Arya Nielsen
Introduction and history
Gua sha and Ba guan are Traditional East Asian Medicine (TEAM) therapies used for centuries in Asia, in Asian immigrant communities as a form of self or familial care and by acupuncturists and practitioners of TEAM worldwide in clinical practice (Chirali 2014, Manz 2009, Nielsen 2013, So 1987, Zhang & Hao 2000). Both Gua sha and ‘dry cupping’ are instrument-assisted techniques applied to the surface of the body that result in
transitory therapeutic petechiae
and ecchymosis called ‘sha’ in Chinese medicine (
Fig. 11.1
). With Gua sha, sha petechiae and ecchymosis are produced over a body area, sometimes as stripes; cupping sha often appears as round, ‘nummular’ shapes of petechiae and ecchymosis, with larger areas associated with moving cups (
Fig. 11.2
). (In a variant known as ‘wet cupping’ a surface site is superficially poked with a needle or lancet and then cupped to intentionally draw blood into the cup. Wet cupping will not be detailed here except to note that both wet and dry cupping have been a part of TEAM, the traditional medicine of Gulf Arabs (hijamah) (Al Bedah et al. 2016) and in early Western medicine descending from ancient Greek, Roman and Egyptian traditions.)
TEAM dates from the twenty-first century BC with the earliest known medical texts dating to 200 BC (Lu & Needham 1980). The first acupuncture text is found in 90 BC (Epler 1980); the earliest Chinese text linked to Gua sha is the
Shi Yi De Xiao Fang
(1337) (Nielsen 2013). Cupping dates to the Han scripts (200 BC), specifically the
Bo Shu
(Cao et al. 2010).
This chapter discusses Gua sha and Ba guan in medical terms, indications and specifics of palpation, evidence of effect, biomechanism and relationship to connective tissue, recommendations for safe practice, and a palpation exercise for practitioners to confirm or rule out the presence of sha. Techniques like Graston and instrument-assisted soft-tissue mobilization, derivatives of Gua sha, are not discussed here but can be accessed elsewhere (Hammer 2014).
Gua sha, Ba guan terms and tools
Gua sha
The literal translation of ‘gua’ to ‘scrape’ or ‘scratch’ (So 1987) has led to mistaking Gua sha as ‘dermabrasion’ which removes the epidermis and is clearly distinct from transitory surface sha petechiae and ecchymosis. Other common translations of Gua sha in Western medical literature include ‘coining’, ‘spooning’, ‘cao gio’ (Vietnamese) and kerik (Indonesian) (Nielsen 2009).
Gua sha consists of repeated unidirectional press-stroking with a smooth-edged tool at a lubricated area of the body surface until sha petechiae appear. Traditional tools include a soup spoon, coin, honed horn, bone, jade or stone. These blunt tools create a certain discomfort for the patient, avoided with the smooth-edged, thinner gauged cap that is also disposable after a single use (
www.guasha.com/gua-shatools
) (Nielsen et al. 2012, Nielsen et al. 2014).
Ba guan
The Chinese term ba
means to pull out or pull up, while the term guan
refers to a jar or pot. Ba guan
cupping involves the application of suctioned round cups on the skin (Nielsen et al. 2012). A vacuum is produced in each cup by flame (fire cupping) or by mechanical suction (suction cupping) that causes the tissue to tumefy and stretch into the cup. Nummular shaped areas of petechiae and ecchymosis are produced from the vacuum.
Sha
In TEAM, Qi stasis pain is defined as responsive to movement, massage, acupuncture or even a hot
shower. ‘Blood stasis’ pain is fixed, persistent or recurring at an area. It can be severe and does not resolve with movement, massage, acupuncture or application of heat alone.
Sha
is a polysemous term describing the presence of surface blood stasis associated with pain or sickness. Sha is also the petechiae/ecchymosis that are raised from applying Gua sha or Ba guan. The literal translation of
sha
from Chinese is ‘sand, sharkskin or red, raised, millet-size rash’. The fresh petechiae raised from Gua sha or Ba guan immediately begin to fade and blend to ecchymosis, disappearing in several days for Gua sha, longer for cupping depending on the length of time that cups are applied (
Figs 11.1
and
11.2
).
Sha pathology may be asymptomatic, pre-symptomatic, or mildly symptomatic with potential to worsen. Symptomatic pathology includes persistent, fixed, recurring, even excruciating pain. Sha may be associated with ‘sha syndrome’, defined as ‘
disease caused by the exposure leading to blockage of channels and manifesting as chilliness, fever, distension and pain of the body, or vomiting and diarrhea, or rigidity and numbness of extremities
’ (Nielsen 2013).
Figure 11.1
Applying Gua sha.
Sha is also translated as cholera (Weiger 1965) wherein sha petechiae and ecchymosis resemble cholera’s end-stage rash. Gua Sha in the East, like frictioning in early Western medicine (Jackson 1806), was used in the treatment of cholera and cholera-like disorders (So 1987), mimicking the crisis stage of an illness that is deployed as a cure per Hippocrates and Hippocratic doctrine ‘the crisis is the cure’ (Nielsen 1996).
Indications
Gua sha and Ba guan are used for acute or chronic pain, problems with movement or range of motion, and/or disturbed organ or system function, including acute infectious or chronic illness (Nielsen 2013, Zhang & Hao 2000, Manz 2009) for reduction of fever and in the case of Gua sha, for thermal dysregulation in potentially life-threatening heat stroke (Ruan & Cui 2005, Nielsen 2013). Blood stasis pain is fixed, persistent and or recurring. This can be associated with trigger point ‘loading’ or reflect deeper organ pathology or fascial constriction (Nielsen 2013).
