Chapter 26
A Comparison between Psychosocial and Pharmacological Treatments
Mark B. Powers
Brooke Y. Kauffman
Allison Diamond
Jasper A.J. Smits
Department of Psychology, University of Texas-Austin, Austin, TX
Abstract
In this chapter we summarize the differences between pharmacological and psychosocial treatments for social anxiety disorder (SAD). Using empirical evidence we first describe both psychosocial and pharmacological treatments used, their effectiveness, and their advantages and disadvantages. Though practitioners may utilize many treatments, we limit our discussion to those with empirical support. Then, using data from meta-analyses and individual trials, we compare both treatment modalities (alone and in combination). After discussing both treatment options, we turn to learning theory and translational research and present data on novel pharmacological and psychosocial treatments guided by this research. Finally, we describe how these findings may affect clinical practice.
Keywords
psychological
pharmacological
treatment
comparison
augmentation
In this chapter we summarize the differences between pharmacological and psychosocial treatments for social anxiety disorder (SAD). Using empirical evidence we will first describe both psychosocial and pharmacological treatments used, their effectiveness, and their advantages and disadvantages. Though practitioners may utilize many treatments, we limit our discussion to those with empirical support. Then, using data from meta-analyses and individual trials, we will compare both treatment modalities (alone and in combination). After discussing both treatment options, we will turn to learning theory and translational research and present data on novel pharmacological and psychosocial treatments guided by this research. Lastly, we will describe how these findings may affect clinical practice.
Psychosocial treatments
There are many evidence-based psychosocial treatments for SAD. The current psychosocial treatment of choice is cognitive behavioral therapy (CBT), a family of learning-based approaches that help patients eliminate the core fears, associated avoidance and anticipatory anxiety in anxiety disorders. Though anxiety management skills such as muscle relaxation and breathing retraining can provide benefit, CBT is different in that it currently emphasizes helping patients relearn a sense of safety, rather than simply coping, with feared situations and events (Otto, Smits, & Reese, 2004). This systematic relearning utilizes informational, cognitive, and exposure strategies, and can be delivered in both individual and group formats. In exposure-based procedures, patients are repeatedly exposed to feared stimuli under controlled conditions, allowing fears to dissipate (extinguish) as patients acquire a sense of safety in the presence of these stimuli. To achieve this repeated learning, CBT protocols emphasize education about anxiety psychopathology as well as repeated exposure to fear-eliciting cues, often in combination with restructuring of false threat appraisals. The therapy usually lasts 12 to 15 sessions. Examples of exposure exercises for patients with SAD might include giving a speech, attending social engagements, or creating embarrassing situations in which they must engage until anxiety dissipates. From a neurobiological perspective, Gorman, Kent, Sullivan, & Coplan (2000) proposed that CBT deconditions contextual fear at the level of the hippocampus and enhances the ability of the prefrontal cortex to inhibit the amygdala.
In the most recent meta-analysis, cognitive-behavioral group therapy (CBGT) showed a moderate effect size relative to control interventions (0.53) with a number-needed-to-treat of 3.24 (Wersebe, Sijbrandij, & Cuijpers, 2013). Another recent meta-analysis of randomized placebo-controlled trials indicated that CBT protocols are associated with clinically meaningful improvements at the conclusion of acute-phase treatment in SAD and other anxiety disorders (Hofmann & Smits, 2008). Although long-term follow-up studies are sparse in SAD (as in other disorders), the available data suggest that the gains achieved with CBT can be durable over time (Gould, Buckminster, Pollack, Otto, & Yap, 1997). Similar gains were found in a meta- analysis by Powers, Sigmarsson, & Emmelkamp (2008); their literature search produced 32 randomized controlled trials (n = 1479) that were included in the final analysis, showing a clear overall advantage of treatment compared to wait-list (d = 0.86), psychological placebo (d = 0.34), and pill placebo (d = 0.36) conditions at post-treatment on the primary outcome measures. The average treated participant fared better than 80% of the wait-list and 66% of the placebo participants. Patients receiving CBT also fared better than control conditions across secondary outcomes including cognitive measures (d = 0.55), behavioral measures (d = 0.62), and general subjective distress measures (d = 0.47). Importantly, treatment gains were maintained at the follow-up (d = 0.76). They also found that combined exposure and cognitive therapy (versus control: d = 0.61) was not significantly different from exposure (versus control: d = 0.89; p = 0.33) or cognitive treatments (versus control: d = 0.80; p = 0.70) alone. Likewise, group treatments (versus control: d = 0.68) were not significantly different from individual treatments (versus control: d = 0.69; p = 0.62). Effect sizes were not associated with treatment dose (p = 0.91), sample size (p = 0.53), or publication year (p = 0.77). Importantly, these results are in line with previous meta-analytic findings supporting the use of psychological treatments for social anxiety disorder, showing no significant differences in treatment type or format.
The outcome over follow-up periods suggests that during acute treatment, patients learn a method for approaching their social fears and avoidance, and then continue to increase the magnitude of their treatment gains over time (Heimberg, Salzman, Holt, & Blendell, 1993). We are not including additional psychotherapies, such as interpersonal psychotherapy (IPT) and psychodynamic therapies, among others, due to limited available data.
