Gastrointestinal Disease
Gastroesophageal Reflux Disease (GERD)
Acute Gastroenteritis and Diarrhea
AUTOIMMUNE (CHRONIC) HEPATITIS
Esophageal Atresia
 A full-term infant was noted to have copious oral secretions requiring frequent suctioning
to prevent choking. Attempts to place a nasogastric tube were unsuccessful, with the
tube curling in the esophagus. X-ray is shown in the figure. What is the likely diagnosis
and management of this condition?
A full-term infant was noted to have copious oral secretions requiring frequent suctioning
to prevent choking. Attempts to place a nasogastric tube were unsuccessful, with the
tube curling in the esophagus. X-ray is shown in the figure. What is the likely diagnosis
and management of this condition?
The nasogastric tube with the tip in the proximal esophagus and failure to advance further signifies an esophageal atresia. The most common type is where the proximal esophagus ends in a blind pouch (as in this case) and there is a distal tracheoesophageal fistula. Also evident are ribs and vertebral anomalies in this case. This could be part of VATER (vertebral anomalies, anal atresia, tracheoesophageal anomalies, renal anomalies) syndrome. Infant was noted to have a single right kidney on renal ultrasound. Management includes surgical repair of the tracheoesophageal fistula.
 EXAM TIP
EXAM TIP
Esophageal atresia can be associated with the VACTERL sequence:
Vertebral
Anorectal
Cardiac
Tracheal
Esophageal
Renal
Limb anomalies
DEFINITION
 The esophagus ends blindly ~10–12 cm from the nares.
The esophagus ends blindly ~10–12 cm from the nares.
Occurs in 1/3000–1/4500 live births.
In 85% of cases the distal esophagus communicates with the posterior trachea (distal
tracheoesophageal fistula [TEF]).
 WARD TIP
WARD TIP
Suspect esophageal atresia in a neonate with drooling and excessive oral secretions.
SIGNS AND SYMPTOMS
History of maternal polyhydramnios.
Newborn with ↑ oral secretions.
Choking, cyanosis, coughing during feeding (more commonly aspiration of pharyngeal
secretions).
Esophageal atresia with fistula.
Aspiration of gastric contents via distal fistula—life threatening (chemical pneumonitis).
Tympanitic distended abdomen.
Esophageal atresia without fistula.
Recurrent coughing with aspiration pneumonia (delayed diagnosis).
Aspiration of pharyngeal secretions common.
Airless abdomen on abdominal x-ray.
WARD TIP
Inability to pass a rigid nasogastric tube from the mouth to the stomach is diagnostic of esophageal atresia.
DIAGNOSIS
Usually made at delivery.
Unable to pass nasogastric tube (NGT) into stomach (see coiled NGT on chest x-ray).
May also use contrast radiology, video esophagram, or bronchoscopy.
Chest x-ray (CXR) demonstrates air in upper esophagus (see Figure 11-1).
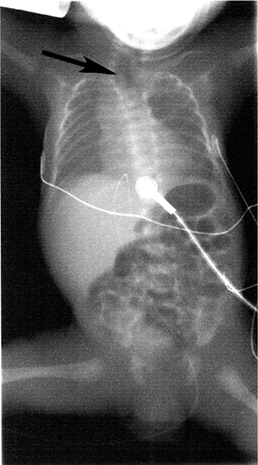
FIGURE 11-1. Esophageal atresia. Radiograph demonstrating air in the upper esophagus (arrow) and GI tract, consistent with esophageal atresia.
TREATMENT
Surgical repair (may be done in stages).
Esophageal Foreign Body
Most commonly due to swallowing of radiopaque objects: Coins, pins, pills, screws,
and batteries.
Preexisting abnormalities (i.e., tracheoesophageal repair) result in ↑ risk of
having foreign body impaction at site of abnormality.
WARD TIP
The most common site of esophageal impaction is at the thoracic inlet.
Site of impaction:
70%: Thoracic inlet (between clavicles on CXR).
15%: Midesophagus.
15%: Lower esophageal sphincter (LES).
SIGNS AND SYMPTOMS
Gagging/choking.
Difficulty with secretions.
Dysphagia/food refusal.
Throat pain or chest pain.
Emesis/hematemesis.
DIAGNOSIS
History, sometime witnessed event.
X-ray (AP/lateral CXR; see Figure 11-2).
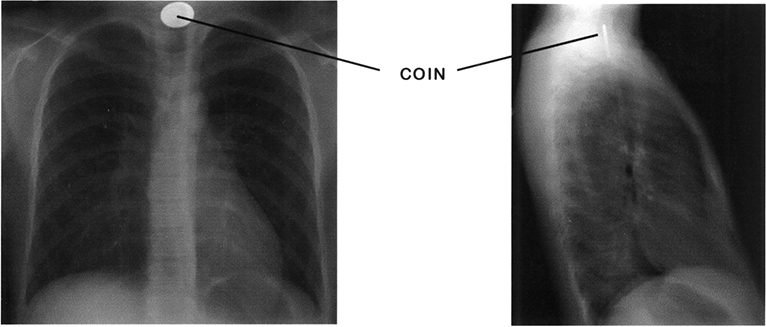
FIGURE 11-2. Esophageal foreign body. A coin in the esophagus will be seen flat or en face on an AP radiograph, and on its edge on a lateral view. (Used with permission from Dr. Julia Rosekrans.)
TREATMENT
Objects found within the esophagus are generally considered impacted.
Generally require endoscopic treatment if symptomatic or fail to pass to stomach
(below diaphragm on x-ray) within a few hours.
Impacted objects, pointed objects, and batteries must be removed immediately.
Important to assess time of ingestion; >24 hours can → erosion or necrosis of esophageal
wall.
WARD TIP
Button batteries may rapidly cause local necrosis.
Gastroesophageal Reflux Disease (GERD)
An 8-month-old preterm infant has been hospitalized for 4 months in the neonatal
care unit. In the past 2 weeks, the nurses have noted that he is regurgitating several
times an hour. He makes chewing movements preceding these episodes of regurgitation.
Think: Rumination.
Gastroesophageal reflux (GER) is common in preterm infants. Transient relaxation of the lower esophageal sphincter is the most common mechanism implicated. Signs and symptoms include apnea, chronic lung disease, poor weight gain, and behavioral symptoms. Frequent regurgitation and feeding difficulties may occur.
DEFINITION
Passive reflux of gastric contents due to incompetent lower esophageal sphincter
(LES).
Approximately 1 in 300 children suffer from significant reflux and complication.
Functional gastroesophageal reflux is most common.
RISK FACTORS
Prematurity.
Neurologic disorders.
Incompetence of LES due to prematurity, asthma.
Medications (theophylline, calcium channel blockers or β-blockers).
SIGNS AND SYMPTOMS
Excessive spitting up in the first week of life (in 85% of affected).
Symptomatic by 6 weeks (10%).
Symptoms resolve without treatment by age 2 (60%).
Forceful vomiting (occasional).
Aspiration pneumonia (30%).
Chronic cough, wheezing, and recurrent pneumonia (later childhood).
Rarely may cause laryngospasm, apnea, and bradycardia.
Regurgitation.
WARD TIP
GERD is the etiology for Sandifer syndrome (reflux, back arching, stiffness, and torticollis). Sandifer syndrome is most often confused with a neurologic or apparent life-threatening event.
DIAGNOSIS
Clinical assessment in mild cases.
Esophageal pH probe studies and barium esophagography in severe cases.
Esophagoscopy with biopsy for diagnosis of esophagitis.
TREATMENT
Positioning following feeds—keep infant upright up to an hour after feeds.
In older children, mealtime more than 2 hours before sleep and sleeping with head
elevated.
Thickening formula with rice cereal.
Medications:
Antacids, histamine-2 (H2) blockers (ranitidine), and proton pump inhibitors (PPIs; omeprazole).
Motility agents such as metoclopramide and erythromycin (stimulate gastric emptying).
Surgery—Nissen fundoplication.
Peptic Ulcer
DEFINITION
Includes primary and secondary (related to stress).
SIGNS AND SYMPTOMS
Primary—pain, vomiting, and acute and chronic gastrointestinal (GI) blood loss.
First month of life: GI hemorrhage and perforation.
Neonatal—2 months: Recurrent vomiting, slow growth, and GI hemorrhage.
Preschool: Periumbilical and postprandial pain (with vomiting and hemorrhage).
>6 years: Epigastric abdominal pain, acute/chronic GI blood loss with anemia.
Secondary:
Stress ulcers secondary to sepsis, respiratory or cardiac insufficiency, trauma,
or dehydration in infants.
Related to trauma or other life-threatening events (older children).
Stress ulcers and erosions associated with burns (Curling ulcers).
Ulcers following head trauma or surgery usually Cushing ulcers.
Drug related—nonsteroidal anti-inflammatory drugs (NSAIDs) or steroids.
Infectious––Helicobacter pylori.
DIAGNOSIS
Upper GI endoscopy.
Barium meal not sensitive.
Plain x-rays may diagnose perforation of acute ulcers.
Angiography can demonstrate bleeding site.
H. pylori testing (hydrogen breath test, stool antigen).
TREATMENT
Antibiotics for eradication of H. pylori: Triple therapy—PPI + 2 antibiotics (amoxicillin, clarithromycin, PPI).
