[CHAPTER 2]
Preparation
Make Your Body Ready
IN ORDER TO MAXIMIZE YOUR CHANCES OF COMING THROUGH ANY GRIDCRASH SCENARIO, YOU must optimize your health before any event that might significantly disrupt societal infrastructure. This requires that you begin to aggressively protect your health now, including maximizing your fitness and minimizing your risk for illness and injury. Part of this can be done through simple lifestyle choices and, as is so often the case in life, we know what we should do but don’t always do what we know we should.
Before gridcrash, fitness is a highly desirable trait: A New England Journal of Medicine study showed that for each hour you spend engaged in vigorous exercise, you are rewarded with an additional two hours of life, probably of a higher quality.
After any societal cataclysm, a good level of fitness will be more than just a way to improve your quality of life or looks, or to extend your years on this Earth. Fitness will be essential to survival. The fight for survival will be just that at times: a physical struggle. You must be fit for that struggle. This gives new meaning to “survival of the fittest.”
Physical fitness, like money, is fungible: Once made, it can be spent in a variety of manners. What does this mean? Fitness gained from riding your bike to work may help improve your ability to walk to the store, grow crops in the garden, chop firewood, push a wheelbarrow up a hill or run from danger. If you are fit and healthy, you can expect that these tasks will be much easier for you than for somebody else who has not done any regular exercise.
A good base of fitness will keep your weight down, enhance your ability to recover from physical insults and emotional stresses, and improve your tolerance to extremes of weather such as heat waves. In all likelihood you will also have larger mental reserves, making it easier to think clearly under stressful situations or when you are tired. The endorphins released during vigorous exercise also improve your mental outlook in general and improve your morale in hard times, making depression and anxiety less likely.
Functional Fitness for a Crash
IF YOU ARE READING THIS, YOU ARE PROBABLY ACTIVELY ENGAGED IN SOME FORM OF A FITNESS regimen already. It is much less likely that you are someone who smokes, eats to excess, binge-drinks alcohol or plays video games at the expense of even a modicum of exercise. Still, this chapter is important: Hard times call for hard folks. Not necessarily emotionally hard, but people who are able to meet the potential physical demands of a world without modern conveniences.
How should you go about getting fit? While treadmills, rowing machines, elliptical trainers, yoga and group exercise classes are all beneficial for developing some elements of fitness, and may even be fun, I would argue that you need more than this--or if not more, perhaps a different approach. I like to call it functional fitness.
Functional fitness is just what it says: fitness that allows you to perform functions, not just the contrived motions of the elliptical trainer or aerobics class. Functional means you can DO something useful. In the variety of scenarios following gridcrash, these functions are things that allow you to get done the things you need to do in order to eat and drink, have shelter, travel and the like. Again, these are things we take for granted today, but may not be able to so easily in the future. I mean the strength and endurance to collect firewood, dig a latrine, walk several miles to the store and carry back a load of groceries and to complete other similar tasks.
How do I suggest you go about obtaining this functional fitness? Well, after you have a base of fitness from the gym or your recreational pursuits, you should start doing those activities that you may end up being forced to do by circumstances. This offers you some distinct advantages. First, you can get in a good workout. Fitness is also somewhat specific: We are what we train to become. Doing diverse tasks will build muscle strength and agility over the whole body. As your agility for these tasks improves, you will be less prone to mistakes that can lead to injury, especially as you learn new tasks. Finally, there are time and potential money savings realized by combining your workout with sustainability measures.
For example, let’s say you have a wood stove in your home. Instead of paying someone to deliver wood to your house already cut and split, do the following: Put on boots and grab a pack. Go to a wooded area near your house (with permission or permits as required). Bring a saw and a splitting maul, plus protective equipment. Find trees that have been blown over and section them with the saw, then split them. Carry a load out to your car or truck. Repeat. Not only will you now have firewood, but you will have learned some useful skills and improved your functional fitness level.
Think about what tasks you might need to do to keep your family or your home going after gridcrash. Heat from that woodstove may be lifesaving, but only if YOU can get the fuel. Veggies and starches from the garden? Can you grow them? Not “harvest” them from the store, but turn the compost pile, hoe the row for the seeds, bend and pull weeds, and all the other tasks needed to be self-sufficient, day in and day out? Maybe you just need to get a few miles to work; what if you have to walk or bicycle because there’s no gas and the buses sit idle?
These questions are important because if you are not healthy and in good shape before bad times, you probably WON’T be able to get healthy and fit afterward. The time to prepare is now; waiting until you “need to prepare” might be too late. It is best to figure out NOW if you have a problem and then fix it—be it a shoulder that won’t let you split wood with a maul, a knee that keeps you from carrying a load of groceries home or a back that limits you to two hours of gardening per day.
But you say you can run a marathon. Good for you. You have a great fitness base. Maybe instead of running 5-6 days per week, you should diversify and do some functional fitness activities—walking or bicycling to the store or other brief errands, or working in the garden. As in nature, diversity builds resilience. Repetition is important too, so choosing activities that you enjoy doing will help you sustain your exercise regime. What about swimming, rock climbing, rowing, cross country skiing? At least do something that covers all of the major components of fitness—strength, speed, endurance, agility, and flexibility. Make sure you don’t neglect major muscle groups or motions.
Maybe you live in the city, and the idea of playing Paul Bunyan is impractical. If so, look for ideas like “boot camp.” “strongman” or “dinosaur training” style workouts. These old-school training philosophies focus more on functional fitness attributes that aren’t usually emphasized in gyms.
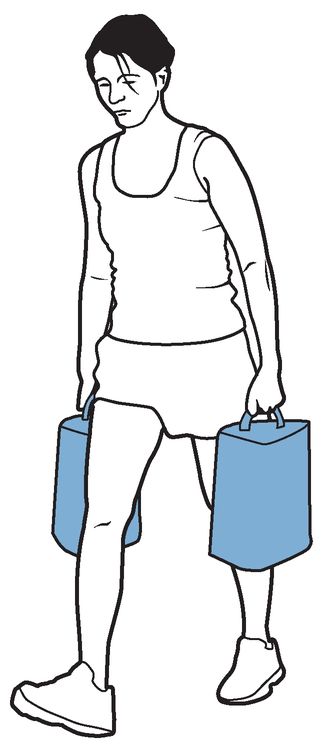
I think that, in our modern world, we have several glaring weaknesses when it comes to attaining functional fitness. First is load carrying. Look at folks from the rest of the world: Huge numbers of people in Africa, Asia and Central and South America have to carry food, water or fuel many miles. Forget about walking unladen; they have that down, too. In my mind, you need to be able to cover at least 4 miles with 30-40 pounds on your back in an hour. Unsupported: no stops, no food, no water. We evolved as bipeds, so this is programmed into our biology. Start by walking one mile at a brisk pace, then add a little weight, gradually increasing your pace, distance, and weight.
There is a reason most elite military units use long marches under heavy packs as part of their training and selection processes. The fatigue they induce brings out our personalities. As Vince Lombardi said, “Fatigue makes cowards of us all.” A benefit of this kind of work is learning how you respond to stress, both bodily and more importantly emotionally. Believe me when I tell you that even if you have a stressful life now, it will be worse after the lights have been off for a week!
“Farmer’s walk”
Another deficient area for a lot of people is grip strength. Many of us have soft hands from our relatively pampered lives, and weak grips result from a lifestyle that doesn’t force us to use our hands. Even fit people don’t do a lot of exercises that force them to use their grip. What happens when you need to carry a five-gallon bucket of water, waste or food, repetitively or over long distance? How about swinging an axe or a maul or a sledge to clear land or split firewood?
Finally, many of us are fair-weather exercisers: If the weather isn’t PERFECT, we head indoors for the workout, the iPod in our ears, the TV in our face, and the water bottle close at hand. A gridcrash scenario will force you to bear the summer day’s heat and humidity, and the winter night’s cold and dark. Now is the time to get used to them, too.
