The official definition of clinical depression is based on the following eight primary criteria:
• Poor appetite accompanied by weight loss, or increased appetite accompanied by weight gain
• Insomnia or excessive sleep habits (hypersomnia)
• Physical hyperactivity or inactivity
• Loss of interest or pleasure in usual activities, or decrease in sexual drive
• Loss of energy; feelings of fatigue
• Feelings of worthlessness, self-reproach, or inappropriate guilt
• Diminished ability to think or concentrate
• Recurrent thoughts of death or suicide
The presence of five of these eight symptoms definitely indicates clinical depression; an individual with four is probably depressed. The symptoms must be present for at least one month to be called clinical depression.
Depression reflects a disturbance in mood. Used in this context, mood means a prolonged emotional tone that dominates an individual’s outlook. Normal moods (sadness, grief, elation, etc.), which are typically transient, are a part of everyday life, making the demarcation between “normal” and “abnormal” often difficult to determine. Depression is the most common mood disorder.
Obviously, there is a spectrum of clinical depression, ranging from mild feelings of depression to serious consideration of suicide. Mild depression is also known as dysthymia. Like clinical depression, dysthymia is diagnosed according to certain criteria. In order to be officially diagnosed as dysthymic, a person must be depressed most of the time for at least two years (one year for children or adolescents) and have at least three of the following symptoms:
• Low self-esteem or lack of self-confidence
• Pessimism, hopelessness, or despair
• Lack of interest in ordinary pleasures and activities
• Withdrawal from social activities
• Fatigue or lethargy
• Guilt or ruminating about the past
• Irritability or excessive anger
• Lessened productivity
• Difficulty concentrating or making decisions
Approximately 20 million Americans suffer from true clinical depression each year, and more than 30 million Americans take antidepressant drugs. The obvious question is: “Why are so many people depressed?” From a nonphysiological standpoint, several basic theoretical models of depression attempt to answer this question:
• The “aggression-turned-inward” construct. Although this behavior is apparent in many clinical cases, the theory has no substantial proof.
• The “loss model.” This model postulates that depression is a reaction to the loss of a person, a thing, status, self-esteem, or even a habit.
• The “interpersonal relationship” model. This theory holds that depression is an extension or outgrowth of behaviors used to control others, such as pouting, silence, or ignoring something or someone. The initial behaviors fail to serve the need, and so the problem worsens.
• The “learned helplessness” model. This theorizes that depression is the result of habitual feelings of pessimism and hopelessness.
• The “biogenic amine” hypothesis. This stresses biochemical derangement characterized by imbalances of biogenic amines.
• The analytical (or adaptive) rumination hypothesis. In this model, the ruminative thinking processes of a person with depression facilitate complex, social problem solving.
Of the various psychological theories of depression, the one that may have the most merit is the learned helplessness model, developed by Martin Seligman, Ph.D. During the 1960s, Dr. Seligman discovered that animals could be trained to be helpless. His animal model provided a valuable clue to human depression, as well as serving as the research model to test antidepressant drugs.1
The “Learned Helplessness” Model
Seligman’s early experiments were performed on three groups of dogs. The first group of dogs received an escapable electrical shock. The dogs could turn off the shock by simply pressing a panel with their noses. This group of dogs would thus have control. The dogs in the second group were “yoked” to the first group. They got exactly the same shocks as the first group but could not turn off the shock. The shock would cease only when the “yoked” dog in the first group would press its nose to the panel. Thus the second group of dogs had no control over the degree of shock they received. The third group of dogs received no shocks at all.
Once the dogs went through this first part of the experiment, they were placed in a “shuttle box,” a box separated in the middle by a small barrier that the dogs could jump over. The dogs would be electrically shocked but could escape the shock by simply jumping over the barrier to the other side. Seligman hypothesized that the first and third groups would quickly figure this out but that the second group of dogs would have learned to be helpless in that they would believe nothing they could do mattered. Seligman thought that the dogs in the second group would simply lie down and accept the shock.
As predicted, the first and third groups of dogs learned within seconds that they could avoid the shock by jumping over the barrier, while the dogs in the second group would simply lie down and not even make an effort to jump over the barrier, though they could see the other side of the shuttle box. Seligman and his colleagues went on to show that many humans react in a fashion identical to that of animals in these experiments.
The adoption of Seligman’s model was revolutionary in psychopharmacology, as it became an effective experiment to test antidepressant drugs. Basically, when animals that had learned to be helpless were given antidepressants, they would unlearn helplessness and start exerting control over their environment. Researchers discovered that when animals learned to be helpless, this resulted in alteration of brain monoamine content. The drugs would restore proper monoamine balance and alter the animals’ behavior. Researchers also discovered that when animals with learned helplessness were taught how to gain control over their environment, their brain chemistry also normalized. The alteration in brain monoamine content in the animals with learned helplessness mirrors the altered monoamine content in human depression.
Although most physicians look quickly to drugs to alter brain chemistry, helping patients to gain greater control over their lives actually produces even greater biochemical changes. One of the most powerful techniques to produce the necessary biochemical changes in the brains of depressed individuals is to teach them to be more optimistic.
Outside the laboratory setting, Seligman discovered that the determining factor in how a person would react to uncontrollable events, either “bad” or “good,” was his or her explanatory style—the way in which the person explained events. Optimistic people were immune to becoming helpless and depressed. However, individuals who were pessimistic were extremely likely to become depressed when something went wrong in their lives. Seligman and other researchers also found a direct correlation between an individual’s level of optimism and the likeliness of developing not only clinical depression but other illnesses as well.2 In one of the longer studies, patients were followed for a total of 35 years. Optimists rarely got depressed, but pessimists were extremely likely to battle depression and other psychological disturbances.
For more information, see the chapter “A Positive Mental Attitude.”
