12
HIV/AIDS
Despite the global threats of SARS (severe acute respiratory syndrome), bird flu, and Ebola virus, AIDS (acquired immunodeficiency syndrome) is perhaps the most feared disease on the planet. Often fatal, especially in developing countries, it slowly destroys the immune system until the individual is vulnerable to a wide variety of diseases that rarely affect noninfected persons. These diseases, such as Pneumocystis jiroveci pneumonia and Kaposi sarcoma, may affect the brain, lungs, eyes, or other organs. Persons with AIDS also can experience debilitating weight loss, diarrhea, weakness, and depression.
AIDS has been the most controversial disease of our time. Because it first affected primarily homosexuals, bisexuals, and intravenous drug users in the United States, critics charge that society’s negative feelings toward these groups led the government to be slow to respond to the growing epidemic. Today infection is greatest among intravenous drug users in North America, followed by those who became infected through heterosexual transmission and homosexual transmission. There is also a great deal of controversy surrounding the methods used to treat persons who are infected with the virus believed to cause AIDS—HIV (human immunodeficiency virus)—and those who reveal one or more symptoms of the disease.
AIDS has given birth to an entire “industry” involving physicians, nurses, hospitals, pharmaceutical companies, medical equipment manufacturers, government agencies, insurance companies, alternative therapists, testing laboratories, AIDS counselors, support groups, information networks, writers, publishers, researchers, educators, and magazines. Billions of dollars are involved in AIDS research, treatment, care, prevention, and education.
Physicians, scientists, and laypeople advocating the use of ozone and hydrogen peroxide can be included in this group. Some are motivated by altruism and the desire to serve humanity; others are primarily interested in money. For many providers of goods and services to AIDS patients, this epidemic has become an economic windfall of gigantic proportions.
By 2006 more than one hundred approved or experimental drugs for HIV-related problems were used in the United States. These included protease inhibitors (PIs), which prevent T cells that have been infected with HIV from producing new copies of the virus, as well as nucleoside/ nucleotide reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs), and entry inhibitors, all of which prevent healthy T cells in the body from becoming infected with HIV. In addition, a wide range of medications have been developed to help control opportunistic diseases associated with HIV, including bacterial infections, malignancies (cancer), viral infections, fungal infections, protozoal infections, neurological conditions, sores, low platelet counts, and wasting syndrome.
Many of these new medications have brought about suppression of symptoms, longer life, improved quality of life, and hope to millions of people who have been infected with HIV in countries where they are able to afford them. However, like all medications, those for treating HIV have side effects. Depending on the drug, they can include nausea, vomiting, rash, diarrhea, stomach pain, loss of appetite, pain in the arms and legs, anemia, muscle wasting, and tingling, pain, or numbness in the hands and feet (peripheral neuropathy). In rare cases liver and pancreatic damage can result from taking such medications. Another problem is that some of these drugs lose their effectiveness over time, so other medications are constantly being developed.
The total cost of these medications easily runs into the tens of billions of dollars each year. For example, a recommended “cocktail” of two protease inhibitors (six 400 mg tablets of Crixivan and two 100 mg tablets of Norvir) costs approximately $33 a day (more than $12,000 a year) per patient, even if no other medications are used. Some individual drugs, like Fuzeon (marketed by Hoffman-La Roche), carry an annual price tag of $20,000 a year or more. In addition to the pharmaceutical companies themselves, many physicians, hospitals, and insurance companies involved with AIDS have discovered that this disease is a big source of income and profit. For this reason, the quest to find inexpensive therapies and modalities to treat the disease has never been a high priority.
Since the late 1990s, several developing countries—such as India and Brazil—have begun developing their own medicines to combat HIV, often using the patented formulas of the pharmaceutical companies. As a result, they have been able to make the drugs available to patients at less than one-tenth the cost of patented drugs sold in developed countries like the United States. Yet even with these lower costs, the Joint United National Programme on HIV/AIDS estimated that $12.3 billion would be needed for treatment and care alone for patients living in low- and middle-income countries between 2006 and 2008.1
This has led people infected with the virus to explore other avenues of treatment, often using a combination of traditional and nontraditional approaches, including nontoxic therapies like acupuncture, acupressure, Chinese and/or Western herbs, ayurvedic medicine (an ancient Indian healing tradition that stresses diet and herbal medicines), homeopathy, chiropractic, ultraviolet blood irradiation (UBI) therapy, and nutritional therapy.
Oxidative therapies—especially when combined with either traditional therapies or other natural methods—make up one of these approaches. The potential of ozone and hydrogen peroxide for helping people with HIV and AIDS is enormous, because laboratory evidence has shown that ozone and hydrogen peroxide can inhibit (if not kill) the virus believed to cause AIDS. This result is deceiving because ozone can inactivate HIV only in a saline solution in vitro. How does this happen?
Figure 12.1 depicts a chemical model of a virus that is about to infect a cell. It also shows how ozone can affect the process of infection. The virus is encapsulated in an envelope made of lipids (fats or fat-like substances). Tiny bulbs on the virus spikes are known as receptors. It is through these receptors that a virus can connect with, and eventually infect, other cells.