There are lots of potential gym exercises suggested to help remedy these weak areas, but as Nike’s famous slogan says: “Just Do It”! Do those things that maybe modern life and our neighbors discourage us from doing. Ditch the snow blower and shovel the driveway and walkways. Walk or bike to work or the store. Put on a backpack and go hiking on the weekend instead of playing golf or lounging by a pool.
If you have to rely on a gym, there are alternatives. While many personal trainers in trendy health clubs with lots of chrome dumbbells can be heard exhorting their clients to build core strength, you will go a long way toward this kind of fitness with simple body weight exercises like pull-ups, push-ups and sit-ups. Add “Farmer’s walk” where you simply carry a dumbbell (or similar weight) in each hand and walk as far as you can. You get both grip strength and load carrying benefits at the same time.
If you don’t want to do this, you could walk around your back yard carrying a 5 Gallon bucket in each hand; simply add water as your strength and endurance improve. Similarly, you could carry groceries from the store or books from the library in a pack, walking each way. Could there be a simpler way to functional fitness?
Healthy Habits Before Gridcrash
BODY PREPARATION ALSO INCLUDES MA XIMIZING YOUR HEALTH. LET ’S SAY THAT YOU ENJOY more than the occasional drink, or maybe you smoke a few cigarettes with coworkers each day, but you say you “can kick the habit” anytime. I have only two words for you: Quit now! Not only are these habits a drag on your health, but after the widespread disruption caused by gridcrash, you may be forced to go “cold turkey”.
Do you know how you will be affected when this happens? If you really can’t quit that easily, are you willing to incur the added cost of these items, which is certain to rise in the future? This concern goes even for folks like me that rely on that morning cuppa Joe to get us going. Ever had a caffeine withdrawal headache? The time to find these things out is now, not later when you are stressed because your stocks just tanked, or there is an hour-long line to buy rationed gas or a curfew because of a recent terrorist attack. Try a “drug holiday” where you see what happens when you quit, cold turkey, even for a day.
If you have more of a problem, either with frequent heavy use of alcohol, routine use prescription medications like pain pills or sedatives, or if you use illegal drugs, you are probably not reading this book. Still, if use of alcohol or drugs is an issue for you or a loved one, keep in mind that withdrawal from them can not only be painful, but could kill you in some cases. Again, the time is now to do something about this.
Most of the determinants of health that we can affect ourselves are related to our lifestyle habits: diet, exercise, rest, vices and the like. Genetics impact our health, as do the nature of our fallible biological structures, but we can do very little to change the impact of these on our health. Much as we are what we eat, we are also what we drink, smoke or otherwise put in our bodies. We are what we are because of what we do to ourselves.
A recurring theme of this book is that now is the time to prepare, while things are relatively good. If the predictions of climate change, economic despair or petrocollapse come true it will be even harder than it is now to use willpower to bring about positive changes, be it in your habits or in any other area of preparation addressed in this book.
Nutritional Optimization of Health Prior to a Crash
DIET AND NUTRITION HAVE ALWAYS BEEN CONTROVERSIAL AREAS. YOU CAN FIND PASSIONATE advocates for just about any kind of diet: The low-carb, high-fat fans decry the high-carb, low-fat proponents. Some say megadose vitamins are necessary and could prevent cancer, while others say well-balanced diets are just fine without supplements. Other folks have come up with even more exotic or exacting, or both, dietary advise. Look in any bookstore, and you will find a huge array of diet books. The grizzled sages among us say that if any single diet worked we wouldn’t need all these books! Still, now is the time to find a healthy diet that you can follow. I can’t pick one for you, so it’s up to you to find out how to have a nutritionally sound diet.
From my viewpoint, working towards self-sufficiency dictates that you learn about diet and then make choices you feel are best for yourself and your family. Having said that, your doctor or a health educator or nutritionist, if you have access to one through your insurance or your job, can steer you in the right direction. In addition, the USDA and a number of other organizations have published some basic guidelines on what constitutes good nutrition.
For all intents and purposes, the key to sound nutrition is probably variety and moderation in everything. There should be a focus on “whole foods” with as much of your diet being fresh foods like fruits and vegetables as possible, with a minimum of pre-packaged processed foods. You should especially avoid foods high in simple sugars, fats or preservatives. See the list of resources at the end of the chapter for ideas on how to optimize your nutrition.
We have already looked at the medicinal use of one food, honey. There are a number of other foods that have also been shown to have useful clinical effects. This has been known since the days of Hippocrates, the founder of the western medical tradition, who said “Let food be thy medicine.”
Sticking with that theme, we know that diets rich in fruits and vegetables help reduce the risk of cancer, while processed foods and meats are associated with heightened cancer risks. In general, a diet composed of whole foods like fresh fruits and vegetables but low in processed foods with their simple sugars and unhealthy fats is best overall. Some foods, though, seem to possess additional benefits.
Medicinal foods offer benefits in that they are likely to be cheaper than a lot of medicines and may have fewer side effects, plus you can grow your own, and they are dual-use—you may get a yummy meal with your medicine, a different take on Julie Andrews’ spoonful of sugar!
Teas are consumed world wide because they are pleasant, socially acceptable, economical, and safe. Teas contain biologically active compounds that may prevent a wide variety of diseases: It is the best source of an antioxidant class called flavonoids, and contains many other useful components such as vitamins and fluoride. Based on this, doctors have identified many potential beneficial medical and health effects of a number of teas, which are under study for further uses even now.
Black tea has been shown to generally give a positive effect on health. Evidence has shown risk reduction for coronary artery disease at intakes of at least 3 cups per day, and for improved antioxidant status at intakes of 1 to 6 cups per day.
Green tea may also help to reduce the risk of cardiovascular disease and some forms of cancer. It also promotes oral health and may have anti-hypertensive effects, help to control body weight, protect against solar ultraviolet radiation, and increase bone mineral density.
Extensive use of spices probably came about when folks recognized that not only did they add flavor to foods but they seemed to offer some preservative effects, making foods last longer in the time before refrigeration. These benefits probably derived from either anti-microbial or anti-oxidant effects, and it is these effects that earn spices the focus of modern medicine in the search for new drugs from old herbs.
Garlic has been used as a medicinal agent for thousands of years, starting with the ancient Egyptians. In more modern times, Louis Pasteur, considered the father of infectious disease, reported the antibacterial effects of garlic in the 1850s. Garlic seems to have other immune system boosting effects as well.
Garlic is currently recommended as an aid to lowering cholesterol, reducing other cardiovascular risk factors, and for anti-neoplastic (cancer fighting) and antimicrobial properties. For these effects, you need about 1-2 raw garlic cloves per day, which some feel can lead to unpleasant breath and body odors as well as gas and stomach upset; topical use can lead to burns and dermatitis.
Some studies have shown about 10% reduction in cholesterol in those taking a garlic supplement compared to those taking a placebo. There is an ongoing clinical trial to characterize the usefulness of garlic, sponsored and funded by the US Government through the National Center for Complementary and Alternative Medicine (NCCAM).
There is weak evidence that garlic improves blood pressure, lowers blood sugar in diabetics, reduces the stickiness of blood platelets (the effect we seek in prescribing aspirin for heart attacks) and slows development of atherosclerosis.
Taken together, these effects if real could not only make garlicky foods taste good but reduce the rate of heart attack and stroke, two of the biggest killers of the modern age.
In terms of cancer, folks who eat a lot of garlic and similar vegetables (allium class like onions) show lower occurrence of stomach and colon cancer than those who consume lower amounts of these foods.
Garlic extracts exert activity against bacteria, viruses and fungi in vitro (“in glass” or test-tube based experiments). Currently there seems to be very little clinical evidence of useful antimicrobial effects, but garlic has traditionally been used for a wide range of infectious conditions.
Ginger works to help reduce the severity of symptoms from osteoarthritis, the degenerative form that occurs from wear and tear associated with age, overuse and prior injury. It has been shown to work, although not as well as ibuprofen, in relieving knee pain; presumably it would help pain in other joints as well.
