Chapter 8
Social Phobia1 as a Deficit in Social Skills
Ariel Stravynski
Angela Kyparissis
Danielle Amado
Department of Psychology, University of Montreal, Montreal, Canada
Abstract
When considering social phobia as a presumably unique pattern of behaviors strongly characterized by reticence, evasion, withdrawal, and absences, one is struck by the extent to which the social functioning of the socially phobic is disturbed. One of the various conceivable explanations for this wide-ranging diffidence is that socially phobic individuals lack the requisite social skills in order to perform proficiently in various social (and anxiety-evoking) situations. Anxiousness in this view would appear to be a by-product of the inability to act effectively. The hypothesis of skills deficits has also important therapeutic implications. As a putative causal factor of social phobia, it is viewed as calling for and indeed amenable to treatment by, namely social skills training. Our principle goal in this chapter is to examine the evidence having a bearing on the “skill-deficits” account of social phobia. In order to do so, we first attempt to clarify the concept of “social skills”. Subsequently, as psychological constructs cannot exist apart from the way in which they are measured, we shall investigate the validity of the corresponding tests devised to identify and quantify social skills deficits. Once the matter of their validity is dealt with, we should be able to proceed and tackle the more precise questions of whether subgroups of socially phobic individuals differ from one another in this respect and whether the socially phobic differ in their social skills from normal and/or other contrast populations. Finally, we shall gauge the value of the concept of skills deficits indirectly, through the perspective of treatment by means of social skills training.
Keywords
social phobia, social skills deficits, social skills training, social functioning
Introduction
When considering social phobia as a presumably unique pattern of behaviors, one is struck by its elusive and mostly negative quality as well as by the extent to which the social functioning of the socially phobic (in various spheres of life) is perturbed (e.g., Schneier, Heckelman, Garfinkle, Campeas, Fallon, et al., 1994). The socially phobic conduct is strongly characterized by reticence, evasion, withdrawal, and absences. In short, from an observer’s point of view, what looms large is what these individuals do not do or fail to achieve.
Some activities and situations vital to participation in social life are seldom engaged in or entered into. Opportunities for advancement and the enrichment of social or personal life are often forgone. In the relatively circumscribed social interactions these patients engage in, little is said and feelings or opinions are walled in and remain mostly unexpressed. These individuals’ very real suffering is concealed as well. Their anxious distress—a permanent feature of their lives—is typically dissimulated and kept secret.
What could account for this peculiar pattern of conduct?
One of the various envisageable explanations for this wide-ranging diffidence is that socially phobic individuals lack the requisite social skills in order to perform proficiently in various social (and anxiety-evoking) situations (Curran, 1979, p. 319; Stravynski & Greenberg, 1989, p. 208; Marks, 1985, p. 615). The anxiousness reported by the socially phobic would appear in such a scheme of things to be a by-product of the inability to act effectively. Alternatively, as the received view would have it, one could claim just as plausibly that performance is undermined by an unmanageable and therefore disorganizing level of anxiousness (e.g., Eysenck & Calvo, 1992).
Whether currently unskilled socially phobic individuals have ever been socially skilled and if so, how these skills were lost, is an additional theoretical puzzle awaiting resolution. Not least, the hypothesis of skills deficits has also important therapeutic implications. As a putative causal factor of social phobia, it is viewed as calling for and indeed amenable to treatment by, namely, social skills training.
Aim and method
Our principle goal in this chapter is to examine the evidence having a bearing on the “skill-deficits“ account of social phobia. Before reaching that stage however, several intermediate steps need to be taken.
We must first clarify the concept of “social skills” generally and then inquire into its soundness with regard to social phobia specifically. Subsequently, as psychological constructs cannot exist apart from the way in which they are measured, we shall have to investigate the validity of the corresponding tests devised to identify and to quantify social skills deficits generally and their extent in social phobia in particular.
The theoretical construct (if it is that) of skills deficits as well as the psychometric measures assessing it, are indispensable to the practical testing of the hypothesis. Once the matter of their validity is dealt with, we should be able to proceed and tackle the more precise questions of whether subgroups of socially phobic individuals differ from one another in this respect and whether the socially phobic differ in their social skills from normal and/or other contrast populations. The demonstration of such differences is a necessary (but not sufficient) condition for the ultimate query: do skills deficits play a causal role in the socially phobic pattern of behavior?
Finally, we shall gauge the value of the concept of skills deficits indirectly, through the perspective of treatment by means of social skills training. As the critical period for onset of social phobia is likely to be between the ages of 15 to 18 (see Stravynski, 2007, p.89) we have not included studies of “childhood social phobia”. We regard social phobia (as distinct from anxious states) in children with skepticism.
The notion of social skills
The notion of social skills originates in attempts to make sense of normal social conduct. One possible perspective on social behavior is to consider it in analogy (first put forward by Argyle & Kendon, 1967) to a motor skill. Seen in that light an individual would be acting according to pre-established rules in pursuit of certain goals (e.g., dancing, skating or writing). This perspective stresses the rule-bound aspect of social behavior as well as its dynamism (i.e. undergoing constant changes in light of various signals emanating from the social environment). A failure to perform proficiently—as in a sporting activity—is accounted for (by analogy) in terms of inadequacy or lack of requisite skills (Trower, Bryant, & Argyle, 1978).
This outlook of problematic or deficient “social skills” is an attempt to account for the commonplace observation that certain individuals are socially inept, are forgoing socializing, or have failed to realize a certain normative potential (e.g., finding a mate or holding a position commensurate with their level of education).
Heuristically, this explanatory hypothesis has caught the imagination of numerous theoreticians and has had a wide influence not least among practicing clinicians. In consequence, it has been applied to various patterns of abnormal behavior: depression (Lewinsohn, 1974), sexual dysfunction in men (Lobitz & LoPiccolo, 1972) and of course social phobia (see Stravynski & Greenberg, 1989), among others. Such an account ties problems in social skills with membership in certain categories of abnormality (e.g., Hersen, 1979). However, the very breadth of application of this concept may paradoxically beg the question: does it have any specific content?
What are social skills?
Before delving into the meaning of social skills, it may be useful to clarify the concept of skill. The notion of skill in itself, despite its frequent use and wide-ranging application, has proved exceedingly difficult to define (see Adams, 1987). One definition puts it as: “… clearly a learned ability which involves co-ordination of different elements in a goal-directed manner … Skilled behavior may be viewed as an active self-assembled coalition of diverse resources in the service of a unitary goal. This relational aspect of skill includes not only the interactive relations among different segments of the act in question but the interaction between this act and the external environment” (O’Connor, 1989, p. 219).
This rather abstract definition is in stark contrast with the fact that a very appealing feature of the “skills deficits” hypothesis is that it involves a seemingly sensible and down to earth reasoning, unburdened by abstract concepts. The impression of clarity and concreteness is, unfortunately, somewhat deceptive. As remarked by Curran (1979) “… everyone seems to know what good and poor social skills are …” but “… no one can define them adequately” (p. 321). One of the first and oft quoted definitions of social skills (Libet & Lewinsohn, 1973) regarded it as “the complex ability to maximize the rate of positive reinforcement and to minimize the strength of punishment from others” (p. 311). This functional definition does not pinpoint specific behaviors, but relies on their success in generating rewards and minimizing punishment as an indication of skill. This is so ambiguous as to leave, for example, the less than socially successful individuals without any guidance as to what they could do to improve their lot. Furthermore, this definition doubtlessly also encompasses behaviors that are usually considered less than adequate (e.g., temper tantrums, illness behavior) or morally unsavory (e.g., hypocrisy, manipulativeness, deceit).
Another functional (and rather sweeping) definition (albeit a negative one in terms of social inadequacy) emphasizes control over others: “a person can be regarded socially inadequate if he is unable to affect the behavior and feelings of others in the way he intends and society accepts” (Trower, et al., 1978, p. 2).
A different sort of definition (see Curran, 1979 and McFall, 1982 for overviews) goes to the other extreme by specifying what are deemed essential elements of skillful performance. Eye contact, appropriate content of speech, and reciprocity, among others, are put forward as such. Lists of elements, however concrete or comprehensive, do not make a definition. Nor is it clear why the listed elements are given prominence while many others that come to mind (e.g., posture, facial expression), remain languishing in obscurity.
Other definitions (e.g., Bellack, 1979), further argue for the integration of an amalgam of cognitive processes (e.g., social perception), to the behavioral elements of social skills (p. 98). Although this splitting of constituting elements must be ultimately judged by its validity and utility, this may also pose a risk of weakening the construct of social skills through its expansion, to the extent of it becoming a metaphor for all behavior.
Although no satisfactory definition of social skills (and by implication their absence or inadequacy) is available today, the term has wide currency in clinic-lore and seems to be endowed with a certain concrete obviousness in the eyes of its users. Embedded in this face validity seems to be the sense that “it” is a set of behaviors or characteristics and therefore, palpably recognizable. In Wlazlo, Schroeder-Hartig, Hand, Kaiser and Münchau (1990) for example, clinicians had little trouble identifying skill-deficient patients from the clinical notes. Conversely, Juster, Heimberg, and Holt (1996) argue that “in our clinic most social phobic persons are found to possess adequate social skills but are inhibited when it comes to applying their skills in social situations” (p. 84). The conceptual and empirical basis for both sets of observations remains unclear. By using the same term for skill, are they all referring to the same construct encompassing the same set of activities?
Perhaps greater clarity in this respect might be profitably gained from considering the way the notion of social skills has been used in research.