Pharmacological treatments
In contrast to CBT, pharmacological interventions aim to directly target biochemical pathways underlying the anxiety elicited by disorder-specific cues (e.g., social scrutiny for SAD) by decreasing activity in the amygdala (Gorman et al., 2000), a region of the brain involved in emotion. The hypothesized mechanism is the modulation of anxiety via specific biochemical pathways when anxiety is elicited by disorder-specific cues, such as social scrutiny in SAD (e.g., Otto, Safren, Nicolaou, & Pollack, 2003a). The first-line pharmacological treatments for social anxiety disorder include: monoamine inhibitors (MAOI), serotonin selective reuptake inhibitors (SSRIs), tricyclic antidepressants, benzodiazepines, and beta-adrenergic blockers (Lydiard, Brawman-Mintzer, & Ballenger, 1996; Smoller & Pollack, 1996). Currently, the largest evidence base supports the use of MAOIs (e.g. phenelzine sulfate) and SSRIs (i.e., fluvoxamine, sertraline, paroxetine, citalopram, escitalopram, and fluoxetine) for anxiety treatment. This was further supported in a 2011 meta-analysis of clinical trials comparing second-generation antidepressants to placebo controls; Paroxetine, Sertraline, Fluvoxamine, Escitalopram, and Venlafaxine were shown to be consistently more effective than placebo for treatment of SAD, with no difference in efficacy amongst these drugs (Menezes, Coutinho, Fontenelle, Vigne, Figueira, & Versiani, 2011).
Now that we have discussed both treatment types, we will review the advantages and disadvantages of both. Starting with psychosocial therapy, one of the consistent features of CBT is that it has strong relapse-prevention effects. This is a particularly important feature when assessing cost-effectiveness of psychosocial treatments relative to medications; short-term CBT is associated with strong maintenance of treatment gains, whereas pharmacotherapy often requires ongoing treatment to prevent relapse (e.g., Antonuccio, Thomas, & Danton, 1997; Haug et al., 2003; Otto, Pollack, & Maki, 2000). A five-year follow-up study illustrates these results; the authors used a sample of 80 participants, implementing Internet-Based Cognitive Behavior Therapy (Hedman, Furmark, Carlbring, Ljótsson, Rück, Lindefors, & Andersson, 2011). The central feature of treatment was nine self-help text modules, each covering specific themes such as exposure and cognitive restructuring. Participants also had access to therapists, and online discussions, and were assigned homework exercises over the nine weeks of treatment. Participants showed improvements on social anxiety measures at the one-year follow-up that was also sustained at the five-year follow-up. This shows not only the long-term benefits of CBT, but also the possible cost benefits. Although this article did not report on economic data, other studies have demonstrated that Internet-based CBT is more cost-effective than group CBT due to the lower cost of the treatment (Titov, Andrews, Johnston, Schwencke, & Choi, 2009).
CBT also might be a more tolerable treatment relative to medications (e.g., Antonuccio et al., 1997; Hofmann et al., 1998; Otto et al. 2000). A summary of dropout rates, as evaluated in meta-analytic reviews of acute pharmacotherapy and CBT trials, indicates that CBT is equal to or more tolerable than pharmacologic alternatives across the anxiety disorders.
Importantly, studies have shown that CBT is an effective treatment for individuals who have failed to respond to medication treatment for PTSD (Otto et al., 2003b), OCD (Kampman, Keijsers, Hoogdiun, & Verbraak, 2002) and PD (Otto, Pollack, Penava, & Zucker, 1999; Pollack, Otto, Kaspi, Hammerness, & Rosenbaum, 1994; Heldt et al., 2006). Heldt et al. (2006) offered 12 weekly sessions of CBGT to individuals with panic disorder who had remained symptomatic despite an average of three years of pharmacotherapy. At the one-year follow-up, nearly two-thirds of the participants met remission criteria. The most readily available treatment for the anxiety disorders is often medication since psychiatrists and primary care physicians greatly outnumber psychologists trained in CBT. Thus, using CBT as a treatment for individuals who have not benefited from medication may be a practical solution when treatment resources are limited.
A last advantage of psychosocial treatments is that it is not a long-term proposition, whereas treatment-free follow-up data for pharmacotherapy suggest that it is a long-term commitment; relapse is common following medication discontinuation (e.g., Mavissakalian & Perel, 1992; Noyes, Garvey, Cook, & Suelzer, 1991; Stein, Versiani, Hair, & Kumar, 2002; Walker et al., 2000). For the average patient, attenuation of the anxiety response appears to work as long as medication treatment is continued. When treatment is discontinued, however, relapse is common (Noyes, Garvey, Cook, & Samuelson, 1989; Noyes et al., 1991; Pollack & Smoller, 1996). Some studies of panic disorder indicate that relapse rates are attenuated the longer a patient is kept on medication (Mavissikalian & Perel, 1993), though they still must remain on pharmacotherapy for the longer period of time. Pharmacotherapy is sometimes difficult as a long-term treatment option because patients often fail to adhere to pharmacological prescriptions over the long run (Cowley, Ha, & Roy-Byrne, 1997; Sirey et al., 1999; Weilburg et al. 2003), yet the same does not exist in psychosocial treatments.
Advantages of pharmacological treatments
Fewer advantages exist for pharmacological treatment, though a striking one is that it requires far less effort and time than psychosocial interventions. Patients who are too busy or cannot commit to a full course of CBT may be particularly well suited for this option, as they only need to work with their physician to find a therapeutic dose; once that is accomplished, they only need periodic appointments for assessments and refills.
Additionally, there is some evidence, albeit only in panic disorder, that pharmacotherapy may be effective when CBT fails. In a study on the two treatments, Kampman, Keijsers, Hoogduin and Hendriks (2002) randomly assigned individuals with panic disorder who remained symptomatic after 15 sessions of CBT, to continued CBT plus paroxetine, or CBT plus placebo. Those subjects who received the paroxetine experienced significant improvement on measures of avoidance and anxiety whereas those who received placebo did not. These data suggest that pharmacotherapy may be affective for certain individuals who have not had success with CBT alone.
Comparison of psychosocial and pharmacological treatments
Meta-analyses
The first major meta-analysis to compare CBT and pharmacotherapy for SAD included 24 studies with 1079 participants (Gould et al., 1997). Of this meta-analysis, sixteen studies included cognitive behavioral interventions, and 10 included pharmacotherapy. Only two studies included a combined approach (pharmacotherapy with psychosocial treatment). The mean duration of SAD in these trials was 15.92 years, and interestingly the researchers found that both treatments were effective with no significant differences between CBT (ES = 0.74) and pharmacological (ES = 0.62) treatments (see Figure 26.1).
