CHAPTER 70
Biology of the Lungs and Airways
To sustain life, the body must produce sufficient energy. Energy is produced by burning molecules in food, which is done by the process of oxidation (whereby food molecules are combined with oxygen). Oxidation involves carbon and hydrogen being combined with oxygen to form carbon dioxide and water. The consumption of oxygen and the production of carbon dioxide are thus indispensable to life. It follows that the human body must have an organ system designed to exchange carbon dioxide and oxygen between the circulating blood and the atmosphere at a rate rapid enough for the body’s needs, even during peak exercise. The respiratory system enables oxygen to enter the body and carbon dioxide to leave the body.
Respiratory System
The respiratory system starts at the nose and mouth and continues through the airways and the lungs. Air enters the respiratory system through the nose and mouth and passes down the throat (pharynx) and through the voice box, or larynx. The entrance to the larynx is covered by a small flap of tissue (epiglottis) that automatically closes during swallowing, thus preventing food or drink from entering the airways.
The largest airway is the windpipe (trachea), which branches into two smaller airways: the left and right bronchi, which lead to the two lungs. Each lung is divided into sections (lobes): three in the right lung and two in the left lung. The left lung is a little smaller than the right lung because it shares space in the left side of the chest with the heart.
The bronchi themselves branch many times into smaller airways, ending in the narrowest airways (bronchioles), which are as small as one half of a millimeter across. The airways resemble an upside-down tree, which is why this part of the respiratory system is often called the bronchial tree. Large airways are held open by semiflexible, fibrous connective tissue called cartilage. Smaller airways are supported by the lung tissue that surrounds and is attached to them. Circular airway smooth muscle can dilate or constrict, thus changing airway size.
Inside the Lungs and Airways

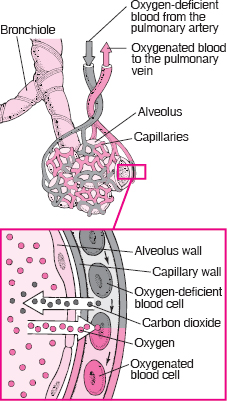
At the end of each bronchiole are thousands of small air sacs (alveoli). Together, the millions of alveoli of the lungs form a surface of more than 100 square meters. Within the alveolar walls is a dense network of tiny blood vessels called capillaries. The extremely thin barrier between air and capillaries allows oxygen to move from the alveoli into the blood and allows carbon dioxide to move from the blood in the capillaries into the air in the alveoli.
The pleura is a slippery membrane that covers the lungs as well as the inside of the chest wall. It allows the lungs to move smoothly during breathing and as the person moves. Normally, the two layers of the pleura have only a small amount of lubricating fluid between them. The two layers glide smoothly over each other as the lungs change size and shape.
Chest Cavity
The lungs are housed in the chest cavity, a space that also includes the mediastinum. The mediastinum is in the center of the chest and contains the heart, thymus, and lymph nodes, along with portions of the aorta, vena cava, trachea, esophagus, and various nerves. It encompasses the area bordered by the breastbone (sternum) in front, the spinal column in back, the entrance to the chest cavity above, and the diaphragm below. Functionally, the mediastinum isolates the left and right lung from each other. For example, if the chest wall is punctured on one side, causing the lung on that side to collapse, the other lung remains inflated and functioning, because the two lungs are separated by the mediastinum.
The lungs and other organs in the chest are protected by a bony cage, which is formed by the sternum, ribs, and spine. The 12 pairs of ribs curve around the chest from the back. Each pair is joined to the bones (vertebrae) of the spine. In the front of the body, the upper seven pairs of ribs are attached to the sternum by cartilage. The eighth, ninth, and tenth pairs of ribs join the cartilage of the pair above; the last two pairs (floating ribs) are shorter and do not join in the front (see page 447).
