Electro-Acupuncture
Science, Theories, Current Research, and Their Clinical Applications
The subject of this chapter has been in practice since the 1930s and 1940s in China. We know traditional acupuncture has a history of approximately 3000–5000 years. It is just incredible to see how it has evolved with the advancements of science, into what we know now as “Electro-Acupuncture” (EA). Electro-Acupuncture was initially developed to replace manual stimulation and allow doctors to treat more patients. From that, EA has been modified with different frequencies, different wave forms, separate polarities, different currents, all having special effects on the nervous system. This research has led to today’s design of evidenced-based protocols that target pathology directly. I use the term “Electro-Neuropuncture” for all of these applications brought together. That is, utilizing EA’s scientific research and applying the neuroanatomy of acupuncture, and clinical experience, to create protocols with reproducible clinical outcomes. I would like to feel that the well-known Chinese medicine doctor Hua Tuo himself would be very proud.
In this chapter I am going to share with you the science of EA, how and when to best utilize it, and groundbreaking research that I am personally involved in that I feel will help change our profession and the world. I personally use EA on nearly every patient. I use it as an excellent way of focusing a healing electrical signal on the patient’s nervous system in a way that communicates with that patient’s nervous system. I see EA as physical therapy (PT) for the CNS, a treatment that balances, heals, and rehabilitates the damaged nervous tissue.
First the science: I have found that EA is either misunderstood or is simply not being utilized properly by acupuncture practitioners today. There are many common questions that I am repeatedly asked by veteran practitioners and students alike. Some that I always get asked are: What is the difference between millicurrent and microcurrent? Which frequency should I use for a specific condition? Which lead goes where—red and black? What are the contraindications? So, before I get into specifics, let’s look at some basic physics to do with electricity. The main parameters that you should understand and differentiate between are the electric current, amperes, frequency, hertz, and voltage.
Current
An electric current is the flow, or rate, of the electric charge. This is the result of the effect of moving electrons. Voltage is the energy that the flow generates. In EA this movement is found inside the wires attached to the needles. This electric charge also generates an electromagnetic field locally, which has its own direct effect on humans. The international system of units measures current with amperes. So, when you see current and amperes, they are interchangeable. We acupuncturists tend to use the terms “microcurrent” or “microamps,” and “millicurrent” or “milliamps.” These are the two currents that I use in my clinical practice and that I will be discussing throughout the book.
Microcurrent is 1/1,000,000 of one ampere. Millicurrent is 1/1000 of one ampere. One ampere will illuminate an average household light bulb. These are very tiny charges. Nowadays all EA stimulator machines use AC voltage. AC stands for alternating current, as opposed to DC, direct current. DC means that the electrical flow is unidirectional—it flows only in one direction and can result in electrolysis. AC means that the electrical flow reverses periodically from one direction to the other. AC eliminates any risk of electrolysis and therefore reduces the risk of causing tissue damage.
Frequency
Frequency is the number of times the waveform completes itself in one second. Frequency is measured in hertz—1 Hz is one cycle per second. So, 15 Hz means that the waveform hits the needles 15 times per second. Increased hertz should not increase the sensation but can surprise patients. That is why I tell practitioners to begin with 2 Hz and then work up to 100 Hz in subsequent treatments. Always slowly and gradually increase the intensity dial until the patient can barely feel the stimulation. Then you can increase it until it is comfortably strong for maximum effect. Your patient should never feel pain or a burning or strong electrical sensation. Also, if you are using a mixed or burst stimulation—let’s say 2–100 Hz—you want to increase the intensity while the 100 Hz is active. In this way you won’t surprise your patient when the machine switches from 2 Hz to 100 Hz. One thing for sure is that the protocols I have listed in Chapter 8 are frequency specific.