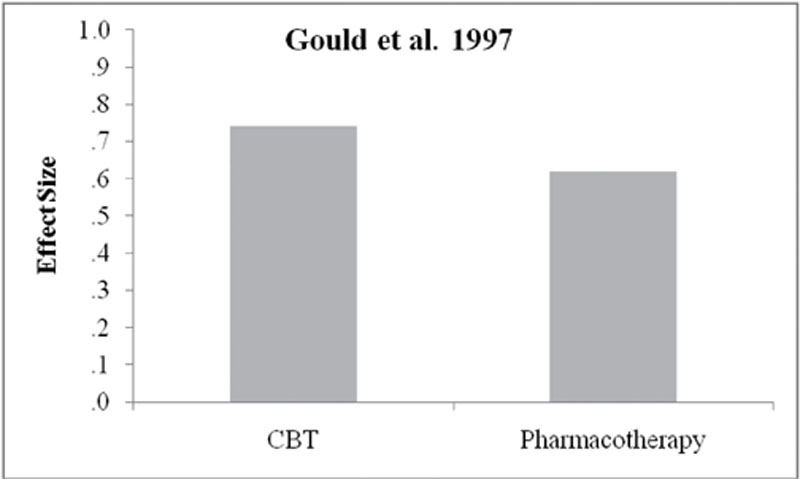
Figure 26.1
Mean effect sizes for CBT and pharmacotherapy in social anxiety disorder trials.
(Data from Gould et al., 1997.)
The treatments with the largest effect size for both types were exposure therapy for CBT (ES = 0.89) and SSRI treatment for pharmacotherapy (ES = 1.89). In total, a cost projection analysis for all treatment types showed that group CBT was by far the most cost-effective treatment option. In 1997, the authors estimated the total cost for cognitive behavioral group therapy (CBGT) to be approximately $600 compared to a yearly cost of $1000 for the cheapest pharmacological intervention (clonazapam). A larger meta-analysis of 108 trials showed that benzodiazepines and SSRIs were equipotent and more effective than applied relaxation and control conditions at post-treatment (Fedoroff & Taylor, 2001). Finally, a recent meta-analysis compared the post-acute efficacy of CBT plus pharmacotherapy with CBT plus pill placebo for the range of anxiety disorders (Hofmann, Sawyer, Korte, & Smits, 2009). The effect size for SAD was small and not significant (ES = 0.16). Unfortunately, there were insufficient follow-up data to determine long-term outcome. Taken together, meta-analyses suggest that medications and CBT are both effective and not significantly different from each other, and combined strategies are not significantly better than monotherapies. Due to this, treatment decisions must be based on other factors, such as cost, long-term commitment, history, and comorbidity.
Individual trials
In this section, we briefly discuss eight randomized controlled trials that include psychosocial and pharmacological treatments in combination for SAD, along with follow-up studies when available. See Table 26.1 for a summary of these trials.
Table 26.1
Randomized Controlled Trials of Psychotherapy and Pharmacotherapy
| Study | Conditions | n | Overall Outcome |
| Clark & Agras., 1991 | CBT + BUS CBT + PL BUS PL |
94 | CBT + BUS = CBT + PL > BUS = PL |
| Gelernter et al., 1991 | SE + Alp SE + Phen SE + PL CBT |
65 | SE + Alp = SE + Phen = SE + PL = CBT |
| Turner et al., 1994 | Exp Atenolol PL |
72 | Exp > Atenolol = PL |
| Heimberg et al., 1998; Liebowitz et al. 1999; | CBGT Phen Psych PL PL |
133 | CBGT = Phen > Psych PL = PL |
| Blomhoff et al., 2001; Haug et al. 2003; | Exp + Sert Exp + PL Sert PL |
387 | Exp + Sert = Exp + PL > Sert > PL |
| Clark et al., 2003 | CT SE + Flu SE + PL |
60 | CT > SE + Flu = SE + PL |
| Davidson et al., 2004 | CBT + Flu CBT + PL CBT Flu PL |
295 | CBT = CBT + Flu = CBT + PL = Flu > PL |
| Blanco et al., 2010 | CBGT + Phen CBGT Phen PL |
128 | CBGT + Phen > CBGT = Phen > PL |
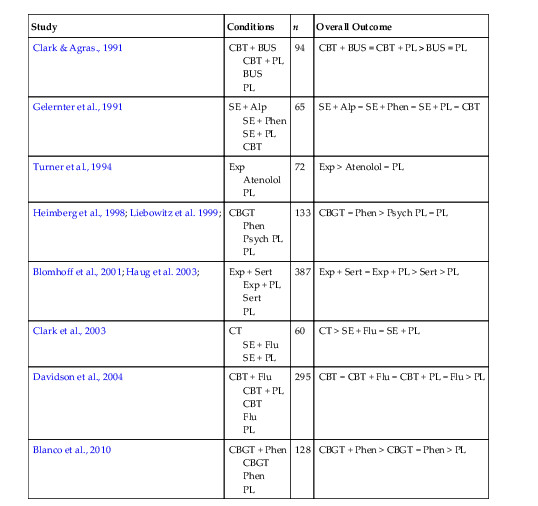
Note: Alp = alprazolam; BUS = buspirone; CBGT = cognitive behavioral group therapy; Exp = exposure; Flu = fluoxetine; Phen = phenelzine; PL = pill placebo; Psych PL = psychological placebo; SE = instructions for self-exposure; sert = sertraline.
