
Thanks to all the hype generated by the beauty contests and advertisements, one message that has gone across is that ‘slim is beautiful’. This has led to a growing awareness about diet and weight loss. On the flip side, it has also generated a host of unhealthy fad diets, which promise to melt away the fat without any pain.
Obesity is becoming the single leading cause for many ailments. Right from high blood pressure to diabetes, it is the root cause of all problems. The changing lifestyle has led to the birth of a generation that is increasingly becoming unhealthy. Lack of exercise, fast food and stress, all have added to the growing number of obese people in the society. In this age of computers when the only kind of exercise is the moving of a mouse, fat is not burnt but accumulated in the body. This accumulated fat results into an obese condition.
In a way it is good that weight loss has become an obsession with most people because being overweight means to invite a whole lot of diseases. Obesity is defined simply as an excess of body fat. Your body is made up of water, fat, protein, carbohydrate and various vitamins and minerals. It is the excess fat that causes the problems.
Obesity and hypertension: It has been proved beyond any doubt that hypertension is a common outcome of obesity. In overweight young adults, age 20-45, the prevalence of hypertension is 6 times that of their normal-weight peers. We all know that fat children, generally, make fat adults and weight gain in young adult life is a potent risk factor for the later development of hypertension. In races where people tend to weigh less with advancing years, cases of hypertension are infrequent. Doctors have also found that the distribution of fat in the body may have an important affect on blood pressure risk. People with more flab and fat in the abdomen or upper body region are more likely to suffer from high blood pressure than those with lower body fat in the gluteal or thigh region. In obese persons, an accumulation of abdominal fat results in the release of free fatty acids into the portal vein, which causes incidents of insulin resistance and hyperinsulinemia.
Obesity and diabetes: Even moderate obesity, particularly abdominal obesity, can increase the risk of non-insulin dependent diabetes mellitus (NIDDM), tenfold. Fat tissue apparently has two roles in promoting diabetes: it increases the demand for insulin and, in obese individuals; it creates insulin resistance, and, therefore, hyperinsulinemia. It is possible that nutrients are preferably sent into fat for storage. Some of the insulin resistance in obesity can be attributed to a decrease in insulin receptors. Weight reduction in the obese NIDDM can lead to improvement of glycemic control as well as improvement of related medical problems such as hypertension or hyperlipidemia.
Obesity – cardiovascular disease and fat distribution:
In recent findings, an increased risk of cardiovascular disease has been noted with increasing obesity. In a recent finding doctors calculated that, for each 10% increase in body weight in men, there is approximately a 20% increase in the incidence of coronary artery disease. For every 10% increase in relative body weight, the following effects take place:
 Systolic blood pressure increases 6.5 mm/Hg,
Systolic blood pressure increases 6.5 mm/Hg,
Plasma cholesterol 12 mg/dL and
Fasting blood glucose 2 mg / dL.
Most men tend to accumulate fat in the midriff region and both the degree of obesity and the distribution of body fat, independently and collectively contribute to the risk factors for cardiovascular disease. The simplest way to measure the degree of abdominal obesity is to record the waist circumference and divide it by the hip circumference. In men, the risk of cardiovascular disease increases sharply when waist/hip ratio (WHR) is above 1.0. In women the same disease risks increase when the WHR is above 0.8. Numerous reports have indicated that a high proportion of abdominal fat is associated with insulin resistance, hyperinsulinemia, impaired glucose tolerance, diabetes, and an elevated blood pressure.
To assess cardiovascular risk, the Waist-Hip ratio should be used simultaneously with total body fat.
Obesity and cancer: Overweight men have a significantly higher mortality rate for colorectal and prostate cancer; men whose weight is 130% or more above average are 2.5 times more likely to die of prostate cancer during a 20 year follow-up, compared to men of average weight. Women, who have gone through their menopause and have upper body fat accumulation, have an increased risk of developing breast cancer. Overweight women also have higher rates of cancer of uterus and ovaries.
