personal awareness; instead, they are split off [dissociated] from consciousness and voluntary control…. extreme emotional arousal results in failure to integrate traumatic memories…. The memory traces of the trauma linger as unconscious “fixed ideas” that cannot be “liquidated.”…They continue to intrude as terrifying perceptions, obsessional preoccupations, and somatic reexperiences. (1996, p. 52, emphasis added)
There is now agreement that “traumatic stress in childhood could lead to self-modulation of painful affect by directing attention away from internal emotional states” (Lane et al., 1997, p. 840). Given that the right hemisphere is dominant not only for regulating affects but also for attention (Raz, 2004), negative affect (Davidson & Cacioppo, 1992), and pain processing (Symonds et al., 2006), the right-brain strategy of dissociation represents the ultimate defense for blocking conscious awareness of emotional pain. If early trauma is experienced as “psychic catastrophe,” the autoregulatory strategy of dissociation is expressed as “detachment from an unbearable situation,” “a submission and resignation to the inevitability of overwhelming, even psychically deadening danger,” and “a last resort defensive strategy” (Schore, in press).
Right Brain Processes in Psychotherapy: Unconscious Affect, Transference, and Primary Process
At the beginning of this chapter I suggested that the regulation of not only conscious but also unconscious affects is an essential mechanism of the psychotherapeutic change process. All forms of therapy currently view affect dysregulation as a fundamental condition of every psychiatric disorder (Taylor et al., 1997), including personality disorders (Sarkar & Adshead, 2006), and therefore share a common goal of improving the effectiveness of emotional self-regulatory processes (Beauregard, Levesque, & Bourgouin, 2001). In terms of regulation theory defense mechanisms are forms of emotional regulation strategies for avoiding, minimizing, or converting affects that are too difficult to tolerate. Treatment, especially of early-forming severe psychopathologies, must attend not only to conscious dysregulated affects but also to the early-forming survival defense that protects patients from consciously experiencing overwhelming painful negative affects—dissociation. This bottom-line defense thus represents the major counterforce to the emotional–motivational aspects of the change process in psychotherapy (Schore, 2007). This clinical principle is supported by research demonstrating that insecurely attached dissociative patients dissociate as a response to negative emotions arising in psychodynamic psychotherapy, leading to a less favorable treatment outcome (Spitzer et al., 2007).
Basic research suggests that “while the left hemisphere mediates most linguistic behaviors, the right hemisphere is important for broader aspects of communication” (van Lancker & Cummings, 1999, p. 95). Incorporating these data into the regulation theory model of the psychotherapeutic process, I have delineated the central role of implicit right-brain to right-brain nonverbal communications (facial expression, prosody, gesture) in unconscious transference–countertransference affective transactions—an essential treatment element of severe psychopathologies and a common mechanism of all forms of psychotherapy. Interdisciplinary data and updated clinical models lead me to conclude that the right hemisphere is dominant in treatment, and that psychotherapy is not the “talking cure” but the affect communicating and regulating cure (Schore, 2005b).
Clinical workers now describe transference as “an established pattern of relating and emotional responding that is cued by something in the present, but oftentimes calls up both an affective state and thoughts that may have more to do with past experience than present ones” (Maroda, 2005, p. 134). In a parallel formulation, neuroscience now documents that the right hemisphere is fundamentally involved in the unconscious processing of emotional stimuli (Mlot, 1998), and that
the right hemisphere holds representations of the emotional states associated with events experienced by the individual. When that individual encounters a familiar scenario, representations of past emotional experiences are retrieved by the right hemisphere and are incorporated into the reasoning process. (Shuren & Grafman, 2002, p. 918)
Furthermore, “the right hemisphere operates in a more free-associative, primary process manner, typically observed in states such as dreaming or reverie” (Grabner, Fink, & Neubauer, 2007, p. 228). In line with current developmental and relational models I have argued that right-brain to right-brain communications represent interactions of the patient’s unconscious primary-process system and the therapist’s primary-process system (Schore, 1994), and that primary process cognition is the major communicative mechanism of the relational unconscious.
Enactments, Autonomic Arousal Dysregulation, and Dissociation
Primary process right-brain to right-brain nonverbal communications especially predominate in the stressful transference-countertransference contexts of clinical enactments. In a major contribution integrating clinical models and neurobiological data, Ginot (2007, p. 317) convincingly argues: “Increasingly, enactments are understood as powerful manifestations of the intersubjective process and as inevitable expressions of complex, though largely unconscious self-states and relational patterns” (emphasis added).
