Chapter 2
Avoidant Personality Disorder and its Relationship to Social Anxiety Disorder
James Reich Department of Psychiatry, UCSF Medical School, and Department of Psychiatry and Behavioral Health, Stanford Medical School, San Francisco, CA
Abstract
This chapter is a review of the empirical literature on the relationship of avoidant personality disorder (APD) and social anxiety disorder (SAD). Research reviewed included comorbidity, longitudinal treatment outcome, statistical analysis of social anxiety symptoms in large populations and genetic findings. APD is found to be an internally consistent personality disorder that can be reliably measured. APD causes morbidity through interfering with social interactions and may affect such important life parameters as dating, marriage, friendship and employment. APD is also relatively common in general and clinical populations. This prevalence and morbidity make it an appropriate focus of clinical treatment. APD and SAD share symptoms (differing only in severity), are responsive to the same pharmacological and psychotherapeutic interventions and seem to be identical genetically. The best conceptualization is that SAD is a milder variant of APD and that they are the same disease. The DSM diagnoses of SAD and APD have gradually moved closer together and currently there are no specific distinguishing features of the two disorders found.
Keywords
social anxiety disorder
avoidant personality disorder
diagnosis
Introduction
There has been a long-standing question as to how social fears relate to personality disorders. At one time anxiety was considered the hallmark of a personality disorder, e.g., the concept of neurosis. The development of the avoidant personality disorder (APD) category in DSM-III stimulated interest in the relationship of social fears to personality disorders. By examining the relationship of social anxiety disorder (SAD) to the personality disorders, clinicians and researchers could examine this question empirically in disorders defined by specific criteria.
The conceptualization of APD in DSM-III relied heavily on the work of Millon (1991). Millon felt that although APD would overlap to some extent with schizoid, schizotypal, dependent and paranoid personality disorders, it was a clear category in its own right. (Many DSM personality disorders overlap with each other to some extent.) For Millon the distinction between APD and SAD was clear. As he put it, “Avoidant is essentially a problem of relating to persons; social anxiety disorder is largely a problem of performing in situations. The avoidant PD has a feeling of low self-esteem; social anxiety disorder implies no such self critical judgment” (Millon, 1991, p. 356).
Diagnostic issues using the DSM
The diagnosis of both SAD and APD using the DSM system has been a moving target as the criteria change somewhat with each revision (see Table 2.1). The DSM-III criteria for APD emphasized low self esteem, social withdrawal and sensitivity to rejection. SAD emphasized social withdrawal, but also lists fear of being humiliated, which could be seen as very similar to the APD criteria of low self esteem. Already we have questions about the overlap of the two disorders. If someone is afraid of social situations due to fear of humiliation, wouldn’t that lead to low self esteem? If someone avoided social situations due to low self esteem, but did not have performance difficulties, behavior theory would tell us that the low self esteem would decondition as societal pressures brought the person into more and more social situations. At the DSM-III level there are two reasons the disorders would be diagnosed separately, one is a matter of scope and the second is arbitrary. The item of scope is the concept that the difficulty in SAD is much more restricted (applies to fewer situations) than APD. The second reason for separate diagnosis was definitional, that SAD could not be diagnosed in the presence of APD by definition in DSM-III.
