Chapter 8
Living Matter
Most allopathic and holistic therapists alike, when presented with an individual’s infection, will seek to eradicate it using either pharmaceuticals or natural compounds. I know both as a therapist and as a sufferer that this approach has little long-term value (although it may be necessary on occasions) and that invariably the ‘infection’ returns. So what if our fundamental assumptions on this topic are completely wrong? The paradigm that I outline below is most probably a complete reversal of everything that you think you know about infections. It also requires that we trace the roots of this approach back to their inception with Louis Pasteur in 19th-century Paris.
Germ Theory
Pasteur posited that germs could only exist in one form (monomorphism) and that they attacked the organism from without. This is the military model of infection which gives rise to the wish to defend oneself from these invasions and also to the notion that killing the ‘enemy’ microbe will restore order. Since the release of Pasteur’s documents (which he specifically requested remain secret for a hundred years after his death), it has become evident that much of his research was not as claimed at the time. He famously recanted on his deathbed, but by then his deceptions had earned him and his theory the pre-eminent place in history he had probably wanted. Pasteur’s Parisian contemporary and rival, Antoine Beauchamp, had proposed a competing theory (which was eclipsed by Pasteur’s germ theory) he called pleomorphism. In it he maintained that microbes can take a variety of different forms and are generated within the individual from granules in the blood and cells (which are clearly visible in live specimens) in response to changes in the terrain. His work was later confirmed by many others, including Dr Günther Enderlein, who identified the granules as being micro-organisms that he called ‘endobionts’. Dr Enderlein observed that under increasingly acidic conditions, these endobionts morphed first into bacteria, then fungi and finally, under extreme conditions, into viruses. In those who primarily eat a natural diet high in fruits and vegetables alkaline conditions will prevail, whereas the modern diet of refined and processed foods is acid-forming. The endobionts’ ultimate function is to serve as an inbuilt mechanism that biodegrades living matter and returns it to the soil from which it arose. This theory may also explain why microbes possess such sophisticated means of controlling their host’s behaviour using small molecules (which are often toxic) to communicate with the host’s brain.
Infection is no war in which the body is fighting invaders. The bacteria that come to these sites are symbiotic and help the body in elaborating dead cells and tissue for expulsion. Infection … is a body cleaning process for a body burdened with toxic materials.
T C Fry
There is obviously enough truth in Pasteur’s theory for it to have survived over a hundred years and whilst bacteria and viruses may be infective once generated they also require a hospitable terrain in which to multiply. This explains why some people do not catch colds or even HIV when exposed to the causative agents and why some survived the great plagues that claimed so many lives. This also accounts for why most people test positive to most microbes. The organisms responsible for MRSA and meningitis, for instance, are both commonly found, so why do they become such potent pathogens in some and yet appear to co-habit perfectly well in others?
To advance this theory further, what if this mechanism is nature’s way of dealing with pathology? What if the microbe, rather than being our foe, is our greatest ally? When all potential detoxification routes are overwhelmed, causing toxins to back up in the tissues, is it possible that these organisms are generated in order to clean up or bind these toxic wastes to prevent them harming the individual? This may only be intended as a temporary measure until the processes of detoxification can resume. However, if no such reversal is ever forthcoming, is it then possible that parasite eggs (to which we are all constantly exposed) may develop in this compromised system in order to further bind and engulf the microbes?
Using any method – allopathic or holistic – to kill microbes and parasites is a ‘germ theory’ approach and is treating a symptom rather than a cause. It can also be counterproductive because the microbes or parasites release their cargo of toxic metals in addition to many other noxious breakdown products. Heavy overgrowth of any microbe then is a response to toxicity and the amount of necrotic tissue being generated. The pathologists in Mozart’s Vienna were apparently all too familiar with the grey organs in the bodies of those who had died of mercury poisoning. Can you imagine how compromised the circulation must have been and how much necrotic tissue, toxicity and fungal overgrowth there has to be before organs actually become grey? The endobionts have effectively been signalled to start their job of decomposition whilst these unfortunate individuals were still alive and this may be the process at work in FRS!
Unlike bacteria and yeasts, viruses are not regarded as living, because they are just genetic material in a protective outer shell with an injecting mechanism. They function by inserting their genome into the host’s cells and in this manner can control the cell’s functions and use the cell to replicate.