Two views of social skills
The notion of social skills has been thoroughly analyzed by McFall (1982, pp. 1-12) and Curran (1979, pp. 319-354) and our discussion relies on both.
The construct of social skills may be said to have been construed in two different ways. One might be termed intra-personal and the other interpersonal. The intra-personal outlook considers social skills to be a mental construct or trait, while the interpersonal defines it behaviorally as a pattern of activities. In some studies, the two approaches are confusingly mixed. While the design and measurement follow a behavioral perspective, the conclusions are compatible with a mental trait perspective.
The intra-personal view of social skills
Regarding social skills as a psychological process “within” the individual or, in short, a trait is the most common use of the term. A trait is a hypothetical mental construct, constituting a shorthand for certain mental processes that predispose an individual to act in a particular way. Being “socially skilled” in the intra-personal sense is not an observable performance. Rather, it is an underlying quality that manifests itself in or may be inferred from, actual behavior. Trower (1995, p. 55) for example distinguishes between the components of social skills (i.e. behaviors or repertoires of actions) and social skill (i.e. the process of generating skilled behavior). The value of such a view is in the explanation it offers: the mental construct (or process) is the driving force within, which gives rise to the action without. As a trait, social skills are something that one has (or lacks) and are an attribute of the person.
With social skills, as with all traits, such an analysis runs the risk of resorting to what amounts to a tautology. Initially, inadequate social skills are inferred from an inept performance. Yet the very same lackluster performance is subsequently seen as resulting from the deficient skills. Such an account is untenable as the inferred trait cannot be used simultaneously as a causal explanation for the same behavior. For a hypothetical structure to be endowed with explanatory power, it must be shown to be valid in a series of independent studies. Namely, that it makes a difference and that it has a myriad of predictable consequences. Such independent demonstrations are lacking.
An advantage of the trait approach to social skills is that it does not require a specific definition of such skills; for such a definition, as we have seen earlier, is clearly unavailable. As it is an abstraction, it is sufficient that such construct meets certain psychometric criteria to be considered useful, even if not entirely valid. The practical question we shall be considering later is whether it does. The omens in this respect are not encouraging.
As with all trait conceptions (e.g., intelligence), social skills are seen as inherent to an individual; ploddingly stable over time and fairly consistent over situations. These assumptions are central to and embedded in the assessment of social skills as a trait; these methods would be incoherent otherwise. Whether this is actually the case remains to be seen.
The interpersonal view of social skills
Within this approach, social skills are construed as specific features of behavior and deemed the “building blocks of the individual’s overall performance in each interpersonal situation” (McFall, 1982, p. 7). The specific appropriate social skills are a function of given situations and the ensuing interactions with the persons involved. Thus, “social skills are an attribute of a person’s situation-specific behavior, not of the person per se” (ibid.). It follows that “no particular behavior can be considered intrinsically skillful, independent of its context” (ibid.). Although clear at a theoretical level (and especially as an incisive critique of the trait approach), the interpersonal perspective has its own shortcomings and ambiguities.
It is not clear for example what units of behavior (constituent structures of behavior) are important to consider and how to measure their effects (function of behavior) on the environment. Nor is it obvious what makes a performance satisfactory. The implication of this approach for assessment is that situations must be taken into account so that behaviors are set in context. Its most far-reaching consequence however, is that, ultimately, social skills are idiosyncratic and context-dependent. Consequently, these cannot be measured by some general test.
This then is the backdrop against which the intricate issue of how to assess and quantify social skills or their deficits, to put it negatively, has to be addressed.
Assessment of the social skills of the socially phobic
Given the theoretical ambiguity of the fundamental notion of “social skills”, the task of developing precise and valid measurement methods has to be carried out on rather unstable foundations. Undaunted, researchers have constructed a number of such devices.
The various proposed methods for the assessment of social skills have been comprehensively reviewed in McNeil, Ries, and Turk (1995) and earlier in Glass and Arnkoff (1989) and Hersen and Bellack (1977). These may be divided roughly in two: self-report inventories of behavior and simulations of behavior observed by assessors. In what follows, the psychometric characteristics of the measurement methods we have selected will be summarized in their application to socially phobic individuals whenever available. It must be borne in mind however, that most instruments have been developed with student or other participants.
Schematically, the characteristics of the assessment methods we are interested in are typically designated as reliability and validity. Reliability refers to the accuracy of the measurement, conceived of as agreement between assessors, occasions of testing or different items of the test and the overall score. Whereas several types of validity studies can be imagined, commonly two kinds have been reported. Convergent validity concerns the degree of correspondence between the measurement of aspects of social skills and other measures of related phenomena. Discriminant validity denotes a negative relationship.
Occasionally, two types of criterion validity have been reported. Concurrent validity concerns the degree to which the measurement of social behavior goes hand in hand with related features of psychopathology at the present or—as in predictive validity—that might occur in the future.
As carrying out a comprehensive review is not our purpose, we shall only consider those instruments with sufficient background research to document some of their psychometric characteristics with socially phobic subjects. These are of the most direct relevance to our inquiry.
Self-reports
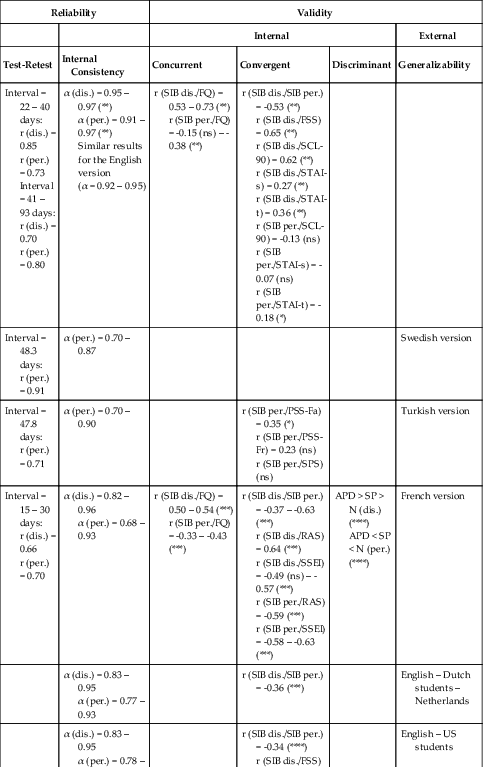
Scale for Interpersonal Behavior
The Scale for Interpersonal Behavior (SIB; Arrindell & van der Ende, 1985) is a multi-dimensional self-report scale (originally devised in Dutch) of assertiveness measuring four domains rated each for performance and related distress. The domains are:
1. display of negative feelings (15 items);
2. expression of personal shortcomings (14 items);
3. display of assertion (9 items);
4. expression of positive feelings (8 items).
Distress is rated on a 5-point dimension ranging from 1 = “not at all” to 5 = “extremely”. Performance is quantified in terms of categories of frequency ranging from 1 = “never do” to 5 = “always do”. Each domain has a score; a general score (separate for distress and performance) is the summation of the scores of all domains. Table 8.1 below summarizes the evidence regarding the soundness of the test.
Table 8.1
Psychometric characteristics of the Scale for Interpersonal Behavior (SIB)1,2
| Reliability | Validity | ||||
| Internal | External | ||||
| Test-Retest | Internal Consistency | Concurrent | Convergent | Discriminant | Generalizability |
| Interval = 22 – 40 days: r (dis.) = 0.85 r (per.) = 0.73 Interval = 41 – 93 days: r (dis.) = 0.70 r (per.) = 0.80 | α (dis.) = 0.95 – 0.97 (**) α (per.) = 0.91 – 0.97 (**) Similar results for the English version (α = 0.92 – 0.95) | r (SIB dis./FQ) = 0.53 – 0.73 (**) r (SIB per./FQ) = -0.15 (ns) – -0.38 (**) | r (SIB dis./SIB per.) = -0.53 (**) r (SIB dis./FSS) = 0.65 (**) r (SIB dis./SCL-90) = 0.62 (**) r (SIB dis./STAI-s) = 0.27 (**) r (SIB dis./STAI-t) = 0.36 (**) r (SIB per./SCL-90) = -0.13 (ns) r (SIB per./STAI-s) = -0.07 (ns) r (SIB per./STAI-t) = -0.18 (*) | ||
| Interval = 48.3 days: r (per.) = 0.91 | α (per.) = 0.70 – 0.87 | Swedish version | |||
| Interval = 47.8 days: r (per.) = 0.71 | α (per.) = 0.70 – 0.90 | r (SIB per./PSS-Fa) = 0.35 (*) r (SIB per./PSS-Fr) = 0.23 (ns) r (SIB per./SPS) (ns) | Turkish version | ||
| Interval = 15 – 30 days: r (dis.) = 0.66 r (per.) = 0.70 | α (dis.) = 0.82 – 0.96 α (per.) = 0.68 – 0.93 | r (SIB dis./FQ) = 0.50 – 0.54 (***) r (SIB per./FQ) = -0.33 – -0.43 (***) | r (SIB dis./SIB per.) = -0.37 – -0.63 (***) r (SIB dis./RAS) = 0.64 (***) r (SIB dis./SSEI) = -0.49 (ns) – -0.57 (***) r (SIB per./RAS) = -0.59 (***) r (SIB per./SSEI) = -0.58 – -0.63 (***) | APD > SP > N (dis.) (****) APD < SP < N (per.) (****) | French version |
| α (dis.) = 0.83 – 0.95 α (per.) = 0.77 – 0.93 | r (SIB dis./SIB per.) = -0.36 (***) | English – Dutch students – Netherlands | |||
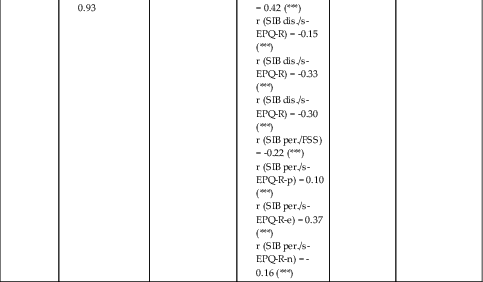
| α (dis.) = 0.83 – 0.95 α (per.) = 0.78 – 0.93 | r (SIB dis./SIB per.) = -0.34 (****) r (SIB dis./FSS) = 0.42 (***) r (SIB dis./s-EPQ-R) = -0.15 (***) r (SIB dis./s-EPQ-R) = -0.33 (***) r (SIB dis./s-EPQ-R) = -0.30 (***) r (SIB per./FSS) = -0.22 (***) r (SIB per./s-EPQ-R-p) = 0.10 (***) r (SIB per./s-EPQ-R-e) = 0.37 (***) r (SIB per./s-EPQ-R-n) = -0.16 (***) | English – US students | |||
Note: There are no p values given for test-retest correlations.