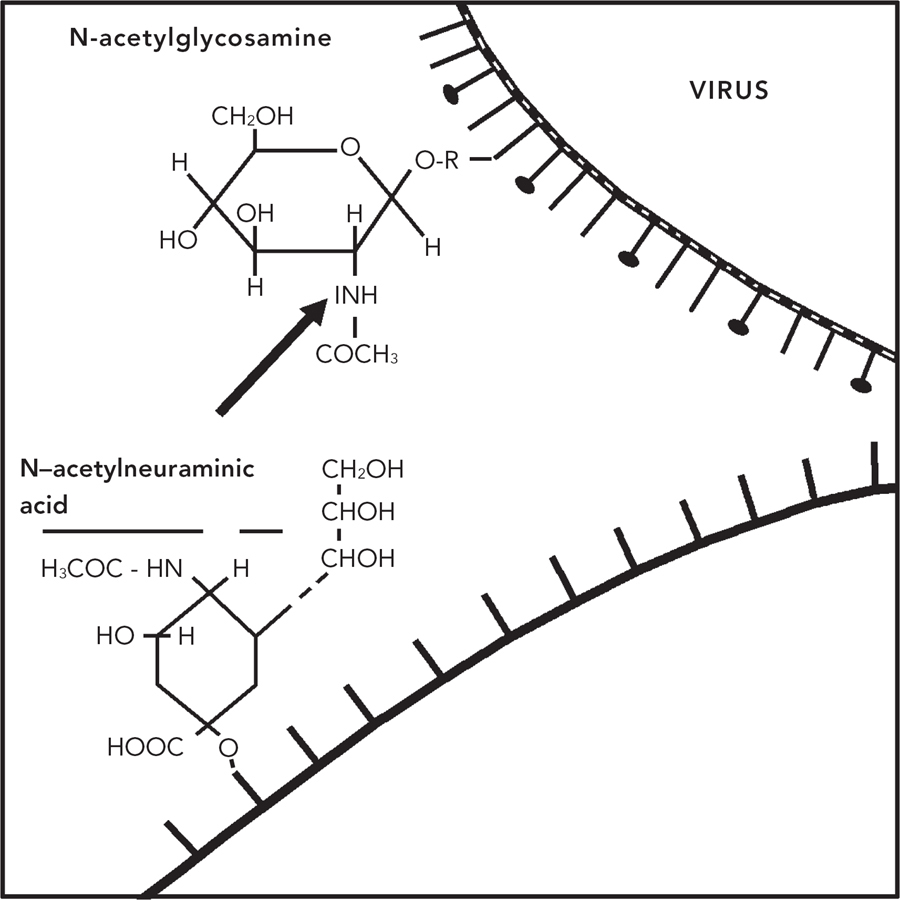
Figure 12.1. Chemical model of a virus and its encounter with ozone. (From Siegfried Rilling and Renate Viebahn, The Use of Ozone in Medicine [Heidelberg: Haug Publishers, 1987], 43. Reprinted courtesy of Dr. Siegfried Rilling and Haug Publishers.)
With the application of ozone or hydrogen peroxide, several events rapidly take place. The virus spikes are inactivated because the addition of ozone to the blood changes the structure of the receptor. Although still alive, the virus cannot join with the cell. At the same time, the ozone oxidizes the virus’s outer envelope.2 Without this envelope, it cannot survive.
In addition to the effects of hydrogen peroxide introduced from outside the body, the threatened cell naturally defends itself by producing its own hydrogen peroxide. In some cases, especially when the cell is unhealthy to begin with, the hydrogen peroxide produced by the cell causes it to “burst” before reproduction of the virus can take place. In other cases the peroxides introduced by added ozone or hydrogen peroxide act synergistically with the hydrogen peroxide inside the cell, destroying any virus that has penetrated it.3 Stated more simply, if the cell is unhealthy to begin with, it is destroyed by a hydrogen peroxide burst. If it is strong, it kills off the virus and becomes even stronger than before due to the increased oxygenation brought about by added ozone or hydrogen peroxide. As a result, the virus is either inhibited or destroyed.
Another possible benefit of ozone therapy for people with HIV is its ability to stimulate the production of superoxide dismutase, a vital enzyme that catalyzes the conversion of two molecules of superoxide into one molecule of oxygen and one molecule of hydrogen peroxide. According to a report in American Medical News, researchers at the Webb-Waring Institute in Denver, Colorado, discovered that HIV inhibits the body’s natural production of superoxide dismutase. Indeed, HIV, like many other viruses, induces a chronic oxidative stress that aggravates the disease. The news release added that researchers are testing human cell cultures to determine whether a drug can inhibit HIV’s ability to suppress the enzyme. They believe that if they are able to safeguard the enzyme’s levels in cells, the time during which HIV stays inactive could be prolonged. This finding points to the value of ozone therapy in helping prevent HIV-related symptoms from manifesting.4
As immunomodulators, ozone and hydrogen peroxide can also strengthen a compromised immune system. They can help guard against opportunistic infections and enable persons suffering from the disease to lead longer, more active, and more productive lives. While oxidative therapies should not be considered a cure for AIDS, they may open the door to long-term remission, especially when used in synergistic combination with other immune-strengthening therapies. Investigations are now taking place to delineate such combinations, including ozone and/or hydrogen peroxide and oral alpha interferon, staph vaccine, lentinan (shiitake mushroom extract), and Chinese herbs. Readers interested in updates regarding these combinations may contact an organization called Keep Hope Alive (see the list of organizations in appendix 2).
ONE CAUSE?
Although few people disagree that AIDS destroys the body’s immune system, many researchers, physicians, and patients have taken issue with the “one cause” theory for AIDS and the established approaches for treatment. One approach states that the person is already immunosuppressed and that the HIV virus, if it is a factor at all, is only taking advantage of a previously compromised immune system rather than being the cause of it.
