CHAPTER 11
Drug Dynamics
Drug dynamics (pharmacodynamics) involves what a drug does to the body.
Drug dynamics describes the therapeutic effects of drugs (such as relief of pain and reduction of blood pressure) and their side effects. But drug dynamics also describes where (the site) and how (the mechanism) a drug acts on the body. A drug’s effects on the body may be influenced by many factors, such as a person’s age (see pages 89 and 1896), genetic makeup, and other medical conditions the person has other than the one being treated.
Site Selectivity
After being swallowed, injected, inhaled, or absorbed through the skin, most drugs enter the bloodstream and circulate throughout the body. Some drugs are administered directly to the area where they are wanted—for example, to the eyes in eyedrops. The drugs then interact with cells or tissues where they produce their intended effects (target sites). Some drugs are relatively nonselective. They affect many different tissues or organs. For example, atropine, a drug given to relax muscles in the digestive tract, may also relax muscles in the eyes and in the respiratory tract. Other drugs are relatively selective. For example, nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin and ibuprofen (see page 644), target any area where inflammation is present. Still other drugs are highly selective. They affect mainly a single organ or system. For example, digoxin, a drug given to manage heart failure, affects mainly the heart, increasing its pumping efficiency. Sleep aids target certain nerve cells of the brain.
How do drugs know where to exert their effects? The answer involves how they interact with cells or substances such as enzymes.
Receptors on Cells
On their surface, most cells have many different types of receptors. A receptor is a molecule with a specific three-dimensional structure, which allows only substances that fit precisely to attach to it—as a key fits in its lock. Receptors enable natural (originating in the body) substances outside the cell, such as neurotransmitters and hormones, to influence the activity of the cell. That influence may be to stimulate or inhibit a process inside the cell. Drugs tend to mimic these natural substances and thus use receptors in the same way. For example, morphine and related pain-relieving drugs act on or affect the same receptors in the brain used by endorphins, which are substances produced by the body to help control pain. Some drugs attach to only one type of receptor. Other drugs, like a master key, can attach to several types of receptors throughout the body. A drug’s selectivity can often be explained by how selectively it attaches to receptors.
A Perfect Fit
A receptor on the cell’s surface has a three-dimensional structure that allows a specific substance, such as a drug, hormone, or neurotransmitter, to bind to it because the substance has a three-dimensional structure that perfectly fits the receptor, as a key fits a lock.
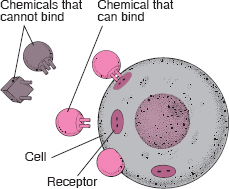
TARGETS IN THE BODY: CELL RECEPTORS
Certain natural substances in the body, such as neurotransmitters and hormones, target specific receptors on the surface of cells. When these substances bind with the receptor on a cell, they stimulate that receptor to perform its function, which is to produce or to inhibit a specific action in the cell. Drugs can also target and bind with these receptors.
Some drugs act as agonists, stimulating the receptor in the same way that the body’s natural substances do. Others act as antagonists, blocking the action of the natural substance on the receptor. Each type of receptor has many subtypes, and drugs may act on one or several subtypes of receptors.
Agonists and Antagonists: Drugs that target receptors are classified as agonists or antagonists. Agonist drugs activate, or stimulate, their receptors, triggering a response that increases or decreases the cell’s activity. Antagonist drugs block the access or attachment of the body’s natural agonists, usually neurotransmitters, to their receptors and thereby prevent or reduce cell responses to natural agonists.
Agonist and antagonist drugs can be used together in patients with asthma. For example, albuterol can be used with ipratropium. Albuterol, an agonist, attaches to specific (adrenergic) receptors on cells in the respiratory tract, causing relaxation of smooth muscle cells and thus widening of the airways (bronchodilation). Ipratropium, an antagonist, attaches to other (cholinergic) receptors, blocking the attachment of acetylcholine, a neurotransmitter that causes contraction of smooth muscle cells and thus narrowing of the airways (bronchoconstriction). Both drugs widen the airways (and make breathing easier) but in different ways.