The Effects of Different Levels of Serotonin |
|
OPTIMAL LEVEL OF SEROTONIN |
LOW LEVEL OF SEROTONIN |
Hopeful, optimistic |
Depressed |
Calm |
Anxious |
Good-natured |
Irritable |
Patient |
Impatient |
Reflective and thoughtful |
Impulsive |
Loving and caring |
Abusive |
Able to concentrate |
Short attention span |
Creative, focused |
Blocked, scattered |
Able to think things through |
Flies off the handle |
Responsive |
Reactive |
Does not overeat carbohydrates |
Craves sweets and high carbohydrate foods |
Sleeps well with good dream recall |
Insomnia and poor dream recall |
Depression as a Result of Low Serotonin Level
Serotonin is an important neurotransmitter—a chemical messenger responsible for transmitting information from one nerve cell to another. Serotonin has been referred to as the brain’s own mood-elevating and tranquilizing drug. There is a lot of support for this sentiment. Because the manufacture of serotonin in the brain is dependent upon how much tryptophan is delivered to the brain, in experimental studies researchers can feed human volunteers or animals diets lacking tryptophan and note the effects of such a diet. The results from these sorts of studies have contributed greatly in our understanding on just how vital proper levels of serotonin are to a positive human experience. The table opposite contrasts optimal and low serotonin levels.
The lower the level of serotonin, the more severe the consequences. For example, low levels of serotonin are linked to depression, with the lowest levels being observed in people who have committed or attempted suicide.
Therapeutic Considerations
Modern psychiatry primarily focuses on manipulating neurotransmitter levels in the brain rather than identifying and eliminating the psychological, nutritional, and environmental factors that are responsible for producing the imbalances in serotonin, dopamine, GABA, and other neurotransmitters.
Most of the commonly used antidepressant drugs work primarily by increasing the effects of serotonin. Once serotonin is manufactured in the brain it is stored in nerve cells waiting for release. Upon release, the serotonin carries a chemical message by binding to receptor sites on the neighboring nerve cell. Almost as soon as the serotonin is released enzymes are at work that will either break down the serotonin or work to uptake the serotonin back into the brain cells. Either event results in stopping the serotonin effect. It is at this point that various drugs typically work to either inhibit the reuptake of serotonin or prevent its breakdown. Most popular drugs are referred to as SSRIs (selective serotonin reuptake inhibitors). Because serotonin reuptake is inhibited, there is more serotonin hanging around, capable of binding to receptor sites.
The effectiveness of antidepressant drugs has been the subject of several reviews. The results indicate that they have not been shown to work any better than a placebo in cases of mild to moderate depression, the most common reason for prescription medication, and claims that antidepressants are more effective in more severe conditions have little evidence to support them.3,4 In fact, the research indicates that SSRIs and other antidepressant drugs might actually increase the likelihood of suicide in adults and children.5
An additional alarming finding is that 25% of patients taking antidepressants do not even have depression or a diagnosable psychiatric problem.6 So the bottom line is that millions of people are using antidepressants for a problem they do not have, and for the people who have a diagnosable condition, these medications do not work in most cases anyway and may cause significant side effects. As one group of researcher concluded, “Given doubt about their benefits and concern about their risks, current recommendations for prescribing antidepressants should be reconsidered.”3 This statement is a clear mandate to consider natural medicine to deal with the causes of these mood disorders.
While antidepressant drugs are only marginally successful at best in alleviating depression, they do produce many side effects. Approximately 20% of patients experience nausea, 20% headaches, 15% anxiety and nervousness, 14% insomnia, 12% drowsiness, 12% diarrhea, 9.5% dry mouth, 9% loss of appetite, 8% sweating and tremor, and 3% rash. SSRIs also definitely inhibit sexual function. In studies where sexual side effects were thoroughly evaluated, 43% of men and women taking SSRIs reported loss of libido or diminished sexual response. There is also a significant risk for weight gain and the development of type 2 diabetes (see the box below).

SSRIS, WEIGHT GAIN, AND DIABETES
A little-appreciated side effect of SSRIs is weight gain. Statistics show that once weight gain begins in a patient taking these medications it usually does not stop. These drugs induce weight gain because they alter an area of the brain that regulates both serotonin levels and the utilization of glucose.7 While the human brain will usually make up 2% of our overall body mass, it is so metabolically active that it uses up to 50% of the glucose in the body for energy. Evidently the SSRIs disrupt the utilization of glucose in the brain in such a way that the brain senses that it is low in glucose. That sets in motion very powerful signals to eat. And, typically if a person has had sugar cravings or other food urges, those cravings will be dramatically enhanced by the drug. Other changes produced by the drug will lead to insulin resistance, setting the stage for inevitable weight gain and perhaps even type 2 diabetes. Studies have shown that individuals predisposed to diabetes are two to three times more likely to become diabetic if they use an antidepressant medication.8
There are effective alternatives to antidepressant drugs. For example, there are a number of lifestyle and dietary factors that lead to reduced serotonin levels. Chief among these factors are cigarette smoking, alcohol abuse, a high sugar intake, too much protein, blood sugar disturbances (hypoglycemia and diabetes), and various nutrient deficiencies. All of these factors have one thing in common: they lower serotonin levels by impairing the conversion of tryptophan to serotonin. A health-promoting lifestyle and diet go a long way in restoring optimal serotonin levels and relieving depression. But in the interim, natural agents such as 5-HTP, Saint-John’s-wort, lavender, or saffron extract can provide the necessary boost in mood to help make important changes in diet and lifestyle easier to accomplish.
Depression can often have an underlying organic (chemical) or physiological cause. Identification and elimination of the underlying cause is a critical step in most cases. Failure to address an underlying cause will make any antidepressant therapy less successful. It is important to rule out simple organic factors that are known to contribute to depression, such as nutrient deficiency or excess, drugs (prescription, illicit, alcohol, caffeine, nicotine, etc.), hypoglycemia, excessive consumption of alcohol, hormonal derangement, allergy, environmental toxins, and microbial factors. Each of these is discussed below. Regardless of any underlying organic cause, counseling is always recommended for the depressed individual.
