Traumatic injuries, gastrointestinal (GI) foreign bodies, and conditions related to neoplasia make up the majority of surgical diseases in ferrets in the United States, and it is not uncommon to identify more than one indication for surgery as an incidental finding during the diagnostic workup for another disease [1–5]. When considering the value of surgical intervention of any particular condition in ferrets, it is important to recognize that 2 years represent 25% of the average lifespan of ferrets in the United States [5].If the goal of surgical treatment is to prolong and improve the quality of life of the ferret, then a 1–2-year survival with good quality of life is considered a success.
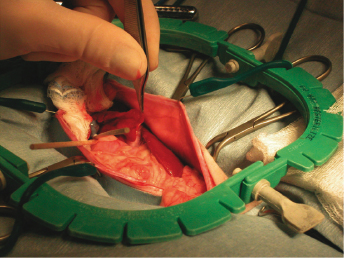
Surgical procedures in ferrets are similar to those performed in dogs and cats. Because of the small body size of ferrets, microsurgical instruments, magnifying loupes, smaller suture sizes, body temperature support devices, and smaller retractors (Lone Star retractor, Lone Star Medical Products, Stafford, TX) are important tools for the practitioner or investigator performing procedures on ferrets (Fig. 13.1).
Fig. 13.1. A self-retaining retractor is routinely used for abdominal surgery in ferrets. A ring or Lonestar retractor (Lone Star Medical Products) is ideal for ferret abdominal surgery. The plastic outer ring has notches around its circumference allowing for multiple skin hooks to be used to keep the incision open.
Presurgical Considerations
All ferret patients, regardless of signalment and health, should have a complete physical examination before undergoing anesthesia and surgery. All patients will also benefit from presurgical hematological and biochemical screening that, at a minimum, should include the following: packed cell volume, total protein, blood glucose, renal and liver profile, blood smear, and urine specific gravity. Depending on the signalment, underlying disease, and indication for surgery, a more complete assessment of the patient may be indicated including a full biochemical profile, complete blood count, urinalysis, coagulation profile, and a variety of imaging modalities.
Hemostasis
Loss of 10% of the total blood volume is usually safe (approximately 1% of body weight) in a healthy patient under anesthesia. Blood vessels are frequently torn, sheared, and cut during surgery. Many are small and do not result in significant hemorrhage as a result of properly functioning intrinsic and extrinsic clotting mechanisms. A transected vessel will undergo vasospasm, resulting in a decreased diameter at the cut end, making it easier for a clot to stop the bleeding. Platelets and clotting factors are stimulated by the trauma to form a clot, plugging leaks from damaged vessels and resulting in hemostasis. Hemorrhage from larger vessels requires intervention by the surgeon in the form of direct pressure, electrocautery, electrosurgery, radiosurgery, laser, ultrasonic scalpels, and application of hemostats, topical agents, ligatures, clips, staples, and vascular collagen sealing technologies.
Applying pressure to a bleeding vessel prevents blood from escaping while allowing the patient's clotting mechanisms time to create a clot. The hemorrhage that is created from a skin incision or a transected vessel within a muscle is a good example of bleeding that can often be stopped by gentle pressure. Most surgeons use sterile gauze squares or cotton-tipped applicators (CTAs) to assist with hemostasis. It is important to have knowledge of a patient's blood volume, acceptable (safe) amount of blood loss, and the potential volume of blood contained within each of the hemostatic agents utilized in surgery. For example, a CTA holds about 0.1 cc of blood, a 2 × 2 gauze holds 3–5 cc, a traditional 4 × 4 sponge holds about 10 cc, a 4 × 4 with a radiopaque strip commonly holds 10–20 cc, and a traditional laparotomy sponge can hold up to 100 cc of blood [6].A healthy 1-kg ferret under anesthesia can safely lose 10 cc of blood, that is equivalent to 100 fully saturated CTAs or a single saturated 4 × 4 sponge.
It is important to allow blood to get to the site of vessel injury. If too much pressure is applied, the clotting factors and platelets will not reach the site and no clot will form. Each time pressure is released, additional hemorrhage will occur. Once a clot forms, it must not be disturbed. Blood must be blotted or dabbed with gauze and not wiped, as this would carry the freshly formed clot away.
Hemostatic forceps are designed to occlude and crush the damaged vessel. The additional damage to the vessel wall further attracts clotting factors and platelets to the site for clot formation. The smallest size hemostat appropriate for the vessel should be used and a minimum amount of additional tissue should be grasped. Tissue within the forceps will be crushed and likely undergo necrosis. The hemostats should be left on the vessel several minutes to allow the clot to form. Traditional encircling square knots or transfixation ligatures are used for larger vessels. It is important to note that the larger (greater diameter) the suture material and the bulkier the knot (surgeons throw, Miller's knot), the less secure the knot will be.
Hemostatic clips, such as Hemoclips (Hemoclips and Samuels Hemoclip Applier, RICA Surgical Products, Inc, Chicago, IL) serve the same purpose as ligatures. They are quick and easy to apply. They are especially valuable in small, deep, and tight spaces where it is difficult to apply a ligature accurately and securely or to add to the security of an already placed ligature. Hemoclips and surgiclips are useful for ligating arteries, veins, ducts, or bronchi in ferrets. They are available in various sizes and it is recommended that the length of the clip be twice or thrice the diameter of the vessel or structure to which they are being applied. Another way to estimate appropriate clip size is if the diameter of the vessel to which the clip is being applied is less than one-third of the length of the clip, the clip is likely to slip or migrate. If the diameter of the vessel is greater than two-thirds the length of the clip, the clip is likely to fail and incompletely engage the vessel diameter. Some companies (RICA Surgical) will provide an applier when one purchases a box of clips. Right-angled appliers are also available and are especially useful for applications deep in the body cavity of small patients and have proven extremely useful for ferret adrenalectomy.
The linear stapler (also known as the thoracoabdominal stapler or thoracic anastomosis stapler; Infiniti Medical, Palo Alto, CA) is useful for partial and complete liver lobectomy, lung lobectomy, and partial and complete splenectomy in ferrets (Fig. 13.2). The linear stapler comes in three staple-line lengths and two sizes of staples. The linear stapler 55-mm- and 90-mm-long staple lines place two staggered rows of staples in the tissues and can be helpful in stopping hemorrhage from liver lobes; however, without the use of direct pressure or topical hemostatic agents, oozing often persists after placement of these staples. The linear stapler 30 mm V3 is a shorter staple line but applies three staggered rows of staples to the tissue and will often arrest local hemorrhage from a partial liver lobectomy or reinforce ligatures placed on the portal vein branch, hepatic artery, and hepatic vein branch supplying and draining a liver lobe, respectively.
Fig. 13.2. Thoracoabdominal (TA) stapler, applier, and staple cartridge. The white cartridge is a TA30 V3. This is the shortest cartridge available and applies three 30-mm long staggered rows of staples. This is the ideal cartridge size for partial or complete liver lobectomy or partial splenectomy.
Thrombin is commercially available as a topical hemostatic agent. It is available as Thrombin-JMI (GenTrac, Middleton, WI) in vials of different volumes and can be applied directly to the tissue or used to soak gelatin sponge or cellulose to further promote clotting. Thrombin binds to fibrinogen and forms soluble fibrin monomers that polymerize. Factor VIIIa links the polymers to form insoluble cross-linked fibrin and a clot. Fibrin also promotes many other procoagulation reactions in the clotting cascade.
Gelatin sponge (Gelfoam; Pfizer, distributed by Pharmacia & Upjohn Co, New York, NY and Vetspon; Ethicon, Johnson & Johnson, Sommerville, NJ) is a sterile, absorbable hemostatic agent. It promotes clot formation by providing a matrix on which a clot can form. It is absorbed in 4–6 weeks and invaded by fibrous tissue. This is commonly used over the stump left by partial liver lobectomy or to pack off the hepatic fossa after cholecystectomy. Small pieces can be broken off and rolled to fit into a punch liver biopsy site. Because it is thick, it retains its shape and does not conform well to the tissue on which it is placed.
Oxidized regenerated cellulose (Surgicel, Ethicon, Johnson & Johnson) is also absorbable and functions by providing a matrix for clot formation. It is a cloth-like material with less absorptive capacity than gelatin sponge but is ideal for use on the concave or convex surface of any organ that requires hemostasis.
Electrosurgery can also be used for hemostasis. Electrosurgery uses an alternating current to generate heat resulting in vaporization of intracellular water. This results in cell rupture and cuts tissue or generates heat that coagulates protein for hemostasis. Most units use a frequency of 0.4–1.5 MHz and have monopolar and bipolar capability. Monopolar electrocautery requires a ground (or patient) plate. The energy generated while using the device passes through the patient to the ground plate. The ground plate must be in complete contact with the patient at all times and the surface area of contact should be maximized. If the contact area has a small surface area, the energy passing through the patient is not dispersed widely and a severe thermal burn occurs. The larger the surface area of contact, the more energy is dispersed over a larger area, and the chance of a thermal burn occurring is proportionally diminished. Bipolar electrosurgical forceps contain both electrodes in the forceps so there is no need for a ground plate. Bipolar electrosurgery is useful for surgery in small mammals and is a necessity for more advanced surgical procedures in ferrets, for example, right-sided adrenalectomy. The forceps are insulated except for the tips. If a noninsulated portion of the forceps contacts tissue, the current will pass from one electrode through the tissue, and to the other electrode without accomplishing the required function at the tips. They are most useful for hemostasis within body cavities and near larger neurovascular structures as bipolar electrosurgery does not pass through the patient
Radiosurgery (SurgitronR, Ellman International, Inc., Hewlett, NY) uses radio frequency current, which is received by the indifferent electrode acting as an antenna. As such, the indifferent electrode or ground does not have to be in contact with the patient, eliminating the concern of burning the patient at the exit site of ground plate contact. Ellman has created an adapter switch for older generators that allows the surgeon to switch from monopolar (used for cutting skin and muscle), to bipolar (used for coagulating within a body cavity), and back without having to unplug electrodes.
LigaSureTM (Valleylab, Boulder, CO) is a vessel sealing system that has gained popularity for traditional open and minimally invasive procedures in veterinary and human medicine. This technology can be used in ferrets for lung lobectomy, liver lobectomy, intestinal resection and anastomosis, splenectomy, adrenalectomy, and amputation. The generator senses the type of tissue within the tips, then delivers exactly the right amount of current to result in the melting of the collagen and elastin within the tips, which reforms to create a permanent seal. The manufacturer claims that this device permanently seals vessels up to 7 mm in diameter and generates <1 mm of collateral heat damage. The use of this system has replaced the need for titanium stapling devices, such as the TA 30 V3, in many lobectomy surgeries. The device is unable to predictably seal hollow luminal organs or ducts.
Blood Products
Many of the surgical diseases presented in this chapter require aggressive and challenging operative procedures. The use of perioperative blood products may be needed in some cases. Whole blood or packed red blood cell transfusions have been used in clinical patients. Ferrets only have one blood type, and transfusion reactions have not been reported, but minor cross-matches are still recommended by some [7–9]. Oxyglobin (Biopure, Cambridge, MA) is a hemoglobin replacement product that increases the oxygen-carrying capacity of the blood and has been used in ferrets with no reports of adverse reactions [10]. The beneficial effects are still speculative. The product has a long shelf life but is no longer readily available.
Instrumentation and Patient Preparation
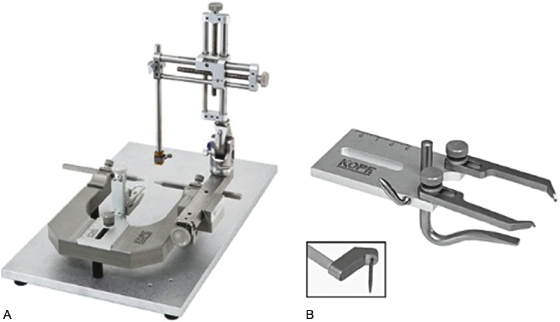
Standard aseptic technique is essential with small mammal patients. Cutting corners with patient preparation is a common cause of increased morbidity and mortality in exotic animal anesthesia and surgery. Many small mammal surgical patients are delicate, with a large body surface : volume ratio predisposing them to hypothermia. A short operative time accomplished by having all of the necessary equipment ready and accessible will diminish the development of hypothermia. Alcohol as a surgical preparation solution should be avoided as the evaporative cooling will predispose the patient to hypothermia. Instead of alcohol, prewarmed 0.9% NaCl can be used to rinse the skin preparation solution from the skin of the patient. A circulating warm water blanket under the patient should be set at 104°F as these patients have a higher resting body temperature than most domestic pets. Instead of, or in addition to more traditional heating strategies, such as warm water bottles or circulating warm water system, a forced warm air system (Bair Hugger®, 3M Infection Prevention Division | 3M Center, 275-4E-01 St. Paul, MN) or a conductive fabric warming system (HotDog®, Augustine Temperature Management, Eden Prairie, MN), can be used to maintain appropriate core body temperature (Fig. 13.3). Draping the patient as quickly as possible is beneficial as heat is entrapped beneath the drape. Clear plastic and paper drapes generally help retain heat better than cloth drapes, and plastic drapes allow for an unobstructed view of the patient during the procedure. Also, plastic, paper drapes, and gowns are less permeable compared with cloth, decreasing the risk of contamination from the striking through of body fluids, saline, and pathogens. A plastic drape with a 3.5 × 5 in. adhesive center and an overall size of 24 × 24 in. is available from Veterinary Specialty Products, Inc. (VSP; Boca Raton, FL). This drape is placed over the patient and a table drape is placed over that. A large fenestration is then cut into the paper drape over the plastic drape. This allows the surgeon to maintain a sterile field over the entire table and still be able to monitor the patient.