Palpation and palpation literacy
Palpation in myofascial work evaluates asymmetry, range of motion, tissue texture changes and tenderness (ARTT) with emphasis on ‘temperature, texture, surface humidity, elasticity, turgor, tissue tension, thickness, shape, irritability, motion
’ (Chaitow 2012). In TEAM there are additional filters to palpation: indications of surface ischemia called ‘sha’, as well as focus on patterns of pain trajectory, ‘affiliation’ and relationship with known points, channels and organs. The TEAM channels are now recognized to
coincide with cleavages of connective tissue planes (Langevin & Yandow 2002), with potential for propagation of mechanical signaling (Langevin et al. 2001, Langevin 2006) and a ‘body-wide mechanosensitive signaling network
’ (Langevin 2006).
Palpating for ‘sha’ is informed by observable changes that represent ‘blood stasis’ or ischemia in the surface tissue. If there is tenderness and pain with pressing palpation, where resulting blanching is slow to fade, indicating normal surface perfusion is hindered – that is sha! (So 1987) (
Figs 11.2
and
11.3
) Surface ischemia should be part of palpation literacy because any perfusion restriction can be associated with persistent pain, reduced oxygen and glucose, leading to muscle or relevant tissue ‘fatigue’ (Chaitow & Delany 2011), restriction in tissue stretch, mobility, and myofascial dysfunction (Chaitow 2012).
Causes of dysfunction in myofascial tissues have been reduced to misutilization: overuse, misuse, abuse or disuse, with exceptions for congenital problems and impact of emotion or psychological stress (Chaitow & Delany 2011). A glaring omission that is based in every system of original medicine is the effect of exposure. Exposure to elements of wind, cold, heat, dryness and dampness beyond the body’s ability to compensate, or even because of how the body compensates, can lead to pain and illness. For example, cooling of the feet provokes symptomatic lower urinary tract infection in cystitis-prone women (Baerheim & Laerum 1992).
For decades, researchers held that the rhinovirus was the cause of the common cold and exposure to cold was considered to be an ‘old wives’ tale’. However, exposure to cold can influence the onset of common cold symptoms. A decline in either temperature or humidity, and not necessarily low temperature or humidity in the three days prior to onset, increases the risk of influenza (Jaakkola et al. 2014) and human rhinovirus infections (Ikaheimo et al. 2016) in a cold climate. Increased duration of exposure to cold is associated with greater susceptibility to infection (Mourtzoukou & Falagas 2007). Respiratory epidemics following a period of very cold weather may also be due to conversion of subclinical infections into symptomatic clinical infections (Mourtzoukou & Falagas 2007). Not every exposure results in an infection; every person exposed is not equal in terms of vulnerability to exposure or compounding risks like lack of sleep, proper nutrition, immune status or stress. It is conceded now that exposure is a risk.
Exposure can contract the surface vessels, result in surface ischemia that does not resolve with warming and is discoverable in ‘sha’ palpation. Pain stasis related to sha often becomes exacerbated by body
work. Patients may feel better with massage or a hot shower but will report feeling worse later. This should trigger an evaluation and palpation inspection for sha. See
Box 11.1
for indications for Gua sha or Ba guan.
Figure 11.2
Detail of sha from Gua sha and cupping, representing transitory therapeutic petechiae and ecchymosis that fade in 3–5 days.
Evidence
Changes from Gua sha and Ba guan are commonly felt immediately and are sustained, to some degree, over time, where repeating treatment may be indicated to reach maximum benefit. The recovery of the tissue is expressed by immediate improvement in myofascial pain, with changes in pulse, tongue, digestion, urine, stool, sleep, libido, flexibility, mood and so on (Nielsen 2013). In the language of TEAM Gua sha and Ba guan: resolve blood stasis and pain related to stasis, dredge the channels, vent heat, and quicken internal organ function
.
Chinese randomized controlled trials (RCTs), comparative studies and case series apply Gua sha for adult and pediatric painful musculoskeletal conditions, acute infectious illness, respiratory conditions, autoimmune and inflammatory disorders including organ disease states (Nielsen 2013). In Western RCTs Gua sha was found to be effective in painful breast engorgement, mastitis (Chiu et al. 2010), chronic neck pain (Braun et al. 2011), and for chronic neck and back pain (Lauche et al. 2012b). A 2017 systematic review with network analysis found that compared with placebo-sham, acupuncture and Gua sha combined with warming acupuncture and moxibustion
were effective for decreasing pain intensity in myofascial pain syndrome (Li et al. 2017b).
Figure 11.3
Palpating for sha.
Compared to controls, 8 weeks of weekly Gua sha therapy decreased perimenopausal symptoms: hot flashes, sweating, paresthesia, insomnia, nervousness, melancholia, fatigue and headache (Meng et al. 2017). The benefits in these perimenopausal symptoms were not mediated by any changes in serum estrogen, follicle-stimulation hormone or luteinizing hormone.
Gua sha has been shown to improve muscle strength of university students performing a bench press (Zhao et al. 1995) and to enhance the performance of weightlifters where a series of Gua sha treatments allowed greater weight to be lifted while the subject’s weight sense remained stable (Wang et al. 2014). This benefit may relate to interoceptive nerve stimulation altering sympathetic output, which increases local blood flow, and matrix hydration, as discussed below. Gua sha was found to benefit parasympathetic nervous activity and modulate heart rate variability (HRV) in healthy men and weightlifters (Wang et al. 2015). In the latter trial, serum markers showed a sparing of creatinine kinase (CK) and blood urea nitrogen (BUN) that is associated with exertional muscle damage indicating the potential of Gua sha to facilitate muscle and fascia loading in athletic performance.
Cupping has been described in Western medical literature longer than Gua sha (Dekkers 1694). In systematic reviews of trials, the main purpose of cupping therapy was to relieve pain, whether related to disease or musculoskeletal problems (Cao et al. 2010, Cao et al. 2012). A 2017 systematic review found cupping to be comparable to acupuncture in relieving pain related to cervical spondylosis, scapulohumeral periarthritis and lateral femoral cutaneous neuritis (Zhang et al. 2017). Dry cupping has been found effective for neck pain (Lauche et al. 2011, Lauche et al. 2012a, Lauche et al. 2013a), chronic neck and shoulder pain (Chi et al. 2016), carpal tunnel syndrome (Michalsen et al. 2009) and equal to E-stim for plantar fasciitis (Ge et al. 2017). Home-based cupping ‘massage’ was found superior to progressive muscle relaxation in patients with chronic neck pain (Lauche et al. 2013b).
