16
NEW TECHNOLOGIES CAN CONTRIBUTE TO A SUCCESSFUL EDUCATIONAL PROGRAMME
John Sandars
Learning technologies have moved from being esoteric tools used by a few pioneering faculty to mainstream applications integrated into the medical school educational enterprise.
The last decade has seen an increasing global availability and use of a wide range of new technologies, especially social media and mobile devices. These new technologies have become almost ubiquitous and are an integral part of daily life for many people, especially the younger generation who have grown up using these technologies at home and school (Lenhart et al. 2010). The internet has had a major impact on the delivery of educational programmes, increasing their accessibility to students in terms of content, resources, and when and where they can study. Social media is a wide term and includes social networking sites (such as Facebook and Twitter), blogs and wikis (such as WordPress and MediaWiki), media sharing sites (such as Flickr and YouTube) and communication technology for instant messaging and live chat (such as Skype). The original distinction between different social media has become increasingly blurred, with the integration of several functions within each site. For example, Facebook comprises blogs (an easily updated webpage for sharing with others on the network) with media sharing (photographs and videos) and live chat. Mobile devices have also become increasingly integrated, with smartphones and tablet computers (such as iPads) enabling users to take and share photographs and videos, and have access to the many social media sites at a time and place that are convenient for them.
Most readers of this chapter will have experience of using some or all of the above new technologies in their personal lives and many will also have used the same technologies in their professional or clinical practice. New technologies provide unrivalled opportunities to create content, provide a link to existing content, share content with other people and facilitate communication between people, either one to one or one to many. However, the potential for the use of these technologies to enhance teaching and learning will only be fully realised and effective if there is careful attention to integrating the needs of the learner, the opportunities that can be offered by the technology and the context within which the technology is to be used. This integration requires an essential ‘learning-centric’ focus, which is underpinned by educational principles to provide a structure to the learning experience, instead of a ‘technology-centric’ focus, that introduces a new technology without consideration of how it provides value to the educational process.
Responding to the needs of the learner
There is increasing focus on the learner being at the centre of the learning process, with the essential recognition that all learners have their own unique needs. An important aspect is the learner’s preferred approach to learning, since meeting the needs of the learner improves motivation and engagement with the learning process, resulting in a more effective learning experience. The South African case study and the Dundee, UK case study highlight how the needs of the learner were recognised and used to inform the development of an innovative and effective learning experience with technology.
Case study 16.1 Digital story telling (DST) to enhance reflection on service learning, University of Pretoria, South Africa
Jannie Hugo
One response to the challenge of serious inequity in health in South Africa has been to engage students in service learning in rural district healthcare. At the University of Pretoria, students had a 7-week block in district health in the final 18 months of the course. Students worked in maternity, emergency unit and district clinics across 15 different districts distributed in Mpumalanga, a large rural province. Rural service learning is costly and labour intensive. It was therefore important to ensure that optimum learning was taking place. Reflection is an important component of this learning and students performed several reflection tasks during the block, including a daily learning journal, reflections about obstetric deliveries and written reflection on patient care.
Students regarded reflection tasks as an added responsibility that bores some and frustrates others. As with South African society, the MBChB class of 240 students was also very diverse, with students coming from different ethnic and cultural backgrounds, from rural or urban areas, and from at least 11 different home-language groups. Although English was the language of instruction and working, it was a second language to most students, and students were encouraged to speak the patient’s language as much as possible. Writing narrative in English did not come naturally to these students.
The aim of the DST task was to integrate reflection and learning at the end of the district health block. This task was compulsory: all students received orientation and guidance on how to prepare the story, but it was not formally addressed. Students were expected to identify important learning experiences and provide a picture to represent these experiences. The pictures could be obtained from the internet but most students would take a series of photographs during the block, mainly using their own mobile phone. For ethical reasons, no pictures of staff or patients were allowed.
During the last week of the block, students returned to the campus in Pretoria where they went through all of their reflections and pictures to integrate them into a reflective digital story. This story of their experience and learning during the block was presented to the group in the form of a PowerPoint presentation of five to seven pictures.