What hope is there for medical science to ever become a true science when the entire structure of medical knowledge is built around the idea that there is an entity called disease which can be expelled when the right drug is found?
Dr John H Tilden, MD
The Appearance of Infectivity
There are several possibilities that might account for the appearance of infectivity.
• The first is that we all collectively become vulnerable through vitamin D deficiency as we head into the winter months.
• The second is that with toxicity comes cell death and the dismantling of the cell’s components for recycling (known as apoptosis). Viruses may be the fragments of genetic material that are being packaged for transport and not the cause of the destruction.
• Another theory relates to the fact that we are all passengers on a planet hurtling through space at unimaginable speeds. On our adventures in outer space we travel through photon bands and are subject to local changes in background electrical and magnetic radiation. This is in addition to the daily, monthly, seasonal and annual cycles we are all familiar with, the solar flares and sunspots generated in our own solar system and the changes in barometric and atmospheric conditions that occur with changes of weather. Epidemics have a history of burning around the globe and then dying out – often against a background of deprivation as with the great flu epidemic at the end of the First World War. These may be generated in some way we don’t fully understand by the global conditions to which we are all exposed. This may be allied to the theory that viruses may have ‘hitched a ride’ in our DNA for one or more generations and are actually being expelled from the cell under certain atmospheric conditions.
So in summary, it is man-made toxicity that is the problem and not nature, which is working in our best interests at all times. Of course, we have only polluted our bodies with the same careless disregard that we have shown our host planet and in a holographic universe how could it not be thus?
The part can never be well unless the whole is well.
Plato
Chronic and Recurrent Infections
For the reasons outlined above and because the delicate mechanisms of the immune system have been poisoned, chronic and recurrent infections are a universal issue in FRS. In the following section, we examine the various microbes and parasites that are frequently associated with the failing health of FRS. However, focusing on the particular ‘infective’ organism rather than on changing the terrain to encourage a more normal ecology might be a giant allopathic germ theory ‘red herring’!
Bacterial Infections
The bacteria associated with salmonella, pneumonia, chlamydia and tuberculosis and a particular subset of bacteria known as mycoplasma are all suspected of involvement in FRS. However, by far the most important bacteria is Borrelia burgdorferi which is associated with Lyme disease or borreliosis, and we examine this in detail below.
Lyme Disease
Lyme borreliosis is a spirochete infection contracted from a tick bite in much the same way as malaria is transmitted by mosquitoes. Deer, cows, sheep, cats, birds and rodents can all carry these ticks, which, possibly because of global warming appear to be flourishing and now inhabit areas that previously did not pose a problem. The initiating tick bite will induce an angry rash, but for many FRS sufferers this event is lost in the mists of time. In the early stages the individual may have headaches and flu-like symptoms, but the disease can then progress to affect almost any body system and mimics other infections, for which Lyme disease has earned the title ‘the great imitator’. Secondary sites of infection can cause muscle and joint pains, arthritis, heart abnormalities, neurological and psychiatric complaints and/or profound fatigue. Although the initial infection is probably contracted via a tick bite, it seems to be possible for the disease to be passed to intimate family members and certainly from mother to child through the placenta. Lyme disease is one of the fastest-growing infectious diseases and whilst it seems to be carried by a majority of people, it often finds a hospitable environment in those suffering with mercury toxicity. The ubiquitous staphylococcus is closely related to borrelia and it may also be that the body does not mount an effective response to borrelia, mistaking it for its less aggressive and more familiar cousin. Antibiotics are ineffective against borrelia and this may be because the heavy metals that encourage growth of these bacteria also deactivate the antibiotics deployed against them.
Fungal Infections
Fungi propagate by releasing spores (their yeast form) which, when they settle upon a suitable substrate can grow into their filamentous mould or fungal form. There are several fungi that are associated with FRS including various members of the Candida family. Although fungi reproduce asexually (usually resulting in identical ‘copies’), Candida has developed a means of changing its genes dynamically in response to its environment and so has created a huge family tree. Several members of the Candida and Aspergillus families of moulds have been implicated in FRS, however Candida albicans is widely regarded as being the most common fungal infection found in FRS and is examined in detail below.
Overgrowth of Candida Albicans
Candida: It may not kill you, but it will take your life.