Michael Ellner, from the former New York alternative AIDS organization HEAL (Health Education AIDS Liaison), regarded “AIDS as a condition of toxicity rather than a viral disease; it is a disturbance of immune function caused by a lifetime of toxins.”5 His view was also proposed to me during a 1994 interview with Dr. Juliane Sacher of Frankfurt, Germany, who had one of the largest medical practices treating AIDS patients with ozone in Germany. She placed special emphasis on the combined effects of air pollution (especially in the large cities), the growing number of pesticides in our food supply, the widespread use of antibiotics and other immune-suppressing drugs, recreational drug use such as “poppers” (isobutyl nitrite, butyl nitrite, and amyl nitrite), eating heavily processed and devitalized foods, and a variety of vitamin and mineral deficiencies that occur as a result. For this reason, she believed that a greater emphasis should be placed on building up the person’s immune system while assisting the patient to become (and remain) as free of toxins as possible.6 However, some researchers, like Dr. Bocci, believe that to dismiss the relevance of the virus is untenable, although other immunosuppressive factors can accelerate the progression of the disease.7
Although I cite laboratory evidence that ozone can inactivate the human immunodeficiency virus (and that some people who once tested HIV-positive revert to HIV-negative), I reiterate that neither ozone, hyperbaric oxygen, nor hydrogen peroxide is a cure for AIDS. However, if correctly applied, they can play an important role in a holistic approach to treatment. This perspective was succinctly expressed in a communication from Frank Shallenberger, M.D., H.M.D., of Nevada, who was among the first practitioners to treat HIV patients with ozone and other natural therapies:
1. Ozone therapy does not cure AIDS. [It] never has and probably never will.
2. AIDS has a multifaceted causation and is not an infectious disease. Therapy for AIDS will never work if it is only aimed at anti-infectious protocol.
3. Ozone therapy works in AIDS by acting as an immune system modulator. In this capacity, it is very effective, safe, inexpensive, and readily available.
4. Proper therapy for AIDS will be directed at:
• Early interve1ntion (i.e., CD4 count >300)
• Ozone plus other synergistic immune-augmented therapy
• Intestinal cleansing, which is paramount due to the immunosuppressive aspect of parasites8
In the following pages, we will explore the laboratory and clinical findings related to HIV, plus the ways in which ozone and hydrogen peroxide are being used by patients today.
IN VITRO STUDIES
In vitro studies to evaluate the ability of ozone to kill HIV in the test tube have been undertaken by eminent scientists in the United States, Russia, and Canada. The first researchers in the world to prove that ozone can inactivate HIV were the late Michael T. F. Carpendale, M.D. (chief of medicine and research services at the Veterans Administration Hospital in San Francisco and professor at the University of California School of Medicine, San Francisco), and his associate, Dr. Joel K. Freeberg of the Veterans Administration Hospital. They first presented their findings at the Fourth International Conference of AIDS in Stockholm, Sweden, and later published their report in the peer-reviewed journal Antiviral Research. Carpendale and Freeberg showed that HIV could be 99 percent inactivated with only 0.5 µg ozone/ml of human serum, and completely inactivated by ozone concentrations of 4 µg/ml of human serum. Those concentrations of ozone did not harm healthy cells.9
Another in vitro study, supported in part by the U.S. Public Health Service and Medizone International, a manufacturer of a patented medical ozone delivery system, was reported in the October 1, 1991, issue of the medical journal Blood. Using ozone generated from medical-grade oxygen and delivered into a cultured cell medium of HIV-1, a team of four scientists from the State University of New York Health Science Center in Syracuse, the Brooklyn Hospital, and Merck Pharmaceutical found that ozone deactivated the virus completely, yet without causing significant biological damage to noninfected cells. In evaluating their findings with HIV, the researchers concluded, “The data indicate that the antiviral effects of ozone include viral particle disruption, reverse transcriptase inactivation, and/or a perturbation of the ability of the virus to bind its receptor to target cells.”10
In Russia, scientists at the Institute of Virusology in Moscow also used a concentration of 4 µg ozone/ml on an infected culture containing HIV. Within minutes, the cells of the virus decomposed and died. The researchers noted that “complete deactivation of [the] extra cell virus is achieved by putting gaseous ozone through [the] virus-containing [liquid].”11 This will not happen in vivo.
In chapter 4, brief reference was made to a major study in Canada coordinated by the surgeon general of the Canadian Armed Forces to determine the ability of ozone to kill HIV, hepatitis, and herpes viruses in blood used for transfusion. After a three-minute ozonation of serum spiked with one million HIV-1 particles per milliliter, a 100 percent deactivation of the virus (in vitro) was achieved.12 Referring to this study during his interview in the video documentary Ozone and the Politics of Medicine, Captain Michael E. Shannon, a scientist and medical doctor with the Canadian Department of National Defence, said: “We are dealing not with concentrations that are toxic to the human, but are in fact concentrations of ozone that have been used in clinics in Germany for the last thirty years with thousands of patients without any evidence of any harm.”13
Despite the importance of the results (which would indicate that simple ozonation of the blood supply would render it free of HIV, as well as herpes, hepatitis, and other viruses), these Canadian findings received little notice in the North American press.
CLINICAL EXPERIENCE
Germany
Dr. Horst Kief, who is perhaps best known for his work with patients suffering from cancer and neurodermatitis, as well as the development of autohomologous immunotherapy (AHIT), is believed to have been the first physician in the world to treat AIDS patients with hyperbaric ozone “blood washings” in the early 1980s. His standard AIDS protocol was a session of autohemotherapy once a week for three months, to be repeated if necessary.
In a monograph published in the German medical journal Erfahrungsheilkunde in July 1988, Dr. Kief recalled that the patients experienced a near-complete alleviation of various AIDS-related symptoms, including thrush and oral hairy leukoplakia. In addition, their T4-cell count increased dramatically, as did the T4:T8 ratio over a time period of sixty-five days.14 In an interview shown in Ozone and the Politics of Medicine, Dr. Kief said that a seven-year follow-up of his first patients found them alive, working, and “doing very, very well.”15
However, the first documented cases of using ozone to treat AIDS were reported by German physician Alexander Pruess in 1986. In his work with four patients, Dr. Pruess used ozone in combination with Suramin (a reverse transcriptase inhibitor), immunomodulation therapy, vitamin and mineral supplementation, and the hygienation (cleansing) of intestinal flora (bacteria present in the intestines). He wrote the following about his decision to use ozone: “As it is well-known that the actual disease(s) occurring through AIDS consists of a combination of viral, fungal and bacteriological infections, I searched for a substance which is virucidal, fungicidal and bactericidal at the same time. Ozone was here the obvious choice.”16
Dr. Pruess noted immediate improvement in all four patients, including the elimination of HIV-related problems like skin diseases, fungal infections, gastrointestinal problems, and low energy. More than a year after treatment, all subjects were considered clinically healthy.