In a focus group evaluation, students reported overwhelmingly positive experiences of using DST. During the block, students consciously thought of their experiences ‘in pictures’: they remembered their experiences and the learning of the block as pictures about people and not in academic terms. Some reflection appeared to happen while taking the photograph, and then it was relived when the pictures were reviewed and chosen for the presentation. There was also an opportunity to work through negative experiences, share and come to terms with these experiences. Further reflection occurred while doing the presentation and watching the other presentations and even continued afterwards by reminding the student about experiences related to pictures.
For tutors the DST was enjoyable, time efficient and very informative as to what students really experience and learn during the block. Teachers regarded DST as that part of the block that provided most job satisfaction!
As a learning task, students preferred DST to written and more structured reflective assignments. It was experienced as non-judgemental and pictures made it possible to say things that were difficult to say in words, especially when English was a second language. The opportunity to reflect also appeared to be enhanced, with numerous points for reflection both during the creation of the DST and after the presentation.
There is research on present-day medical students that suggests that there is a preference for a more active and visual approach to learning rather than the more traditional text-based approaches to teaching (Sandars and Homer 2008). This is likely to be more important in cultures that have an oral narrative tradition and also where English is a second language. Active learning usually has a collaborative component, with ‘one-to-one’ or ‘one-to-many’ interactions. Information and opinion are shared to create a mutual and deeper understanding. The South African case study utilised group presentations to enhance the learning from reflection and the Dundee, UK case study (see below) offers several opportunities to collaborate, including the development of content and networking between students and with their teaching staff.
Case study 16.2 Using blogs to engage students and teaching staff in a medical school, University of Dundee, UK
Natalie Lafferty
Medical schools have been early adopters of educational technologies yet have faced challenges in delivering an integrated spiral curriculum in traditional virtual learning environments (VLEs), such as Blackboard and Moodle. With a focus on how they want to teach and support learning, medical educators are increasingly exploring the potential of social media tools, including blogging platforms such as WordPress and microblogs such as Twitter, to support their teaching. Inspired by medical blogs such as Life in the Fast Lane and Clinical Cases and Images hosting growing medical education libraries of cases and resources, Dundee Medical School explored the potential of the WordPress blogging platform to support undergraduate teaching.
The Medical School set up its own WordPress server (MedBlogs) and teaching leads began to explore, using it as an alternative to the VLE to deliver their teaching. Students were also engaged in this process, helping staff to develop sites in different specialties. Blogs were initially piloted in the respiratory and musculoskeletal system teaching blocks to supplement core teaching resources delivered via the VLE. Teaching staff found MedBlogs straightforward to use and used their blogs to link to journal articles and websites, comment on topical news stories and embed videos. Patient scenarios were also posted which students discussed via blog comments, and at the end of the week a post from teaching staff provided a detailed explanation of each case. The response from students to the blogs was positive and enthusiastic, and analytics showed students made extensive use of them both during the teaching blocks as well as in revision periods. Students found them easy to use and to post questions, which were promptly answered by teachers, and they asked for more to be set up for other teaching blocks. Students reported higher levels of engagement with learning resources and repeatedly highlighted that the blogs supported more self-directed learning and increased their engagement, enthusiasm and motivation for learning than when resources were delivered via the VLE.
Further teaching blocks were added to MedBlogs and feedback from staff and students continued to be positive, with both sets of users finding the emerging MedBlogs learning portal more intuitive and easier to use than the VLE. There was increased teaching staff engagement to support online learning, with a new level of autonomy to personalise their online teaching space through links to journals, specialist organisations and embedding Twitter feeds in their blogs. There was also improved support for integration of themes, systems and specialities across the curriculum.
Ongoing positive evaluation and feedback from staff and students has led to the decision to migrate online delivery of the medical curriculum from the original VLE to a new Dundee MBChB MedBlogs learning portal built in WordPress. The flexibility and usability of blogs have been recognised, with increased engagement of both students and teaching staff.