Antacids, sucralfate, and misoprostol.
H2 blockers and PPIs.
Give prophylaxis for peptic ulcer when child is NPO or is receiving steroids.
Endoscopic cautery.
Surgery (vagotomy, pyloroplasty, or antrectomy) for extreme cases.
WARD TIP
Antimicrobials: 14 days
PPIs: 1 month
Colic
DEFINITION
Rule of 3’s: Crying >3 hours/day, >3 days/week for >3 weeks between the ages of
3 weeks and 3 months.
Frequent complex paroxysmal abdominal pain, severe crying.
Usually in infants <3 months old.
Etiology unknown. Can be related to under- or overfeeding, milk protein allergy,
parental stress, and smoking.
Colic is a diagnosis of exclusion. First look for other causes (hair in eye, corneal
abrasion, strangulated hernia, otitis media, sepsis, etc.).
SIGNS AND SYMPTOMS
Sudden-onset loud crying (paroxysms may persist for several hours).
Facial flushing.
Circumoral pallor.
Distended, tense abdomen.
Legs drawn up on abdomen.
Feet often cold.
Temporary relief apparent with passage of feces or flatus.
WARD TIP
A head-to-toe examination is essential.
Physical examination MUST be normal.
TREATMENT
No single treatment provides satisfactory relief.
Careful exam is important to rule out other causes.
Improve feeding techniques (burping).
Avoid over- or underfeeding.
Resolves spontaneously with time.
WARD TIP
Parents and caretakers of children with colic are often very stressed out, putting the child at risk for child abuse.
Pyloric Stenosis
A 4-week-old male infant has a 5-day history of vomiting after feedings. Physical
exam shows a hungry infant with prominent peristaltic waves in the epigastrium. Laboratory
evaluation revealed the following: Na 129, Cl 92, HCO3 28, K 3.1, BUN 24. Think: Hypertrophic pyloric stenosis.
Pyloric stenosis is the most common cause of intestinal obstruction in infants. It is more common in males (M:F 4:1). It usually presents during the third to fifth week of life. Initial symptom is nonbilious vomiting. Classic sign of olive mass is not as common since increasing awareness has resulted in ultrasound imaging and early diagnosis. Criteria for diagnosis include pyloric muscle thickness >4 mm and length of pyloric canal >14 mm. Hypochloremic, hypokalemic metabolic alkalosis is the classic electrolyte abnormality.
DEFINITION
Most common etiology is idiopathic.
Not usually present at birth.
Associated with exogenous administration of erythromycin, eosinophilic gastroenteritis,
epidermolysis bullosa, trisomy 18, and Turner syndrome.
First-born male.
SIGNS AND SYMPTOMS
Typical: Projectile vomiting, palpable mass, and peristalsis—not always present.
Nonbilious vomiting (projectile or not).
Usually progressive, after feeding.
Usually after 3 weeks of age, may be as late as 5 months.
Hypochloremic, hypokalemic metabolic alkalosis (rare these days due to earlier
diagnosis).
Palpable pyloric olive-shaped mass in midepigastrium (difficult to find).
Visible peristalsis: Left to right.
DIAGNOSIS
Ultrasound (90% sensitivity).
Elongated pyloric channel (>14 mm).
Thickened pyloric wall (>4 mm).
Radiographic contrast series (Figure 11-3).
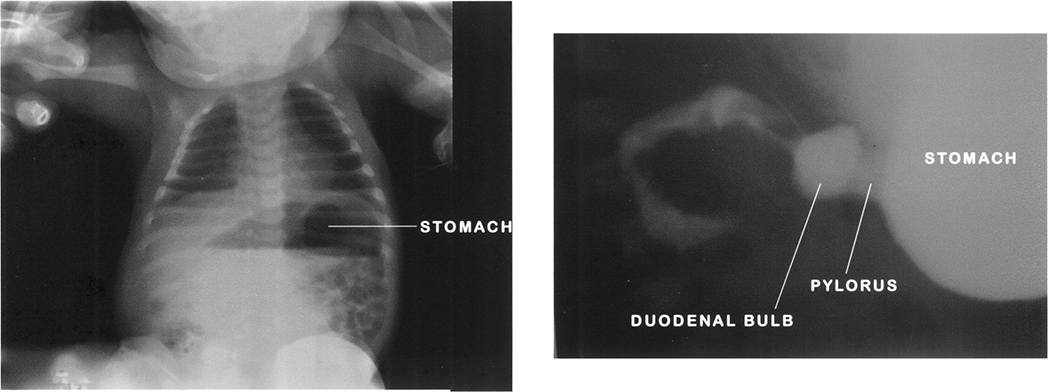
FIGURE 11-3. Abdominal x-ray on the left demonstrates a dilated air-filled stomach with normal caliber bowel, consistent with gastric outlet obstruction. Barium meal figure on the right confirms diagnosis of pyloric stenosis. The dilated duodenal bulb is the “olive” felt on physical exam. Note how there is a paucity of contrast traveling through the duodenum. (Used with permission from Drs. Julia Rosekrans and James E. Colletti.)
String sign: From elongated pyloric channel.
Shoulder sign: Bulge of pyloric muscle into the antrum.
Double tract sign: Parallel streaks of barium in the narrow channel.
TREATMENT
Surgery: Pyloromyotomy is curative.
Must correct existing dehydration and acid-base abnormalities prior to surgery.
Duodenal Atresia
DEFINITION
Failure to recanalize lumen after solid phase of intestinal development.
Several forms.
SIGNS AND SYMPTOMS
Bilious vomiting without abdominal distention (first day of life). Onset of vomiting
within hours of birth.
Can be nonbilious if the defect is proximal to the ampulla of Vater.
Scaphoid abdomen.
Placement of orogastric tube typically yields a significant amount of bile-stained
fluid.
History of polyhydramnios in 50% of pregnancies.
Down syndrome seen in 20–30% of cases.
Associated anomalies include malrotation, esophageal atresia, and congenital heart
disease.
DIAGNOSIS
Clinical.
X-ray findings: Double-bubble sign (air bubbles in the stomach and duodenum) proximal
to the site of atresia (Figure 11-4).
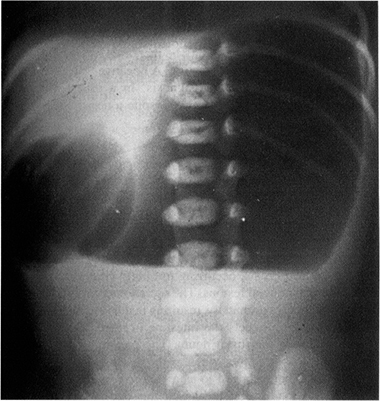
FIGURE 11-4. Duodenal atresia. Gas-filled and dilated stomach shows the classic “double-bubble” appearance of duodenal atresia. Note no distal gas is present. (Reproduced, with permission, from Rudolph CD, et al (eds). Rudolph’s Pediatrics, 21st ed. New York: McGraw-Hill, 2002: 1403.)
TREATMENT
Initially, nasogastric and orogastric decompression with intravenous (IV) fluid
replacement.
Treat life-threatening anomalies.
Surgery.
Duodenoduodenostomy.
Volvulus
DEFINITION
Gastric and intestinal:
Gastric: Sudden onset of severe epigastric pain; intractable retching with emesis.
Intestinal: Associated with malrotation (Figure 11-5).
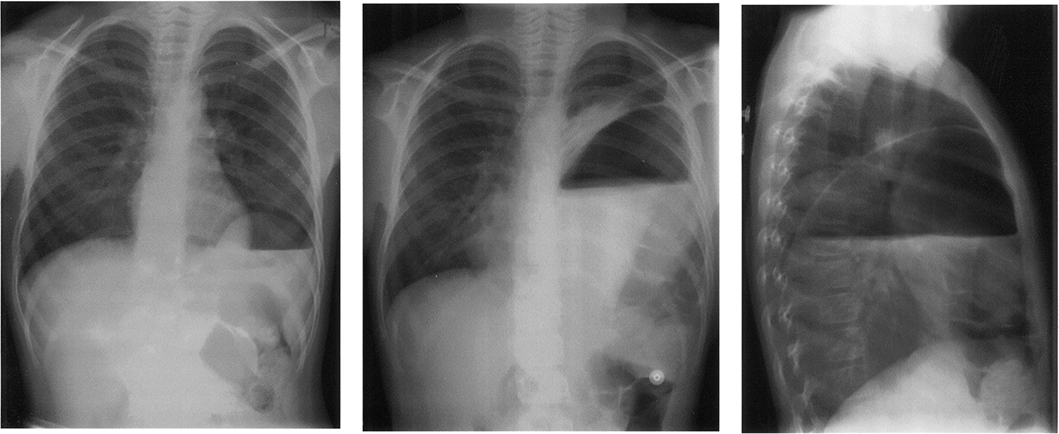
FIGURE 11-5. Volvulus. First AP view done 6 weeks prior to the second AP and corresponding lateral view. Note the markedly dilated stomach above the normal level of the left hemidiaphragm in the thoracic cavity. Also present is a large left-sided diaphragmatic hernia. (Used with permission from Dr. Julia Rosekrans.)
Volvulus occurs as a consequence of intestinal malrotation—obstruction is complete,
and compromise to the blood supply of the midgut has started.