1 Based on the following studies: Arrindell, Bridges, van der Ende, St. Lawrence, Gray-Shellberg, Harnish, et al. (2001); Arrindell, Sanderman, Hageman, Pickersgill, Kwee, et al. (1990); Arrindell, Sanderman, van der Molen, van der Ende, & Mersch (1988); Arrindell & van der Ende (1985); Arrindell, van der Ende, Sanderman, Oosterhof, Stewart, et al. (1999); Bouvard, Arrindell, Guérin, Bouchard, Rion, et al. (1999); Bridges, Sanderman, Breukers, Ranchor, & Arrindell (1991); Eskin (1993; 1992); Mersch, Breukers, & Emmelkamp (1992).
2 Abbeviations, acronyms, and symbols: dis. = distress; FQ = Fear Questionnaire (social phobia subscale); FSS = Fear Survey Schedule (social fear items); ns = non-significant; per. = performance; PSS = Perceived Social Support (Fa = from family; Fr = from friends); RAS = Rathus Assertiveness Scale; SCL-90 = Symptom Checklist (social inadequacy subscale); s-EPQ-R = short-scale Eysenck Personality Questionnaire-Revised (e = extraversion scale; n = neuroticism scale; p = psychoticism scale); SPS = Suicide Probability Scale; SSEI = Social Self-Esteem Inventory; STAI = State-Trait Anxiety Inventory (s = state; t = trait); (*) = p <.05; (**) = p <.01; (***) = p <.001; (****) = p <.0001.
Altogether, the accuracy of this instrument is rather impressive. However, it is not quite certain what it ultimately measures as its validity rests on moderate correlations with other instruments. The relationship of the SIB with the social behavior of the socially phobic in their own lives remains for the time-being unexplored.
The Social Performance Survey Schedule
The Social Performance Survey Schedule (SPSS; Lowe & Cautela, 1978) is a 100-item self-report questionnaire of “social performance” listing social behaviors rated on a 4-point scale of categories of frequency ranging from 0 = “never” to 4 = “very much”. The social behaviors were generated from lists supplied by undergraduate students with some additions by the investigators.
Fifty items describe positive and an additional fifty describe negative behaviors. The scale rests on the assumption that “the more often positive social behaviors are emitted, and the less often negative social behaviors are emitted, the better one’s social performance” (pp. 537-538). The raw score is a straightforward summation of ratings on positive items, and negative ones for which the ratings are inversed, e.g., “never” = 4 and “very much” = 0 to reflect their negative valuation in a positive way. The adjusted scores are meant to be the absolute difference between a normative rating on each item, minus an actual score.
To create the norms, 12 students were asked to rate the scale in an “ideal way.” Table 8.2 summarizes the evidence regarding the soundness of the test.
Table 8.2
Psychometric characteristics of the Social Performance Survey Schedule1,2
| Reliability | Validity | |||
| Test-Retest | Internal Consistency | Predictive | Convergent | Discriminant |
| Unadjusted scores: r = 0.87 r (SPSS-P) = 0.88 r (SPSS-N) = 0.85 | Unadjusted scores: α = 0.94 | Unadjusted scores: r (SPSS/SADS) = -0.42 (***) | Unadjusted scores: F > M | |
| Adjusted scores: r = 0.86 r (SPSS-P) = 0.76 r (SPSS-N) = 0.87 | Adjusted scores: α = 0.88 | Adjusted scores: r (SPSS/SADS) = -0.38 (***) | Adjusted scores: F > M | |
| r (SPSS-P/SPRS) = 0.29 (ns) r (SPSS-N/SPRS) = 0.35 (*) | r (SPSS-P/KAS-R1) = -0.12 (ns) r (SPSS-P/KAS-R1-P) = 0.52 (*) r (SPSS-P/KAS-R1-N) = -0.19 (ns) r (SPSS-N/KAS-R1) = -0.73 (**) r (SPSS-N/KAS-R1-P) = 0.38 (**) r (SPSS-N/KAS-R1-N) = -0.74 (**) | TBI < N (SPSS, SPSS-P) TBI = N (SPSS-N) TBI < N (SPSS-P, SPSS-N) | ||

Note: There are no p values given for test-retest correlations.
1 Based on the following studies: Long, McDonald, Tate, Togher, & Bornhofen (2008); Lowe & Cautela (1978).
2 Abbeviations, acronyms, and symbols: F = Females; KAS_R1 = Katz Adjustment Scale (P = positive scale; N = negative scale); M = Males; N = Normal control subjects; ns = non-significant; SPRS = Sydney Psychosocial Reintegration Scale; SPSS = Social Performance Survey Schedule (P = positive social behaviors; N = negative social behaviors); TBI = Traumatic Brain Injury Patients; (*) = p <.05; (**) = p <.01; (***) = p <.001.
In summary, although the test shows reasonable accuracy, evidence that it measures the actual social behavior that we are interested in is rather weak.
Overall then, although on the face of it self-report measures show satisfactory accuracy, it ultimately remains unclear to what extent what is being reported actually corresponds to the subject’s actions in real life. Furthermore, although in principle social performance is usually regarded as considerably influenced by context, the measures do in fact treat social performance as a trait.
Role-play tests
The construction of most role-play tests is guided by the interpersonal view of social skills, namely as being situation-specific and rather individual. As such, most role-play tests were ad-hoc creations. Most however departed from a straightforward behavioral focus on active conduct in combining role-play with a rating of subjective anxiety experienced during the simulations. This theoretical hybrid goes usually by the name of the “Behavioral Assessment Test” (BAT). A major complication in role-play tests is how to analyze and make sense of the performance they elicit from the participants. To resolve this dilemma, there is no help but seeking guidance from theory. This brings us back to the definition of “social skills”. In this respect, the definitions are of high practical importance, not simply a matter of logical tidiness. In practice, two approaches have been taken.
The first—the “molecular”—focuses on various verbal (i.e. speech content), and para-linguistic dimensions (e.g., intonation, length of speech, pauses), as well as non-verbal (e.g., gaze, posture, hand-movement) elements of social performance. These are sought across behaviors. Such elements were in all likelihood chosen because they have an intuitive appeal (as seeming like building blocks) and easy to “make sense” of, in the absence of theoretical grounding to this practice.
The second—the “molar”—focuses on global behaviors in key domains (e.g., assertion, courtship), deemed to be essential to social performance. These are typically rated (on Likert-type scales) by assessors on the strength of their intuitive judgment of what constitutes a skillful performance of a specific activity. Although it is reassuring to know that there seems to be evidence of good reliability in such practice, its validity remains uncertain for “it is not clear precisely what these ratings actually reflect” (Bellack, 1979, p. 168).
These two levels of assessment are not mutually exclusive and have been combined in some studies. As such, they create a degree of confusion as the results cannot be compared. For the sake of analysis, we have chosen the most psychometrically elaborate and sophisticated role-play test, the Simulated Social Interaction Test.
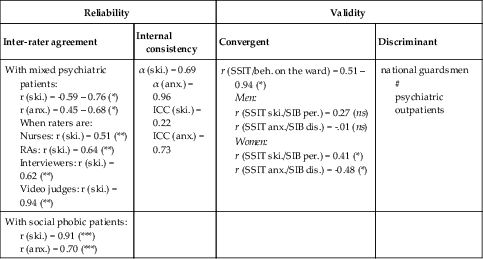
The Simulated Social Interaction Test
The Simulated Social Interaction Test (SSIT; Curran, 1982) provides descriptions of eight short situations described by a narrator. A confederate is present and gives the prompt to which the subject is meant to respond. All the proceedings are video-recorded.
The situations include criticism, being the focus of attention, anger, meeting someone of the opposite sex, expression of warmth, conflict with a close relative, interpersonal loss, and receiving compliments. These themes were drawn from factor-analytic investigations identifying the most common difficulties (e.g., Richardson & Tasto, 1976; Goldsmith & McFall, 1975). At the end of each description, the subject is prompted to respond. Although the role-plays are intended to be short, no specific duration is suggested.