It is interesting that the Dundee case study used a ‘formal’ institutionally provided blogging platform instead of asking students to use more familiar social media (such as Facebook). Previous studies have noted that students prefer to use technologies that are familiar but wish to keep social and university activities separate (Joint Information Systems Committee (JISC) 2007). This may sound contradictory, but it is important for teaching staff to respect the privacy of students. However, students may set up their own ‘informal’ networks using social media and there are increasing numbers of doctors and students worldwide using social media to support personal development and reflective practice as well as collaborative learning across specialties. The accessibility, social nature and ease of use of social media have supported the development of global online communities of practice across the continuum of medical education. Their use is very much learner-centred and driven by the desire to engage in regular learning conversations. There are several open medical education blogs that are remixing open content from around the web. This approach has become known as free open-access medical education – FOAMed. Content from social media sites, such as YouTube, Vimeo and Flickr, can be surrounded by learning conversations via blog comments and Twitter. An example of the FOAMed approach is Gasclass, an anaesthetics blog, where a case scenario is posted as a blog post and then discussed by anaesthetists around the world on Twitter using the hashtag #gasclass, with additional information introduced over the course of the week.
Responding to the needs of the community
New technologies have provided an unrivalled opportunity to respond to health workforce shortages in rural and remote locations by enabling the development of decentralised medical education programmes and distance learning. The US case studies from Idaho State University and the University of Washington present two models of decentralised medical education, one using video and audio connections to deliver classroom-based teaching and the other in-person delivery supported by VLE.
Case study 16.3 Two models of decentralised medical education, United States
Ruth Ballweg,David Talford and Jared Papa
Two physician assistant (PA) programmes in the US Pacific Northwest rural states have responded to health workforce shortages by developing decentralised medical educational models to serve their region better. The University of Washington’s (UW) MEDEX Northwest PA Program and Idaho State University’s (ISU) PA Program share common goals in developing their decentralised educational sites; however, each institution chose a different model of delivery to respond best to the needs of their specific service area.
Both programmes are required to meet the educational standards of their accrediting body – the Accreditation Review Commission on the Certification of Physician Assistants (ARC-PA), which requires that decentralised educational sites demonstrate educational equivalency between campuses. This includes curriculum, facilities, faculty, staff and university oversight.
By creating decentralised sites, both the UW and ISU sought to provide opportunities which would not otherwise be available to ‘place-bound’ students in rural and widely dispersed geographic areas. These decentralised expansions assured the delivery of proven high-quality curricula without the expensive ‘start-up’ costs of newly established programmes. They also allowed for utilisation of local-community resources (clinicians practising in the communities) and previously unused clinical training facilities.
Idaho State University case study
Idaho is one of America’s most rural states and ranks 49 out of 50 US states in physician-to-population ratio. As the designated health education institution in Idaho, ISU is located in Pocatello, Idaho, 250 miles away from Boise, the main population centre. In deciding to establish an additional site, the PA programme chose a technologically unified classroom approach with both video and audio connections.
Major factors in the ISU implementation included assuring adequate internet bandwidth between the two sites, the inclusion of annual equipment maintenance/upgrade expenses, consideration of classroom acoustics and provision for one full-time audio/visual technician per site. The start-up costs were US$40,000 per classroom. Technical issues included camera considerations and planning for open microphones. Planning for teaching needed to include the engagement of the distant site, developing plans for managing interactive delays and the acquisition of new presentation tools for this type of delivery.
ISU reported positive outcomes and findings. Data revealed high levels of student satisfaction between campuses with continued increase in satisfaction over time. There was equality between the two sites in clinical and written exam scores as well as high National Certification Exam results. The programme is now in the process of expanding to a third training site.
ISU pearls and pitfalls
• Pearls – It is important to maintain an adequate faculty-to-student ratio at all physical sites. Technology inevitably does occasionally fail, so an audio/visual technician at each site is critical to resolve glitches and maintain backup recordings.
• Pitfalls – The central campus can easily be perceived by faculty and students as being superior to the other sites. Engaging faculty at satellite sites in leadership roles can help avoid this.