Bi-phasic wave patterns are important to understand as well. Bi-phasic wave patterns mean that the wave polarity switches from one direction to the other—positive to negative and the reverse. So, in reference to red and black leads, there is no scientific reason to place one color at any specific end; it is purely a matter of aesthetics if your machine is bi-phasic. They switch polarity, meaning the red or black leads truly do not indicate any specific charge. There are three machines on the market today that are FDA approved for EA, and they are the Pantheon, The Great Wall, and Ito. Pantheon is the only company that offers a bi-phasic wave form.
|
Table 5.1 Basic physical electrical definitions |
||
|
Electrical qualities |
Purpose |
SI (International System of Units) |
|
Electrical current |
Charge of circuit |
Amperes |
|
Frequency |
Cycles per second |
Hertz |
|
Voltage |
Energy of circuit |
Volts |
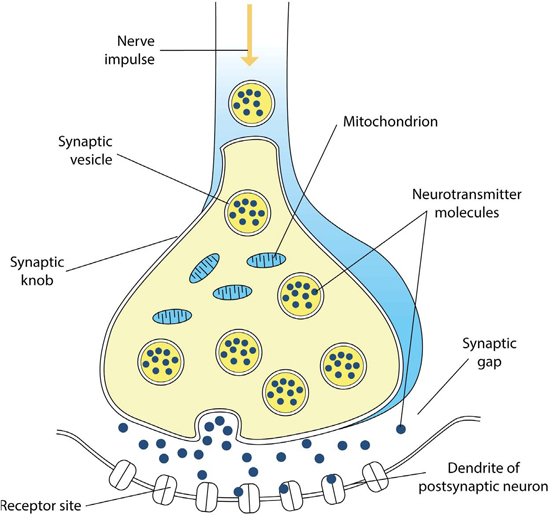
As we discussed in Chapter 4, we now have confirmed specific frequencies that target specific neural receptors. What this means is that we have discovered that our nervous system responds to specific electrical frequencies. We can “communicate” with the CNS via electrical stimulation. We now know that at certain acupuncture points we can target specific areas of the brain and segments of the spinal cord to release specific neurochemicals and that this is all frequency specific. This is all made possible by simply understanding the neuroanatomy of the system, its response to electricity, and how and where to apply EA.
Figure 5.1 Neural synapse
|
Endorphin |
Receptor |
Frequency* |
Location |
|
NK cells |
Immune |
4 Hz |
Widespread |
|
Beta-endorphins |
Mu |
2–4 Hz |
Mid-brain/PAG |
|
Enkephalins |
Delta |
2–4/15 Hz |
Dorsal horn |
|
Dynorphins |
Kappa |
100 Hz |
Brainstem/spine |
|
Orphanin |
Mu |
2/15 Hz |
Widespread CNS |
|
5-HTP |
5-HTPr |
20–50 Hz |
Hypothalamus |
|
Oxytocin |
OXTR |
2–15/30 Hz |
CNS |
|
Dopamine |
D1 |
2, 15–30 Hz |
Prefrontal |
|
nos |
Epithelium |
2, 15–30 Hz |
Widespread |
|
* All frequencies are millicurrent. |
|||
Clinical EA settings and utilizing mixed frequencies, especially in the treatment of pain
So, for many, there is always a question of when to use microcurrent vs. millicurrent, and which frequency to apply and how intense should the stimulation be. I want to use this section to review a clinical application that I have found to be effective when applying EA stimulation. I utilize this theory when mainly treating pain cases that require mixed frequencies from low to high. The theory that research has produced in EA is that microcurrent has the ability to penetrate cellular walls and increase cellular respiration by increasing ATP production. This helps to heal tissues, especially soft tissue. So, I always begin using 25 Hz microcurrent to initiate and support the healing process of the local tissues and reduce inflammation.