Table 2.1
DSM criteria for Social Anxiety Disorder and for Avoidant Personality Disorder
| Social Anxiety Disorder | Avoidant Personality Disorder | |
| DSM-III criteria | A persistent, irrational fear of and compelling desire to avoid, a situation in which the individual is exposed to possible scrutiny by others and fears that he or she may act in a way that will be humiliating or embarrassing. Causes significant distress. Not due to Avoidant Personality Disorder or other mental disorder. | Hypersensitivity to rejection. Unwillingness to enter into relationships. Social withdrawal. Desire for affection and acceptance. Low self esteem. |
| DSM-III-R criteria | A persistent fear of one or more social phobic situations in which the person is exposed to possible scrutiny by others and fears that he or she may do something or act in a way that will be humiliating or embarrassing. Unrelated to other Axis I or III disorders. Exposure to phobic stimulus causes anxiety response. Situation is avoided or endured with anxiety. Causes occupational or social dysfunction or subjective distress. May be generalized. | A pervasive pattern of social discomfort, fear of negative evaluation and timidity, beginning in early adulthood and present in a variety of contexts as indicated by four of the following: easily hurt by criticism; no close friends; unwilling to get involved with people; avoids activities with significant interpersonal contact; reticent in social situations; fears being embarrassed; exaggerates potential difficulties. |
| DSM-IV criteria | A marked and persistent fear of one or more social or performance situations. Exposure to feared social situation invariably provokes anxiety. Feared situations are avoided or endured with distress. Significant occupational or social dysfunction. May be generalized. | A persistent pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation as indicated by four of the following: avoids activities involving significant interpersonal contact; unwilling to get involved with people; shows restraint in intimate relationships; preoccupied with being criticized or rejected; inhibited in new interpersonal situations; views self as socially inept, unappealing or inferior; is unusually reluctant to take personal risks. |
| DSM-5 criteria | Fear or anxiety related to one or more social situations. Patient fears that their acts or anxiety will result in humiliation, embarrassment or rejection by others. Social situations almost always provoke fear or anxiety. The fear is out of proportion to the actual threat. Minimum duration six months. The only subtype is “performance” which is restricted to speaking or performing in public. | Unchanged from DSM-IV. |
At the DSM-III-R level there was still the same conceptual overlap, but several factors have now made the overlap stronger. The definitional exclusion of a SAD diagnosis in the presence of APD has (appropriately) been dropped. Research in SAD showed that it can appear in more than one setting and therefore can be generalized. The DSM-III-R has responded to this empirical data by creating a generalized version of SAD which was then called generalized social phobia (GSP). This again reduces the distance between the two disorders. The underlying theoretical concept that APD is social withdrawal without performance problems and SAD was performance problems without self esteem difficulties is more or less retained. The APD criteria of reticence in social situations and fears of being embarrassed do begin to sound like performance difficulties, however.
DSM-IV made some changes but we are still basically left with the initial diagnostic question of whether we are cutting nature at the joints by postulating one disorder (APD) of internal image (problems with self esteem) without performance anxiety, and another disorder (SAD) of social performance problems without internal image problems (e.g. problems with self esteem.)
DSM-5 left the definition of APD unchanged. SAD has somewhat different wording but the basic criteria are unchanged. GSP has been dropped with the only subtype now “performance” for problems related to speaking or performing in public. The text describing SAD in DSM-5 indicates there will be overlap with APD. The text discussing APD in DSM-5 states, “There appears to be a great deal of overlap between avoidant personality disorder and social anxiety disorder (social phobia), so much so that they may be alternative conceptualizations of the same or similar conditions...”
Basically the DSM-5 has stopped trying to differentiate between SAD and APD except in the degree of symptoms. Why the two disorders are listed separately is not explained. To further examine the relationship between the two we must turn to the empirical data.
Review of early findings
The findings until 2009 have been reviewed previously (Reich, 2000; 2009; 2010). I will summarize some of the earlier findings here.
Studies comparing SAD to APD
There is the older empirical literature comparing SAD and APD. One aspect examined is the comorbidity of the two disorders. If the disorders were separate we would expect, at best, modest comorbidity. If they were highly related or identical disorders we would expect a much higher overlap. (We wouldn’t expect 100% overlap due to inherent measurement errors—especially for the personality disorders—and the different wording of the two sets of criteria). If there was a high overlap we would want to examine differences between GSP and APD to determine whether, although highly overlapping and similar, there were distinct criteria or features which justified a distinction between the two.
