The best method of billing and collections is customized to the practice and regards the patient as a consumer who should be respected. Patients want to know in advance what charges and fees to expect whenever possible. Accurate billing techniques will make the cash flow and collection process smoother in the medical office. The best time for collection is at the time of service. This assures prompt collection, eliminates further bookkeeping work, and provides better cash flow for the practice.
In those cases where a payment schedule is arranged, it must be determined by the office whether or not interest will be charged. Ambulatory care settings may decide to charge interest for installment arrangements. The Truth-in-Lending Act (also called the Consumer Credit Protection Act of 1968) was established to protect consumers by requiring that providers of installment credit state the charges clearly in writing and express the interest as an annual rate. When there is a bilateral agreement between the physician and patient to pay more than four installments, the physician must disclose finance charges in writing. Even if no finance charges are made, the forms must still be completed.
The billing schedule is often determined by the size of the medical practice. In monthly billing, all accounts are billed at the same time each month. In a cycle billing system, all accounts are divided alphabetically into groups, with each group billed at a different time. In this way, personnel in a large practice with numerous bills to process each month will be able to handle them in a more efficient manner.
Third-party payers may deposit funds directly into an account or send a check to the practice. If a patient has a copayment, it is imperative to address the need to pay that at the time of the visit. Rather than ask if the patient is going to pay for the visit, the best approach is to ask, “How would you like to pay today?” A strong office policy is to collect copayments before the patient is seen by the health care provider. Providing the option of various payment methods further enhances the ability of the practice to collect payment.
Different payment methods involve different levels of risk. Here are precautions for different payment types.
It is important for the medical office to provide accurate information on the bills. Demographic information regarding the patient will include the correct spelling of the name, the date of birth, the social security number, mailing address, and phone number. The office will also need to provide the third-party payer with the correct address, name and provider number of the physician, date of service, and the date of submission of the claim.
Coding is the basis for establishing the charges listed on the claim form. Medical coding is mandatory for the accurate transmission of procedures and diagnosis information between health care providers and the insurance companies or other payers. Codes are assigned both to identify the diagnoses of the patient and to specify the treatment or procedure that was provided as care and treatment.
The process of converting descriptions of diseases, injuries, and procedures into numerical designations is termed coding. Current Procedural Terminology (CPT) was developed by the American Medical Association (AMA) to convert commonly accepted, uniform descriptions of medical, surgical, and diagnostic services rendered by health care providers into five-digit numeric codes. These codes must be listed correctly on claim forms and bills to specify what services were rendered to patients.
The International Classification of Disease, 10th Revision, Clinical Modification (ICD-10-CM) was compiled by the World Health Organization (WHO). It is designed for the classification of patient diagnostic morbidity and mortality information. ICD codes are assigned for disease states, surgical procedures, and the full range of causative events such as injuries and poisonings. Level II HCPCS codes identify services and supplies that lack CPT codes but are covered by many insurers.
Procedure codes and codes for patient encounters of all kinds—office, hospital, nursing facility, home services—are found in Current Procedural Terminology (CPT). This listing is updated annually. The CPT manual is divided into six sections, and each CPT code is five digits long:
For the insurance company to understand what is being billed, the claim form is completed or generated electronically by the medical assistant in the office setting. The physician documents the services at the time of the visit, which will be used in determining the charges.
