A LARGE VARIETY OF DRUGS are known to affect orgasm in positive or negative ways. In many cases, the reports of positive effects are anecdotal or have been described in uncontrolled (that is, not scientifically rigorous) studies using a small number of individuals. So we need to take some claims about the positive effects of certain drugs with a grain of salt. However, there is reliable information, based on sound scientific studies, about the effect on orgasm of several drugs, particularly prescription drugs that are used to treat sexually and non-sexually related health problems. We will do our best to explain what is known about the effects of many drugs, legal and illegal, on orgasm. It’s important to keep in mind that a lot of drugs can have serious side effects and their use should not be considered lightly.
The positive effect of steroids, particularly testosterone, on orgasm in both men and women has been established in many well-controlled studies. Testosterone is found to be effective for individuals with low levels of testosterone in their bloodstream, usually older men or post-menopausal women. Its possible aphrodisiac effect on individuals who have normal levels of steroids produced by their gonads (testicles and ovaries) remains controversial.
Yohimbine has for many years had the reputation of being an aphrodisiac, and this has been validated in several studies. This drug counteracts several aspects of sexual disorders. Initially, yohimbine was used to facilitate or prolong penile erection, but it was later found to improve sexual arousal and orgasm as well. It acts mainly by increasing the release of noradrenaline (also called norepinephrine), a neurotransmitter in the brain and nerves that is involved in various aspects of sexual activity.
We need to get a bit technical here to explain how yohimbine works, but this information is also useful in understanding the actions of some other drugs. Neurons (nerve cells) that produce noradrenaline have a particular type of receptor, called an “autoreceptor,” that recognizes and responds specifically to the same neurotransmitter that the cell produces. In this case, neurons that produce and dispense noradrenaline contain autoreceptors (called alpha-2 receptors) on their surface that respond to their own or other neurons’ released noradrenaline by slowing down the further release of their own noradenaline. This is a process called “negative feedback.” It’s similar to how a thermostat works, responding to the increased temperature in the room by turning off the source of heat—the furnace. Yohimbine has its effect by blocking the action of noradrenaline on the neuron’s autoreceptor (much like a key that breaks off in a lock so that another key can’t be inserted into the lock). This results in the continued release of noradrenaline from the neuron, and this increased noradrenaline has an orgasm-stimulating effect. Again using the analogy of the thermostat, it’s as if the thermostat is blocked from sensing when the room gets warm, so it fails to shut off the furnace, and the room gets hotter.
Yohimbine is effective when taken two to four hours before sexual activity. An effective dose of yohimbine to counteract orgasmic dysfunction in men is about twenty milligrams. At this dose, side effects seem minor. There is insufficient comparable information for women.
Another neurotransmitter that has a stimulating effect on orgasm is dopamine. Drugs such as amphetamine that stimulate the release of dopamine can stimulate or prolong orgasm. However, the undesirable side effects of amphetamine, particularly serious paranoid schizophrenic symptoms, prevent its medical use for the treatment of sexual disorders.
Cocaine has a similar effect of increasing the levels of dopamine in specific brain regions, thereby stimulating orgasm in men and women. Cocaine blocks the reabsorption (reuptake) of dopamine by the neurons that released it, keeping it available to neighboring neurons—which increases the stimulatory effect of the dopamine. Because cocaine is highly addictive, its use as a treatment for sexual disorders is not recommended.
The antidepressant drugs known as selective serotonin reuptake inhibitors (SSRIs) have a negative effect on orgasm and other sexual functions. Since the nineteenth century, depression has been known to be associated with sexual disorders, and it was logical to think that an improvement in the depressive illness would result in improvement of sexual function. So, it’s ironic that a class of drugs that reduces the effects of depression creates sexual disorders as a side effect. Recent studies suggest that 90 percent of patients taking antidepressants that increase serotonin levels—which is how SSRIs work—experience sexual disorders. The SSRIs act by interfering with the reuptake of serotonin into the serotonin-producing neurons, thereby prolonging the action of serotonin on neighboring neurons. Some recent studies that examine specific aspects of sexual disorders in patients treated for major depression with SSRIs and other medications show that men are more likely than women to have problems experiencing orgasms.