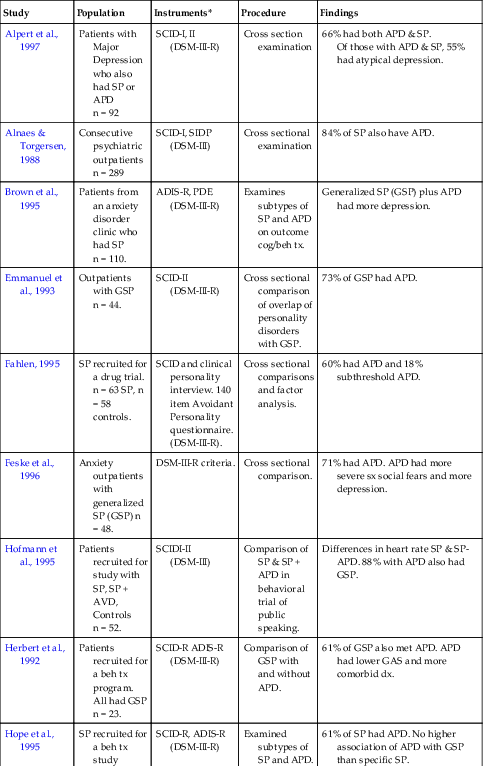
Of the 13 studies reporting on overlap, the average comorbidity was 56% (range 22% to 89%) (see Table 2.2). These figures were drawn from a wide range of populations using different measurement instruments in a wide range of settings. Different interview techniques were used in different settings and interviewers had different levels of training in diagnosing personality disorders. In addition, as disorders wax and wane, there is an additional source of variability. Given that this is about the same level of agreement that might be found comparing two different DSM personality measurement instruments on the same population, and that subthreshold cases were usually not taken into account, this probably represents the highest level of overlap we could expect from these diverse settings and measurement techniques. It seemed clear that GSP highly, if not completely, overlapped with APD.
Table 2.2
Earlier studies comparing Social Phobia (SP) to Avoidant Personality Disorder (APD)
| Study | Population | Instruments* | Procedure | Findings |
| Alpert et al., 1997 | Patients with Major Depression who also had SP or APD n = 92 | SCID-I, II (DSM-III-R) | Cross section examination | 66% had both APD & SP. Of those with APD & SP, 55% had atypical depression. |
| Alnaes & Torgersen, 1988 | Consecutive psychiatric outpatients n = 289 | SCID-I, SIDP (DSM-III) | Cross sectional examination | 84% of SP also have APD. |
| Brown et al., 1995 | Patients from an anxiety disorder clinic who had SP n = 110. | ADIS-R, PDE (DSM-III-R) | Examines subtypes of SP and APD on outcome cog/beh tx. | Generalized SP (GSP) plus APD had more depression. |
| Emmanuel et al., 1993 | Outpatients with GSP n = 44. | SCID-II (DSM-III-R) | Cross sectional comparison of overlap of personality disorders with GSP. | 73% of GSP had APD. |
| Fahlen, 1995 | SP recruited for a drug trial. n = 63 SP, n = 58 controls. | SCID and clinical personality interview. 140 item Avoidant Personality questionnaire. (DSM-III-R). | Cross sectional comparisons and factor analysis. | 60% had APD and 18% subthreshold APD. |
| Feske et al., 1996 | Anxiety outpatients with generalized SP (GSP) n = 48. | DSM-III-R criteria. | Cross sectional comparison. | 71% had APD. APD had more severe sx social fears and more depression. |
| Hofmann et al., 1995 | Patients recruited for study with SP, SP + AVD, Controls n = 52. | SCIDI-II (DSM-III) | Comparison of SP & SP + APD in behavioral trial of public speaking. | Differences in heart rate SP & SP-APD. 88% with APD also had GSP. |
| Herbert et al., 1992 | Patients recruited for a beh tx program. All had GSP n = 23. | SCID-R ADIS-R (DSM-III-R) | Comparison of GSP with and without APD. | 61% of GSP also met APD. APD had lower GAS and more comorbid dx. |
| Hope et al., 1995 | SP recruited for a beh tx study n = 23. | SCID-R, ADIS-R (DSM-III-R) | Examined subtypes of SP and APD. | 61% of SP had APD. No higher association of APD with GSP than specific SP. |
| Holt et al., 1992 | Patients recruited from an anxiety disorders clinic n = 30. | ADIS-R PDE (DSM-III-R) | GSP with and without APD and SP without APD compared. | APD appears to just identify a slightly more severe type of GSP. |
| Jansen et al., 1994 | Patients from a Netherlands outpatient psych clinic n = 117. | Axis I clinical interview, Axis II SCID-II (DSM-III-R). | Panic vs SP for personality variables. | Fear of being embarrassed discriminated best between Panic and SP. 31% of SP had APD. |