Fig. 13.3. HotDog® (printed with permission from Hot Dog Patient Warming. Augustine Temperature Management, Eden Prairie, MN), a conductive fabric warming system used to maintain appropriate core body temperature in a ferret recovering from abdominal exploratory surgery.
The doses of emergency drugs should be calculated and drawn up prior to inducing anesthesia. They will frequently require dilution to a measurable volume. Insulin syringes (0.5 cc) are accurate to a volume of 0.01 cc; however, the needle cannot be easily disconnected from the syringe. These drugs are inexpensive and having them ready preoperatively will minimize drug preparation time and delay in administration.
Some form of magnification is recommended for surgery in patients weighing less than 1 kg or for any-size patient requiring vascular or ureteral procedures. Individual vessels are much more easily identified for coagulation under magnification, minimizing the degree of hemorrhage associated with a procedure. The dexterity and manipulation of fingers and hands are far greater than can be achieved using unaided vision. It is recommended that microsurgeons abstain from the use of alcohol, too much caffeine, other stimulants, and heavy exercise prior to surgery because of their potential to exacerbate tremors. Surgeons accustomed to caffeine should not abstain completely as this can also induce hand tremors. The major disadvantage of performing surgery under magnification is that it generally requires more time to complete a procedure.
Binocular loupes are a less expensive alternative but have certain limitations. Various styles are available, with the hobby loupe being the simplest and least expensive ($20–50). They have a set focal distance, such that only objects that distance from the lens are in focus. As a result, surgeons must hold the head at that distance from the patient. The higher the magnification, the shorter the focal distance. With a 5× lens, the surgeon's face will be only a few centimeters from the patient. The lenses are located in front of the eyes, such that the surgeon is obliged to look through the lenses. Hobby loupes do not have an attached light source, making it difficult to see within body cavities, and most overhead surgical lights will not provide adequate illumination for accurate visualization of deep structures.
Many companies sell loupes with a focal range that provide magnification over a range of distances from the patient (SurgiTelR General Scientific Corp., Ann Arbor, MI; starting at $1200). Such loupes eliminate many of the problems associated with the hobby loupes. Xenon, halogen, or light-emitting diode (LED) light sources are available with a rechargeable battery so that the surgeon is not tethered to a wall outlet. The standard light generator is very small and lightweight. The lenses and light source are attached to either a pair of glasses or a headset. They are interchangeable in the event that a different magnification is required. The surgeon can either look through the lenses or look over them if looking for suture or instruments. The focal range of the lens varies with the specific magnification of the lens but is generally from 10 to 30 in. With this system, any object within that focal range will be in focus, allowing the surgeon to look around during surgery without becoming nauseous or dizzy.
Microsurgical instrumentation should be considered for many operations performed in ferrets, especially adrenal surgery, small intestinal procedures, and some urinary tract surgeries. Many microsurgical instruments are constructed such that only the tips are miniaturized. The handles should be of normal length to help provide stability to the tips, thereby diminishing the effects of tremors. The handles of needle holders should be round to facilitate the required rolling action needed to appropriately drive a curved needle through delicate tissue without tearing it. These instruments are very delicate and must be treated with care. The microsurgical pack should include microscissors, microneedle holders, and microforceps. Many prefer needle holders without a clasp or box lock as the motion that occurs when the lock is set and released may be enough to cause the needle to tear tissues. The following instruments are recommended by the author and are available from RICA Surgical (Schiller Park, IL; http://www.ricasurgical.com). Long jeweler's forceps #3 has a fine delicate tip but flat handles, round-handled microsurgical forceps, Castroviejo pen needle holder 5.25 in. has fine jaws and rounded handles, and Tew-Barraquer scissors curved 7 in. have rounded handles and are spring loaded for easy opening and closing. These instruments will allow the surgeon to dissect and suture with fine control, minimizing tissue crushing, stretching, and tearing, all of which lead to excessive amounts of inflammation, excessive hemorrhage, delayed wound healing, and higher rates of partial and complete dehiscence.
Experience in microsurgery can be gained through continuing education courses, instruction from an experienced microsurgeon, and by practicing on cadaver specimens. Rat femoral arteries and veins are approximately 1 mm in diameter and are routinely used for practicing microvascular surgery. Penrose drains can be used as an inexpensive model for practicing microsurgical cutting and suturing.
The Lonestar retractor or ring retractor is ideal for use during abdominal surgery in the ferret. In some larger ferrets, a small Balfour abdominal retractor or Gossett retractor will work well.
Abdominal Surgery
For a majority of the surgical diseases described in this chapter, a ventral midline laparotomy is indicated. Ferrets have relatively thick skin, little subcutaneous tissue, and a wide, thin linea alba [11].A complete abdominal exploratory should be performed anytime the peritoneal cavity is entered. This can only be accomplished by making an incision from the caudal aspect of the xyphoid to the cranial aspect of the pubis [10].
Abdominal Exploratory
The abdominal exploratory in a ferret is performed in the same systematic method as in other mammals. There is no right or wrong place to start; however, it is important to evaluate all of the structures in the peritoneal cavity and to perform the exploratory the same way every time, so that nothing is missed. An example of a systematic exploration of the abdomen begins with the peritoneal surface of the diaphragm. The diaphragm is easily evaluated by sliding the palmer surface of the hand against the ventral and cranial convex surface of the liver and applying gentle caudal retraction of the liver [10]. The diaphragm should be concave and the central white tendinous portion is surrounded by a radial muscular portion. The lobes of the liver are evaluated next. Each lobe is evaluated individually and all surfaces of the lobe are palpated and visualized. The gallbladder is then identified between the quadrate lobe and the right medial liver lobe. The gallbladder in ferrets is similar to that of cats and may be bilobed [12]. Gentle and constant pressure is applied uniformly to the gallbladder to make sure it expresses readily. The spleen is then identified on the left side of the abdomen and the dorsal and ventral surfaces are visualized and palpated. The spleen is retracted ventrally and to the right of midline to expose the left retroperitoneum, kidney, left adrenal, and, if present, the left ovary. The peritoneal membrane should be incised to enter the retroperitoneum to visualize and palpate the entire left adrenal. The duodenum is identified on the right side of the peritoneal cavity and it is retracted ventrally and to the left of midline to expose the right retroperitoneum (right kidney, adrenal, and ovary). The esophageal hiatus is visualized next by applying gentle traction to the body of the stomach. The esophageal hiatus is located dorsally and on the left side of the diaphragm. The distal esophagus and cardia are palpated, as well as the body, fundus, pyloric antrum, and pylorus. The stomach should have two distinct palpable layers. The first layer is the submucosa-mucosa layer and the second is the seromuscular layer. These are identified by placing a fold of the stomach body between the thumb and index finger and allowing the deeper layer to slip out of the grip of the thumb and finger while still maintaining a hold on the outer seromuscular layer. The novice surgeon may misinterpret the pylorus as a mass or abnormal thickening of the gastric outflow tract: remember, the pylorus is a thick, circular band of overlapping muscle systems and will palpate very thick and masslike at times. The small intestine is evaluated next by beginning at the most orad segment of the duodenum. The duodenum is relatively short in the ferret [13]. The entire jejunum and ileum (jejunoileum) is evaluated. The cecum is absent in ferrets, making the ileocolic junction impossible to identify grossly [12,13]. The colon is evaluated along its entire length. The urinary bladder is then identified and palpated. In males, the prostate, vas deferens, and prostatic urethra are visualized by gently retracting the urinary bladder cranially. The apex of the bladder is retracted ventrally and caudally to expose the dorsal aspect of the urinary bladder, the termination of the vasa deferentia as they enter the prostate, the ureters as they enter the lateral ligaments of the bladder, and the trigone at the ureterovesicular junction. In females, the uterine body and uterine horns are visualized dorsal to the urinary bladder and ventral to the descending colon.
The pancreas is evaluated by first evaluating each limb separately and then visualizing the entire pancreas. The right (duodenal) limb is evaluated by identifying the descending duodenum and retracting it ventrally. The dorsal and ventral surfaces of the right limb of the pancreas are visualized and palpated by moving the ventrally retracted duodenum to the left and right respectively. The left limb is identified along the ventral and caudal border of the greater curvature of the stomach and is often found extending to the hilus of the midbody of the spleen. The entire pancreas can be evaluated at the same time by creating a rent in the ventral leaf of the greater omentum. With the descending duodenum on the right side, the spleen on the left, and the stomach in its normal position, the left and right limb of the pancreas, as well as the body, are visualized.
Gastrointestinal (GI) Surgery
Indications for GI surgery in pet ferrets include GI foreign body, biopsy, and resection of benign and malignant tumors. GI neoplasia has been reported in ferrets [14–21],but is not a common site for primary neoplasia [22].
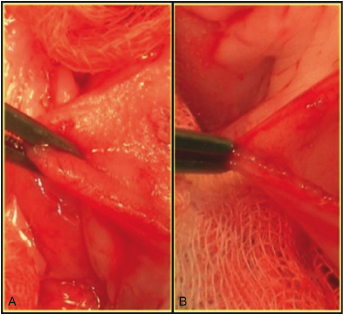
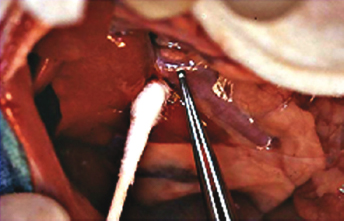
Ferrets have a similar GI tract to that of other carnivores; however, ferrets lack an obvious and distinct ileum as there are no antimesenteric vessels covering the ileum in this species, and there is no appreciable cecum [11,23,24]. The principles and techniques of GI surgery used in domestic small animals are applied to ferret GI surgery. Delicate tissue handling, the use of stay sutures instead of direct manipulation with thumb forceps, or, if using forceps, grasping the serosa and not full thickness bowel (Fig. 13.4), use of appropriate suture size and type, and minimization of trauma, desiccation, and tension during surgery will minimize dehiscence and other untoward outcomes during healing. A monofilament, absorbable suture material with a consistent, known rate of absorption and minimal reactivity is suitable for use in the small intestine. The smallest diameter suture material on the smallest diameter needle that is appropriate for the size of the patient is used. Polydioxanone and polyglyconate are most commonly used. Nonabsorbable monofilament sutures such as polyamide (nylon) and polypropylene are also acceptable. Braided or multifilament suture materials are not good choices as they cause more trauma and tissue drag as they pass through the tissue and may harbor bacteria. Chromic gut is not used due to its unpredictable rate of absorption, especially in the presence of inflammation. Gut will also incite a significant inflammatory response. When suturing the bowel, 4-0 or 5-0 suture material is typically used. A double layer closure is usually preferred for the stomach of ferrets when a simple gastrotomy has been performed. The first layer is a simple continuous pattern in the mucosa and submucosa, followed by an inverting continuous pattern in the seromuscular layer. Single layer, direct apposition of the bowel is preferred for rapid healing and preservation of bowel luminal diameter. A single layer appositional pattern in the small intestine decreases luminal diameter by 4%, compared to a 54% decrease with a two-layer inverting pattern, and a 39% decrease with a one-layer inverting pattern [25]. In small intestinal surgery, accurate apposition is difficult to obtain because of mucosal eversion. There are three recommended methods to limit mucosal eversion; mucosal trimming with scissors, mucosal trimming combined with the use of an interrupted modified Gambee suture pattern, or use of a simple continuous suture pattern.
Fig. 13.4. Enterotomy for foreign body retrieval in a ferret. Panel A demonstrates an inappropriate method for manipulating the bowel wall. This technique will induce full thickness swelling and inflammation, which affects the healing potential and holding power of the submucosa. Panel B depicts the appropriate technique for manipulating the bowel wall. Only the outer layer of the small intestine is being grasped, limiting the posttraumatic swelling to the holding layer of the intestine.
Colorectal surgery is rarely indicated in ferrets. Colorectal tumors, perforations from trauma or neoplasia, and biopsies are the most common reasons for operating on the colon or rectum. The extremely high bacterial counts and the relatively high collagenase levels present in the colon of mammals during early wounding are associated with a higher postoperative morbidity when compared with similar procedures performed in the small bowel. It is imperative that the surgeon is thorough in the packing off of the bowel to prevent contamination of the abdomen, that the wound is closed without any tension, and that mucosal apposition is achieved in the closure. A monofilament, long-lasting absorbable suture material on a tapered needle in a simple interrupted pattern is used for colotomy or colonic resection and anastomosis.