RISK FACTORS
Embryological abnormalities: Arrest of development at any stage during embryological
development of GI tract can → changes in anatomical position of organs and narrowing
of mesenteric base, resulting in ↑ risk for volvulus.
Male-to-female presentation: 2:1.
SIGNS AND SYMPTOMS
Vomiting in infancy.
Emesis (commonly bilious).
Abdominal pain → acute abdomen.
Early satiety.
Blood-stained stools.
Distention.
A neonate with bilious vomiting must be considered at risk for having a midgut
volvulus.
DIAGNOSIS
Plain abdominal films: Characteristic bird-beak appearance.
May also see air-fluid level without beak.
TREATMENT
Treatment is surgical correction.
Gastric: Emergent surgery.
Intestinal: Surgery or endoscopy.
COMPLICATIONS
Perforation.
Peritonitis.
Intussusception
A 9-month-old female infant was brought to the ED due to vomiting and crying. She
had a “cold” 3 days ago. On arrival she was sleepy but arousable. When she woke up,
she cried and vomited. Physical examination revealed distended abdomen with an ill-defined
mass in the right upper abdomen. What is the cause of her symptoms? Intussusception.
How she should be treated? A contrast enema should be performed to reduce the intussusception. It is both diagnostic and therapeutic. It should be performed in consultation with a pediatric surgeon caring for the child and a pediatric radiologist interpreting the study. It is the most common cause of intestinal obstruction between 5 months and 6 years of age. Most children with intussusception are under 1 year of age. The classic triad of intermittent, colicky abdominal pain; vomiting; and bloody, mucous stools occur in only 20–40%.
DEFINITION
Invagination of one portion of the bowel into itself. The proximal portion is usually drawn into the distal portion by peristalsis.
EPIDEMIOLOGY
Incidence: 1–4 in 1000 live births.
Male-to-female ratio: 2:1 to 4:1.
Peak incidence: 5–12 months.
Age range: 2 months to 5 years.
Most common cause of acute intestinal obstruction under 2 years of age.
Most common site is ileocolic (90%).
EXAM TIP
Intussusception is the most common cause of bowel obstruction in children ages 2 months to 5 years.
ETIOLOGY
Most common etiology is idiopathic.
Other causes:
Viral (enterovirus in summer, rotavirus in winter).
A “lead point” (or focus) is thought to be present in older children 2–10% of the
time. These lead points can be caused by Meckel’s diverticulum, polyp, lymphoma, Henoch-Schönlein
purpura, cystic fibrosis.
EXAM TIP
Intussusception
Classic triad is present in only 20% of cases.
Absence of currant jelly stool does not exclude the diagnosis.
Neurologic signs may delay the diagnosis.
SIGNS AND SYMPTOMS
Classic triad:
Intermittent colicky abdominal pain.
Bilious vomiting.
Currant jelly stool (late finding).
Neurologic signs:
Lethargy
Shocklike state.
Seizure activity.
Apnea.
Right upper quadrant mass:
Sausage shaped.
Ill defined.
Dance’s sign: Absence of bowel in right lower quadrant.
DIAGNOSIS
Abdominal x-ray:
X-ray is neither specific nor sensitive. Can be completely normal.
Paucity of bowel gas (Figure 11-6).
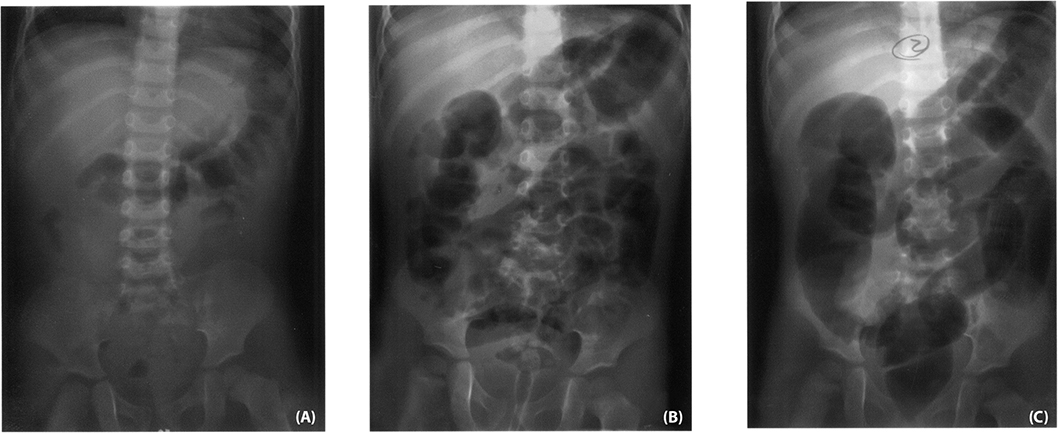
FIGURE 11-6. Intussusception. Note the paucity of bowel gas in film (A) Air enema partially reduces it in film (B) and then completely reduced it in film (C).
Loss of visualization of the tip of liver.
“Target sign”: Two concentric circles of fat density.
Ultrasound:
Test of choice.
“Target” or “donut” sign: Single hypoechoic ring with hyperechoic center.
“Pseudokidney” sign: Superimposed hypoechoic (edematous walls of bowel) and hyperechoic
(areas of compressed mucosa) layers.
Barium enema:
Not useful for ileoileal intussusceptions.
May note cervix-like mass.
Coiled spring appearance on the evacuation film.
Contraindications: Peritonitis, perforation, profound shock/hemodynamic instability.
Air enema:
Air enema is preferred (safe, with a lower absorbed radiation).
Often provides the same diagnostic and therapeutic benefit of a barium enema without
the barium.
WARD TIP
Contrast enema for intussusception can be both diagnostic and therapeutic. Rule of threes:
Barium column should not exceed a height of 3 feet.
No more than 3 attempts.
Only 3 minutes/attempt.
TREATMENT
Correct dehydration.
NG tube for decompression.
Hydrostatic reduction.
Barium/air enema (see Figure 11-7).

FIGURE 11-7. Abdominal x-ray following barium enema in a 2-month-old boy, consistent with intussusception. Note paucity of gas in right upper quadrant and near obscuring of liver tip.
Surgical reduction:
Failed reduction by enema.
Clinical signs of perforation or peritonitis.
Recurrence:
With radiologic reduction: 7–10%.
With surgical reduction: 2–5%.
Meckel’s Diverticulum
DEFINITION
Persistence of the omphalomesenteric (vitelline) duct (should disappear by seventh week of gestation).
EXAM TIP
Meckel’s Rules of 2
2% of population
2 inches long
2 feet from the ileocecal valve
Patient is usually under 2 years of age
2% are symptomatic
SIGNS AND SYMPTOMS
Usually in first 2 years:
Intermittent painless rectal bleeding (hematochezia—most common presenting sign).
Intestinal obstruction.
Diverticulitis.
Occurs on the antimesenteric border of the ileum, usually 40–60 cm proximal to
the ileocecal valve.
WARD TIP
Meckel’s diverticulum may mimic acute appendicitis and also act as lead point for intussusception.
DIAGNOSIS
Meckel’s scan (scintigraphy) has 85% sensitivity and 95% specificity. Uptake can
be enhanced with cimetidine, glucagons, or gastrin.
Most common heterotopic mucosa is gastric.
TREATMENT
Surgical: Diverticular resection with transverse closure of the enterotomy.
Appendicitis
DEFINITION
Acute inflammation and infection of the vermiform appendix.
Most common cause for emergent surgery in childhood.
Perforation rates are greatest in youngest children (can’t localize symptoms).
Occurs secondary to obstruction of lumen of appendix.
Three phases:
1. Luminal obstruction, venous congestion progresses to mucosal is chemia, necrosis, and ulceration.
2. Bacterial invasion with inflammatory infiltrate through all layers.
3. Necrosis of wall results in perforation and contamination.
SIGNS AND SYMPTOMS
Classically: Pain, vomiting, and fever.
Initially, periumbilical pain; emesis infrequent.
Anorexia.
Low-grade fever.
Diarrhea infrequent.
Pain radiates to right lower quadrant.
Perforation rate >65% after 48 hours.
Rectal exam may reveal localized mass or tenderness.
DIAGNOSIS
History and physical exam is key to rule out alternatives first.
Pain usually occurs before vomiting, diarrhea, or anorexia.
Atypical presentations are common—risk for misdiagnosis.
Most common misdiagnosis: Gastroenteritis.
Labs helpful to rule other diagnosis but no laboratory test specific for appendicitis.
Computed tomographic (CT) scan (Figure 11-8) indicated for patients in whom diagnosis is equivocal—not a requirement for all
patients.
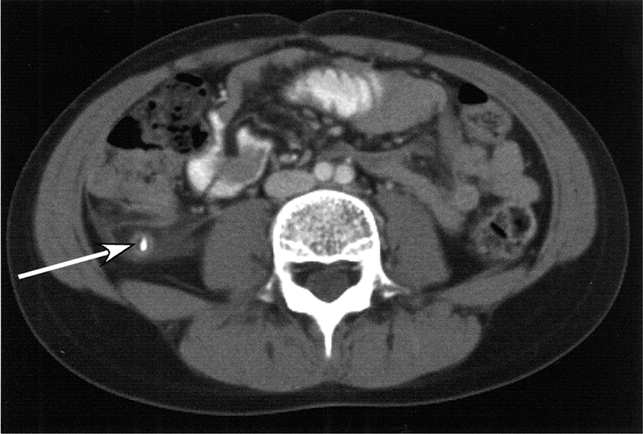
FIGURE 11-8. Abdominal CT of a 10-year-old girl demonstrating enlargement of the appendix, some periappendiceal fluid, and an appendicolith (arrow), consistent with acute appendicitis.