Obesity and endocrine abnormalities: Obese women, especially those with upper body obesity, show more irregularity in menstrual cycles as well as greater frequency of other menstrual abnormalities than normal weight women. They also have more problems during pregnancy with an increased frequency of toxaemia and hypertension. In obese girls, the onset of menarche occurs at a younger age than in normal weight girls. This could be due to the fact that menstruation is probably initiated when body weight reaches a critical mass.
Obesity and gall bladder: Obese women in the 20-30 year age range have a six-fold increase in the risk of developing gall bladder disease compared to normal-weight women. By age 60, nearly one-third of obese women can be expected to have developed gall bladder disease.
For each kilogram of fat, approximately 20 mg/dL of cholesterol is synthesized. In obese persons, the bile is therefore more saturated with cholesterol. Likewise, fatty infiltration of the liver is associated with obesity.
Obesity and pulmonary abnormalities: There are several abnormalities in pulmonary function in obese individuals. As an individual becomes more obese, the muscular work required for respiration increases. In addition, respiratory muscles may not function normally in obese individuals.
Obesity and arthritis: It has also been found that incidence of arthritis is higher in obese people. Although the cause is unclear, there is a significant correlation between uric acid levels, which causes arthritis, and weight. In the 45-64 year old age group, the prevalence of gout goes up dramatically when relative weight is higher by 130%, above desirable. An increase in body weight adds pressure to weight bearing joints. In middle-aged women excess body weight is a major reason for the osteoarthritis of the knee. The good news is that losing weight can, markedly, decrease the chance of developing osteoarthritis.
Obesity and functional and psychological disorders: The obese individuals are slower, more lethargic and inactive. This affects their activities of daily living. Obese patients also have physical incapacity due to back and joint problems and shortness of breath. This contributes to their proneness to fatal accidents and falls.
Research proves that in the severely obese people, there is an increased incidence of absenteeism and unemployment. Discrimination against obese persons is common in both academic and work settings. This leads to significant erosion in their body image, which is the major form of psychological disturbance specific to obese persons. Emotional disturbances are often likely to be a consequence of obesity rather than the cause. However, in some studies, obese persons were found to be significantly less anxious and depressed than normal weight persons.
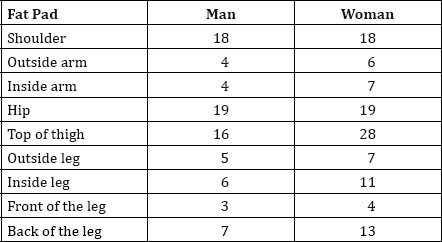
Accumulation of fat is the result of eating more food than the body needs for its daily expenditure of energy. Thus fat represents the body’s main reserve of available energy. The body of a healthy 20-year-old man is about 20% fat. This rises to 25% by the time he is 50. The softer bodies of women contain a correspondingly greater proportion of fat. A 20-year-old girl’s body is 25% fat. This rises to 45% by the time she is 50. Not only do women have a thicker layer of fat under the skin than men, it tends to be concentrated around certain areas, notably the breasts, buttocks and legs.
The table given here demonstrates the distribution of fat pads in the various parts of the body.
The body of a healthy individual is composed as –
Water – 60% (intracellular & extracellular)
Fat – 18%
Protein – 16%
Carbohydrates – 0.7%
Minerals – 5.2%
Fat is distributed in the following manner-
Subcutaneous tissue – 50%
In abdominal cavity – 10-15%
In renal space – 10-15%
Intra-muscular space – 5%
Fat is required for cushioning joints and organs, protection of organs, regulation of body temperature and storing vitamin. So, we can’t eliminate it totally from our diet. But, it definitely needs to be controlled to the desirable level.
Most of us understand that weight management depends upon the energy balance equation; the amount of energy you put into your body (food calories) versus the amount of energy you expend (activity). It is logical that a person consuming more calories, than is required by his body for the daily activities, is likely to store the extra calories as fat. But how do you know how many calories your body needs to reach or maintain a certain weight?
Understanding your body’s energy requirements can help guide you when making nutritional choices. We’ll show you two ways to determine your energy requirements, the accurate way and the easy way.
