The right way to wholeness is made up of fateful detours and wrong turnings.
—C. G. Jung
To be touched by the revelation of love or scientific discovery is among the greatest and most wondrous blessings of being alive. While the year 1969 was a dud for romance, it was for me a time of thrilling scientific illumination. While a momentous technical event occurred in outer space that year, for me, an awakening in inner space changed the course of my life.
At summer’s beginning my friends and I sat glued to the TV screen, our jaws dropped in awe. The Eagle lunar module had landed on the Bay of Tranquility, and Neil Armstrong assuredly stepped onto the lunar surface. Transfixed, we listened to the immortalized (though grammatically challenged) phrase: “One small step for man, one giant leap for mankind.” Men not only walked on the moon, they leaped in technological exuberance! Images of Earth were relayed from our nearest celestial neighbor, offering a visual reminder that we were not at the center of the universe.
In spite of that day’s historical significance, I doubt that many people remember the month or even the year of the Apollo 11 moon landing. However, that date, July 20, 1969, and the thrill of inner discovery were indelibly etched in my mind. A “chance” event occurred around the same time in my mind/body practice that was every bit as compelling. This singular event, a first step in a new professional life, gave birth to a fresh perspective on the human condition, as well as confronting me with my own formidable hang-ups and inner trauma demons.
This incident was occasioned by the referral of a young woman from a psychiatrist who was aware of my keen interest in the fledgling fields of stress and mind-body healing. Nancy (not her real name) had been suffering from frequent migraines, hyperthyroidism, and fatigue, as well as chronic pain and debilitating premenstrual syndrome. Today, such symptoms would probably have been diagnosed as fibromyalgia and chronic fatigue syndrome. Her life was further diminished by severe panic-anxiety attacks and agoraphobia that kept her tied to home. I had been developing some body awareness–based relaxation and stress-reduction procedures that the psychiatrist thought might be beneficial to her.
Nancy entered my office, clinging nervously to her husband’s arms. She was fidgeting with his hands; he was transparently burdened by her complete dependence. I noticed how tight her neck was, pulling in like an injured turtle, while her eyes were wide with the startled look of a deer in the headlights. Her posture was stooped, conveying a pervasive sense of fear and defeat. Nancy’s resting heart rate was high—almost 100 beats per minute (which I was able to surmise from the pulsing of the carotid artery in her neck). Her breathing was so shallow as to seem barely able to sustain life.
At first I taught Nancy to become aware of, and then to release, her chronically tense neck and shoulder muscles. She appeared to be relaxing deeply. Her heart rate decreased to a more normal range as her breathing deepened. However, moments later she abruptly became intensely agitated. Her heart, pounding wildly, shot up to approximately 130 beats per minute. Her breath was rapid and shallow as she gasped erratically. Then, as I watched helplessly, she abruptly froze in terror. Her face turned deathly white. She appeared paralyzed and barely able to breathe. Her heart seemed to almost stop, dropping precipitately to about 50 beats per minute (an action of the heart I will discuss later in Chapter 6). Fighting my own impending panic, I was at a loss as to what to do.
“I’m dying. Don’t let me die,” she pleaded in a small taut voice. “Help me, help me! Please don’t let me die.” Her disturbing helplessness evoked, in my subconscious, an archetypal solution. Suddenly, in my mind’s eye, a dreamlike image appeared: a tiger, crouched in readiness to strike, materialized out of the far wall of the room.
“Run, Nancy!” I commanded without thinking, “A tiger is chasing you. Climb those rocks and escape.” Bewildered by my own outburst, I gazed in amazement as Nancy’s legs began to tremble and then move up and down in what appeared to be spontaneous running movements. Her whole body started shaking—first convulsively, then more softly. As the shaking gradually subsided (over the better part of an hour), she experienced a feeling of peacefulness that, in her own words, “held her in warm tingling waves.” (See Figure 2.1a and 2.1b.)
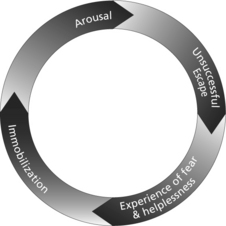
Fear/Immobility Cycle
Figure 2.1a This shows the vicious cycle by which fear and immobility feed off each other. It is what engulfs and traps us in the “black hole” of trauma.
Later, Nancy reported that during the session she had seen nightmarish images of herself as a four-year-old child, struggling to escape the grasp of the doctors who held her down in order to administer ether anesthesia for a “routine” tonsillectomy. Until now, she recounted, this event had been “long forgotten.” To my utter amazement, these unusual gyrations turned Nancy’s life around. Many of her symptoms improved significantly, and some disappeared altogether. The panic attack that occurred during the session was her last; and, over the next two years, until her graduation from graduate school, her chronic fatigue, migraines, and premenstrual symptoms improved dramatically. In addition, she reported the following “side effect”—she “felt more alive and happier than [she could] remember.”