As with acupuncture therapy, Gua sha and Ba guan are applied segmentally to a region of interest (Nielsen 2013). This creates more petechial substrate and increases areas of tissue stretch, which, per TEAM perspective, resolves stasis, and supplies and drains an affected area. For example, in treating carpal tunnel syndrome, Gua sha is applied to the neck, shoulder area, upper back and then the arm (Nielsen 2013, Braun et al. 2011). In a trial of cupping for carpal tunnel syndrome, cups were applied to the trapezius muscle on the affected side (Michalsen et al. 2009).
Contraindications
Gua sha and dry cupping are contraindicated where the dermis or flesh is injured or compromised as in sunburn, abrasion, rash or contusion. Gua sha or Ba guan are indicated for injury but are not applied directly at the area of trauma but adjacent, proximal or distal to a site. Gua sha and Ba guan are always applied to areas that are relaxed, allowing for painless tissue stretch and expression of petechiae (Nielsen 2013).
Gua sha, Ba guan and acupuncture are contraindicated in areas where a patient has regularly used topical antibiotics or steroid creams as in eczema, for example (see
Safety
below), since such topicals increase the risk of colonization of
Staphylococcus
or even MRSA at the skin (Hon et al. 2013), whereby penetrating treatment can deepen the pathogen into the body causing systemic infection.
Gua sha and Ba guan are safe for patients who are weak or menstruating, or pregnant. Effective manual techniques may be preferable to some medications that may carry risk in pregnancy, for sinusitis, colds and cough, for headache, neck, shoulder, back and hip pain, and sciatica. Gua sha and Ba guan can be used safely in patients with a stable INR (International
Normalized Ratio) who take anticoagulation medication because the capillary bed is not damaged with Gua sha (Nielsen et al. 2007). With Ba guan, the practitioner must be attentive to the amount of suction and length of application of the cups to avoid hematoma, erroneously attributed to acupuncture by Kenz et al. (2012).
Biomechanism/physiology
Observation
When applying Gua sha, the practitioner experiences a clear stretching of the surface tissue with a gradual expression of small red petechiae (sometimes brown, blue, very deep red or nearly black). Gua sha is continued until all the sha is expressed, something gained from experience. The patient often feels exhilarated, invigorated, even excited. Pain is immediately affected, sometimes completely resolved. Nausea and vomiting cease, wheezing, shortness of breath and/or coughing lessen or completely resolve (Nielsen 2013). It is the closely timed repeated press-stroking and unidirectionality that facilitates the appearance of petechiae. And it is the myofascial stretching, the intentional extravasation of petechiae and their resolution over time that has unique physiological significance.
When applying cups, a practitioner observes surface tissue draw into the cup. The expression of petechiae may be similar if slower. Stationary cups reduce the area of sha expression seen with Gua sha or moving cups. Patients also report a shift in symptoms including improvement in pain and mobility.
Patients experience a warming effect with both Gua sha and Ba guan, with a notable adaptogenic response where a cold or chilled patient will become warm and a patient who has fever or is overheated, as in sunstroke, will have heat and stasis ‘vented’ (Nielsen 2013).
Biological measures
Biologic research contributes to a partial and building knowledge of the therapeutic physiology involved with Gua sha and Ba guan. Basic lab studies in perfusion, temperature and serum markers help to contextualize the immediate and longitudinal effects.
Perfusion
Gua sha increases surface microperfusion 400% for 7.5 minutes and significantly for 25 minutes after treatment at but not outside a treated area, while immediately reducing pain locally and distally (Nielsen et al. 2007). Skin blood flow increases with moving dry cupping, the technique that is closer to Gua sha, at 10 minutes following treatment (Tian et al. 2013). Increase in local blood oxygen at and surrounding a treatment site is reported in a five-minute cupping study that produced nummular petechiae similar to Gua sha (Li et al. 2017a).
Temperature
Gua sha and Ba guan treatment both result in sense of warming in the area treated, with measured increase in surface skin temperature (Xu et al. 2012, Chi et al. 2016). It is important to note that while there is an established increase in temperature, this may or may not result in an increase in overall body temperature, but rather, as in the case of fever and inflammation, results in a reduction.
Pain, inflammation and immunity
Nitric oxide (NO) mediation
Nitric oxide (NO) is an important mediator in both health and disease affecting smooth muscle relaxation, vasodilatation, platelet function, inflammation, and pain perception (Mackenzie et al. 2008) with roles in angiogenesis, neurotransmission and wound healing (Nichols et al. 2012). Blood flow is normalized in the presence of NO which may reduce ischemic pain and inflammation, even with small amounts of transiently produced NO (Abramson 2008). Nitric oxide’s action on physiology is highly dependent on location, source, and concentration (Nichols et al. 2012). While nitric oxide is a small molecule
produced in confined compartments within different types of cells, its site-specific effects are sensed throughout the entire organism. The effects of this molecule at the organism level are not the result of a long half-life, high stability or free diffusion, but the consequence of localized effects of nitric oxide at various cellular levels and in different cell types, modulating and orchestrating complex responses requiring cross-talk among organs (Villanueva & Giulivi 2010). Production of NO in the process of increased perfusion and vasodilation is one hypothesis for the immediate pain relief experienced locally and distally with Gua sha (Nielsen 2013).