David Newman
Candida albicans is a commensal yeast that is found practically universally on skin and in the intestines. Its growth is normally checked by the 500 other organisms it cohabits the intestines with and is ultimately controlled by the immune system. However, in recent decades candidal overgrowth has become an increasing issue with many people exhibiting persistent and very resistant overgrowth of this yeast. Women tend to suffer from candidiasis more than men and this may be because oestrogen encourages the growth of Candida.
There may be many factors that contribute to candidal overgrowth including:
• The almost universal exposure to antibiotics which kill all the endogenous ‘friendly’ bacteria, thus removing one of the main factors controlling the spread of Candida.
• Drinking chlorinated water and the use of preservatives in foods which, in addition to killing any pathogens, also kill the friendly bacteria in the intestines.
• The use of steroid drugs such as asthma inhalers, corticosteroid creams, the contraceptive pill and HRT which suppress the immune response.
• A diet deficient in fruits and vegetables and rich in sugars, dairy, refined carbohydrates and yeast-containing foods which promote overgrowth of Candida.
• The use of pharmaceuticals – especially ulcer drugs, tranquillizers, sleeping pills and antacids and the frequent use of over-the-counter medication such as painkillers and any recreational drugs.
• Chronic stress, which raises blood sugar levels and depresses the immune system.
However, the single biggest reason for epidemic overgrowth of Candida albicans relates to the use of mercury in dental amalgam and we will examine this in more detail below. Candida is able to convert mercury from one form to another and also to generate energy in the process. The immune system is also adversely affected by the presence of mercury which means that wherever mercury is stored, candidal overgrowth will be supported.
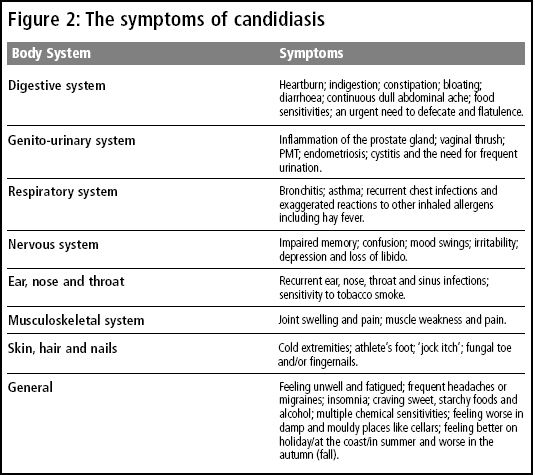
In nature, yeast spores which land on a fallen leaf, for instance, will change into their fungal form with mycelia that penetrate into the body of the leaf and that also perforate through the leaf where they release more spores. Normally our intestinal lining acts as a barrier between our tissues and the contents of our intestines which are technically outside the body and there is selective absorption of chemicals from digested food across this membrane. However, the ‘roots’ of the mycelial form of Candida penetrate between the cells of the intestinal lining and release spores – this time into the lymph and blood circulation of the host. By breaching this barrier the Candida is able to release the approximately 90 toxins that it produces into the body, making the host feel generally unwell. In the process, the Candida also creates a ‘leaky gut’, whereby foods are absorbed into the circulation before they are properly digested. These large food molecules are then identified by the immune system as ‘foreign proteins’ and attacked in the same way as a bacterial infection would be. In this fashion, multiple food intolerances can develop and become more severe and more numerous as the intestinal lining becomes ever more ‘leaky’. In addition, the spores released into the circulation can colonize other organs by changing into their fungal forms and thus breaching their membranes. This process is responsible for the myriad different and often confusing symptoms of FRS detailed in figure 2.
Treatment of Candidiasis
Whilst treating candidal overgrowth with anti-fungal medications or herbs may provide some temporary relief from symptoms, some people can become indefinitely dependent upon these methods as they experience worse symptoms every time they try to wean themselves off the medications. Also, whilst the drugs kill Candida, they may allow other fungi and organisms to proliferate, thus compounding the problem. Candida is estimated to produce up to 400 highly toxic substances when it dies, and instigating a massive drug-induced Herxheimer reaction (die-off) in someone whose organs of excretion are already heavily compromised floods the system with toxins and can produce some very unpleasant symptoms. This approach most probably results in the re-storage of these toxins in possibly more vulnerable organs and tissues and this process is known as retoxification. Two of the drugs most commonly used (Ketaconozal and Nystatin) are quite toxic to the liver in addition to inducing die-off and may not cover the full spectrum of yeasts. The goal of effective treatment has to be to remove the cause – which is largely mercury – while supporting the organs of excretion and providing the high-quality nutrients the body requires to regenerate.
