754
PART 4 Regulation and Maintenance
TABLE 21.14
Blood Pressure Classification in Adults

Source:
The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, U.S. Dept. of Health and HumanServices, NIH Publication No. 03–5233, May 2003.
blood pressure at the arterial end of the capillaries is approximately30 mm Hg, and it decreases to approximately 10 mm Hg at thevenous end. Resistance to blood flow in the veins is small becauseof their relatively large diameter; by the time the blood reaches theright atrium in the venous system, the average pressure hasdecreased from 10 mm Hg to approximately 0 mm Hg.The muscular arteries and arterioles are capable of constrict-ing or dilating in response to autonomic and hormonal stimulation,altering resistance and blood flow. If vessels constrict, resistanceto blood flow increases, less blood flows through the constrictedblood vessels, and blood is shunted to other, nonconstricted areasof the body. Muscular arteries help control the amount of bloodflowing to each body region, and arterioles regulate blood flow
through specific tissues. Constriction of an arteriole decreasesblood flow through the local area it supplies, and vasodilationincreases blood flow.

ASSESS
YOUR PROGRESS
44.
List the percent distribution of blood in the large arteries,small arteries, arterioles, capillaries, small veins, and largeveins.
45.
Describe the total cross-sectional areas of the aorta,arteries, arterioles, capillaries, venules, veins, and venaecavae.
46.
Describe how the rate changes as blood flows throughthe aorta to the venae cavae.
47.
Describe the changes in resistance and blood pressure asblood flows through the aorta to the venae cavae.
48.
Explain how constriction and dilation of muscular arteriesshunt blood from one area of the body to another and howconstriction and dilation of arterioles change blood flowthrough local areas.
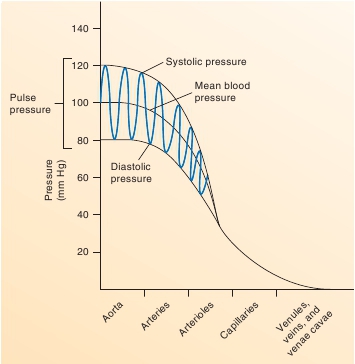
Pulse Pressure
Pulse pressure
is the difference between systolic and diastolicpressures (figure 21.34). For example, in a healthy, young adult atrest, systolic pressure is approximately 120 mm Hg, and diastolicpressure is approximately 80 mm Hg; thus, the pulse pressure isapproximately 40 mm Hg (= 120 mm Hg – 80 mm Hg). Twomajor factors influence pulse pressure: (1) stroke volume of theheart and (2) vascular compliance. Pulse pressure is directlyrelated to stroke volume. When stroke volume decreases, pulsepressure also decreases; when stroke volume increases, pulse pres-sure increases. For example, during exercise, such as running, thestroke volume increases; as a consequence, the pulse pressure alsoincreases. After running, the pulse pressure gradually returns to itsresting value as the stroke volume of the heart decreases.Pulse pressure is inversely related to vascular compliance. Asvascular compliance increases, pulse pressure decreases. Con-versely, as vascular compliance decreases, pulse pressureincreases. The vascular compliance decreases as a person ages.Arteries in older people become less elastic, or arteriosclerotic,causing the pressure in the aorta to rise more rapidly and to agreater degree during systole and to fall more rapidly to its diastolicvalue. Thus, for a given stroke volume, systolic pressure and pulsepressure are higher as vascular compliance decreases.
FIGURE 21.34
Blood Pressure in the Major Blood Vessel Types
In small arteries and arterioles, blood pressure fluctuations betweensystole and diastole are reduced. No fluctuations in blood pressure occurin capillaries and veins.