In a monograph published in 1993, Dr. Kief wrote about a study comparing thirty patients from the Kief Clinic who were given ozone in the form of AHIT and twenty patients from the University of Frankfurt School of Medicine who received conventional treatment, including AZT (azidothymidine). Dr. Kief’s patients were observed for 251 days while the Frankfurt patients were observed for 363. T4:T8 ratios rose from 0.324 to 0.352 among Kief ’s patients, while they fell from 0.293 to 0.223 among the Frankfurt patients.
In a related study of twenty-seven AIDS patients receiving AHIT, the percentage surviving after eighteen months was 80 percent, and the percentage surviving after 45 months was 70 percent. This represented a much higher percentage than patients receiving conventional medical therapy anywhere.17
While these figures were encouraging, I learned that Dr. Kief is no longer using AHIT to treat people with AIDS. In 1992 German health authorities ordered him to create and maintain a separate (and highly secure) laboratory to make AHIT for his HIV and AIDS patients. Since the cost to build and secure a new facility was considered prohibitively expensive, Dr. Kief decided to stop using AHIT, and his HIV/AIDS practice became confined to treating patients with major autohemotherapy.
United States
In the United States, pilot studies were developed by Dr. Carpendale and Dr. John Griffiss of the Department of Laboratory Medicine at the University of California School of Medicine in San Francisco to find out if there is a role for medical ozone in the treatment of HIV and associated infections.
The study focused on two asymptomatic persons infected with HIV, one (known as “Patient G”) who began with a T-cell count of 309, and one (“Patient I”) who began with a T-cell count of 907. The treatment protocol consisted of doses of ozone and oxygen given via rectal insufflation daily for twenty-one days, once every three days for sixteen weeks, and once weekly for fifteen weeks, for a total of seventy-three treatments over a period of thirty-four to thirty-six weeks. For the next two years, the subjects treated themselves with a three-week “booster dose,” which was repeated from time to time, as seen in figure 12.2 below.
The researchers reported that T-cell levels remained acceptable (i.e., over 430) over the next six years, and both individuals “remained in the best of health, with increased feeling of well-being and energy, while on ozone therapy and with no infections and no adverse symptoms of malaise for the first five years.” By that time, Patient I, who began the study with a higher T-cell level, not only attained a T-cell count of 1,185 but later tested HIV-negative. However, three months into the sixth year, Patient G died suddenly from lobar pneumonia (not the AIDS-related Pneumocystis jiroveci pneumonia) after getting soaked in a storm while recuperating from the flu. When he died, Patient G was still HIV-positive, yet he had maintained a T-cell count between 500 and 700.

Figure 12.2. Absolute CD4 (“T”) cell count in HIV+ patients treated with ozone plotted against time. (From Michael T. Carpendale, M.D., and John Griffiss, M.D., “Is There a Role for Medical Ozone in the Treatment of HIV and Associated Infections?” in Ozone in Medicine: Proceedings of the Eleventh Ozone World Congress, Stamford, Conn., International Ozone Association, Pan American Committee, 1993, M–1–39, 40.)
In their report, which was published in Ozone in Medicine: Proceedings of the Eleventh Ozone World Congress, the researchers concluded:
These normalizing results support the hypothesis that ozone may be effective in suppressing and possibly eliminating HIV, especially in the stages of the disease when the patient is asymptomatic and has a CD4 cell count in the normal range. It also indicates the potential for self treatment [via rectal insufflation] for long term prophylaxis, treatment or care.18
In a related study, which was published in the Journal of Clinical Gastroenterology, Dr. Carpendale and his associates gave five AIDS patients suffering from intractable diarrhea daily rectal insufflations of ozone (at doses from 2.7 to 30 mg) for twenty-one to twenty-eight days. By the end of the study, three of the four patients were completely relieved of their symptoms, while one patient, whose diarrhea was the result of the parasite Cryptosporidium, experienced no change. Relief from secondary infections including herpes simplex, folliculitis, and sycosis barbae was also reported. Patients experienced less toxicity, less discomfort, and more energy than they had before being treated with ozone. No adverse side effects were reported.19
Dr. Carpendale was so encouraged by the results of these studies that he attempted to secure government funding for additional ozone studies involving many more people. He met with no success.
The results of another pilot study with ozone were presented at the Fourth International Bio-Oxidative Medicine Conference in April 1993 by Dr. Frank Shallenberger. He administered intravenous ozone over a period of fourteen days to five randomly selected men diagnosed with AIDS. The total daily dose was calculated to be 0.15 µg ozone/kg of body weight. On the first day, one-quarter the daily dose was given; on the second, one-half; and on the third, three-quarters. From the fourth to the fourteenth day, the full dose was administered. Patients were carefully monitored and evaluated before and after each treatment. During the period after therapy, no other therapies were given, except for one patient who began taking ddI (didanosine) after the fourth month.
Before the ozone treatments began, each patient participated in a holistic protocol including a whole-food nutritional program, meditation and deep breathing, lymphatic drainage massage, nutritional supplements, safer sex practices, and regular exercise.
Although Dr. Shallenberger considered the sample too small to be statistically significant, the results included at least a six-month period of overall survival, an immediate increase in the number of T cells, relief of symptoms from opportunistic infections among most patients, and higher energy levels overall. Dr. Shallenberger’s clinical observations follow:
- S.W. (34 years old): Diffuse cutaneous Kaposi sarcoma of two-year duration went into clinical remission for six months before the lesions returned. Otherwise continues to be in good health.