The first effective antidepressants introduced into clinical practice were the MAO inhibitors (monoamine oxidase inhibitors). Monoamine oxidase is an enzyme that breaks down and inactivates the class of neurotransmitters known as the monoamines. These include noradrenaline, dopamine, and serotonin. By inhibiting this breakdown, MAO inhibitors increase the levels of these three monoamines in the brain. Although dopamine and noradrenaline, as we’ve seen, tend to stimulate orgasm, these effects are counteracted by the increased levels of serotonin, which has an overriding inhibitory effect on sexual responses.
Fortunately, several new antidepressant drugs avoid the side effect of sexual disorders, and some of them even enhance sexual responses. Studies show particularly consistent results in enhancing orgasm with the use of bupropion. In addition, a new generation of antidepressants, such as moclobemide, which are known as “reversible inhibitors of MAO,” are reported to strongly stimulate orgasm in some individuals.
Another class of frequently prescribed drugs that depress sexual activity is the antipsychotics, which are used for treating schizophrenia and a particular form of depression known as malignant depression. These were among the first drugs that were recognized to impair or prevent orgasm in men and women.
More recent, “atypical” antipsychotics such as clozapine, which act on several types of neurotransmitter receptors other than the dopamine receptor, apparently have a less negative effect on orgasm and sexual activity than other antipsychotics.
There is a widespread belief that certain recreational stimulant drugs enhance or alter sexual pleasure and orgasm. Many marijuana users claim they have more prolonged, intense, and hence more rewarding orgasms than those experienced without the drug. These marijuana-related changes in the quality of orgasm, rather than changes in frequency or in ease of stimulation, are difficult to evaluate. Some well-controlled studies do report an increase in awareness of muscular contractions in the genital area during orgasm. Perhaps it’s more significant, however, that a recent analysis of sexual disorders resulting from drug use in 3,004 men and women found that chronic use of marijuana was significantly associated with anorgasmia.
The drug Ecstasy, a derivative of amphetamine, is considered to affect social interactions and sexual response. Some studies were designed to test the reported aphrodisiac effects of this drug. Sexual desire was increased in most men and women taking Ecstasy, although, paradoxically, erectile dysfunction was noted in 40 percent of the men. Some Ecstasy users claim to experience a different, more rewarding type of orgasm, but this effect is difficult to evaluate objectively.
A variety of drugs that have the common property of depressing the central nervous system (brain and spinal cord), including alcohol, opiates, barbiturates, and benzodiazepines (such as diazepam), have at times been described as reducing social inhibitions to sexual intercourse. In some cases, when sexual activity is inhibited by high levels of anxiety, moderate amounts of alcohol or diazepam are found to facilitate sexual activity, but in general these drugs impair orgasm.
UNFORTUNATELY, THERE IS VERY limited scientific research on orgasms while sleeping. One question that is raised is whether the person experiencing the orgasm was in fact making contact between his or her genitals and the bed or sheets. However, there is good reason to believe that orgasms while sleeping are not, in fact, the result of genital stimulation but instead are created in the brain. For example, men and women with spinal cord injuries—with no nerve connections between their external genitals and their brain—are known to experience orgasms while asleep.
In a rare, and lucky, case in a laboratory study, researchers made physiological measurements while a woman had an orgasm during a dream. When she awoke, the woman described the dream and the orgasm she had experienced. The researchers reported that the rate of blood flow to her vagina, her heart rate, and her respiration rate all increased during the dream. Specifically, her heart rate increased from 50 to 100 beats per minute, her respiration rate increased from 12 to 22 breaths per minute, and she had a “very marked” increase in vaginal blood flow. Her vagina showed cyclic episodes of engorgement with blood during her REM (rapid eye movement) sleep stages. In sleep studies, the greater ease of measuring penile erection than vaginal blood flow has resulted in research showing that men typically have penile engorgement during 95 percent of REM sleep stages.