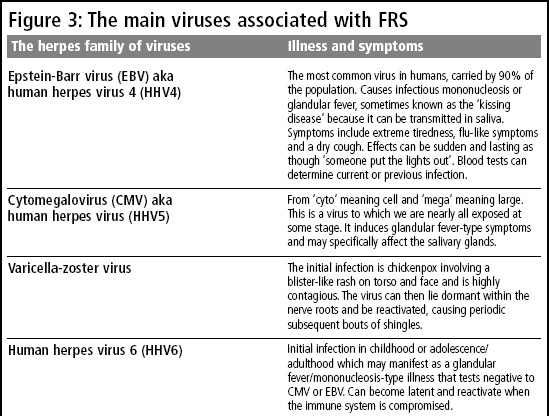
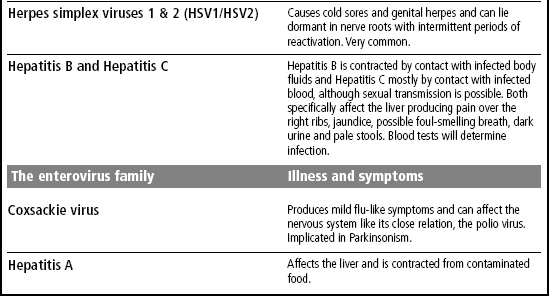
Viral Infections
Many viruses have the ability to lie low for decades and possibly lifetimes within the cells whilst evading destruction – and this is known as latency. This can be clearly witnessed in the particular case of an initial herpes simplex viral infection and the recurring cold sores that can affect the individual over a lifetime thereafter. As mercury toxicity is addressed, usually several latent viruses will appear that the body will require support in clearing. Although many viruses have been suspected of involvement in FRS including enterovirus, adenovirus, parvovirus and various so-called ‘stealth’ viruses, the spotlight seems to have fallen upon the herpes family of viruses. These viruses derive their name from the word ‘to creep’ and this refers to the insidious nature of their infection, latency and recurrence. Please see figure 3 for a list of these viruses and their associated illnesses.
Parasitic Infections
Unlike bacteria, fungi and viruses which may arise from within, parasites are acquired from the environment but find a supportive milieu in which to grow. A parasite is an organism that lives in or on a host and either feeds on the host’s tissues or competes with the host for nutrients and usually produces substances that are toxic to the host. There are at least a hundred types of common human parasites ranging from the microscopic to large intestinal worms. Parasitic infections are actually very common, with only the obvious ones being acknowledged, such as head lice. In fact, they are the single biggest cause of death and illness in the world and half the population of the developed world carries at least one parasite – and a quarter of those have an active infection. Giardia lamblia is the fourth most common parasite in the world with one in five having been infected at some time in their lives; half of all sufferers of irritable bowel syndrome carry the parasite. Forty per cent of children in developed countries have had more than one parasitic infection and parasites are often a factor in chronic disease, with one in five chronically sick people testing positive for their presence. It is possible that the primary causes of parasitic infections include inadequate stomach acid (which kills parasite eggs) and inadequate digestive enzymes and bile. This means that improperly digested proteins can support parasite growth within the intestine.
Over the millennia, parasites have evolved sophisticated mechanisms to evade destruction by their host’s immune system and to produce cravings for their preferred foodstuff in their host. They can also multiply at an incredible rate producing thousands of eggs a day and many parasites have developed a ‘belt and braces’ approach to avoiding removal such as the tapeworm, which attaches itself to the intestinal lining using both suckers and hooks. Many also have complex life cycles involving different hosts and quiescent and active phases, so laboratory tests often fail to correctly identify parasitic infections.
Sources of Parasites
Like fungal spores, parasite eggs are found everywhere. The most common method of transmission is through drinking contaminated water or eating undercooked meat or fish. Fruit and vegetables can be cross-contaminated during preparation by infected meat products or may carry soil that harbours eggs or cysts. Many cases of infection are through unwitting faecal–oral contact by those involved in food preparation or packing not washing their hands after going to the toilet. Other methods of transmission include direct sexual contact, inhaling contaminated dust, insect bites, walking barefoot and contact with infected pets or animals.