Organic and Physiological Causes of Depression
• Preexisting physical conditions
![]() Diabetes
Diabetes
![]() Heart disease
Heart disease
![]() Lung disease
Lung disease
![]() Rheumatoid arthritis
Rheumatoid arthritis
![]() Chronic inflammation
Chronic inflammation
![]() Chronic pain
Chronic pain
![]() Cancer
Cancer
![]() Liver disease
Liver disease
![]() Multiple sclerosis
Multiple sclerosis
• Prescription drugs
![]() Anti-inflammatory agents
Anti-inflammatory agents
![]() Birth control pills
Birth control pills
![]() Antihistamines
Antihistamines
![]() Corticosteroids
Corticosteroids
![]() Tranquilizers and sedatives
Tranquilizers and sedatives
• Premenstrual syndrome
• Stress/low adrenal function
• Heavy metals
• Food allergies
• Hypothyroidism
• Hypoglycemia
• Nutritional deficiencies
• Sleep disturbances
There are a number of counseling techniques that can be quite useful. The therapy that has the most merit and support in the medical literature is cognitive therapy. In fact, cognitive therapy has been shown to be as effective as antidepressant drugs in treating moderate depression.9,10 However, while there is a high rate of relapse of depression when drugs are used, the relapse rate for cognitive therapy is much lower. People taking drugs for depression tend to have to stay on them for the rest of their lives. That is not the case with cognitive therapy because the patient is taught new skills to deal with the psychological factors that cause depression.11
Psychologists and other mental health specialists trained in cognitive therapy seek to change the way the depressed person consciously thinks about failure, defeat, loss, and helplessness. Cognitive therapists employ five basic tactics.
First, they help patients recognize the negative automatic thoughts that flit through consciousness at the times when the patient feels the worst. The second tactic is disputing the negative thoughts by focusing on contrary evidence. The third is teaching patients a different explanation to dispute the negative automatic thoughts. The fourth involves helping patients learn how to avoid rumination (the constant churning of a thought in one’s mind) by better controlling their own thoughts. The final tactic is questioning depression-causing negative thoughts and beliefs and replacing them with empowering positive thoughts and beliefs.
Cognitive therapy does not involve the long-drawn-out process of psychoanalysis. It is a solution-oriented psychotherapy designed to help patients learn skills to improve the quality of their lives.
Many hormones are known to influence mood; however, it is beyond the current scope of this chapter to address all of them. Instead, the focus will be on the effects of the thyroid and adrenal hormones.
Low Thyroid Function
Depression is often a first or early manifestation of thyroid disease, as even subtle decreases in available thyroid hormone are suspected of producing symptoms.12,13 The link between low thyroid function (hypothyroidism) and depression is well known in medical circles, but whether the low thyroid function is a result of depression or the depression is a result of low thyroid function remains to be answered. It is probably a combination. Please see the chapter “Hypothyroidism” for more information on determining thyroid function and promoting function when needed.
Stress and Adrenal Function
As with the thyroid gland, altered function of the adrenal gland is closely associated with depression. Often this dysfunction is the result of chronic stress—a major factor to consider in depression. It is critical to develop a positive way of dealing with the stress of modern life. See the chapter “Stress Management” for more information.
A laboratory technique that many nutritionally oriented physicians use to assess a patient’s level of and response to stress is the adrenal stress index. This test measures the level of the adrenal hormones cortisol and dehydroepiandrosterone (DHEA) in the saliva. The typical pattern found in depression is an elevated morning cortisol level and a decreased DHEA level.
The elevations in cortisol reflect a disturbance in the control mechanisms for adrenal function that reside in the hypothalamus and pituitary gland located at the center of the brain. Defects in adrenal regulation seen in affective disorders include excessive cortisol secretion (independent of stress responses) and abnormal release of cortisol. Defects in control mechanisms for adrenal hormones and thyroid function are hallmark features of depression.
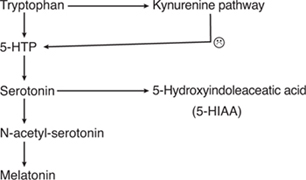
The brain effects of increased release of natural cortisol by the adrenal gland mirror the effects of synthetic cortisones such as prednisone: depression, mania, nervousness, insomnia, and, at high levels, schizophrenia. The effects of cortisol on mood is related to its activation of tryptophan oxygenase. This activation results in shunting of tryptophan to the kynurenine pathway at the expense of serotonin and melatonin synthesis.14 The significance of this shunting is described below.
Heavy metals (lead, mercury, cadmium, arsenic, nickel, and aluminum) as well as solvents (cleaning materials, formaldehyde, toluene, benzene, etc.), pesticides, and herbicides have an affinity for nervous tissue, where they are particularly damaging. As a result, a variety of psychological and neurological symptoms can occur, including depression, headaches, mental confusion, mental illness, tingling in extremities, abnormal nerve reflexes, and other signs of impaired nervous system function.15–17
History of exposure and urinary challenge testing are good screening mechanisms for environmental toxicity. Challenge testing employs a chelating agent—such as DMSA (meso-2,3-dimercaptosuccinic acid), which binds to lead; or DMPS (2,3-dimercapto-1-propane sulfonate), which binds to mercury—and promotes its excretion in the urine. These mobilization tests measure the level of toxic metal excreted in the urine for a period of 6 hours after taking the chelating agent.
For more information on dealing with environmental toxins, see the chapter “Detoxification and Internal Cleansing.”
A health-promoting lifestyle and diet are important in the treatment of depression. It is particularly important to stop smoking and decrease the consumption of alcohol, sugar, and caffeine. These lifestyle changes, coupled with regular exercise and a healthful diet, are more than likely to produce better clinical results than antidepressant drugs, with no side effects.
Alcohol
Alcohol is a brain depressant that increases adrenal hormone output, interferes with many brain cell processes, and disrupts normal sleep cycles. Chronic alcohol ingestion will deplete a number of nutrients, all of which will disrupt mood. Alcohol ingestion also leads to hypoglycemia. The resultant drop in blood sugar produces a craving for sugar because it can quickly elevate blood sugar. Unfortunately, increased sugar consumption ultimately aggravates the hypoglycemia. Hypoglycemia aggravates the mental and emotional problems of the alcoholic. Treatment options that can address both the depression and the addiction of the individual simultaneously are best.18 Supplementation with selenium in alcoholics can improve mood stability and help change drinking habits as well (see the section below on selenium).