It is important to thoroughly pack off and protect the rest of the abdomen and viscera with moistened gauze squares or laparotomy sponges during GI surgery. The part of the GI tract of interest is surrounded by multiple layers of sponges or gauze squares so that the superficial layers can be removed from the surgical field as they become contaminated with GI material. The enterocytes of mammals require direct nutrition from luminal glutamate for energy and healing, so immediate postoperative enteral nutrition is critical in the successful outcome of ferrets undergoing GI surgery. This, accompanied with the rapid GI transit time, high metabolic rate, and propensity for the development of hepatic lipidosis in ferrets, demand early postoperative enteral nutrition in this species. If the patient will be unable or unlikely to voluntarily ingest adequate calories in the early postoperative period, an esophageal, gastric, or jejunal feeding tube is recommended.
Foreign Body Obstruction
Foreign body ingestion is common in pet ferrets [11,26].Ferrets are inquisitive and have a propensity to chew on rubber and plastic [22,24]. Ingestion of foreign objects usually occurs in ferrets under the age of 2 years, whereas trichobezoars are more commonly observed in older ferrets. Linear foreign bodies are rarely seen in ferrets, and intestinal perforation secondary to foreign body obstruction is uncommon. In the author's recent experience of GI foreign body in 24 ferrets, 18 caused pyloric outflow or proximal duodenal obstruction and six were located within the small intestine. Age did not determine the type or location of the foreign body. One ferret had a linear foreign body and secondary duodenal perforation of the mesenteric surface of the distal duodenal segment. All 24 ferrets survived to discharge.
Clinical signs of GI foreign bodies in ferrets include anorexia or inappetance, diarrhea, ptyalism, facial rubbing, and vomiting (although this is not commonly reported by the owners) [22,26]. Abdominal palpation may elicit discomfort, and palpation of the foreign body is usually possible, especially if it is in the intestinal tract [15,22,26]. Pyloric adenocarcinoma has been described in ferrets and clinical signs include those associated with an upper GI obstruction; vomiting, weight loss, anorexia, and lethargy [14,19,20].
Diagnosis is based on signalment, history, and physical examination. The ferret abdomen is easy to palpate, making most foreign bodies readily palpable within the GI tract [27]. A complete blood count, serum biochemistry panel, and urinalysis should be performed. Abdominal radiographs and ultrasonography are useful in confirming the diagnosis and determining the location of the obstruction. The ferret should be stabilized with intravenous fluids before surgical removal is pursued.
The majority of GI foreign bodies in ferrets need to be removed surgically. GI foreign bodies in ferrets rarely pass on their own. The use of GI lubricants and fluid replacement therapy may allow smaller nonobstructive materials to pass, especially hairballs [22].
A ventral midline abdominal exploratory should be performed in any ferret with a GI foreign body. The pancreas, adrenal glands, and other abdominal viscera should be carefully evaluated for concurrent diseases. A gastrotomy and/or enterotomy are usually indicated, with intestinal resection and anastomosis less frequently necessary.
Gastrotomy
Gastrotomy preparation in ferrets is similar to that of other species [25,28]. It is recommended to utilize stay sutures and to pack off the stomach with layered moistened laparotomy sponges or gauze squares. Stay sutures are used instead of thumb forceps or other instruments for manipulation of the stomach to decrease iatrogenic trauma and swelling. The stay sutures are placed in the ventral aspect of the stomach halfway between the greater and lesser curvature in an area where there is decreased vasculature. This is where the terminal arterial branches of the gastric arteries (from the lesser curvature) and gastroepiploic arteries (from the greater curvature) are located and is readily identified in ferrets. The stay sutures are placed at the edges of the beginning and ending of the proposed gastrotomy incision. The length of the incision is appropriate for the size of the foreign material that is to be removed. Sutures are placed into the holding layer of the submucosa or are placed full thickness. The stay sutures are tensioned in a ventral direction, pulling the ventral wall of the stomach away from the dorsal wall. A full gastrotomy incision is initiated with a number 11 blade. Tension is maintained on the stay sutures as a full thickness stab incision is made into the stomach along the proposed incision site. The incision is then extended parallel to the curvature of the body of the stomach with a blade or fine pair of Metzenbaum scissors. Before closing, it is recommended in ferrets to obtain a full thickness tissue sample of gastric mucosa for assessment of potential concurrent Helicobactermustelae infection. This sample is obtained with a blade or scissors from either of the margins of the incision. Closure is performed in two layers. The submucosa is the holding layer and it is closed first in conjunction with the mucosa. This is performed using a fine (4-0 or 5-0) monofilament, absorbable, synthetic suture swaged on to a taper needle in a simple continuous pattern. The second layer is performed within the seromuscular layer or through all four layers and is placed using a continuous inverting pattern (Lembert or Cushing). The closed gastrotomy incision is cleaned with sterile saline and the stay sutures are removed.
Enterotomy
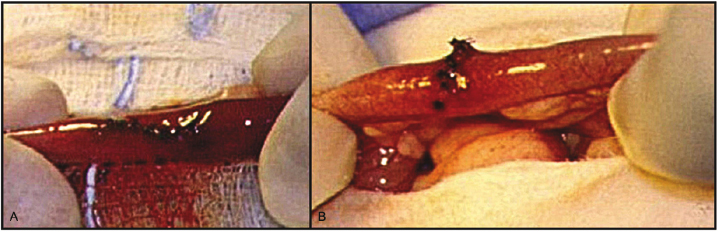
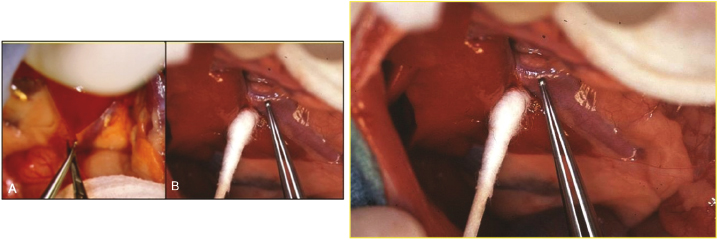
The preparation for an enterotomy in a ferret is similar to that of other species. The small intestine of ferrets is subjectively narrow for their body size, which may make them prone to iatrogenic stricture after routine enterotomy closure. A longitudinal incision is made in the small intestine when performing an enterotomy or biopsy, but in cases where the lumen appears narrow, the incision is closed in transverse manner, which increases luminal diameter at the location of the incision (Fig. 13.5).
Fig. 13.5. Intraoperative image of an enterotomy in a ferret created for procurement of a full thickness biopsy. Note the longitudinal incision (A) and transverse closure with simple interrupted sutures (B).
Intestinal Biopsy
Full thickness intestinal biopsy is performed by isolating the segment of small intestine to be biopsied with moistened sponges or gauze squares. The biopsy is performed by inserting a number 11 blade into the lumen of the small intestine at the antimesenteric border and extending the length of the incision in a longitudinal direction for a few millimeters. It is common for the biopsy site to resemble an elliptical defect in the antimesenteric border. An ellipse allows for a cleaner apposition of tissue planes and, in this case, is defined as having a length to width ratio of 4 : 1.
Small Intestine Resection and Anastomosis
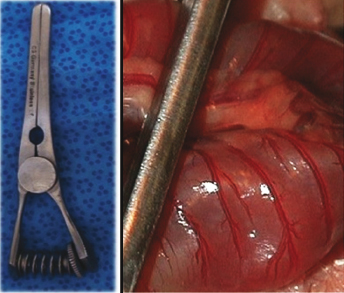
Intestinal resection and anastomosis in ferrets is rarely indicated and reserved for patients with devitalized or perforated bowel secondary to a foreign body obstruction or small intestinal neoplasia. Principles and techniques for small intestinal resection and anastomosis in ferrets are identical to that of other species and descriptions can be found in many veterinary references. Pediatric Doyen intestinal forceps or sterile bobby pins can be used to prevent spillage of intestinal contents into the abdomen during intestinal surgery [11,25,28]. The author prefers the use of Bulldog vascular clamps for temporary and nontraumatic occlusion of the small intestine of small mammals (Fig. 13.6).
Fig. 13.6. Bulldog vascular clamp. This is a mildly traumatic clamp useful for preventing spillage of intestinal contents during intestinal resection and anastomosis.
In general, ferrets have an excellent prognosis after surgery for foreign body removal as long as a perforation and septic peritonitis are not present. Intestinal necrosis or perforation seem to occur less frequently in ferrets compared with dogs and cats with foreign body obstruction [10]. Preventing foreign body ingestion can be difficult in ferrets. Usually by 2 years of age, ferrets less frequently ingest foreign bodies. The routine use of GI lubricants to prevent trichobezoars is helpful.
Hepatobiliary Surgery
Indications for surgery of the liver and biliary tract include mass removal, biopsy and tissue culture procurement, cholelithiasis, cholecystitis, and other diseases of the gallbladder.
Liver Biopsy
The most common indications for liver biopsy are to confirm the underlying disease associated with a chronic liver enzymopathy, hepatic lipidosis, infectious and inflammatory liver diseases, and neoplasia. Techniques described for other species including guillotine and punch biopsy are often utilized in ferrets [11,25,28]. The guillotine method is used when diffuse disease is expected and all liver lobes appear grossly similar. A preformed encircling loop of 4-0 monofilament, absorbable suture material is placed around a readily available marginal segment of liver. The suture is tightened until it has crushed through the capsule of the liver and softer parenchyma. Several throws are placed to complete the knot and the sample is excised 1–2 mm distal to the ligature [11]. For a punch biopsy, a 4–6-mm punch biopsy instrument is used and an absorbable hemostatic agent is used to plug the biopsy hole. Two to three biopsies are collected from various liver lobes when diffuse disease is present. If infectious disease is suspected, tissue samples are also submitted for aerobic and anaerobic culture.
Liver Lobectomy
Indications and techniques for partial and complete liver lobectomy in ferrets are similar to those described for dogs and cats [25,28]. The use of stapling devices (TA stapler, Covidien, Mansfield, MA) makes partial and complete liver lobectomy a safer and faster procedure.
Cholecystecomy
Surgical diseases of the gallbladder of the ferret are not common; however, cholecystotomy and cholecystecomy are the most common extrahepatic biliary tract (EHBT) surgeries performed. A cholecystotomy can be performed in ferrets for removal of choleliths. However, since the gallbladder is the source of the stones, a cholecystectomy is recommended to prevent recurrence of cholelithiasis. A cholecystectomy is performed in ferrets for cholelithiasis, cholecystitis, gallbladder rupture secondary to trauma, and neoplasia. The anatomy of the ferret EHBT is similar to that of cats and humans. The terminal bile duct fuses with the terminal segment of the main pancreatic duct at the major duodenal papilla [12]. Techniques for cholecystectomy have been described for ferrets and are similar to those reported for other species [11,25,28]. Before removing the gallbladder, the surgeon should assess the bile duct to be certain there is no obstruction. An irresolvable obstruction of the common bile duct would preclude a cholecystectomy, and a cholecystoenterostomy might have to be performed in such cases. Before removing the gallbladder, the extrahepatic bile ducts must be externally palpated and internally flushed with saline to assure the patency of the system. This can be accomplished by either antegrade or retrograde access and flushing. An antegrade approach is performed by utilizing a cholecystotomy incision that has been made to evacuate the sludge from the gallbladder. A 3.5- or 5-Fr catheter is advanced from a cholecystotomy into the cystic duct and the bile duct. The duct is then flushed with sterile saline. Patency is assessed by direct visualization of saline at the major duodenal papilla or by palpating the flow of lavage solution entering the proximal duodenum. A second method of confirming a patent extrahepatic duct system is by retrograde catheterization. The major duodenal papilla is identified by making a duodenotomy over the papilla at the antimesenteric surface of the proximal descending duodenum. Once the papilla is identified, a red rubber catheter is introduced and a gentle flush with sterile saline is performed. Because the EHBT is a closed system, when flushing retrogradely, it is possible to exert enough force that sludge or concretions may enter the hepatic ducts or intrahepatic biliary system. One method to avoid this is to complete the cholecystectomy after assuring that the bile duct is patent and leave the transected cystic duct open as described for antegrade flushing. The sludge will come through the open cystic duct instead of being pushed into the hepatic ducts. Some surgeons have also recommended using a red rubber catheter that is half or less the diameter of the major duodenal papilla so that retrograde flushing against a closed EHBT will allow excess saline to leak out around the catheter at the papilla. The catheter is inserted retrogradely through the major duodenal papilla to the level of the cystic duct. This is performed with great care as iatrogenic rupture of the bile duct may occur. With this retrograde technique, the seal of the cystic duct can be tested after closure of the cystic duct.
The cystic artery is double ligated. Biliary sludge within the cystic duct is milked into the gallbladder and vascular clips or encircling sutures are used to close off the cystic duct. The cystic duct is then transected between the two sutures or clips. The cystic duct remnant is inspected, and if the duct appears friable, a distally placed transfixation suture or an oversew of the duct is required. After completion of ligation of the cystic duct, gentle lavage with a retrograde catheter allows testing of the security of the ligatures on the cystic duct remnant, as well as permitting evacuation of the extrahepatic bile ducts.