Acupuncture is associated with production of nitric oxide (Tsuchiya et al. 2007) with authors suggesting that regional increase in NO accounts for changes in local circulation and that both are implicated in the complex analgesic effect of acupuncture. NO contribution has shown potential benefit in wound healing from increase in NO secretion, sensitivity or both (Cao et al. 2013), including burn wounds and in connective tissue repair (Nichols et al. 2012). NO release from fibroblasts promotes collagen synthesis, highlighting the potential of NO-releasing therapies in tendon repair (Witte et al. 2000). In an observational study of 1008 patients including children, acupuncture given as first aid immediately after, optimally within 48 hours, of a burn injury reduced pain, reddening, pigmentation, scarring and PTSD that commonly follows traumatic burns (Loskotova & Loskotova 2017).
Other manual therapies have been studied in terms of their release of NO including osteopathic manipulation (Salamon et al. 2004), cranial–thoracic trapezius stretch (Kiernan 2010), and self-myofascial release using a foam roller also shown to reduce arterial stiffness (Okamoto et al. 2014), increase joint range of motion, muscle recovery and performance (Cheatham et al. 2015). In vitro study found that reduced wound closure rates and enhanced cell death activity in response to injurious repetitive motion strain was attenuated by a single dose of modeled myofascial release (Cao et al. 2013, Meltzer et al. 2010).
Interoception
Interoception is the sense of the physiological condition of the body, which includes muscle effort and homeostasis sensations such as the need to get warm, urinate, train or to run. Interoceptive nerve endings are prevalent in muscle tissue. With a large initial drop in interstitial fluid pressure at the onset of acute inflammation (Langevin et al. 2013), stimulation of interoceptive receptors results in increased matrix hydration via plasma extravasation (Schleip 2003) as is seen with Gua sha and Ba guan. Gua sha’s potential to alter interoception is seen in enhanced athletic performance, muscle and fascia loading (Wang et al. 2015).
Ferroheme metabolism: upregulation of heme oxygenase-1 (HO-1)
Extravasated petechiae immediately change to ecchymosis, blend and fade over 3–5 days with Gua sha and a bit longer for cupping depending on the extent of pressure and length of time the cups are applied (Zhao et al. 2009). The resolution of petechiae involves what is called the ferroheme metabolic pathway. Extravasated blood cells are re-absorbed and metabolized, catalyzing the transformation of ferroheme into biliverdin, carbon monoxide (CO), and free iron with upregulation of genetic expression of HO-1. HO-1 is the rate-limiting enzyme of the ferroheme metabolic pathway that has the functions of anti-oxidation, anti-inflammation, anti-apoptosis and anti-smooth muscle hyperplasia (Xia et al. 2008). A Harvard study has shown Gua sha upregulates genetic expression of HO-1 at multiple internal organ sites and over a period of days following a single treatment (Kwong et al. 2009).
Activation HO-1 is described as an adaptive response in tissue injury (Agarwal & Bolisetty 2013).
A study of acute exercise such as a half marathon (Thompson et al. 2005), but not a short exhaustive run or ‘eccentric’ exercise (Fehrenbach et al. 2003), increased HO-1 mRNA accumulation in human lymphocytes (Thompson et al. 2005). HO-1 is an emerging therapeutic target in many disease models such as asthma, organ transplant rejection, inflammatory bowel disease and experimental autoimmune encephalomyelitis, even though the immune pathological mechanisms of these diseases are dissimilar (Xia et al. 2008).
Upregulation of HO-1 has been reported to be effective in the control of hepatitis B virus (HBV) infection and offers hepatoprotection in animal models (Protzer et al. 2007, Wunder & Potter 2003). Induction of HO-1 decreases hepatitis C virus (HCV) replication, as well as protecting against oxidative damage, suggesting a potential role for HO-1 in antiviral therapy and therapeutic protection against hepatocellular injury in HCV infection (Zhu et al. 2008). Even before discovery of these mechanisms, Gua sha has been used and studied for acute and chronic hepatitis in China (Nielsen 2013). Chan et al. (2011) describe a case in a Western journal where a single Gua sha treatment in a patient with active chronic hepatitis reduced levels of liver enzymes, modulated T-helper (Th)1/Th2 balance and enhanced HO-1, which they suggest is responsible for the hepatoprotective effect (Chan et al. 2011).
While Gua sha provides an anti-inflammatory rescue to an inflamed liver, it does not alter liver function in healthy subjects (Chan et al. 2013). Benefit for hepatitis is not attributed to placebo as ‘liver status’ is not subject to expectation.
HO-1 can exert a significant antiviral activity against a wide variety of viruses, including HIV, hepatitis C virus, hepatitis B virus, ‘enterovirus 71’, influenza virus, respiratory syncytial virus, dengue and Ebola virus (Espinoza et al. 2017) and acute inflammatory, infectious even neoplastic gastrointestinal disease (Chang et al. 2015). A single Gua sha treatment has been shown to increase the immune response to intradermal vaccination (Chen et al. 2016).
Connective tissue model
Painful conditions or illness may be accompanied by altered or inflamed connective tissue and are observed to respond to manual therapies, including Gua sha and cupping. Palpable sensations of physical release reported by manual therapists cannot be due to ‘deformations produced’ in the firm or dense fascial tissue, since dense fascial tissues require very large forces, far outside human physiologic range, to produce even a 1% compression or shear (Chaudhry et al. 2008). Rather, manual therapy may stimulate fascial mechanoreceptors that trigger tonus changes in connected skeletal muscles, in addition to NO relaxation of skeletal muscles vis-à-vis vasodilation.
Subcutaneous tissue is a part of a bodywide network of ‘loose’ connective tissue that is intimately associated with all other tissues, including organ systems (Langevin 2006). ‘Loose’ connective tissues serve to transmit mechanical signals to and from abundant fibroblasts, immune, vascular and neural cells present within tissues (Iatridis et al. 2003). They generate dynamic evolving patterns that interact with one another as a ‘body-wide mechanosensitive signaling network’ that influences, and is influenced by, function that is normal, pathological (Langevin et al. 2006, Langevin 2006) and, by inference, responsive to manual intervention.