The NCCAM has evaluated the available studies, and has also funded investigators to study interactions of ginger with some drugs (immunosuppressants), plus its effect of reducing nausea in patients receiving chemotherapy, and the safety and effectiveness of its use for preventive health purposes, as well as its impact on inflammation. When these studies are done, ginger’s utility will be clearly outlined and available for incorporation into mainstream therapy, and also for post-gridcrash use. Ginger may not be a true “universal remedy” as some label it now, but it may be proven in the future to have widespread medicinal value.
Another spice that can help with inflammatory diseases like arthritis is cur-cumin, a major constituent of the spice turmeric. This staple of Ayurvedic medicine seems very safe as a topical or oral treatment of pain from arthritis.
Many other foods have utility as either preventive measures or as therapeutic agents:
Vitamin D (the sunshine vitamin) seems to improve respiratory health, and may reduce the impact of tuberculosis, respiratory viruses and asthma and emphysema. Supplements also have been shown to increase lifespan.
Essential fatty acids like omega-3 and omega-6 fatty acids (that our bodies can’t make) from fish oils, berries, nuts and eggs have a wide range of benefits, including reducing cardiovascular diseases, depression and dementia, among other maladies.
Probiotics (helpful living organisms found in foods like yogurt, sour-dough, sauerkraut) help maintain intestinal health and seem to play a role in protecting us from a variety of inflammatory reactions that could cause us problems ranging from irritable bowel syndrome to preterm labor and hospital-borne infections.
Cloves, oregano, cinnamon, pepper, ginger and garlic have high levels of antioxidants that may protect against cancer and vascular disease.
A wide variety of edible mushrooms seem to have anti-tumor activity in lab studies, though none have been proven to treat or prevent cancer.
It also pays to remember that obesity-- and the diabetes and other metabolic changes that come with it-- can impair immunity and put you at risk for infections, so go easy on the food.
Functional foods, those like those discussed above, may offer the utility of medicines while having advantages like ease of procurement or cultivation. Some may have fewer side effects than drugs used to treat the same condition, although no medicine, even natural, is truly free of side effects for every user. Still, keep an eye on sites like those listed in the appendix for further word on the value of these low-tech dual-use commodities.
Water is a key nutrient that most people ignore. Humans are about 70% water. Most of us probably don’t drink enough water; we know that some physical and mental performance measures are worsened by dehydration, beyond simply feeling worse. A 2-3% drop in body water makes you less attentive to details and you will have to concentrate more and work harder on simple tasks. More importantly, though, is that folks who are dehydrated feel worse: They feel more tired and less alert. Any parent knows that kids get confused, irritable and lethargic when they’re thirsty.
In addition, people frequently confuse hunger and thirst. Try it yourself: When you feel hungry, drink 8 ounces of water and wait. See if the hunger passes or persists before you chow down!
Staying well-hydrated helps to prevent dental disease, constipation, kidney stones and urinary tract infections. Nobody would want any of these ailments to strike in the best of times, so just imagine how nice it will be to minimize your risk of these occurring after gridcrash or in some other scenario (like travel or camping) when care may not be easy to find.
A final benefit of water for health has to do with respiratory infections. There is some evidence that staying hydrated protects you from viral respiratory infections and also helps people with asthma control their symptoms.
We have already talked about the importance of exercise and fitness in order to be adaptable to a future shift and to thrive after gridcrash. Exercise can also help prevent or control many of the chronic diseases (diabetes, high blood pressure, elevated cholesterol, heart disease, arthritis, cancer and depression, among others) that are the bane of modern life, even in the developing world. Again, even if you think all this talk of gridcrash is exaggerated, I hope I have convinced you of the utility and benefits of these lifestyle changes. Nowhere is this more important than with exercise: Modest exercise, like one hour of brisk walking each week, proved enough in most studies to have significant positive impact on your health. As noted above, though, I think you should be seeking a higher level of functional fitness than this.
Inactivity has been found to be just as dangerous as a moderate level of cigarette smoking. And it’s almost never too late to reap the benefits of exercise. Even if you have emphysema, diabetes or coronary artery disease, for example, you can extend your life and improve your years’ quality by improving your fitness.
Finally, as you go through all the efforts to get ready, don’t forget to rest. In our rush-rush-rush Crackberry Facebook 24-hour news cycle text-messaging world many people don’t get enough rest. We know that those who don’t get enough sleep are at higher risk for cancer, chronic disease, obesity and injury. A recent study showed that those who sleep less than 7 hours per night have 3 times the risk of getting a cold after being given a dose of rhinovirus, one of the causes of the common cold, than those who sleep 8 hours a night. Even resting in bed while not sleeping did not confer the benefit of sleep.
The good news is that exercise alone helps improve both how much and how well you sleep when you go to bed. How cool is that: All of this stuff ties together. Drinking water may reduce your weight, exercise improves your sleep, and all of these changes will improve your health!
Conclusion:
Despite optimism in some quarters that we have seen the end of history, it is clear we live in turbulent times. The recent economic roller-coaster, climate change fears, potential energy insecurity and any number of other news items show that we can’t simply rely upon naive optimism. It pays to make your life ready for gridcrash, but not just because of a post-crash world; you can derive benefits from your own efforts to make your body ready. If you don’t want to do these things for cynical or selfish reasons alone, recognize that these activities can also reduce the impact your life exerts on others and on the Earth. For all of these reasons, now is the time to make your body ready: Get fit, get rid of your vices, and get yourself on a good diet with plenty of water. Then get a good night’s rest!
Make Your Mind Ready
SELF-SUFFICIENCY IN ANY ARENA DEMANDS THAT YOU HAVE KNOWLEDGE AND SKILLS TO apply to activities needed for daily living. For many of these activities, the knowledge you need is easy to acquire, and for some areas, you already have much of the knowledge. You may have hobbies that give you skills that bear on sustainability. You may be a green-thumb, for instance, a master at raising flowers. This knowledge could be easily adapted to use in growing vegetables for helping to feed your family.
Other areas of knowledge needed for self-sufficiency are more esoteric and less commonly studied avocationally. Health care is certainly one of these areas. Few people read anatomy and physiology for fun. Instead, we rely on those further up the health care pyramid to use their interests and aptitudes to help us.
This chapter will guide you through some ways in which you can begin to acquire knowledge and skills in health care. As with most issues related to self-sufficiency, it is entirely up to you to decide how deep and broad you want these skills to be. For some, knowing simple first aid and hygiene measures will suffice. Others want more advanced skills, perhaps at the level of a nurse or EMT. A few will seek to gain credentials akin to an independent practitioner like a physician, an NP (nurse practitioner) or a PA (Physician Assistant) (PA). All of these are laudable goals.
Additionally, I will show you how you can use a community or neighborhood coalition, or “Village University.” approach to train yourself and those close to you in obtaining these skills using experts that may already be among your circle of friends.
Finally, new media tools like the Internet, YouTube and iTunes make acquisition of skills in self-sufficiency cheap and easily accessible without having to attend classes or pay for materials or instruction. I will show you some of these to get you started “surfing the web” and will also talk about other ways of getting some training on the cheap.
Credentials vs. Competencies
FOR STARTERS, WE NEED TO EXAMINE THE GOALS YOU HAVE IN GETTING TRAINING AND KNOWLEDGE in health care. This is a key matter that is not an issue in most other areas of sustainable living.
Credentials basically allow you to add initials to your title: EMT, PA, RN, NP, MD, etc. They convey to others that you have engaged in the training and experiences needed to acquire competency in a field of knowledge, and that you have demonstrated competency in that field of knowledge to a degree that a licensing body (state or national) allows you to practice the skills appropriate to that credential.
You can develop competency equivalent to a lot of the credentials in health care without getting credentialed, but woe betide you if you attempt to use that competency but don’t do it by the book with appropriate licensing. I am NOT suggesting that you try to practice without a license.
There are some people who argue, compellingly, that we have a right to self-treatment, and that the government monopoly on licensing creates a “cartel” that forces us to pay higher prices and forego other forms of treatment. Keep in mind that if you rely on the government or someone else to provide your health care, you get what they want you to have. You also get it only when they are willing and able to provide it.
Consider, for example, that you live in central Missouri and let’s say that the New Madrid earthquake fault lets loose, as some are saying it will soon. Roads, power grids and waterways are all inoperable. Buildings in cities are damaged, some even collapsing. Your neighborhood has houses down, too, and trees litter roadways.