Beta-blockers, such as propranolol, are a widely used group of antagonists. These drugs are used to treat high blood pressure, angina (chest pain caused by an inadequate blood supply to the heart muscle), and certain abnormal heart rhythms and to prevent migraines. They block or reduce stimulation of the heart by the agonist hormones epinephrine (adrenaline) and norepinephrine (noradrenaline), which are released during stress. Antagonists such as beta-blockers are most effective when the concentration of the agonist is high in a specific part of the body. Similar to the way a roadblock stops more vehicles during the 5:00 PM rush hour than at 3:00 AM, beta-blockers, given in doses that have little effect on normal heart function, may have a greater effect during sudden surges of hormones released during stress and thereby protect the heart from excess stimulation.
Enzymes
Instead of receptors, some drugs target enzymes, which regulate the rate of chemical reactions. Drugs that target enzymes are classified as inhibitors or activators (inducers). For example, the cholesterol-lowering drug lovastatin inhibits an enzyme called HMG-CoA reductase, which is critical in the body’s production of cholesterol. A side effect of the antibiotic rifampin is the activation of the enzymes involved in metabolizing oral contraceptives. When women who are taking an oral contraceptive also take rifampin, the contraceptive is metabolized (that is, broken down into inactive components) and removed from the body more quickly than usual and may therefore be ineffective.
Drug Action
Drugs affect only the rate at which existing biologic functions proceed. Drugs do not change the basic nature of these functions or create new functions. For example, drugs can speed up or slow down the biochemical reactions that cause muscles to contract, kidney cells to regulate the volume of water and salts retained or eliminated by the body, glands to secrete substances (such as mucus, stomach acid, or insulin), and nerves to transmit messages.
Drugs cannot restore structures or functions already damaged beyond repair by the body. This fundamental limitation of drug action underlies much of the current frustration in trying to treat tissue-destroying or degenerative diseases such as heart failure, arthritis, muscular dystrophy, multiple sclerosis, and Alzheimer’s disease. Nonetheless, some drugs can help the body repair itself. For example, by stopping an infection, antibiotics can allow the body to repair damage caused by the infection.
Some drugs are hormones, such as insulin, thyroid hormones, estrogens, or cortisol. They can be used to replace hormones that are missing from the body.
Reversibility
Most interactions between a drug and a receptor or between a drug and an enzyme are reversible: After a while, the drug disengages, and the receptor or enzyme resumes normal function. Sometimes an interaction is largely irreversible, and the drug’s effect persists until the body manufactures more enzyme. For example, omeprazole, a drug used in the management of gastroesophageal reflux and ulcers, irreversibly inhibits an enzyme involved in the secretion of stomach acid.
Affinity and Intrinsic Activity
A drug’s action is affected by the quantity of drug that reaches the receptor and the degree of attraction (affinity) between it and its receptor on the cell’s surface. Once bound to their receptor, drugs vary in their ability to produce an effect (intrinsic activity). Drugs vary in their affinity and intrinsic activity.
Drugs that activate receptors (agonists) must have both great affinity and intrinsic activity: They must bind effectively to their receptors, and the drug bound to its receptor (drug-receptor complex) must be capable of producing an effect in the targeted area. In contrast, drugs that block receptors (antagonists) must bind effectively but have little or no intrinsic activity, because their function is to prevent an agonist from interacting with its receptors.
Potency and Efficacy
A drug’s effects can be evaluated in terms of strength (potency) or effectiveness (efficacy).
Potency refers to the amount of drug (usually expressed in milligrams) needed to produce an effect, such as relief of pain or reduction of blood pressure. For instance, if 5 milligrams of drug A relieves pain as effectively as 10 milligrams of drug B, drug A is twice as potent as drug B.
Efficacy refers to the potential maximum therapeutic response that a drug can produce. For example, the diuretic furosemide eliminates much more salt and water through urine than does the diuretic chlorothiazide. Thus, furosemide has greater efficacy than chlorothiazide. However, greater potency or efficacy does not necessarily mean that one drug is preferable to another. When judging the relative merits of drugs for a person, doctors consider many factors, such as side effects, potential toxicity, duration of effect (which determines the number of doses needed each day), and cost.