In line with earlier neuropsychoanalytic speculations (Schore, 1997) and in support of the central thesis of this chapter, Ginot observes:
This focus on enactments as communicators of affective building blocks also reflects a growing realization that explicit content, verbal interpretations, and the mere act of uncovering memories are insufficient venues for curative shifts…. As intense manifestations of transference–countertransference entanglements, enactments seem to generate interpersonal as well as internal processes eventually capable of promoting integration and growth. (2007, p. 317–318)
She concludes that these “unconscious affective interactions” “bring to life and consequently alter implicit memories and attachment styles” (p. 318). Recall the hypothesis of Stern et al. (1998) that “implicit relational knowledge” stored in a nonverbal domain is at the core of therapeutic change.
In previous neuropsychoanalytic work, I offered interdisciplinary evidence deomonstrating that the right hemisphere is the locus of implicit memory (Schore, 1999). In discussing the right hemisphere as “the seat of implicit memory,” Mancia notes: “The discovery of the implicit memory has extended the concept of the unconscious and supports the hypothesis that this is where the emotional and affective—sometimes traumatic—presymbolic and preverbal experiences of the primary mother–infant relations are stored” (2006, p. 83). Implicit memories of dysregulating ultra-high arousal experiences are stored and expressed in sympathetic dominant rapid extreme increases of autonomic arousal associated with heart rate acceleration. Conversely, implicit memories of dysregulating ultra-low arousal experiences are stored and expressed in dorsal vagal parasympathetic dominant rapid extreme decreases of arousal associated with rapid heart rate deceleration. The principle of the state-dependent recall of implicit memories thus applies to each of these two domains: Achieving a particular bodily state is necessary to access certain affects, behaviors, and cognitions.
It is often overlooked that affects reflect an individual’s internal state and have an hedonic (valenced) dimension and an arousal (intensity-energetic) dimension (Schore, 1994). A body of studies now demonstrates that the right hemisphere is generally more important than the left in activating arousal systems (Heilman, 1997; Meadows & Kaplan, 1994), yet more capable of operating at reduced arousal levels (Casagrande et al., 2007). The right brain is superior in processing emotional arousal and in the automatic response to emotional stimuli (Gainotti et al., 1993), and it is dominantly affected by feedback of bodily stress-induced arousal (Critchley et al., 2004). As opposed to left-brain “anxious apprehension,” expressed in cognitive anxiety, worry, verbal rumination, and muscle tension, right-brain “anxious arousal” is associated with panic states and somatic symptoms, including shortness of breath, pounding heart, dizziness, sweating, and feelings of choking. In this latter state the right side of the brain continuously monitors the external environment for threat and “exerts hierarchical control over the autonomic and somatic functions for responding to threat” (Nitschke et al., 1999, p. 635).
In states of right-hemispheric hyperarousal that generate a massive density of intense sympathetic-dominant, energy-expending, high-arousal negative affect, arousal levels are so extremely elevated that they interfere with the individual’s capacity to adaptively engage with the social (object relational, intersubjective) environment. Bromberg (2006) links trauma, at any point in the lifespan, to autonomic hyperarousal, “a chaotic and terrifying flooding of affect that can threaten to overwhelm sanity and imperil psychological survival” (p. 33).
In contrast, states of right-hemispheric parasympathetic-dominant, energy-conserving hypoarousal generate a massive density of intense low-arousal negative affect. In these latter affective states arousal levels are so extremely reduced that they interfere with the individual’s capacity to adaptively disengage from the social environment. Thus, early relational trauma, reactivated in transference–countertransference enactments, manifests in dysregulated autonomic hyperarousal associated with sympathetic-dominant affects (panic/terror, rage, and pain), as well as dysregulated autonomic hypoarousal and parasympathetic-dominant affects (shame, disgust, and hopeless despair).
In terms of Porges’s (1997) polyvagal model (see Figure 5.3), the sympathetic hyperarousal zone processes states of danger (fight/flight), whereas the dorsal vagal hypoarousal system is dominant in states of life survival/threat (see Schore, in press). Recall that the early development of these two stress-responsive psychobiological domains is directly impacted by dysregulated (abuse and neglect) attachment experiences. These imprinted right-brain implicit memories of the hyperarousal and dissociative-hypoarousal responses to early relational trauma are reactivated in the transference–countertransference.
Clinical work in these dyadic enactments implies a profound commitment by both therapeutic participants and a deep emotional involvement on the therapist’s part (Tutte, 2004). In these highly stressful contexts the therapist’s affect tolerance is a critical factor in determining the range, types, and intensities of emotions that are explored or disavowed in the transference–countertransference relationship and the therapeutic alliance (Schore, 2003b).