The channels of TEAM communicate through what the ancients called the ‘li’ or ‘cou li’ lining which corresponds to fascia and connective tissue (Nielsen 2013, Lin and Yu 2009) (
Fig. 11.4
). TEAM was the first medical system to propose this ‘lining’ as an actual organ, the San Jiao or Triple Burner (Unschuld 1986), the only organ that lacked a recognized Western analogous structure, until the relatively recent focus on fascia and connective tissue. The San Jiao governs and links the ‘exterior with the interior’, the outer flesh to the organs via the channels that reside in the ‘li’, lining (Epler 1980, Unschuld 1986); hence the fundamental construct of a global physiologic network that coincides with the connective tissue model (Langevin 2006, Langevin & Yandow 2002).
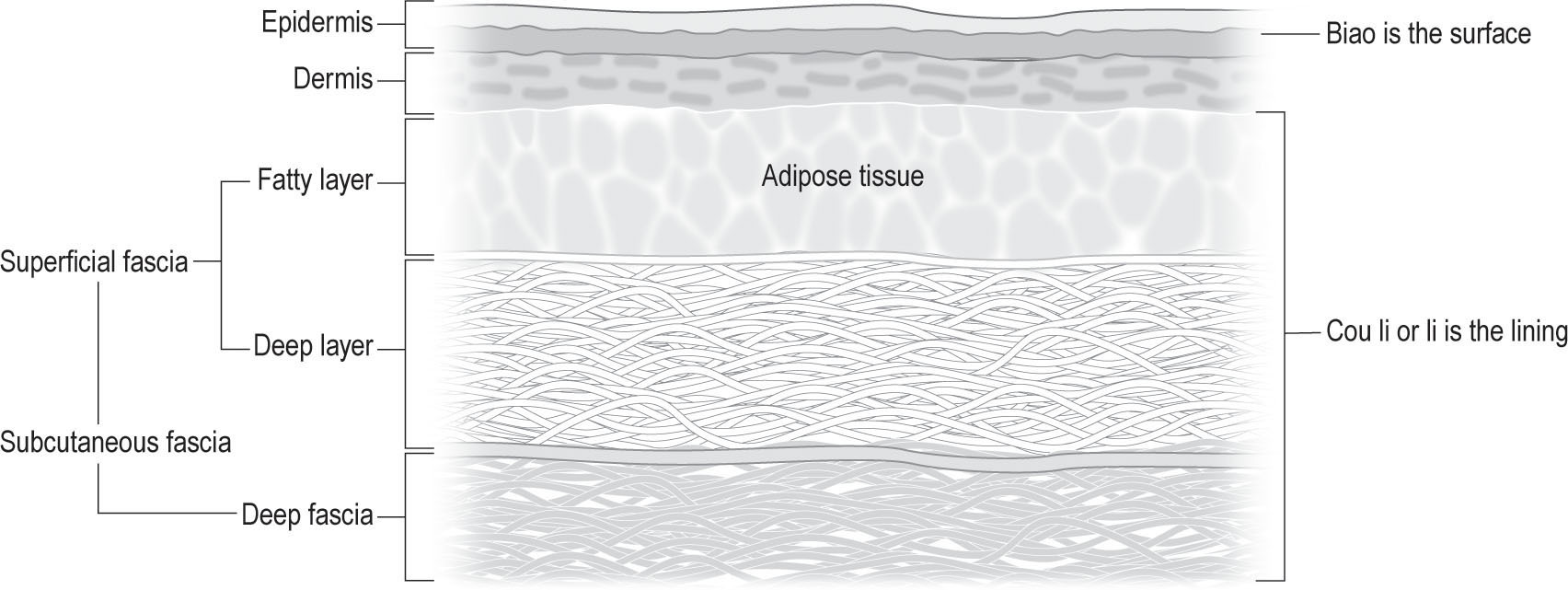
Figure 11.4
Western and Eastern surface anatomy. Biao is the surface. The Cou Li, or lining, corresponds to the superficial fascia in Western anatomy. Arteries, veins, nerves, lymph vessels and nodes run through the deep layer of superficial fascia and Jing Lo vessels also run through this layer. Wei Qi moves through the fatty layer. From Nielsen A 2013 Gua sha, a traditional technique for modern practice, 2nd edn. Churchill Livingstone Elsevier, Edinburgh, p 34, with permission.
Connective tissue is sensitive to directionality of manual therapy. Dense ‘regular’ connective tissue of tendons, ligaments, aponeuroses and intermuscular septa respond to tensile loading with collagen strands in parallel arrangement along the direction of the loads imposed (Langevin & Huijing 2009).
Directionality
Gua sha and Ba guan share in the NO release associated with manual therapies, but to a greater degree with the increased vasodilation seen with Gua sha or Ba guan. Directionality of manual therapy also elicits a specific response. Acupuncture needle rotation that is unidirectional produces more torque in connective tissue that is, in turn, more responsive, than to bi-directional rotation (Langevin et al. 2007). Endothelial constitutive nitric oxide synthase (ecNOS) mRNA expression has been shown to be time- and mechanical force-dependent (Ziegler et al. 1998b) wherein the effect of unidirectional force or stress differs from oscillating or alternating force or stress in vascular endothelium production of nitric oxide (Ziegler et al. 1998a).
The mechanical response behavior of ‘loose’ connective tissue is linear and viscoelastic under uniaxial tension (Iatridis et al. 2003). Anti-inflammatory cytokine secretion is activated by directionality of myofascial release: pressure and shear that create uni-axial fibroblast strain can account for improved range of motion (ROM), decreased edema, and reduced analgesic requirements as well as for ‘long-term benefits despite short-term treatment’ (Meltzer et al. 2010, Standley & Meltzer 2008). Gua sha is always applied with unidirectional stroking. While dry cupping may
be stationary or slow gliding bidirectionally, it is typically with and not across the muscle fiber direction.