It is likely, based on all these observations and other, less scientific reports, that orgasms during sleep are not a response to genital stimulation, but rather are the result of brain activity. In other words, the physiological responses seem not to be “reflexive” responses to genital stimulation but to be generated intrinsically by the brain. So, it seems that during sleep, the brain can behave in a way that turns on all the systems involved in the experience of orgasm.
THE ANSWER DEPENDS LARGELY on what we mean by “happens.” Everything a person feels is sensed in the brain. So, orgasms are felt in the brain, and to some that means they happen in the brain. But the process of orgasm involves virtually every body system. Looked at in this way, the brain is not the only place where orgasms “happen,” but rather, the brain is the conductor of the orgasmic orchestra.
In recent years, technology has made it possible to directly observe three-dimensional activity in the human brain. This has led to an explosion of research that correlates activity in specific brain regions with people’s perceptions and feelings. Some investigators have begun to analyze the parts of the brain that are activated by genital stimulation and orgasm, through the use of a technology called “functional magnetic resonance imaging,” or functional MRI, or simply fMRI. All the major regions of the brain become activated during orgasm. Perhaps this is not surprising, because many different body systems are activated during orgasm—systems that are under the influence of the brain. The muscles of the arms, legs, trunk, face, and genitals become more active, as do the muscles that produce increased heart rate, blood pressure, uterine contractions, and dilation of the pupils. Sweating and the secretion of hormones (including oxytocin and prolactin) increase, while arousal and pleasurable feelings intensify. Using fMRI, researchers can visualize these events in the brain. If you compare the fMRIs of a brain before orgasm and a brain during orgasm, it’s like comparing a Christmas tree with just a few scattered light bulbs and one festooned with many strings of lights. With this imaging technology, researchers are starting to chart the effects of orgasm on the brain.
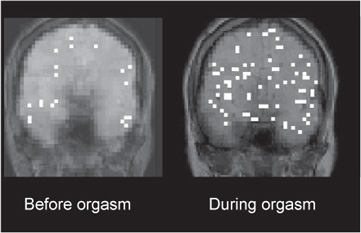
Images of brain activity recorded by fMRI (functional magnetic resonance imaging). The left image is of a woman’s brain during the first minute of vaginal self-stimulation. The image on the right shows the same brain several minutes later, during orgasm. The much greater brain activity during orgasm is revealed by the regions covered with white squares.
ACCORDING TO CHRISTINE MCGINN, who is one of the few surgeons in the United States who performs this type of surgery, some specific terminology is preferred. The surgery is referred to as “gender-confirming” surgery or “genital reassignment.” Transmen refers to persons who undergo female-to-male surgery, and transwomen to persons who undergo male-to-female surgery.
For transwomen, the standard surgery is “penile inversion vaginoplasty.” The surgery re-forms the main components of the penis into female proportions. The penile glans (the cone-shaped tip) is surgically reduced in size and sutured into position as a sensitive clitoris. Although many of its nerve endings are removed during this step, orgasmic ability remains intact. The testicles and erectile tissue of the penis are removed. The penile skin is left with an intact blood and nerve supply and is used to create the labia, clitoral hood, and vaginal wall. The vagina is created by surgically opening a space between the scrotum and the rectum and placing the inverted penile skin-tube within this space. The penile skin-tube is further lengthened by using a skin graft from the scrotum. The newly formed vagina ends blindly without a cervix and is located between the prostate and rectum. The prostate in transwomen remains in place after surgery and is an important source for orgasm, much like the G spot. Transwomen frequently report a decrease in desire as well as a change in character of their orgasms with estrogenic hormone therapy.
For transmen, there are two types of genital surgery: phalloplasty and metoidioplasty. Due to exclusion policies of many U.S. health insurance companies, the costly phalloplasty is not routinely performed in the United States; consequently, transmen undergo this surgery in other countries. While there are many techniques for phalloplasty, the basic method creates a penis from a flap of tissue from another area of the body (commonly, the forearm), using microsurgery. A nerve within the flap is attached to the ilioinguinal nerve and the clitoral branch of the pudendal nerve, allowing for sensation in the new phallus. The clitoris is incorporated into the base of the new phallus flap. The scrotum is created from the labia majora, and prosthetic silicon testicles are inserted.