Caffeine
Although caffeine is a well-known stimulant, the intensity of response to caffeine varies greatly, with people who are prone to feeling depressed or anxious tending to be especially sensitive to caffeine. The term caffeinism is used to describe a clinical syndrome similar to generalized anxiety and panic disorders; its symptoms include depression, nervousness, palpitations, irritability, and recurrent headache.19
Several studies have looked at caffeine intake and depression. For example, one study found that among healthy college students, those who drank moderate or high amounts of coffee scored higher on a depression scale than did low users. Interestingly, the moderate and high coffee drinkers also tended to have significantly lower academic performance.20 Several other studies have shown that depressed patients tend to consume fairly high amounts of caffeine (e.g., >700 mg per day).21,22 In addition, caffeine intake has been positively correlated with the degree of mental illness in psychiatric patients.23,24
The combination of caffeine and refined sugar seems to be even worse than either substance consumed alone. Several studies have found an association between this combination and depression. In one of the most interesting studies, 21 women and 2 men responded to an advertisement requesting volunteers “who feel depressed and don’t know why, often feel tired even though they sleep a lot, are very moody, and generally seem to feel bad most of the time.”25 After baseline psychological testing, the subjects were placed on a caffeine- and sucrose-free diet for one week. The subjects who reported substantial improvement were then challenged in a double-blind fashion. The subjects took either a capsule containing caffeine and a Kool-Aid drink sweetened with sugar or a capsule containing cellulose and a Kool-Aid drink sweetened with NutraSweet. Each challenge lasted up to six days. About 50% of test subjects taking caffeine and sucrose became depressed during the test period.
Another study using a format similar to the Kool-Aid study described earlier found that 7 of 16 depressed patients were depressed with the caffeine and sucrose challenge but symptom free during the caffeine- and sucrose-free diet and cellulose and NutraSweet test period.26
The average American consumes 150 to 225 mg caffeine per day, or roughly the amount of caffeine in one to two cups of coffee. Although most people appear to tolerate this amount, some people are more sensitive to the effects of caffeine than others. Even small amounts of caffeine, as found in decaffeinated coffee, are enough to affect some people adversely. Anyone with depression or any psychological disorder should avoid caffeine completely.
Exercise
Regular exercise may be the most powerful natural antidepressant available. In fact, many of the beneficial effects of exercise noted in the prevention of heart disease may be related just as much to its ability to improve mood as to its improvement of cardiovascular function.27 Furthermore, obesity is associated with depression.28 Various clinical studies have clearly indicated that exercise has profound antidepressant effects.29 These studies have shown that increased participation in exercise, sports, and physical activities is strongly associated with decreased symptoms of anxiety, depression, and malaise. Furthermore, people who participate in regular exercise have higher self-esteem, feel better, and are much happier than people who do not exercise.
Much of the mood-elevating effect of exercise may be attributed to the fact that regular exercise has been shown to increase the level of endorphins, which are directly correlated with mood.30 One of the most interesting studies that examined the role of exercise and endorphins in depression compared the beta-endorphin levels and depression profiles of 10 joggers with those of 10 sedentary men of the same age. The 10 sedentary men tested were more depressed, perceived greater stress in their lives, and had a higher level of cortisol and lower levels of beta-endorphins. As the researchers stated, this “reaffirms that depression is very sensitive to exercise and helps firm up a biochemical link between physical activity and depression.”31
At least 100 clinical studies have now evaluated the efficacy of an exercise program in the treatment of depression. In an analysis of 64 studies conducted before 1980, physical fitness training was shown to relieve depression and improve self-esteem and work behavior.32 In fact, exercise can be as effective as other antidepressants, including drugs and psychotherapy.33–35
The best exercises are either strength training (weight lifting) or aerobic activities such as walking briskly, jogging, bicycling, cross-country skiing, swimming, aerobic dance, and racket sports.
Diet
The dietary guidelines for depression are identical to the dietary guidelines for optimal health (see the chapter “A Health-Promoting Diet”). It is now a well-established fact that certain dietary practices cause a wide range of diseases, while others prevent them. Quite simply, a health-promoting diet provides optimal levels of all known nutrients and low levels of food components that are detrimental to health, such as sugar, saturated fats, cholesterol, salt, and food additives. A health-promoting diet is rich in whole, unprocessed foods. It is especially high in plant foods such as fruits, vegetables, grains, beans, seeds, and nuts, as these foods contain not only valuable nutrients but also additional compounds that have remarkable health-promoting properties. Although no one diet is a perfect fit for everyone, a four-and-a-half-year study of more than 10,000 people reported that those who ate a healthful Mediterranean diet were about half as likely to develop depression as those who said they did not stick to the diet.36
Elements of the Mediterranean Diet
High ratio of monounsaturated fatty acids to saturated fatty acids*
Moderate alcohol intake
High intake of legumes*
High intake of cereal (such as bread)
High intake of fruits and nuts*
High intake of vegetables
Low intake of meat and meat products
Moderate intake of milk and dairy products
High fish intake
* Elements mostly correlated with low depression risk
Stabilizing Blood Sugar Levels
One of the key dietary goals is to ensure blood sugar stability, as the brain requires a constant supply of glucose. In particular, hypoglycemia (low blood sugar) must be avoided. Symptoms of hypoglycemia can range from mild to severe and can include the following:
• Depression, anxiety, irritability, and other psychological disturbances
• Fatigue
• Headache
• Blurred vision
• Mental confusion
Several studies have shown hypoglycemia to be common in depressed individuals.37–39 A study of six countries showed a highly significant correlation between sugar consumption and the annual rate of depression.39 Simply eliminating refined carbohydrate from the diet is occasionally all that is necessary for effective therapy in patients who have depression due to reactive hypoglycemia.
A deficiency of any single nutrient can alter brain function and lead to depression, anxiety, and other mental disorders. However, the role of nutrient deficiency is just the tip of the iceberg with regard to the effect of nutrients on the brain and mood. Melvin Werbach, M.D., author of Nutritional Influences on Mental Illness, wrote:40
Behavioral Effects of Some Vitamin Deficiencies |
|
DEFICIENT VITAMIN |
BEHAVIORAL EFFECTS |
Thiamine |
Korsakoff’s psychosis, mental depression, apathy, anxiety, irritability |
Riboflavin |
Depression, irritability |
Niacin |
Apathy, anxiety, depression, hyperirritability, mania, memory deficits, delirium, organic dementia, emotional lability |
Biotin |
Depression, extreme lassitude, somnolence |
Pantothenic acid |
Restlessness, irritability, depression, fatigue |
B6 |
Depression, irritability, sensitivity to sound |
Folic acid |
Forgetfulness, insomnia, apathy, irritability, depression, psychosis, delirium, dementia |
B12 |
Psychotic states, depression, irritability, confusion, memory loss, hallucinations, delusions, paranoia |
Vitamin C |
Lassitude, hypochondriasis, depression, hysteria |
Vitamin D |
Depression, fatigue, seasonal affective disorder, cognitive impairment, memory loss |
Omega-3 fatty acids |
Depression, poor concentration, memory loss |
It is clear that nutrition can powerfully influence cognition, emotion, and behavior. It is also clear that the effects of classical nutritional deficiency diseases upon mental function constitute only a small part of a rapidly expanding list of interfaces between nutrition and the mind. Even in the absence of laboratory validation of nutritional deficiencies, numerous studies utilizing rigorous scientific designs have demonstrated impressive benefits from nutritional supplementation.
