Face



Analysis: the checklists
Midface injury
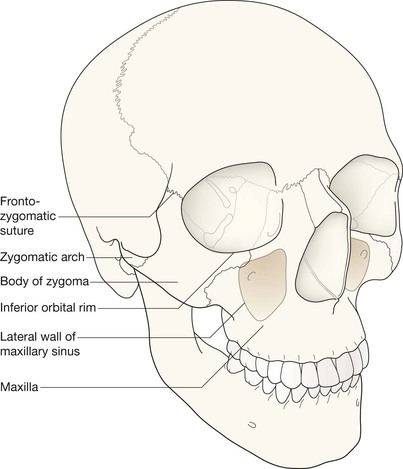
The midface anatomy appears very complex. Try this approach. Think of the zygoma (malar bone) as a midface stool with four legs. The seat of the stool is very strong. The four legs are much weaker, so you need to assess each leg very carefully.
A five-point checklist
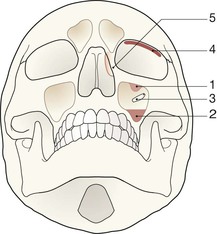
Inspect the OM views as follows:
Concentrate on the stool's legs. For each leg compare the injured side with the other (normal) side. Look for any asymmetry or any difference between the appearance of the matching legs. Check as follows:
2. Leg 2: frontal process of the zygoma.
4. Leg 4: lateral wall of the maxillary antrum.
5. Look for fractures and look for:
□ a fluid level (blood from a fracture) in the maxillary antrum;
Always apply this rule: If any one of the legs is fractured then always, always, double check whether the other three legs of the midface stool are intact (see Tripod fracture, p. 63).



Midface stool—Leg 1
The zygomatic arch. The arch is easy to identify on the OM view, where it may be likened to an elephant's trunk. This is a frequent site of fracture, either as an isolated injury or as part of a tripod fracture. This radiograph is normal.
Potential pitfall: The normal elephant's trunk often has a normal developmental bump on its inferior surface, about half way along the trunk.
Midface stool—Legs 2 & 3
▪ Leg 2: frontal process of zygoma (arrow). The normal frontozygomatic suture will often be lucent. Compare this lucency with the uninjured side.
▪ Leg 3: orbital floor (arrowheads). This leg is slightly peculiar—it runs backwards and posteriorly from the rim of the orbit.
Normal radiograph.

Midface stool—Leg 4
Lateral wall of the maxillary antrum (arrow).
Normal radiograph.

Suspected blow-out fracture
Evaluate the OM view (see p. 66).
Injury to mandible
Evaluate the OPG view (see pp. 68–70).
The common injuries
Casemix varies by hospital type.
| Emergency Department serving a general hospital | Major centre receiving and treating high velocity blunt trauma4 |

Injuries to the midface
Isolated fracture of the zygomatic arch.
This is a common injury (arrow).

Fracture of the inferior orbital margin.
This may occur in isolation or may occur as part of a tripod fracture. An isolated rim fracture (arrow) usually involves the inferior and lateral aspect of this thick, strong, bone.