The simulated performance is rated on two dimensions with an 11-point Likert-type scale ranging from “not at all skillful” (1) to “extremely skillful” (11) for performance; and ranging from “extremely anxious” (1) to “not at all anxious” (11) for anxiety.
Two key features of the test may give rise to some concern even at this point.
Firstly, it adopted a global (a molar) approach to the rating of social skills because the authors “… have not yet empirically determined the components of social skills for our criterion situation” (Curran, 1982, p. 363). It is a matter of concern that such an important choice was determined by nothing better than the lack of a better option.
Secondly, aspects of the training of the judges of social skill raise questions. Initially, six senior clinicians had reached agreements on ratings of bogus patients’ performance. Subsequently, these ratings became the criterion ratings (i.e. the proper normative response that the assessors must rate). Thus, the process of training consisted in “recalibration” of the assessors’ judgments (correlation coefficients had to be at least r = 0.80) to conform to those which the senior clinicians agreed upon.
Although this procedure forces agreement (i.e. enhances reliability) among assessors, it may paradoxically, through pressure to conform, undermine the validity of what constitutes skillful behavior. Table 8.3 below summarizes the evidence regarding the soundness of the test.
Table 8.3
Psychometric characteristics of the Simulated Social Interaction Test (SSIT)1,2
| Reliability | Validity | ||
| Inter-rater agreement | Internal consistency | Convergent | Discriminant |
| With mixed psychiatric patients: r (ski.) = -0.59 – 0.76 (*) r (anx.) = 0.45 – 0.68 (*) When raters are: Nurses: r (ski.) = 0.51 (**) RAs: r (ski.) = 0.64 (**) Interviewers: r (ski.) = 0.62 (**) Video judges: r (ski.) = 0.94 (**) | α (ski.) = 0.69 α (anx.) = 0.96 ICC (ski.) = 0.22 ICC (anx.) = 0.73 |
r (SSIT/beh. on the ward) = 0.51 – 0.94 (*) Men: r (SSIT ski./SIB per.) = 0.27 (ns) r (SSIT anx./SIB dis.) = -.01 (ns) Women: r (SSIT ski./SIB per.) = 0.41 (*) r (SSIT anx./SIB dis.) = -0.48 (*) | national guardsmen # psychiatric outpatients |
| With social phobic patients: r (ski.) = 0.91 (***) r (anx.) = 0.70 (***) | |||
1 Based on the following studies: Curran (1982); Curran, Wessberg, Farrel, Monti, Corriveau, et al. (1982); Curran, Wessberg, Monti, Corriveau, & Coyne (1980); Mersch, Breukers, & Emmelkamp (1992).
2 Abbeviations, acronyms, and symbols: anx. = anxiety; beh. = behaviours; dis. = distress; ICC = inter-class correlations; ns = non-significant; per. = performance; RAs = Research Assistants; SIB = Scale for Interpersonal Behavior; ski. = skills; (*) = p <.05; (**) = p <.01; (***) = p <.001.
In summary, the strengths of this test reside in it having a representative selection of difficult situations, and a high rate of inter- and intra-assessors’ reliability. This assessment method differentiated psychiatric patients from normal control participants.
Its weaknesses consist in modest agreement (convergent validity) with independent ratings performed in other settings and with non-trained observers (nurses, research assistants) or even with those of the participants themselves. Surprisingly, despite the setting of a high threshold by the experimenters, assessors’ agreements varied.
Perhaps the greatest shortcoming of this test however, is the absence of any support for its external (ecological) validity. Namely, that it provides information that may be considered as equivalent to observing what people do in actual life. Being on the ward can hardly be considered a representative sample of routine social life. The author of the test concedes: “… we are still not content with the information yield from such ratings” (Curran, 1982, p. 371).
Overall then, this one method for measuring social skills has, accuracy aside, few confidence-inspiring psychometric characteristics.
Is the use of role-play tests as behavioral measures of social skills warranted?
Our critique draws on thorough discussions by McNamara and Blumer (1982) and Bellack (1979). Role-play tests are typically used as substitutes for the observation of real social conduct in its natural setting. “Role-play assessment is based on the assumption that actions displayed in the role-play reflect behavior of that person in a corresponding non-role-play setting” (McNamara & Blumer, 1982, p. 520).
This cardinal postulate is backed by little research in general and none with regard to social phobia. The paradigms in use for validation studies either compare role-plays to non-role-plays (usually observation of behavior during a waiting period before engaging in role-play) or having the role-play assessed by a significant person of the participant’s as to its representativeness. Although appealing as economical substitutes for observation, each alternative is inadequate in some respect as neither is a proper reflection of behavior in real-life settings.
Nevertheless, role-play tests are typically used for the following ends:
1. to estimate treatment effects: differentiating the patients’ post-treatment state from that at pre-treatment;
2. to tell contrast-groups apart: distinguishing groups identified beforehand as socially skilled and non-skilled or of different degrees of skill (e.g., discrete vs. generalized social phobia, social phobia with and without an additional avoidant personality disorder).
Overall, some studies that have used role-play tests (or behavioral assessment tests) with socially phobic individuals, indeed reported the above- mentioned distinctions. However, the differences highlighted were usually in terms of severity of subjective anxiety ratings rather than in conduct. Behavior moreover was not always assessed. Such use of the role-play as a seemingly superior anxiety test is paradoxical as the impetus behind the use of role-plays is the possibility of observing behavior.
Although good reliability has been reported by Curran (1982) for the SSIT, it is not—as we have seen earlier—synonymous with validity. Construct validity is at this point not demonstrated while there is little interest in what is perhaps the most important test of validity—a predictor of real-life behavior. This shortcoming calls into question the very foundation of the use of role-play tests.
After searching reviews, both Bellack (1979, p. 167) and McNamara and Blumer (1982, p. 545) had suggested suspending the use of role-plays until better demonstrations of validity emerge. “Firm conclusions regarding role-play’s ultimate ecological validity must be therefore postponed until further research delimits how useful role-playing is at representing real world behavior” (ibid.). These recommendations are probably as pertinent today.
Finally, a framework for analyzing the performance displayed in role-play tests is sorely lacking. This is the upshot of the fact that no theoretical or operational definition of social skills is available. In practice, the analysis of performance is conducted in ways that generally preclude comparisons and paradoxically diminish the likelihood of outlining elements of convergent validity.
In sum, if we were very strict and narrowly purposeful, our survey might have come to a halt here. Lacking a clear theoretical vision of what social skills (and conversely their absence or deficiency) are, as well as meaningful means to identify and quantify them, we could have dismissed our quest out of hand and put an end to our inquiry at this stage. However, as our purpose is the exploration itself, we shall carry on regardless and attempt to answer several questions while temporarily ignoring the earlier-mentioned drawbacks.
Skills deficits and social phobia—direct and indirect evidence
Are highly shy/socially anxious individuals less skilled than those who are not?
Although not concerning social phobia as identified in diagnostic manuals, but rather shyness—a wider but related construct—the pioneering studies of Twentyman and McFall (1975) and Pilkonis (1977), may nonetheless be useful in shedding some light on it. It is likely that some of the participants in these studies would fulfill the criteria for social phobia current today.
In Twentyman and McFall (1975), (31) shy (operationally defined as having had less than one date a month) male students were compared to nine confident ones. Participants’ behavior was measured in several ways:
1. weekly diaries of all their interactions with women;
2. role-play simulating a phone call proposing a date;
3. role-play of social interactions involving three-minute conversations with an unseen confederate (hidden behind a one-way mirror), and a four- to five-minute role-play “asking out a classmate” face to face. These were recorded and analyzed.
The shy subjects reported greater levels of subjective anxiety in the simulation of a phone call and face to face but not in the other situations. Nor were there differences in pulse rates during and in between the role-plays. The shy subjects, however, took less time to complete the role-play.
Independent raters found the shy subjects globally less skillful and more anxious in two out of three role-plays (ratings on a 5-point Likert-type scale).
Most importantly, shy subjects—as gathered from their diaries—had fewer interactions with women in fewer situations and these were of shorter duration. In other words, shy individuals behaved differently in the domain most important to their lives. Whether this is due to lack of skill or the result of purposeful behavior (e.g., active avoidance), or some other reason cannot be ascertained from the study.
In Pilkonis (1977), (22) shy students (selected on the basis of scores on the Stanford Shyness Survey) were compared to 24 non-shy subjects on a number of social activities involving interacting with an individual of the opposite sex and giving a speech. Although the tasks were performed in the laboratory, these were not strictly speaking role-plays, as the subjects were mislead about the goals of the study.
The shy sat further away from the experimenter and were less able to initiate and structure conversations as well as taking longer before starting the conversation. During the exchange, they talked less and paused more. Shy individuals performed less well in an unstructured situation, (e.g., conversation) as opposed to a well defined one (e.g., making a speech), and tended to smile and nod more as well as engaged in “self-manipulation”. There were no differences between the groups either in terms of the duration or the quality of speech. The author interpreted this to suggest that “a willingness to employ social skills may be at issue here, rather than a complete deficit of such skills” (p. 602).
Some differences between the sexes were found. Shy men had more difficulties than anyone did, whereas non-shy men did best. According to the author, men and women are anxious in different ways. This study, in addition to highlighting behavioral differences (a discriminant function allowed the correct reclassification of 91% of the shy subjects), strongly brought out the interaction between behavior and situation.
Following Twentyman and McFall (1975), Wessberg, Mariotto, Conger, Farrel, and Conger (1979) adopted “low-frequency dating” as an operational definition of social anxiousness. In this study of male students, nine low-frequency daters were compared to 19 medium- and 17 high-frequency daters on two role-plays, each involving getting acquainted, punctuated by a waiting period.