A high-potency multiple vitamin and mineral supplement provides a good nutritional foundation on which to build. In selecting a formula, it is important to make sure that it provides the full range of vitamins and minerals. Deficiencies of a number of nutrients are quite common in depressed individuals. The most common deficiencies are folic acid, vitamin B12, and vitamin B6. The significance of these deficiencies is discussed below.
Folic Acid and Vitamin B12
Folic acid and vitamin B12 function together in many biochemical processes. Folic acid deficiency is the most common nutrient deficiency in the world. In studies of depressed patients, 31 to 35% have been shown to be deficient in folic acid.41–44 In elderly patients this percentage may be even higher. Studies have found that among elderly patients admitted to a psychiatric ward, the proportion with folic acid deficiency ranges from 35 to 92.6%.45,46 Depression is the most common symptom of a folic acid deficiency. In the past, vitamin B12 deficiency has been less common than folic acid deficiency; nonetheless, it can also cause depression, especially in the elderly.47,48 The fortifying of the food supply with folic acid has reduced the incidence of deficiency and may actually accentuate the effects of vitamin B12 deficiency. Correcting folic acid and vitamin B12 deficiencies results in a dramatic improvement in mood.
Folic acid, vitamin B12, and a form of the amino acid methionine known as SAM-e (S-adenosyl-methionine) function as “methyl donors”—they carry and donate methyl molecules to important brain compounds including neurotransmitters. SAM-e is the major methyl donor in the body. The antidepressant effects of folic acid appear to be a result of raising brain SAM-e content.
One of the key brain compounds dependent on methylation is tetrahydrobiopterin (BH4). This compound functions as an essential coenzyme in the activation of enzymes that manufacture monoamine neurotransmitters such as serotonin and dopamine from their corresponding amino acids. Patients with recurrent depression have been shown to have reduced BH4 synthesis, probably as a result of low SAM-e levels. BH4 supplementation has been shown to produce dramatic results in these patients.49 Unfortunately, BH4 is not currently available commercially. However, since BH4 synthesis is stimulated by folic acid, vitamin B12, and vitamin C, it is possible that increasing these vitamin levels in the brain may stimulate BH4 formation and the synthesis of monoamines such as serotonin.50
Some evidence supports the contention that supplementing the diet with folic acid, vitamin C, and vitamin B12 can increase BH4 levels. In addition, the folic acid supplementation and the promotion of methylation reactions have been shown to increase the serotonin content.51–53 The serotonin-elevating effects are undoubtedly responsible for much of the antidepressant effects of folic acid and vitamin B12.
One review of three folate trials involving 247 depressed patients has been published.54 Two of the studies involving 151 people assessed the use of folate in addition to other treatment and found that adding folate reduced Hamilton Depression Scale (HDS) scores on average by a further 2.65. One of the studies, involving 96 people, assessed the use of folate instead of the antidepressant trazodone. This study did not find a significant benefit from the use of folate. Although the authors of this analysis considered these data “limited,” they acknowledged the potential role of folate as a supplement to treat depression. No side effects or toxicities were noted in any of the studies reviewed.
Typically the daily dosages of folic acid in the antidepressant clinical studies have been high: 15 to 50 mg.55 We do not recommend this dosage level. A dosage of 800 mcg of folic acid and 800 mcg of vitamin B12 should be sufficient in most circumstances to prevent deficiencies. Folic acid supplementation should always be accompanied by vitamin B12 supplementation to prevent folic acid from masking or aggravating a vitamin B12 deficiency.
Vitamin B6
B6 levels are typically quite low in depressed patients, especially women taking birth control pills or on hormone replacement therapy for menopausal symptoms.56–60 Considering the many functions of vitamin B6 in the brain, including the fact that it is absolutely essential in the manufacture of all monoamines, it is likely that many of the many people taking antidepressants may be suffering depression simply as a result of low vitamin B6. Patients with low B6 status usually respond well to supplementation. The typical effective dosage is 50 to 100 mg.
Zinc
Zinc serves as the mineral cofactor in more than 70 enzymes in the body.61 Not surprisingly, a growing body of evidence implicates low levels of zinc in mood disorders. Interestingly, it has been shown that depressed patients who have low baseline levels of zinc experience increases in these concentrations in the hippocampus and other brain regions after being given prescription antidepressant therapies.62,63
One small, placebo-controlled, double-blind pilot study of zinc supplementation in antidepressant therapy was conducted with patients who were diagnosed with major depression. Six patients received 25 mg zinc supplementation per day, while eight patients took a placebo. These patients were also treated with standard antidepressant therapy such as tricyclic antidepressants and selective serotonin reuptake inhibitors (SSRIs). Using standard scales to assess the efficacy of these antidepressant therapies, the researchers found that zinc supplementation significantly reduced depression scores after 6 and 12 weeks of supplementation when compared with a placebo.64 Although this was a small trial, it seems reasonable to use zinc as part of a multiple vitamin and mineral supplement.
Selenium
Low selenium status contributes to depressed mood, whereas high dietary or supplementary selenium has been shown to improve mood. Research has consistently reported that low selenium status was associated with a significantly increased incidence of depression, anxiety, confusion, and hostility.65,66
Chromium
Chromium functions in helping insulin as well as serotonin work properly. A small double-blind study of chromium picolinate was conducted in 15 patients with unusual types of major depressive disorder. Ten patients started with a dose of 400 mcg per day, which was increased to 600 mcg for the remainder of the study.67 The other five patients took a placebo. Of the patients on chromium, 70% responded positively to the treatment, vs. 0% of the placebo patients. Other outcomes were consistent with greater effect of chromium. Three patients on chromium failed to show any improvement. The chromium picolinate was well tolerated. Another successful study of eight patients with depression found some improvements as well.68
Low levels of vitamin D could be involved in depression in several ways given this vitamin’s importance in the human brain.69 In a study of 441 overweight people vitamin D levels were strongly associated with depression.70 Those with vitamin D levels below 16 mcg/dl were shown to be more depressed than people with higher vitamin D levels. When these subjects with low vitamin D levels were given vitamin D (20,000 IU or 40,000 IU per week) or a placebo, those given 40,000 IU had a 33% reduction in depression scores, those given 20,000 IU had a 20% reduction, and the placebo group had a 5% decrease. In another study, involving more than 12,000 subjects, low vitamin D levels were associated with depression.71 We recommend determination of vitamin D levels for people with a history of depression.