Restoration of Active Defense Responses

Figure 2.1b I was able to lead Nancy out of her immobility/fear and hyperarousal by allowing her to re-create the experience of running and successfully escaping from her would-be attackers. It is essential for the client to feel the sensation of running. Running without inner sensing has only limited value.
What allowed Nancy to emerge from her frozen symptomatic shell and reengage in life was the same mechanism that prevented me from becoming traumatized after I was hit by the automobile. The shaking and trembling, occurring in the warm and reassuring presence of a reliable other person, and allowed to continue to completion, helped both of us to restore equilibrium and wholeness, and to be freed from trauma’s grip.
Through focused awareness and micro-movements to reenact and complete our unfinished, instinctually rooted protective actions, both Nancy and I were able to discharge the residual nervous system “energy” that had been activated for survival. Nancy experienced the long-delayed escape that her body wanted to make while she was being tied down and overpowered as a defenseless little girl. In short, we both experienced and embodied the innate and powerful wisdom of our instinctual responses as they mobilized to ward off mortal danger.
The mindful sensing of this protective primal force stood in stark contrast to the overwhelming helplessness that had engulfed each of us. The major difference between Nancy’s experience and mine was that I had the luck of receiving self-administered first aid, and the fortunate presence of the pediatrician, to nip the potential PTSD symptoms in the bud. Nancy, like millions of others, unfortunately did not. She had suffered years of needless distress until we briefly revisited and “renegotiated” her childhood surgery in my office, some twenty years afterward.*
Had I not sensed the raw muscular power of my survival instincts, contrasting with my helpless condition, I surely would have developed the debilitating symptoms of PTSD that had so shadowed and crippled Nancy. I would have, like Nancy, been left too frightened to venture out confidently into the world again. Just as Nancy was able to escape her tormenters in retrospect, I was able to both escape my destruction and preventatively “reset” my nervous system in real time.
When acutely threatened, we mobilize vast energies to protect and defend ourselves. We duck, dodge, twist, stiffen and retract. Our muscles contract to fight or flee. However, if our actions are ineffective, we freeze or collapse. Nancy’s four-year-old body had tried to escape from her masked predators. Her body wanted to run away and escape, but it could not. She was overpowered and held down against her will by all-powerful masked and gowned giants. In our hour together Nancy’s body contradicted her panicky feelings of being overwhelmed and trapped. And as her body learned this, so did her mind.
When any organism perceives overwhelming mortal danger (with little or no chance for escape) the biological response is a global one of paralysis and shutdown. Ethologists call this innate response tonic immobility (TI). Humans experience this frozen state as helpless terror and panic. Such a state of shutdown and paralysis is meant to be temporary. A wild animal exhibiting this acute physiological shock reaction will either be eaten or, if spared, presumably resume life as before its brush with death; it will be none the worse for the encounter and perhaps wiser. It may be more vigilant (not to be confused with hypervigilant) about similar future sources of threat and thus of early intimations of danger. A deer might, for example, avoid certain rocky outcroppings where it had previously escaped the lunging attack of a mountain lion.
Humans, in contrast to animals, frequently remain stuck in a kind of limbo, not fully reengaging in life after experiencing threat as overwhelming terror or horror. In addition, they exhibit a propensity for freezing in situations where a non-traumatized individual might only sense danger or even feel some excitement. Rather than being a last-ditch reaction to inescapable threat, paralysis becomes a “default” response to a wide variety of situations in which one’s feelings are highly aroused. For example, the arousal of sex may turn unexpectedly from excitement to frigidity, revulsion or avoidance.
In an attempt to understand the episode with Nancy, I was pulled in several new directions. First, I realized that, if not for trusting my gut instincts and a little bit of blind luck, I might just as easily have inadvertently “retraumatized” Nancy, leading to a worsening of her already severe symptoms. In addition, like the gambler who hits the jackpot early in his career, I would soon find out that such dramatic—one-time—“cures” would not always be the case. I was drawn into a consuming journey to uncover just what had transpired that summer day in 1969. As I discovered, it was crucial to “titrate” (gradually access) these physiological reactions so that they were not overwhelming. Just exposing a client to his or her traumatic memories and having the person relive them was, at best, unnecessary (reducing integration and feelings of mastery and goodness) and at worst retraumatizing for the individual. I also learned that the shaking and trembling, which constitute the discharge reactions, were often so subtle as to be barely noticeable to an outside observer. Often the manifestation of the discharge was a gentle muscular fasciculation (minute muscular trembling and quivers) or temperature change—such as going from very cold to very hot. These changes are generally monitored by observing color changes in the hands and face.