First, Clark and Agras (1991) randomized 94 participants with SAD (DSM-III-R) to CBT plus buspirone, CBT plus placebo, buspirone alone, or placebo only over a six-week period. The CBT consisted of five group sessions. Overall, results favored the CBT conditions (with and without buspirone). Both CBT groups showed lower fear ratings during behavioral tasks and on other measures compared to buspirone alone and placebo alone. Interestingly, buspirone was not significantly superior to placebo in this trial. CBT is the clear treatment winner of this trial (with or without buspirone) over buspirone alone.
In a different study, Gelernter et al. (1991) randomized 65 participants with SAD (DSM-III-R) to one of four conditions including: alprazolam with self-exposure instructions, phenelzine with self-exposure instructions, placebo with self-exposure instructions, or CBT alone. Results showed that all four conditions resulted in significant improvement in social anxiety symptoms. They found, however, no differences between any of the treatments. The one consistent component across all four treatments was the inclusion of exposure (in addition to non-specific factors). Thus, the results suggest there was no added benefit of adding pharmacotherapy to exposure therapy. However, the lack of a no-treatment comparison group suggests caution in interpreting these results in this way.
In another study, Turner, Beidel, and Jacob (1994) randomized participants with SAD to exposure only, atenolol, or placebo. Treatment proceeded over a three-month period and the trial included a six-month follow-up. Overall, exposure was superior to both atenolol and placebo. In fact, atenolol did not outperform placebo in this trial. Atenolol, however, is not considered a first-line treatment for social anxiety. Thus, many researchers point out that the outcome of this trial is not surprising.
Later on, Heimberg et al. (1998) randomized participants with SAD (n = 133) to one of four treatments: CBGT, phenelzine, psychological placebo, or pill placebo. The psychological placebo was an educational supportive group and showed equal credibility to the CBGT condition. The participants were then followed for one-year post-treatment (Liebowitz et al. 1999), which included a six-month maintenance phase followed by a six-month treatment-free phase. Overall the CBGT and phenelzine conditions were roughly equivalent over the course of the trial, and both were clearly superior to the control conditions. Phenelzine outperformed CBGT on some measures during the acute phase. Phenelzine, however, also showed a trend for greater relapse during the treatment-free follow-up. In addition, phenelzine is an MAOI and therefore requires dietary restrictions to prevent a hypertensive crisis (i.e., cheese, lunch meats, snow peas, beer and red wine, etc.), which may be difficult for patients to adhere to.
In an interesting community/general practice double-masked design, Blomhoff et al. (2001) randomized 387 treatment-seeking participants with generalized SAD (DSM-IV) to exposure plus sertraline, exposure plus placebo, sertraline alone, or placebo alone. Forty-seven trained physicians with private practices provided the treatments, and the exposure treatment was manualized and monitored for adherence. Participants were followed for one-year post-treatment (Haug et al. 2003), and it should also be noted that funding was provided for this trial by Pfizer. The results of the study showed an advantage of sertraline and exposure plus sertraline during the acute phase of treatment, with response rates at the end of acute phase-treatment equal to 45.5% (sertraline + exposure), 40.2% (sertraline), 33% (placebo + exposure) and 24% (placebo). These findings suggest that sertraline can augment the effects of exposure treatment, particularly when exposure treatment is delivered with minimal therapist contact (i.e., eight 20-minute sessions involving instructions for homework exposures). Relative to CBT alone, however, these benefits of combined treatment were no longer evident at a one-year follow-up evaluation (Haug et al., 2003). During the treatment-free phase, the exposure-alone condition showed substantial continued improvement, whereas the sertraline conditions showed considerable deterioration. This finding is consistent with similar trials in other anxiety disorders. More specifically, treatment gains obtained during CBT while in a medication context may not transfer to the non-medication context (Barlow, Gorman, Shear, & Woods, 2000; Liebowitz et al., 1999; Marks et al. 1993). This phenomenon will be discussed in greater detail later in the chapter. The authors concluded that: (1) sertraline, exposure therapy, and their combination are all effective treatments for SAD; (2) treatment with exposure therapy appears to confer longer-lasting gains than sertraline; and (3) exposure alone is more effective in the long term than when given in combination with sertraline. Thus, exposure alone was the treatment of choice in this trial.
In a separate study, Clark et al. (2003) randomly assigned 60 participants with generalized SAD (DSM-IV) to one of three conditions: cognitive therapy, fluoxetine plus self-exposure instructions, or placebo plus self-exposure instructions. Acute treatment occurred over 16 weeks and participants were followed for one-year post-treatment. Significant improvement was observed in all three conditions, though there was a clear advantage for the cognitive therapy group on SAD measures compared to both the fluoxetine plus exposure and placebo plus exposure conditions. The fluoxetine/exposure and placebo/exposure conditions were not significantly different from each other.
In a more recent large trial, Davidson and associates (2004) randomized patients with generalized SAD (n = 295) to one of five conditions: CBT alone, CBT plus fluoxetine, CBT plus placebo, fluoxetine alone, or placebo alone. All active treatments were superior to placebo on primary outcomes, but investigators found less than a 3% improvement in response rates with the addition of fluoxetine to CBT. Patients treated with CBT plus fluoxetine demonstrated an intent-to-treat response rate of 54% relative to intent-to-treat response rates of 52% for CBT alone, 51% for fluoxetine alone, and 32% for the pill-placebo condition. Overall, at the end of the 14-week trial all active treatments showed significant improvement relative to placebo alone. There were, however, no significant differences between active treatments.
More recently, Blanco et al. (2010) randomly assigned 128 participants with social anxiety disorder (DSM-IV) to CBGT plus phenelzine, CBGT alone, phenelzine alone, or pill placebo alone. The study included four phases: acute phase (12 weeks), continuation phase (12 weeks), maintenance phase (28 weeks), and a 12-month naturalistic follow-up. The data presented only included the acute and continuation phases, and results clearly supported the superiority of combined treatment (CBGT plus phenelzine) throughout the acute and continuation phases. The response rates at the 24-week assessment were 78% (CBGT + phenelzine), 53% (CBGT), 49% (phenelzine), and 33% (placebo) (see Figure 26.2).