Higher rate of ruptured appendix on presentation in young children.
TREATMENT
Surgery as soon as diagnosis made.
Antibiotics are controversial in nonperforated appendicitis.
Broad-spectrum antibiotics needed for cases of perforation (ampicillin, gentamicin,
clindamycin, or metronidazole × 7 days).
Laparoscopic removal associated with shortened hospital stay (nonperforated appendicitis).
Constipation
A 4-year-old girl has not had a bowel movement for a week, and this has been a recurring
problem. Various laxatives and enemas have been tried in the past. Prior to toilet
training, the girl had one bowel movement a day. Physical examination is normal except
for the presence of stool in the sigmoid colon and hard stool on rectal examination.
After removing the impaction, the next appropriate step in management would be to
administer mineral oil or other stool softener.
Constipation is a common problem in children. It is the most common cause of abdominal pain in children. Functional constipation is more common in children, and organic causes are common in neonates. The physical examination often reveals a large volume of stool palpated in the suprapubic region. The finding of rectal impaction may establish the diagnosis.
DEFINITION/SIGNS AND SYMPTOMS
Common cause of abdominal pain in children.
Passage of bulky or hard stool at infrequent intervals.
During the neonatal period usually caused by Hirschsprung, intestinal pseudo-obstruction,
or hypothyroidism.
Other causes include organic and inorganic (e.g., cow’s milk protein intolerance,
drugs).
May be metabolic (dehydration, hypothyroidism, hypokalemia, hypercalcemia, psychiatric).
TREATMENT
↑ oral fluid and fiber intake.
Stool softeners (e.g., mineral oil).
Glycerin suppositories.
Cathartics such as senna or docusate.
Nonabsorbable osmotic agents (polyethylene glycol) and milk of magnesia for short
periods only if necessary—can cause electrolyte imbalances.
Hirschsprung’s Megacolon
A full-term male infant was noted to have progressive abdominal distention on the
second day of life, with no stool since birth. He was feeding well on demand whether
mother’s milk or infant formula. He was otherwise healthy, active, and had no signs
of infection. Abdominal x-ray is consistent with distended loops of bowel with no
evidence of free air. Contrast enema is notable for a narrowed segment of the colon
leading to a very distended loop.
The diagnosis is likely Hirschsprung disease. Hirschsprung disease results from absence of ganglion cells in the bowel wall and resultant narrowed segment of the bowel. The proximal normal bowel progressively dilates due to accumulated food. Definitive diagnosis is made by rectal biopsy, which demonstrates absent ganglion cells.
DEFINITION
Abnormal innervation of bowel (i.e., absence of ganglion cells in bowel).
↑ in familial incidence.
Occurs in males more than females.
Associated with Down syndrome.
SIGNS AND SYMPTOMS
Delayed passage of meconium at birth.
↑ abdominal distention →↓ blood flow → deterioration of mucosal barrier → bacterial
proliferation → enterocolitis.
Chronic constipation and abdominal distention (older children).
DIAGNOSIS
Rectal manometry: Measures pressure of the anal sphincter.
Rectal suction biopsy: Must obtain submucosa to evaluate for ganglionic cells.
TREATMENT
Surgery is definitive (usually staged procedures).
Imperforate Anus
DEFINITION
Absence of normal anal opening.
Rectum is blind; located 2 cm from perineal skin.
Sacrum and sphincter mechanism well developed.
Prognosis good.
Can be associated with VACTERL anomalies.
SIGNS AND SYMPTOMS
First newborn examination in nursery.
Failure to pass meconium.
Abdominal distention.
DIAGNOSIS
Physical examination.
Abdominal ultrasonography to examine the genitourinary tract.
Sacral radiography.
Spinal ultrasound: Association with spinal cord abnormalities, particularly spinal
cord tethering.
TREATMENT
Surgery (colostomy in newborn period).
WARD TIP
Imperforate anus is frequently associated with Down syndrome and VACTERL.
Anal Fissure
A well-nourished 3-month-old infant is brought to the ED because of constipation,
blood-streaked stools, and excessive crying on defecation. Think: Anal fissure.
Anal fissure is a painful linear tear or crack in the distal anal canal. Constipation may be exacerbated because of fear of pain with defecation. Diagnosis often can be made based on history and physical examination.
DEFINITION
Painful linear tears in the anal mucosa below the dentate line induced by constipation
or excessive diarrhea.
Tear of squamous epithelium of anal canal between anocutaneous junction and dentate
line.
Often history of constipation is present.
Predilection for the posterior midline.
Common age: 6–24 months.
SIGNS AND SYMPTOMS
Pain with defecation/crying during bowel movement.
↑ sphincter tone.
Visible tear upon gentle lateral retraction of anal tissue.
DIAGNOSIS
Anal inspection.
TREATMENT
Sitz baths, fiber supplements, ↑ fluid intake.
Inflammatory Bowel Disease
DEFINITION
Idiopathic chronic diseases include Crohn disease and ulcerative colitis (UC).
EPIDEMIOLOGY
Common onset in adolescence and young adulthood.
Bimodal pattern in patients 15–25 and 50–80 years of age.
Genetics: ↑ concordance with monozygotic twins versus dizygotic (↑ for Crohn versus
UC).
SIGNS AND SYMPTOMS (TABLE 11-1)
TABLE 11-1. Crohn Disease versus Ulcerative Colitis
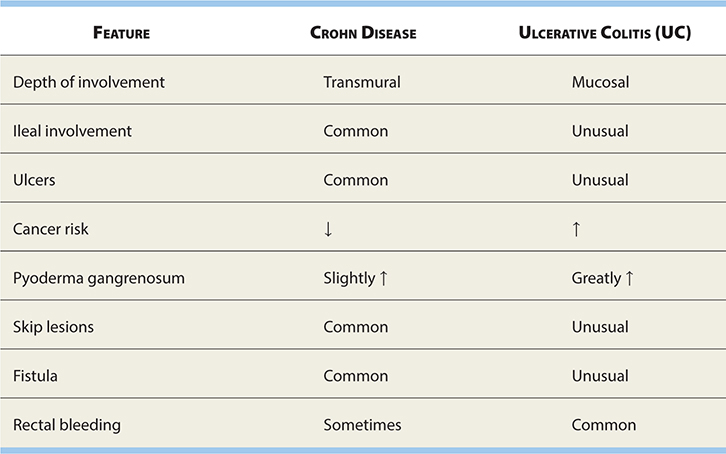
Crampy abdominal pain.
Extraintestinal manifestations greater in Crohn than UC.
Crohn: Perianal fistula, sclerosing cholangitis, chronic active hepatitis, pyoderma
gangrenosum, ankylosing spondylitis, erythema nodosum.
UC: Bloody diarrhea, anorexia, weight loss, pyoderma gangrenosum, sclerosing cholangitis,
marked by flare-ups.
TREATMENT
Crohn disease: Corticosteroids, aminosalicylates, methotrexate, azathioprine, cyclosporine,
metronidazole (for perianal disease), sitz baths, anti–tumor necrosis factor-α, surgery
for complications.
UC: Aminosalicylates, oral corticosteroids, colectomy.
Irritable Bowel Syndrome
DEFINITION
Abdominal pain associated with intermittent diarrhea and constipation without organic basis; ~10% in adolescents.
SIGNS AND SYMPTOMS
Abdominal pain.
Diarrhea alternating with constipation.
DIAGNOSIS
Difficult to make, exclude other pathology.
Obtain CBC, ESR, stool occult blood.
TREATMENT
None specific.
Supportive with reinforcement and reassurance.
Address any underlying psychosocial stressors.
Acute Gastroenteritis and Diarrhea
DEFINITION
Diarrhea is the excessive loss of fluid and electrolytes in stool, usually secondary to disturbed
intestinal solute transport. Technically limited to lower GI tract.
Gastroenteritis is an inflammation of the entire (upper and lower) GI tract, and thus involves both
vomiting and diarrhea.
EPIDEMIOLOGY
↑ susceptibility seen in young age, immunodeficiency, malnutrition, travel, lack
of breast-feeding, and contaminated food or water.
Most common cause of diarrhea in children is viral: (1) rotavirus, (2) enteric
adenovirus, (3) Norwalk virus.
Bacterial: (1) Campylobacter, (2) Salmonella and Shigella species and enterohemorrhagic Escherichia coli.
Children in developing countries often also get infected by bacterial and parasitic
pathogens:
Enterotoxigenic E. coli number one in developing countries.
Parasitic causes: (1) Giardia and (2) Cryptosporidium.
WARD TIP
Acute diarrhea is usually caused by infectious agents, whereas chronic persistent diarrhea may be secondary to infectious agents, infection of immunocompromised host, or residual symptoms due to intestinal damage.
SIGNS AND SYMPTOMS
Important to obtain information regarding frequency and volume.
General patient appearance important (well appearing versus ill appearing).
Associated findings include cramps, emesis, malaise, and fever.