With the significant epidemiological evidence documenting a strong association between vitamin D deficiency and depression (as well as dementia, memory loss, and a whole host of other indications of impaired brain function) it was inevitable that researchers would try supplemental vitamin D for depression. While the research is still early, several studies have now shown success. In general, the lower the person’s vitamin D level, the more improvement is experienced with supplementation.72 In addition, the greater the increase, the greater the benefit. Typical effective dosages were in the range of 50,000 IU per week, with low levels of supplementation showing inconsistent results. A single dose of 50,000 IU once a year was not found effective.73
Omega-3 Fatty Acids
An insufficiency of the long-chain omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) has been linked to depression.74 Studies have also reported that countries with high rates of fish oil consumption have low rates of depressive disorder. This may be related to the impact of dietary fatty acids on the phospholipid composition of brain cell membranes. Although it is thought that the cell is programmed to selectively incorporate the different fatty acids it needs to maintain optimal function, a lack of essential fatty acids (particularly the omega-3 oils) and an excess of saturated fats and animal fatty acids lead to the formation of cell membranes that have much less fluidity than normal.
A relative deficiency of essential fatty acids in cellular membranes substantially impairs cell membrane function. Because the basic function of the cell membrane is to serve as a selective barrier that regulates the passage of molecules into and out of the cell, a disturbance of structure or function disrupts homeostasis. The medical literature has demonstrated that there are changes in fatty acid levels in the red blood cells of depressed patients and in serum fatty acid composition in depressive disorder.75
Because the brain is the richest source of fats in the human body and proper nerve cell function is critically dependent on proper membrane fluidity, alterations in membrane fluidity affect behavior, mood, and mental function. Studies have shown that the physical properties of brain cell membranes (including fluidity) directly influence neurotransmitter synthesis, signal transmission, uptake of serotonin and other neurotransmitters, neurotransmitter binding, and the activity of monoamine oxidase. All of these factors have been implicated in depression and other psychological disturbances.
In one small study, 20 patients diagnosed with major depressive disorder participated in a four-week, double-blind evaluation of either a placebo or EPA added to their ongoing antidepressant therapy. The effect of EPA was significant from week two of treatment, similar to the time course for effectiveness of antidepressant medications. The effect of the placebo was minimal. Item analysis showed that EPA also reduced core depressive symptoms such as depressed mood, guilt feelings, and feelings of worthlessness, as well as insomnia.76
Omega-3 fatty acids may reduce the development of depression just as they reduce the development of coronary artery disease.77 The evidence supporting this statement includes:
• The quantity and type of dietary fats consumed influence serum lipids and alter the biophysical and biochemical properties of cell membranes.
• Epidemiological studies in various countries and the United States have indicated that decreased consumption of omega-3 fatty acids correlates with increasing rates of depression.
• A consistent association between depression and coronary artery disease also exists.
S-adenosyl-methionine (SAM-e)
SAM-e is involved in the methylation of important brain chemicals, including neurotransmitters and phospholipids such as phosphatidylcholine and phosphatidylserine. Normally, the brain manufactures all the SAM-e it needs from the amino acid methionine. However, SAM-e synthesis is impaired in depressed patients. Supplementing the diet with SAM-e in depressed patients results in increased levels of serotonin, dopamine, and phosphatidylserine, and improved binding of neurotransmitters to receptor sites. This produces increased serotonin and dopamine activity and improved brain cell membrane fluidity, and thus significant clinical improvement.78–80
The results of a number of clinical studies suggest that SAM-e is one of the most effective natural antidepressants. Unfortunately, its use is still limited, owing to its high price. Many clinical trials used injectable SAM-e. However, more recent studies using a new oral preparation at a dosage of 400 mg four times per day (1,600 mg total) have demonstrated that SAM-e is just as effective orally. SAM-e is better tolerated and has a quicker onset of antidepressant action than typical antidepressant drugs. Overall, in double-blind studies comparing SAM-e with antidepressant drugs, 76% of the SAM-e group showed significant improvements in mood compared with only 61% in the drug group.81–90
No significant side effects have been reported with oral SAM-e. However, because SAM-e can cause nausea and vomiting in some people, it is recommended that it be started at a dosage of 200 mg twice per day for the first day, and increased to 400 mg twice per day on day 3, then to 400 mg three times per day on day 10, and finally to the full dosage of 400 mg four times per day after 20 days.
Individuals with bipolar (manic) depression should not take SAM-e. Because of SAM-e’s antidepressant activity, these individuals are susceptible to experiencing hypomania or mania. This effect is exclusive to some individuals with bipolar depression.
Depression and fatigue have been linked to food allergies for more than 65 years. In 1930, Rowe coined the term allergic toxemia to describe a syndrome that included the symptoms of depression, fatigue, muscle and joint aches, drowsiness, difficulty in concentration, and nervousness.91 Although the term is not used anymore, food allergies still play a major role in many cases of depression.92
For more than 30 years, L-tryptophan was used by millions of people in the United States and around the world safely and effectively for insomnia and depression. But in October 1989, some people taking tryptophan started reporting strange symptoms to physicians—severe muscle and joint pain, high fever, weakness, swelling of the arms and legs, and shortness of breath.93 It was dubbed eosinophilia-myalgia syndrome (EMS).
Laboratory studies showed that the blood of subjects with EMS contained a high level of eosinophils. In patients with EMS, eosinophil levels rose to greater than 1,000/mm3, roughly double the normal level, and the proportion of eosinophils often increased to levels above 30% of white cells, whereas the normal level is below 5%.