Over the following decades, I explored the biological basis of trauma from a comparative study of animals and their nervous systems. This, I felt, would help me develop a systematic approach to healing trauma that could be reproduced reliably and systematically, as well as being sufficiently safe. This journey also fulfilled an early dream of mine: I became a (small) part of the space adventure. While still a Berkeley graduate student in medical biophysics, I was given a fellowship as a stress consultant at NASA for a year. My primary task—to help prepare our astronauts for the first space shuttle flight—gave me a unique opportunity to study people whose stress resilience was unusually robust. These observations inspired me to reflect back on my session with Nancy some years earlier: on her profound lack of resilience and her spontaneous transformation. It seemed possible that the astronauts’ super-resilience was a skill that even the most highly traumatized individuals could learn to activate, a birthright that needed to be reclaimed.
In attempting to understand what had transpired that day with Nancy, I was struck by a “footnote” in an informal graduate seminar I was taking in comparative animal behavior. One of the professors, Peter Marler, had mentioned some peculiar behaviors exhibited by prey animals such as birds and rabbits when they were physically restrained. That night I awoke, shaking in excitement. Could Nancy’s reaction (when held down by the doctors) be similar to those of the experimentally restrained animals? As for my “hallucination” of the crouching tiger, that was undoubtedly a creative “waking dream” stimulated by that inspiring graduate seminar.
In pursuing the arcane allusion from my seminar, I came across a 1967 article titled “Comparative Aspects of Hypnosis.”6 I brought this article, along with my ideas about it, to my graduate research advisor, Donald M. Wilson.† His field was invertebrate neurophysiology, and he was familiar with these types of “freezing” behaviors. However, for one dedicated solely to the study of creatures like insects and lobsters, he was understandably skeptical about “animal hypnosis.” Nonetheless, I remained fascinated by the broadly observed phenomenon of animal paralysis and spent endless hours in the musty, dusty stacks of the Life Sciences graduate library. At the same time, I continued to see more clients referred primarily by Ed Jackson, the psychiatrist who had referred Nancy to me. I was exploring with them how various imbalanced patterns of muscular tension and postural tone were related to their symptoms—and how releasing and normalizing these entrenched patterns often led to unexpected and dramatic cures. Then in 1973, in the acceptance speech for his share in the Nobel Prize in Physiology or Medicine,‡ the ethologist Nikolaas Tinbergen unexpectedly chose to talk not primarily about his study of animals in their natural environment, but about the observed human body as it goes through life and as it functions and malfunctions under stress. I was struck by his observations about the Alexander technique§ This body-based reeducation treatment, which he and members of his family had undergone with notable health benefits (including a normalizing of his high blood pressure), paralleled my observations with my body-mind clients.
Clearly, I needed to talk to this elder. I managed to locate him at Oxford University; with unassuming generosity, this Nobel Laureate spoke to me, a lowly graduate student, via transatlantic cable on a number of occasions. I told him about my first session with Nancy and other clients, and about my speculation concerning the relationship of her reactions to “animal paralysis.” He was excited about the possibility that animal immobility reactions might play an important role in humans under conditions of inescapable threat and extreme stress, and encouraged me to pursue this line of investigation.‖ I occasionally wonder if without his support, as well as that from Hans Selye (the first stress researcher) and Raymond Dart (the anthropologist who discovered Australopithecus), I might have thrown in the towel.
In a memorable phone conversation, Tinbergen chided me in his kind, grandfatherly voice, “Peter, we are, after all, just a bunch of animals!” According to recent polls, however, only half of the Western world (and even fewer in the United States) seem to believe in evolution and, thus, in our intimate relation to other mammals. Yet given obvious patterns in anatomy, physiology, behavior, and emotions, and since we share the same survival parts of the brain with other mammals, it only makes sense that we share their reactions to threat. Hence, there would be great benefit gained from learning how animals (particularly mammals and higher-level primates) respond to threat, and then observing how they rebound, settle and return to equilibrium after the threat has passed. Many of us humans, unfortunately, have become alienated from this innate capacity for resilience and self-healing. This, as we shall explore, has made us vulnerable to being overwhelmed and traumatized.