May see systemic manifestations, GI tract involvement, or extraintestinal infections.
Extraintestinal findings include vulvovaginitis, urinary tract infection (UTI),
and keratoconjunctivitis.
Systemic manifestations: Fever, malaise, and seizures.
Inflammatory diarrhea: Fever, severe abdominal pain, tenesmus. May have blood/mucus
in stool.
Noninflammatory diarrhea: Emesis, fever usually absent, crampy abdominal pain,
watery diarrhea.
WARD TIP
Diarrhea and emesis—noninflammatory
Diarrhea and fever—inflammatory process
Diarrhea and tenesmus—large colon involvement
DIAGNOSIS
Examine stool for mucus, blood, and leukocytes (colitis).
Fecal leukocyte: Presence of invasive cytotoxin organisms (Shigella, Salmonella).
Patients with enterohemorrhagic E. coli and Entamoeba histolytica: Minimal to no fecal leukocytes.
Obtain stool cultures early.
Clostridium difficile toxins: Test if recent antibiotic use.
Proctosigmoidoscopy: Diagnosis of inflammatory enteritis.
WARD TIP
Diarrhea is a characteristic finding in children poisoned with bacterial toxin of Escherichia coli, Salmonella, Staphylococcus aureus, and Vibrio parahemolyticus, but not Clostridium botulinum.
TREATMENT
Rehydration.
Oral electrolyte solutions (e.g., Pedialyte®).
Oral hydration for all but severely dehydrated (IV hydration).
Rapid rehydration with replacement of ongoing losses during first 4–6 hours.
Do not use soda, fruit juices, gelatin, or tea. High osmolality may exacerbate
diarrhea.
Start food with BRAT diet.
Antidiarrheal compounds are not indicated for use in children.
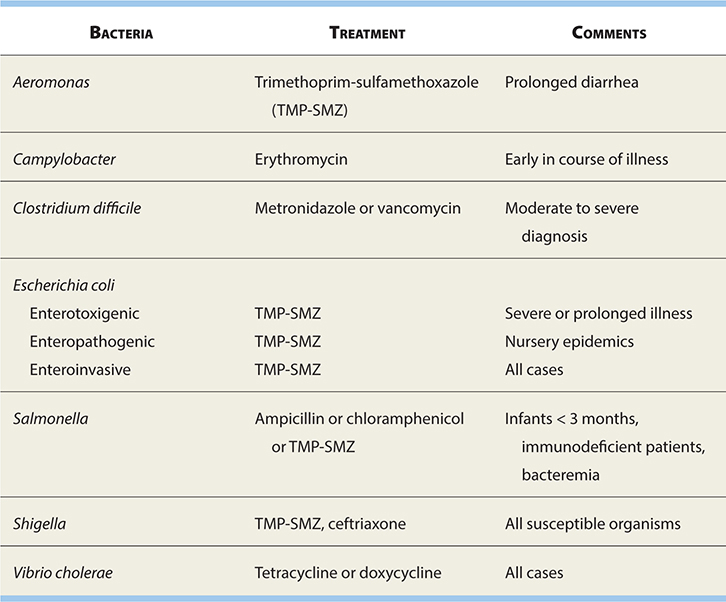
See Table 11-2 for antibiotic treatment of enteropathogens (wait for diagnosis via stool culture,
empiric antibiotics generally not indicated).
TABLE 11-2. Antimicrobial Treatment for Bacterial Enteropathogens
WARD TIP
BRAT Diet for Diarrhea
Bananas
Rice
Applesauce
Toast
Prevention
Hospitalized patients should be placed under contact precautions (hand washing,
gloves, gowns, etc.).
Education.
Exclude infected children from child care centers.
Report cases of bacterial diarrhea to local health department.
Vaccines for cholera and Salmonella typhi are available.
EXAM TIP
Do not treat E. coli O157:H7 with antibiotics, as there is a higher incidence of hemolytic uremic syndrome with treatment.
Intestinal Worms
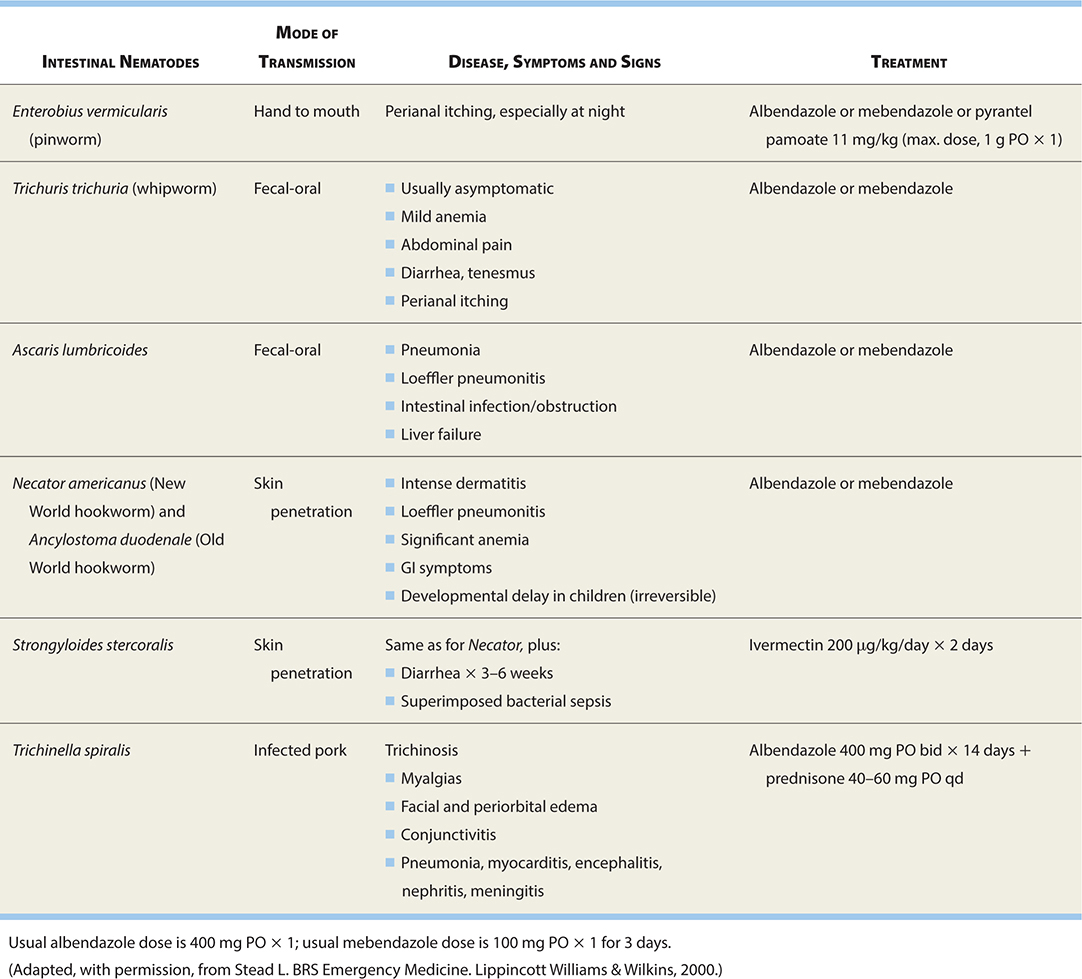
See Table 11-3 for common intestinal worm infestations.
TABLE 11-3. Common Intestinal Worms
Pseudomembranous Colitis
DEFINITION
Major cause of iatrogenic diarrhea.
Rarely occurs without antecedent antibiotics (usually) penicillins, cephalosporins,
or clindamycin.
Antibiotic disrupts normal bowel flora and predisposes to C. difficile diarrhea.
Stool should be tested for C. difficile toxins if there is a recent history of antibiotic use.
EXAM TIP
The most frequent symptom of infestation with Enterobius vermicularis is perineal pruritus. Can diagnose with transparent adhesive tape to area (worms stick).
SIGNS AND SYMPTOMS
Classically, blood and mucus with fever, cramps, abdominal pain, nausea, and vomiting days or weeks after antibiotics.
DIAGNOSIS
Recent history of antibiotic use.
C. difficile toxin in stool of patient with diarrhea.
Sigmoidoscopy or colonoscopy.
TREATMENT
Discontinue antibiotics.
Oral metronidazole or vancomycin × 7–10 days.
Abdominal Hernias
UMBILICAL
DEFINITION
Occurs because of imperfect closure of umbilical ring.
Common in low-birth-weight, female, and African-American infants.
Soft swelling covered by skin that protrudes while crying, straining, or coughing.
Omentum or portions of small intestine involved.
Usually 1–5 cm.
TREATMENT
Most disappear spontaneously by 1 year of age.
Strangulation rare.
“Strapping” ineffective.
Surgery not indicated unless symptomatic, strangulated, or grows larger after age
1 or 2.
INGUINAL
DEFINITION
Most common diagnosis requiring surgery.
Occurs in 10–20/1,000 live births (50% <1 year).
Indirect > direct (rare) > femoral (even more rare).
Indirect secondary to patent processus vaginalis.
↑ incidence with positive family history.
Embryology: Patent processus vaginalis.
Incidence: 1–5%.
Males > females 8–10:1.
Preemies: 20% males, 2% females.
Premature infants have ↑ risk for inguinal hernia.