In metoidioplasty, the clitoris is first enlarged by preparatory testosterone use. In the surgery, it is released from its attached ligaments in order to add length. Next, the urethra is extended and incorporated into the phallus. The dorsal nerves of the clitoris are left intact, and the individual is able to urinate from the standing position.
Transmen frequently report an increased desire as well as a change in character of their orgasms with androgenic hormone therapy. This may be related to the effects of hormone therapy on the frequency and quality of erectile tissue stimulation, but more research needs to be conducted in this area.
Anyone contemplating gender-confirming surgery should carefully consult with the surgeon about the expected changes and possible side effects. Psychological counseling is advisable to address the complexities of personal and social interactions.
VARIOUS MACHINES AND DEVICES can be used as sex toys for recreational pleasure or as treatments to help overcome a sexual disorder. The simplest sex toys are vibrators, powered by battery or wall current. They are available in different sizes, shapes, textures, and colors, and are used by women and, although less so, by men.
Some vibrators are worn on the back of the hand, behind the fingers, so that genital contact is made by the vibrating fingers rather than by the vibrator itself. Other vibrators are applied directly to the genital region. This type of device varies in diameter of the stimulating head. Some women prefer to start out using a wider, rather than a narrower, vibrator for ease of stimulating the clitoris, and then, with practice, they make a transition to a narrower vibrator. The wider vibrators are also easier for a woman’s partner to use. Vibrators that focus on clitoral stimulation are particularly appropriate for beginners or for individuals who want to avoid possible tearing of their hymen while enjoying self-stimulation. The hymen is a membrane inside the vagina near the vaginal entrance. The hymen only partially blocks the vaginal canal, thereby allowing the passage of menstrual flow.
Dildos resemble an erect penis in shape, size, and/or texture, and they may or may not contain a vibrator mechanism. They are made from a variety of materials, including pliable silicone or hard plastic, glass, or metal. They can stimulate the vaginal walls and give a woman a sense of penetration. The “Rabbit” is a Y-shaped dildo that is designed to stimulate the vagina internally at the same time as stimulating the clitoris externally. Another type of dildo is the “G spot stimulator,” which is typically curved to apply pressure to the G spot, the anterior (belly-side) wall of the vagina, just behind the pubic bone. There are vibrating and nonvibrating designs. Some dildos have remote controls, which could be helpful for persons with physical limitations such as rheumatoid arthritis or obesity.
“Butt plugs” are small dildos designed specifically to stimulate the anus and rectum of women or men. They typically have a widened base at the end to prevent the dildo from inadvertently entering too deep into the rectum. Some butt plugs, such as Aneros, are devised to stimulate the prostate gland, which some men describe as pleasurable. Another type of sex toy for men is the artificial vagina. One example of this is the Fleshlight, which resembles a flashlight and contains a soft silicone vagina-shaped canal and an external vulva.
There are also devices that stimulate both partners simultaneously, such as penile ring vibrators, which the man puts around his penis to help him prolong his erection, and vibration from the ring stimulates his partner’s clitoris during vaginal intercourse.
Some massagers, designed for use on the back, neck, or face, can also be used for sexual pleasure.
Other devices, such as Eros and vacuum constriction devices (the “sex pump,” or VCD), increase blood flow to the genital area. The Eros is battery-powered, and the VCD has both mechanical and battery-powered models. The VCD was initially recommended for men who were experiencing erectile dysfunction as a complication of diabetes, prostate surgery, or spinal cord injury. The Eros, which is newer, was originally designed to help women who have arousal or orgasmic disorders related to low genital blood flow. Reports indicate that it’s also useful for treating urinary urgency-frequency and urge incontinence (“overactive bladder”) in women. While both Eros and the VCD are reported to be generally safe, you are advised to seek medical advice before embarking on use of these devices.
The Sybian is a large, electric motor-driven device that a woman sits astride. This device was made famous by its use on shows hosted by television and radio personality Howard Stern. The motor drives a thrusting dildo that can be moved at variable speed. The Venus is a large, electric motor-driven device that contains an artificial vagina into which a man inserts his penis; air is pushed and pulled rhythmically through the “vagina” at variable speed.