| Mersch et al., 1995 | Patients recruited by Swedish newspaper for SP tx study n = 34. | Axis I, clinical interview Axis II, SCID-II (DSM-III-R). | SP with and without personality disorder. | 23% had APD. Those with APD were somewhat more disabled. |
| Noyes et al., 1995 | Panic and SP patients recruited from news media. SP n = 46. | SICD (DSM-III-R), PDQ (DSM-III) | Examines personality traits in Panic and SP. | GSP had 50% more personality traits from the anxious and schizoid clusters than SP. |
| Reich et al., 1989 | SP outpatients n = 14. | Axis I, SCID-I, SCID-II (DSM-III-R). | Pharm tx study | 50% of SP also had APD. |
| Sanderson et al., 1994 | SP, GSP outpatients n = 51. | SCID-II (DSM-III-R). | Cross sectional comparison. | 61% had a personality disorder and 37% had APD. |
| Schneier et al., 1991 | SP drawn from an anxiety disorders clinic n = 50. | Axis I, semi-structured interview Axis II, SCID-II (DSM-III-R). | Comparison of subtypes of SP and relationship to APD. | APD in discrete SP = 21%. APD in GSP = 89%. |
| Tran and Chambless, 1995 | Outpatients with a primary dx of SP n = 45. | Axis I, SCID (DSM-III-R) Axis II, MCMI or MCMI-II. | Comparison of subtypes of SP. | GSP more socially disabled than SP. APD-GSP had more depression than GSP. |
| Turner et al., 1991 | Outpatients SP, GSP = 71. | SCID (DSMII-R). | Cross sectional, association with personality disorders. | 37% had a personality disorder, 22% prevalence of APD. |
| Turner et al., 1992 | SP from an anxiety disorder clinic n = 89. | ADIS-R, SCID-II (DSM-III-R). | Comparison of specific SP, GSP and APD. | GSP is more similar than different from APD, differing on only one of four dimensions (social anxiety). There was no difference in social skills between GSP and APD. |
| Turner et al., 1986 | SP from an anxiety disorder clinic n = 21. | Axis I, ADIS Axis II, consensus (DSM-III). | Comparison of SP and APD. | GAS and SP very similar, but indication that APD have poorer social skills. |


PDE = Personality Disorder Examination (Loranger et al., Cornell University)
SCID = Structured Clinical Interview for DSM Disorders (Spitzer et al., New York State Psychiatric Institute)
ADIS-R = Anxiety Disorder Interview Schedule—Revised (Barlow et al., Boston University)
The association of SAD to other Personality Disorders
Earlier studies which examined SAD and other personality disorders showed some mild association with the DSM schizoid personality disorder cluster, but more strongly to the DSM anxious personality disorder cluster. It is quite possible that some of the association with the schizoid personality cluster (especially in the self report instruments) may be due to measurement artifact. The artifact is due to SAD and the schizoid personality cluster sharing the symptoms of social withdrawal as one of the most prominent symptoms. This means that if a measurement instrument focuses on social withdrawal and does not distinguish between those who wish social contact and those who don’t, two very different disorders will be identified as identical. Overall, after APD, dependent personality disorder had the strongest association.
Treatment and outcome studies for SAD and APD
Although treatment response is not part of the definition for SAD or APD these studies can give us valuable nosologic information. If the same treatments work for different disorders, or symptoms of one disorder get better as a second disorder is treated, this increases the possibility that these disorders are related or may even be the same disorder.