Sixty percent right (delayed descent of the right testicle), 30% left, 10% bilateral.
EXAM TIP
In inguinal hernia, processus vaginalis herniates through abdominal wall with hydrocele into canal.
SIGNS AND SYMPTOMS
Infant with scrotal/inguinal bulge on straining or crying.
Do careful exam to distinguish from hydrocele (see Figure 11-9).
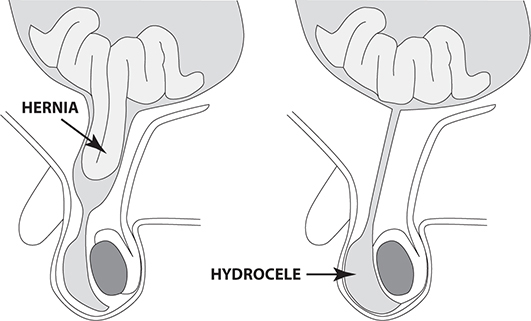
FIGURE 11-9. Inguinal hernia (slippage of bowel through inguinal ring) vs. hydrocele (collection of fluid in scrotum adjacent to testes).
Bulge in groin ± scrotum, incarceration.
TREATMENT
Surgery (elective).
Avoid trusses or supports.
Contralateral hernia occurs in 30% after unilateral repair.
Antibiotics only in at-risk children (e.g., congenital heart disease).
Prognosis excellent (recurrence <1%, complication rate approximately 2%, infection
approximately 1%).
Complications include incarceration.
Therapy: Incarceration––sedation and manipulation 90–95% reduced. Immediate operation
if not reduced. Repair soon after diagnosis especially infants since 60% progress
to incarceration by 6 months.
WARD TIP
Inguinal hernia ↑ with straining; hydrocele remains unchanged.
Peutz-Jeghers Syndrome
A 15-year-old girl with spots on her lips has some crampy abdominal pain associated
with bleeding. Think: Peutz-Jeghers syndrome.
Peutz-Jeghers syndrome is multiple GI hamartomatous polyps + mucocutaneous hyperpigmentation. There is a higher risk of intestinal and extraintestinal malignancies.
DEFINITION
Mucosal pigmentation of lips and gums with hamartomas of stomach, small intestine,
and colon.
Rare; low malignant potential.
SIGNS AND SYMPTOMS
Deeply pigmented freckles on lips and buccal mucosa at birth.
Bleeding and crampy abdominal pain.
DIAGNOSIS
Genetic and family studies may reveal history.
TREATMENT
Excise intestinal lesions if significantly symptomatic.
Gardner Syndrome
DEFINITION
Multiple intestinal polyps, tumors of soft tissue and bone (especially mandible).
SIGNS AND SYMPTOMS
Dental abnormalities.
Pigmented lesions in ocular fundus.
Intestinal polyps (usually early adulthood) with high malignant potential.
DIAGNOSIS
Genetic counseling.
Colon surveillance in at-risk children.
TREATMENT
Aggressive surgical removal of polyps.
Carcinoid Tumors
DEFINITION
Tumors of enterochromaffin cells in intestine—usually appendix.
SIGNS AND SYMPTOMS
May cause appendicitis.
May cause carcinoid syndrome (↑ serotonin, vasomotor disturbances, or bronchoconstriction)
if metastatic to the liver.
TREATMENT
Surgical excision.
Familial Polyposis Coli
DEFINITION/ETIOLOGY
Autosomal dominant.
Large number of adenomatous lesions in colon.
Secondary to germ-line mutations in adenopolyposis coli (APC) gene.
SIGNS AND SYMPTOMS
Highly variable.
May see hematochezia, cramps, or diarrhea.
Extracolonic manifestations possible.
DIAGNOSIS
Consider family history (strong).
Colonoscopy with biopsy (screening annually after 10 years old if positive family
history).
TREATMENT
Surgical resection of affected colonic mucosa.
Juvenile Polyposis Coli
DEFINITION
Most common childhood bowel tumor (3–4% of patients <21 years).
Characteristically, mucus-filled cystic glands (no adenomatous changes, no potential
for malignancy).
EPIDEMIOLOGY
Most commonly between 2 and 10 years; less common after 15 years; rarely before 1 year.
SIGNS AND SYMPTOMS
Bright-red painless bleeding with bowel movement.
Iron deficiency.
DIAGNOSIS
Colonoscopy.
May use barium enema (not best test).
TREATMENT
Surgical removal of polyp.
Malabsorption
SHORT BOWEL SYNDROME
DEFINITION
Occurs with loss of at least 50% of small bowel (with or without loss of large
bowel).
↓ absorptive surface and bowel function.
ETIOLOGY
May be congenital (malrotation, atresia, etc.).
Most commonly secondary to surgical resection.
SIGNS AND SYMPTOMS
Malabsorption and diarrhea.
Steatorrhea (fatty stools): Voluminous foul-smelling stools that float.
Dehydration.
↓ sodium and potassium.
Acidosis (secondary to loss of bicarbonate).
TREATMENT
Total parenteral nutrition (TPN).
Give small feeds orally.
Metronidazole empirically to treat bacterial overgrowth.
CELIAC DISEASE
A 5-year-old girl presents with a protuberant abdomen and wasted extremities. Think: Gluten-induced enteropathy.
Celiac disease is an autoimmune disorder. The disease primarily affects the small intestine. Gluten is the single major factor that triggers celiac disease. Gluten-containing foods include rye, wheat, and barley. Common presentation: diarrhea, borborygmus, abdominal pain, and weight loss. Other systems, including skin, liver, nervous system, bones, reproductive system, and endocrine system, may also be affected. Serologic marker: Serum immunoglobulin A (IgA) endomysial antibodies and IgA tissue transglutaminase (tTG) antibodies.
DEFINITION
Sensitivity to gluten in diet.
Most commonly occurs between 6 months and 2 years.
ETIOLOGY
Factors involved include cereals, genetic predisposition, and environmental factors.
Associated with HLA-B8, -DR7, -DR3, and -DQW2.
SIGNS AND SYMPTOMS
Diarrhea.
Failure to thrive.
Vomiting.
Pallor.
Abdominal distention.
Large bulky stools.
DIAGNOSIS
Anti-endomysial and anti-tissue transglutaminase antibodies (check total lgH level
at the same time).
Biopsy: Most reliable test.
TREATMENT
Dietary restriction of gluten (must avoid barley, ryes, oats, and wheat).
Corticosteroids used rarely (very ill patients with profound malnutrition, diarrhea,
edema, and hypokalemia).
TROPICAL SPRUE
DEFINITION
Generalized malabsorption associated with diffuse lesions of small bowel mucosa.
Seen in people who live or have traveled to certain tropical regions—some Caribbean
countries, South America, Africa, or parts of Asia.
SIGNS AND SYMPTOMS
Fever, malaise, and watery diarrhea, acutely.
After 1 week, chronic malabsorption and signs of malnutrition including night blindness,
glossitis, stomatitis, cheilosis, muscle wasting.
DIAGNOSIS
Biopsy shows villous shortening, ↑ crypt depth, and ↑ chronic inflammatory cells in lamina propria of small bowel.
TREATMENT
Antibiotics × 3–4 weeks.
Folate.
Vitamin B12.
Prognosis excellent.
LACTASE DEFICIENCY
DEFINITION
↓ or absent enzyme that breaks down lactose in the intestinal brush border.
ETIOLOGY
Congenital absence reported in few cases.
Usual mechanism relates to developmental pattern of lactase activity.
Autosomal recessive.
Also ↓ because of diffuse mucosal disease (can occur post viral gastroenteritis).
SIGNS AND SYMPTOMS
Seen in response to ingestion of lactose (found in dairy products).
Explosive watery diarrhea with abdominal distention, borborygmi, and flatulence.
Recurrent, vague abdominal pain.
Episodic midabdominal pain (may or may not be related to milk intake).
TREATMENT
Eliminate milk from diet.
Oral lactase supplement (Lactaid) or lactose-free milk.
Yogurt (with lactase enzyme–producing bacteria tolerable in such patients).
Hyperbilirubinemia
Physiology: See Gestation and Birth chapter.
DEFINITION
Elevated serum bilirubin.
EPIDEMIOLOGY
Common and in most cases benign.
If untreated, severe indirect hyperbilirubinemia neurotoxic (kernic-terus).
Jaundice in first week of life in 60% of term and 80% of preterm infants—results
from accumulation of unconjugated bilirubin pigment.
SIGNS AND SYMPTOMS
Jaundice at birth or in neonatal period.
May be lethargic and feed poorly.
WARD TIP
Indirect hyperbilirubinemia, reticulosis, and red cell destruction suggest hemolysis.
Direct hyperbilirubinemia may indicate hepatitis, cholestasis, inborn errors of
metabolism, cystic fibrosis, or sepsis.
If reticulocyte count, Coombs’, and direct bilirubin are normal, then physiologic
or pathologic indirect hyperbilirubinemia is suggested.
DIAGNOSIS
Direct and indirect bilirubin fractions.
Hemoglobin.
Reticulocyte count.
Blood type.
Examine peripheral smear.
TREATMENT
Goal is to prevent neurotoxic range.
Phototherapy.
Exchange transfusion.
Treat underlying cause.