- S.S. (27 years old): Chronic diarrhea (cryptosporidium), chronic fatigue, and weight loss >20%. All symptoms disappeared within two months, and the patient remains healthy one year later. CD4 count remains at 7.
- R.J. (34 years old): Oral thrush, fatigue, and mild lymphadenopathy [swollen lymph nodes]. Thrush disappeared for six months. Fatigue is gone. Lymphadenopathy has not progressed, and the patient remains in good health one year later.
- T.B. (32 years old): Hairy leukoplakia and mild lymphadenopathy. Neither of these symptoms changed. He remains in otherwise good health one year later.
- M.P. (41 years old): Neuro-leukodystrophy. Needs assistance to walk, has urinary incontinence and impotence. Within one week of treatment his incontinence and gait improved considerably. One month later, he was walking easily without assistance and had no incontinence. MRI remains stable, showing no progression of lesions, as does the patient at a ten-month interval.20
Dr. Shallenberger’s findings support the hypothesis that ozone therapy can have long-term positive effects on AIDS patients. While not a cure, ozone therapy can play a role in improving the quality of life of persons living with AIDS. Soon after the results of the Shallenberger study were released, the Nevada medical authorities attempted to close down his practice.
Positive results from oxidative therapies were also reported by John C. Pittman, M.D., from North Carolina, who worked extensively with HIV and AIDS patients over several years. Pittman’s holistic treatments, including ozone and hydrogen peroxide, reportedly helped a number of patients to become HIV-negative. He also began to collect data relating to HIV-infected patients who received oxidative therapy throughout the country.
One of these patients was a thirty-four-year-old man referred to as “D.M.” He was diagnosed HIV-positive in March 1991 and had a CD4+ T-cell count of 600, considered to be in the low range of normal. In April 1991 he began receiving autohemotherapy once a day for ten days, along with intravenous hydrogen peroxide and intravenous vitamins, including especially large amounts of vitamin C. In July, he repeated a thirty-day treatment protocol with ozone, hydrogen peroxide, vitamins, and antiviral compounds, as well as nutritional therapies designed to aid in intestinal cleansing and metabolic detoxification. During the first two weeks of therapy, D.M. experienced fever and a drop in his T-cell count to 400, which Dr. Pittman attributed to a die-off of virus particles and infected lymphocytes. Following the thirty-day protocol, D.M. reported that his enlarged neck and inguinal lymph nodes became much smaller. Laboratory tests showed that his CD4+ T-cell count rose to 900.
D.M. continued receiving occasional treatments with ozone and vitamin C, and by November 1992, his helper T-cell count reached 1,400 and his enlarged lymph nodes had returned to normal. Although D.M. still tested positive for the HIV antibody, there was no sign of viral activity by P24 antigen testing.21 (An antigen is a substance that induces the formation of antibodies.)
Like Dr. Shallenberger, Dr. Pittman’s treatment protocol encompassed a holistic approach. Dr. Pittman recommended using intravenous ozone, intravenous hydrogen peroxide, intravenous vitamin C, EDTA (ethylenediamine tetra-acetic acid) chelation, external oxygenation (baths with ozone and hydrogen peroxide), hyperbaric oxygen, metabolic and intestinal detoxification, a raw and living food diet, nutritional supplements, and exercise.22
It was mentioned earlier that hyperbaric oxygen (HBO) therapy has also been found useful in the treatment of AIDS. In 1990 Michelle R. Reillo, R.N., began a six-year research program on three hundred patients with late-stage AIDS who underwent HBO treatment for diverse AIDS-related complications, primarily in the Baltimore, Maryland, area. Reillo investigated how HBO works in the manifestation of peripheral vascular insufficiency, pulmonary complications, neurological manifestations, dermatological manifestations, metabolic disorders, and liver problems. Although their life expectancy was just two years at the time the study was begun, more than half of the patients were still alive and enjoying a good quality of life six years later, although they did not take antiviral drugs.
In her book AIDS under Pressure, Reillo offered many case studies. The following case history of a thirty-five-year-old male who received HBO treatments three times a week for eight months is typical. The initial tests recorded plasma viral load at 28,550 copies/ml. After three months, another test indicated a viral load of 15,000 copies/ml. Three months later, the results were negative (less than 4,000 copies/ml), even though the patient was not taking antiviral drugs or other medications. Reillo reported, “Clinically, the patient gained ten pounds, felt an increase in energy and stamina, and had relief of fatigue. He reported no adverse effects from HBO [therapy].”23 She not only found the treatment cost-effective and without adverse side effects, but also concluded:
Managing AIDS with hyperbaric medicine restores immune function, enhances the body’s ability to fight infections, directly destroys microorganisms that the immunosuppressed body cannot eliminate, and ameliorates complications related to the presence of HIV. . . . As a primary and adjunctive therapy, hyperbaric oxygen therapy is a technology that prolongs and enhances the quality of life of people with AIDS.24
Reillo also found that HBO therapy enhanced the effectiveness of antiviral drugs, as well as other drugs used to manage opportunistic infections or drug-related side effects such as anemia, yeast infections, nausea, liver toxicity, anorexia, and leukopenia.25
Yet in spite of the research, mainstream physicians have not embraced the use of HBO therapy to treat AIDS. As is the case for other oxygen therapies, the scope of HBO therapy is often misunderstood, and many physicians do not fully appreciate its possibilities. In the United States and Canada, most hyperbaric chambers are hospital-based (where conservative treatment is the norm), and the use of HBO therapy must be recommended by a licensed physician, who may know very little about hyperbaric oxygen in the treatment of AIDS. In her book AIDS under Pressure, Reillo wrote: “Regardless of the beliefs of the health care practitioner, the responsible position is to share all options with the patient. Often, however, it is the patient who educates and encourages the health practitioner to explore all options.”26
Canada
Heartened by the in vitro blood studies done by the Canadian Armed Forces, the Canadian government decided to sponsor a study with actual AIDS patients. Coordinated by Captain Michael E. Shannon, M.D., in collaboration with Dr. Michael O’Shaughnessy, a virologist with the Laboratory Centre for Disease Control in Ottawa, the study employed twenty-four volunteers suffering from AIDS in two trials using minor autohemotherapy. The Phase I study, which involved ten patients, showed an increase in T cells among those who had 300 or more to begin with, while those who had 90 T cells or fewer experienced a decrease.27 A Phase II random study was then begun with fourteen patients, with half to receive ozone treatments and the other half a placebo. The findings were inconclusive, however, because the ozone generator used in the study failed to produce ozone. Since the study was double-blind, no one knew about the defect until it was too late.