Subjects who dated frequently were rated as less anxious than those who dated least (but not the intermediate group). Furthermore, there were differences between them in terms of ratings of skills (e.g., compliments, smiling). Subjects in all groups however, exhibited greater skill in the role-plays than in the naturalistic waiting period during which the subjects were unaware of being filmed. It is noteworthy that all subjects recognized this period as resembling most the way they were naturally.
In an additional study, Dow, Biglan, and Glaser (1985) compared 25 socially anxious women (scoring above 15 on Social Avoidance and Distress (SAD), Watson & Friend, 1969) to eight non-anxious ones (scoring less than 8) on role-plays of “getting acquainted” with strangers of the same and the opposite sex. Additional role-plays to taped descriptions of situations and prompts were performed as well.
Highly anxious subjects were rated as having less social skills by peers, confederates and observers. However, as in Pilkonis (1977), only one significant difference on specific behavioral variables was found: anxious women spoke less. This reoccurred in the recorded situations’ test, in which anxious women differed only in giving fewer compliments and making fewer “positive statements”.
In the self-monitoring of their own real-life social behavior, socially anxious women observed themselves as speaking to fewer people. When speaking to someone they tended to give fewer compliments, to share less personal experiences and to agree more. The authors interpreted these differences as evidence of “skill deficits in specific conversational skills” (p. 280). However that may be, the study illustrates the fact that socially anxious women engage in real-life social situations differently even if their performance in forced and imaginary circumstances cannot be easily distinguished from that of non- anxious individuals. These recall the results reported by Wessberg, et al. (1979) described earlier. Because of the relatively small original sample size, made worse by seemingly catastrophic losses of data, these results must be viewed as tentative.
In a study inquiring into verbal communication skills (Lewin, McNeil, & Lipson, 1996), student subjects were divided into three groups according to their ratings of subjective anxiety: “circumscribed speech fear” (n = 8), “generalized social anxiety” (n = 8) and “low anxiety” individuals (n = 16), and compared. It is not clear whether the anxious subjects may be considered socially phobic.
All participants role-played a five-minute speech and filled out the State-Trait Anxiety Inventory-state form (STAI-S; Spielberger, 1970) before and after it. The verbal data were analyzed in four categories of speech dysfluency.
There were differences between the groups in terms of the number of subjects who finished their speech before the allotted five minutes. This was considered as escaping/avoiding the situation; escape behavior was highest in the speech fear group and lowest in the low anxiety group. This was not true however in terms of the number of words spoken: differences were detectable only between speech fear and low anxiety groups.
On the many variables quantifying the various speech dysfluencies, both anxious groups tended to differ from the less anxious one. Whether these features reflect skill or are features of a state of anxiety is difficult to say. However, there were no correlations between any verbal measures and the STAI-S score. If we do consider the measures as aspects of skill, their abstract nature does not allow us to reconstruct any meaningful behaviors that they could be related to.
In an attempt to approach the question more naturalistically, Segrin and Kinney (1995) divided 64 undergraduate students into the socially anxious (SA, n = 31) and the non socially-anxious (NSA, n = 33) by means of a cut-off point on the Social Reticence Scale (Jones & Briggs, 1986). All participants unwittingly took part in a five-minute unstructured interaction with a confederate while “waiting for the experiment to start”.
Subjects in the SA group were considered by the confederates (who were unaware of group membership) as having poorer social skills than those of the NSA group. In contrast, independent observers who rated recordings of the same interactions, considered the groups equivalent in their social skills. Similar results emerged in an analysis of the verbal content of subjects’ responses. Overall, SA subjects—with one exception—were mostly like the NSA subjects.
In Strahan and Conger (1998), (333) undergraduate male students completed the Social Phobia Scale of the Social Phobia and Anxiety Inventory (Turner, Beidel, Dancu, & Stanley, 1989); the highest and lowest third of subjects in the distribution of social anxiety scores were selected (high SA, n = 27, and low SA, n = 26). Subsequently, all participants underwent a simulated interview conducted by a female confederate; judges rated the recorded interviews.
Overall, no differences between the two groups were found on either performance or verbal content.
In a study comparing a naturalistic and a contrived social exchange, Thompson and Rapee (2002) administered the Fear of Negative Evaluation (FNE; Watson & Friend, 1969) to 245 female students and selected the highest and the lowest 28 from the distribution. Fifty were accepted to participate and were divided into low SA (n = 24) and high SA (n = 26).
All participants took part in an unstructured (waiting in the company of a confederate for the experiment to begin) and structured (simulation of getting to know someone at a party) phase.
In contrast to the two earlier studies, observers rated the SA participants as less skilled during the waiting period; the differences were less pronounced during the simulated conversation.
Wenzel, Graff-Dolezal, Macho and Brendle (2005) investigated a narrowly defined population—romantically involved undergraduate couples. Those who scored one standard deviation above (SA, n = 13) and below (NSA, n = 14) the mean of the SAD and FNE (Watson & Friend, 1969) and had a “romantic partner” were included.
All couples discussed three topics (neutral, problematic and positive features of their relationship) and were rated on five types of communication skills. While no differences were found on three of the communication skills (e.g., asking questions, offering an opinion, paraphrasing the other’s point of view), members of the SA group had greater difficulties in expressing themselves clearly during the problem discussion while fidgeting more and speaking more softly during all tasks. Additionally, they displayed less eye contact, smiled and initiated less (during conversation) and gave fewer compliments.
To sum up, the available studies give a conflicting picture as to whether disparities in social skill may be said to distinguish groups of socially anxious individuals. However that may be, the relative and rather small differences between these subgroups when found, are not foremost from the point of view of our inquiry, as these may be indicative of differences of degree. A plodding musician at home is but a pale reflection of the virtuoso concert pianist, yet both play the piano. It is the absolute level of social performance that is of most interest to us. Unfortunately, we have neither valid means nor norms of social skill that would allow us to determine the standing of the socially phobic as a group on that dimension.
The Twentyman and McFall (1975) and Wenzel, et al. (2005) studies then, although not of socially phobic individuals in a formal sense, do suggest that the socially anxious individuals behave differently at least as far as courtship of the opposite sex and communication among romantic partners is concerned. Whether this reflects deficits in skills is impossible to say.
Are the socially phobic different from normal individuals in their skills?
Only a small number of studies allow us to pursue this question directly. The fact that they have used various definitions of social skill complicates matters even further.
Rapee and Lim (1992) compared 28 socially phobic (13 generalized, 15 specific) to 31 control participants. The role-play test that all subjects underwent consisted of a brief speech given in front of a small audience. The performance was analyzed in terms of two broad categories: specific elements of behavior (e.g., eye contact, clarity of voice) and global aspects (e.g., subject’s ability to arouse interest), and rated on 5-point Likert-type scales by observers and the subjects themselves.
Significant differences were found on comparisons of the amalgamated scores of both specific and global aspects of performance. Most importantly, no differences in terms of specific behaviors were reported. For this reason, although statistically significant, the meaning of the association between lesser skill and social phobia remains obscure. Typically, subjects’ self-ratings of performance tended to be lower than that of observers, especially for the socially phobic.
In Alden and Wallace (1995), (32) (generalized) socially phobic participants were contrasted to 32 control community residents who simulated “getting acquainted” for five minutes. Half the subjects from both groups were assigned to a “positive” condition (e.g., the confederate was friendly and encouraging) and half to a “negative” (e.g., the confederate was cool and allowed silent pauses).
Meaningfully, both groups performed better with an encouraging rather than with a distant confederate. The socially phobic were more visibly anxious (non-verbal indices), spoke less, were found to convey less warmth, and to be less likeable than the control participants. Theoretically, the meaning of these statistical differences is not entirely clear. Although the authors did conclude that “ … the social phobic patients in both conditions were less skillful than control subjects …,” what this statement relates to is ambiguous, as we ignore what constituent elements of skill were rated or how any of this relates to the subjects’ conduct in real-life.
In Hofmann, Gerlach, Wender, and Roth (1997), 24 socially phobic and 25 normal participants were compared. The tasks (i.e. role-plays) included were: speaking with the interviewer, telling the interviewer what they did the day before, preparing a talk with the interviewer, sitting in front of two people (three minutes each), and a simulation of giving a speech prepared earlier (10 minutes).
The participants’ performance in all five situations was analyzed in terms of gaze while the first two minutes of the speech were also rated for speech disturbances (defined as silent pauses, errors and dysfluencies).
No differences between the experimental groups were found in terms of gaze across situations, however calculated. As to speech disturbances, the socially phobic displayed mostly less fluidity than the controls, regardless of subgroup (the only difference was that the generalized subgroup had a longer overall time of pauses).
These results, although suggesting that the socially phobic experience difficulties in conversation, do not allow the drawing of general conclusions as to the state of their communication skills. Curiously, although differences in subjective anxiety ratings between subgroups were highlighted on some scales, these failed to show on the STAI-S (Spielberger, 1970). This would suggest that while the subgroups are located on different points of a continuum of severity—it is not necessarily one of anxiousness.
In a study testing hypotheses issued from Trower and Gilbert’s (1989) model of social anxiety, Walters and Hope (1998) compared 22 socially phobic to 21 non-anxious control participants in terms of a simulated impromptu speech, and conversations with same and opposite sex confederates (not for all subjects). The recorded role-plays were rated for behaviors assumed to reflect cooperation, dominance, submissiveness, and escape/avoidance.