University of Washington case study
The University of Washington and its MEDEX Northwest PA Program serve as the medical education resources for multiple rural states in the Pacific Northwest. Since the Washington, Wyoming, Alaska, Montana, Idaho (WWAMI) Regional Medical Program was created in 1971, the institution has offered Year 1 of medical education – and some clinical training opportunities – in the states it serves. The expanded need for PAs as a result of health reform generated requests from states, hospitals and local communities to train PAs closer to home as a strategy for building the rural health workforce:
• Central Washington (Yakima) geographic isolation of Central Washington created barriers for students to become PAs. The community was interested in a partnership (1993–2013).
• Eastern Washington (Spokane) is also distant from a medical school: this economic centre needed PAs to provide care in the surrounding rural communities and refer them into Spokane’s regional and tertiary care hospitals (opened 1996).
• Alaska (Anchorage) PAs had become a major fixture of healthcare in Alaska; however it was a hardship for Alaskans to be in Seattle, a large urban centre so far from home (opened 2008).
• Western Washington (Tacoma) is a military town where returning military members sought additional training slots in their home community (opened 2013).
As compared to the ISU technology model, the UW chose an ‘in-person’ delivery model combined with electronic tools (e.g. Moodle) for curriculum management.
Faculty requirements for each distant site (24 students per site) include three full-time PA faculty, and one full-time staff person per site. A large cadre of faculty and staff at the programme’s ‘home’ in Seattle support teaching and administrative needs of all sites. The Seattle site on the UW campus admits 40 students per year. The programme leadership (Program Director and Medical Director) serves all sites. Other faculty rotate across sites to allow students to benefit from their individual expertise.
All courses are ‘chaired’ by a PA faculty member who ‘hires’, orients and monitors teaching by community-based faculty. PA faculty serve as advisors, mentors and role models for students at their sites. An overarching Student Progress Committee reviews student performance regularly. Faculty representatives of all sites serve on this committee. Annual faculty retreats for each course result in updates and modifications, which are implemented across all sites.
In terms of outcomes, student characteristics – upon admission – are similar across all sites (32 years of age and 8 years of clinical experience prior to entry). Students in rural sites appear more likely to enter primary care employment. Students in decentralised sites tend to choose employment in their home communities. Student performance varies little across sites with respect to grades or board performance.
UW pearls and pitfalls
• Pearls – It is important to recruit stable faculty who are willing to integrate themselves fully into their new community. Similarly, it is important to create systems in the community as a substitute for those usually found in a larger academic setting.
• Pitfalls – The coordination of faculty and students takes time – and commitment – from programme leadership. Flexibility in response to crises is the key to success.
Two PA programmes have successfully developed and implemented decentralised medical educational programmes in two very different models. Both programmes have been successful in increasing student throughput and expanding access in remote and rural communities.
Similarly, the case study from Uganda demonstrates how communication technologies can be used to support teaching effectively across international boundaries. This case study, it may be argued, offers a vital opportunity for medical schools to share expertise and support work in less well-resourced communities and countries.
Case study 16.4 Using communication technology for surgical skills teaching in Uganda – a pilot study among intern doctors at Mulago National Referral and Teaching Hospital
Josaphat Byamugisha, Yosam Nsubuga, Mark Muyingo, Amy Autry, Sharon Knight, Felicia Lester, Gerald Dubowitz and Abner Korn
Mulago National Referral and Teaching Hospital in Kampala, Uganda, delivers babies for 32,000 mothers annually. Interns rotate through obstetrics, medicine, paediatrics and surgery every 3 months. Given such a large service demand, it made sense to explore the use of technology such as the internet to augment instruction in basic skills such as suturing.
Video internet communication through Skype to teach and evaluate basic surgical skills was explored for intern physicians rotating in obstetrics and gynaecology. A selected group had three video teaching sessions with the University of California San Francisco (UCSF) faculty via Skype. We found an improvement of 50 per cent or more for interns who participated in online suture session. Participation in the sessions improved two-handed knot tying significantly and was found to be helpful. The interactive nature of the online teaching was enjoyable, equal to in-person teaching. All UCSF faculty involved in the teaching sessions enjoyed participating and thought the interns improved their knot-tying skills.