The Symptoms of Parasitic Infection
There is no part of the body that is immune to parasitic infection. One third of parasites inhabit the digestive tract, the other two-thirds invade the brain, the muscles, the heart, the thyroid gland and other tissues. The symptoms that parasites produce are many and varied and include: erratic bowel habits with alternating constipation and diarrhoea, foul-smelling stools, sore breasts (not related to the menstrual cycle), flu-like symptoms, an itchy anus (especially at night), weight loss and fatigue. Addressing an inadequate digestive system and the underlying metal toxicity will ultimately help the immune system to tackle these unwelcome guests.
Vaccinations
The road to hell is paved with good intentions.
Samuel Johnson
The term vaccination comes from the Latin ‘vacca’ for cow. Vaccination began in 1796 when Dr Edward Jenner injected pus from the blisters of a milkmaid suffering with cowpox into his gardener’s young son. It had been observed that milkmaids who had contracted cowpox appeared immune to smallpox. This theory, happily, was borne out when he subsequently injected the child with smallpox and the boy did not contract the disease. Unfortunately, many of the viruses and other microbes that require treatment during a programme of metal detoxification appear to have been introduced, albeit unwittingly, by vaccinations. The technique for production of vaccines often involves taking pus or lymph from an infected person or animal and then cultivating it on decomposing animal tissue such as chicken eggs, monkey kidneys or aborted human foetuses. An adjuvant or poison such as aluminium sulphate is then added to this material in order to provoke an immune reaction when injected. This means that a two-month old baby in the US will have been exposed to more than 50 times the recommended ‘safe’ levels of aluminium by the vaccination schedule. This material is then preserved in a base containing such substances as mercury (thimerosal), formaldehyde or squalene. Vaccinations can introduce live material such as that used in the BCG, MMR, oral polio and chickenpox vaccines or ‘inactivated’ material such as that in the Polio (Salk), DPT, hepatitis B, HIB and meningitis vaccines.
A bit like a medieval castle, the body presents a series of defences that ramp up from being fairly general to highly specific as each layer is breached, with the production of antibodies by the immune system as the ultimate response. Initial defences include skin and mucous membranes and their secretions and the acid environment of the stomach which kills swallowed pathogens. The immune system functions by reacting to and ‘memorizing’ a particular protein on each pathogen. The researchers at the pharmaceutical companies try to establish which part of the microbe the immune system is responding to and then attempt to isolate and introduce this part in an inactivated form. The goal is to provoke the body into responding and storing the appropriate immune ‘memory’ without exposure to the dangerous pathogen.
Some problems inherent in this approach are listed below.
• The material may not be as harmless or as inactive as is assumed.
• We don’t normally encounter three diseases at exactly the same time, however, with the DPT or MMR vaccines, several immune challenges are administered together. This may overwhelm the most robust of systems, but may prove especially challenging to the immature immune system of a young child.
• The effects of the toxic metals that are added to the vaccine are highly detrimental and synergistic. For example, the dose of aluminium and of mercury that would separately kill 1 per cent of laboratory rats, when combined kills all of the experimental rats.
• The chemical constituents such as thimerosal, aluminium sulphate and formaldehyde are injected along with possibly multiple pathogens and may combine to adversely affect the immune system.
• Many vaccinations are given long before the infant’s immune system has had a chance to start functioning effectively and the sheer number of assaults on young immune systems may also be an issue. Children in the UK receive 9 vaccinations before the age of 3 years old and 16 vaccinations by 15 years of age and children in the US receive multiple vaccinations against 11 different diseases before the age of 6 years old.
• The exposure to multiple doses of the mercury preservative thimerosal alone may have very deleterious effects on the developing child.
• Normally when you encounter a pathogen, it has to breach all your outer defences before gaining entry to the inner sanctum of your circulation and immune system. When foreign substances are encountered in this way Th 1 lymphocytes are produced which results in lifelong immunity. With vaccination the infected material is introduced directly into the circulation without the priming that might have occurred if this were to happen naturally. Also, the immunity that vaccination provides may only be shortlived as it is Th 2 lymphocytes, rather than Th 1 lymphocytes, that are stimulated.