Overall, the socially phobic faced their interlocutors less, expressed less praise (construed as cooperation), and engaged in less bragging and commanding (construed as dominance). It is noteworthy that in other respects (i.e. in terms of other descriptors of the constructs), no differences were observed. Unexpectedly and counterintuitively, the socially phobic were neither found more submissive nor more avoidant than the nonanxious control participants.
This study is important in showing that the socially phobic behave somewhat differently from controls in simulated social interactions. Whether and to what extent these behaviors are indicators of the studied theoretical constructs remains an open question. How these constructs reflect adequate social behavior and what this might possibly be (optimally equidistant between dominant vs. submissive and cooperative vs. avoidant?) remains to be justified.
Fydrich, Chambless, Perry, Buergener, and Beazley (1998) asked 34 socially phobic, 28 normal, and 14 individuals meeting criteria of various other anxiety disorders, to simulate initiating and maintaining a conversation with a confederate of the opposite sex. Overall, observers rated the quality of the performance of the socially phobic group as poorer than that of the normal and the other anxiety disorders groups.
In Norton and Hope (2001), (54) socially phobic, 28 normal, and 23 dysthymic individuals simulated: (1) giving a brief speech, (2) engaging in a conversation (unstructured), (3) engaging in conversation with a neighbor who just moved in (structured). Observers rated the performance of the socially phobic as poorer than that of the dysthymic and the normal participants, either on single tasks or all three pooled together.
In Baker and Edelmann (2002), (18) (generalized) socially phobic were compared to 18 normal, and 18 individuals characterized by other anxiety disorders, in terms of a simulated interaction with a person they were meeting for the first time.
Independent observers found the performance of the socially phobic less adequate than that of the normal group; the differences in comparison with the other abnormal (anxiety disorders) group were, although still significant, less pronounced.
Despite statistically significant differences between the groups on average, the authors emphasized the considerable overlap between them. For example, two socially phobic individuals were rated as adequate as the most adequate normal subjects. At the other end of the spectrum, one normal participant was considered as barely more adequate than the least adequate of the socially phobic.
In Stangier, Heidenreich, and Schermelleh-Engel (2006), 20 (generalized) socially phobic, 17 normal and 14 participants with other anxiety disorders simulated giving a short speech and engaging in conversation with a confederate.
Observers rated the socially phobic group as displaying greater “nervousness” (e.g., less eye contact) and less friendliness than subjects of the two control groups who did not differ.
In Voncken and Bogels (2008), (48) (generalized) socially phobic and 27 normal individuals simulated giving a short speech and engaged in conversation with two confederates.
In contrast to previous studies, confederate ratings showed no statistically significant difference (at p <.05) between the groups in either speech-making or the adequacy of engaging in conversation.
Beidel, Rao, Scharfstein, Wong, Alfano, et al., (2010) compared 119 generalized to 60 non-generalized and to 200 normal participants in terms of role-plays of several interactions. The first block of simulations was provided by the SSIT reviewed earlier (in the assessment section). The second included two unstructured conversations. The third was an impromptu speech of 10-minute duration. Social anxiety and skill were rated by independent observers.
On the SSIT, normal participants did best (they were most skillful and least anxious) followed by the non-generalized socially phobic. The generalized socially phobic were least skillful and more anxious than the other groups. In terms of clinical significance, this was detectable only between the generalized socially phobic and the other two groups (who did not differ). These results were mostly replicated in the unstructured conversations. In the improvised speech task, the normal participants were found significantly more skilled than the socially phobic groups.
Altogether, the statistical differences in skill detected by the experiments involve differences in degree rather than in kind. It is doubtful whether these may be characterized as deficits.
In Levitan, Falcone, Placido, Krieger, Pinheiro, et al., (2012) 18 socially phobic and 18 normal participants were compared in terms of a three-minute speech-giving. Five elements of social skills as well as the overall performance were rated.
Two of the five elements (voice intonation, fluency of speech) and overall performance of the socially phobic were rated by independent observers as less adequate. No significant differences were noted on the other dimensions (visual contact, gestures, facial expression). Nor were there differences between the two groups in terms of self-rated overall performance. While some differences in degree have been found, these do not amount to differences in kind or in skill.
In summary, the studies available do not allow us to answer the question we have asked. Firstly, on a global level of “performance”, results are contradictory. Secondly, on the level of specific skills, where differences have been identified, no convergence in deficits is in evidence. In most studies, social skill remains undefined and role-play performance, as its measure, is analyzed in ways that do not allow the integration of the fragmented bits into a meaningful whole (i.e. as a means to an end).
Are any socially phobic sub-groups deficient in their social skills?
To our knowledge there were no studies that have attempted to put this question to a test directly; we shall therefore have to seek answers indirectly, through byways as it were.
A number of studies lend themselves to such purpose in that they have used role-plays as “behavioral assessments” (i.e. a measure of social skills or social anxiety, within a battery of other tests), with the original purpose being that of investigating social phobia itself (e.g., in comparison to avoidant personality disorder) or its putative subtypes (specific, generalized) as distinct entities. In what follows we shall proceed to review these studies.
In Turner, Beidel and Townsley (1992), 88 socially phobic participants were divided into specific (n = 27) and generalized subgroups (n = 61). All subjects role-played: (1) a 10-minute speech that had to last “at least three minutes” rated in terms of subjective anxiety; (2) a conversation with a first date; and (3) a conversation with a new neighbor of the same sex. These were rated for a number of molecular components of behavior, (e.g., gaze, voice tone, number of verbal initiations, length of speech) and overall impression of skill.
No differences between experimental groups were found on any dimension. No differences were observed between the two subsets also following a subsequent analysis of the subjects within the generalized group that met or did not meet criteria for avoidant personality disorder.
In a similar study, Herbert, Hope, and Bellack (1992) compared two subsets of 23 “generalized” socially phobic participants of which 14 also met criteria for avoidant personality disorder.
The subjects underwent a role-play consisting of three situations: making an impromptu speech of three minutes, initiating a conversation and maintaining it. The subjects rated their subjective anxiety and the performance was analyzed in terms of overall skill, paralinguistic behavior, speech content, and non-verbal behavior.
As in the earlier study, no differences in behavior were found between the two experimental groups although participants with avoidant personality disorder were more anxious before simulating the speech (but not afterwards).
These results were further reanalyzed, in light of a more stringent definition of the generalized subtype of social phobia proposed by Heimberg and Holt (1989). After reclassification, it was found that this more severe group of (generalized) socially phobic participants were rated as significantly less skilled on an overall composite score than their reclassified counterparts; no specific differences however, in either behavior or thought processes were observed.
A study in similar vein was conducted by Tran and Chambless (1995) who had 16 specific, 13 generalized, and 16 generalized socially phobic participants also meeting criteria for avoidant personality disorder participate in three four-minute role-plays: impromptu speech, conversation with individuals of the same and the opposite sex.
Assessors behind a one-way mirror rated performance for general impression of social skill. Simultaneously, the subjects rated their impression of their own skill as well as the subjective anxiety they have experienced.
The specifically socially phobic were rated as giving a better impression of skill than did the generalized participants also meeting criteria for avoidant personality disorder. These results were obtained consistently with both self-ratings and observer ratings across role-plays.
In summary, from the comparisons of several subcategories of social phobia, there is little evidence to suggest that despite apparent differences in severity, these might differ in degree or quality of social skills—however measured.
Are better skills acquired through social skills training?
An indirect way of inquiring into the validity of the concept of social skills in social phobia would be to see whether it improves following a course of therapy designed to remedy it, namely social skills training.
Uncontrolled studies
Chambless, Tran and Glass (1997) describe a trial of cognitive behavior therapy with the sample described earlier in Tran and Chambless (1995). The outcomes measured by various behavioral assessment tests were as follows: self-ratings showed significant improvements across role-plays and remained at that level at the six-month follow-up. Observer ratings of social skills showed an improvement after treatment but this was not maintained at follow-up. Ostensibly, this study suggests that inadequate social skills may be changed in the course of therapy and perhaps maintained over time—the results are conflicting on this. As we were unable to answer the question of whether the socially phobic are deficient in their skills in an absolute sense, it is difficult to gauge the meaning of the changes documented in Chambless, et al. (1997).
In Turner, Beidel, Cooley, Woody, and Messer (1994), 13 socially phobic patients underwent 29 sessions (a total of 54 hours) of “social effectiveness therapy”. Among other tests, patients took part in role-plays which required making a speech of 10 minutes and having a conversation with confederates of the same and the opposite sex. There was a significant improvement in “overall effectiveness” (as measured by the conversation role-play) after treatment which involved a spell of social skills training (eight sessions of two hours each) in addition to variants of exposure and practice in between sessions. Whether this improvement in performance implies an improvement in component social skills is not clearly established.
In van Dam-Baggen and Kraaimaat (2000a), (56) socially phobic participants were divided into two equal groups as “reticent” and “non-reticent” on the basis of their scores on the Inventory of Interpersonal Situations (van Dam-Baggen & Kraaimaat, 1999) and treated by a varying number of sessions of social skills training determined by demand.
In both sets of patients, a significant and equivalent improvement in the frequency of social activities was reported. Whether the increased activity resulted from the deployment of better skills cannot be determined.