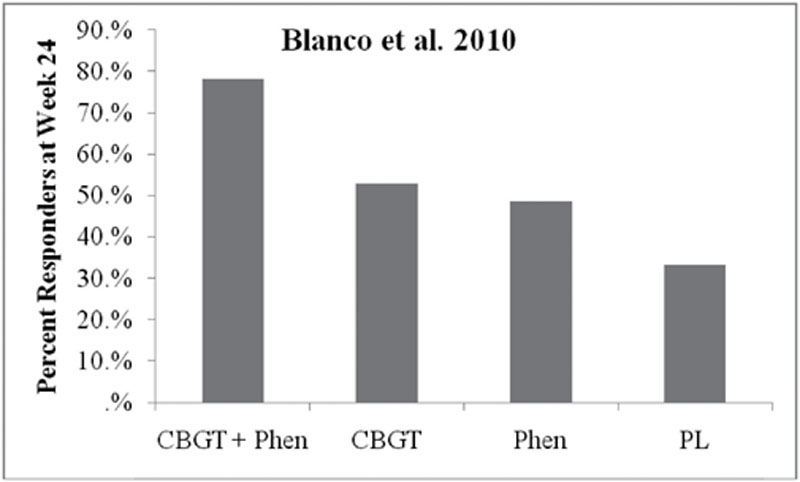
It should be noted, however, that these assessments took place while participants were still in continuation treatment; it will be interesting to find out how the treatments compare after the naturalistic follow-up results are published. Overall, the combined approach was more effective during the acute and continuation phases, though it remains unclear how the participants will fare in the long run.
In summary, the individual randomized controlled trials support the efficacy of both psychosocial and pharmacological approaches. The decision to apply one treatment over the other must then rely on other factors such as cost, long-term outcome, side effects, etc. In the next section we discuss some advantages of each approach to treatment.
Novel therapeutics: combining “cognitive enhancers” with psychosocial treatment
The combination treatment strategies reviewed above represent the application of two independent strategies, each designed to treat disorders on its own. Are there, however, alternative ways to conceptualize the combination of psychosocial and pharmacologic strategies? Rather than focusing on the anxiolytic, antidepressant, or mood-stabilizing effects of pharmacotherapy, can medication be used to enhance the change processes specific to psychotherapy more directly? One such strategy relies not on anxiolysis, but on the enhancement of the extinction learning that occurs during cognitive behavioral therapy.
The idea behind this approach emerged from advances in animal research, which mapped some of the core pathways and neurotransmitters involved in fear extinction (e.g., Davis, Falls, & Gewirtz, 2000; Davis & Myers, 2002). Specifically, animal studies suggest that fear learning and extinction are both blocked by antagonists at the glutamatergic NMDA receptor. Partial agonists at this receptor should then augment learning; which was found to be the case with D-cycloserine (DCS), in animal trials (for review see Davis, 2002; Richardson, Ledgerwood, & Cranney, 2004). More specifically, DCS given in individual doses prior to or soon after extinction (exposure) trials in animals facilitated the process of extinction of conditioned fear, and may even aid the generalization of extinction to related cues (Ledgerwood, Richardson, & Cranney, 2005).
Investigating this more in a groundbreaking study, Ressler et al. (2004) randomly assigned acrophobic patients (n = 28) to one of three treatment conditions: (1) virtual-reality exposure therapy plus DCS 500 mg; (2) VRE plus DCS 50 mg, or (3) virtual-reality exposure plus a pill placebo. Pills were administered in a double-blind fashion one hour prior to each of two weekly virtual-reality exposure sessions. Results indicated that by the second exposure session, patients who had received DCS reported significantly greater reductions in acrophobia symptoms and skin conductance levels during virtual exposures, as well as greater improvement on general acrophobia symptoms as applied to real-world situations, relative to those treated with placebo. Furthermore, this differential benefit was maintained at three months following treatment termination. When combined, these two published studies have examined the ability of DCS to enhance the effects of exposure in the treatment of social anxiety disorder (see Table 26.2
), and have shown very positive and exciting results.
Table 26.2
Randomized Controlled Trials of Psychotherapy Augmentation
| Study | Conditions | n | Overall Outcome |
| Hofmann et al., 2006 | Exp + DCS Exp + PL |
27 | Exp + DCS > Exp + PL |
| Guastella et al., 2008 | Exp + DCS Exp + PL |
56 | Exp + DCS > Exp + PL |
| Guastella et al., 2009 | Exp + oxytocin Exp + PL |
25 | Exp + oxytocin = Exp + PL |
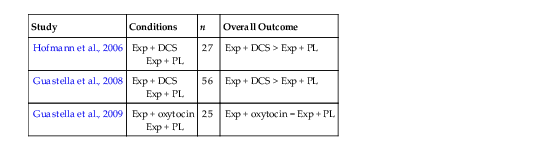
Note: DCS = D-cycloserine; Exp = exposure; PL = pill placebo.
In a very important extension, Hofmann et al. (2006) examined the efficacy of adjunctive DCS in a placebo-controlled trial of CBT for SAD. Using the social anxiety disorder population in this study as a next step was important as SAD is a disorder known for its marked disability and distress, and has been the target of more traditional combination treatment strategies discussed earlier in the chapter (e.g., Davidson et al., 2004). Furthermore, the study examined DCS as applied to a longer course of treatment: a total of five sessions of exposure-based CBT, with DCS or placebo administration one hour before four of these sessions. A total of 27 participants were randomized in a double-blind fashion to receive treatment, and results indicated that patients in the DCS group reported significantly more gains from exposure treatment than those who had received adjunctive placebo plus exposure. These benefits were seen both at post-treatment and at the one-month follow-up assessment. Between-group effect sizes for the advantage of adjunctive DCS versus placebo were in the range from medium (d = 0.72) to large (d = 1.43) according to Cohen’s standards. In a second study investigating DCS treatment for SAD, Guastella et al. (2008) randomized 56 participants with SAD to exposure plus DCS or exposure plus placebo. Consistent with previous findings, the participants who received DCS prior to exposures reported greater improvement in symptoms of social anxiety, dysfunctional cognitions, and life impairment compared to those who received placebo.