Under these circumstances, waiting for credentialed providers to come rapidly will be misguided. You will be on your own. The federal government may take days to arrive with help: Look at what happened after Hurricane Katrina in New Orleans. You may not have the credentials, but I hope you have the competencies should you find yourself facing one of these events.
In fact, Dr. Peter Safar, one of the inventors of CPR, said 20 years ago that every household should be able to provide six basic rescue and first aid skills for itself in the event of an earthquake. Can yours?
Basic Rescue and First Aid Skills
1. Airway control
2. Mouth-to-mouth rescue breathing
3. External bleeding control by compression
4. Recovery position
5. Shock position
6. Rescue pull
A look at the 2003 earthquake in Bam, Iran showed that 90% of initial care that was provided to survivors was given by family and neighbors. It took on average 1 hour and 45 minutes for credentialed rescuers to arrive at the side of the quake victims. Unfortunately, 90% of these friends and families did nothing for their loved ones, which led many to suffer and some to die, needlessly.
So, when I recommend that you obtain competencies, I don’t expect that you get credentialed to practice them under normal circumstances in exchange for a fee. If you choose to do so, more power to you. I do hope that you at least obtain (and maintain) competencies to protect, maintain and restore health when the usual infrastructure, discussed in the introduction, is down.
Some writers (Aric McBay, Zachary Nowak, and Howard Kunstler, among others) think that things will soon be getting much worse. Rather than a discrete disaster, contained in time and scope, they foresee a gradual decline when we will be largely on our own in all areas needed to sustain life. Sending someone to find a professional with the needed credentials may be giving them a fool’s errand under those circumstances; now is the time to make sure you have as many competencies as you can acquire in order to replace those with the credentials.
Acquiring Knowledge and Skills
TRADITIONAL SOURCES ARE GREAT PLACES TO START ON YOUR JOURNEY TO SELF-SUFFICIENT health care competency. Some cost real money—colleges and tech schools, for example. Others, like the Red Cross and some government agencies, only cost a little more than the time and energy you invest in the course. In these austere economic times for most families, I’d suggest you optimize your use of inexpensive resources, so we’ll start there.
If you have not recently had first aid training, start by contacting your local Red Cross chapter. Most countries have offices, and larger countries will have them in several larger cites. Find out about taking a basic Red Cross First Aid course for about $50 or so. You can find out if you are motivated and interested enough to pursue further health care training; if you aren’t, you will at least know more than when you started and can avoid having to worry that a Bam-like scenario might occur to your family. These courses are taught by lay people, and you could also further your own skills by becoming an instructor if interested.
Speaking of families: Take yours with you. Most older kids can handle the curriculum, and there are specific courses for youth as well. Bring your friends and neighbors, too. This would be a gentle introduction for them to the idea of starting down the sustainability trail with you.
The Red Cross also teaches CPR and a number of other useful courses like wilderness first responder and pet first aid, and they have a wealth of useful materials on their websites for free download that will help with disaster preparedness in general, in addition to first aid.
As noted above, other countries have the Red Cross or Red Crescent. Check out the website for the International Committee of the Red Cross/ Crescent to find your local or national office. There are also a number of useful publications on the ICRC site available for free download.
English-speaking countries of the former British Empire also are likely to have an active St John Ambulance Association that teaches similar courses. Look at their website for your country.
Another potential source of low-cost training in the US is the American Heart Association, which teaches basic CPR and some first aid courses that may be helpful to the neophyte, including some online versions. Many of these are geared to be taught in the workplace; maybe you and some coworkers can see if your boss will host a course. Having this training for employees may lower the insurance cost for the business and get you started for free.
In the United States, the federal government used to teach a medical self-help course as part of the civil defense efforts in the Cold War era. This course, like the Cold War that spawned it, has faded into the past, but the US government still has agencies that teach useful courses, often online and for free. (You can still download the manuals for the medical self-help course from the Federation of American Scientists website for interesting, although somewhat dated, reading.)
Now, the Federal Emergency Management Agency (FEMA), the Department of Homeland Security (HLS) via its website, and the Department of Health and Human Services (HHS) are the repositories of the tradition of the Medical Self-Help Course.
FEMA offers a number of courses for free on its website. In addition, if you are willing to invest the time and effort, the Citizens’ Corps with its “Community Emergency Response Team” or CERT concept offers excellent training in disaster response, including disaster medical and stress response, as well as rescue and fire suppression. If you have a neighborhood, work or family-based group banding together for self-sufficiency, this would be an excellent starting point for a few dedicated individuals. Be aware, though, that the expectation is that you be available to the whole community in the event of a disaster.
Similarly, if you live in a small town or rural area, volunteering to be an EMT for the local volunteer fire or EMS agency may be an avenue to allow you to get some basic skills and supplies for only the cost of the time you devote to the training, plus the obligation of service you agree to when you join. You also will get to use your skills for real, and other advanced courses will open up to you. If you have more time and flexibility in your schedule and lifestyle, and money is a significant concern, CERT or volunteering are attractive options.
The next tier of training courses are offered to the public by private groups offering training in areas like “Wilderness EMT.” “Wilderness First Responder.” “tactical medicine” or “operational medicine.” Google searches for any of these terms will turn up a plethora of potential vendors. Many are offered with law enforcement and military contracts in mind, but most will take unaffiliated students as well. Be aware that caveat emptor applies: You may not get what you pay for, so make sure you find someone reputable that has been teaching for a while and is not just taking advantage of the recent trend. Keep in mind, too, that some of these are directed toward the hard-core survivalist type, and while the information presented may still be useful and accurate, the delivery style may not appeal to you.
Another similar avenue, and one that may be more applicable to a crash scenario as we’ll discuss later, is maritime medicine. Most of these courses last about 1 week. They are designed for those who truly live the title of this book as they cross big bodies of water without a physician or hospital nearby or easily reached. Talk about being self-reliant!
Both the land-based and maritime medicine courses cost more. You pay tuition, and may need to pay for supplies, above and beyond travel and lodging. Some are offered in nice resort locales, so you pay for that, too. As most courses run for several days, time away from home and work also factor into the burden. Again, if you have formed an intentional community to support neighborhood or family sustainability, this (like CERT) may be a place to send your key designated medical person.
Taking it to the next level, your local university, community college or technical college may offer EMT classes, nursing degrees and other advanced courses. In most cases, the expectation is that you are seeking the credential, not just competency in the subject. There will likely be less flexibility in terms of scheduling than with some of the courses listed above, and admissions requirements and cost become an issue as well. For instance, nursing schools will have prerequisites like chemistr y courses that will add to the time and financial commitment of this route. Because of this, you may want to consider this route for a member of your family or group with clearly demonstrated commitment and aptitude for the health care subject area.
Other avenues to obtain training are out there. Brainstorm and let your fingers do the walking, via the internet. Look at your local, state and county medical societies, Rotary and other service organizations, and your local hospital websites to see if they are hosting courses of interest.
A hospital or other organization in your area doing continuing education, may sometimes need “victims” who agree to act out the roll of the sick and injured. Easy now: They don’t require you to be sick or injured, but they may “moulage” you with makeup so you appear to have hideous injuries that disappear at the end of the day. When you volunteer, ask if you can audit the course in exchange for volunteering. Make it clear you are doing this for interest and edification only, and to make you a better victim, not as a back door to the credential. They may even be willing to let you have extra handouts or borrow course texts as well. Courses like Basic and Advanced Trauma Life Support fall into this realm.
Medical Auxiliary Model for Sustainable Health care
MEDICAL EDUCATION LEADING TO A DOCTORAL DEGREE IN MEDICINE (MD OR DO) IS A LONG road and is likely inaccessible to most people without causing significant upheaval in their current lives. In part this is due to the long preclinical or “basic science” phase of the first two years of medical school. Physician assistant school is shorter, only two years, but most PA programs require you to have a bachelor’s degree, and others that you also have experience in a health care field, before entry into training. Nurse practitioners need a nursing degree prior to entering NP school.