Safety
The most significant and consistent complication reported in the Western medical literature for Gua sha is the misattribution of the sha petechiae and ecchymosis as a burn, bruise, or dermatitis/factitial dermatitis caused by ‘abuse’, ‘battery’, ‘torture’, ‘pseudo-abuse’ (Nielsen et al. 2007; Nielsen 2009). This ignorance and bias represents a risk to patients that can be mitigated by providing a handout explaining the technique, describing the normal presence of therapeutic petechiae, and providing the clinician’s contact information (
www.guasha.com
).
A report of acute epiglottitis following Gua sha at the trachea represents a negligent use and not a side effect or risk of appropriate Gua sha (Tsai & Wang 2014). Adverse events associated with negligent cupping include suction bullae blisters, fire cupping burns, psoriatic Koebner phenomenon, factitial panniculitis, keloid formation, and
Staphylococcus
, herpes simplex, and
Mycobacterium
infection (Xu et al. 2013, Nielsen 2015, Hon et al. 2013).
Practitioners need to be aware of patients who may have an increased risk of infection – have reduced immune response via disease, chemotherapy, steroids or other immune suppressant medication, altered skin barrier, use of topical steroids or antibiotics that may in turn increase colonization of staph and MRSA (Nielsen 2015).
Universal precautions and contamination risks
Gua sha and cupping instruments that are intended for re-use are considered semi-critical instruments according to the Centers for Disease Control and Prevention (CDC) and must be high-level disinfected or sterilized before reuse (Rutala et al. 2008). Because bone and horn tools cannot sustain high-level disinfection or sterilization required, single-use disposable caps with a smooth edge are recommended (Nielsen et al. 2012, Nielsen et al. 2014). Dedicated instruments intended for specific patients must also be sterilized or high-level disinfected between each use to be compliant with CDC standards.
References
Abramson SB 2008 Nitric oxide in inflammation and pain associated with osteoarthritis. Arthritis Res Ther 10:S2–S2
Agarwal A, Bolisetty S 2013 Adaptive responses to tissue injury: role of heme oxygenase-1. Trans Am Clin Climatol Assoc 124:111–122
Al Bedah AM, Khalil MK, Posadzki P et al 2016 Evaluation of wet cupping therapy: systematic review of randomized clinical trials. J Alt Complement Med 22:768–777
Baerheim A, Laerum E 1992 Symptomatic lower urinary tract infection induced by cooling of the feet. A controlled experimental trial. Scand J Prim Health Care 10:157–160
Braun M, Schwickert M, Nielsen A et al 2011 Effectiveness of traditional Chinese “gua sha” therapy in patients with chronic neck pain: a randomized controlled trial. Pain Med 12:362–369
Cao H, Han M, Li X et al 2010 Clinical research evidence of cupping therapy in China: a systematic literature review. BMC Complement Altern Med 10:70.
Cao H, Li X, Liu J 2012 An updated review of the efficacy of cupping therapy. PloS One 7:e31793
Cao TV, Hicks MR, Standley PR 2013 In vitro biomechanical strain regulation of fibroblast wound healing. J Am Osteopath Assoc 113:806–818
Chaitow L 2012 The ARTT of palpation? J Bodyw Mov Ther 16:129–131
Chaitow L, Delany J 2011 Clinical application of neuromuscular techniques, vol 2: the lower body. Churchill Livingstone, Elsevier, Edinburgh
Chan ST, Yuen JW, Gohel MD et al 2011 Guasha-induced hepatoprotection in chronic active hepatitis B: a case study. Clin Chim Acta 412:1686–1688
Chan ST, Yuen JW, Gohel MD et al 2013 Does guasha offer hepatoprotective effect to chronic inactive hepatitis B carriers? A built-in design to control subject expectation. J Altern Complement Med 19:772–776
Chang M, Xue J, Sharma V et al 2015 Protective role of hemeoxygenase-1 in gastrointestinal diseases. Cell Mol Life Sci 72:1161–1173
Chaudhry H, Schleip R, Ji Z et al 2008 Three-dimensional mathematical model for deformation of human fasciae in manual therapy. J Am Osteopath Assoc 108:379–390
Cheatham SW, Kolber MJ, Cain M et al 2015 The effects of self-myofascial release using a foam roll or roller massager on joint range of motion, muscle recovery and performance: a systematic review. Int J Sports Phys Ther 10:827–838
Chen T, Liu N, Liu J et al 2016 Gua Sha, a press-stroke treatment of the skin, boosts the immune response to intradermal vaccination. Peer J 4:e2451
Chi LM, Lin LM, Chen CL et al 2016 The effectiveness of cupping therapy on relieving chronic neck and shoulder pain: a randomized controlled trial. Evid Based Complement Altern Med 2016:7358918.
Chirali IZ 2014 Traditional Chinese medicine cupping therapy. Elsevier, Edinburgh
Chiu JY, Gau ML, Kuo SY et al 2010 Effects of Gua-Sha therapy on breast engorgement: a randomized controlled trial. J Nurs Res 18:1–10
Dekkers F 1694 Exercitationes Practicae. Lugduni Batavorum, Leiden.