The use of adjunctive DCS to enhance therapeutic learning from exposure is fully congruent with concerns against affect modulation and context effects in combination treatments. DCS is taken only prior to sessions, and exposure practice following each week of therapy is during a drug-free state. Even during acute administration DCS is not an anxiolytic and in the 50 mg dose range appears to be virtually free of side effects (e.g., D’Souza et al., 2000; Heresco-Levy et al., 2002; Hofmann et al. 2006;; van Berckel et al., 1998). Thus, DCS emerges, at this early stage, as a particularly promising candidate for enhancing CBT.
Ongoing work is investigating the efficacy of adjunctive DCS across the anxiety disorders. One aspect of DCS treatment that is not known is the number of times it can be used successfully within a treatment episode. Studies of isolated versus chronic dosing (i.e., 20 minutes prior to testing versus daily for 15 days prior) of DCS in animal paradigms have revealed limitations for chronic dosing (Parnas, Weber, & Richardson, 2005; Quartermain, Mower, Rafferty, Herting, & Lanthorn, 1994). As suggested by Ressler et al. (2004), DCS may need to be taken on an isolated rather than a chronic dosing schedule in order for it to have its intended effect on NMDA receptor activity.
The most recent DCS study was a multisite randomized placebo-controlled efficacy study involving 169 patients (Hofmann, Smits, Rosenfield, Simon, Otto, Meuret, & Pollack, 2013). This study was the first large-scale study that evaluated d-cycloserine as an augmentation strategy with a full course of comprehensive CBT for SAD. Participants were enrolled in a 12-session cognitive-behavioral group treatment in which patients were randomly assigned to receive 50 mg of D-cycloserine or placebo, one hour before each of the five exposure sessions that were a part of the treatment. D-cycloserine was not superior to placebo-augmented CBT in this study. However, DCS augmented therapy showed temporary accelerated gains. There was no significant difference between groups in completion rates, response rates, or remission rates at the post-treatment and follow-up assessments. This shows that perhaps d-cycloserine, in combination with a full course of comprehensive CBT, may not be more effective than such a powerful full intervention on its own. Further research of effective dosage and dosage timing should be considered.
With mixed data about the efficacy of d-cycloserine to augment standard full-course CBT, Smits et al. wanted to determine if d-cycloserine enhancement of exposure therapy for SAD depended on the participant’s success in the session (Hofmann et al., 2013 & Smits, Rosenfield, Otto, Marques, Davis, Meuret, & Hofmann, 2013). Using the Subject Units of Distress Scale (SUDS), participants provided their fear ratings at the beginning of their exposure session and just prior to the end of their session. Additionally, after the session, participants were asked to indicate their highest level of SUDS during the exposure session. Blind evaluators used The Clinical Global Impressions Severity and improvement scales (CGI-S and CGI-I) to assess participants. They found that when patients reported low fear at the end of the session, those receiving DCS demonstrated significantly greater clinical improvements than those receiving the placebo. When patients reported high end of session fear, however, those receiving DCS showed significantly fewer clinical improvements than those receiving placebo. Therefore, DCS enhancement was only evident among patients who, on average, had lower fear ratings at the end of their sessions. This suggests that DCS augmentation in successful sessions can lead to significant improvements, yet DCS augmentation in unsuccessful ones may interfere with improvements. This finding is in line with the proposed mechanism of DCS augmentation—it augments whatever is learned (fear reduction or fear “incubation;” e.g., Hofmann, in press).
Another interesting augmentation candidate for exposure-based treatments is the use of intranasal oxytocin. Oxytocin, a hormone, is involved in several social processes, including bonding, communication, social threat, and encoding of positive social cues. Guastella et al. (2009) randomized 25 participants with social anxiety disorder to exposure with oxytocin or exposure with a placebo, and results showed improvements in both groups. The oxytocin condition, however, did not significantly outperform the placebo condition on primary outcome measures for SAD, so it is unclear whether oxytocin will be a viable augmentation agent at this time. A more recent study suggests that attachment style is an important moderator in the effect of oxytocin on social behaviors and cognitions among patients with SAD (Fang, Hoge, Heinrichs, & Hofmann, in press). Therefore, it is possible that the effect of oxytocin depends on certain personality traits.
A third novel therapy that has recently emerged is yohimbine hydrochloride (YOH). Translational research has shown that administration of this alpha2-receptor antagonist is successful as an alternative strategy for enhancing extinction learning (Cain, Blouin, & Barad, 2004). Yohimbine is a rapid-acting compound with an absorption half-time of 10 minutes and an elimination half-life of 36 minutes. Cain et al. (2004) found that, following injection of yohimbine hydrochloride (5mg/kg), fear extinction in mice was accelerated (from 30 trials to 5 trials). Additionally, the mice treated with yohimbine hydrochloride were protected from the negative effects of spacing extinction trials (20-minute intertrial intervals) in comparison to mice treated with placebo.