Herbert, Rheingold, and Goldstein (2002) treated 21 socially phobic patients by six sessions of cognitive behavior therapy combined with social skills training. Social skills were measured by means of three simulated activities: interactions with one and two strangers and an impromptu speech. An improvement in the performance observed during the role-plays after treatment was observed.
In summary, social skills training has been shown to result in improvement in performance in role-plays and increase in social activities of socially phobic patients. Whether this occurred as a consequence of improved social skills remains uncertain. Moreover, it is unclear whether the improvement is specific to social skills training. Perhaps a more definitive answer to this question may be provided by controlled studies of social skills training.
Controlled studies
In Wlazlo, et al. (1990), 167 patients (corresponding to generalized social phobia/avoidant personality disorder in DSM-III terms) were treated by either group social skills training or exposure in vivo—administered individually or in a group. Social skills training was administered over 25 sessions of 1.5 hours each. Group exposure involved a total of 34 hours of treatment, whereas the individual format included 12 hours. One hundred and three patients completed treatment and 78 were followed up for two and a half years on average. At the end of treatment, the three regimens brought about significant and equivalent improvement in terms of social anxiety and tendency to avoid. These gains maintained and slightly strengthened over the follow-up period.
For the sake of subsequent analysis, the sample was subdivided into two groups: those with primary “skills deficits” and those with primary “social anxiety.” Overall, those classified as “skill deficient” did less well in treatment. Matching type of problem with kind of treatment (i.e. social skills training for those identified as skill deficient) did not yield greater improvement. The internal validity of this study, however, is somewhat compromised by the fact that the exposure condition also included some training in social skills as well as in “social perception.”
Skills deficits were said to be measured in this study by a self-report scale (UF-questionnaire—in German). As the content of the measure seems to be a mixture of feelings (e.g., fear of failure and criticism, feeling of guilt) as well as abilities (e.g., making requests, refusing), it is doubtful that skill deficits however defined were actually assessed. Nonetheless, on the strength of improvements registered on this scale, patients in all treatment conditions (i.e. also in exposure) were said to have acquired social skills.
Subsequently, patients were divided into primarily “socially phobic” (anxious) or “skill deficient” based on case records by experienced clinicians. It is not clear what the basis of this subdivision was as neither independent definition nor its anchoring points were provided. On the evidence of treatment outcome, one may surmise that the patients labeled “skill deficient” could be the most severely phobic.
In Mersch, Emmelkamp, Bogels, and Van der Sleen (1989) and Mersch, Emmelkamp, and Lips (1991), social skills training was compared to cognitive restructuring while also testing the value of matching treatment with patients’ patterns of fear. On the basis of extreme responses to a role-play and a “rationality” test, 39 patients were classified as either predominantly “behavioral” (unskilled but rational) or “cognitive” (irrational but skillful). Half of each category of patients was assigned to the behavioral treatment (social skills training) and half to the cognitive treatment. Both treatment conditions resulted in significant and equivalent improvement on all measures. There was no support however for the notion that a match between predominant feature and treatment results in greater therapeutic gains. Nor did a significant lessening of social anxiety in this study lead to increased social activity.
Social skills were measured in this study by the SSIT described earlier (Curran, 1982). Patients’ (classified as behavior reactors) skills improved following social skills training or a cognitive therapy (only on patients’ self-ratings).
In van Dam-Baggen and Kraaimaat (2000b), (48) socially phobic patients were assigned to 17 1.5-hour sessions on a weekly basis of either group social skills training or cognitive therapy. These were followed by three monthly sessions during a three-month follow-up.
Self-reports of frequency of social activities were considered as measurement of social skills. Social skills training did result in a statistically greater frequency of social activities than did cognitive therapy, both at the end of treatment as well as at a three-month follow-up. Whether this is due to newly improved skills remains unknown.
In Stravynski, Arbel, Bounader, Gaudette, Lachance, et al. (2000), 60 socially phobic patients were assigned to 14 sessions of an interpersonal approach to the treatment of social phobia with or without social skills training (conducted in groups). Both treatment conditions included the setting of interpersonal targets that constituted the content of treatment and had them assigned as homework to be performed in between sessions.
Social functioning in both groups improved significantly and equivalently after treatment, remaining stable at six- and 12-month follow-ups. Contrary to some of the previous results, social skills training in this study was not shown to result in or enhance distinct changes in social functioning.
In a related, as yet unpublished study (Stravynski, Arbel, Gaudette, & Lachance, 2013), 102 socially phobic patients were randomly assigned to 14 sessions of either an interpersonal approach aiming at improving participation in individually relevant social encounters and including social skills training, a discussion group or a brief individual supervision. All treatment conditions included interpersonal homework to be performed between sessions.
Seventy-six patients completed treatment. Patients in all treatment conditions improved significantly and equally in terms of reduced anxiety and avoidance, general psychopathology and better social functioning that was maintained over the six- and 12-month follow-ups. As in Stravynski, Arbel, Bounader, et al., (2000), social skills training had no unique or greater effect on social functioning.
Herbert, Gaudiano, Rheingold, Myers, Dalrymple, et al. (2005) assigned 65 socially phobic patients to 12 sessions of either cognitive behavior therapy alone or combined with social skills training (both conducted in groups).
Social skills were estimated by means of simulated interactions with one and two strangers, and an impromptu speech. The combined condition resulted in significantly better performance on all features of the three role-plays measured.
In summary, in Mersch, et al. (1989) and Herbert, et al. (2005), social skills training resulted in improved social skills as measured by role-plays. Paradoxically, in Mersch, et al., (1989, 1991) a predicted superior improvement following a matching treatment failed to materialize, thereby weakening both the notion of skills deficits as well as the treatment—social skills training—meant to make them good.
As to the other studies surveyed in this section that mostly used wider measures of social activity or social functioning, these did not show social skills training to result in unique improvements.
Is improvement in performance of social tasks related to skill-acquisition?
Stravynski, Marks, and Yule (1982) assigned 27 out-patients (generalized social phobia/avoidant personality disorder in DSM-IV terminology) to twelve 1.5-hour sessions of either social skills training alone or social skills training combined with cognitive restructuring. Twenty-two patients completed treatment. In each treatment condition patients improved significantly and equally on all measures of outcome. Lower subjective anxiety, increased social activities, and a corresponding improvement in social functioning with friends and at work were reported. Only treated behaviors improved, little meaningful generalization to other behaviors occurred. During an initial no-treatment phase, no improvement was observed. At six-month follow-up, improvement remained stable.
Although changes in social skills were not measured in this study, it did document performance during interpersonal encounters in real-life through self-monitoring by the participants. A subsequent re-analysis of this data (Stravynski, Grey, & Elie, 1987) revealed that treatment had a sequentially diminishing impact on trained behavior. In other words, the greatest improvement in terms of frequency of performance was found in the first targeted interpersonal behavior; it gradually diminished with the introduction of treatment to each newly targeted interpersonal behavior. The sequentially diminishing impact of treatment did not seem to be compatible with “… a skills-acquisition process that might be reasonably expected to take the form of gradual competence building and similarly gradual and steady improvement” (ibid., p. 228).
Discussion
Our inquiry into social phobia from the perspective of social skills deficits—although instructive—has been disappointing overall, not least because of the elusiveness of the master-concept and the inescapable attendant difficulties arising from practical attempts to measure it. Perhaps this is fitting, as the socially phobic interpersonal pattern of behavior itself is strongly characterized by reticence and evasiveness (in pursuit of safety); we may need more sophisticated (or less crude) notions to tease it out of its self-protective shell.
What appeared initially a potentially productive way of understanding social phobia (or some subtypes of it) and a guiding light for clinicians toward proper treatment, has proven insubstantial.
No evidence has emerged to link social phobia consistently with “deficits of social skills”, let alone to suggest that they may play a causal role in its genesis. Nor has social skills training—the method presumed to improve deficiencies in social skills—been shown consistently to result in such outcomes in social phobia. At most, its results have been comparable to other psychological approaches or their main ingredient (e.g., cognitive modification—see Mersch, et al., 1991), that did not attempt improving social skills. Furthermore, when change in social behavior following social skills training was measured (Stravynski, et al., 1987), improvement had not been found to follow a skills-acquisition pattern.
In sum, social skills and their putative deficiencies in social phobia seem to be metaphors, a manner of speaking of the ineffable—as if it were something else. However sad for those attached to it, the demise of an idea need not be a destructive event. Conversely, it may set the stage for the surveying of familiar territory from new or different vantage points.
Social phobia as a problem in social functioning
Although not much that is wrong with the social skills of the socially phobic has come to light, it is undeniable that something is very much the matter with the way these individuals live socially, be it in limited situations or generally. This we know at least indirectly, from the repercussions of this way of being. Perturbed social and personal lives and lower economic and social attainments are typical of the socially phobic (see Stravynski, 2007, pp. 114-115 for a summary). We do know very little however, about the particular socially phobic pattern of social functioning.
Most research on social phobia assumes such a pattern while attempting for example to explain what causes it. In keeping with the diagnostic manuals (DSM, ICD), we conceive social phobia in abstract terms, namely as a hypothetical entity characterized by additional hypothetical constructs such as anxiety, but not in terms of (observable) social activities. In this case (e.g., Clark & Wells, 1995), it is assumed that high levels of anxiety inhibit social activity and disorganize it, resulting in impaired social functioning.
The merit of the skills deficits hypothesis (as an outlook) was that it attempted to account for social phobia in its own terms, as a difficulty in social functioning. Its drawback, common to many other attempts, was to conceive of social phobia as an entity in need of etiological explanation.