Psychopharmacological treatment studies
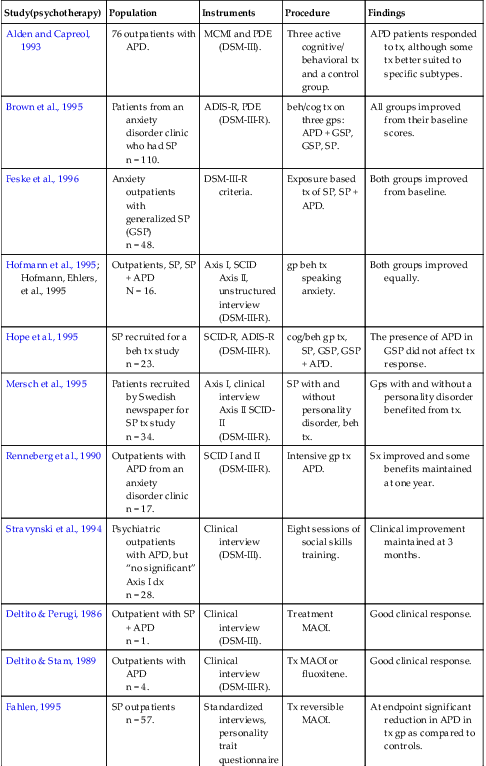
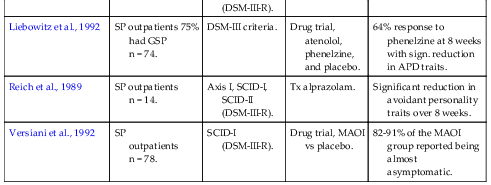
Although the early studies in this area vary in many respects, there was evidence that benzodiazepines, SSRIs and various forms of MAOIs may be effective for APD or for avoidant traits associated with SAD. Many of these studies had good sample size and careful measurements of avoidant personality traits and demonstrated that as SAD symptoms were treated, avoidant personality traits were also reduced (see Table 2.3).
Table 2.3
Earlier treatment studies of Social Phobia (SP) and Avoidant Personality Disorder (APD)
| Study(psychotherapy) | Population | Instruments | Procedure | Findings |
| Alden and Capreol, 1993 | 76 outpatients with APD. | MCMI and PDE (DSM-III). | Three active cognitive/ behavioral tx and a control group. | APD patients responded to tx, although some tx better suited to specific subtypes. |
| Brown et al., 1995 | Patients from an anxiety disorder clinic who had SP n = 110. | ADIS-R, PDE (DSM-III-R). | beh/cog tx on three gps: APD + GSP, GSP, SP. | All groups improved from their baseline scores. |
| Feske et al., 1996 | Anxiety outpatients with generalized SP (GSP) n = 48. | DSM-III-R criteria. | Exposure based tx of SP, SP + APD. | Both groups improved from baseline. |
| Hofmann et al., 1995; Hofmann, Ehlers, et al., 1995 | Outpatients, SP, SP + APD N = 16. | Axis I, SCID Axis II, unstructured interview (DSM-III-R). | gp beh tx speaking anxiety. | Both groups improved equally. |
| Hope et al., 1995 | SP recruited for a beh tx study n = 23. | SCID-R, ADIS-R (DSM-III-R). | cog/beh gp tx, SP, GSP, GSP + APD. | The presence of APD in GSP did not affect tx response. |
| Mersch et al., 1995 | Patients recruited by Swedish newspaper for SP tx study n = 34. | Axis I, clinical interview Axis II SCID-II (DSM-III-R). | SP with and without personality disorder, beh tx. | Gps with and without a personality disorder benefited from tx. |
| Renneberg et al., 1990 | Outpatients with APD from an anxiety disorder clinic n = 17. | SCID I and II (DSM-III-R). | Intensive gp tx APD. | Sx improved and some benefits maintained at one year. |
| Stravynski et al., 1994 | Psychiatric outpatients with APD, but “no significant” Axis I dx n = 28. | Clinical interview (DSM-III). | Eight sessions of social skills training. | Clinical improvement maintained at 3 months. |
| Deltito & Perugi, 1986 | Outpatient with SP + APD n = 1. | Clinical interview (DSM-III). | Treatment MAOI. | Good clinical response. |
| Deltito & Stam, 1989 | Outpatients with APD n = 4. | Clinical interview (DSM-III-R). | Tx MAOI or fluoxitene. | Good clinical response. |
| Fahlen, 1995 | SP outpatients n = 57. | Standardized interviews, personality trait questionnaire (DSM-III-R). | Tx reversible MAOI. | At endpoint significant reduction in APD in tx gp as compared to controls. |
| Liebowitz et al., 1992 | SP outpatients 75% had GSP n = 74. | DSM-III criteria. | Drug trial, atenolol, phenelzine, and placebo. | 64% response to phenelzine at 8 weeks with sign. reduction in APD traits. |