The problem with such severe elevations in eosinophils is that these white blood cells contain packets that have high levels of histamine and other allergic and inflammatory compounds. When the eosinophils release these compounds, this leads to intense symptoms of an allergic and inflammatory nature (e.g., severe muscle and joint pain, high fever, weakness, swelling of the arms and legs, skin rashes, and shortness of breath)—the same symptoms as those experienced by people with EMS. It was suspected that one or more newly introduced contaminants that activated eosinophils and other white blood cells had to be the reason behind EMS because L-tryptophan had been used successfully by more than 30 million people worldwide without side effects.
Detailed analysis of all evidence by the Centers for Disease Control and Prevention (CDC) led to the conclusion that the cause of the EMS epidemic could be traced to one Japanese manufacturer, Showa Denko.94,95 Of the six Japanese companies supplying L-tryptophan to the United States, Showa Denko was the largest, supplying 50% to 60%. The L-tryptophan was used not only as a nutritional supplement but also in infant formulas and nutrient mixtures used for intravenous feeding.
The L-tryptophan produced from October 1988 to June 1989 by Showa Denko became contaminated with substances now linked to EMS owing to changes in the filtration process. Examination of the pre-filtered material indicated that it had no detectable levels of the impurities linked to EMS. Somehow the filtration process produced the contaminants.
Although the epidemic of EMS during the last half of 1989 was clearly related to the contaminated L-tryptophan produced by Showa Denko, there have been a handful of other reported cases of EMS in people who never took L-tryptophan and in people who took L-tryptophan before the contaminated batch manufactured by Showa Denko hit the shelves. It is likely that in these earlier reports of EMS-like illnesses among L-tryptophan users, the subjects were also using contaminated L-tryptophan and they also had a predisposition to EMS (discussed later).96,97 This conclusion is based on the fact that uncontaminated tryptophan has never produced EMS. Clearly, it is absolutely essential that uncontaminated L-tryptophan be used to avoid the possibility of EMS.
The total number of reported cases of EMS in the United States eventually reached 1,511, with 36 deaths.94–97 An interesting aspect of the entire L-tryptophan catastrophe is that it did not affect more people. Based on very detailed studies, it was concluded that EMS affected 144 out of every 100,000 men and 268 out of every 100,000 women taking L-tryptophan.98 If 50% of these L-tryptophan users were taking Showa Denko’s L-tryptophan, we can assume that EMS affected 72 of every 100,000 men and 134 of every 100,000 women taking contaminated L-tryptophan. In other words, roughly 1 of every 250 people who took the contaminated L-tryptophan developed EMS.
The obvious question is why not everyone taking the contaminated L-tryptophan experienced EMS. The answer appears to be that only those with an abnormal activation of the kynurenine pathway reacted to the contaminant.99 Kynurenine and its metabolites (especially quinolic acid) are linked to other EMS-related illnesses as well, including toxic oil syndrome, one of the largest food-related epidemics to date. This syndrome occurred in Spain during May 1991. It affected more than 20,000 people and caused more than 12,000 hospitalizations. It was caused by the ingestion of canola oil contaminated with a compound similar to one found in the contaminated Showa Denko L-tryptophan.100
An interesting finding from studies conducted by researchers from the Centers for Disease Control was that people who took a multivitamin preparation were extended some protection against EMS.101 When regular vitamin users did develop EMS, it was less severe than the EMS experienced by those who didn’t use vitamins. A likely explanation for this occurrence is that either the vitamins (particularly vitamin B6 and niacin) shunted tryptophan metabolism away from the kynurenine pathway or the contaminants were somehow metabolized by vitamin-dependent enzymes.
Tryptophan in Depression
Uncontaminated L-tryptophan eventually returned to the marketplace, though we prefer 5-HTP (discussed below). The basic theory of tryptophan supplementation in depression (and insomnia) is that it will increase the level of serotonin and melatonin in the brain. This theory is supported by considerable evidence that many depressed individuals have low tryptophan and serotonin levels. Unfortunately, supplementation with L-tryptophan in depressed patients has produced mixed results in published clinical trials. In only two out of eight studies comparing L-tryptophan with a placebo was L-tryptophan shown to be more effective than the placebo. But, interestingly, 9 of 11 studies comparing L-tryptophan with conventional antidepressant drugs showed no difference.102–107
Among the many factors to consider when looking at these studies are study size, severity of depression, duration, and dosage. In addition, a number of factors such as hormones (e.g., estrogen and cortisol), as well as tryptophan itself, stimulate the activity of tryptophan oxygenase, with the result that tryptophan is converted to kynurenine and less tryptophan is delivered to the brain.
In summary, L-tryptophan is only modestly effective in the treatment of depression when used alone.108 In order to gain any real benefit from L-tryptophan, it must be used along with vitamin B6 and the niacinamide form of vitamin B3 to help block the kynurenine pathway to provide better results. Better yet is the use of 5-HTP.
5-Hydroxytryptophan (5-HTP)
Tryptophan must be converted to 5-hydroxytryptophan before it is metabolized to serotonin. Unlike tryptophan, 5-HTP cannot be converted to kynurenine and easily crosses the blood-brain barrier. As a result, while only 3% of an oral dose of L-tryptophan is converted to serotonin, more than 70% of an oral dose of 5-HTP is converted to serotonin. In addition to increasing serotonin levels, 5-HTP causes an increase in endorphin and catecholamine levels. Numerous double-blind studies have shown that 5-HTP is as effective as SSRIs and tricyclic antidepressants and is less expensive, better tolerated, and associated with fewer and much milder side effects.109–113
Some of the first clinical studies on 5-HTP for the treatment of depression began in the early 1970s in Japan. These patients received 5-HTP at dosages ranging from 50 to 300 mg per day. The researchers observed a quick response (within two weeks) in more than half of the patients. More than 70% of the patients either experienced complete relief or were significantly improved, and none experienced significant side effects. An interesting aspect in two of these studies was the fact that 5-HTP was shown to be effective in some patients (50% in one study, 35% in another) who had not responded positively to any other antidepressant.114,115
The most detailed of the Japanese studies was conducted in 1978.116 The study enrolled 59 patients with depression: 30 male and 29 female. The groups were mixed in that both unipolar and bipolar depressions were included, along with a number of other subcategories of depression. The severity of the depression in most cases was moderate to severe. Patients received 5-HTP in dosages of 50 or 100 mg three times per day for at least three weeks. The antidepressant activity and clinical effectiveness of 5-HTP were determined by using a rating scale developed by the Clinical Psychopharmacology Research Group in Japan. Results indicated that 5-HTP was helpful in 14 out of 17 patients with unipolar depression and 12 out of 21 patients with bipolar depression. The degree of improvement in most cases ranged from excellent to very good. The results achieved in this study were quite impressive given how rapidly they were achieved. Thirty-two of the 40 patients who responded to 5-HTP did so within the first two weeks of therapy. Typically, in most studies with antidepressant drugs, the benefits are not apparent until after two to four weeks of use. For this reason, the length of a study assessing antidepressant drugs should be at least six weeks because it may take that long to significantly affect brain chemistry in a positive manner. In contrast, many of the studies with 5-HTP were shorter than six weeks because statistically significant results were achieved so soon. However, the longer 5-HTP is used, the better the results. Some people may need to be on 5-HTP for at least two months before experiencing benefits.