Authorities in Great Britain have recognized that there is a lot of basic science knowledge in medical education’s first two years that is never used by most physicians, according to the 2003 report “Tomorrow’s Doctors”. Public health and prevention, as well as listening and other communication skills are neglected. Still, there needs to be a foundation of some basic information like anatomy and physiology in order to maximize chances of accurate diagnosis and effective treatment.
Medical auxiliaries are trained for use in many parts of the world to work in places where physicians don’t or won’t work. (See Barefoot Doctors and Medical Auxiliaries.) They all share the common theme that they are non-physician clinicians trained over a shorter course than the 8-10 years required to train physicians, but they provide many of the same services as physicians.
TIP
Barefoot Doctors and Medical Auxiliaries
FOR MANY CENTURIES, NON-PHYSICIAN MEDICAL AUXILIARIES HAVE BEEN PROVIDING health care delivery in other countries, carrying out functions usually found under the scope of physician practice. In many cases, these auxiliaries have grown out of military practice, economic austerity or political upheaval. The current professions of nurse practitioner and physician assistant are the more modern, Western evolution of this concept.
Feldshers, perhaps the first recognizable auxiliaries, appeared in Europe in the 17th century. The concept probably originated in Germany, but flourished in the Russian military system under Peter the Great.
After training, the feldsher performed many physician functions, such as diagnosing and treating minor injuries and common illnesses. Many settled in rural areas of Russia and continued healthcare practice after ending service in the military; some even served in Alaska in the 1800s. The Soviet regime stopped training feldshers in the 1920s, but resumed it in 1937. Present day feldshers continue to serve in underserved areas of central Asia and some former Soviet Republics.
China trained more than 1.3 million barefoot doctors in the mid1960s when physician training, along with other university education, stalled China during Mao’s Cultural Revolution. These village-based auxiliaries received a 2-3 month training course; they learned by watching and listening to physicians. They also worked in hospital settings for additional supervision and training in Western medicine and the traditional Chinese arts of acupuncture and herb treatment. Initial training was interrupted by periods of military training and political indoctrination. Most worked in rural villages, applying public health measures to prevent common diseases.
The barefoot doctor was expected to get to know his co-workers and neighbors intimately. They were assigned to maintain immunization records, track the contraception methods used by women in the area, and arrange for consultation with a “real doctor” when necessary. Hygiene was another of the barefoot doctor’s specialties. This personal approach helped improve the health of a nation considered backward because of poor public health and nutrition.
China still has about a million rural barefoot doctors who care for the country’s hundreds of millions of rural farmers and peasants. Most of them have no formal medical education and little knowledge of Western medicine or how to use it. Mao’s system was dismantled in the 1980s and ’90s as China shifted the burden of paying for health care to individuals.
China’s health authorities are using video-based distance education and other non-traditional education techniques to improve the skill level of these auxiliaries, and plan to have all barefoot doctors certified to a higher standard of training by 2010.
The barefoot doctor concept has most recently been applied in India, where women are trained as barefoot doctors to provide maternal and child health services to underserved women in their villages.
NOTE
One final model is the clinical officer concept, which has been used successfully in post-colonial Africa for many years. Doctors are only rarely trained in Africa, and many who study abroad stay behind in the US or Europe after their training has been completed. To help meet the shortfall of doctors, clinical officers are used. These medical practitioners have up to three years of training after high school. With this training, they are able to examine and diagnose patients, do minor surgeries, attend to pregnant mothers and the like. In fact, the only thing they don’t really do is major surgery.
These experiences have shown that medical auxiliaries have a major role to play in health care delivery when physicians are not readily available, and that there are successful models outside the Western PA and NP credentials. These models can be applied to the village university concept to allow people to exercise their right to self-care.
In a gridcrash scenario, it makes sense to have continued access to health care even if access to physicians is not possible because of the situation. Having a level of skill approaching that of a medical auxiliary, built up slowly and as inexpensively as possible is one way of doing this.
As noted above, I am not suggesting you hang out your own shingle as a feldsher or clinical officer, as that would require that you take a recognized course to earn and be granted that credential, which may not even be recognized where you live.
Rather, I am suggesting that you develop the competencies that would allow you to function safely and effectively as the “barefoot doctor” for your “village” in the event that an earthquake, flood, war or similar widespread disaster disables the societal infrastructure.
Traditional and non-traditional routes all can be utilized to acquire the training needed to have the competency of a medical auxiliary, although you will have to work hard at innovative approaches in order to gain hands-on clinical experiences if you are not enrolled in a formal program. For these reasons, it may make more sense to ally yourself with someone working in health care already and appoint them your village doctor, as described below.
Non-traditional Approaches
NEW MEDIA, ESPECIALLY THE INTERNET, MAKE THE ACQUISITION OF KNOWLEDGE ONCE HELD closely by select professions much easier. Electronic courses via iTunes University for example, allow someone in the rural intermountain West to listen to lectures from Stanford, Cambridge and Yale, provided they have decent connectivity with the internet.
Books that are either out of print or that are not widely circulated, and may be prohibitively expensive for either reason, are now available for download via the web from a variety of sites. Many simply require that you register. You can download the classic books Where There is No Doctor and Where There is No Dentist, for example, among other useful volumes, at the Hesperian Foundation website just by registering your email.
A large number of the textbooks made available for free are relevant to a gridcrash scenario as many of them are collected for and directed at people who live in developing countries or serve in the military. Either of these situations closely approximates a post-crash scenario, so they are relevant.
There is a huge cache of health-related digital publications collected from various international and non-governmental organizations such as the World Health Organization and Doctors Without Borders. Finally, there is a wealth of information, primarily written for military health care providers, but useful nonetheless, for download from the Borden Institute.
If you are serious about becoming competent in gridcrash medicine so that you can care for yourself and those near and dear to you, it behooves you to become facile with accessing and using the medical resources available online.
Most of the resources you need will be available right from your home or work computer, but others like current medical, nursing and dental textbooks may require subscription services. In this case, you may find that a library at your local college or university has computer privileges you can use to access these materials, or you could also ask your local hospital if they have a library where you could access the material as well. Some larger public libraries may even subscribe to some of these services.
Many medical schools and large teaching hospitals have educational programs like community medical schools (where medical professionals give free lectures on medical subjects to the community at large) or Grand Rounds (weekly or monthly conferences given by subject-matter experts on wide-ranging medical and nursing topics). Surf the web to find out about what is available in your community.
Even agriculture colleges get in the act with some extension services having first aid, nutrition, health and disaster preparedness resources available at low or no cost.
Finally, you may be able to audit some health professions classes if you get permission from course directors. Find out if they need physical exam models, and they may let you listen in on the lectures teaching how these things are done; you may need to turn and cough, but they may even let you listen to lung and heart sounds with some basic coaching if you frame your request for information in the spirit of being a better model, as discussed above.
For hands-on experiences with procedures, you can make models for a number of procedures like inserting IVs, suturing wounds and the like; see Cheap Models for Medical Procedure Training. If you have a village university set up, some skills you need could be learned on other students as they learn on you. After all, countless nurses and doctors first practiced their skills on their classmates…
TIP
Cheap Models for Medical Procedure Training
INSERTION OF INTRAVENOUS CATHETERS (IVs) IN ORDER TO GIVE A PERSON FLUIDS and medication is a basic nursing or medical technician-level procedure that many people involved in preparation activities focus on, with good reason. In the event of any number of illnesses or injuries that result in blood or fluid loss, the ability to resuscitate someone with IV fluid is potentially lifesaving. Medications may also need to be given intravenously, especially to unconscious patients or those with nausea and vomiting.
Another important activity, if you look at the lists of supplies and equipment recommended by preparedness-types, is suturing for repair of lacerations. We can anticipate that in an era when we are using manual tools or doing chores with our hands we will see more wounds, so this, too is a reasonable skill to acquire.
How can you learn how to do these things without having access to live patients? Models have been used for many years to provide this type of practice and training. When you couple old-school models with newer technology like YouTube and iTunes, you can add tremendously to the effectiveness of your Village University. There are lots of other models out there, and more are being developed all the time. If you have a particular skill you want to learn, look online to find potential models to help you master your art.