I will continue this up to 2–4 treatments, depending on the patient’s response. If the patient is responding well then why “fix something that is not broken,” and I will continue until the condition is resolved. If it is time to change to millicurrent, then I will increase the stimulation to 2 Hz millicurrent at the following session. I will continue this for several treatments. I will then change the setting to 2–15 Hz for a mixed, or burst, stimulation effect, for a few treatments, then go to 2–30 Hz, and finally end up at 2–100 Hz (see Table 5.3).
|
Table 5.3 Sample Electro-Acupuncture treatment protocol |
|||
|
Treatment |
Frequency |
Current |
Time interval |
|
1–2 |
25 Hz |
Micro |
25–45 min |
|
2–3 |
2 Hz |
Milli |
25 min |
|
3–6 |
2–15/2–100 Hz |
Milli |
25 min |
Theories of Electro-Acupuncture’s effects
In this section I would like to share with you groundbreaking research and theories that help to explain EA’s powerful effects. These theories are scientifically fascinating and are currently leading research in the area of EA and spinal nerve regeneration, oncology-electrochemotherapy, and EA-induced stem cell proliferation. These theories are in the process of mouse model clinical trials in Southern California by the International Association for Research of Electro-Acupuncture (IAREA). The team consists of a group of physicians,1 Eastern and Western, who have come together in their own time to help gather and conduct EA research and establish a platform for international relationships between EA researchers.
I personally have seen much more successful research being done in EA than in straight manual acupuncture, and I therefore focus my own investigations on EA. The fact that EA protocols can be further quantified by time, specifically calibrate the amount of stimulation, and are reproducible makes things easier for research and clinical applications. EA has also been shown to maximize acupuncture’s effects and produce the most benefit, so this is another reason why I have chosen to research this specific area of acupuncture and share what I have found with you. There are five main theories that IAREA is currently discussing and researching. I believe that using these theories, and the neurophysiological mechanism described earlier, we can explain all of EA’s effects and in some cases we can combine theories to support the conclusive data. Below I will list each theory, explain it in simple terms, and give an example of how it can be used, or where it may be applied. All of these theories are evidence-based and scientifically rooted.
1. Stem cell theory
With an MD and PhD in quantum mechanics, both from Harvard medical school, Dr. James Dunn is the leader of stem cell theory. Dr. Dunn is investigating the proliferation of stem cells after an EA treatment. He hypothesizes that the electrical stimulation communicates on a quantum level to release more stem cells for healing. Its application is of particular interest where tissue regeneration is needed. Dr. Dunn is a pediatric surgeon and is interested in utilizing this technique to help treat children who have been born with a portion of their small intestine missing. We hope to discover an exact protocol to aid in communicating with a child’s stem cells to heal and regenerate the bowel without surgery, or perhaps assist in the healing post-surgery.
One of our goals is to determine the “amplitude window,” or “frequency window,” of the stem cells’ cellular wall. This infor-mation will give us a direct electrical protocol that will specifically target stem cells, resulting in a proliferation of these stem cells for amazing clinical applications.
Dr. Duong Ha first brought this theory to my attention. A free radical is a negatively charged particle that severely damages human tissue. It has a negative charge because it lacks an electron but it has the potential to gain an electron and become stable, which reduces its harmful effect on live tissue. An antioxidant is a particle that lends or donates an electron to the free radical and therefore stabilizes it. In our research we are trying to measure the human voltage prior to an EA session and then again afterwards to see if there is a measurable difference. Dr. Duong Ha hypothesizes that we are adding electrons to the human body and that the additional electrons act systemically as antioxidants. The question is, which acupuncture points and which frequency and hertz are best to potentiate the delivery of these free electrons to act as antioxidants?
3. Modified “gate theory” (gating the notch) mechanism
Dr. Laura Kelly, who works with spinal cord injury and paralysis, presented this theory to me. The theory is that when there is a spinal cord injury the human body will respond with a “notch signaling mechanism” that blocks the body’s innate healing abilities from healing the damaged nerves. From her experience of reversing paralysis, Dr. Kelly believes that EA stimulation has a “gate theory” application on this notch signaling pathway. Where the EA blocks the notch signaling mechanism, the spinal nerves heal (i.e. the electro-stimulation inhibits the notch signaling pathway and promotes neural stem cell proliferation which heals the spinal cord lesion). See the Kelly Protocol at the end of this chapter. IAREA will be conducting mouse model trials to evaluate and measure the effect of EA on stem cells.