There are three primary components that make up your body’s energy expenditure. Adding these three components together, basal metabolic rate, energy expended during physical activity, and the thermic effect of food is the most accurate way of determining how many calories your body requires each day.
Basal metabolic rate (BMR) – Most of the body’s energy, about 60-70%, goes to supporting the ongoing metabolic work of the body’s cells. This includes such activities as heart beat, respiration and maintaining body temperature. Here is a simple method to determine your BMR:
For adult males – Multiply the body weight by 10; add double the body weight to this value. [i.e., for a 150 lb male, 1,500 + (2 × 150)=1,800 cal/day BMR]
For adult females – Multiply body weight by 10; add the body weight to this value. [i.e., for a 120 lb female, 1,200 + 120=1,320 cal/day BMR]
Energy expended during physical activity – The second component of the equation depends upon your level of physical activity. Physical activity has a profound effect on human energy expenditure and contributes 20-30% to the body’s total energy output. One of the most reliable methods in calculating calories burned during physical activity is the Metabolic Energy (MET) Method.
Thermic effect of food – The last component to calculate has to do with your body’s management of food. The increase in energy required to digest food is referred to as the thermic effect of food (TEF) and it’s simple to determine:
TEF = total kcals consumed × 10% [i.e., 2,000 kcals consumed/day × 0.10 = 200 kcals expended for TEF]
If all of those calculations seem too confusing or tedious, you can roughly estimate your daily calorie requirements using this simple formula:
For sedentary people:
Weight × 14 = estimated cal/day
For moderately active people:
Weight × 17 = estimated cal/day
For active people:
Weight × 20 = estimated cal/day
(Note: Moderately Active is defined as 3-4 aerobic sessions per week. Active is defined as 5-7 aerobic sessions per week).
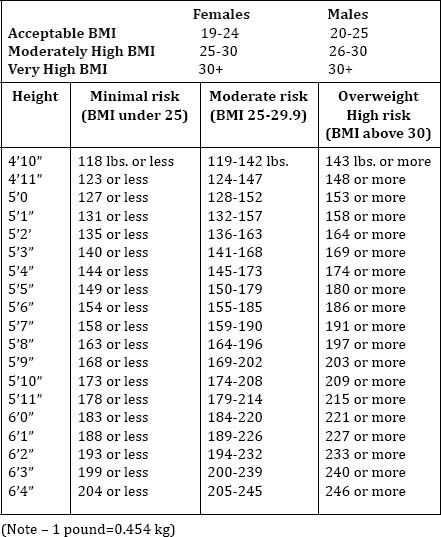
The waist circumference and the body mass index (B.M.I.) are indirect methods to assess a person’s body composition. The waist-to-hip ratio (W.H.R.) is another index of body fat distribution. However, WHR is less accurate than waist circumference and is no longer a recommended measure. What is the waist circumference?
The waist circumference is a simple measure around a person’s natural waist (just above the navel). A high-risk waistline is defined as more than 35 inches (88 cm) for women, and more than 40 inches (102 cm) for men.
The body mass index is a formula to assess a person’s body weight relative to height. It’s a useful, indirect measure of body composition, because it co-relates highly with body fat in most people. Weight in kilograms is divided by height in meters squared (kg/m2). Or multiply weight in pounds by 705, divide by height in inches, then divide again by height in inches.
Use a weighing scale on a hard, flat, uncarpeted surface. Wear very little clothing and no shoes.
Obtain your weight to the nearest kilogram and write it down. With your eyes facing forward and your heels together, stand very straight against a wall. Your buttocks, shoulders and the back of your head should be touching the wall.
Use a ruler held at a right angle to the wall to mark your height at the highest point of your head. Then use a yardstick held flat against the wall to measure from the floor to the point you marked with the ruler. Write down your height in metres to the nearest centimetre.
For example – if your height is 1.65 metres and weight is 59 kgs.

Some people who have trained bodies with dense muscle mass may have a high BMI score but very little body fat. For them the waist circumference, the skin-fold or fat-fold measurements, or more direct methods of measuring body fat may be more useful.
Once you have discovered that you are over-weight, the next step is to lose weight through proper diet and exercise regimen.
![]()