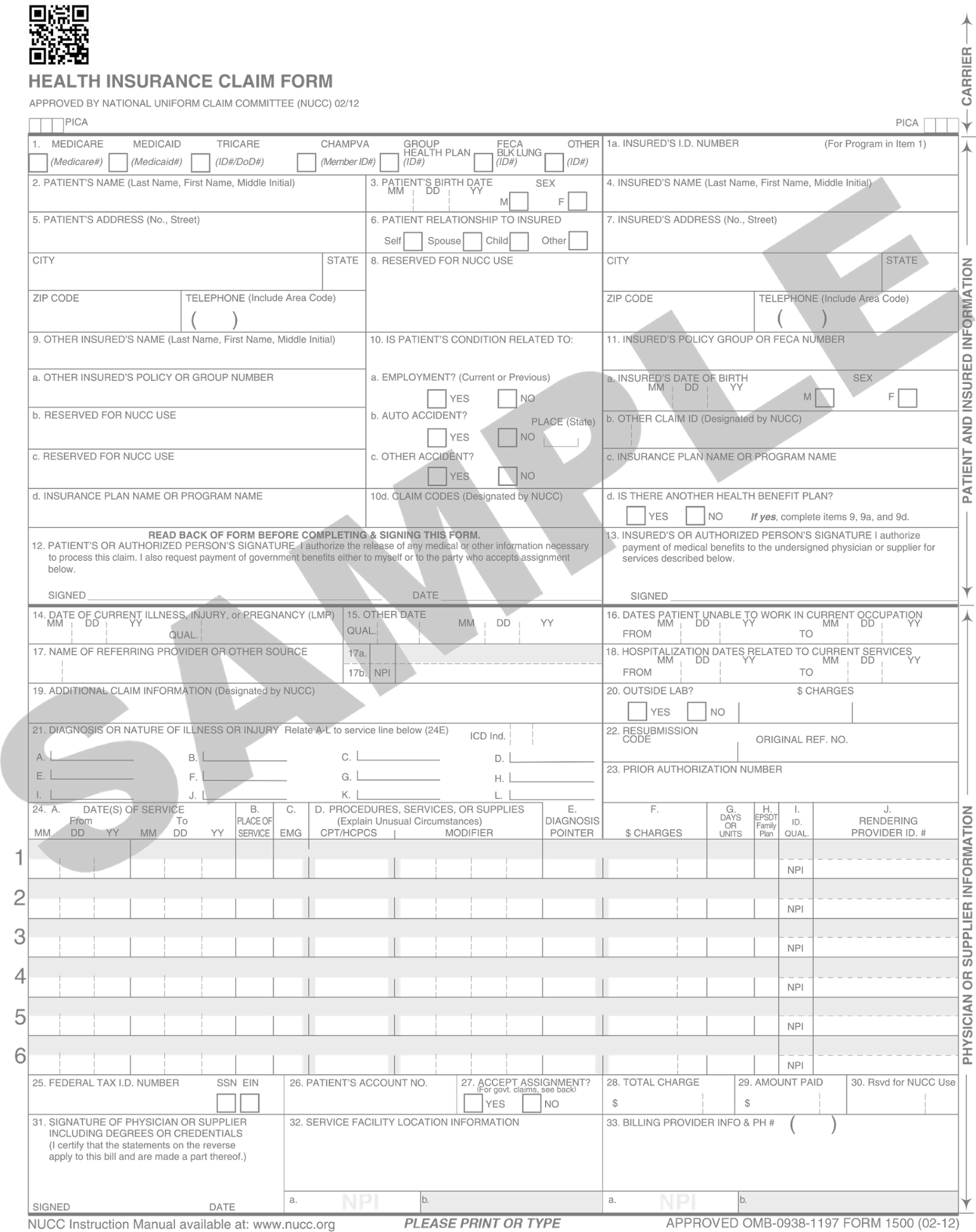
The CMS-1500 is the claim form accepted by most insurance carriers. This form is prepared using both name identifiers and CPT codes for procedures performed and ICD-10-CM codes for pertinent patient diagnoses. If the coding is omitted, incomplete, or noted to be in error, payment may be denied or delayed. Coding must correlate with the physician’s note in the chart and the actual status of the patient. It is likely that individual insurance companies will require some unique information or procedures for correctly submitting medical claims information. Most claims are generated electronically now, but the same information noted on the CMS-1500 form is collected in software programs. Electronic claims are often sent to clearinghouses, which will review the documentation for completeness and accuracy prior to forwarding the claim to the payer.
When submitting claims, the medical assistant must be aware of the importance of accurate billing and the legal ramifications of not following prescribed guidelines. Under the bundled payment model, facilities and/or providers are paid one fee for an episode of care. Bundling services is a way to control health care costs and avoid repetition of charges. An episode of care is defined as care for a certain condition or care over a specified time period. Unbundling is considered fraud and an attempt to gain higher pay than agreed for services rendered.
In October 2015, the health care industry transitioned to an entirely new coding system that brought major changes to systems, processes, and staff involved in health information and health care delivery. As a medical assistant, you should remain current on changes to the new coding system to ensure appropriate billing that maximizes provider reimbursement.
In 1979, the federal government—through the Health Care Financing Administration (HCFA)—adopted a procedure coding system to use in tandem with the International Classification of Diseases, 9th Revision, as established by the World Health Organization (WHO). Since 1983, government and private payers had used the system of diagnostic and procedure coding for reimbursement of health care services. As the complexity of health care grew, the need for accuracy and specificity of coding systems escalated. The code sets designed in the 1970s were no longer an adequate reflection of the care and treatment rendered in the United States in the 21st century. In addition, the structure of the coding system had run out of space and it was difficult for experts to accommodate changes and additions that reflected new medical practice and newer disease states. It had also been determined that the ICD-9 system did not allow enough detail to describe complex patient statuses or account for the variety of health care encounters that occurred in practice.