4. Electromagnetic field theory
This is a simple application of electromagnetism to EA that I stumbled upon myself. Wherever electricity is traveling along a metal wire, an electromagnetic field is produced. So, when we attach leads to our acupuncture needles, we are generating a local electromagnetic field around the needle. This I particularly apply to scalp acupuncture. I love utilizing EA on scalp points! In the Neuropuncture protocols where I use scalp points, it is this mechanism that I am applying. This is similar to transcranial electromagnetic stimulation. I have even seen research where EA of the scalp is termed “DCEA—deep cranial electro acupuncture” (Bun, 2014). This type of scalp EA has the same effects as transcranial electromagnetic stimulation does on the brain. It helps to increase blood circulation locally, increases neural activity locally, and helps to heal and regulate cerebral electrical activity. So, if you want, or need, to target the prefrontal cortex, then with an acupuncture point prescription like GB14 to ST8, or ST8 to Taiyang and applying EA, you will. I think this really opens up scalp acupuncture’s application, especially when reviewing the scalp lines and their associated cerebral regions. It is no coincidence that the scalp acupuncture lines are directly over that region of the brain that they treat.
5. Frequency-specific concept—Hilton’s law/stimulating the CNS/PNS via millicurrent and microcurrent
By now you will be aware of EA affecting specific receptors with specific frequencies. This research has been going on since the 1950s. Today we have a very nice understanding of how, when, and where to apply different frequencies to affect specific neural tissue. Research has confirmed the outcomes of the effects of specific frequencies, with specific amps, on specific tissue. For example, is has been confirmed that a 2 Hz millicurrent has the targeted effect on the mu opioid receptor at certain neural anatomical acupuncture points. A 100 Hz millicurrent has the effect of targeting the kappa receptor located in the dorsal horn of the spinal column and affects the enkephalin endogenous endorphin system. Notice they are both millicurrents. In addition, a 2 Hz millicurrent has been shown to help with IgG (immunoglobulin class G) factors and NOS blood levels, 2–15 Hz has been shown to increase fallopian tube blood circulation, and 100 Hz has a neuroprotective effect on the brain. (For protocols, please see Chapter 8.)
When reviewing research with microcurrent, we come across an interesting finding. For starters, the results are always intracellular, affecting cellular organelles. At 25 Hz microcurrent, it has been confirmed that the waveform penetrates the cellular walls and stimulates the mitochondria and stimulates ATP production. This is the mechanism that I have found which explains the findings in many clinical studies, and which is currently being researched. It illustrates the effect of the size of the waveform on the cellular wall and its penetration ability. It is clear that if this waveform penetrates the cellular wall and stimulates the mitochondria, then this same waveform may also have the effect of signaling the generation of the stem cells.
We can also target specific spinal segments with EA by utilizing the dermatome and myotome charts and needling acupuncture points within those areas. EA will also help us to utilize Hilton’s law. By needling major acupuncture points, or motor points of the large muscles that surround a joint of focus and applying EA, we can then affect that joint directly via Hilton’s law.
Oncology cellular wall permeability research: “Electrochemotherapy”
Cancer has been described as a dysfunction of electromagnetism on a cellular level. It can be seen as an invasion into the surrounding intracellular organelles as it affects multicellular systems. The loss of adhesiveness plays a major role in cancer’s metastatic properties. The electrostatic interaction with positively charged atoms at the outer surface could change protein conformation (Pokorny, 2008). It is at this level of focus that EA has an effect. Electrochemotherapy utilizes a cytotoxic chemical in the body and then applies electricity, which changes the cellular membrane and allows the chemotoxic agent into the cells. What IAREA is looking for is the best frequency and hertz to aid in the penetration of cancer cellular walls—this is termed the “frequency window,” or “amplitude window,” and will give us the most effective wave form, frequency, current, and time interval.
This is a very important area for me. I am currently involved in the treatment of children who have been diagnosed with diffuse intrinsic pontine plioma (DIPG). DIPG is a devastating, aggressive brain tumor found in children. It arises in the pons, a region of the brainstem involved in critical body functions. Though brainstem tumors are extremely rare among adults, they comprise approximately 10–15 percent of all pediatric brain tumors. What seems to be the issue is that there is a 100 percent mortality rate for children diagnosed with DIPG. They cannot find a way for the chemotherapy to pass the blood brain barrier and target the cancer. I am therefore working on developing a protocol that will possibly assist in opening channels with EA so that the chemotherapy can permeate the brain and have its desired effect. There is also an EA protocol that I use that increases the “natural killer” cells of our immune system, as well as the IgG factors. I am working on combining techniques and protocols for the best reproducible outcomes.