Epler DCJ 1980 Bloodletting in early Chinese medicine and its relation to the origin of acupuncture. Bull Hist Med 54:337–367
Espinoza JA, Gonzalez PA, Kalergis AM 2017 Modulation of antiviral immunity by heme oxygenase-1. Am J Pathol 187:487–493
Fehrenbach E, Niess AM, Passek F et al 2003 Influence of different types of exercise on the expression of haem oxygenase-1 in leukocytes. J Sports Sci 21:383–389
Ge W, Leson C, Vukovic C 2017 Dry cupping for plantar fasciitis: a randomized controlled trial. J Phys Ther Sci 29:859–862
Hammer W 2014 Instrument-assisted soft tissue mobilization. In: Chaitow (ed) Fascial dysfunction: manual therapy approaches. Handspring Publishing, Edinburgh, Ch 12
Hon KL, Luk DC, Leong KF et al 2013 Cupping therapy may be harmful for eczema: a PubMed search. Case Rep Pediatr 2013:605829
Iatridis JC, Wu J, Yandow JA et al 2003 Subcutaneous tissue mechanical behavior is linear and viscoelastic under uniaxial tension. Connect Tissue Res 44:208–217
Ikaheimo TM, Jaakkola K, Jokelainen J et al 2016 A decrease in temperature and humidity precedes human rhinovirus infections in a cold climate. Viruses 8(9)
Jaakkola K, Saukkoriipi A, Jokelainen J et al 2014 Decline in temperature and humidity increases the occurrence of influenza in cold climate. Environ Health 13:22
Jackson H 1806 On the efficacy of certain external applications. University of Pennsylvania: New York Medical College Library Rare Books Room
Kenz S, Webb H, Laggan S 2012 Thigh haematoma following acupuncture treatment in a patient on warfarin. BMJ Case Rep 2012
Kiernan JE 2010 Effects of a manual medicine treatment procedures on nitric oxide release in 23 healthy adults. J Manipulative Physiol Ther 33:76–79
Kwong KK, Kloetzer L, Wong KK et al 2009 Bioluminescence imaging of heme oxygenase-1 upregulation in the Gua Sha procedure. J Vis Exp (30)
Langevin HM 2006 Connective tissue: a body-wide signaling network? Med Hypotheses 66:1074–1077
Langevin HM, Bouffard NA, Badger GJ et al 2006 Subcutaneous tissue fibroblast cytoskeletal remodeling induced by acupuncture: evidence for a mechanotransduction-based mechanism. J Cell Physiol 207:767–774
Langevin HM, Bouffard NA, Churchill DL et al 2007 Connective tissue fibroblast response to acupuncture: dose-dependent effect of bidirectional needle rotation. J Altern Complement Med 13:355–360
Langevin HM, Churchill DL, Cipolla MJ 2001 Mechanical signaling through connective tissue: a mechanism for the therapeutic effect of acupuncture. FASEB J 15:2275–2282
Langevin HM, Huijing PA 2009 Communicating about fascia: history, pitfalls, and recommendations. Int J Ther Massage Bodywork 2:1–6
Langevin HM, Nedergaard M, Howe AK 2013 Cellular control of connective tissue matrix tension. J Cell Biochem 114:1714–1719
Langevin HM, Yandow JA 2002 Relationship of acupuncture points and meridians to connective tissue planes. Anat Rec 269:257–265
Lauche R, Cramer H, Choi KE et al 2011 The influence of a series of five dry cupping treatments on pain and mechanical thresholds in patients with chronic non-specific neck pain--a randomised controlled pilot study. BMC Complement Altern Med 11:63
Lauche R, Cramer H, Hohmann C et al 2012a The effect of traditional cupping on pain and mechanical thresholds in patients with chronic nonspecific neck pain: a randomised controlled pilot study. Evid Based Complement Altern Med 2012:429718
Lauche R, Cramer H, Langhorst J et al 2013a Cupping for chronic nonspecific neck pain: a 2-year follow-up. Forsch Komplementmed 20:328–333
Lauche R, Materdey S, Cramer H et al 2013b Effectiveness of home-based cupping massage compared to progressive muscle relaxation in
patients with chronic neck pain--a randomized controlled trial. PloS One 8:e65378
Lauche R, Wubbeling K, Ludtke R et al 2012b Randomized controlled pilot study: pain intensity and pressure pain thresholds in patients with neck and low back pain before and after traditional East Asian “gua sha” therapy. Am J Chinese Med 40:905–917
Li T, Li Y, Lin Y et al 2017a Significant and sustaining elevation of blood oxygen induced by Chinese cupping therapy as assessed by near-infrared spectroscopy. Biomed Opt Express 8:223–229
Li X, Wang R, Xing X et al 2017b Acupuncture for myofascial pain syndrome: a network meta-analysis of 33 randomized controlled trials. Pain Physician 20:e883–e902
Lin Y, Yu B 2009 Anatomical discovery of meridians and collaterals. Fascia Congress 2009, Amsterdam:
www.fasciacongress.org
.