Remote teaching is feasible, effective and well accepted by both learners and teachers. Repetitive remote teaching sessions may encourage more independent learner practice of skills. In under-resourced settings, where faculty time is limited and visiting faculty are not always possible, this technology can improve surgical skills teaching and retention, even for basic skills.
The opportunities offered by new technologies
The Dundee and Singapore case studies highlight how new technologies can offer new and innovative opportunities for learning compared with existing technologies, especially VLEs and organisational information repositories that archive material.
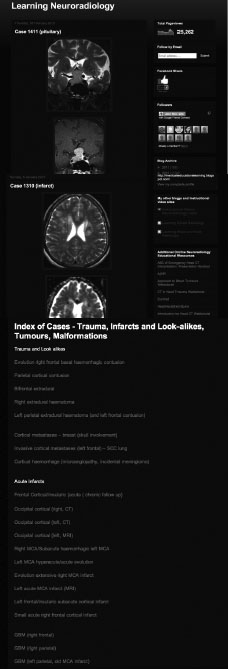
Case study 16.5 An online hyperlinked radiology case repository to facilitate postgraduate training in diagnostic radiology, National University of Singapore
Goh Poh Sun
The Department of Radiology has both a clinical and academic role, with 30–40 residents in radiology following the residency guidelines of the Accreditation Council for Graduate Medical Education International (ACGME-I 2013). The 24 clinical radiologists in the department have a subspecialty focus and share teaching duties. The objective of building up an online radiology case repository was to develop a collection of clinical cases that present the major and important diagnostic categories encountered in clinical practice, to allow residents in training the opportunity to be exposed to a wide variety of cases in each category, with a standardised and comprehensive exposure to cases representing the full clinical spectrum (from typical, to less typical, and atypical cases, and clinical examples with confounding features and multiple diagnoses) and to provide authentic radiology cases for exemplar teaching for postgraduates.
The neuroradiology case repository has over 2,000 online cases accumulated over the last 2 years. Every day the clinical radiologists used a mobile device to photograph all cases with potential teaching value. The photographs were taken directly off reporting workstations and then anonymised and uploaded on to the case repository. These cases were displayed via an online blog which presented radiology cases thematically, as unknown cases for quiz and drill exercises, and as a hyperlinked index for self-study (Figures 16.1–16.3; Goh 2013). The online case repository closely mirrored the range and complexity of actual clinical radiology practice, with authentic case material. Reusability of material was possible without the need for copyright considerations as the material has been selected and authored in house.
The popularity of the neuroradiology teaching blog was reflected in viewership statistics (over 25,000 views since its inception 2 years ago). Feedback from residents showed that they valued the efficiency of case presentation via online blogs, as well as opportunities for revision and self-study. They also valued online case material to supplement their daily supervised clinical practice since it broadened their clinical exposure. The teaching staff used the online cases to provide a uniform exposure of the core spectrum of case material in neuroradiology for the residents. Having a large and continually developing online repository of cases allowed a written curriculum to be elaborated with the actual spectrum of clinical case material that residents are expected to have reviewed. This has been used for daily case review and discussed in topic-focused tutorials, and in assessments. The case repository has also facilitated peer review of teaching and assessment case material.
The major challenge was to convince fellow departmental teaching staff that this method was the most efficient way of archiving material, as compared to making a note of interesting cases and coming back on another day. The process of building up and utilising the online case repository provided evidence via a working prototype that this process was an efficient and effective method of building up a collection of case material, which was of sufficient quality for teaching purposes.
The online repository provided the wide variety of different cases for drill and practice that is required for mastery training in radiology. Developing a working prototype has demonstrated the value of using instructional technology to users and the development process fostered collaboration amongst students and teachers.
The Dundee case study appeared to be successful, since the blogging platform was not only more intuitive to use but also offered increased functionality that was not possible within current VLE platforms. The usability (ease of use) of a technology is an important, but often neglected, aspect of using technologies in medical education because it determines the motivation of both learners and teaching staff to engage with technology (Sandars and Lafferty 2010). Any new technology may be potentially useful for learning but will never achieve its intended potential unless it has high usability.