GILBERT SYNDROME
Benign condition caused by missense mutation in transferase gene resulting in low enzyme levels with unconjugated hyperbilirubinemia.
EXAM TIP
Children with cholestatic hepatic disease need replacement of vitamins A, D, E, and K (fat soluble).
CRIGLER-NAJJAR I SYNDROME
DEFINITION
Autosomal recessive, secondary to mutations in glucuronyl transferase gene.
Parents of affected children show partial defects but normal serum bilirubin concentration.
Complete absence of the enzyme uridine diphosphate glycosyltransferase.
Much rarer than Gilbert syndrome.
SIGNS AND SYMPTOMS
In homozygous infants, will see unconjugated hyperbilirubinemia in first 3 days
of life.
Kernicterus common in early neonatal period.
Some treated infants survive childhood without sequelae.
Stools pale yellow.
Persistence of ↑ levels of indirect bilirubin after first week of life in absence
of hemolysis suggests this syndrome.
DIAGNOSIS
Based on early age of onset and extreme level of bilirubin in absence of hemolysis.
Definitive diagnosis made by measuring glucuronyl transferase activity in liver
biopsy specimen.
DNA diagnosis available.
TREATMENT
Maintain serum bilirubin <20 mg/dL for first 2–4 weeks of life.
Repeated exchange transfusion.
Phototherapy.
Treat intercurrent infections.
Hepatic transplant.
CRIGLER-NAJJAR II SYNDROME
DEFINITION
Autosomal dominant with variable penetrance.
May be caused by homozygous mutation in glucuronyl transferase isoform I activity.
↓ enzyme uridine diphosphate glycosyltransferase.
SIGNS AND SYMPTOMS
Unconjugated hyperbilirubinemia in first 3 days of life.
Concentration remains ↑ after third week of life.
Kernicterus unusual.
Stool normal.
Infants asymptomatic.
DIAGNOSIS
Concentration of bilirubin nearly normal.
↓ bilirubin after 7- to 10-day treatment with phenobarbital may be diagnostic.
TREATMENT
Phenobarbital for 7–10 days.
ALAGILLE SYNDROME
DEFINITION
Absence or reduction in number of bile ducts.
Results from progressive destruction of the ducts.
SIGNS AND SYMPTOMS
Variably expressed.
Unusual facies (broad forehead, wide-set eyes, underdeveloped mandible).
Ocular abnormalities.
Cardiovascular abnormalities (peripheral pulmonic stenosis).
Tubulointerstitial nephropathy.
Vertebral defect.
Prognosis
Long-term survival good but may have pruritis, xanthomas, and ↑ cholesterol and neurologic complications.
ZELLWEGER SYNDROME
DEFINITION
Rare autosomal-recessive condition causing progressive degeneration of liver and
kidneys.
Occurs in 1 in 100,000 births.
SIGNS AND SYMPTOMS
Usually fatal within 6–12 months.
Severe generalized hypotonia.
Impaired neurologic function with psychomotor retardation.
Abnormal head and unusual facies.
Hepatomegaly.
Renal cortical cysts.
Ocular abnormalities.
Congenital diaphragmatic hernia.
DIAGNOSIS
Absence of peroxisomes in hepatic cells (on biopsy).
Genetic testing available.
EXTRAHEPATIC BILIARY ATRESIA
DEFINITION
Distal segmental bile duct obliteration with patent extrahepatic ducts up to porta hepatis.
EPIDEMIOLOGY
Most common form (85%): Obliteration of entire extrahepatic biliary tree at/above
porta.
Occurs in 1 in 10,000 to 1 in 15,000 live births.
SIGNS AND SYMPTOMS
Acholic stools (stools are very light in color, almost beige).
↑ incidence of polysplenia syndrome with heterotaxia, malrotation, levocardia,
and intra-abdominal vascular anomalies.
DIAGNOSIS
Ultrasound.
Hepatobiliary scintigraphy.
Liver biopsy.
TREATMENT
Exploratory laparotomy and direct cholangiography to determine presence and site
of obstruction.
Direct drainage if lesion is correctable.
Surgery if lesion is not correctable (liver transplant, Kasai procedure).
Hepatitis
Continues to be major problem worldwide.
Six known viruses cause hepatitis as their primary manifestation—A (HAV), B (HBV),
C (HCV), D (HDV), E (HEV), and G (HGV).
Many others cause hepatitis as part of their clinical spectrum—herpes simplex virus
(HSV), cytomegalovirus (CMV), Epstein-Barr virus (EBV), rubella, enteroviruses, parvovirus.
HBV is a DNA virus, whereas HAV, HCV, HDV, HEV, and HGV are RNA viruses.
HAV and HEV are not known to cause chronic illness, but HBV, HCV, and HDV cause
important morbidity and mortality through chronic infection.
HAV causes most cases of hepatitis in children.
HBV causes one-third of all cases; HCV found in 20%.
HEPATITIS A
DEFINITION
RNA-containing member of the Picornavirus family.
Found mostly in developing countries.
Causes acute hepatitis only.
Two-thirds of children are asymptomatic.
Transmission by person-to-person contact; spread by fecal-oral route.
Percutaneous transmission rare, maternal-neonatal not recognized.
↑ risk in child care centers, contaminated food or water, or travel to endemic
areas.
Mean incubation 4 weeks (15–50 days).
SIGNS AND SYMPTOMS
Abrupt onset with fever, malaise, nausea, emesis, anorexia, and abdominal discomfort.
Diarrhea common.
Almost all recover but may have relapsing course over several months.
Jaundice.
DIAGNOSIS
Consider when history of jaundice in family contacts or child care playmates or
travel history to endemic region.
Serologic criteria:
Immunoglobulin M (IgM) anti-HAV presents at onset of illness and disappears within
4 months. May persist for >6 months (acute infection). IgG is detectable at this point.
↑ alanine transaminase (ALT), aspartate transaminase (AST), bilirubin, and gamma-glutamyl
transpeptidase (GGT).
TREATMENT
Careful hand washing.
Vaccines available (preferred over immunoglobulin in children >2 years).
HEPATITIS B
DEFINITION
DNA virus from the Hepadnaviridae family.
Most important risk factor for infants is perinatal exposure to hepatitis B surface
antigen (HbsAg)-positive mother.
SIGNS AND SYMPTOMS
Many cases asymptomatic.
↑ ALT prior to lethargy, anorexia, and malaise (6–7 weeks post exposure).
May be preceded by arthralgias or skin lesions and rashes.
May see extrahepatic conditions, polyarteritis, glomerulonephritis, aplastic anemia.
Jaundice: Icteric skin and mucous membranes.
Hepatosplenomegaly and lymphadenopathy common.
EXAM TIP
Chronic hepatitis B is a risk factor for hepatocellular carcinoma.
DIAGNOSIS
Routine screening requires assay of two serologic markers: HbsAg (all infected
persons, ↑ when symptomatic) and hepatitis B core antigen (HbcAg) (present during
acute phase, highly infectious state).
HbsAg falls prior to symptom resolution; IgMAb to HbcAg also required because it
is ↑ early after infectivity and persists for several months before being replaced
by immunoglobulin G (IgG) anti-HbcAg.
HbcAg most valuable; it is present as early as HbsAg and continues to be present
later when HBsAg disappears.
Only anti-HbsAg detected in persons immunized with hepatitis B vaccine, whereas
anti-HbsAb and anti-HbcAg are seen in persons with resolved infection.
PREVENTION
Screening blood donors.
Screening pregnant women to prevent vertical transmission.
TREATMENT
No available medical treatment effective in majority of cases.
Interferon-α is approved treatment in children.
Liver transplant for patients with end-stage HBV.
HEPATITIS C
DEFINITION
Single-stranded RNA virus.
Perinatal transmission described but uncommon except with high-titer HCV.
SIGNS AND SYMPTOMS
Acute infection similar to other hepatitis viruses.
Mild and insidious onset.
Fulminant liver failure rare.
After 20–30 years, 25% progress to cirrhosis, liver failure, or primary hepatocellular
carcinoma.
May see cryoglobulinemia, vasculitides, and peripheral neuropathy (extrahepatic).
DIAGNOSIS
Detection of antibodies to HCV or direct testing for RNA virus.
Polymerase chain reaction (PCR) detection possible.
↑ ALT.
Confirmed by liver biopsy.
TREATMENT
Treat to prevent progression to future complications.
INF-α2b for patients with compensated liver disease (response rate long term ~25%).
May use with ribavirin for higher frequency of sustained response.
HEPATITIS D (DELTA AGENT)
DEFINITION
Smallest known animal virus.
Cannot produce infection without HBV infection (coinfective or superinfection).
Transmission by intimate contact.
SIGNS AND SYMPTOMS
Similar to but more severe than other hepatitis viruses.
In coinfection, acute hepatitis is more severe, risk of developing chronic hepatitis
low; in superinfection, risk of fulminant hepatitis is highest.
DIAGNOSIS
Detect IgM antibody to HDV (2–4 weeks after coinfection, 1 week after superinfection).
PREVENTION
No vaccine for hepatitis D, but can minimize against hepatitis B (needs hepatitis B to infect).
HEPATITIS E
DEFINITION
RNA virus with nonenveloped sphere shape with spikes (similar to caliciviruses).
Non-A, non-B hepatitis.
SIGNS AND SYMPTOMS
Similar to HAV, but more severe.