| Reich et al., 1989 | SP outpatients n = 14. | Axis I, SCID-I, SCID-II (DSM-III-R). | Tx alprazolam. | Significant reduction in avoidant personality traits over 8 weeks. |
| Versiani et al., 1992 | SP outpatients n = 78. | SCID-I (DSM-III-R). | Drug trial, MAOI vs placebo. | 82-91% of the MAOI group reported being almost asymptomatic. |
Psychological treatments
Eight psychological treatment studies of APD or SAD associated with APD are reviewed in Table 2.3. These studies used cognitive or behavioral treatments or both. Overall it appears that both APD and SAD comorbid with APD do respond to treatment. The SAD without GSP tends to be least disabled, followed by GSP followed by GSP comorbid with APD. Although all start at different baselines of morbidity, all seem to respond to treatment (see Table 2.3).
Course of SAD
Early prospective studies on the course of SAD generally find that SAD tends to be chronic with low remission rates. This rate is the same for SAD with GSP and without. Although we have no specific measures of course of GSP plus APD, the high level of overlap of GSP and APD seemed to indicate a similar course for APD and GSP.
APD and state effects
There is also evidence that APD symptoms could be affected by state anxiety and depression (see longer discussion below).
Findings from more recent literature
Recent empirical evidence on the construct of APD
An interesting report analyzing data from the National Comorbidity Study indicates that subclinical social anxiety forms a continuum with SAD (Ruscio, 2010).
Two reports focused on whether APD represented an internally consistent diagnosis (Baille & Lampe, 1998; Grilo, McGlashan, & Morey, 2001). Both of these studies examined several hundred patients and examined whether APD appeared to be an internally consistent diagnosis. Both reports found that a single factor model seemed to fit the data best and that APD was internally consistent. A third report had over a thousand subjects and examined whether the APD criteria fit a prototype and whether there was a natural cut off point to indicate transition into a disorder from a trait (Humelen, Wilberg, Pedersen, & Karterud, 2006). The findings were that APD appeared to be a homogenous disorder and that there was no number of criteria to indicate where the pathology increased to indicate a personality disorder. APD appeared to be a dimensional construct. This agreed with a fourth report, an empirical study of the taxonomy of SAD and APD which found them to be part of a one-dimensional dimension (Crome, Baillie, Slade, et al., 2010) as did a fifth report, an analysis of a large, national epidemiological population (El-Gabalawy, Cox, Clara, et al., 2010). A sixth examination of two large epidemiological studies found that the structure of SAD was dimensional (Humelen, Wilberg, Pedersen, & Karterud, 2007). A seventh evaluation of an epidemiological study of the structure of SAD found a dimensional structure with increased morbidity as the number of symptoms increased (Lampe, Slade, Issakidis, & Andrews, 2003). Basically these seven studies are in agreement.