The National Center for Health Statistics worked with a variety of professional organizations and experts to devise the U.S. Clinical Modifications in the ICD-10-CM system. A major effort was made to add detail and specificity to the system and to add language that fits the current clinical practice activities in health care. The new ICD-10-CM system uses 68,069 codes, up from the 14,025 in use with ICD-9-CM conventions. Extensive testing and public and professional input were sought in forming this new coding system. In addition to adding more levels of detail to the codes, professionals are better able to work with the system to add new codes and revise as medical advances occur. The new coding system is able to provide better and more detailed information to evaluate the quality of patient care. It provides more detail on patient complications, clinical outcomes, and comparison of treatments and conditions across the globe. In addition, the system enables public health officials to track disease outbreaks and bioterrorism events internationally and allows more sharing of practice patterns used to treat disease states.
The following items are proposed as the areas for data improvement based on the ICD-10 coding systems:
In addition to these improvements, the ICD-10 systems aim to contribute to lowering the cost of health care and improving operating efficiency of health systems through the following means:
The WHO ICD-10 system contains a completely new alphanumeric, structure for coding. The first character in all codes is a letter. All letters are used except U, which has been set aside for new diseases with uncertain causes or causes from bacterial agents that are resistant to antibiotics. The ICD-10-CM includes a tabular list organized alphabetically with indentations for qualifiers and descriptors. Unlike codes in the ICD-9 system, which contain up to five digits, the ICD-10 system uses seven digits. Below is a comparison of the coding structures across the two systems.
XXX.XX, where the first three digits signify the category of the disease and the last two digits (after the decimal) signify the etiology of the disease, the anatomic site and the manifestations presented.
XXX.XXXX, where the first three digits signify the category of the disease; the fourth, fifth and sixth digits signify the etiology, anatomic site, and severity; and the seventh digit signifies the extension.
In addition to the coding structure noted above, the following major changes have been made in the organization of the codes, the structure of the codes and the level of detail of coding.
In addition to the changes listed, many chapters have been updated and changed significantly from the ICD-9-CM system. These include injuries, diabetes, substance abuse, and postoperative complications. Along with changes in the coding of diseases and illnesses, significant changes also have been made to the ICD-10-PCS (procedural coding system). These changes, however, will only be used in inpatient facilities and are thus outside of the scope of this manual. Medical offices and clinics will continue to use the current CPT (Current Procedural Terminology) and HCPCS codes.
Medical assistants should keep their knowledge of ICD-10 fresh by attending professional conferences, doing independent reading, or taking advantage of training and education provided by billing or software vendors.
With the implementation of electronic health records, the use of manual claim submission has decreased dramatically. Regardless of the method of submission, it is important that to file claims in a timely fashion, as close to the date of service as possible. Claims should be numbered and tracked in a filing system for review. Once the claim is submitted, an accounting record should be made of the amount due in the accounts receivable system as money due to the practice. As a general rule, the older the account is from the date of payment, the less likely the practice is to collect the money. Some third-party payers may take time to submit claims payment. In order to keep a steady cash flow, an office should track payments through a claims register.
In filing claims, it may be that more than one payer is billed. Initially, the office practice should submit the bill to the patient’s identified primary insurer or governmental payer. If the primary payer denies coverage, you may need to bill a secondary source. Many practices require the patient to sign a statement indicating that they will pay for any charges not covered by their insurance (or third-party payer). Most third parties require that claims be submitted in a sequential or chronological order based on the date of service. It is common for high-cost services to require supplemental documentation or clinical records to justify payment.
As claims are paid, the office staff will need to post the payments onto the patient’s account records and determine if any unpaid balances are due. If all or part of the claim goes unpaid, the payer should be contacted for an explanation of benefits. The physician should then determine if the partial payment will be accepted or if another party should be billed for the balance.
In working with managed care organizations (MCO), you will still need to provide accurate and timely billing records. Each MCO will have unique forms and systems for payment that you must follow as part of your contractual obligation. Most MCOs require prior authorization for specialty referrals, elective surgery, or any needed patient equipment and supplies. You need to refer to the specific processes of each event or patient need as required for your patients and their insurance companies and third-party payers.