Loskotova A, Loskotova J 2017 The use of acupuncture in first aid of burns - Clinical report. Burns 43(8):1782–1791
Lu G-D, Needham J 1980 Celestial lancets: a history and rationale of acupuncture and moxa. Cambridge University Press, Cambridge
Mackenzie IS, Rutherford D, MacDonald TM 2008 Nitric oxide and cardiovascular effects: new insights in the role of nitric oxide for the management of osteoarthritis. Arthritis Res Ther 10(Suppl 2):S3
Manz H 2009 The art of cupping. Thieme, New York
Meltzer KR, Cao TV, Schad JF et al 2010 In vitro modeling of repetitive motion injury and myofascial release. J Bodyw Mov Ther 14:162–171
Meng F, Duan PB, Zhu J et al 2017 Effect of Gua sha therapy on perimenopausal syndrome: a randomized controlled trial. Menopause 24:299–307
Michalsen A, Bock S, Ludtke R et al 2009 Effects of traditional cupping therapy in patients with carpal tunnel syndrome: a randomized controlled trial. J Pain 10:601–608
Mourtzoukou EG, Falagas ME 2007 Exposure to cold and respiratory tract infections. Int J Tuberc Lung Dis 11:938–943
Nichols SP, Storm WL, Koh A et al 2012 Local delivery of nitric oxide: targeted delivery of therapeutics to bone and connective tissues. Adv Drug Deliv Rev 64:1177–1188
Nielsen A 1996 Gua sha as counteraction: the crisis is the cure. J Chin Med 50:4–10
Nielsen A 2009 Gua sha research and the language of integrative medicine. J Bodyw Mov Ther 13:63–72
Nielsen A 2013 Gua sha, a traditional technique for modern practice. Churchill Livingstone Elsevier, Edinburgh
Nielsen A 2015 Safety: reports, risks and guidelines for Gua sha (press-stroking) and Ba guan (cupping). Gua sha Certification Course. ProD Seminars
Nielsen A, Kligler B, Koll BS 2012 Safety protocols for gua sha (press-stroking) and baguan (cupping). Complement Ther Med 20:340–344
Nielsen A, Kligler B, Koll BS 2014 Addendum: Safety standards for Gua sha (press-stroking) and Ba guan (cupping). Complement Ther Med 22:446–448
Nielsen A, Knoblauch NT, Dobos GJ et al 2007 The effect of Gua Sha treatment on the microcirculation of surface tissue: a pilot study in healthy subjects. Explore (NY) 3:456–466
Okamoto T, Masuhara M, Ikuta K 2014 Acute effects of self-myofascial release using a foam roller on arterial function. J Strength Conditioning Res 28:69–73
Protzer U, Seyfried S, Quasdorff M et al 2007 Antiviral activity and hepatoprotection by heme oxygenase-1 in hepatitis B virus infection. Gastroenterology 133:1156–1165
Ruan Z-Q, Cui Y 2005 Gua sha treatment for sunstroke. J. Ningde Teachers College (Natural Science) 17:410–411
Rutala WA, Weber DJ, Committee HICPA 2008 Guideline for disinfection and sterilization in healthcare facilities. Centers for Disease Control and Prevention (CDC), Atlanta, GA
Salamon E, Zhu W, Stefano GB 2004 Nitric oxide as a possible mechanism for understanding the therapeutic effects of osteopathic manipulative medicine (Review). Int J Mol Med 14:443–449
Schleip R 2003 Fascial plasticity – a new neurobiological explanation, Part 2. J Bodyw Mov Ther 7:104–116
So JTY 1987 Treatment of disease with acupuncture. Paradigm, Brookline, MA
Standley PR, Meltzer K 2008 In vitro modeling of repetitive motion strain and manual medicine treatments: potential roles for pro- and anti-inflammatory cytokines. J Bodyw Mov Ther 12:201–203
Thompson D, Basu-Modak S, Gordon M et al 2005 Exercise-induced expression of heme oxygenase-1 in human lymphocytes. Free Radic Res 39:63–69
Tian YY, Wang GJ, Huang T et al 2013 [Impacts on skin blood flow under moving cupping along meridians in different directions]. Zhongguo Zhen Jiu 33:247–251
Tsai KK, Wang CH 2014 Acute epiglottitis following traditional Chinese gua sha therapy. CMAJ 186:E298
Tsuchiya M, Sato EF, Inoue M et al 2007 Acupuncture enhances generation of nitric oxide and increases local circulation. Anesth Analg 104:301–307
Unschuld PU 1986 Nan-Ching, the classic of difficult questions. University of California Press, Berkeley, CA
Villanueva C, Giulivi C 2010 Subcellular and cellular locations of nitric-oxide synthase isoforms as determinants of health and disease. Free Radic Biol Med 49:307–316
Wang X, Chatchawan U, Nakmareong S et al 2015 Effects of GUASHA on heart rate variability in healthy male volunteers under normal condition and weightlifters after weightlifting training sessions. Evid Based Complement Alternat Med 2015:268471
Wang X, Eungpinichpong W, Yang J et al 2014 Effect of scraping therapy on weightlifting ability. J Trad Chin Med 34:52–56
Weiger L 1965 Chinese characters, their origin, etymology, history, classification and signification: a thorough study from Chinese documents. Dover, New York
Witte MB, Thornton FJ, Efron DT et al 2000 Enhancement of fibroblast collagen synthesis by nitric oxide. Nitric Oxide 4:572–582
Wunder C, Potter RF 2003 The heme oxygenase system: its role in liver inflammation. Curr Drug Targets Cardiovasc Haematol Disord 3:199–208
Xia ZW, Zhong WW, Meyrowitz JS et al 2008 The role of heme oxygenase-1 in T cell-mediated immunity: the all encompassing enzyme. Curr Pharm Des 14:454–464
Xu QY, Yang JS, Zhu B et al 2012 The effects of scraping therapy on local temperature and blood perfusion volume in healthy subjects. Evid Based Complement Altern Med 2012:490292
Xu S, Wang L, Cooper E et al 2013 Adverse events of acupuncture: a systematic review of case reports. Evid Based Complement Altern Med 2013:581203.
Zhang X, Hao W 2000 Holographic meridian scraping therapy. Foreign Language Press, Beijing
Zhang YJ, Cao HJ, Li XL et al 2017 Cupping therapy versus acupuncture for pain-related conditions: a systematic review of randomized controlled trials and trial sequential analysis. Chin Med 12:21
Zhao XX, Tong BY, Wang XX et al 2009 [Effect of time and pressure factors on the cupping mark color]. Zhongguo Zhen Jiu 29: 385–388
Zhao ZL, Yin KJ, Liu WB 1995 The study of Traditional Chinese Medicine to the effect of upper limb function in bench press. Shanxi J Trad Chin Med 18:34–35
Zhu Z, Wilson AT, Mathahs MM et al 2008 Heme oxygenase-1 suppresses hepatitis C virus replication and increases resistance of hepatocytes to oxidant injury. Hepatology 48:1430–1439
Ziegler T, Bouzourene K, Harrison VJ et al 1998a Influence of oscillatory and unidirectional flow environments on the expression of endothelin and nitric oxide synthase in cultured endothelial cells. Arterioscler Thromb Vasc Biol 18:686–692
Ziegler T, Silacci P, Harrison VJ et al 1998b Nitric oxide synthase expression in endothelial cells exposed to mechanical forces. Hypertension 32:351–355



Patient reports pain that is fixed, persistent or recurring
Patient reports pain that is fixed, persistent or recurring