Technology is becoming increasingly used in healthcare organisations for information management systems and an important aspect of these systems is the storage of vast amounts of information, both text and images. The complexity of existing systems and their information governance controls, to ensure confidentiality of stored clinical information, limit their potential use for learning. The Singapore case study used a blogging tool to archive radiographical images that were selectively obtained by teaching staff using their own mobile devices. The online images were shared between learners and with their tutors by the use of the social networking capability of the blogging platform to create effective online learning communities.
Both the Dundee and Singapore case studies describe the essential opportunity for personalised learning that new technologies can offer learners. Central to personalised learning is the recognition that the learning needs for an individual learner are unique and there is no ‘one size fits all’ approach to meeting these needs. In response to an identified need, the learner proactively meets these needs by selectively integrating a range of different learning resources, such as content on blogs or from interactions on social networks. This approach is in marked contrast to more traditional didactic approaches.
The context of the use of new technologies
The Leeds, UK, case study highlights how the context in which new technologies are used can produce innovative opportunities for teaching and learning, but also highlights the challenges that have to be overcome if the potential benefits are to be realised. The main advantage of workplace-based assessment is that actual performance of learners in authentic situations can be achieved. These authentic contexts are usually busy clinical environments and the use of mobile devices has great potential; clinical procedures and encounters with patients can be observed by assessors and assessment templates can be completed and uploaded to electronic portfolios (e-portfolios) for both formative and summative assessment.
Case study 16.6 Mobile devices for learning and assessment in clinical settings, University of Leeds, UK
Gareth Frith
Learning through clinical practice is an increasingly important part of the undergraduate curriculum, with students in Years 4 and 5 spending the majority of their time in a range of primary and secondary care clinics and hospitals. It is important that students can effectively learn from this experience by getting prompt assessment of their performance and good-quality feedback from the medical and healthcare professionals with whom they are working.
Since 2010, undergraduate medical students at the University of Leeds have been part of a mobile learning programme (MLP) which has provided students with an iPhone that has both 3G and wireless data connection. The students had the device from the beginning of Year 4 until they graduated at the end of Year 5.
In order to support students’ placement learning, they were provided with access to specific medical content through the Medhand Dr Companion app with copies of medical texts such as the British National Formulary, Oxford Handbooks of Clinical Medicine, Clinical Specialties, and other titles. These interactive books are resident on students’ phones so that they are not dependent on network connectivity. As further support, a website with guidance on suitable medical apps relevant to their learning was provided.
Students were encouraged to seek timely ‘near-patient’ feedback on their clinical work through multiple feedback exercises with clinical and other healthcare professionals who had observed them working with patients. Students were provided with a workplace-based assessment iPhone app (MiniCEX/WPBA) to record the assessments and these were synchronised with their progress file (e-portfolio). The accumulated records supported their reflection on their progress through the curriculum to identify strengths and areas for improvement.
Feedback from students was positive about the MLP, but not all students appeared to be technically savvy and a few struggled with the experience. The student response to the use of mobile devices for assessment was tentative at the start, with few assessments undertaken in the first 2 weeks but with a flurry of activity towards the end of the rotation. Interviews with students noted that this was due to lack of confidence in both using a new approach to assessment and also a new technology. Students had to be confident in asking for feedback from a busy clinical team and there was some reticence with appearing unprofessional by using a phone in a clinical environment. As the MLP developed, however, there was increasing confidence and this was partly due to more engagement with the clinical teams by the school taking time to explain the MLP to the professionals and letting them know what to expect from the students. The students were given iPhone cases with the school logo and a text, ‘This is a learning tool provided by the University of Leeds, School of Medicine’, on the back so they could show professionals and patients. Over the long term, students became increasingly engaged with the MLP and many became fully engaged with all aspects of the work, including actively seeking out professionals to provide assessment and feedback.
Also popular was the provision of the mobile content and e-books. Because these were loaded on to the device and not dependent on the networks, they were more usable than internet-based resources. Clinicians also became more engaged with the students in terms of prescribing and challenging the student to use the device and material to look up content.