A general principle of this work is that the sensitive empathic therapist allows the patient to reexperience dysregulating affects in affectively tolerable doses in the context of a safe environment, so that overwhelming traumatic feelings can be regulated and integrated into the patient’s emotional life. In agreement with Ogden et al. (2005), Bromberg (2006) also points out that the therapeutic relationship must “feel safe but not perfectly safe. If it were even possible for the relationship to be perfectly safe, which it is not, there would be no potential for safe surprises” (p. 95). This affect-focused work occurs of at the edges of the regulatory boundaries of affect tolerance (Ogden, Chapter 8, this volume), or what Lyons-Ruth describes as the “fault lines” of self-experience where “interactive negotiations have failed, goals remain aborted, negative affects are unresolved, and conflict is experienced” (2005, p. 21).
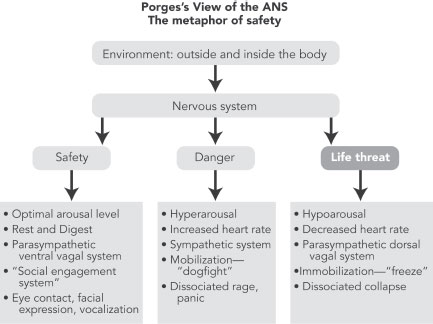
FIGURE 5.3
Porges’s polyvagal model of the autonomic nervous system. Adapted from Porges (2006).
The usual concept of “window of tolerance” used by Ogden, and Siegel, describes the range of optimal arousal to sustain secondary-process cognition (conscious, verbal, explicit) and striatal motor activities (voluntary action; controlled overt behavior). These cognitive and behavioral functions are dependent upon a moderate rather than high or low arousal range, represented by a classical inverted U. This window of optimal verbal processing and overt behavioral expression reflects moderate arousal levels that sustain left-hemispheric functions. Current cognitive–behavioral and insight-driven clinical models operate in this arousal range and focus on these left–hemispheric functions.
On the other hand, the right brain has a different range of arousal tolerance to sustain its unique nonconscious psychobiological functions and can operate at very high or very low arousal levels. Right-brain “windows of affect tolerance” thus refers to an optimal range of arousal for different affects and motivational states, which vary in arousal intensity. This affect tolerance is severely restricted in the emotional deadening defense of pathological dissociation. An expansion of both negative and positive affect tolerance is a goal of the affectively focused psychotherapy described in this chapter.
In such work, at some point the threatening dissociated affect must be activated, but in trace form, and regulated sufficiently so as not to trigger new avoidance. “The questions of how much and when to activate or to permit this activation, so as to repair the dissociation rather than reinforce it, must be addressed specifically for each patient” (Bucci, 2002, p. 787). According to Bromberg, “Clinically, the phenomenon of dissociation as a defense against self-destabilization…has its greatest relevance during enactments, a mode of clinical engagement that requires a [therapist’s] closest attunement to the unacknowledged affective shifts in his own and the patient’s self-states” (2006, p. 5). This self-destabilization of the emotional right brain in clinical enactments can take one of two forms: high-arousal explosive fragmentation versus low-arousal implosion of the implicit self.
Coconstruction of Intersubjective Fields
Visualize two planes of one window of affect tolerance in parallel to another: One represents the patient’s window of affect tolerance, the other the therapist’s. At the edges of the windows, the regulatory boundaries, the psychobiologically attuned empathic therapist, on a moment-to-moment basis, implicitly tracks and matches the patterns of rhythmic crescendos/decrescendos of the patient’s regulated and dysregulated ANS with his or her own ANS crescendos/decrescendos. When the patterns of synchronized rhythms are in interpersonal resonance, this right-brain to right-brain specifically fitted interaction generates amplified energetic processes of arousal, and this interactive affect regulation, in turn, cocreates an intersubjective field.
The dynamic intersubjective field is described by Stern (2004) as “the domain of feelings, thoughts, and knowledge that two (or more) people share about the nature of their current relationship…. This field can be reshaped. It can be entered or exited, enlarged or diminished, made clearer or less clear” (p. 243, emphasis added). In my work on the interpersonal neurobiology of intersubjectivity, I have asserted that the right hemisphere is dominant for subjective emotional experiences, and that the interactive transfer of affect between the right brains of the members of therapeutic dyad is therefore best described as intersubjectivity (Schore, 1999). An intersubjective field is more than just an interaction of two minds, but also of two bodies, which, when in affective resonance, elicit an amplification and integration of both CNS and ANS arousal (see Chapter 3 of Schore 2003b on the communication of affects in an intersubjective field via projective identification).