Tripod fracture. In this combination injury the cheekbone (ie the zygoma) is detached from its four points of attachment to the rest of the facial skeleton3.
A tripod fracture comprises:
Arguably it would be more accurate to call it a quadripod fracture4,13.
The Tripod fracture is also known as: Zygomaticomaxillary fracture complex; Zygomaticofacial fracture; and Trimalar fracture3.
Tripod or quadripod? Terminological discord
The term “tripod fracture” is accepted common usage, derived from an analogy to a three legged stool to describe the midface anatomy3,4,14. We agree with Daffner4 that there are really four legs supporting the stool (the zygoma), so we evaluate the four legs (pp. 58–59). Some other authors envisage a three legged stool as follows:
▪ The malar eminence of the zygomatic bone (the cheek bone) is regarded as the seat of a stool3,4,14.
▪ The three legs are: (1) the zygomatic arch running backwards; (2) the fronto-zygomatic process running upwards; (3) the maxillary process running anteriorly and medially. This third leg is visualised as a somewhat splayed and hollowed out structure4 forming the floor of the orbit as well as the lateral wall of the maxillary antrum.
Orbital blow-out fracture
Following blunt trauma, this injury may be isolated, or accompany any other major or minor facial injury13. It results from a direct compressive force to the globe (ie the eyeball), commonly from a fist, elbow, dashboard, car seat, or small object such as a squash ball.
The diameter of the object that compresses the eyeball is invariably greater than the diameter of the eyeball itself. The blow causes a sudden increase in the intraorbital pressure behind the eyeball, resulting in a fracture or fractures of the thin and delicate plates of bone that form the floor and the medial wall of the orbit.
Approximately 20–40% of patients with an orbital floor blow-out fracture also have a fracture of the medial wall of the orbit15.
Clinical impact guidelines
▪ Imaging for a suspected orbital blow-out fracture: only patients with a clear clinical indication for surgery require imaging16. Ultrasound evaluation is generally preferable to radiography.
▪ If some of the orbital contents herniate downwards through the orbital floor then the inferior rectus muscle may become tethered. Tethering will result in diplopia/opthalmoplegia.
▪ Decisions regarding the need for surgery revolve around:
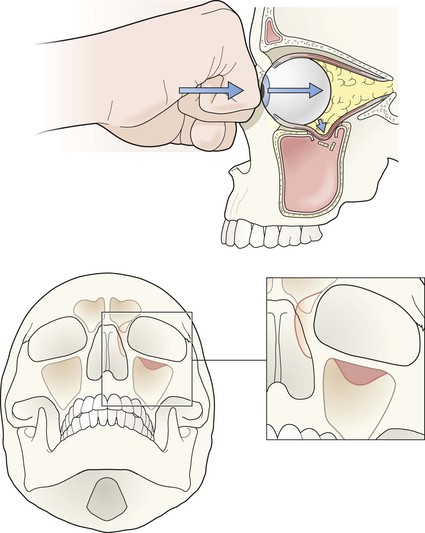
Isolated blow-out fracture.
The blow to the eyeball has increased the intraorbital pressure and resulted in a fracture of the thin plate of bone that forms the floor of the orbit. The soft tissue teardrop in the roof of the maxillary antrum represents herniated orbital contents (dark shading). Herniation through the medial wall of the orbit into the ethmoid sinus (light shading) commonly occurs but is difficult to detect on a radiograph.
Orbital blow-out fracture—the OM findings
▪ The strong inferior orbital margin remains intact when a blow-out fractureis an isolated injury.
▪ Some orbital contents (fat and/or the inferior rectus muscle) may herniate downwards through the delicate orbital floor. This appearance has been likened to an opaque teardrop hanging from the roof of the maxillary antrum1. This teardrop may be the only radiographic evidence of a blow-out fracture.
▪ The bone fragment (from the orbital floor) is very thin and is rarely seen.
▪ Sometimes a blow-out fracture may be inferred because air from the breached sinus has entered the orbit. This orbital emphysema may be positioned above the eyeball. Air appears black on the radiograph. This has given rise to the description of the “black eyebrow” sign.

Blow-out fracture with a teardrop. Soft tissue can be seen hanging from the roof of the right maxillary antrum.

Blow-out fracture with a black eyebrow. Note the black eyebrow sign above the left eyeball. Also note the teardrop in the roof of the antrum.
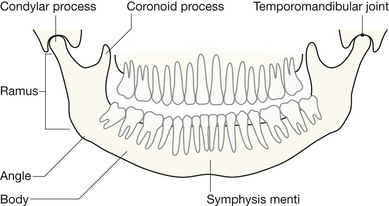
Injuries to the mandible
Assessing the OPG
Sometimes the panoramic view (OPG) fails to show a fracture17. It is very important that radiological evaluation of the mandible is correlated with the precise site of clinical concern. The symphysis is particularly difficult to evaluate on an OPG; a near normal appearance may occur when fragments override each other. Clinical suspicion must always take precedence over a seemingly normal OPG. If there is any doubt, then additional radiography is indicated—a PA radiograph in the first instance.
Important points to check
▪ Think of the mandible as a rigid ring of bone. When a ring of bone is broken it is very common for two fractures to occur in the ring. 50% of mandible fractures are bilateral18.
▪ Always check for symmetry—compare one side of the mandible with the other.
▪ Check for fractures of the body and angle of the mandible.
▪ Assess the mandibular condyles carefully. Fractures here may be very subtle.
▪ Check for correct dental occlusion. The upper and lower teeth should have even and equal spacing on the radiograph. Displaced fractures, or a fracture through the neck of a condyle, frequently produce uneven spacing between the teeth4,11.
▪ Check for any step deformity in the line of the teeth of the lower jaw. This invariably indicates a fracture.
▪ Assess the temporomandibular joint (TMJ, see p. 56).
Be careful. The OPG will produce some appearances that can be confused with a fracture. These artefacts are mainly due to the overlapping image of the pharynx or tongue. Familiarity with the possible artefacts (pp. 69 and 72) will prevent an incorrect interpretation.


OPG.
Two mandible fractures (arrows).
Note: in the OPGs on this page we have excluded the TMJs for illustrative purposes.



OPG.
Normal, showing artefact due to the tongue (arrows).
Occasionally an artefact may be misinterpreted as a fracture.

Pitfalls

Normal bump (arrow) on the inferior aspect of a zygomatic arch. A common normal variant—a muscular attachment.

Frontal sinus extension into the orbital plate of the frontal bone (arrow) can mimic the Black Eyebrow Sign.


Asymmetry of the normal zygomaticofrontal sutures on an OM (arrows). This is an occasional normal variant.

The common artefacts/normal shadows on an OPG radiograph.
Soft palate (white shaded area). Dorsal surface of the tongue (black arrows). The oropharyngeal airway between the soft palate and the dorsal surface of the tongue creates a black line across the ramus of the mandible (white arrows). The band of increased density projected over the midline is due to the cervical spine which lies outside the focal plane (black arrowheads). Hyoid bone (white arrowheads).