Recent empirical evidence on the relationship of APD and SAD
There are also a number of empirical reports on the relationship of APD to SAD. One report examined over a thousand patients with standardized techniques (Humelen, Wilberg, Pedersen, & Karterud, 2007). They found that the two disorders were highly related in symptoms, but that APD had more disability and appeared to be a more severe disorder with more personality problems and a lower lever of conscientiousness. An Australian epidemiologic study of over 10,000 subjects compared SP to APD (Lample, Slade, Issakidis, & Andrews, 2003). There was a high degree of overlap of symptoms. Those subjects severe enough to have the APD diagnosis had a greater burden of affective disorder. APD prevalence was 6.5% with no gender difference. Those with more significant APD and SAD symptoms had deficits in ability to form relationships, employment and had increased comorbid with anxiety and depressive disorders.
A large national epidemiologic study found that GSP and APD were basically the same disorder existing along a continuum (Cox, Pagura, & Stein, 2009). A small clinical study found no difference between generalized social anxiety disorder and APD once severity of symptoms was adjusted for (Chambless, Fydrich, & Rodebaugh, 2008). A re-analysis of a large epidemiologic study which did not originally measure APD could not find evidence that there was a difference between SAD and APD (Lampe & Sunderland, 2008). An analysis of a sample of patients with GSP recruited for a treatment trial showed no difference between GSP and APD with the exception of increased morbidity with increased number of symptoms (Marques, Porter, Keshaviah et al., 2012).
A longitudinal study of personality disorders (n = 157) found a significant association between APD and SP (McGlashan, Grilo, Skodol et al, 2000). Another report from the same group examined whether those subjects with APD who also had SAD differed (Ralevski, Sanislow, Grilo et al., 2005). The authors concluded that these two groups did not differ and felt that this was evidence that APD and SP might be alternate conceptualizations of the same disorder. A Swedish self report epidemiological study with 581 subjects examined the overlap of APD and SP (Tillfors, Furmark, Ekselius, & Fredrikson, 2004). They found that the disorders were similar, the major difference being a decrease in function in the APD group which appeared to be related to the level of anxiety. A large clinical epidemiological study of 859 psychiatric outpatients and personality disorders found a 14.9% prevalence of APD (Zimmerman, Rothschild, & Chelminski, 2005). There was a high association with SAD, and the presence of major depression, generalized anxiety disorder, panic disorder and post traumatic stress disorder significantly increased the probability of finding APD.
A slightly dissenting view was found in a paper and pencil test of healthy college students (Carter & Wu, 2010). APD and SAD were found to be highly correlated but the authors felt SAD had a greater relation to panic and APD to depression. Given the low morbidity of this population and the use of only self report measures given across a one hour period, this report would have to be considered exploratory at this point. Also as depression can increase the apparent level of symptoms of personality traits, the APD relationship to depression may have been found for that reason.
Basically all the empirical findings in this section are similar and find that APD and SAD do not have differentiating major features although they find that APD has more dysfunction than SAD. This would be expected if APD is the same disorder only with somewhat more severe symptoms
State Personality Effects
Recently there has been the increased understanding of state effects, also referred to as state personality disorder (Reich, 2005; 2007). This is the phenomena where personality traits appear under the stress of an Axis I disorder or other stress and remit when that stress is gone. It has become more and more recognized that many personality disorders have both state (transient stress induced symptoms) and trait (relatively enduring) components.
There are a number of reports that lend credence to the idea that APD has state components. One report indicates that the presence of APD in GSP can be predicted with 85% accuracy by a combination of introversion and depression (van Velzen, Emmelkamp, & Scholing, 2000). It would appear that the depression would be predicting state personality aspects. A two-year follow-up of 266 subjects with APD indicated both state and trait components (McGlashan, Grilo, & Sanislow, 2005). Two state components which were specified were (1) avoiding jobs that are interpersonal and (2) avoiding potentially embarrassing situations. In another report from the same group the finding was that APD tended not to remit if an underlying anxiety or depressive disorder had not remitted, which would be consistent with the state personality model (Shea, Stout, Yet et al., 2004). The findings cited above of increased prevalence of APD with the presence of certain Axis I disorders is also consistent with this finding. Overall the empirical findings are consistent with a state personality component to APD.