• The use of animal material in production means that the vaccine includes fragments of animal RNA and DNA. Other contaminants that have been identified include retro viruses (which can cause cancer in animals), simian (monkey) cytomegalovirus in polio vaccine and chicken viruses in measles vaccine.
• In addition to the additives mentioned elsewhere vaccines may also intentionally include phenol, acetone, glycerin and monosodium glutamate (MSG). Additionally and unintentionally they may also contain faecal matter, animal kidney or brain, animal blood and serum, yeast proteins and antibiotics.
• Perhaps most remarkably, very few long-term studies have been done on the safety or efficacy of vaccinations!
• Whilst vaccination may or may not afford protection from specific diseases, what price might we inadvertently be paying? Are the current explosions in the incidence of asthma, hyperactivity or autism a result? If vaccinations have life-long benefits as is claimed, why too can they not have life-long consequences?
• No meaningful data of adverse effects are kept as symptoms have to manifest within a remarkably short period of time to be legally attributed to the vaccine. However, the sudden illness of George Fisher, a healthy toddler, the day after vaccination and his subsequent death 10 days later was deemed by a UK court in 2008 to have occurred ‘too soon’ to have been caused by the vaccine!
• So keen are the medical profession on the vaccination programme, that they now want to introduce vaccinations for babies against hepatitis B and cervical cancer. The threat posed by these diseases may never be encountered and certainly not for decades, so is it entirely appropriate that young babies are subjected to this additional immune insult?
• Perhaps, most shockingly, there is little evidence that vaccinations work. Many people who have been vaccinated subsequently contract the disease that they have been vaccinated against but doctors will attribute whooping cough to bronchitis or asthma for instance – assuming the vaccine to have been effective. Also, only 10 per cent of the world’s population was ever vaccinated against smallpox and yet this disease died out in unvaccinated populations too.
• Vaccinosis is a term used by veterinarians to refer to the overuse of vaccinations producing chronic ill health and even death in animals, and you have to wonder why this is not also acknowledged in humans.
• There is a great deal of evidence to show that there had been a massive decline in incidence of many of the diseases that we vaccinate against before the vaccination programme was introduced. This can be attributed to the provision of clean water and proper sanitation, improved nutrition and hygiene, and better housing providing relief from the squalid and overcrowded conditions that the majority of people lived in.
• Fundamentally, these microbes may arise from within rather than infecting us from without as discussed previously, so the whole concept underlying vaccination may be based on a false premise.
• Last, but not least, the body does not need to be introduced to every pathogen it is ever likely to encounter in order to effectively combat it. The immune system works on the basis of defending against proteins it does not recognize (non-self) as opposed to those belonging to the body (self).
The harm for you may already have been done. However, where you can avoid the need for vaccination, such as choosing holidays that do not require vaccinations for tropical diseases like yellow fever, try to do so – at least until you are considerably stronger. If you have a child, make sure you really understand the risks you might be exposing your child to in having a vaccination. If there is any history of autism in your family, consider the consequences very carefully indeed, because an autistic spectrum response to vaccinations tends to run in families. Also, if your family has a history of immune disorders such as eczema, asthma or autoimmune disease, ensure that you are fully informed, as an adverse reaction to vaccination is more likely in these individuals.
Miasms
Before finally leaving the subject of infective organisms, it is worth mentioning the concept of miasms, created by the father of homeopathy Samuel Hahnemann in the 19th century. Miasms are predispositions to certain illnesses that have been handed down through generations from our antecedents who were exposed to the many plagues that swept through Europe in the Middle Ages. This has resulted in four predispositions against which an individual may struggle for an entire lifetime unless treated. Most people carry two miasms (one from either parental line), and a practitioner versed in homeopathy will be able to address this aspect of treatment.
Dental Infections
The once widely accepted notion of ‘foci of infection’ fell out of favour in the 20th century, but is being embraced again in the light of recent evidence. The concept is that the mouth in particular can become a reservoir from which infective agents can colonize other regions in the body and from which their noxious products can spread, affecting overall health. The three main oral sources of infection that the FRS sufferer needs to be aware of are addressed below.