People use sex toys, including vibrators, for many different reasons. Some people might find it difficult or unacceptable to self-stimulate by hand, but don’t feel the same way about self-stimulating with a device. In a sexual relationship, some may find it easier to give their partner pleasure using a device, rather than their hands. This may be especially true in elderly couples or in persons with physical limitations. Other people may just want to experiment with a new wrinkle in their sex life. It goes without saying that these devices won’t solve relationship issues that may underlie interpersonal sexual difficulties. Casual sharing of sex toys should be viewed as being potentially as risky as unprotected sex, so they should not be shared. Sex toys should be cleaned according to the manufacturer’s instructions.
In the United States and elsewhere, there are museums dedicated to these sexual devices. The Prague SexMachines Museum has more than two hundred objects and mechanical appliances available for view on its website, including machines from hundreds of years ago and devices with multiple functions, such as stimulating the clitoris while scratching the back. Another museum, the Museum of Sex, in New York City, exhibits a variety of patented sexual devices.
MALES OF EVERY SPECIES of mammal ejaculate, and many researchers have concluded that the activity seems to be rewarding, just as it is in humans. The orgasmic experience, however, must differ considerably among mammalian species, considering the great variability in ejacula-tory patterns in terms of the amount of genital interaction required to ejaculate and the duration of the ejaculatory process itself. For a few species, we have precise information on the duration of the distinct behavioral events involved in mating (copulation, or coitus), including ejaculation.
In male rats, copulation lasts for an average of about one-third of a second, and then, after several of these brief copulations over the next few minutes, ejaculation occurs, lasting about two-thirds of a second. In rabbits, ejaculation occurs immediately following penile insertion; the contraction of the seminal vesicles, which produces the ejaculation, lasts about one second. If the perceptual experience of orgasm is directly related to these peripheral events, such as occurs in men, orgasm would last about one second. So, orgasm in rats and rabbits would be considerably shorter than in humans. The conscious perception of orgasm in most men has been timed to last twenty seconds or less.
One might wonder about the duration of the perceptual orgasm in a male pig, whose seminal emission and ejaculation lasts about five minutes! But what about the female pig? She stands still during these five minutes. Studies have shown that the male pig’s breath immobilizes the female pig, and the essence in his breath has been identified as the biochemical 16-androstene. If this chemical is sprayed onto a female pig’s nose, she stops moving. It is not known, however, whether the female pig stands immobilized for the five-minute duration of the male’s ejaculation because of the effect of his breath or because it’s rewarding to her, or perhaps both. (One might not be surprised if the breath of a copulating male pig had an immobilizing—or knockout—effect on a human, as well.)
The female pig exemplifies the problem of determining whether nonhuman females experience orgasm—we simply lack a good marker (such as ejaculation). The issue has been much debated, particularly among investigators interested in the idea that female orgasm is a specialized adaptation in humans, supposedly related to the reinforcement of bonding between the sexes. This position draws a clear distinction between women and other female primates. However, many data support the existence of female orgasm in other primates. Physiological responses identical to those occurring in women during orgasm have been observed in female monkeys of several species. In his book Primate Sexuality, Alan Dixson lists eight species of primates in which behavioral and physiological responses in females strongly suggest the presence of orgasm. Among the behavioral responses are a quick backward glance at the male, changes in facial expression (“climax face, open mouth, and grimaces”), and vocalizations. Among the physiological responses are uterine contractions, contractions of other tissues surrounding the vagina, and increased heart and respiratory rate.
Some researchers have claimed that other, nonprimate female mammals also experience orgasms, based on four kinds of evidence: (1) changes in heart rate, blood pressure, and respiration similar to those observed during orgasm in women, which have been recorded in several nonprimate mammalian species during copulation; (2) vaginal and uterine contractions in several species during copulation, comparable to those observed in women; (3) hormonal changes, some of them specifically associated with orgasm in women (such as release of prolactin), in nonprimate females; and (4) females’ vocalizations during coitus.