At present there is an intense interest in how the body can be incorporated into psychotherapeutic treatment. The solution to this problem is to integrate into clinical models information about the ANS, “the physiological bottom of the mind” (Jackson, 1931). This system generates vitality affects and controls the cardiovascular system, effectors on the skin, and visceral organs. Stress-induced alterations in these dynamic psychobiological parameters mediate the therapist’s somatic countertransference to the patient’s nonverbal communications within a coconstructed intersubjective field. In previous writings on the psychophysiology of countertransference, I stated:
Countertransferential processes are currently understood to be manifest in the capacity to recognize and utilize the sensory (visual, auditory, tactile, kinesthetic, and olfactory) and affective qualities of imagery which the patient generates in the psychotherapist (Suler, 1989). Similarly, Loewald (1986) points out that countertransference dynamics are appraised by the therapist’s observations of his own visceral reactions to the patient’s material. (Schore, 1994, p. 451)
Recall that the ANS contains dissociable sympathetic energy-expending and parasympathetic energy-conserving components. Extending this intraorganismic concept to the interpersonal domain, two dissociable intersubjective fields can be cocreated: (1) a sympathetic-dominant high-energy intersubjective field that processes state-dependent implicit memories of object relational and attachment transactions in high arousal states (see Table 5.1); and (2) a parasympathetic-dominant low-energy intersubjective field that processes state-dependent implicit memories of object relational and attachment transactions in low arousal states (see Table 5.2).
Note the contrast of somatic transference–countertransferences in the dual intersubjective fields. Also, the form of primary-process expressions in affect, cognition, and behavior differ in altered ultra-high-and low-arousal states of consciousness. Thus the high and low arousal states associated with, respectively, terror and shame will show qualitatively distinct patterns of primary-process nonverbal communication of “body movements (kinesics), posture, gesture, facial expression, voice inflection, and the sequence, rhythm, and pitch of the spoken words” (Dorpat, 2001, p. 451). Recall that sympathetic nervous system activity is manifest in tight engagement with the external environment and high levels of energy mobilization and utilization, whereas the parasympathetic component drives disengagement from the external environment and utilizes low levels of internal energy. This principle applies not only to overt interpersonal behavior but also to covert intersubjective engagement–disengagement with the social environment, the coupling and decoupling of minds–bodies and internal worlds. Models of the ANS indicate that although reciprocal activation usually occurs between the sympathetic and parasympathetic systems, these two systems are also able to uncouple and act unilaterally (Schore, 1994). Thus the sympathetic hyperarousal and parasympathetic hypoarousal zones represent two discrete intersubjective fields of psychobiological attunement, rupture, and interactive repair of what Bromberg (2006) terms “collisions of subjectivities.”
It should be noted that just as emotion researchers have overemphasized sympathetic-dominant affects and motivations (fear, flight/fight), so have psychotherapists overly focused on the reduction of anxiety/fear or aggression/rage states. One outstanding example of this continuing bias is the devaluation of the critical role of dysregulated parasympathetic shame and disgust states in all clinical models. Similarly, psychodynamic models have highlighted the roles of rage and fear/terror in high-arousal enactments, and subsequent explosive fragmentation of the high-energy intersubjective field and the implicit self. As a result there has been an underemphasis on the low-energy parasympathetic-dominant intersubjective field. This is problematic, because clinical work with parasympathetic dissociation—that is, detachment from an unbearable situation (Mollon, 1996)—is always associated with parasympathetic shame dynamics.
TABLE 5.1 High-Energy Charge Intersubjective Field
Hyperarousal = hypermetabolic CNS–ANS limbic–autonomic circuits = stressful, sympathetic-dominant, energy-expending psychobiological states
- High-energy explosive dyadic enactments; fragmenting of implicit self
- Sympathetic-dominant intersubjectivity; overengagement with social environment
- Somatic countertransference to communicated high-arousal affects expressed in heart rate acceleration; focus on exteroceptive sensory information
- Regulation/dysregulation of hyperaroused affective states (aggression/rage, panic/terror, sexual arousal, excitement/joy)
TABLE 5.2 Low Energy Charge Intersubjective Field
Hypoarousal = hypometabolic CNS–ANS circuits = stressful, parasympathetic-dominant, energy-conserving psychobiological states
- Low-energy implosive dyadic enactments; collapsing implicit self
- Parasympathetic-dominant intersubjectivity; dissociation/disengagement from social environment
- Somatic countertransference to communicated low-arousal affects expressed in heart rate deceleration; focus on interoceptive information
- Regulation/dysregulation of hyporaroused affective states (shame, disgust, abandonment, hopeless despair)
In my very first work, I proposed that the parasympathetic low-arousal state of shame, subjectively experienced as a “spiraling downward,” represents a sudden shift from sympathetic hyperarousal into parasympathetic dorsal vagal hypoarousal (Schore, 1991). Recall that the collapse of the implicit self is subtle, signaled by amplification of the parasympathetic affects of shame and disgust, and by the cognitions of hopelessness and helplessness—common accompaniments of traumatic experiences. Working deep in the low-arousal intersubjective field, Bromberg (2006) observes that shame is present in those patients who “disappear” when what is being discussed touches upon unprocessed early trauma, and that shame is the most powerful affect a person is unable to modulate. He concludes:
The task that is most important, and simultaneously most difficult for the [therapist], is to watch for signs of dissociated shame both in himself and in his patient—shame that is being evoked by the therapeutic process itself in ways that the [therapist] would just as soon not have to face…. The reason that seemingly repeated enactments are struggled with over and over again in the therapy is that the [therapist] is over and over pulled into the same enactment to the degree he is not attending to the arousal of shame. (p. 80)
Perhaps the most pointed observation is made by Nathanson:
The entire system of psychotherapy, as we had been taught it, worked only if we overlooked the shame that we produced day in and day out in our therapeutic work…. It became clear that post-Freudian society had been treated for almost everything but shame, and that the degree and severity of undiagnosed and untreated shame problems far exceeded anything we had ever imagined. (1996, p. 3)
Clinicians and researchers need to pay more attention to the energy-conserving parasympathetic-dominant intersubjective field of psychobiological attunement, rupture, and repair.