However, in a private communication I received in January 1994, Captain Shannon wrote: “Of interest, however, the three patients (out of ten volunteers) who responded to minor autohemotherapy in the first trial, are still alive after four years post-treatment, with CD4 counts in excess of two hundred. These patients theoretically should have succumbed to AIDS within a year post-treatment.”28 Captain Shannon added that although these initial results must still be explained, there was little interest within the Health Protection Branch of Health and Welfare Canada to pursue the matter further.
In a letter dated January 13, 1995, and addressed to Ed McCabe, Dr. Shannon (who by that time was both promoted to the rank of commander and appointed deputy surgeon general of Canada) offered his candid evaluation of the future of ozone in treating patients with HIV and contradicted the views of one of the other researchers who participated in the second study. At Dr. Shannon’s request, the letter is reproduced here in its entirety.
Notwithstanding the negative findings of Dr. Garber’s 1991 clinical trial, I firmly believe that ozone therapy has potential to play a valuable role in the medical management of AIDS. From a regulatory point of view, it is clear that not all forms of ozone therapy will be considered sufficiently safe and/or efficacious in this regard; however, there is no doubt in my mind that a protocol will eventually emerge with proven benefit.
Looking back at my past experience with minor autohemotherapy in the treatment of AIDS, there still remains a discrepancy between the Phase 1a and 1b trial results, which may, in part, relate to the lack of sophisticated technology to control for O3 concentrations in both trials. Given the lack of any significant therapeutic breakthroughs in the treatment of AIDS since that ill-fated trial and the growing testimonial support for its efficacy, the need for further clinical research with ozone is certainly indicated. It is indeed unfortunate that the North American medical community and its funding agencies could not take a more neutral stance on this subject; tragically, professional opinion has been somewhat polarized on this issue. I believe that it is time to take the emotion out of the arguments, both pro and con, and commence a systematic examination of the evidence currently available on the merits of this therapy. Where information gaps exist (particularly in peer-reviewed scientific studies) which might preclude any regulatory decision on the validity of certain claims, properly designed research initiatives should be encouraged with the same kind of public support normally afforded any other scientific endeavour of this import.29
At the time of this writing, no large-scale research is being done on the ability of ozone to treat either HIV infection or AIDS.
Cuba
AIDS has not been a major health problem in Cuba. When the AIDS epidemic first came to light, everyone on the island was tested for HIV infection, and the several hundred who tested positive (many of whom were believed to have contracted the virus in Angola, where Cuba was involved in military operations) were quarantined by the government. They were placed in campus-like settings and given free housing, medical care, and healthy food but were not allowed to leave the area. By 1998 this policy became liberalized for those who were not likely to spread the virus to the general population, which had received a crash course in HIV prevention by the Cuban health authorities.
During my interviews with scientists from the National Center for Scientific Research in Havana, I learned that ozone had been given to several of the detainees with some success, although undertaking a study of ozone to treat AIDS was not a high priority due to the low number of infected people.
Dr. Silvia Menendez, a chemist who cofounded the Ozone Research Center with Dr. Manuel Gomez in 1985, told me that ozone works best when administered as soon as possible after infection, before the virus has penetrated the lymphatic system and bone marrow. She believed that, if caught early, ozone could deactivate the virus in the blood and prevent it from infecting other cells. She added that ozone therapy could help prevent and treat some of the opportunistic infections that are common among AIDS patients.30
Her comment regarding the early use of ozone for those infected with HIV is very important. If a person could be treated with ozone as soon as possible after infection, perhaps the normal progression of the disease could be interrupted. The economic and social ramifications of this possibility cannot be underestimated.
Africa
Concerned with improving and maintaining health through homeopathy and complementary and alternative therapies, Abha Light Foundation (affiliated with Ananda Marga Universal Relief in India) has been treating a limited number of African patients with HIV and AIDS with a combination of intravenous hydrogen peroxide and ultraviolet blood irradiation (UBI)—also known as photo-oxidation—for years.
Patients are treated in a doctor’s office. A normal treatment usually takes two hours and is done in two parts. First, hydrogen peroxide is added to a glucose or normal saline IV solution and is slowly infused into the patient. In the second part of the procedure, about 50 ml of the patient’s blood is taken out and passed over an ultraviolet light source. It is then transfused back into the patient in a sterile “closed circuit” system.
The clinic reports that treatments are usually given once or twice a week in the case of chronic illness, with one to twenty treatments administered depending on the condition of the patient and the illness being treated. The patient is evaluated periodically for progress, and the physician determines if additional treatments are necessary. It’s important to point out that no one has been cured of AIDS at Abha Light, although hydrogen peroxide therapy appears to be a useful adjunct in helping prolong life and increase the quality of life among AIDS patients.
UBI therapy has also been used in other countries either alone or as an adjunct to oxidative therapies in treating patients with HIV/AIDS. UBI treatment produces a number of therapeutic benefits often related to ozone and hydrogen peroxide: inactivation of toxins, destruction and inhibition of growth of bacteria, increase in the oxygen-combining power of the blood and oxygen transportation to organs, activation of steroid hormones, vasodilation (the dilatation of blood vessels, which decreases blood pressure), activation of white blood cells, stimulation of cellular and humoral immunity, removal of blood clots, decreased viscosity of blood, improved circulation, stimulation of corticosteroid production, and decreased platelet aggregation. Some physicians have found that UBI is effective in the treatment of pneumonia and other respiratory diseases.