No chronic illness.
High prevalence of fulminant hepatic failure and death in pregnant women.
DIAGNOSIS
Antibody to HEV exists.
IgM and IgG assays available.
Can detect viral RNA in stool and serum by PCR.
PREVENTION
No vaccines available.
HEPATITIS G
DEFINITION
Single-stranded RNA virus of Flaviviridae family.
Virus not yet isolated.
Reported in all population groups in ~1.5% U.S. blood donors.
One percent transmission through transfusions but also by organ transplant.
Vertical transmission occurs.
SIGNS AND SYMPTOMS
Symptoms associated with hepatic inflammation.
Coinfection does not worsen course of HBV or HCV.
DIAGNOSIS
Only PCR assays available for testing.
TREATMENT
No method available.
NEONATAL HEPATITIS
DEFINITION
Hepatic inflammation of unknown etiology.
Most result from systemic disease (e.g., sepsis).
Also caused by CMV, HSV, human immunodeficiency virus (HIV).
Nonviral causes include congenital syphilis and toxoplasmosis.
HBV results in asymptomatic infection.
SIGNS AND SYMPTOMS
Jaundice.
Vomiting.
Poor feeding.
↑ liver enzyme levels.
Fulminant hepatitis.
TREATMENT
Antibiotics for bacteria-associated hepatitis.
Acyclovir for HSV.
Ganciclovir and foscarnet for CMV.
AUTOIMMUNE (CHRONIC) HEPATITIS
DEFINITION
Hepatic inflammatory process manifested by ↑ serum aminotransferase and liver-associated
autoantibodies.
Variable severity.
Fifteen to twenty percent of cases associated with HBV.
Clinical constellation that suggests immune-mediated disease process responsive
to immunosuppressive treatment.
SIGNS AND SYMPTOMS
Variable.
May mimic acute viral hepatitis.
Onset insidious.
May be asymptomatic or may have fatigue, malaise, anorexia, or amenorrhea.
Extrahepatic signs include arthritis, vasculitis, and nephritis.
Mild to moderate jaundice.
DIAGNOSIS
Detection of autoantibodies (anti-smooth muscle, anti-liver-kidney-microsome, anti-soluble
live antigen).
Liver biopsy.
Exclude other disease.
TREATMENT
Corticosteroid.
Azathioprine.
Reye Syndrome
DEFINITION
Acute encephalopathy and fatty degeneration.
Hepatic dysfunction (>3-fold ↑ in ALT, AST, and/or ammonia levels).
No other explanation for cerebral edema or hepatic abnormality.
↓ incidence secondary to awareness about association with the use of aspirin during
the illness relation to acetylsalicylic acid (ASA) ingestion, most commonly associated
with influenza and varicella.
Many other “Reye-like” syndromes exist (medium-chain fatty-acid oxidation defect
or urea-cycle defects).
SIGNS AND SYMPTOMS
Stereotypic, biphasic course.
Usually see prodromal illness, upper respiratory infection (URI), influenza, or
varicella chickenpox initially, followed by a period of apparent recovery, then see
abrupt onset of protracted vomiting 5–7 days after illness onset.
May see delirium, combative behavior, and stupor.
First neurologic manifestation: Lethargy.
Neurologic symptoms including seizures, coma, or death.
Slight to moderate liver enlargement.
DIAGNOSIS
Based on clinical staging.
Liver biopsy may show yellow to white color because of high triglyceride content.
TREATMENT
Airway, breathing, circulation (ABC) is the priority.
Bedside glucose (provide dextrose to manage hypoglycemia).
No specific treatment.
Control intracranial pressure (ICP) secondary to cerebral edema.
Supportive management depending on clinical stage.
α1-Antitrypsin Deficiency
DEFINITION
α1-Antitrypsin is a major protease inhibitor (PI).
A small percentage of homozygous patients have neonatal cholestasis, and later
in childhood cirrhosis.
Present in >20 codominant alleles; only a few associated with defective PI.
PI ZZ usually predisposes to clinical deficiency (<20% develop neonatal cholestasis).
EXAM TIP
The most likely clinical manifestation of α1-antitrypsin deficiency in the newborn is jaundice (neonatal cholestasis).
SIGNS AND SYMPTOMS
Variable course.
Jaundice, acholic stools, and hepatomegaly in first week of life; jaundice clears
by second to fourth month.
May have complete resolution, persistent liver disease, or cirrhosis.
Older children may present with chronic liver disease.
DIAGNOSIS
Determination of α1-antitrypsin phenotype.
Confirmed by liver biopsy.
TREATMENT
Liver transplant curative.
No other effective treatment.
Wilson Disease
DEFINITION
Autosomal-recessive disease characterized by excessive copper deposition in brain
and liver.
Worldwide incidence: 1/30,000.
SIGNS AND SYMPTOMS
Variable manifestations, including:
Asymptomatic in early stages.
Jaundice, abdominal pain.
Hepatomegaly, subacute/chronic hepatitis or fulminant liver failure.
Portal hypertension, ascites, edema, esophageal bleeding.
Delayed puberty, amenorrhea, or coagulation defect.
Psychosis.
Tremors.
Kayser-Fleischer rings are greenish-brown rings of pigment seen at the limbus of
the cornea, reflecting deposits of copper in Descemet membrane. They can be seen with
the naked eye in patients with blue eyes. In patients with dark eyes, a slit lamp
is often needed to identify them. Ninety percent of patients with Wilson disease have
Kayser-Fleischer rings.
EXAM TIP
Consider ordering serum ceruloplasmin for any patient with an unexplained elevation of liver function tests (LFTs).
DIAGNOSIS
Copper indices reveal:
Low serum ceruloplasmin.
High serum copper level.
Liver biopsy for histochemistry and copper quantification.
Genetic testing, including siblings.
TREATMENT
Disease is always fatal if left untreated.
Zinc: Newest Food and Drug Administration (FDA)-approved agent; works by blocking
absorption of copper in GI tract.
Copper-chelating agents to ↓ deposition (e.g., penicillamine and trientine).
Restrict copper intake. Foods high in copper include (Source: Mayo Clinic Diet Manual):
Lamb, pork, pheasant, quail, duck, goose, squid, salmon, all organ meats (liver,
heart, kidney, brain), all shellfish (oysters, scallops, shrimp, lobster, clams, crab),
meat gelatin, soy protein, meat substitutes, tofu, all nuts and seeds, dried beans
(soybeans, lima beans, baked beans, garbanzo beans, pinto beans), dried peas, and
lentils.
Soy milk, chocolate milk, cocoa, chocolate.
Nectarines, commercially dried fruits (okay if dried at home).
Mushrooms, sweet potatoes, vegetable juice cocktail.
Barley, bran breads and bran cereals, cereals with >0.2 mg of copper per serving
(check label), millet, soy flour, soy grits, wheat germ, brewer’s yeast.
Patients with hepatic failure require liver transplant.
Hepatic Neoplasms
HEPATOBLASTOMA
DEFINITION
Rare in children.
Fewer than 65% of malignant tumors are hepatoblastomas.
Associated with Beckwith-Wiedemann syndrome.
Usually arises from the right lobe of the liver and is unifocal.
Two histologic types—epithelial and mixed.
SIGNS AND SYMPTOMS
Generally present in first 18 months of life.
Large, asymptomatic abdominal mass.
Abdominal distention and ↑ liver size.
Weight loss, anorexia, vomiting, and abdominal pain (as disease progresses).
May spread to regional lymph nodes.
DIAGNOSIS
α-Fetoprotein (AFP) level helpful as marker.
Diagnostic imaging includes ultrasound to detect mass, CT, or magnetic resonance
imaging (MRI).
TREATMENT
Complete resection of tumor.
Cisplatin and doxorubicin adjuvant chemotherapy.
More than 90% survival with multimodal treatment (surgery with chemotherapy).
Liver Abscesses
ECHINOCOCCUS
DEFINITION
Most widespread cestode.
Transmitted from domestic and wild canine animals.
Two species: Echinococcus granulosus and the more malignant Echinococcus multilocularis.
Hosts are dogs, wolves, coyotes, and foxes that eat infected viscera.
Humans are infected by ingesting contaminated food or water.
SIGNS AND SYMPTOMS
Majority of cysts in liver; most never symptomatic.
Early, nonspecific symptoms; later on, ↑ abdominal girth, hepatomegaly, vomiting,
or abdominal pain.
Anaphylaxis secondary to rupture and spillage of contents.
Second most common site is lungs; symptoms include chest pain and coughing or hemoptysis.
DIAGNOSIS
Clinical.
Ultrasound.
Serologic studies have high false-negative rate.
WARD TIP
Avoid spillage during surgery for Echinococcus—a major complication.
TREATMENT
Surgery.
May be CT guided.
If not amenable to surgery, may be treated with albendazole.
AMEBIC ABSCESS
DEFINITION
A very serious manifestation of disseminated infection.
SIGNS AND SYMPTOMS
Abdominal pain, distention, and liver enlargement with tenderness.
DIAGNOSIS
May see slight leukocytosis.
Moderate anemia.
↑ ESR.
Nonspecific ALT ↑.
Stool exam negative in >50% of patients.
CT or MRI.
TREATMENT
Metronidazole.
Chloroquine.
Aspiration of left-lobe abscesses if rupture is imminent.