Urogenital
Nephrectomy
Removal of the kidney is indicated in cases of severe and unresolved pyelonephritis and hydronephrosis, as well as cases of primary renal or ureteral neoplasia. In ferrets, the retroperitoneum often contains large amounts of adipose tissue that impedes good visualization of the kidney and its associated vasculature. The peritoneum overlying the kidney is gently grasped and elevated from the kidney and incised with a blade or sharp scissor. Once the retroperitoneum is opened, CTAs are used to dissect fat off of the kidney and from the area immediately lateral and dorsal to the kidney. It is much easier to visualize the renal artery, vein, and ureter from the dorsal aspect of the kidney than from the ventral. Blunt dissection is continued laterally, cranially, and caudally until the kidney is freed from the retroperitoneal space. With gentle elevation of the kidney medially and ventrally, the renal hilus is identified. The renal artery and vein are individually isolated and ligated close to the descending aorta and caudal vena cava using clips or ligatures. The artery and vein should be double ligated. Once the renal artery and vein are ligated and transected, the ureter is gently exteriorized from the retroperitoneal space and a clip or encircling suture is placed at the junction of the ureter with the bladder neck, and the distal ureter is transected. Leaving the ureter intact can predispose to vesicoureteral reflux and recurrent lower urinary tract infections.
Urolithiasis
Urolithiasis in ferrets can be characterized by solitary or multiple renal or cystic calculi or by the presence of sandy material in the urinary bladder and urethra [29,30]. Clinically, obstructive urolithiasis appears to be decreasing in frequency in ferrets [10].Obstructive urolithiasis is more common in male ferrets than in female ferrets due to the narrow diameter of the urethra as it passes through the os penis in males. Historically, the most common type of stone identified in ferrets has been magnesium ammonium phosphate (struvite), but other stone types have been identified [29].Although not studied as extensively as in dogs and cats, the pathogenesis of struvite urolithiasis in ferrets is probably related to diet [29]. Ferrets are carnivores with an approximate normal urine pH of 6.0, and struvite can crystallize when the urine pH rises above 6.4. Although the mineral content of the food was once thought to be the cause of urolithiasis in ferrets, it is now thought to be caused by ingestion of plant proteins [29] in poor quality dog and cat diets that contained a high percentage of plant-based protein. The metabolism of organic acids in plant protein produces an alkaline urine that results in the formation of struvite crystals, as demonstrated in a group of pregnant jills fed a diet high in plant protein (mainly corn), and in a group of ferrets fed a commercial dog food [31,32]. In recent years, many commercial ferret diets have become available and ferrets are no longer commonly fed dog and cat foods with plant proteins.
The systemic effects of obstructive urolithiasis in ferrets are the same as those in dogs and cats and include dysuria, hematuria, stranguria, frequent licking of the perineum, and urine dribbling. The presence of lower urinary tract signs and palpation of a firm, distended, unexpressable urinary bladder confirms the diagnosis. Obstructive urolithiasis can be identified with abdominal radiographs because struvite stones are radioopaque; sand however, is not always visible radiographically. Abdominal ultrasound is often useful, as the fine sand-like crystals are easily identified. It is also helpful in identifying radiolucent urinary calculi or other causes of obstructive urolithiasis (e.g., prostate disease secondary to adrenal neoplasia). Serum chemistry and hematologic profiles should be performed to determine the existence of concurrent disease and to evaluate the extent of azotemia and electrolyte abnormalities.
If severe cardiac arrhythmias and electrolyte abnormalities are present, they are treated before attempting to relieve urethral obstruction. Once intravenous fluids and supportive care have been initiated, the urethra should be unblocked. The treatment of obstructive urolithiasis is male ferrets can be challenging because of the distinctive anatomy of the distal urethra and meatus in males. Males have an operculum covering the distal urethra and a hook directed dorsally at the tip of the os penis, making it difficult to identify the urethral opening. A technique for urinary catheterization in ferrets has been described, and the use of a Slippery Sam (Slippery Sam Tomcat Urethral Catheter, Smiths Medical, Dublin, OH) is preferred for retrograde catheterization in male ferrets [33]. Fluids should be administered for diuresis and the catheter left in place until the ferret is stable enough for definitive surgery, if indicated. If the distal urethra cannot be cleared of stones or if the ferret has recurrence of obstruction, a perineal urethrostomy (PU) may be indicated.
If a urethral catheter cannot be passed, cystocentesis will provide temporary decompression. An emergency cystotomy or percutaneous tube cystostomy can be performed if the ferret is stable [10]. Many ferrets with obstructive urolithiasis can be managed with cystotomy and anterograde flushing of the urethra. A PU can be performed in ferrets, as is done in cats, if the ferret cannot be catheterized.
Cystotomy
If the stone(s) can be flushed retrograde into the urinary bladder, a ventral cystotomy is preferred over a dorsal cystotomy so that the ureters are not damaged during entry into the bladder or during closure of the cystotomy incision. The technique for ventral cystotomy in ferrets is identical to that described for dogs and cats, but a 4-0 to 5-0 monofilament and absorbable suture material is required for closure, using a single layer, simple interrupted, or simple continuous closure [11,34].
Perineal Urethrostomy
If the stone is lodged in the postpubic urethra, a PU is performed. The anatomy of a ferret penis is similar to that of a dog [35]. The penis exits the pelvic canal, runs subcutaneously along the ventral pelvis, and lies along the caudal ventral abdominal body wall [35]. The opening of the prepuce is just caudal to the umbilicus. Given that the ferret os penis terminates just caudal to the caudal ischium, the PU site should be between the cranial portion of the os penis and the caudal border of the ischium. The stoma should be perineal and not ventral to avoid trauma to the site during normal ambulation. The ferret is placed in a perineal stand and a 1-cm incision through the skin and urethra is made 1 cm ventral to the anus. It is important to avoid the cavernosus tissue on each side of the urethra, as it will bleed extensively if incised [35,36]. The penis is not resected as is done in cats because of the cranial and ventral location of the penis in ferrets. A 3.5–5.0-Fr red rubber catheter is then placed in the proximal urethrostomy site to assess the patency and diameter of the urethra. A fine (6-0 to 8-0), synthetic, and monofilament suture is used to appose the mucosa of the urethra to the skin. The urethral drain board should be at least 1 cm in length. This technique works well in ferrets and is well tolerated long term.
If the ferret is on an inappropriate diet, it should be changed to a commercial ferret diet with no plant protein source. The ferret should be monitored for recurrent urolithiasis every 3–6 months with a urinalysis and abdominal radiographs or focal abdominal ultrasound. The prognosis is good for ferrets with obstructive urolithiasis if there is no evidence of permanent renal damage secondary to obstruction. Recurrence of cystic calculi is uncommon when appropriate dietary changes are made.
Sterilization
Sterilization is often performed at a young age in domestic ferrets in the United States. This practice may be a contributing cause of the high incidence of sex steroid hormone disorders in this species. Alternatives to ovariectomy and castration are available and are recommended by some veterinarians. See Chapter 17 for more information.
Ovariohysterectomy
Ovariohysterectomy is not a commonly performed procedure in veterinary practice because most pet ferrets are spayed at breeding farms before they are adopted. Female ferrets are induced ovulators, and without proper stimulation for ovulation, develop estrogen-induced pancytopenia [13,30].
Ovariohysterectomy is performed through a ventral midline incision initiated 0.5–1.5 cm caudal to the umbilicus. The uterus of ferrets is bicornuate and located immediately dorsal to the urinary bladder. The ovaries and ovarian vasculature are located in the adipose-filled retroperitoneal space and are immediately caudal to the caudal pole of the kidney. The technique for ovariohysterectomy is identical to that performed in the cat.
Ovariectomy/Ovarian Remnant Removal
Removal of the ovaries without removal of the uterine horns or uterus is a common practice in cats and dogs. This is justified because all of the uterine diseases in these species are hormone related, including most uterine tumors. Although similar uterine tumors (leiomyoma and fibroma) are reported in ferrets, it is unknown if these are related to the presence of estrogen. However, given the high incidence of sex steroid hormone production in adrenal endocrinopathy of ferrets, removal of the entire reproductive tract is recommended at the time of surgical sterilization.
In a female ferret with a history of ovariohysterectomy, signs of estrus are often related to the presence of adrenal production of sex steroids. There are few instances when the signs of estrus are actually caused by a remnant of ovary left behind from the time of ovariohysterectomy. Signs of estrus caused by an ovarian remnant in an ovariohysterectomized jill, though reported, are uncommon [37]. It is always important when performing an abdominal exploratory in a female ferret to evaluate the retroperitoneal space caudal to the kidneys to be certain there is no ovarian tissue present. Laparoscopy is being used in ferrets for ovariectomy, ovariohysterectomy, and for the exploration of the retroperitoneum for evidence of residual ovarian tissue. The benefit of laparoscopy is a minimally invasive approach with intense illumination and magnification of abdominal viscera [38].
Castration
It is recommended that male ferrets be castrated by 6 months of age to reduce aggression, odor, and prevent the occurrence of prostatic disease and testicular neoplasia [11,30].Castration in ferrets can be performed from a prescrotal incision with 3-0 or 4-0 encircling ligatures, as is described in dogs, or through a scrotal approach with an autoligation or self-tie technique, as is described in cats. The castration can be performed as open or closed.
Surgical Disease of the Prostate
Many male ferrets with adrenal disease (see later) will have secondary changes to the epithelium of the prostate due to chronic stimulation by androgens and estrogens. This can lead to prostatic hyperplasia, prostatic cyst, and prostatic abscess formation. The prostate is not grossly visible in a castrated, healthy, adult male ferret. If paraurethral or prostatic cysts or abscesses are present, they are surgically addressed in a routine manner with a partial prostatic resection and prostatic omentalization. The contents of the cyst are aspirated intraoperatively and submitted for culture and sensitivity [39]. A portion of the cyst is resected and the omentum is tunneled through the cranial and ventral portion of the prostate and tacked to itself with a stay suture (Fig. 13.7) [10]. Care should be taken not to damage any of the nerves associated with the dorsal prostate. It is important to make sure to determine that the urethra is not leaking. If it is damaged and leaking, uroabdomen will result. If there is leakage, a urethral catheter is left in place for 2–3 days to allow the urethra to heal. Prostatic omentalization is preferred over marsupialization because the latter exposes the peritoneal and retroperitoneal cavity to the environment and increases the risk of septic peritonitis. After complete removal of the adrenal neoplasia, cystic structures regress rapidly. If the ferret presented with a urinary obstruction from prostatic disease, a urinary catheter should be left in place for several days to help assure normal micturition.
Fig. 13.7. Intraoperative picture of the caudal abdomen of a ferret undergoing left adrenalectomy and partial prostatectomy with omentalization for a prostatic abscess. Note the greater omentum sutured to the capsule of the ventral prostate for adequate fixation. Omentalization of the debrided prostate will assist in healing, drainage, and bring a healthy blood supply to the diseased tissue.
Anal Sacculectomy
Ferret anal glands are located lateral to the anus at the 3 and 9 o'clock positions. When the animal is frightened or excited, the glands excrete a musk substance with a strong, noxious odor. The glands are usually removed when the animal is spayed or castrated; consequently, many suppliers remove these glands quite early in life. Some commentators are opposed to the removal of the glands and believe that it deprives the animals of a defensive mechanism (Cooper [40]). Most veterinarians agree that castration or suppression of sex steroid hormones suppress almost all odor-rendering scent gland removal unnecessary. A surgical procedure which is a modification of the procedure to remove canine anal sacs has been described and is summarized below (Creed and Kainer [41]).
A binocular loop magnifier helps to locate the minute end of each anal sac. The duct is grasped with a mosquito forceps, taking care to include only a minimal amount of skin and mucous membrane. A circumferential skin incision is made with a number 15 scalpel blade immediately distal to the tip of the forceps. The skin and mucosa are reflected off the duct with gentle scraping. The glandular complex surrounding the duct for 3–4 mm makes dissection difficult. Dissection should be fairly superficial with respect to the overlying tissue and, as the dissection proceeds beyond the glandular complex, a fascial plane is encountered. The anal sac can be removed readily by continuing to use a scraping action with the scalpel blade. Staying on the proper fascial plan will not only enhance removal of the anal sac, but will also minimize hemorrhage and damage to the internal and external anal sphincter muscles. The entire sebaceous component of the glandular complex is removed during surgery, but most of the apocrine component is either destroyed by the dissection or remains, with the contiguous external and internal sphincter muscles. Sutures are not required, and infusion of antimicrobial medications into the defect is unnecessary. Ferrets recover easily from this procedure and heal remarkably well. Analgesics should be used.
Surgery of the Endocrine System
Insulinoma
The most commonly reported tumors in ferrets are endocrine tumors, with an incidence of 39.7–53% [5,14,42]. Pancreatic beta cell tumors or insulinomas are the most common endocrine tumors and adrenal tumors are the second most common [5,14,42].Pancreatic beta cell tumors have a reported incidence of 21.7–25% [14,15,23,42–46].The median age of ferrets with insulinomas is 5 years (range 2–7 years), with males being diagnosed more frequently than females [16,42,47].