Interactive Affect Regulation as a Central Mechanism
of the Change Process
Various authors have described the subtle psychological activities of the sensitive clinician who scaffolds the cocreation of an intersubjective field with the patient. Bromberg observes:
When [a therapist] gives up his attempts to “understand” his patient and allows himself to know his patient through the ongoing intersubjective field they are sharing at that moment, an act of recognition (not understanding) takes place in which words and thoughts come to symbolize experience instead of substitute for it. (2006, p. 11)
The dyadic nature of this deep affective exploration of the self was noted by Jung’s (1946) suggestion that the clinician must go to the limit of his subjective possibilities, otherwise the patient will be unable to follow suit. According to Lichtenberg (2001), staying with the patient’s immediate communication longer and more intensely usually gains more understanding than is achieved either by a defense focus or a genetic focus on what isn’t said. And Whitehead describes the affect-amplifying effects encountered in the deep strata of the unconscious:
Every time we make therapeutic contact with our patients we are engaging profound processes that tap into essential life forces in our selves and in those we work with…. Emotions are deepened in intensity and sustained in time when they are intersubjectively shared. This occurs at moments of deep contact. (2005, p. 624, emphasis added)
As previously discussed, a central tenet of regulation theory dictates that the interpersonal resonance within an intersubjective field triggers an amplification of state. The resultant cocreated increased arousal (metabolic energy) allows for hypoaroused dissociated unconscious affects to be intensified and thereby experienced in consciousness as a subjective emotional state. This bottom-up interactive regulation enables the affect beneath conscious awareness to be intensified and sensed in both. Thus the “potential beginning” of an unconscious affect (Freud, 1915/1957) is intersubjectively energized into emergence. According to Fosha (2003), the initiating mechanism of the change process is the alteration of “defense-dominated functioning” and “the state transformation leading to the visceral experience of core affective phenomena within an emotionally engaged therapeutic dyad” (p. 519).
As in all attachment dynamics, the dyadic amplification of arousal–affect intensity that is generated in a resonant transference–countertransference context facilitates the intensification of the felt sense in both therapist and patient. This same interpersonal psychobiological mechanism sustains the affect in time; that is, the affect is “held” within the intersubjective field long enough for it to reach conscious awareness in both members of a psychobiologically attuned therapeutic dyad. It should be noted that this affect charging-amplifying process includes an intensification of both negative and positive affects in an intersubjective field.
But more than empathic affect attunement and deep contact are necessary for further therapeutic progression. At the psychobiological core of the intersubjective field is the attachment bond of emotional communication and affect regulation. The clinician’s psychobiological interactive regulation–repair of dysregulated, especially unconscious (dissociated), bodily based affective states is an essential therapeutic mechanism. Recall Bucci’s (2002) proscription that the threatening dissociated affect must be sufficiently regulated. Sands notes that “Dissociative defenses serve to regulate relatedness to others…. The dissociative patient is attempting to stay enough in a relationship with the human environment to survive the present while, at the same time, keeping the needs for more intimate relatedness sequestered but alive” (1994, p. 149).