The theorized mechanism for yohimbine hydrochloride is the stimulation of the medial prefrontal cortex (mPFC), signaling safety both during and following extinction trials. Specifically, yohimbine hydrochloride stimulates c-Fos expression in the mPFC, making it capable of accelerating fear reduction and enhancing subsequent recall of safety learning. YOH blocks inhibition of norepinephrine release, thus increasing norepinephrine in the forebrain regions important for fear extinction including the hippocampus, amygdala, and prefrontal cortex. Indeed, animal literature indicates that mPFC is implicated strongly in extinction learning (Morgan, Romanski, & LeDoux, 1993; Quirk, Russo, Barron, & Lebron, 2000). For example, mPFC activity in healthy rats increases (thereby signaling safety) during testing on the day following extinction learning (Milad & Quirk, 2002), and stimulation of the mPFC in rats enhances extinction learning (Milad & Quirk, 2002; Herry & Garcia, 2002). Likewise, removal of the mPFC in rats precludes the continuation of successful extinction from one day to the next (Morgan et al., 1993; Quirk et al., 2000). In a randomized controlled study in 2009, Powers, Smits, Otto, Sanders, & Emmelkamp (2009) examined the potential exposure-enhancing effect of yohimbine in claustrophobic humans. Participants displaying marked claustrophobic fear (n = 24) were randomized to take 10.8 mg yohimbine or placebo before being treated with two one-hour in vivo exposure sessions. Both groups improved equally post-treatment, and, consistent with predictions, the group that took yohimbine showed significantly greater improvement at the one-week follow-up. This pilot study provides support for the use of yohimbine to enhance exposure therapy.
Importantly, a more recent randomized controlled trial in 2013 explored the effectiveness of yohimbine on social anxiety (Smits, Rosenfield, Davis, Julian, Handelsman, Otto, Tuerk, Shiekh, Rosenfield, Hofmann, & Powers, 2013). Forty adults with a diagnosis of SAD were randomized to placebo or yohimbine HCI (10.8mg). Participants were instructed to take the medication one hour before each of the four exposure sessions, and results showed that the yohimbine condition resulted in faster improvement and better outcomes on self-reports of SAD and depressed mood severity compared to placebo. Although differences were found amongst the self-report measures, no significant differences were found on clinician-rated assessments of social anxiety symptoms. These results indicate moderate support for yohimbine augmentation of exposure therapy for those with social anxiety disorder, and trials are currently under way to determine if yohimbine also enhances fear reduction in social anxiety disorder.
Discussion
As discussed above, current data suggest that pharmacotherapy, CBT, and their combination are effective treatments for the symptoms of social anxiety disorder, and that interestingly there are few differences between treatment modalities when compared directly. There is some suggestion that a combined approach may yield faster results in acute treatment, and after treatment discontinuation there may be less relapse with CBT. In reality, however, most patients are given pharmacotherapy as a first-line treatment for social anxiety. Thus, if they do arrive at a psychotherapy clinic they are most likely taking medication. This partly reflects the fact that primary care physicians far outnumber experts in delivery of CBT for SAD, as well as the fact that patients typically approach their primary care doctor for advice about anxiety first. The question is then, if full programs of CBT are not available, should elements of CBT be added to pharmacotherapy in order to yield greater treatment gains? Research shows that instruction for patients to do exposures themselves in a stepwise fashion offers benefits similar to therapist-guided exposure for some disorders, and that the addition of elements of CBT, particularly instruction in stepwise exposure, has been shown to enhance pharmacologic treatment in both specialty care and primary care settings (Craske et al., 2005; Marks et al., 1988; Mavissakalian & Michelson, 1986; Telch, Agras, Taylor, Roth, & Gallen, 1985). Indeed, the “prescription” of exposure assignments conjoint with medications has been and is currently recommended as standard practice in pharmacotherapy for SAD (Sutherland & Davidson, 1995). Accordingly, one strategy for combination treatment is to consider elements of CBT as “add on’s” to pharmacotherapy, helping ensure that patients have a framework for re-entering and persisting in avoided situations. This approach has the advantage of extending the benefit of pharmacotherapy without substantially increasing costs when a CBT specialist is not available for a full program of treatment. It has the limitation, however, of failing to use the more comprehensive programs of CBT that have shown particular acceptability, tolerability, efficacy, and cost-efficacy on their own (Deacon & Abramowitz, 2005; Heuzenroeder et al., 2004; Otto et al., 2000).
The issue of adding pharmacotherapy to full packages of CBT requires greater consideration of whether core fears associated with anxiety disorders can be treated adequately when these fears are being attenuated by medication. A number of accounts of the fear reductions from exposure stress the importance of evoking a full anxiety response during exposure (for a review, see Powers, Smits, Leyro, & Otto, 2006). For example, in their emotional processing theory, Foa and Kozak (1986) stress the importance of adequate activation of fear-related memories so that new (safety) information can be incorporated in these memories. Adequate activation depends in part on whether the exposure procedures are a realistic representation of the feared event or situation, including the elicitation of fear itself during exposure. This theoretical account is consistent with findings showing that reduction of the perceived threat of the exposure situation also reduces the efficacy of exposure. For example, the availability of escape strategies (Powers, Smits, & Telch, 2004) or strategies such as distraction from the feared stimulus (e.g., Kamphuis & Telch, 2000; Rodriguez & Craske, 1993) or “playing it safe” in the presence of the stimulus (Sloan & Telch, 2002) can each reduce the efficacy of exposure. Thus, adding pharmacotherapy to full CBT protocols may diminish the effect of CBT by diminishing the full anxiety response.
This increased risk of relapse following termination of combined exposure-based and pharmacological treatment is the role of context (for review, see Bouton, 2002; Powers et al. 2006) and may be due to other reasons as well. Specifically, animal studies have shown that extinction learning, which involves procedures similar to exposure-based treatments, is context-specific (Bouton, 2002). That is, extinction of fear that occurs in one context (e.g., room A) may not generalize to a second context (e.g., room B). Accordingly, shifts in context such as medication discontinuation (i.e., the drug-state is withdrawn) may account for the loss of gains apparent during acute-phase treatment (i.e., the extinction memory is specific to the state of being on medication). Mystkowski, Mineka, Vernon, & Zinbarg (2003) tested this hypothesis using a sample of participants fearful of spiders. They randomly allocated these participants to ingest either caffeine or a pill placebo before receiving treatment involving exposure to live spiders, and they assessed outcome by means of a behavioral approach task immediately following treatment completion. To test the hypothesis that extinction learning during CBT is context-specific, and thus would be lost as a result of changing the drug state, the investigators retested participants one week following treatment under conditions of either the same or opposite drug context. Consistent with predictions, participants who were tested under the incongruent condition (e.g., treated while taking caffeine and later tested while taking placebo) displayed greater return of fear compared to those tested under the congruent condition (e.g., treated while taking caffeine and later tested while taking caffeine).