It was not until 1978, however, that I could plant my observations on firmer ground. While working at the NASA Ames labs in Mountain View, California, and continuing to develop my body-mind practice in Berkeley, I spent every spare moment frequenting the biology graduate library. One dark and rainy December day in 1978, I was making my usual library rounds. In that era, long before Google or anything remotely resembling a PC, my usual mode of library research was to pack a lunch and then leaf through the large volumes of possibly relevant journals. With this supposedly inefficient, meandering method, I came across many wonderful gems that I might not have discovered by a “high-tech” search engine. These formative research efforts set the theoretical groundwork for my life’s work.
One day I chanced upon a mind-blowing article by Gordon Gallup and Jack Maser that described how “animal paralysis” was evoked, with variables experimentally controlled.7 This paper, which I discuss in Chapter 4, gave me the key that allowed me to weave observations of my body-mind clients (like Nancy) with an appreciation for how certain fear-based survival instincts both shape trauma and inform its healing. I was fortunate to have the freedom to speculate in this manner since trauma had not yet been formally defined as posttraumatic stress disorder (PTSD), and would not be for over a decade. For this reason, I am happy to say, I never pigeonholed trauma as a reified and incurable disease, as it became known in the early PTSD literature.
A synchronous and full-cycle return occurred several years ago. I was presenting my work at a conference titled “Frontiers in Psychotherapy,” put on by the Psychiatry Department at the University of California, San Diego, School of Medicine. At the end of my talk, a lively, impish man jumped up to introduce himself: “Hi, I’m Jack Maser!” I shook my head, dubious at first; not quite believing my ears, I burst into spontaneous laughter. After exchanging a few words, we arranged to lunch together. At this time he shared with me his delight in discovering that his animal work had found a clinical application in real-life therapy. I was sort of a clinical godchild to his experimental godfather.
In 2008, Jack Maser forwarded to me an article that he and a colleague, Stephen Bracha, had just published. In this article they proposed a fundamental change to the “Bible” of psychiatric diagnosis. They wanted to include the concept of tonic immobility in explaining trauma.8 My jaw dropped so far that a bird might have flown in and nested there. The Diagnostic and Statistical Manual of Mental Disorders, or DSM, is the encyclopedic book that psychologists and psychiatrists use to diagnose “mental disorders,” including Posttraumatic Stress Disorder. (The DSM is now in its “IV-R” edition, the “R” denoting a partial revision of the fourth edition.) The next edition—the DSM-V—will (ideally) be a significant step forward.
The previous versions of the PTSD diagnosis have been careful not to suggest a mechanism (or even a theory) to explain what happens in the brain and body when people become traumatized. This absence is important for more than academic reasons: a theory suggests rationales for treatment and prevention. This avoidance, and sole reliance on taxonomy, is an understandable overreaction to the Freudian theory’s previous stranglehold on psychology. I believe that it is only with intimate collaboration that science and praxis will co-evolve into a lively, vibrant partnership capable of generating truly innovative therapies. An open multidisciplinary effort could begin to help us discern what is or is not effective and to improve at our primary aim of helping suffering people heal!
The article by Jack Maser and Steven Bracha offers a spirited challenge to those entrusted to write the DSM-V. In their audacious commentary, these two researchers put forth the bold premise that there exists a theoretical basis for the mechanisms underlying PTSD: an evolutionary (instinctual) basis for trauma, similar to what I had observed with Nancy in 1969. With this article, I had come full circle. Gallup and Maser’s 1977 experimental studies on fear and “animal paralysis” had inspired my explanation for her behavior. Now Maser and Bracha concluded their 2008 article with these tickling couple of sentences:
Along swith the many changes that are being suggested for DSM-V, we urge the planners to seek out empirical studies and/or theories that place psychopathology in an evolutionary context. The field will then have a connection to broader issues in biology, the data on psychopathology can be placed within a widely accepted concept, and clinicians will have the possibility of developing more effective behavioral treatments (e.g., Levine, 1997).9
Oh, what divine delight! I could not help but wonder if my lecture at the San Diego Medical Conference had contributed in part to stimulating Maser and Bracha to make this proposal. The mere possibility that I might somehow, through fateful detours and twisted turns, have influenced the course of the psychiatric diagnosis of trauma (or at least contributed to the dialogue) was mind-blowing. Let us take a brief look at that diagnostic history.
* I use the term renegotiation to refer to the reworking of a traumatic experience in contrast to the reliving of it.
† Tragically, Donald Wilson was killed in a rafting accident in 1970.
‡ This transcript was published in the journal Science in 1974.
§ The Alexander technique takes its name from F. Matthias Alexander, who first observed and formulated its principles between 1890 and 1900. It is an approach for reducing harmful postural habits that interfere with both the physical and the mental conditions of the individual as a whole.
‖ At this time the chairman of my doctoral committee was quite dubious, even antagonistic, about my thesis.