There are four types of islet cells; beta cells (insulin secretion), alpha cells (glucagon secretion), delta cells (somatostatin secretion), and F cells (pancreatic polypeptide secretion) [48–50]. Islet cell tumors in ferrets arise from the beta cells and produce insulin, which, when present in excess amounts, lead to hypoglycemia [7,14,39,48,51].Functional insulin-secreting conditions in ferrets include pancreatic islet hyperplasia, adenoma, and adenocarcinoma [14,42,47,52]. Neuroglucopenic signs occur because cells in the central nervous system have a higher metabolic rate and glucose is their primary energy source [48,53]. Prolonged and severe hypoglycemia can cause brain damage and a clinical presentation of neurologic dysfunction [48,51,53,54].
Clinical signs of insulinoma may not be apparent and the tumor is sometimes diagnosed on biochemical examination during health screen or at exploratory laparotomy for another reason. Clinical signs are related to the systemic effects of hypoglycemia, the rate of decline of the blood glucose concentration, and the duration and degree of hypoglycemia [48]. Clinical signs in ferrets with hypoglycemia include hind limb ataxia, paresis or paralysis, seizures, weight loss, ptyalism, gagging, vomiting, and pawing at the mouth [14,42–44,47,52,55,56].Pawing at the mouth is thought to be associated with nausea, but may lead owners and clinicians to believe that there is a foreign object in the mouth or throat [7,8].Owners may report a prolonged, waxing and waning history of lethargy and episodes of collapse. They often describe the ferret as having a glazed-eye appearance [48]. Physical examination of ferrets with an insulinoma may be unremarkable as the hypoglycemia can be episodic.
The reference range for resting blood glucose concentration in ferrets is 94–207 mg/dL and normal fasting blood glucose levels are 90–125 mg/dL [48]. Insulin levels can be run concurrently but will only be diagnostic if the patient is hypoglycemic at the time of sampling [48,57,58].If serum glucose levels are normal and a high clinical suspicion for insulinoma exists, a controlled fast can be performed for no more than 4 hours to better establish hypoglycemia but is not recommended by the author. If a controlled fast is performed, it is best to fast the ferret in the hospital in case a hypoglycemic crisis occurs. Because ferrets have a rapid GI transit time (3–4 hours), a shorter fast than in dogs and cats is diagnostic. A 4-hour fasting glucose concentration less than 60 mg/dL is consistent with a pancreatic islet cell tumor in a ferret [39,52,58]. Typically, abdominal radiography and ultrasonography are not helpful in detecting these masses as they are usually only millimeters in diameter [7,48].
Treatment is aimed at increasing blood glucose levels by both medical and surgical means. It is common (>50% of surgical cases) that after surgical excision, medical management is still indicated [47]. Only 14–15% of ferrets with insulinoma are cured long term with surgery [42,47,48,59]. This may be due to the high recurrence rate or micrometastatic rate of ferret insulinoma to other regions of the pancreas, regional lymph node, spleen, or liver; however, some have found the metastatic potential to be low [47,56].
Surgical excision is the treatment of choice for ferrets under 6 years of age or for those suspected of having concurrent adrenal disease [48]. Surgery is indicated for confirmation of insulinoma, decreasing the tumor burden, and to better evaluate metastatic and concurrent disease [58].Use a ventral midline celiotomy for exploratory biopsies of abnormal structures and inspection of the entire pancreas. Both limbs of the pancreas should be gently and thoroughly palpated both ventrally and dorsally for small nodules. Pancreatic tumors are usually firm and have an increased vascular supply. It is common to find multiple nodules within the pancreas at surgery [44,47]. If there is one or only a few visible nodules, nodulectomies are performed. If several nodules are present in one portion of the pancreas, a partial pancreatectomy is recommended. If no nodules or masses are found, a left and right partial pancreatectomy is performed to debulk the pancreas and get a diagnosis. Removal of the left lobe of the pancreas is technically less challenging than removal of the right lobe because of the close proximity of the right lobe to the pancreatic ducts, duodenum, and adjacent blood vessels [52,60];however, removal of the most distal portion of the right limb is readily performed in most cases.
Removal of a part of the right or left limb of the pancreas is performed with the use of a pediatric right angle forcep, hemoclips, and CTAs. The distal tip of the limb is identified and blunt dissection is used to free the limb of the pancreas from its surroundings. It is important to stay close to the pancreas and use hemoclips when vessels are encountered. The further dissection occurs from the pancreas, the more likely damage will occur to vessels supplying the duodenum and remaining right pancreatic limb (right limb dissection) or to the vasculature of the spleen (left limb dissection). It is often possible to isolate 1–2 cm of pancreas from each of the distal limbs with careful dissection. Using a single encircling suture of 3-0 monofilament suture, the distal pancreatic limb is ligated and transected. Partial left and right limb resection is an acceptable technique in ferrets in which an insulinoma is highly suspected, but a gross primary mass is not visualized. This technique debulks total functional endocrine pancreatic mass and the removed segments may contain the insulinoma. All resected tissue is submitted for histopathology.
Medical management is aimed at increasing blood glucose levels and can be used concurrently with surgery or as the sole modality for treatment. Ferrets with insulinomas managed medically without surgery have a shorter survival than those treated with combined surgical and medical management [47]. Medical management of these tumors is discussed in Chapter 17.
The prognosis for ferrets with insulinomas is generally better than for that of dogs with insulinomas [42,43,52,55–57].Young ferrets without metastatic disease that are diagnosed early in the disease process have the best prognosis [58]. With partial pancreatectomy, mean survival time is 668 days, and multiple surgeries are sometimes needed to achieve longer survival times [7,42].The duration of clinical signs before diagnosis may negatively affect survival time and disease-free interval after surgery [44].No difference in survival time has been identified between ferrets with benign versus metastatic disease [43,47].
Adrenal Disease
Adrenocortical cell tumors are the second most common tumors in ferrets [3,14–17,61–64]. The occurrence of hyperadrenocorticism in domestic ferrets in the United States may be as high as 25% of all ferrets [3,14,65].The first report of hyperadrenocorticism in a domestic ferret was in 1987 [66]. Since then, several reports identifying the hormones elevated in ferret hyperadrenocorticism and the pathophysiology of the disease have been published [3,61,62,67]. The mean age of affected ferrets is 3.4–4.8 years,with females having a predilection for the disease [3,17,63]. One study refutes this finding [65].
These are adrenal cortical reticularis tumors, which produce excessive levels of androgenic hormone precursor and estrogenic hormones. Increases in serum cortisol levels are typically not a feature of this disease in ferrets, nor is primary pituitary disease likely [7,48,58,63,68–70].The tumors, histologically, are characterized as adrenal cortical hyperplasia, adenomas, or adenocarcinomas, and it is possible that this is a continuum of a disease process [3,71]. The clinical signs and prognosis are the same regardless of the histopathologic diagnosis [2,3,7,17,65].Adrenocortical spindle-cell tumors and pheochromocytomas have also been reported alone and concurrently with functional adrenocortical cell neoplasms in ferrets [16,17,48,51,72]. The incidence of adrenal disease in ferrets in Europe and Australia appears to be much lower than in the United States. It has been speculated that adrenal gland hyperplasia and tumor development are due to the early neutering of ferrets (see Chapter 17) [58,73,74]. This has been shown to occur in mice [73]. Other suggested causes include feeding a commercial brand ferret food (instead of whole prey items), inbreeding, and the lack of a natural light cycle for ferrets in the United States [48].
Clinical signs in ferrets with functional adrenocortical tumors are primarily due to the hypersecretion of estrogenic and other steroid hormones by tumor cells [51]. Clinical signs are variable in affected animals and may include a bilaterally symmetrical endocrine alopecia, which may be seasonal, pruritis (sometimes the only clinical sign), vulvar enlargement in females, prostatic enlargement in males, aggressive sexual behavior, comedones on the tail, and mammary gland enlargement [3,39,48,59,61,65,67,75].Males with prostatic disease secondary to hyperadrenocorticism may present with urinary incontinence, stranguria, and dyschezia. Prostatic abscessation, paraurethral cysts, and urinary obstruction can also accompany the disease in males. Large tumors can be palpated in the cranial abdomen.
Hyperadrenocorticism in ferrets is diagnosed based on a combination of clinical signs, abdominal ultrasound, and plasma concentrations of estrogens and androgens [48,62,63,68,69].Serum chemistry and hematologic profiles are usually normal, except for the occasional thrombocytopenia and anemia, thought to occur due to estrogen-induced bone marrow suppression [3].In ferrets with anemia and pancytopenia, a packed cell volume less than 15% is associated with a grave prognosis [48]. A serum endocrine panel has been established and is commercially available at the Clinical Endocrinology Laboratory, University of Tennessee College of Veterinary Medicine. The assay measures levels of 17-hydroxyprogesterone, androstenedione, and estradiol. An elevation of any one of these hormones is considered diagnostic for hyperadrenocorticism in ferrets [48,54,61,62].Elevations in dehydroepiandrosterone may also be detected in ferrets with adrenal disease [68]. Urine cortisol : creatine ratios are not useful in diagnosing hyperadrenocorticism in ferrets because serum cortisol is not elevated in these patients [3,69], although one study disagrees with this [63].
History and physical examination appear to be the most useful in diagnosing the disease. Abdominal radiographs are usually unremarkable unless the mass is large or the affected gland is mineralized [3]. Adrenal lesions are the most commonly found ultrasonographic abnormalities in ferrets [7,76,77]. Ultrasound has been reported to have an 84% sensitivity for detecting adrenal disease in ferrets, with histopathology being the gold standard [71].Ultrasound findings in ferrets with hyperadrenocorticism may also include a prominent uterus or uterine stump, or a prominent prostate with or without prostatic cysts [71]. The author has also observed ultrasonographic evidence of urinary tract dilation (urethra, bladder, and ureters) due to an enlarged prostate obstructing the prostatic urethra. More recently, the use of nonselective angiography, computerized tomography (CT) angiography, and magnetic resonance imaging (MRI) in ferrets with adrenal disease have helped guide strategy for surgery in ferrets with large tumors, bilateral disease, or tumors involving the renal veins and caudal vena cava. These advanced imaging modalities are routinely used in dogs and cats with adrenal disease and should be utilized whenever possible in ferrets.
Currently, medical management of adrenal disease in ferrets is focused on controlling abnormal hormone levels and their effects and is discussed in more detail in Chapter 17. Medical management of adrenal tumors may control the clinical signs but there is no evidence to suggest that the described therapies inhibit or reverse the growth of an adrenal-based tumor.
A ventral midline celiotomy is recommended for exploration of the abdomen, removal of one or both of the adrenal glands, biopsies of abnormal viscera, as well as inspection of the pancreas and prostate or uterine stump [27,36,39,78,79]. A lateral approach has also been described for unilateral adrenalectomy in ferrets, but does not allow for a complete exploratory laparotomy [80]. In 85% of ferrets with hyperadrenocorticism, one adrenal gland is enlarged and the other is small to normal. In the remaining 15% of the cases, bilateral adrenal enlargement is identified [3,65].In the cases of unilateral enlargement, disease may occur in the contralateral gland after the affected adrenal is removed [65]. In some cases, both adrenal glands will appear grossly normal and direct visualization of the entire gland via careful dissection of surrounding retroperitoneal fat is necessary. Historically, the recommended surgical treatment for bilateral adrenal disease in ferrets has been total adrenalectomy of the one side and partial resection of the contralateral side [68,81].This will ultimately lead to recurrence of the disease as the remaining adrenal tissue proliferates and it may not even temporarily relieve clinical signs. Partial ablation of a carcinoma is not recommended, and when performed, may be the source for ectopic or residual adrenal tissue and tumors of the omentum and falciform fat months to years after the initial surgery.