Some Year 4 students have started to develop their own apps. A series of Objective Structured Clinical Examination (OSCE) toolkit apps were developed by students as part of a research component of the curriculum. The objective was to help students revise for this important clinical assessment exam.
The MLP appeared to be successful in engaging students in both learning and also workplace assessment and feedback.
The Leeds, UK, case study describes the use of mobile devices for both assessment, with MiniCEX templates, and also learning, with a range of apps that can be used as learning resources. This combination offers innovative approaches to teaching and learning, such as the ‘assessment sandwich’. Students can use one of the learning resources on the mobile device prior to a clinical experience, their competence can be assessed and further learning can occur by returning to the learning resources in the device. An educational advantage of such an approach is the situated learning that is more meaningful for the learner. However, the Leeds case study also reveals the difficulties of using new technologies, especially in authentic clinical settings. These difficulties include overcoming misconceptions from both teaching staff and patients (‘students are playing with their phones when they should be learning’), concerns about protecting confidential patient information when entering identifying information or taking photographs and institutional firewalls that block access to cellular networks.
How to ensure the potential for teaching and learning
A new range of digital competences will need to be developed by both teaching staff and learners if social media are to be used effectively to enhance teaching and learning (Sero Consulting 2007). These digital competences include enquiry, production, participation and digital literacy.
Enquiry
Finding information in the first place and then critically evaluating what is found is essential if effective learning is to be obtained from the vast number of websites and other internet resources, such as podcasts.
Production
Activities related to the production of content, including multimedia resources, are becoming increasingly important in teaching and learning, especially if teaching staff and learners are to become active contributing members of online communities.
Participation
Successful online networks and collaborative learning do not occur by chance. The new technologies can easily link widely dispersed learners but there is still the necessary human aspect and this is often forgotten. New competences in communicating and participating online need to be developed so that mutual trust and respect can allow individuals to share information and opinions.
Digital literacy
This is an essential competence since there are rights and responsibilities that need to be considered when publicly sharing information, opinions and support. Confidentiality and respect for privacy are essential components of medical practice but several studies of the Facebook entries made by medical students and junior doctors have highlighted the public nature of most comments and many entries often contain identifiable patient information (Guseh et al. 2009). There have also been several high-profile cases where inappropriate comments have been made about tutors or other students.
It is easy to be cynical about the contribution of new technologies in the provision of effective teaching and learning across the continuum of medical education. Much of this concern is the perception that most of the learning is superficial, yet the South African case study highlights the depth of reflective learning that can be facilitated. There are also important aspects related to the nature of knowledge required for professional practice that need to be critically considered. All healthcare professionals require both information (explicit knowledge) and opinion (tacit knowledge) to answer many of their identified learning needs that arise from dealing with the complex ‘messy’ problems of professional practice. The explicit knowledge can be answered through information sources but the tacit knowledge requires opportunities to network and share experiences with other professionals. This online networking is central to social media and is highlighted in the Dundee and Singapore case studies.
The role of the ‘teaching’ with social media has to be redefined, from a ‘sage on the stage’ to ‘the guide on the side’. A shift from a simple provider of content, including entries on blogs, to that of an educational facilitator that is more concerned with the process of learning is required. This facilitation function requires an understanding of some educational theories that may be less familiar to medical educators, such as ecology of learning and connectivism (Sandars and Haythornthwaite 2007). These theories can inform the medical educator to use approaches that either externally scaffold the learning, such as by providing or suggesting a range of resources within a learning landscape (as in the Dundee case study), or by developing the internal scaffolding of learners through opportunities to reflect on the process of learning, in which the various resources can be connected to construct learning that is personally relevant, and not simply on whether learning outcomes have been met (as in the Singapore case study). These insights of meta-learning are essential for the development of lifelong learners.