Gelatin IV Model
Most nurses, physicians and medical technicians recall the first time they started an IV on a living person. Many of us “got” to practice on our classmates, and have them practice on us, often with only a quick look at a video or after watching a live demo by the instructor. There may have also been a model provided. Unfortunately, these models were not very realistic: plastic arms that had track marks from so many previous sticks, and often fluid was seen leaking from their fake veins.
Advances in simulation for medical training have resulted in life-sized computer controlled manikins, but they are very expensive, making them unrealistic for small groups like a sustainability group.
A few years ago, Dr. Susan Stroud, one of my colleagues at the University of Utah Medical School, came up with an inexpensive, simple solution to the problem of training medical students to start IVs without having to bruise each other’s arms and their own egos.
Dr. Stroud looked for models to help train her students, and finding no inexpensive model, made her own. Thus was the gelatin intravenous model (GIM) born. The GIM is easy to build out of readily available (and cheap) materials: a baking pan, real (not instant) gelatin and Penrose-type surgical drains tied off at the ends with “blood” inside. The GIM does not look like a junkie after a party: Its holes are self-sealing, preventing “bleeding” from the gelatin-encased “vein.” Finally, the GIM responds more like human flesh than some of the more expensive, commercially made IV trainers. The gelatin gives a boggy, springy feel like real tissue under pressure, and the “veins” can roll like real ones.
At Yale University, a group of paramedic educators compared the GIM with traditional rubber arms for training neophytes. They found that the GIM is a viable alternative to training IV sticks using a human model and saves the trainees pain and pressure in learning this invasive procedure.
Now, many medical training programs use adjusted recipes to train resident physicians to put in specialized central IV lines or how to place an IV using ultrasound guidance. Other groups have replaced the flat baking pan with round tubular containers that they remove after the gelatin has set; this more accurately recreates the shapes of arms and legs.
Pigs Feet for Sewing?
Perhaps nothing is more de rigueur for the survivalist medic than to have a basic suture set. Knowing how to use it, though, is not always disclosed by proponents of having one of these kits available.
Most medical schools in the US nowadays seem to have at least one club- or curriculum-based lab that teaches interested students how to suture using pigs feet. As a medical educator, I too have made the trek to the butchers and endured the questioning looks as I picked up a few dozen fresh pigs feet in order to be able to teach suturing techniques to my charges.
The benefit of this model is that pigs have thick skin, and you can create all manner of lacerations on their feet with a sharp scalpel. Then, you can sew to your heart’s delight: Simple interrupted, simple running, mattress and corner stitches can all be practiced. You can also become a pro at basics like instrument ties, one method of securing the stitch with a sturdy knot.
One drawback of any model, such as the GIM or pig’s feet, is that you can easily acquire the skills, but you will also need the cognitive background to allow you to apply them appropriately. One of my teachers in medical school used to say he could train a monkey how to do surgery, but learning when to do it took his human trainees many years. A good medical auxiliary will have both cognitive and procedural skills; don’t overemphasize one set at the expense of the other.
The Village University: Learning the Skills You Need
PERHAPS THE LEAST CONVENTIONAL METHOD OF HELPING YOU ACQUIRE KNOWLEDGE IN GRIDCRASH medicine is the village university concept.
This book focuses on sustainability and helping you take care of yourself. Self-reliance only goes so far, though, as no one is an island. We can’t count on being able to weather stormy times completely alone, so we need to look at ways to build relationships in our local communities that will help in our quest for sustainability.
In our post-industrial age, we have replaced community (and the compromise and relationships it requires) with technology. Like so many other areas of life, we don’t often rely on our neighbors to provide assistance, nor they us. We seek a lifestyle that allows us to feed, clothe, shelter, entertain and care for ourselves “independently.” In so doing we make ourselves dependent on technology, especially on cheap, readily available resources. We have seen that there is a cost to these cheap resources in that their use causes rippling impacts on the world’s people and ecology.
In striving to lead a more sustainable life, you have to start with small, individual steps. In the end, however, community sustainability should be your goal: finding or forming a group of individuals that rely on each other more than on technology. The group will have to be interdependent within its walls, but ideally minimally dependent on external inputs.
What does it mean to be interdependent? In a gridcrash scenario, there are many activities needed daily for living that require special knowledge and skills. As much as we might idealize the image of the lone family or person out their making it alone, the breadth and depth of these needs are too much for any one person to acquire. Thus, we are best served by interdependence and a sensible division of specialized labor.
In fact, unlike the sustainability pyramid built on energy I described in the first chapter, I envision a different pyramid based on knowledge: At the base are simple skills and knowledge held by every mature member of the group, while further up, more specialized knowledge and skills are held by fewer people. There will be multiple pyramids for each of the areas of activity needed for sustainability: food procurement and storage, transportation, energy, shelter and health, for example.
Because of this, you may choose not to try to acquire advanced skills in health care for use after gridcrash, leaving that level of sophistication to others. Still, you must be able to do the basics in order to minimize your own illnesses and injury, as well as limiting the impact of those adversities on your group. You might be called on to help with basic care of others as well, just as you might consult someone else’s superior knowledge and abilities in guiding activities like gardening or carpentry while doing the “grunt work” yourself.
The point is, within your group you should seek to identify someone most likely to be able to learn and apply knowledge and a set of skills to restore others to health. Others in the group may have some special training in medicine but won’t emphasize it. If you are lucky, the lead person will already be trained and experienced: a physician, physician assistant or nurse practitioner, for example. Everyone has special skills and interests from work and hobbies; capitalize on these in choosing and allocating specialties within your group.
One way to spread skills is through the concept of a village university. This idea was popularized by three Scandinavian physicians working with victims of violence, especially landmine blasts, in the developing world. Basically, you bring in experts who then train select “village medics” within a community. After the initial training, the newly minted village medics train “helpers” who are deputized to help the medics. Often the helpers are from smaller collections of families living away from the main village.
You probably live in a neighborhood with a rich diversity of talents. If your neighbors are not interested in forming a sustainability group, maybe you can form one based on extended family and friends, coworkers, church members or others. If you live in a relatively large town or city, there is probably a peak oil or sustainability group already; you can go and maybe find like-minded members to help. Just do a web search with terms like “peak oil” or sustainability , plus the name of your town or city, and you are likely to find at least one such group.
Once you find or form your group, look at everyone’s job and educational backgrounds. Then, think creatively: The insurance salesman may have been a medic in the military. The dentist or veterinarian will have a tremendous head start in learning more about human medicine. Most of those who have been to college may have taken classes in several fields before settling on a major or career direction; some may have changed careers after training in a health profession.
As you assemble a roster of knowledge and skills, keep in mind that some folks will have a job in one health field, but the training and experience acquired in pursuit and practice of their craft will stand them in good stead for training helpers in other areas. Trained health professionals can build upon their scope of practice and educational background to teach related areas.
Nurses, for example, do physical exams on patients and can teach basic assessment skills. Pharmacists know about drugs of course, but by necessity also know about microbiology and infectious diseases. Some know a lot about issues like treating patients after exposure to atomic, chemical or biological warfare. Other health care workers could teach skills relevant to their job; a physical therapist could be very useful in teaching basic musculoskeletal anatomy, orthopedic and neurologic exams, and treatment of minor sprains, strains and fractures. These are just a few examples: Think creatively! You should encourage both building on old skills and using them to train other members of your community. Physicians are only really needed to train people in the most specialized topics.
If you don’t have someone already trained as a health care professional in your group, you could sponsor someone to go through the training needed, like a medical auxiliary, starting with courses at the Red Cross and the like and gradually expanding to include CERT training or formal college-level courses. Many universities allow the option of auditing courses for adults at reduced cost; some are even free if you don’t take the exams (and who would want to?).
The reality is that most folks don’t have training or experience in taking care of sick and injured people. Most of the care required, though, is nursing care. A basic course in first-aid and basic safe nursing care, plus one in hygiene, will form the underpinning of further education, and will meet most needs. It forms the base of your health care sustainability pyramid.