A third theory, the self-efficacy theory (Bandura, 1977), offers a possible alternative or complementary mechanism underlying the negative effects of long-term medication on patients also undergoing CBT. The self-efficacy theory posits that phobic behavior is a function of one’s perceived inability to execute effective coping behavior in response to potential phobic threats (Bandura, 1977). It seems plausible that medication-taking may cause patients to attribute their gains to the medication instead of their own efforts and accomplishments, thereby undermining self-efficacy enhancement. Indeed, patients with anxiety disorders tend to attribute treatment gains to external factors (Adler & Price, 1985; Anderson & Arnoult, 1985; Broadbeck & Michelson, 1987; Cloitre, Heimberg, Liebowitz, & Gitow, 1992; Emmelkamp & Cohen-Kettenis, 1975; Hoffart & Martinsen, 1990) rather than to their own efforts. The influence of patients’ attributions of treatment gains to medication on the outcome of combined treatments has been examined in a few studies. Basoglu, Marks, Kilic, Brewin, and Swinson (1994) reported that attributions of improvement to the medication (i.e., alprazolam or placebo) significantly predicted relapse in panic disorder patients treated with exposure in combination with medication. Interestingly, Biondi and Picardi (2003) reported that making external/medication attributions in panic disorder treatment was associated with a 60% relapse rate, whereas making internal attributions was associated with a 0% relapse rate. Thus, the self-efficacy theory could be a factor in why combined pharmacotherapy treatment with CBT has higher relapse rates than CBT alone.
Possibly the strongest evidence for the causal role of external attributions in relapse following the discontinuation of combined treatments, however, comes from a recent analogue study by Powers, Smits, Whitley, Bystritsky, and Telch (2008). Using an experimental design, the investigators first randomly assigned participants displaying marked claustrophobic fear to one of four conditions: wait-list, psychological placebo, exposure-based treatment, or exposure-based treatment plus an inactive pill. They did a post-treatment assessment that revealed an advantage of exposure over control conditions and no effects of pill-taking, and afterwards, they manipulated attributions concerning medication-taking by randomly assigning participants in the exposure-based treatment plus pill-placebo condition to one of three instructional sets: (1) they described the pill as a sedating herb that likely made exposure treatment easier; (2) they described the pill as a stimulating herb that likely made exposure treatment more difficult; or (3) they described the pill as a placebo that had no effect on exposure treatment. Assessments at follow-up showed that the participants who believed that the pill had a sedating effect had a relapse rate of 39%, whereas the participants in the two other medication- taking conditions had a relapse rate of 0%. Interestingly, reduced self-efficacy accounted for the elevated relapse rates associated with the sedating instructional set.
Collectively, these findings suggest that the practice of acute-phase combined treatments may benefit from specific strategies to prevent relapse. These include assessing and modifying patient attributions regarding treatment gains, as well as continuing exposure practice following pharmacotherapy treatment. Indeed, for patients who would like to discontinue medication following successful CBT, research suggests that a slow taper coupled with reapplication of exposures during the taper does reduce relapse (e.g., Otto et al., 1993; Whittal, Otto, & Hong, 2001).
Overall, though, based on the available data as well as cost–benefit considerations (see Otto et al., 2000; McHugh et al., 2007), it appears that there is no strong justification for recommending that combined treatment be adopted as a standard, first-line treatment for optimizing acute outcomes for the social anxiety disorder. Whether combination treatments are indicated for certain subgroups of patients (e.g., those with comorbid depressive disorders) or in settings where CBT cannot be delivered in its most optimized form (e.g., primary care) are questions that deserve further inquiry. Although the evidence to date provides no justification for recommending combined treatments as a first-line intervention for anxiety disorders, it does not rule out that the combined approach holds great value for many patients suffering from social anxiety disorder, as a second or third-line approach.
It appears the efficacy of combined psychosocial and pharmacotherapy treatments varies and depends on many factors, including patient medication preferences, availability of state-of-the-art CBT, and the presence of comorbid conditions at the start of treatment. Another consideration for the efficacy of combined treatments is attenuation; recent large-scale studies of SAD (Davidson et al., 2004) and OCD (Foa et al., 2005) point towards higher dropout rates in combination treatments than CBT alone, but this trend was not evident in a multicenter trial of panic disorder (Barlow et al., 2000). Given these mixed data, a conservative conclusion is that combination treatment offers no reliable advantages to CBT in terms of the acute retention of patients, and may have other unfortunate effects. Considering the availability, tolerability, and efficacy of combined treatment strategies for anxiety disorders, we believe the available evidence illustrates that elements of CBT, particularly instruction in stepwise exposure, offer a fairly reliable benefit to ongoing pharmacotherapy, when these treatment elements can be provided as part of the care of the pharmacotherapy team, and do not require resources from clinicians who otherwise would provide full packages of CBT. When patients in a single treatment condition are not benefitting, clinicians and therapists should consider combination treatment, as well as when a patient wishes to discontinue psychopharmacological-only treatment. The best treatment, however, is when state-of-the-art CBT is available. This intervention can be offered alone and achieve results that rival combination treatment in many cases and offer the potential for greater durability of treatment and lower cost (e.g., Heuzenroeder et al., 2004; Otto, Pollack, & Sabatino, 1996). As such, clinicians should be cautious about recommending routine combination treatment when full packages of CBT can be provided.