The introduction of new technologies can lead to transformational changes in the curriculum (as in the Dundee, Singapore and Leeds case studies), but often the changes are of a lesser degree. The important aspects of connectivity to cellular networks, as well as competence and confidence in using the new technologies, are essential basic requirements that need to be met. There may be poor connectivity in rural and remote areas, and even in urban areas there is often blocking of access due to firewalls in healthcare organisations. The Leeds case study highlights the paradox that is often seen with the so-called net generation of students that have grown up with technology: these students are often only confident and competent in using a small range of familiar technologies (Bennett et al. 2008). Making major changes to existing approaches to educational provision can be highly disruptive and one approach is to blend new teaching and learning approaches supported by new technologies with existing approaches (as in the South Africa case study). One innovative blended approach is the ‘flipped classroom’, in which a phase of online learning deliberately occurs before the face-to-face teaching (Ash 2012).
There appears to be little evidence base to show whether new technologies do produce more effective learning than alternative approaches, but this is typical of other aspects of using technology for teaching and learning, such as more traditional linear learning packages or podcasts. However, all of the case studies identified increased staff and learner satisfaction and motivation to learn, leading to improved engagement with the wider endeavour of teaching and learning across the medical education continuum. It is interesting that the Uganda case study showed improved skills, possibly because of the high interactivity between tutors and learners.
The six case studies have clearly shown that new technologies can contribute to a successful educational programme with increased engagement and contribution by both teaching staff and students. These innovative changes can have transformative aspects with major changes in programmes and the case studies offer useful illustrative examples of the potential impact on teaching and learning. However, there are often barriers to be overcome before the potential of new technologies can be fully realised and these are mainly related to the healthcare and institutional context within which the new technologies are introduced. Future research on the impact of new technologies on teaching and learning is required, especially to identify the critical factors that lead to an impact on learning, such as the design of approaches to learning and the relative potential benefits of different types of new technology, including blended learning.
Take-home messages
• New technologies, such as the internet, have had a major impact on the accessibility and delivery of educational programmes.
• For new technologies to enhance teaching and learning, careful attention needs to be paid to integrating the needs of the learner, the opportunities offered by the technology and the context in which the technology will be used.
• This integration requires a ‘learning-centric’ rather than a ‘technology-centric’ approach.
• The effective use of social media and other new technologies to enhance teaching and learning requires the development of a new range of digital competencies by staff and learners: enquiry, production, participation and digital literacy.
• Used well, social media and new technologies can contribute to increased student engagement and reflective and active learning.
Bibliography
ACGME-I (2013) Accreditation Council for Graduate Medical Education International. Online. Available http://www.acgme-i.org (accessed 24 March 2015).
Ash, K. (2012) ‘Educators evaluate flipped classrooms’, Education Week, 32(2): s6–8.
Bennett, S., Maton, K. and Kervin, L. (2008) ‘The ‘digital natives’ debate: A critical review of the evidence’, British Journal of Educational Technology, 39(5): 775–86.
Goh, P.S. (2013) Learning neuroradiology blog. Online. Available http://learningneuroradiology.blogspot.sg (accessed 12 March 2013).
Guseh, J.S., Brendel, R.W. and Brendel, D.H. (2009) ‘Medical professionalism in the age of online social networking’, Journal of Medical Ethics, 35(9): 584–6.
Joint Information Systems Committee (JISC) (2007) In their own words: Exploring the learner’s perspective on e-learning, Newcastle: Joint Information Systems Committee.
Lenhart, A., Purcell, K., Smith, A. and Zickuhr, K. (2010) Social media and mobile internet use among teens and young adults, Washington, DC: Pew Internet and American Life Project.
Sandars, J. and Haythornthwaite, C. (2007) ‘New horizons for e-learning in medical education: Ecological and Web 2.0 perspectives’, Medical Teacher, 29(4): 307–10.
Sandars, J. and Homer, M. (2008) ‘Reflective learning and the net generation’, Medical Teacher, 30(9–10): 877–9.
Sandars, J. and Lafferty, N. (2010) ‘Twelve tips on usability testing to develop effective e-learning in medical education’, Medical Teacher, 32(12): 956–60.
Sero Consulting (2007) Next generation user skills: A report for digital 2010 and the SQA: Sero Consulting. Online. HTTP: www.sqa.org.uk/sqa/files_ccc/HNComputing_NGUSReport_NextGenerationUserSkills.pdf (accessed 8 May 2014).