Advanced courses in theory like physiology and pharmacology are nice, but may be a bit esoteric for a group trying to develop its own care team. If possible, your group should recruit a training nurse to help in this endeavor.
The only educational prerequisite for trainees is that they be interested, literate and numerate. Take advantage of free, public access materials like iTunesU and other resources found on the internet (see appendix) as your texts to minimize cost. You must make up a schedule that is realistic within your other life demands, with attainable goals. The curriculum should be focused on practical applications, covering essential materials using simple, straightforward terminology. A suggested curriculum is Standards of Training, Certification and Watchkeeping for Seafarers, required by the Coast Guard for the “Medical Person-in-Charge” (MPIC) providing health care on ocean-going vessels. An example of the items covered, which encompass more than simple bandage-and-splint first aid, is seen here.
Topics in the curriculum of the MPIC include:
• Suturing & Wound Care
• Intravenous Fluid Therapy
• Medication Administration & Injections
• Pain Management
• Infectious Diseases
• Behavioral Emergencies
• Eye, Ear, Nose & Throat
• Nasogastric Tubes & Urinary Catheterization
• Altered Mental States
• OB/GYN & Infant Care
• Complications of Drug & Alcohol Use
• Poisoning & Overdoses
• Legal Issues
• Communication & Documentation
• Anatomy
• Patient Assessment
• Respiratory Emergencies
• Cardiovascular Emergencies
• Defibrillation (AED) and CPR
• Bleeding & Shock
• Burns
• Environmental Emergencies
• Spinal Injuries
• Lifting & Moving Injured or Ill Patients
Clearly, this is a very comprehensive skill sets that (of necessity for seafarers) goes well beyond first aid. Whether you form a sustainability group or choose to go it more or less alone, you should strive to have someone trained at least to this level.
Conclusion: Knowledge has been called power. Perhaps one reason for this is the realization that knowledge cannot be taken away. Time and biology can degrade knowledge slowly, but circumstances cannot take it from you once it has been acquired. Through recurrent training and practice you can reduce the effects of time on perishable knowledge. The physical and emotional fitness measures discussed in this book can keep your mind and body in optimal shape, helping to preserve your knowledge.
Gridcrash could potentially take many things away from you and your family, your community, region or nation. It may affect the entire world, like petrocollapse or climate change. In any case, the knowledge you develop prior to any crash will be useful before and after the crash. Rely on others to help you, as they will rely on you to make your family, neighborhood and community self-reliant. Devote time to learning what to do now, so you will have the skills when the time comes that you need them.
As we will talk about in the next section, what you know and how you act are at least as important as what you have.
Make Your Spirit Ready
EXPERTS HAVE TOLD US (AND EXPERIENCE HAS CONFIRMED) TIME AND TIME AGAIN THAT WHAT counts most in survival situations is not what you have, but how you think and behave. Although most of the work done in the psychological determinants of survival focuses on acute events like being lost in the wilderness, engaged in physical combat or held as a captive, we will focus on this body of work in light of gridcrash, as your spirit will bear heavily on your post-gridcrash life.
You are doing a lot to bolster your survival psychology just by reading this book. We know that people who have anticipated a bad event and thought about how it might affect them (and how they’d act in return) improve their odds of survival, even if they do nothing else. Surprise, and feeling overwhelmed because of it, can make you panic. Panic prevents clear thought and purposeful action, and it sets off a chain reaction that can lead you to do foolish things, or to do nothing. In a disaster, either course could be harmful.
What you are doing by reading this book and performing related tasks amounts to psychological stress inoculation. This is the idea of getting your emotional self ready for bad events. It is thus crucial for helping you to help yourself and others in bad times. This is true no matter how long those bad times may last: a minute, a day, or a year. Your forethought is a major element of this inoculation. Just like getting physically fit helps ready your body for physical rigors, so too does getting yourself emotionally fit make you ready for emotional stress.
The military and police as well as other first responders use stress inoculation. The goal of this technique is to expose people at risk for life-threatening danger to training that is so realistic that they are not overwhelmed by events when they occur in the real world. Even a “pre-briefing” before going into danger has been shown to help: Telling people about to be engulfed in a situation how it sounds, smells, looks and feels when they enter the fray has been shown to make them less prone to panic and allows them to be more effective.
In making preparations to safeguard your health and the health of those close to you, you are engaged in a form of stress inoculation. Later, we will talk about how to do medical threat assessments so you have an idea of what kind of emergencies you may face; others have written extensively about the wide variety of possible gridcrash scenarios and other disasters we may face. Taken together, this information can allow you to prepare for many eventualities. This planning, plus acquiring useful knowledge, skills and attitudes, will form the majority of the stress inoculation you need.
Stress inoculation may also help to reduce your vulnerability to the high rates of depression, substance abuse and PTSD found to occur after disasters like Hurricanes Andrew and Katrina. The World Health Organization defines a disaster as an event that overwhelms the coping capacity of a community. The techniques described here can help you bolster your coping capacity.
Additionally, there are other tools that have been used consistently by survivors that you should learn about now. Then, try to practice applying them in your mind in advance of trying times when you’ll need them most. They are tools that could be useful in times other than just after gridcrash; they are applicable to any stressful and/or dangerous time you or your loved ones may encounter.
Traits of Survivors
SINCE THE SECOND WORLD WAR, A LOT HAS BEEN WRITTEN ABOUT SURVIVOR TRAITS THAT are less often found in those who don’t survive similar conditions or circumstances. One classic arena in which these observations were made was in the POW camps of World War Two. Although the austere conditions in these camps were often due to a desire on the part of their captors to punish or torture prisoners, we can still learn a lot from the circumstances found there and the coping mechanisms used by some to help them survive.
Emotional stressors reported to affect these prisoners included shock at finding themselves in their new situation, depression in reaction to suddenly being in that situation, feelings of desertion or abandonment by their countrymen, uncertainty about day-to-day survival and how long they would be in their situation, and loss of self-respect. These psychological burdens compounded the physical deprivations forced upon them by hunger, exhaustion, cold, boredom and squalor.
According to the Oxford Concise Dictionary of English Etymology, disaster is derived from the Latin words for “unfavorable aspect of a star” and hails from a time when a person’s star in the heavens protected them from bad events. As noted above, disasters can so overwhelm coping skills that it seems even the stars are against us. The principal psychological asset attributed to survivors is the nebulous “will” to survive or to live.
In the context of disasters like internment in a POW camp, the survivors, though bowed at times, did not wallow in the present. Instead, they refused to feel like prisoners, thinking of themselves as something else to support their will: as a father, a husband, an American or some other personal ideal. Through this technique, the survivors made conscious decisions to ignore or overlook their current straits and focus on the future. The past was their buttress of emotional support, not a burdensome reminder of better times. This view to the future was balanced and optimistic: A well-controlled “fantasy life” could be used to advantage. The exact nature of the diversion from the present was not so important and, when supported with hard work and courage, was not unrealistic or naive.
For the prisoners, this meant that they recited literature and poetry recalled from youth, taught and learned new foreign languages or had contests solving complex math problems, even at the risk of provoking the ire of their captors who tried to minimize contact among the prisoners.
Other experiences in these settings showed that physical illness and depression about circumstance became partners in a “negative feedback loop” where physical problems made emotional resistance weaken, allowing a worsening of physical illness and so on. Those who reacted realistically but optimistically and willfully against illness did better than those who seemed to give in.
Your Psychological Survival Kit
HOW DO PEOPLE REACT TO CRISES? THERE IS AN OLD SAYING THAT GOES ALONG THE LINE “There are some who make things happen, some who watch things happen and some who wonder what happened.”
Studies into the behavior of people suddenly overcome by catastrophe show that 75% of these people are stunned and confused. At best, they resort to automatic behaviors and reflex action. Another 10% or so panic and give in to useless, inappropriate behaviors like screaming and crying or apathy. These two groups are the ones watching or wondering about events.
Only about 15% prove to be able to respond relatively calmly and are able to carry out useful activity. This small group makes things happen. Stress inoculation and a strong will to live may help keep you in, or move you into, this desirable demographic. . What other methods can be used to maximize your chances during catastrophe?