Such a position however overlooks the fact that at present we are uncertain as to what extent social phobia is a distinct psychological pattern (see Stravynski, 2007, pp. 75-141 for a comprehensive grappling with the question). Rather more important, from our vantage point, is the question of whether there is an overall pattern of social behaviors characterizing social phobia and what this might be.
The social difficulties of the socially phobic are usually seen as a consequence of some pathological process underlying it (e.g., anxiety), while this in turn is a consequence of a breakdown on an intrapersonal (or sub-personal) level (e.g., neurotransmission, patterns of thought).
Such a construal of social phobia in analogy to a medical view separates the disease (that the individual carries within) from the resulting social impairment displayed in the environment (the “sickness”; Stravynski, 2007, p. 68). Whether a reified social phobia may be separated from its problematic social functioning must be considered doubtful. On an observed level (as opposed to a speculative one), social phobia is short-hand for an abnormal pattern of behavior, i.e. how individuals in that category act and live their lives.
Unfortunately, but not surprisingly in light of the above widely shared view, there are no published studies documenting socially phobic behavior in real-life situations nor delineating a socially phobic pattern of behavior in various spheres of life.
To answer these necessary questions a different kind of research is needed, attempting to delineate a way of life. As such it would be closer to ethnography, i.e. the socially phobic individuals as members of an exotic cult (Lillard, 1998), and ethology (Boice, 1982), i.e. socially phobic individuals as organisms struggling to adjust to (and transform) their environments. These, rather than laboratory experiments that seek to probe intrapersonal processes and structures, are more likely to tease out the purposeful nature of the overall socially phobic pattern.
To guide such research, an interpersonal theory of social phobia has been put forward in Stravynski (2013). In the briefest outline, this theory holds that:
“Social phobia can be distinctively described in interpersonal terms. The main interpersonal patterns making up social phobia are best seen as a host of tactics, organized as elements in a defensive strategy, having as aim self- protection from bruising interactions. To this end, risk-taking is minimized by keeping a safe distance from (dangerous) social events whenever possible; when necessary, social activities are engaged in fearful submission and passive dependence (refraining from any provocation as it were).
In aggregate, and abstracted from the specific transactions with a myriad of social dangers personified by individuals and settings, social phobia is a fearful and relatively powerless web of interpersonal patterns (constituted of various sub-patterns), protective against the threat of humiliation (either as public degradation or private personal rejection).
The overall socially phobic pattern has simultaneously an interpersonal and a fearful somatic locus. The interpersonal pattern is enacted, the fearful state that permeates it, is realized somatically. Anxiousness, the all purpose state of alarm, permeating the defensive socially phobic pattern and arising out of its interaction with menacing social situations, undergirds the self-protective tactics, while readying the individual to respond to further threats that may arise.”
A preliminary test of this theoretical outlook is reported in Amado, Kyparissis, and Stravynski (2013) in a study based on field observations of four socially phobic individuals, going about their daily lives. The observations in real life situations were cross validated with the participants themselves, diaries they kept as well as clinical notes and interviews with close significant others.
All socially phobic participants regardless of subtype were characterized by a distinct and overarching self-protective pattern of interpersonal behavior. This was not observed in shy and non-shy normal individuals serving as control subjects.
The socially phobic self-protective pattern was found to come apart gradually and finally vanish after successful therapy by means of the interpersonal approach described earlier (see also Stravynski, Arbel, Lachance, & Todorov, 2000 for a description of individual cases), lending support to the previous findings.
The treatment of social phobia as an antidote to its etiology, or social skills training for social skills deficits
If the poor social functioning of the socially phobic is construed as the consequence of a high level of debilitating anxiety, a reduction in anxiousness ought to result in an improved level of social functioning. Several lines of evidence suggest that it is not the case. For example, Beidel, et al., (2010) found that “… decreasing social anxiety alone does not always result in significantly improved social competence (p. 999). This is also true when reduced anxiety levels are achieved by means of pharmacotherapy (e.g., Scharfstein, Beidel, Rendon Finnell, Distler, & Carter (2011)). There is no helping them but to attend to social functioning in its own right.
What is the appropriate approach?
Regardless of its scientific merits, an “etiological” hypothesis such as that of “skills deficits” often provides a powerful rationale or even a rationalization for a certain approach to treatment. Thus, social skills training is seen as building whatever is lacking in the individual patient’s repertoire of social skills.
Such construction of treatment (of social phobia) as an antidote to its etiology follows an older idealized pattern set by the medical model (of say infectious disease). In keeping with it, psychotropic medication is seen as setting right the dysregulation of neurotransmitters presumed to give rise to the “disease”. In a similar vein, cognitive therapy is assumed to straighten the crooked thinking allegedly causing the anxious distress. It is interesting that the two notions—etiology and treatment—are frequently unveiled simultaneously although the relevant evidence for either is slight.
Against expectations, there are few convincing demonstrations that social skills training results in improved skills (e.g., Wlazlo, et al., 1990; Mersch, et al., 1991). Moreover, the outcomes of social skills training and two anxiety reduction methods it was compared with in the above studies were indistinguishable either in terms of anxiety reduction (to an equal degree) or social functioning (unchanged).
This is in contrast with the outcome reported in Stravynski, et al., (1982) in which social skills training resulted in less anxiety and improved social functioning.
What underlies the difference in outcome? Perhaps the better outcome (from the point of view of social functioning) in the latter approach was due to the fact that its content of treatment was not determined by the idea of building up generic hypothetical skills deemed necessary for social functioning, be they molecular (e.g., appropriate eye contact, timing, etc.) or not. Such an approach might be termed the structuralist perspective. Rather, in Stravynski, et al. (1982) (an approach that might be termed interpersonal or functionalistic), individual patients were trained to develop personal ways to facilitate participation in their real-life social/interpersonal encounters and put them to use in situations which would be very much a part of their daily lives. Assuming a social role, but also admitting to being clumsy, seeking people out and being opinionated and provocative are examples of behaviors targeted in such a treatment.
To reiterate, such an approach undermines defensively fearful and therefore self-protective patterns of interpersonal behavior, through the cultivation of more powerful and collaborative ways of interacting with others (see Stravynski, 2013, Chapters 7 & 8). The withering and ultimate dissolution of self-protective interpersonal patterns leads to a weakening of attendant anxiousness.
Apart from the issue of what is the proper content of training (as dictated by the structuralistic or functionalistic perspectives), a further question arises. Is the framework of social skills training at all necessary for a beneficial improvement in social functioning to occur? The answer to this query is of considerable theoretical and practical interest.
An early study involving patients meeting criteria for avoidant personality disorder (Stravynski, Lesage, Marcouiller, & Elie, 1989) queries the role of social skills training as an essential technique. In it, 28 subjects were assigned to two combined treatment conditions consisting each of five sessions of social skills training plus homework and five sessions of group discussion plus homework, administered in a different order in accordance with a Latin-square (crossover) design.
Equivalent and significant improvements in social functioning and social skills were observed in both treatment conditions (combining each, both treatment modalities, in reverse order). Most importantly from our point of view, no differences in outcome were found between the treatment modalities, i.e. social skills training and discussion during the sessions and homework in between them.
In Stravynski, Arbel, Bounader, et al. (2000), the same hypothesis was put to another test. In this study, two treatment regimens were compared. While both were aimed at the improvement of socially phobic patients’ social functioning, one included social skills training (modeling, role rehearsal, feedback) and the other did not. In both treatment conditions, the patients had pre-determined individual behaviors aiming at better participation in various social encounters. The behaviors targeted for treatment came in for attention in the clinic as well as being assigned as homework tasks to be practiced in between sessions.
The regimen without social skills training promoted improvement in social functioning by means of practicing the targeted behaviors during the session and their assignment as tasks to be performed in between sessions. In contrast to the condition using social skills training however, no attempts were made to improve upon how the patient enacted the targeted behavior spontaneously; nor were the staple ingredients of social skills training (modeling, role-rehearsal, etc.) used. This condition was designed to assume the form of social skills training but without its essence.
Both treatment conditions (30 patients completed treatment in each) resulted in highly significant reductions in the level of subjective anxiety and in improvements in social functioning in most areas of social life (e.g., work, friends).
Clinically however, the most meaningful result was that 60% of patients in each condition no longer met DSM-IV criteria for social phobia at the one-year follow-up.
These outstanding outcomes illustrate the promise of treating the difficulties of social functioning in their own right, unfettered by the intertwined notions of skills deficits, put right by social skills training.
A long-term follow-up was carried out (Gibbs, Stravynski, & Lachance, 2013) among available participants. Altogether, the rate of inclusion in the long-term follow-up (n = 36) was on average 55% of the patients available for assessment. Most participants were assessed between 11 and 15 years after the end of treatment.
Encouragingly, the remission rates continued to rise when compared to those observed at the one-year follow up. Fully 78% of the participants in the Stravynski, Arbel, Bounader, et al. (2000) study were in remission (on average) 12 years after the end of their treatment. These remission rates were a significant increase from the roughly 55-60% remission rates observed at the one-year follow up.
Similar (post-treatment, six-month, 12-month, and 10-year follow ups) results, obtained in a different trial may be found in Stravynski, et al. (2013) and in Gibbs, et al. (2013).
In conclusion, these results suggest that, rather than struggling with putative skills deficits, we ought to (guided by an interpersonal theoretical framework; see Stravynski, 2013) turn our attention to the problems of the socially phobic in social participation, fitting in and assuming social roles.