Exchanging Oxygen and Carbon Dioxide
The primary function of the respiratory system is to exchange oxygen and carbon dioxide. Inhaled oxygen enters the lungs and reaches the alveoli. The layers of cells lining the alveoli and the surrounding capillaries are each only one cell thick and are in very close contact with each other. This barrier between air and blood averages about 1 micron (1/10,000 of a centimeter) in thickness. Oxygen passes quickly through this air-blood barrier into the blood in the capillaries. Similarly, carbon dioxide passes from the blood into the alveoli and is then exhaled.
Oxygenated blood travels from the lungs through the pulmonary veins and into the left side of the heart, which pumps the blood to the rest of the body (see page 317). Oxygen-deficient, carbon dioxide-rich blood returns to the right side of the heart through two large veins, the superior vena cava and the inferior vena cava. Then the blood is pumped through the pulmonary artery to the lungs, where it picks up oxygen and releases carbon dioxide.
To support the exchange of oxygen and carbon dioxide, about 6 to 10 liters of air per minute are brought in and out of the lungs, and about three tenths of a liter of oxygen is transferred from the alveoli to the blood each minute, even when the person is at rest. At the same time, a similar volume of carbon dioxide moves from the blood to the alveoli and is exhaled. During exercise, it is possible to breathe in and out more than 100 liters of air per minute and extract 3 liters of oxygen from this air per minute. The rate at which oxygen is used by the body is one measure of the rate of energy expended by the body. Breathing in and out is accomplished by respiratory muscles.
Gas Exchange Between Alveolar Spaces and Capillaries
The function of the respiratory system is to exchange two gases: oxygen and carbon dioxide. The exchange takes place in the millions of alveoli in the lungs and the capillaries that envelop them. As shown below, inhaled oxygen moves from the alveoli to the blood in the capillaries, and carbon dioxide moves from the blood in the capillaries to the air in the alveoli.
Three processes are essential for the transfer of oxygen from the outside air to the blood flowing through the lungs: ventilation, diffusion, and perfusion. Ventilation is the process by which air moves in and out of the lungs. Diffusion is the spontaneous movement of gases, without the use of any energy or effort by the body, between the gas in the alveoli and the blood in the capillaries in the lungs. Perfusion is the process by which the cardiovascular system pumps blood throughout the lungs. The body’s circulation is an essential link between the atmosphere, which contains oxygen, and the cells of the body, which consume oxygen. For example, the delivery of oxygen to the muscle cells throughout the body depends not only on the lungs but also on the ability of the blood to carry oxygen and on the ability of the circulation to transport blood to muscle.
Control of Breathing
Breathing is usually automatic, controlled subconsciously by the respiratory center at the base of the brain. Breathing continues during sleep and usually even when a person is unconscious. People can also control their breathing when they wish, for example during speech, singing, or voluntary breath holding. Sensory organs in the brain and in the aorta and carotid arteries monitor the blood and sense oxygen and carbon dioxide levels. Normally, an increased concentration of carbon dioxide is the strongest stimulus to breathe more deeply and more frequently. Conversely, when the carbon dioxide concentration in the blood is low, the brain decreases the frequency and depth of breaths. During breathing at rest, the average adult inhales and exhales about 15 times a minute.
The lungs have no skeletal muscles of their own. The work of breathing is done by the diaphragm, the muscles between the ribs (intercostal muscles), the muscles in the neck, and the abdominal muscles. The diaphragm, a dome-shaped sheet of muscle that separates the chest cavity from the abdomen, is the most important muscle used for breathing in (called inhalation or inspiration). The diaphragm is attached to the base of the sternum, the lower parts of the rib cage, and the spine. As the diaphragm contracts, it increases the length and diameter of the chest cavity and thus expands the lungs. The intercostal muscles help move the rib cage and thus assist in breathing. The muscles used in breathing can contract only if the nerves connecting them to the brain are intact. In some neck and back injuries, the spinal cord can be severed, which breaks the nervous system connection between the brain and the muscles, and the person will die unless artificially ventilated.