Due to early learning experiences of severe attachment failures, the patient accesses pathological dissociation in order to cope with potential dysregulation of affect by anticipating trauma before it arrives. In characterological dissociation, an autoregulatory strategy of involuntary autonomic disengagement is initiated and maintained to prevent potentially dysregulating intersubjective contact with others. But as the patient continues through the change process, he or she becomes more able to forgo autoregulation for interactive regulation when under interpersonal stress. Fosha (2005, p. 527) stresses this important principle: “Dyadic affect regulation is a process that is central, not only in infancy, but from the cradle to the grave, a fortiori when we are faced with (categorical) emotions of such intensity that they overwhelm us, in the moment seeming beyond the capacity of our available resources to handle (i.e., that being the definition of trauma).” Similarly, Ogden and her colleagues conclude:
Interactive psychobiological regulation (Schore, 1994) provides the relational context under which the client can safely contact, describe, and eventually regulate inner experience…. Rather than insight alone, it is the patient’s experience of empowering action in the context of safety provided by a background of the empathic clinician’s psychobiologically attuned interactive affect regulation that helps effect…. change. (2005, p. 22)
This interactive affect regulation occurs at the edge of the regulatory boundaries of both high and low arousal in the intersubjective fields. In such work, Bromberg warns, “An interpretative stance…not only is thereby useless during an enactment, but also escalates the enactment and rigidifies the dissociation” (2006, p. 8), and Maroda offers the caveat, “Interpretations given when affect is needed amounts to anti-communication, resulting in the patient getting worse” (2005, p. 138). A therapeutic focus on regulating not only conscious but unconscious (dissociated) affect highlights the conclusion that implicit nonverbal affective factors, more than the explicit verbal cognitive (insight) ones, lie at the core of the change process in the treatment of more severely disturbed patients. At the most fundamental level, the intersubjective work of psychotherapy is not defined by what the clinician does for the patient or says to the patient (left-brain focus). Rather, the key mechanism is how to be with the patient, especially during affectively stressful moments when the patient’s implicit core self is dis-integrating in real time (right-brain focus).
Note the similarity of working at the right-brain regulatory boundaries in the heightened affective moment of enactments to Lichtenberg’s “disciplined spontaneous engagements” that occur within “an ambience of safety”:
Spontaneous refers to the [therapist’s] often unexpected comments, gestures, facial expressions, and actions that occur as a result of an unsuppressed emotional upsurge. These communications seem more to pop out than to have been planned or edited. The [therapist] may be as surprised as the patient. By engagement, we refer to communications and disclosures that are more enactments than thought-out responses. (2001, p. 445)
Tronick’s “moments of meeting,” a novel form of engagement of the therapeutic dyad, also occur at the regulatory boundaries:
The [therapist] must respond with something that is experienced as specific to the relationship with the patient and that is expressive of her own experience and personhood, and carries her signature…. It is dealing with “what is happening here and now between us.” The strongest emphasis is on the now because of the affective immediacy…. It requires spontaneous responses…[which] need never be verbally explicated, but can be, after the fact. (2007, p. 436)
According to Greenberg and Paivio (1997), reexperiencing the traumatic experience in therapy, with the safety and security provided by an empathic, supportive therapist, gives the person a new experience: specifically, the clinician’s interactive regulation of the patient’s communicated dysregulated right-brain hyperaroused and hypoaroused affective states. In support of this model current experimental researchers report: “As suggested in clinical practice, it is necessary to ‘revisit’ an emotionally distressing memory before it can be controlled” (Depue, Curran, & Banich, 2007, p. 218).
This dyadic psychobiological mechanism of the psychotherapeutic change process is described by Adler:
Because people in a caring, i.e., empathic relationship convey emotional experiences to each other, they also convey physiological experiences to each other, and this sociophysiologic linkage is relevant to the understanding the direct physiologic consequences of caring in the doctor–patient relationship—for both parties. (2002, p. 885, emphasis added)
He further argues that the therapeutic relationship—the interaction between the patient’s emotional vulnerability and the therapist’s emotional availability—represents a prime example of how individuals in an empathic relationship coregulate each other’s autonomic activity. More specifically, the therapeutic relationship can act as “the antithesis of the fight-flight response” and “the experience of feeling cared about in a relationship reduces the secretion of stress hormones and shifts the neuroendocrine system toward homeostasis” (Adler, 2002, p. 883). Adler argues that in this way social bonds of attachment embedded in the therapeutic relationship reduce stress-induced arousal.