The anatomy, location, and associated vasculature of the adrenal glands are similar to those of dogs and cats. The left adrenal is relatively easy to remove, in most cases, even if enlarged. As in other mammals, the left phrenicoabdominal vein, which drains the adrenal gland, frequently empties into the caudal vena cava; however, in some cases it drains directly into the left renal vein. Left-sided adrenal tumors can invade the phrenicoabdominal vein and, subsequently, the left renal vein. This requires careful removal of the tumor or tumor thrombus from the vasculature or removal of the left kidney. Iatrogenic trauma to the left renal vein leads to destruction of the left kidney and necessitates nephrectomy. If the left renal vein is accidently ligated or clipped during left adrenalectomy, the left kidney will become engorged and the capsular veins will become increasingly prominent. The right adrenal gland is closely associated with the caudal vena cava and the tumor can surround or invade the vessel, leading to life-threatening complications [35,80]. For removal of either adrenal, the peritoneal lining covering the gland must be carefully opened with a combination of blunt dissection using CTA and a pediatric right-angle forcep (Fig. 13.8), and sharp cutting with a fine pair of scissors. Once the retroperitoneum is exposed, gentle dissection of the fat surrounding the adrenal gland is required to identify the entire extent of the gland and its associated vasculature. This is performed with the use of CTAs and a pediatric right-angle or Mixter forcep (Fig. 13.8). The phrenicoabdominal vein courses dorsal to or ventral to the adrenal gland from a lateral to medial direction, requiring ligation of the vein in two locations; one lateral to the gland and the other between the gland and the caudal vena cava. The use of a right-angle clip applier simplifies the ligation of these vessels. After the phrenicoabdominal vein is ligated, the remainder of the smaller arteries and veins are ligated using a combination of monopolar or bipolar electro or radiosurgery clips and suture. Dissection begins laterally and dorsally and continues cranially and caudally until the last portion to be dissected is medial and dorsal, nearest the termination of the venous drainage into the caudal vena cava. This method of removal allows for the best visualization of the adrenal gland attachments to the caudal vena cava and simplifies identification of the left renal vein and artery to ensure that they are protected during adrenalectomy. In general, right adrenalectomy is more challenging because of its cranial and medial location. A few simple steps are followed to facilitate its removal. Before entering the retroperitoneal space, it is important to identify and isolate the hepatorenal ligament. This structure usually connects the caudate lobe of the liver to the cranial aspect of the right kidney, tethering the lobe and obscuring visualization of the right adrenal gland. Once identified, this ligament is transected with scissors, allowing for safe retraction of the caudate lobe of the liver in a cranial and lateral direction. This exposes the right cranial and medial compartment of the abdomen where the right adrenal gland is located. It is also important to understand the anatomy and location of the right adrenal gland. The gland is often located dorsal to the caudal vena cava on midline or to the immediate right of midline. The caudal vena cava is not a fixed structure in the abdomen, meaning, it is readily moved to the left or right of the midline with gentle manipulation. Taking advantage of these facts allows the surgeon to approach the right adrenal gland from both the left and ride side of the caudal vena cava, making dissection simpler, safer, and complete (Fig. 13.9).
Fig. 13.8. (A) Right-angle or Mixter forcep frequently used for blunt dissection of adrenal tumors, pancreatic tumors, and large blood vessels. (B) Right angle clip applier, frequently used for ferret adrenalectomy, pancreatic mass resection, and nephrectomy. (C) Pediatric Satinsky vascular clamp, a necessity for partial caudal vena caval wall resection for invasive right-sided adrenal tumors. The clamp is applied such that the tumor and cava wall can be transected but blood flow through the vena cava is preserved. (D) A diagram demonstrating the appropriate use of a pediatric Satinsky clamp for partial resection of the wall of the caudal vena cava.Fig. 13.9. (A) The hepatorenal ligament is being grasped with thumb forceps prior to transection. This structure usually connects the caudate lobe of the liver to the cranial aspect of the right kidney tethering the lobe and obscuring visualization of the right adrenal gland. This ligament is transected prior to opening of the retroperitoneal space and identification of the right adrenal gland. (B) Using a CTA, the caudal vena cava is being rolled to the right of midline, exposing the right adrenal gland on the left side of midline.
Resection and closure of a section of the wall of the caudal vena cava may need to be performed if the tumor invades the vessel. After dissection and ligation of the vessels cranial, caudal, lateral, and dorsal as described earlier, the medial attachments of the adrenal tumor to the cava wall are identified. If the tumor has invaded the cava wall but no significant intraluminal tumor or tumor thrombus is identified, a partial resection of the caudal vena cava wall can be safely removed and closed. A pediatric Satinsky vascular clamp (RICA Surgical) is applied to the cava wall. The flat portion of the clamp (Fig. 13.8) is parallel with the long axis of the cava so that the angled tip of the free end of the clamp and the angled shaft end are occluding about 50% of the cava diameter. This application of the clamp allows for continued blood flow through the vena cava but will allow for resection of the affected portion of the vessel wall without any hemorrhage. The diseased vessel wall and tumor are sharply transected leaving a 1–2-mm margin of tissue exposed within the concave surface of the clamp. This lip of tissue is sutured with a 6-0 to 8-0 monofilament suture material on a tapered needle in a simple continuous pattern (Fig. 13.8A). It is extremely important not to use a cutting or reverse cutting needle for suturing the vena cava wall. The clamp is slowly removed, and if significant hemorrhage occurs, the clamp is reapplied and the suture line is reinforced. If mild hemorrhage or oozing is present, a gelatin sponge or regenerated cellulose hemostatic agent is applied to the suture line prior to closing the abdomen.
Ligation and resection of the affected portion of the caudal vena cava, proximal to the renal veins and immediately distal to the liver to achieve complete surgical removal of the affected adrenal gland, has been described [81]. This technique should only be performed if no other surgical option exists. If the caudal vena cava is ligated distal to the renal veins, acute renal failure will ensue. Data from human and canine studies extrapolated to ferrets assumed 75% mortality in acute caudal vena cava ligation; however, ferrets appear to have extremely well-developed collateral venous drainage pathways that may allow for acute ligation with a much lower mortality rate. In a study using normal ferrets, the caudal vena cava was temporarily occluded with a balloon catheter cranial to the right renal vein. Caudal vena cava pressures were recorded before and after occlusion [82]. All eight ferrets survived the temporary occlusion, but two developed severe elevations in caudal caval pressures while the balloon was inflated. All of the ferrets had immediate collateral venous drainage to the vertebral sinuses and the cause of the pressure increase was not determined.
Collateral venous drainage in mammals occurs through the vertebral sinuses and veins, into the azygous vein, and eventually into the cranial vena cava. Preoperative or intraoperative temporary occlusion of the caudal vena cava, with caudal caval pressure measurements before and during occlusion, and intraoperative angiography are useful in determining which ferrets will be able to tolerate complete ligation of the cava. Further research into the effects of caval ligation are needed before this procedure can be recommended in all ferrets.
Just as in dogs and cats, ferrets with complete caudal vena cava occlusion from a tumor or tumor thrombus that have no evidence of ascites, renal failure, or hind limb edema, have likely undergone a gradual occlusion, giving the body enough time to adapt and develop collateral circulation. These patients are perfect candidates for caval resection because the body has already become accustomed to new venous drainage patterns. The use of ameroid constrictors, cellophane bands, and hydraulic occluders in other animal species to gradually occlude the vena cava for adaptation purposes weeks before a definitive surgery is performed, is unlikely to be needed in the ferret.
If both glands are abnormal, bilateral adrenalectomy is achievable and is preferred by the author, despite previous retrospective reports documenting clinical success with partial removal of the right adrenal gland [83]. Removing both adrenal glands can lead to iatrogenic hypoadrenocorticism (Addison's disease); however, most ferrets do well on glucocorticoid supplementation only and do not require long-term mineralocorticoid therapy. It is unknown how ferrets continue to regulate electrolytes after bilateral adrenalectomy, but one study reports a high incidence (38%) of ectopic or accessory adrenal tissue in ferrets [77]. This may also be the reason why some ferrets will not require long-term steroid administration. Periodic electrolyte analysis of ferrets which have had a bilateral adrenalectomy is recommended, as some patients will require concurrent mineralcorticoid therapy. Many ferrets are concurrently diagnosed with insulinoma and already on glucocorticoid therapy for that disease process.
Following complete surgical removal of the affected gland or glands, prostatic and vulvar enlargement decrease within days and hair regrowth occurs within 3 months [7].The prognosis for adrenal gland disease in ferrets is good, if affected tissue has been completely excised, due to a low metastatic potential of these tumors [3,7,17,54,58].
Splenectomy
Splenomegaly is a common finding in adult ferrets but is poorly understood [11,84,85].The spleen in ferrets increases gradually and slightly in size with increasing age [17], but can also enlarge due to proliferative lesions, reactive processes, compensatory mechanisms, or certain anesthetics [60,84].The most common cause of splenomegaly is extramedulary hematopoesis (EMH) in the presence or absence of anemia or other hematologic dyscrasias [84–86].Other associated diseases include lymphoma, insulinoma, cardiomyopathy, adrenal disease, systemic mast cell tumors, Aleutian disease, eosinophilic gastritis, hemangiosarcoma, primary splenic neoplasia, myofasciitis, hypersplenism, and splenitis [27]. Most causes of splenomegaly are not surgical diseases and should be evaluated with clinicopathologic data and imaging modalities before splenectomy is considered. Ultrasound-guided needle aspiration of the spleen is simple, carries little risk, is associated with low morbidity, and provides useful samples.
Indications for splenectomy in ferrets include splenic neoplasia, splenomegaly, or hypersplenism causing compression of abdominal viscera, splenic torsion, and non-self-limiting traumatic fractures of the spleen. Splenectomy is contraindicated in ferrets with bone marrow hypoplasia because the spleen is the primary site of hematopoiesis in these patients [27]. Ferrets with splenic extramedullary hematopoiesis may develop chronic anemia after splenectomy because of the absence of splenic production of erythrocytes. Additionally, the spleen of the isoflurane-anesthetized ferret will sequester a significant proportion of the red cell mass [87]. Clinicians should monitor postoperative hematocrits and be prepared to perform blood transfusions as required on recovering ferrets.
The spleen of the ferret is similar to that of other mammals. The splenic artery is the main blood supply and also supplies the left gastroepiploic artery, the short gastric arteries, the left limb of the pancreas, and to the greater omentum. The splenic veins drain directly into the portal vein. The technique for performing a splenectomy in a ferret is similar to that of the other species. The surgeon may either ligate the small arteries and veins along the hilus of the spleen or identify and ligate the five main arteries described earlier. Ligation of vessels should begin at the tail and move toward the head of the spleen; suture, clips, stapling device, or a vessel sealing device can be used. If larger splenic vessels are encountered and a vessel sealing device is not available, they should be double ligated using an encircling suture and a transfixation suture.
If a neoplastic disease of the spleen is suspected, a liver biopsy is obtained to determine if metastatic disease is present.
Musculoskelatal Trauma and Disease
Trauma
Orthopedic trauma in ferrets occurs from household accidents, injury from a falling object, a closing door, attacks from another animal, an owner stepping on an animal, or by poor cage design. After initial evaluation of other body systems, an orthopedic and neurologic examination is performed. Orthopedic trauma is rarely an emergency, unless a spinal fracture is suspected. Examples of urgent orthopedic trauma include open fractures and articular fractures. Regardless of the type of orthopedic injury, all small mammal trauma patients should be evaluated on an emergency basis to evaluate other body systems and administer appropriate supportive therapy and analgesics. Once the patient is metabolically and cardiovascularly stable, all wounds and open fractures are addressed. Under sedation, wounds are clipped and cleaned, and fractures or unstable joints of the distal limbs (below the elbow and stifle) are bandaged and splinted until definitive surgery can be performed. For fractures proximal to the elbow and stifle, only a spica splint is applied to the leg.
Preoperative planning can be difficult in small mammals because exercise restriction can be challenging. Ferrets also tend to chew at bandages, splints, and wounds. Keeping the patient comfortable with analgesics and preventing possible secondary complications of anesthesia and surgery in these species is critical.
Ferret bone heals well when appropriate orthopedic principles are applied; the application of large implants overprotect the bone, leading to rapid bone resorption (mimicking disuse osteopenia and osteoporosis) and secondary failure of the repair. Overprotection of a long bone with too strong of a repair will lead to this complication in any species. Routine postoperative analgesia and supportive care are instituted as described for other surgical procedures.
Fracture Stabilization Techniques
The techniques described in the next section are a basic outline to fracture repair in small mammal patients. For the very small or juvenile ferret, creativity in fracture stabilization and repair is required.
External Coaptation
Soft bandages, splints, and casts are useful in small mammals with closed simple fractures of the distal limb. Techniques and principles for external coaptation in these species are the same as in dogs and cats. It is important to keep bandaged limbs in a relatively functional position for the patient. Owners must be properly educated on the care and management of bandages and splints. Weekly rechecks are mandatory to prevent severe and life-threatening bandage complications.
Intramedullary (IM) Pinning
IM pinning techniques used in small animals can be applied to small mammals. The pin diameter should occupy 60–70% of the medullary cavity of the bone being pinned. In general, Kirschner wires are used if Steinmann pins are too large for the diameter of their long bones. IM pins in these species are used to overcome bending forces and achieve alignment and maintain length. When possible, pins are placed in normograde fashion to avoid entering and damaging the articular surfaces of joints. The use of Kirschner wires in a cross-pin fashion are best in supracondylar fractures of the humerus and femur in these species, provide excellent alignment, and are strong enough to overcome most fracture forces during bone healing. Cross-pinning techniques are also useful for arthrodesis of the tarsal and carpal joints in small mammals.
Bone Plate and Screws
Although bone plates can be used in small mammal fracture repair, there are limiting clinical factors that may make other means of fixation more appropriate. The standard size ASIF plates are usually too large and stiff for most small mammal fracture repair. Veterinary cuttable plates that accept 1.5-mm and 2.0-mm screws can be used successfully to repair ferret long bone fractures. In complicated fractures where IM pinning or external coaptation may not be appropriate, bone plating may be a better option than external skeletal fixation (ESF).