Journalist Laurence Gonzalez has written several popular books about the psychology of survival. His book Deep Survival describes how survival, regardless of the threat, can force upon us a journey. Those who survive seem to adopt a Zen-like acceptance of the journey and find a way to, if not enjoy it, at least not to fight it. He lists a number of patterns that survivors demonstrate in how they think and act. These patterns are not just directed towards outdoor recreators who may be lost and injured, and they can be condensed into a simple mnemonic device.
If you choose, you will learn (or may already know) that emergency care providers utilize mnemonics to help them recall critical actions in dire circumstances. A key mnemonic for these EMTs, nurses and physicians is ABC: Airway, Breathing and Circulation are priority functions that must be protected or restored.
For the survivor, the mnemonic ABCDEFG covers the keys:
A = Admission
B = Belief
C = Control
D = Discipline
E = Effort
F = Fun
G = Gift
These seven items, along with a strong will to live, will help maximize your chance of bringing yourself and those around you safely through any future shifts.
Gonzalez points out that survivors, ironically, go through the same five stages of grieving as patients given a terminal diagnosis, as described by Elizabeth Kübler-Ross. Denial, the first of these stages, can be deadly if it causes panic, inaction or the wrong action. Survivors move rapidly through denial with their admission of the difficulty of their circumstance to themselves. This does not mean they give in to hopelessness.
Psychologist John Leach has a name for this denial: incredulity response. Sometimes events like the building damage and collapse in the events of 9/11 are so overwhelming and out of the ordinary that some people simply can’t or don’t believe what they’re seeing. They react with what is known as “normalcy bias” by trying to shoehorn the unusual events into the normal run of life. This often leads people to underestimate the danger they face up to the end, or at least until things have gotten so bad that they are in a real pinch. Some of us have seen how this denial occurs in those patients with a lump on the skin that grows and eventually disfigures them before they seek care.
Cancer patients and the doctors and others who care for them understand the power of naming. Learning that the nagging feeling you have is in fact due to cancer, although potentially devastating news, can in fact be liberating. Now, you have a focus for your emotions and your actions. What matters now is how you respond, not the event. The event has occurred and you alone determine how it will affect you.
Belief in themselves prevents survivors from being swallowed by despair. Not, as we saw with POWs, a pie-in-the-sky magical thinking, but capitalizing on self-knowledge of their abilities and their belief in the possible.
We are constantly regaled with stories of superhuman efforts that result in survival under staggering travails: people surviving on rainwater and a few fish for months at sea, or crawling deliriously for miles on injured limbs in freezing cold. All of these sagas share a dogged belief by those who live to tell them. that they will survive.
Many survivors describe how, after they have admitted to themselves the gravity of their position, they became either afraid or angry, or both. There must be Control of that anger and fear; indeed, once controlled, these emotions can be used productively as motivators. The adrenaline released in a “fright, flight or fight” situation will help you see and hear threats around you, and give you increased physical capacity, among other effects. Similarly, the anger or fear you feel, if directed appropriately, can allow you to perform better.
World War II prisoners described how they applied psychological first aid when they used “tough love” to keep their fellow detainees alive: They often used “systematic prodding” on those who seemed to be giving up. The anger thus induced in the subjects of the prodding frequently turned them around. (See Psychological First Aid.)
TIP
Psychological First Aid
PSYCHOLOGICAL FIRST AID (PFA, ALSO CALLED MENTAL HEALTH FIRST AID) IS A TOOL first developed back in the “Duck and Cover” days of the Cold War and Civil Defense. PFA might be needed anywhere traditional “physical” first aid is required.
Beginning in 1954, the American Psychiatric Association wanted the lay public to have the ability to help themselves, plus their loved ones and neighbors, to respond to the psychological consequences of disasters, including global thermonuclear war. The goal was to minimize the disaster syndrome, which afflicts so many after sudden devastation and prevents useful action. Another goal is to reduce feelings of helplessness that might lead to PTSD or depression.
PFA is not designed to turn you into a counselor or a psychiatrist. It is a collection of tools to help you provide compassion and support to reduce the emotional impact of a stressful life event. This is something we all do to a degree for ourselves and loved ones on almost a daily basis.
Most people who live through a disaster are affected emotionally by the event, but are not in need formal psychological help because of those effects. What people do need is protection from further harm, plus comfort, support and information. For some, protection means not having to relive the experience by recounting it, though others may find it supportive to talk about the events with other survivors. In any event, becoming physically “worked up” by talking about the event can cause further harm and should be avoided.
Next, comfort and support are provided. For most cases, this means reunification with loved ones, plus shelter, warmth, nutrition and medical support (if needed). Allowing “venting” of emotions may also help; some folks just want to know that someone is listening. The person giving PFA should appear confident, concerned and compassionate. Some survivors may find that channeling energy into productive activity is most helpful for their recovery from disaster emotionally, not to mention practically.
Finally, most survivors want information: about their loved ones and neighbors affected by the disaster, about the future and the like. This should be reliable information only, not rumor or speculation.
The last tenet of PFA that must be remembered is that, just like in first aid given for illness or injury, some folks will need professional help. Those with dysfunction (who can’t eat, sleep, talk or care for themselves or loved ones, for example) are those most at risk for PTSD and will benefit from referral to professional help as soon as it is available.
See “
Psychological First Aid for First Responders” available at
mentalhealth.samhsa.gov/disasterrelief/pubs/manemotion.asp for more information on disaster psychology services. There is a free downloadable course manual covering mental health first aid available to interested readers for more PFA information; see the resources at the end of the book.
Discipline-led action must become the product of your use of Admission, Belief and Control: organized, planned and deliberate efforts to allow you to overcome the survival situation. Hikers who are lost but uninjured often succumb to exhaustion and cold from denial and panic-driven efforts to find a way out. Survivors recognize the situation, know that they are likely to be rescued, control their emotions and set about to build shelter and a fire to protect themselves.
Sometimes discipline takes the form of active passiveness. Active passiveness is deliberate inaction: “Don’t just do something, stand there.” This passiveness may last just for a blink—only pausing to check where the fire is, then going in the direction needed to get away. Those who don’t take this pause may paradoxically head toward the threat.
Other times, active passiveness is a state of mind where you force yourself simply to be present without responding emotionally to the circumstance. This is part of the idea of a Zen-like state, accepting fate with equanimity.
Once you have your plan, you must apply Effort to make the plan into reality. This is a key component of making your belief in yourself real, rather than mythical. Cancer survivors describe learning to value the pain they endured in their treatments, embracing it as the effort required to get better. Darrell Stingley, a New England Patriot’s receiver paralyzed in a game reportedly spoke to this when he said “Pain is your friend” because it signaled a welcome return of sensation as he went through his rehab.
Gridcrash may not sound like a good time to any sane person, yet survivors have shown that having Fun is essential to keeping going. Small victories, pleasant surroundings, and finding humor in the absurdity of the situation, among other treats, provide the source of that fun for countless survivors.
Finally, as another part of the Zen-like journey, comes the Gift. Survivors recognize that they will learn much about themselves from their triumph over each obstacle. That is treated as a gift in and of itself. Others focus, despite their trial, on the well-being of others: Helping those with you, and thinking of loved ones apart from you, can take the focus away from your burden and help boost morale.
Leach, in his book Survival Psychology, describes how caregivers in disasters have higher rates of survival, as they did in the concentration camps and Gulags of Europe in the recent past; perhaps this is in part due to their focus on making things a little better for others.
Conclusion:
Austere conditions due to economic collapse, natural disaster, or any number of other problems could put us into circumstances similar to those described above.
Surviving and flourishing in any situation requires not only tools, supplies, physical ability and cognitive knowledge, but also (and perhaps most crucially) attitude. Your preparations in other “meatier” or more practical realms like fitness and medical training are essential; these will help your psychological preparation as well. Carrying a strong will to live, plus keeping a psychological survival kit containing the ABCs of a strong survival mindset, will take you a long way under any shift in circumstances the future may bring your way. ●