Brenda Golianu, MD, and Elizabeth Sebestyen, MD, have illustrated that placing acupuncture needles in the “meridians” that travel through the cancerous tumor 1–2 cm proximal to the tumor border, and needling major acupuncture points distal along the same “meridians” and applying 2 Hz millicurrent for 30 minutes, affects the cellular walls of the tumor and definitely potentiates the chemotherapeutics’ effect on shrinking the tumor (Golianu & Sebestyen, 2007).
Contraindications of Electro-Acupuncture
Always listen to your patients. Remember that we are looking for a comfortable, strong sensation (nothing burning or painful). This is what I call the “EA De Qi.” Be sure never to overstimulate and never create any discomfort during treatment. As you have seen and will see with the Neuropuncture protocols, I always cross the spine, cross the head, and even needle into the spinal dura space. You must just be careful, use your common sense, and remember the following:
•Do not EA through an area of the body where there is any electrical device (e.g. pacemakers, medical pumps, spinal stimulators).
•Caution with EA around metal hardware.
•Always use clean needle technique, and use betadine and/or exam gloves when necessary.
•Caution with millicurrent on the face. Microcurrent is safer and effective.
•Caution with epilepsy. Never overstimulate the head and do not cross the brain with any scalp protocols.
•Caution with pregnancy.
•Do not use on any patients who have had electrical trauma (e.g. torture victims, those who have suffered electrical or lightning accidents).
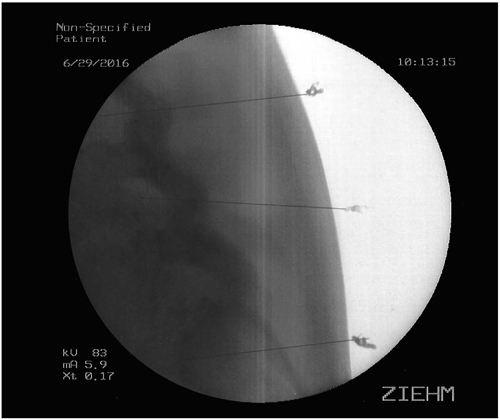
This protocol consists of five steps, to be applied three times a week for up to six months. It is aimed at healing spinal cord lesions including overriding the notch reaction. The theory is that the 25 Hz millicurrent blocks the internal natural noxious signal and allows the body’s natural healing mechanisms to take effect (basically bypassing the signal, or “gating” the noxious notch signal). We have seen this effect clinically in the area of spinal cord injury and paralysis, chronic pain, and with interrupting dysfunctional visceral autonomic reflexes through the spinal segmental Neuropuncture mechanism. The gauge of needle can vary; I use 25 gauge 6 cun needles. Needle placement is illustrated in Figure 5.2.
1.Electrode placement in this case 1 x 6 cun needle into the epidural space at L3, preferably down into the epidural spaces of L4 and L5.
2.Electrode placement in this case 1 x 1 cun needle into all sacral foramen.
3.Electrode placement in this case 4 x 6 cun needles into the epidural space at T12, T8, T4, and T1.
4.Electrode placement in this case 1 cun needles into splenius capitis, splenius cervicis, and longissimus thoracis at C3, C6, T3, T6, T9, T12, L3, and L5, both sides.
5.Simultaneous manipulation of affected limb, either through manual therapy or preferably through assisted movement such as the adapted exercise bicycle as created for the protocol.
Figure 5.2 Fluoroscopy image of the Kelly Protocol for needle placement
1Members of the IAREA team are: James Dunn, MD, PhD; Duong Ha, L.AC.; John Hubacher, MA; Michael Corradino, DAOM, L.AC.; and Laura Kelly, DAOM, L.AC.