Ongoing episodes involving therapeutic interactive regulation of affective arousal impact the patient’s activation threshold of a right-brain stress response to a social stressor. Bromberg observes that the processing becomes “safer and safer so that the person’s tolerance for potential flooding of affect goes up” (2006, p. 79). As a result:
The patient’s threshold for triggering increases, allowing her increasingly to hold on to the ongoing relational experience (the full complexity of the here and now with the therapist) as it is happening, with less and less need to dissociate; as the processing of the here and now becomes more and more immediate, it becomes more and more experientially connectable to her past. (p. 69)
Effective work at the regulatory boundaries of right-brain low and high arousal states ultimately broadens the windows of affect tolerance, thereby al lowing for a wider variety of more intense and enduring affects in future intersubjective contexts. LeDoux offers an elegant description of this advance of emotional development:
Because emotion systems coordinate learning, the broader the range of emotions that [an individual] experiences the broader will be the emotional range of the self that develops…. And because more brain systems are typically active during emotional than during nonemotional states, and the intensity of arousal is greater, the opportunity for coordinated learning across brain systems is greater during emotional states. By coordinating parallel plasticity throughout the brain, emotional states promote the development and unification of the self. (2002, p. 322)
Growth-facilitating experiences cocreated at the regulatory boundaries thus promote the “affective building blocks” of enactments (Ginot, 2007, p. 317). The patient’s increased ability to consciously experience and communicate a wider range of positive and negative affects is due to a developmental advance in the capacity to regulate affect. This further maturation of adaptive self-regulation is, in turn, reflected in the appearance of more complex emotions that result from the simultaneous blending of different affects, and in an expansion in the “affect array” (Schore, 1994).
Psychotherapy of attachment pathologies and severe personality disorders must focus on unconscious affect and the survival defense of pathological dissociation, “a structured separation of mental processes (e.g., thoughts, emotions, conation, memory, and identity) that are ordinarily integrated” (Spiegel & Cardeña, 1991, p. 367). Overwhelming traumatic feelings that are not regulated cannot be adaptively integrated into the patient’s emotional life. This dissociative deficit specifically results from a lack of integration of the right hemisphere, the emotional brain. But effective therapy can positively alter the developmental trajectory of the deep right brain and facilitate the integration between cortical and subcortical right-brain systems. This enhanced interconnectivity allows for an increased complexity of defenses of the emotional right brain—coping strategies for regulating stressful affect that are more flexible and adaptive than pathological dissociation. These improved coping strategies in turn enhance the further maturation of the right hemisphere core of the self and its central involvement in “patterns of affect regulation that integrate a sense of self across state transitions, thereby allowing for a continuity of inner experience” (Schore, 1994, p. 33).
Concordant with this model of the change mechanism of psychotherapy, Fosha (2005) describes a “state in which affective and cognitive processes are seamlessly integrated, the core state that follows the experience of core affect is optimally suited for the therapeutic integration and consolidation that translate deep in-session changes into lasting therapeutic results” (p. 523). In this state of transformation “our view opens up: the entirety of the emotional landscape is visible, and it is evenly illuminated” (p. 523), and adaptive resources, resilience, and mindful understanding are available to the individual. Fosha speculates that this “wide angle lens” is “a capacity centrally mediated by the prefrontal cortex and the orbitofrontal cortex, the ultimate neuro-integrators of the meaning of personal experience (Schore, 2003a; Siegel, 2003),” and it generates “a cohesive and coherent autobiographical narrative” (p. 523). The latter is “primarily mediated by the right hemisphere’ prefrontal cortex” (p. 523).
The increased resilience of unconscious strategies of stress regulation that results from an optimal psychotherapeutic experience represents an experience-dependent maturation of “the right hemispheric specialization in regulating stress-and emotion-related processes” (Sullivan & Dufresne, 2006, p. 55). Studies now indicate that the right hemisphere, which is dominant for autobiographical memory (Markowitsch et al., 2000), provides access to a triggering mechanism that initiates autonomic sympathetic and parasympathetic reactions to socioemotional signals (Spence et al., 1996). The regulation of emotional stress is essentially mediated by higher right cortical regulation of lower arousal systems, autonomic structures, and peripheral organs. Indeed, anterior areas of the right hemisphere are involved in the control of autonomic activation (Aftanas et al., 2005), and right orbitofrontal (ventromedial) cortical activity acts to regulate the sympathetic nervous system (Critchley et al., 2000; Hilz et al., 2006).
In a neuroanatomical description that echoes Fosha’s description of the “wide angle lens” of the orbitofrontal core state, current studies conclude, “the rich connections of orbitofrontal cortex endow it with a panoramic view of the entire external environment, as well as the internal environment associated with motivational factors” (Barbas, 2007, p. 239). According to Barbas, frontal medial and orbitofrontal cortices, which are associated with appreciation of emotions, project to hypothalamic autonomic centers, which innervate brainstem and spinal autonomic autonomic structures. The latter, in turn, innervate peripheral organs whose activity is markedly increased in emotional arousal (Barbas et al., 2003). It is now established that “the peripheral physiological arousal and action tendencies associated with emotion are implicit in the sense that they occur automatically and do not require conscious processing to be executed efficiently” (Lane, 2008, p. 217, emphasis added). Note that the left-brain explicit verbal system that analytically processes interpretations is never directly involved in regulating sympathetic nervous system activity. Both secure attachment experiences and effective psychotherapy increase the complexity of the right-brain affect-regulating system.