External Skeletal Fixation (ESF)
ESF fixation is the most common surgical method used for repairing fractures in small mammal. ESF provides the surgeon with many options for rigidity, pin placement, and dynamizition, while minimizing damage to soft tissue and extraosseal blood supply. The principles for application of ESF in small mammals are similar to those of other species. The pins are inserted with low rotational speed (150 rpm) and not with manual insertion, which results in wobble and leads to premature loosening of the pins. Small diameter threaded pins and nonthreaded pins can be used. Pins are angled at 70° to the longitudinal axis of the bone so that pin pullout is prevented. The benefit of ESF is that a closed or limited open reduction is performed, limiting the soft tissue trauma and further damage to the blood supply. Most small mammals are too small for commercially available external bars and clamps; instead, bone cement and other acrylics can be used as connecting bars.
Three to four pins are placed in each bone segment with the pins at least 1 cm, or one bone diameter, from the fracture line and each pin not to exceed 20% of the bone diameter. Each pin is placed through a separate skin incision. A type I, type I tie in, and type II ESF are the most frequently used configurations in small mammals.
Type I fixators are unilateral and uniplaner. The transosseous pins engage the transcortex but do not exit the soft tissues.
Type I tie-in configuration utilizes an IM pin that is bent at the proximal or distal end of the bone as it exits the skin, and is incorporated or tied in to the side bar used for connecting the transosseous pins.
Type II configurations are bilateral and uniplaner. The transosseous pins engage both cortices and penetrate the soft tissues medial and lateral. This is a very stable and strong design. The connecting bar is made from bone cement or other acrylic, and is 1 cm away from the skin to accommodate postoperative swelling.
The fixator is evaluated every week, the pin tracts cleaned with a dilute chlorhexadine solution, and the bars rewrapped with clean material. Radiographs are assessed at 4 weeks to assess fracture healing and every 3–4 weeks thereafter until the fracture has healed.
Elbow Luxation
Elbow luxation is a common orthopedic injury in ferrets. This usually results from the animal getting its leg caught in the cage flooring and then moving abruptly. A non-weight-bearing lameness of the affected limb and a painful, swollen elbow joint will be present. Ferrets will almost always require open reduction, as closed reduction in this species often fails.
Closed Reduction
Closed reduction of a luxated elbow is the same for other veterinary species. After the elbow is reduced, the leg needs to be immobilized until soft tissues surrounding the joint can scarify. In dogs and cats, the shoulder joint should also be immobilized, but this is difficult in ferrets as it is poorly tolerated. A splint can be placed up to the midhumerus but must be closely monitored for signs of distal swelling, skin abrasions, and slipping of the bandage. It is important to note that joints that reduce easily will reluxate easily in this species.
Open Reduction
Although there are many techniques described for surgical reduction and stabilization of the elbow in small animals, the placement of a transarticular pin through the elbow joint (from the caudal ulna into the distal humerus) works well in ferrets (Fig. 13.10). A splint is then applied to the leg. The pin will keep the joint reduced and the splint will prevent full weight bearing. The pin is removed in 3–4 weeks, and the splint remains on for another 3–4 weeks after pin removal. Although this technique works well, another option would be to place a transarticular fixator for 4 weeks with subsequent application of a splint when the fixator is removed. Complete recovery of range of motion is unlikely with this technique; however, most ferrets tolerate well a long-term decrease in range of motion of the elbow.
Fig. 13.10. (A) Radiographs of a ferret with an elbow luxation secondary to an unknown trauma. (B) Postoperative radiographs of the ferret in panel A demonstrating a temporary transarticular pin placed from the caudal aspect of the proximal ulna into the elbow joint and engaging the distal aspect of the humeral condyle with the elbow joint at a weight-bearing angle.
Amputation
Indications for amputation in small mammals include severe traumatic orthopedic conditions, unresolvable osteomyelitis, primary and metastatic bone tumors, and salvage from failed fracture repair. Most small mammals, including ferrets, tolerate single limb amputation well. For a forelimb amputation, most surgeons prefer removing the scapula as it is faster and more cosmetic; however, some surgeons leave the scapula to protect the thoracic wall. Hind limb amputation can be done through a disarticulation of the coxofemoral joint or a midfemoral approach, which is faster. Disarticulation of the coxofemoral joint is always performed if a neoplastic process is present in the femur. If a midshaft amputation is performed, it is important to make sure that enough muscle and skin are left to facilitate tension-free closure over the bone. The incision is bandaged postoperatively to help decrease dead space and prevent seroma formation. It is important not to make the bandage too tight, as compression of the abdomen and urethra in the male ferret may occur.
Ferrets as Surgical Models
Ferrets are sporadically used for development of novel surgical techniques or surgical materials. More often, they are subjected to surgery for physiologic, anatomic, or drug discovery studies. Techniques used in other species are commonly adapted to the ferret in this latter instance. One such technique, craniotomy, will be described in more detail. Select studies using the ferret in other types of research requiring surgery can be found in Chapters 27–32 of this text.
Stereotaxic Surgery for Craniotomy
The ferret is an important model in several disciplines that require stereotaxic surgery, including auditory and visual neuroscience, neuroplasticity, and emesis. A common stereotaxic apparatus used for ferrets is the Kopf Model 900 Small Animal Stereotaxic instrument with Model 1227 Ferret/Mink Adaptor (David Kopf Instruments, Tujunga, CA; http://www.kopfinstruments.com); Figure 13.11A,B). Other instruments are available. The stereotaxic device rigidly fixes the skull with points of contact that restrict movement in the sagittal (ear bars), coronal (ear bars), and transverse planes (palate bar and infraorbital clamps). An adapter bar allowing rostrocaudal adjustment and adjustable palate and orbital ridge bars are essential to individualizing cranial fixation of ferrets and other animals. This is especially important in the ferret, as there is considerable variation in skull size and shape among ferrets (Lawes and Andrews [88]) This variation in skull size between and within the sexes, the fusion of cranial sutures that ablates the landmarks lambda and bregma, the failure of body weight or skull length index to predict skull size, and the variation in the location of extracranial landmarks have precluded the creation of a generalized stereotaxic atlas. Indeed, an atlas of the mediodorsal nucleus and prefrontal cortex using bregma as a landmark creates coordinates applicable only to ferrets from 6–14 weeks of age (Duque and McCormick [89]).
Fig. 13.11. (A) Kopf Model 900 Small Animal Stereotaxic Instrument and (B) Model 1227 Ferret/Mink Adaptor. (David Kopf Instruments.)
Ferrets must be in a surgical plane of anesthesia to tolerate the robust stimulus of placement in the stereotaxic device. Most surgical approaches require a midline (sagittal) incision. The superficial and deep temporal fascia is incised, and the temporalis muscle is elevated from the cranium subperiostially using a periosteal elevator. The muscle may be retracted using a mastoid or other suitable retractor. Weighted towel clamps are an inexpensive alternative. Craniotomy may then be performed using the drill or trephine of the surgeon's choosing. Proper irrigation is required to avoid thermal injury to bone when using motorized drills. Hemorrhage from the diploë can be controlled using bone wax; bipolar electrocautery can be used on muscle or vessels of the dura mater. Durotomy, if required, can be achieved using an 11 blade. Dural repair is difficult, but dural replacement using Duragen (Integra LifeSciences, Plainsboro, NJ) or temporalis fascia graft can be used over the craniotomy. If a chronic implant is required, screws may be placed into holes predrilled using a motorized drill or hand chuck. The use of self-tapping screws saves time; screws of appropriate size can be ordered from Crist Instrument Company (Hagerstown, MD). The implant can be secured to the screws using the method of the surgeon's choice. If acrylic or orthopedic cements are used, they must be applied in thin laminae with allowance for heat dissipation between laminae, as they generate considerable heat as they cure. Attention to this principle will spare the underlying bone and brain from thermal injury. Bone flaps to close craniotomies are usually not attempted. The remaining closure is anatomic, with approximation of the temporalis muscles achieved if possible. Skin may be closed with a suture pattern of the surgeon's choice. Ferrets tolerate such procedures well. Preemptive and postoperative analgesia is required.
References
1. Jurek RM (1998) A review of national and California population estimates of pet ferrets. In: Calif Dep Fish and Game, Wildl Manage Div, Bird and Mammal Conservation Program Rep. Sacramento.
2. Carpenter JW, Novill MN, Kaiser HL (1981) Neoplasia and other disease problems in black-footed ferrets; implications for an endangered species. In: Kraiser HE, ed. Neoplasms—comparative pathology of growth in animals, plants, and man. Baltimore, MD: Lippincott Williams & Wilkins, pp. 739–746.
3. Rosenthal KL, Peterson ME, Quesenberry KE, Hillyer EV, Beeber NL, et al. (1993) Hyperadrenocorticism associated with adrenocortical tumor or nodular hyperplasia of the adrenal gland in ferrets: 50 cases (1987–1991). J Am Vet Med Assoc 203: 271–275.
4. Stauber E, Kraft S, Robinette J (1991) Multiple tumors in a ferret. J Small Exot Anim Med 1: 87–88.
5. Jenkins JR (1991) Multiple concurrent neoplasia and metabolic diseases in the ferret: selected cases. J Small Exot Anim Med 1: 118–121.
6. Kolb KS, Day T, McCall WG (1999) Accuracy of blood loss termination by health care professionals. CRNA 10: 170–173.
7. Antinoff N, Hahn K (2004) Ferret oncology: diseases, diagnostics, and therapeutics. Vet Clin N A Exot Anim Pract 7: 579–625.
8. Whary MT, Andrews PL (1998) Physiology of the ferret. In: Fox JG, ed. Biology and disease of the ferret, 2nd ed. Baltimore, MD: Lippincott Williams & Wilkins, pp. 103–148.
9. Manning DD, Bell JA (1990) Lack of detectable blood groups in domestic ferrets: implications for transfusion. J Am Vet Med Assoc 197: 84–86.
10. Mehler SJ, Bennett RA (2010) Ferrets. In: Bojrab MJ, Monnet E, eds. Mechanisms of disease in small animal surgery, 3rd ed. Jackson, WY: Teton NewMedia, pp. 750–756.
11. Ludwig L, Aiken S (2004) Soft tissue surgery. In: Quesenberry KE, Carpenter JW, eds. Ferrets, rabbits, and rodents: clinical medicine and surgery, 2nd ed. Philadelphia: W.B. Saunders, pp. 121–134.
12. Poddar S (1977) Gross and microscopic anatomy of the biliary tract of the ferret. Acta Anat 97: 121–131.
13. Evans HE, Quoc An N (1998) Anatomy of the ferret. In: Fox JG, ed. Biology and diseases of the ferret. Baltimore, MD: Lippincott Williams & Wilkins, pp. 19–70.
14. Li X, Fox JG, Padrid PA (1998) Neoplastic diseases in ferrets: 574 cases (1968–1997). J Am Vet Med Assoc 212: 1402–1406.
15. Williams BH, Weiss CA (2004) Neoplasia. In: Quesenberry KE, Carpenter JW, eds. Ferrets, rabbits, and rodents: clinical medicine and surgery, 2nd ed. Philadelphia: W.B. Saunders, pp. 91–106.
16. Li X, Fox JG, Padrid PA (1998) Neoplastic diseases in ferrets (Mustela putorius furo): a review of Veterinary Medical Data Base (1968–1997). J Am Vet Med Assoc 212: 212–219.
17. Brown SA (1997) Neoplasia. In: Hillyer EV, Quesenberry KE, eds. Ferrets, rabbits, rodents: clinical medicine and surgery. Philadelphia: W.B. Saunders, pp. 91–114.
18. Jones TC, Hunt RD (1983) Veterinary pathology, 5th ed. Philadelphia: Lea & Febiger, pp. 116–119.
19. Sleeman JM, Clyde VL, Jones MP, Mason GL (1995) Two cases of pyloric adenocarcinoma in the ferret (Mustela putorius furo). Vet Rec 137: 272–273.
20. Rice LE, Stahl SJ, McLeod CG (1992) Pyloric adenocarcinoma in a ferret. J Am Vet Med Assoc 200: 1117–1118.
21. Weisse C, Hume DZ, Berent A, Briscoe J, Solomon JA (2004) Palliative stenting for malignant obstructions in a dog, cat, and ferret. In: The proceedings of the 2004 annual meeting of the American College of Veterinary Surgeons. Denver, CO, p. 23.
22. Hoefer HL, Bell JA (2004) Gastrointestinal diseases. In: Quesenberry KE, Carpenter JW, eds. Ferrets, rabbits, and rodents: clinical medicine and surgery, 2nd ed. Philadelphia: W.B. Saunders, pp. 25–40.
23. Evans HE, An NQ (1998) Anatomy of the ferret. In: Fox JG, ed. Biology and disease of the ferret, 2nd ed. Baltimore, MD: Lippincott Williams & Wilkins, pp. 19–69.
24. Fox JG (1998) Diseases of the gastrointestinal system. In: Fox JG, ed. Biology and diseases of the ferret. Baltimore, MD: Lippincott Williams & Wilkins, pp. 273–290.
25. Tobias K (2003) Gastrointestinal system. In: Slatter D, ed. Textbook of small animal surgery. Philadelphia: Elsevier, pp. 499–762.
26. Mullen HS, Scavelli TD, Quesenberry KE, Hillyer E (1989) Gastrointestinal foreign body in ferrets: 25 cases (1986–1990). J Am Anim Hosp Assoc 28: 13–15.