Findings on Disability
There are two reports from large epidemiologic studies indicating a high level of comorbid alcohol or substance abuse disorders with social anxiety disorder. The first of these indicates 17% self medication with alcohol and 4.5% self medication with alcohol and drugs for SAD. Those who did so had an increased probability of also being diagnosed with APD (Robinson, Sareen, Cox et al., 2009). The second found an increased rate of alcohol and substance abuse in SAD and those who were comorbid for either had a higher prevalence of other Axis I disorders (Schnier, Foose, Hasin et al., 2010).
One attempt was made to estimate the economic costs of SAD (Acaturk, Smit, de Graaf et al., 2009). The annual costs were approximately 6100 European pounds per person with SP over one year’s time.
Longitudinal studies
There were no longitudinal studies of APD but there were three for SAD (Beard, Mooitra, & Weisberg, 2010; Blanco, Xu, & Schneir, 2011; Vriends, Becker, Meyer et al., 2007). Although there were some remissions the authors of all three concluded that SP could be a chronic disorder. this would leave us with a reasonable assumption that APD, a more severe form of SAD, would be chronic as well.
Genetic findings
There is one major report on the genetics of APD and its relationship to SAD (Reichborn-Kjennerud, Czajkowski, Torgersen et al., 2007). This study examined 1,427 female twin pairs to examine similarities and differences in genetic predisposition. The results were rather striking – the genetic basis of the two disorders is identical, although environment may affect the nature of the development of symptoms.
Discussion
We know that APD appears to be an internally consistent disorder that likely has no cut off number of symptoms to indicate that it is a disorder rather than a dimensional symptom construct. It appears to have both state and trait personality components. With the exception of some increased disability in APD compared to SP the two disorders share the same symptoms, respond to the same treatments, are genetically identical and appear to be the same disorder.
What we have is a well validated dimensional personality disorder with enough clinically significant symptoms to warrant clinical attention and treatment.
The only real question is nosological—how to classify SAD and APD as they appear to be the same disorder.
One question is whether APD belongs in the section of personality disorders. There is no cut off number of criteria where pathology suddenly begins. The DSM approach has been to consider personality pathology disorders with an identifiable cut off point. However, researchers have now come to understand the disability caused by many personality disorders is related more to the number of criteria met and not to specific cut off points. I believe that even though it is continuous, personality pathology of clinical significance is worthy of inclusion in the DSM personality section and is consistent with evolving empirical evidence.
Another aspect worth discussing is treatability. Personality disorders have been considered a class that was relatively treatment resistant. Our evidence is that a fair amount of APD pathology will respond to treatment. This again is consistent with our evolving knowledge of treatment of this and other personality disorders. We have come to understand that the courses of personality disorders are much more variable than we once thought and there is evidence of at least partial response to treatment. Once again the evolving course of knowledge would make us accept amenability to treatment as an aspect of certain personality disorders.
The evidence indicates APD and SAD are different manifestations of one disorder. This is a position the DSM is moving toward slowly. The question then becomes whether this single disorder belongs in the anxiety disorders or the personality disorders. It would appear that the best route would be hierarchical, to merge the less severe form with the more severe. As APD is the more severe form this would have us place both disorders in the personality category, but with the understanding that the milder variant (SAD) resembles an anxiety disorder. Perhaps including it in both sections and cross referencing it as the DSM-5 has done is a reasonable administrative compromise.
Conclusions
APD is an internally consistent personality disorder that can be reliably measured. As with many other personality disorders it has both state and trait personality components. APD causes morbidity through interfering with social interactions and may affect such important life parameters as dating, marriage, friendship and employment. APD is also relatively common in general and clinical populations. This prevalence and morbidity make it an appropriate focus of clinical treatment. APD and SAD share symptoms (differing only in severity), are responsive to the same pharmacological and psychotherapeutic interventions and seem to be identical genetically. The best conceptualization is that SAD is a milder variant of APD and that they are the same disease. APD’s potential response to treatment engenders cautious clinical optimism about its treatment.