Although few people have heard of UBI, scientific research has documented its powerful effects for many years. Early articles attesting to the antibacterial and antiviral properties of ultraviolet light appeared in reputable medical journals like the Archives of Physical Medicine (1946), Review of Gastroenterology (1948), Experimental Medicine and Surgery (1950), and the American Journal of Surgery (1955).31 More recent articles about how ultraviolet light can inactivate viruses (including HIV and cytomegalovirus) and bacteria can be found in professional journals related to blood and blood transfusion, including Blood Cells (1992), Vox Sanguinis: International Journal of Transfusion Medicine (2004), and Transfusion (2004, 2005).32 One of the best reviews of this modality was written by Robert J. Rowan, M.D., and published in the International Journal of Biosocial Medical Research in 1996. In reviewing the promise of UBI and other nonspecific healing modalities like ozone and hydrogen peroxide, he wrote:
Modern medicine has focused on drugs to suppress symptoms or inhibit certain physiology (NSAID drugs as prostaglandin inhibitors, hypertensive drugs as enzymatic blockers) to treat disease. As a result, we have seen the frightening rise of resistant organisms and the side effects of chemical pharmacology. Perhaps medicine should consider the concept of nonspecific modalities that encourage the body’s healing response and immune system.33
Anecdotal Findings
Over the years, hundreds of anecdotal reports have surfaced regarding the positive results of oxidative therapies for the treatment of HIV infection and AIDS. A number of these reports come from patients themselves and their physicians, many of whom must remain anonymous. The use of medical ozone generators remains illegal in most states and Canadian provinces, and physicians—if discovered—can lose their medical licenses or be put in jail.
J.P. of Milwaukee was first diagnosed HIV-positive in 1988 and had a T4-cell count of 237 in June 1992. He decided to use Viroterm (a type of oral alpha interferon) and ozone through the sauna bag method over a period of several months. After three weeks of using ozone daily, J.P. found that his lymph nodes, which had been swollen for three years, subsided to normal. In addition, his T-cell counts increased from 237 in June to 292 in October. In June, he had tested positive for P24, a protein found in the core of the human immunodeficiency virus, and by October, his doctor told him that he had tested negative for P24.34
Brad J. is a registered nurse who was stuck with a needle while taking blood from an AIDS patient in June 1991. By November he had tested positive for HIV, as well as hepatitis B and C. His T-cell count dropped substantially and by February he had lost thirty pounds, was extremely fatigued, and suffered from severe diarrhea, making it almost impossible to work. Despite his physician’s advice, he refused to take AZT and began intravenous infusions of vitamin C five times a week, which caused the diarrhea to abate from twenty movements a day to six. In December 1992, he met Ed McCabe, who told him about ozone, and the following February Brad traveled to Germany to become a certified practitioner in ozone therapy. However, it was not until April 1993 that Brad began taking ozone via autohemotherapy that he administered to himself every seventy-two hours. By the second treatment the diarrhea was eliminated and he felt his old energy return. His hepatitis symptoms disappeared and his viral load index became undetectable after six months of treatment.
Brad has continued using ozone sporadically since that time, augmenting it with Chinese herbs, vitamin C, and other nutritionals. Since he finds the needle stick for autohemotherapy uncomfortable, Brad currently administers ozone in each ear once or twice a week and takes ozone saunas and occasional rectal insufflations. His health situation is stable: after twelve years, he has been free of HIV-related symptoms and his T-cell counts are normal. His energy level is astounding. In addition to his full-time job as a nurse and rebuilding an old house in the country by himself, he has been assisting physicians in setting up ozone clinics. Although Brad credits his good health partly to a spiritual awakening and the use of vitamins and herbs, he says bluntly, “Ozone saved my life.”
Another man, whom I will call Bill, tested HIV-positive in 1982 and by 1993 had a T-cell count of 36. In August of that year, he began using the sauna bag method, and he reported that the breathing difficulties he had disappeared after three treatments. Bill also experienced relief of a chronic herpes problem. He began rectal insufflation with humidified ozone in November twice a day and reported relief of abdominal pain and an improved ability to sleep.
Although the exact dose of ozone to be given via rectal insufflation for each individual should be determined by a physician, Dr. Carpendale disclosed the protocol he used in his San Francisco clinical investigations with AIDS patients at the Eleventh Ozone World Congress in 1993:
Ozone was produced from a portable medical ozone generator (Hansler, Iffezheim, Germany), and was insufflated through a Teflon catheter into the colon. This is a simple, safe, inexpensive and well-documented method for treatment with ozone. Dosage concentration was 22–30 mg O3/ml O2; average volume was 1100 ml for a total dose of 26.2–33 mg O3 per treatment. The treatment program was daily for twenty-one days, once every three days for sixteen weeks, and once weekly for fifteen weeks, for a total of thirty-four to thirty-six weeks and seventy-three treatments containing 2065–2137 mg ozone.35
Further information regarding the rectal insufflation method to treat HIV/AIDS can be found in the literature published by Keep Hope Alive.
John from Illinois had a T-cell count in the 200 range and began taking five drops of 35 percent food-grade hydrogen peroxide in water three times a day about three hours after meals. He gradually increased the dose to twenty drops, which he maintained for another two months. He then reduced it to five drops and got tested again. His T-cell count had risen to 800. In his comments on the case, Mark Konlee, the author of AIDS Control Diet and Immune Restoration Handbook, did not recommend using oral hydrogen peroxide. However, he added that these same results could also result by adding a pint of food-grade hydrogen peroxide to warm bathwater and soaking in it for 20 minutes a day.36
Like Dr. Silvia Menendez of the National Center for Scientific Research in Cuba, Dr. Bocci suggested that if ozone therapy is applied as soon as possible after exposure to HIV, the patient stands a good chance of avoiding illness.