27. Wheeler J, Bennett RA (1999) Ferret abdominal surgical procedures. Part II. Compendium 21: 1049–1057.
28. Hedlund CS, Fossum TW (2007) Surgery of the digestive system. In: Fossum TW, ed. Small animal surgery. St. Louis MO: Mosby, pp. 339–470.
29. Pollock CG (2004) Urogenital diseases. In: Quesenberry KE, Carpenter JW, eds. Ferrets, rabbits, rodents: clinical medicine and surgery. Philadelphia: W.B. Saunders, pp. 41–49.
30. Fox JG, Pearson RC, Bell JA (1998) Diseases of the genitourinary system. In: Fox JG, ed. Biology and diseases of the ferret. Baltimore, MD: Lippincott Williams & Wilkins, pp. 247–272.
31. Bell JA (2004) Periparturient and neonatal diseases. In: Quesenberry KE, Carpenter JW, eds. Ferrets, rabbits, rodents: clinical medicine and surgery. Philadelphia: W.B. Saunders, pp. 50–57.
32. Nguyen HT, Moreland AF, Shields RP (1979) Urolithiasis in ferrets (Mustela putorius). Lab Anim Sci 29: 243–245.
33. Marini RP, Esteves MI, Fox JG (1994) A technique for catheterization of the urinary bladder in the ferret. Lab Anim 28: 155–157.
34. Bjorling DE (2003) Urinary system. In: Slatter D, ed. Textbook of small animal surgery. Philadelphia: Elsevier, pp. 1558–1676.
35. Mullen H (1997) Soft tissue surgery. In: Hillyer EV, Quesenberry KE, eds. Ferrets, rabbits, rodents: clinical medicine and surgery. Philadelphia: W.B. Saunders, pp. 131–144.
36. Mullen HS, Beeber NL (2000) Miscellaneous surgery in ferrets. Vet Clin N A Exot Anim Pract 3: 663–671.
37. Patterson MM, Rogers AB, Schrenzel MD, Marini RP, Fox JG (2003) Alopecia attributed to neoplastic ovarian tissue in two ferrets. Comp Med 53: 213–217.
38. Divers SJ (2010) Exotic mammal diagnostic endoscopy and endosurgery. Vet Clin North Am Exot Anim Pract 13: 255–272.
39. Wheeler J, Bennett RA (1999) Ferret abdominal surgical procedures: Part 1. Adrenal gland and pancreatic beta-cell tumors. Compendium 21: 815–822.
40. Cooper JE (1985) Ferrets. In: Cooper JE, Hutchinson MF, Jackson OF, et al., eds. Manual of exotic pets. West Sussex, England: British Small Animal Veterinary Association, pp. 93–98.
41. Creed JE, Kainer RA (1981) Surgical extirpation and related anatomy of anal sacs of the ferret. JAVMA 179: 575–577.
42. Weiss CA, Williams BH, Scott MV (1998) Insulinoma in the ferret: clinical findings and treatment comparison of 66 cases. J Am Anim Hosp Assoc 34: 471–475.
43. Jergens AR, Shaw DP (1989) Hyperinsulinism and hypoglycemia associated with pancreatic islet cell tumor in a ferret. J Am Vet Med Assoc 194: 269–270.
44. Ehrhart N, Withrow SJ, Ehrhart EJ, et al. (1996) Pancreatic beta cell tumors in ferrets: 20 cases (1986–1994). J Am Vet Med Assoc 209: 1737–1740.
45. Hillyer EV (1992) Ferret endocrinology. In: Kirk RW, Bonagura JD, eds. Kirk's current veterinary therapy, 11th ed. Philadelphia: W.B. Saunders, pp. 1185–1189.
46. Kauffman J, Schwarz P, Mero K (1984) Pancreatic beta cell tumor in a ferret. J Am Vet Med Assoc 185: 998–1000.
47. Caplan ER, Peterson ME, Mullen HS, et al. (1996) Diagnosis and treatment of insulin-secreting pancreatic islet cell tumors in ferrets: 57 cases (1986–1994). J Am Vet Med Assoc 209: 1741–1745.
48. Quesenberry KE, Rosenthal KL (2004) Endocrine diseases. In: Quesenberry KE, Carpenter JW, eds. Ferrets, rabbits, and rodents: clinical medicine and surgery, 2nd ed. Philadelphia: W.B. Saunders, pp. 79–90.
49. Whary MT, Andrews PLR (1998) Physiology of the ferret. In: Fox JG, ed. Biology and diseases of the ferret. Baltimore, MD: Lippincott Williams & Wilkins, pp. 103–148.
50. Meleo KA, Caplan ER (2000) Treatment of insulinoma in the dog, cat, and ferret. In: Bonagura JD, ed. Kirk's current veterinary therapy, 13th ed. Philadelphia: W.B. Saunders, pp. 357–361.
51. Li X, Fox JG (1998) Neoplastic diseases. In: Fox JG, ed. Biology and disease of the ferret, 2nd ed. Baltimore, MD: Lippincott Williams & Wilkins, pp. 405–447.
52. Marini RP, Ryden EB, Rosenblad KS, Murphy JC, Fox JG (1993) Functional islet cell tumor in six ferrets. J Am Vet Med Assoc 202: 430–433.
53. Nelson RW (1995) Insulin-secreting islet cell neoplasia. In: Ettinger SJ, Feldman EC, eds. Textbook of veterinary internal medicine, 4th ed. Philadelphia: W.B. Saunders, pp. 1501–1509.
54. Fox JG, Marini RP (1998) Diseases of the endocrine system. In: Fox JG, ed. Biology and diseases of the ferret. Baltimore, MD: Lippincott Williams & Wilkins, pp. 291–305.
55. Lumeij JT, van der Hage MG, Dorrestein GM, van Sluijs FJ (1987) Hypoglycemia due to a functional pancreatic islet cell tumor (insulinoma) in a ferret. Vet Rec 120: 129–130.
56. Luttgen PJ, Storts RW, Rogers KS, Morton LD (1986) Insulinoma in a ferret. J Am Vet Med Assoc 189: 920–921.
57. Mann FA, Stockham SL, Freeman MB, Wagner-Hann C, Besch-Williford CL, et al. (1993) Reference intervals for insulin concentrations and insulin:glucose ratios in the serum of ferrets. J Small Exot Anim Med 2: 79–83.
58. Fox JG, Marini RP (1998) Diseases of the endocrine system. In: Fox JG, ed. Biology and disease of the ferret, 2nd ed. Baltimore, MD: Lippincott Williams & Wilkins, pp. 291–305.
59. Mehler SJ, Bennett RA (2004) Surgical oncology of exotic animals. Vet Clin N A, Exot Anim Pract 7: 783–805.
60. Marini RP, Fox JG (1998) Anesthesia, surgery, and biomethodology. In: Fox JG, ed. Biology and disease of the ferret, 2nd ed. Baltimore, MD: Lippincott Williams & Wilkins, pp. 449–484.
61. Lipman NS, Marini RP, Murphy JC, Zhibo Z, Fox JG (1993) Estradiol-17 beta-secreting adrenocorticol tumor in a ferret. J Am Vet Med Assoc 203: 1552–1555.
62. Rosenthal KL, Peterson ME (1996) Evaluation of plasma androgen and estrogen concentrations in ferrets with hyperadrenocorticism. J Am Vet Med Assoc 209: 1097–1102.
63. Gould WJ, Reimers TJ, Bell JA, Lawrence HJ, Randolph JF, et al. (1995) Evaluation of urinary cortisol:creatinine ratios for the diagnosis of hyperadrenocorticism associated with adrenal gland tumors in ferrets. J Am Vet Med Assoc 206: 42–46.
64. Neuwirth L, Isaza R, Bellah J, et al. (1993) Adrenal neoplasia in seven ferrets. Vet Radiol Ultrasound 34: 340–343.
65. Weiss CA, Scott MV (1997) Clinical aspects and surgical treatment of hyperadrenocorticism in the domestic ferret: 94 cases (1994–1996). J Am Anim Hosp Assoc 33: 488–493.
66. Fox JG, Pequet-Goad ME, Garihaldi BA, Wiest LM (1987) Hyperadrenocorticism in a ferret. J Am Vet Med Assoc 191: 343–344.
67. Wagner RA, Dorn DP (1994) Evaluation of serum estradiol concentrations in alopecic ferrets with adrenal gland tumors. J Am Vet Med Assoc 205: 703–707.
68. Rosenthal KL (1997) Adrenal disease in ferrets. In: Kintzer PP, ed. Veterinary clinics of North America, small animal practice. Philadelphia: W.B. Saunders, pp. 401–418.
69. Schoemaker NJ, Wolfswinkel J, Mol JA, Voorhout G, Kik MJL, et al. (2003) Urinary corticoid/creatinine ratios in healthy ferrets and ferrets with hyperadrenocorticism. In: Schoemaker NJ. Hyperadrenocorticism in ferrets. PhD thesis.
70. Schoemaker NJ, van der Hage MH, Lumeij JT, Rijnberk A (2003) Morphology of the pituitary gland in ferrets (Mustela putorius furo) with hyperadrenocorticism. In: Schoemaker NJ. Hyperadrenocorticism in ferrets. PhD thesis.
71. Besso JG, Tidwell AS, Gliatto JM (2000) Retrospective review of the ultrasonographic features of adrenal lesions in 21 ferrets. Vet Radiol Ultrasound 41: 345–352.
72. Gliatto JM, Alroy J, Schelling SH, et al. (1995) A light microscopical, ultrastructural and immunohistochemical study of spindle-cell adrenocortical tumors of ferrets. J Comp Pathol 113: 175–178.
73. Murthy AS, Brezak MA, Baez AG (1970) Postcastrational adrenal tumors in two strains of mice: morphological, histochemical, and chromatographic studies. J Natl Cancer Inst 25: 2111–2115.
74. Schoemaker NJ, Schuurmans M, Moorman H, Lemeij JT (2003) Correlation between age at neutering and age at onset of hyperadrenocorticism in ferrets. In: Schoemaker NJ. Hyperadrenocorticism in ferrets. PhD thesis.
75. Rosenthal KL, Peterson ME, Quesenberry KE, et al. (1993) Evaluation of plasma cortisol and corticosterone responses to synthetic adrenocorticotropic hormone administration in ferrets. Am J Vet Res 54: 29–31.
76. O'Brien R, Paul-Murphy J, Dubielzig RR (1996) Ultrasonography of adrenal glands in normal ferrets. Vet Radiol Ultrasound 37: 445–448.
77. Neuwirth L, Collins B, Calderwood-Mays M, et al. (1997) Adrenal ultrasonography correlated with histopathology in ferrets. Vet Radiol Ultrasound 38: 69–74.
78. Beeber NL (2000) Abdominal surgery in ferrets. Vet Clin N A Exot Anim Pract 3: 647–662.
79. Beeber NL (1998) Surgery of pet ferrets. In: Bojrab MJ, ed. Current techniques in small animal surgery, 4th ed. Philadelphia: Lippincott Williams & Wilkins, pp. 763–769.
80. Filion DL, Hoar DM (1985) Adrenalectomy in the ferret. Lab Anim Sci 35: 294–305.
81. Weiss CA, Williams BH, Scott JB, Scott MV (1999) Surgical treatment and long-term outcome of ferrets with bilateral adrenal tumors or adrenal hyperplasia: 56 cases (1994–1997). J Am Vet Med Assoc 215: 820–823.
82. Laraio L, Weisse C, Zwingerberger A, Rosenthal KR, Johnston M, et al. (2003) Collateral circulation during balloon occlusion of the caudal vena cava in ferrets. Proceedings of the annual conference of the American College of Veterinary Surgeons. Washington, D.C.
83. Swiderski JK, Seim HB, MacPhail CM, et al. (2008) Long-term outcome of domestic ferrets treated surgically for hyperadrenocorticism: 130 cases (1995–2004). JAVMA 232: 1338–1343.
84. Erdman SE, Li X, Fox JG (1998) Hematopoietic diseases. In: Fox JG, ed. Biology and disease of the ferret, 2nd ed. Baltimore, MD: Lippincott Williams & Wilkins, pp. 231–246.
85. Petrie JP, Morrisey JK (2004) Cardiovascular and other diseases. In: Quesenberry KE, Carpenter JW, eds. Ferrets, rabbits, and rodents: clinical medicine and surgery, 2nd ed. Philadelphia: W.B. Saunders, pp. 58–71.
86. Brown SA, Rosenthal KL (2000) Causes of splenomegaly in ferrets. Vet Med 95: 599.
87. Marini RP, Callahan RJ, Jackson LR, Jyawook S, Esteves MI, et al. (1997) Distribution of technetium 99m-labeled red blood cells during isoflurane anesthesia in ferrets. Am J Vet Res 58: 781–785.
88. Lawes IN, Andrews PL (1987) Variation of the ferret skull (Mustela putorius furo L.) in relation to stereotaxic landmarks. J Anat 154: 157–171.
89. Duque A, McCormick DA (2010) Circuit-based localization of ferret prefrontal cortex. Cereb Cortex 20: 1020–1036.