Root-Filled Teeth
The body of the tooth is composed of dentine (ivory) which is formed from hundreds of thousands of tiny tubules that run from its surface to the central chamber within that contains the nerves and blood and lymph vessels (the pulp). In a single-rooted incisor (front tooth) there is an estimated 5 km (3 miles) of tubing and in a molar (back tooth) there may be as much as 12 km (10 miles). In addition, the pulp canals within the tooth (normally one per root) have many tiny lateral canals that provide accessory circulation and perforate the body of the tooth from the surface to the interior. Endodontically treated (‘endo-’ means within and ‘-dont’ means tooth) or root-filled teeth in which the dead or dying pulp has been removed and the canals have been cleaned and filled have, by definition, no circulation. It is claimed that the normally benign streptococcal bacteria – especially the diplococci and short-chain Streptococcus viridans – mutate into their pathogenic forms in the absence of oxygen. This occurs in the 30 per cent of teeth with additional canals which may have been missed, in the tiny lateral canals and in the vast system of dentinal tubules. These bacteria can then release very toxic substances that cannot be combated by the immune system. Some teeth present an obvious problem on x-ray, with a dark shadow of a cavity produced by fibrous or abscessed tissue showing clearly against the lighter surrounding bone. However, many x-rays miss infections that lie in front of or behind the tooth being x-rayed. Any tooth with a poor root-filling or such an area is suspect, as is any tooth that you know to occasionally get infected or to be problematic.
The early 20th-century dentist and nutritionist, Dr Weston Price, found pus to be sterile and an indicator of successful quarantine by the body. What is claimed, however, is that in those with severely compromised immune systems, the body is unable to mount a response to this toxic assault and so there are no overt signs of a problem on an x-ray. For this reason, some authorities recommend the removal of all root-filled teeth if you are seriously or chronically ill. Consulting a kinesiologist or a practitioner skilled in Vega testing or using the DIY muscle testing outlined in the Appendix may indicate whether a tooth is likely to be a problem. Alternatively, you will have to make this decision for yourself, taking into consideration the chronology of your illness and how it relates to any dental treatment or problems and, ultimately, how compromised your health is. Dr Price considered that if the previous two generations of your family have been resistant to degenerative diseases, then root-fillings are not normally likely to present an issue. However, he found that those with a family history of serious illness were more vulnerable to the adverse effects of root-fillings. Certainly some root-fillings (historically probably the majority in the UK) have been done using a filling material which combines an antibiotic and a steroid paste rather than compacting a relatively inert material to obturate the canal system of the tooth. These teeth can certainly present a toxic cocktail when opened, frequently smelling awful. Another sign that many dentists might pass over as being of no consequence is that of condensing osteitis (oss-tee-i-tis), which shows as a dense white area around the tip of the root, and this can also indicate a toxicity problem originating from the tooth.
‘Cavitations’
Also implicated are neuralgia-inducing cavitational osteonecrotic (NICO) lesions or what have come to be known as ‘cavitations’ which occur when a tooth – possibly infected – was extracted without removal of the surrounding periodontal membrane (the fibrous ‘joint’ that attaches teeth to the jawbone). These can subsequently form ‘chambers’ within the bone which can harbour anaerobic bacteria which produce toxins such as hydrogen sulphide and methylthiol which can then enter the circulation, detrimentally affecting the body. Cavitations most commonly appear at the sites of lower molar and lower wisdom tooth extraction.
Gum Disease
The majority of people also have some degree or other of periodontal disease (also known as periodontitis or gum disease) and this, too, can be the site of a large number of anaerobic bacteria gaining ready access to the body. It is estimated that the infected area (although hidden from view) is equivalent to that of a tennis ball in someone with moderate periodontal disease. Healthy gums do not bleed, so if you think you may have gum disease and don’t feel that your dentist is addressing the problem properly, ask for a referral to a periodontist (gum specialist). This may cost some serious money for deep cleaning around the roots of all your teeth and you will have to be diligent yourself about brushing and flossing on a daily basis thereafter.
It certainly seems to be worth asking your dentist if any of your teeth seem chronically infected or if there are any apparent cavitations on x-ray. If you have a troublesome tooth or teeth that you have been ‘hanging on to’ and you have an FRS it would seem to be a good idea to consider the possibility of extracting the affected teeth. It is also worth taking good daily care of your mouth by brushing with a non-fluoride toothpaste and flossing as well as seeing the hygienist and/or dentist regularly. Dental treatment is discussed further in chapter 18.