Writing in the journal Mediators of Inflammation, Dr. Bocci stated:
Our working hypothesis is that ozone acts mainly by inducing blood mononuclear cells to produce immunoregulatory cytokines, particularly those produced by lymphocytes with TH1 phenotype. After incubation of ozonized blood we have shown the release of small amounts of practically all cytokines so far tested, particularly GM-CSF, IL-2, IL-8, IFN, TNF and IFN. After reinfusion of ozone-treated blood, mononuclear cells are supposed to home in various lymphoid (spleen, lymph nodes, thymus, Peyer’s patches) and non-lymphoid (lungs, liver) organs thus priming and activating other immune cells. The prolonged repetition of autohemotherapy favors a progressively amplified activation of the immune system via numerous pathways such as activation of either major histo-compatibility complex restricted cytolysis, or nonspecific killing via activation of natural-killer cells, macro phages and neutrophils, that ultimately represents the most efficient system of destruction of viral infected cells.
He concluded, “Optimized autohemotherapy after a brief exposure of blood to ozone may today afford the trick of reprogramming the immune system to keep HIV at bay. The autohaemotherapeutic procedure is simple, safe, inexpensive and most likely is more effective than conventional approaches.”37
HIV AUTOVACCINE
In 2010 Dr. Bocci, along with Drs. Iacopo Zanardy and Valter Travagli of the Department of Pharmaceutical Sciences at the University of Siena, offered a novel proposal for a universal HIV autovaccine for both the prevention and treatment of HIV infection. They proposed collecting HIV-infected plasma samples from HIV-infected individuals from five continents around the world. They outlined the procedure in the medical journal Virulence:
a) Collection of human HIV plasma samples
b) Centrifugation of the pooled plasma samples and filtration through an antibacterial filter
c) Five cycles of freezing (−196°C) and thawing (+4°C) within a week
d) Inactivation of HIV with ozonation (800 μg ozone per ml of plasma)
e) Addition of both human albumin (200 mg/ml) and ozonated ethyloleate, corresponding to 20 μg of ozone
f) Laboratory tests. Preclinical evaluation in animals. Evaluation in volunteers of a mock vaccine and of the actual ozonated vaccine
g) Vaccination schedule
They added, “A potential advantage of this procedure is that a vaccine made of virions obtained from a great variety of patients will contain all possible HIV genetic diversity at the present and possibly in future times. If the immune system is able to efficiently respond to the ozonated antigens, the vaccine could be used as preventive and possibly curative vaccine.”38
HIV, AIDS, AND THE POLITICS OF OXIDATIVE THERAPIES
The use of oxidative therapies for patients with HIV/AIDS is still fraught with controversy. Pharmaceutical companies—which have been earning billions of dollars in profits from anti-AIDS medications—are completely opposed to the use of cheap, safe, and potentially effective oxygen healing therapies in treating this disease, even as an adjunct to traditional medical therapy. In addition, many physicians are either ignorant of or hostile toward using therapies that can be self-administered, like the sauna bag method, steam cabinet method, ear insufflation, or rectal insufflation methods mentioned earlier.
Many reputable and caring physicians who have treated AIDS patients with ozone and hydrogen peroxide have been threatened by state licensing authorities and have had their practices closed down. The U.S. Food and Drug Administration and the National Institutes of Health have refused to sponsor human trials for ozone and hydrogen peroxide and have made it extremely difficult for small, independent companies like Medizone International to undertake such research. Despite the fact that over ten million patients (including thousands of AIDS patients) have received ozone therapy in Europe and that reliable data on the use of ozone and hydrogen peroxide is supported by hundreds of scientific articles and clinical studies, the Food and Drug Administration still maintains that oxidative therapies like ozone have not been proven either safe or effective. Dr. Randolph F. Wykoff, the director of the Office of AIDS Coordination and the acting associate commissioner for science for the U.S. Food and Drug Administration, testified before the Subcommittee on Crime and Criminal Justice of the Committee on the Judiciary at the House of Representatives in Washington on May 27, 1993, saying:
Ozone therapy has also been used to treat AIDS patients without any scientific data to support the agent’s safety or effectiveness. Ozone therapy and ozone generators have been promoted in magazines and newspaper advertisements and in books, videos, and audiocassettes. The introduction of ozone into immunosuppressed AIDS patients without careful study of probable toxicities places the patients at unreasonable and significant risks.39
The political and economic situation in the United States and Canada has led many patients to seek treatment elsewhere, primarily in Mexico. While there are several reputable clinics in Mexico, some unethical promoters have held out promises for a cure at a price approaching $20,000. One scheme even offered patients six-figure salaries if they could promote their success to other prospective patients later on, especially to those who owned homes that could be mortgaged to pay for treatment.40
Until health care consumers speak out to their elected representatives, we will continue to be denied the right to choose the forms of health care we want. Large-scale clinical studies regarding the effectiveness of ozone and hydrogen peroxide to treat AIDS will never be done, and the task of securing research funding will continue to fall on individual researchers themselves. Doctors will be forced to continue to administer these therapies illegally and surreptitiously, and many people without access to these physicians will continue to self-administer ozone or hydrogen peroxide.
While amazingly few adverse side effects have been reported, no one should ever be forced to self-medicate without the benefit of supervision by a qualified health professional. Entrepreneurs eager to fill their pockets will offer magical cures costing tens of thousands of dollars, while many individuals who are infected with HIV or who are dying of AIDS will decide to “go for broke” and try untested treatments from clinics of dubious reputation. Those with the strength and the financial resources will choose to leave their family and friends and seek reliable care in Germany or Cuba.