The right hemisphere continues its growth spurts over the stages of the lifespan, thereby allowing for therapy-induced plasticity in the system. The structural changes that occur from effective psychotherapy occur in descending right cortical top-down pathways from orbitofrontal and ventral medial prefrontal cortices to the amygdala and hypothalamus, thereby providing a more effective mechanism of prefrontal control of the autonomic nervous system, and thus in processes underlying the recognition and expression of emotions. The psychotherapy of patients with attachment pathologies, who all too frequently experience traumatic fearful states of arousal, directly impacts and potentially alters right-lateralized dysregulations of the fear/terror system, driven by the subcortical right amygdala, which specializes in fear conditioning (Baker & Kim, 2004) and “unseen fear” (Morris et al., 1999). Importantly, prefrontal areas that inhibit emotional memories and suppress emotional reactivity are lateralized predominantly to the right hemisphere (Depue et al., 2007). The observations of Phelps et al. (2004) directly relate to the learning process of the psychotherapy context:
Understanding how fears are acquired is an important step in our ability to translate basic research to the treatment of fear-related behaviors. Understanding how learned fears are diminished may be even more valuable…. The amygdala may play an important role in extinction learning as well as acquisition and that ventromedial prefrontal cortex my be particularly involved in the retention of extinction learning. (p. 903)
Efficient functions of the right-brain implicit self are essential for the reception, expression, and communication of socioaffective information; the unconscious regulation of physiological, endocrinological, neuroendocrine, cardiovascular, and immune functions; subjectivity/intersubjectivity; trust and empathy; and an affective theory of mind. Hartikainen et al. summarize the critical role of nonconscious emotion processing for human survival:
In unpredictable environments, emotions provide rapid modulation of behavior. From an evolutionary perspective, emotions provide a modulatory control system that facilitates survival and reproduction. Reflex-like reactions to emotional events can occur before attention is paid to them…. Neuropsychological evidence supports a right hemispheric bias for emotional and attentional processing in humans. (2007, p. 1,929).
At the outset of this chapter I asserted that the emerging paradigm shift is highlighting the primacy of affect in human development, psychopathogenesis, and treatment. A large body of research in the neuroscience literature suggests a special role for the emotion-processing right hemisphere in empathy, identification with others, intersubjective processes, autobiographical memories, own body perception, self-awareness, self-related cognition, as well as self-images that are not consciously perceived—all essential components of the therapeutic process (see Schore & Schore, 2008, for references).
A fundamental theme of this work is that bodily based right-brain affect, including specifically unconscious affect, needs to be addressed in updated psychotherapeutic interventions. Even more than the patient’s late-acting rational, analytical, and verbal left mind, the growth-facilitating psychotherapeutic relationship needs to directly access the regulatory boundaries and deeper psychobiological strata of both the patient’s and the clinician’s right-brain minds. Alvarez (2006) asserts, “Schore points out that at the more severe levels of psychopathology, it is not a question of making the unconscious conscious: rather it is a question of restructuring the unconscious itself” (p. 171).
Earlier I suggested that the right hemisphere is dominant in the change process of psychotherapy. Neuroscience authors now conclude that although the left hemisphere is specialized for coping with predictable representations and strategies, the right predominates not only for organizing the human stress response (Wittling, 1995), but also for coping with and assimilating novel situations (Podell et al., 2001) and ensuring the formation of a new program of interaction with a new environment (Ezhov & Krivoschekov, 2004). Indeed,
the right brain possesses special capabilities for processing novel stimuli…. Right-brain problem solving generates a matrix of alternative solutions, as contrasted with the left brain’s single solution of best fit. This answer matrix remains active while alternative solutions are explored, a method suitable for the open-ended possibilities inherent in a novel situation. (Schutz, 2005, p. 13)
Recall that resilience in the face of stress and novelty is an indicator of attachment security. Therapeutic changes in the patient’s internal working model, encoding strategies of affect regulation, reflect structural alterations within the right brain.
The functions of the emotional right brain are essential to the self-exploration process of psychotherapy, especially of unconscious affects that can be integrated into a more complex implicit sense of self. Both optimal development and effective psychotherapy promote more than cognitive changes of the conscious mind, but an expansion of the right-brain implicit self, the biological substrate of the human unconscious.