Diaphragm’s Role in Breathing
When the diaphragm contracts and moves lower, the chest cavity enlarges, reducing the pressure outside the lungs. To equalize the pressure, air enters the lungs. When the diaphragm relaxes and moves back up, the elasticity of the lungs and chest wall pushes air out of the lungs.
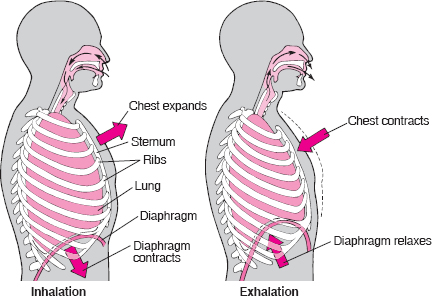
The process of breathing out (called exhalation or expiration) is usually passive when a person is not exercising. The elasticity of the lungs and chest wall, which are actively stretched during inhalation, causes them to expel air out of the lungs when inspiratory muscles are relaxed. Therefore, when a person is at rest, no effort is needed to breathe out. During vigorous exercise, however, a number of muscles participate in exhalation. The abdominal muscles are the most important of these. Abdominal muscles contract, raise abdominal pressure, and push a relaxed diaphragm against the lungs, causing air to be pushed out.
Defense Mechanisms
The average person who is moderately active during the daytime breathes about 20,000 liters of air every 24 hours. Inevitably, this air (which would weigh more than 20 kilograms) contains potentially harmful particles and gases. Particles, such as dust and soot, mold, fungi, bacteria, and viruses, deposit on airway and alveolar surfaces. Only small particles less than 3 to 5 microns in diameter penetrate to the deep lung. Fortunately, the respiratory system has defense mechanisms to clean and protect itself.
One such defense mechanism involves tiny muscular projections (cilia) on the cells that line the airways. The airways are covered by a liquid layer of mucus that is propelled by the cilia. These tiny muscles beat more than 1,000 times a minute, moving the mucus that lines the trachea about 0.5 to 1 centimeter per minute. Particles and pathogens that are trapped on this mucus layer are cleared to the mouth and swallowed.
Because of the requirements of gas exchange, alveoli are not protected by mucus and cilia—mucus is too thick and would slow movement of oxygen and carbon dioxide. Instead, the body has another defense system. Mobile cells on the alveolar surface called phagocytes seek out deposited particles, bind to them, ingest them, kill any that are living, and digest them. Phagocytes in alveoli of the lungs are called alveolar macrophages. When the lungs are exposed to serious threats, additional white blood cells in the circulation, especially neutrophils, can be recruited to help ingest and kill pathogens (foreign particles). For example, when the person inhales a great deal of dust or is fighting a respiratory infection, more macrophages are produced and neutrophils are recruited.
 Did You Know…
Did You Know…
In healthy people, age-related reductions in lung function seldom lead to symptoms, but they can contribute to an older person’s reduced ability to perform vigorous exercise.
Effects of Aging
The effects of aging on the respiratory system are similar to those that occur in other organs: maximum function gradually declines. Age-related changes in the lungs include decreases in the peak airflow, gas exchange, and vital capacity (the maximum amount of air that can be breathed out following a maximum inhalation); weakening of the respiratory muscles; and a decline in the effectiveness of lung defense mechanisms. In healthy people, these age-related changes seldom lead to symptoms, but they can contribute to an older person’s reduced ability to perform vigorous exercise, especially intense aerobic exercise, such as running, biking, and mountain climbing. Obesity also reduces pulmonary function. Additionally, older people are at higher risk of developing pneumonia after bacterial or viral infections. Thus, vaccines for respiratory infections such as influenza and pneumococcal pneumonia are particularly important for older people (see pages 1148 and 1149). Importantly, age-related changes in the lungs compound the effects of heart and lung diseases the person may have, especially those caused by the destructive effects of smoking.