The only major side effect noted in this study was mild nausea. The occurrence of nausea due to 5-HTP is actually less frequent than that experienced with other antidepressant drugs (roughly 10% of subjects taking 5-HTP at a dose of 300 mg per day experience nausea compared with about 23% taking Prozac) and about the same as that which occurs with a placebo. Nonetheless, mild nausea may be a natural consequence of elevated serotonin levels with 5-HTP. About 30% of the 5-HTP taken orally is converted to serotonin in the intestinal tract. This can lead to a mild case of nausea. Fortunately, this effect wears off after a few weeks of use.
A 5-HTP dosage of 150 to 300 mg per day is sufficient in most cases. For example, in one study it was shown that 13 out of 18 subjects with depression given 5-HTP at a level of 150 or 300 mg per day experienced good to excellent results.117 This percentage of responders is quite good, but if the level of serotonin in the blood is viewed as a rough indicator of brain serotonin levels, some interesting conclusions can be made (see the table above). In some cases a higher dosage may be necessary.
Level of Serotonin in Blood (ng/ml): Controls, Responders, and Nonresponders |
||
|
BEFORE |
AFTER 1 WEEK (150 OR 300 MG/DAY 5-HTP) |
Normal subjects |
150 |
NA |
Responders |
78 |
148 |
Nonresponders |
56 |
77 |
The measurements above suggest that serotonin levels in depressed individuals are considerably lower than those found in normal subjects and that individuals who respond to 5-HTP show a rise in serotonin to levels consistent with normal subjects. The level of serotonin in those who do not respond to 5-HTP remained quite low. These results imply that nonresponders may require higher dosages to raise serotonin levels or that additional support may be necessary. When higher doses are prescribed, it is important that the 5-HTP be taken in divided dosages not only to reduce the problem with nausea but also because the rate of brain cell uptake of 5-HTP is limited.
The antidepressant effects of 5-HTP were compared with L-tryptophan in the early 1970s.118 In one study, 45 subjects with depression were given L-tryptophan (5 g per day), 5-HTP (200 mg per day), or a placebo. The patients were matched in clinical features (e.g., age, sex) and severity of depression. The main outcome measure was the Hamilton Depression Scale, the most widely used assessment tool in clinical research on depression.
The HDS score is determined by having the test subject complete a series of questions in which he or she rates the severity of symptoms on a numerical basis, as follows:
0: Not present
1: Present but mild
2: Moderate
3: Severe
4: Very severe
Symptoms assessed by the HDS include depression, feelings of guilt, insomnia, bodily symptoms of depression (gastrointestinal disturbance, headaches, muscle aches, heart palpitations), and anxiety. The HDS is popular in research because it provides a good assessment of the overall symptoms of depression. The table below shows the results of the study.
Hamilton Depression Scale Scores from a Comparative Study of 5-HTP, Tryptophan, and Placebo |
|||
|
5-HTP |
TRYPTOPHAN |
PLACEBO |
Score at beginning of study |
26 |
25 |
23 |
Score at end of 30-day study |
9 |
15 |
19 |
A review of head-to-head comparison studies showed that 5-HTP, at a dosage of 200 mg per day, produced therapeutic improvement on a par with tricyclic antidepressant drugs. Research has also shown that combining 5-HTP with clomipramine and other types of antidepressant drugs produces better results than any of the compounds given alone.110 For example, in one study, 5-HTP combined with a monoamine oxidase (MAO) inhibitor demonstrated significant advantages compared with the MAO inhibitor alone.118 This line of research suggests that 5-HTP might also be used in conjunction with Saint-John’s-wort extract and ginkgo biloba extract, two herbal medicines with proven antidepressant activity.
Because 5-HTP was expensive in 1972, researchers developed a test to determine who was most likely to respond to it, so that it would not be wasted on people who were unlikely to respond. The patients in the test first had a spinal tap to measure the level of 5-hydroxyindoleacetic acid (5-HIAA, the breakdown product of serotonin) in the cerebrospinal fluid (CSF). The drug probenecid, which prevents the transport of 5-HIAA from the CSF to the bloodstream, was given for the next three days. As a result of this blocking action, the amount of serotonin produced over a four-day period could be calculated by a repeat spinal tap. Since the 5-HIAA could not leave the CSF, it accumulated and provided a measure of serotonin manufacture.119,120
The researchers discovered that the average level of 5-HIAA after three days of probenecid was significantly lower in depressed individuals than in controls matched for age, sex, and weight. This low level of serotonin reflected a decreased rate of manufacture within the brain. They also found that 5-HTP was most effective in patients with a low 5-HIAA response to three days of probenecid. In other words, 5-HTP is most effective as an antidepressant when the amount of serotonin manufactured in the brain is reduced.
As stated earlier, 5-HTP often produces good results in patients who are unresponsive to antidepressant drugs. One of the more impressive studies involved 99 patients described as suffering from “therapy-resistant” depression.109 These patients had not responded to any previous therapy, including all available antidepressant drugs and electroconvulsive therapy. These therapy-resistant patients received 5-HTP at dosages averaging 200 mg per day (range: 50 to 600 mg). Complete recovery was seen in 43 of the 99 patients, and significant improvement was noted in 8 more. Such significant improvement in patients suffering from long-standing, unresponsive depression is quite impressive, prompting the author of another study to note:121
5-HTP merits a place in the front ranks of antidepressants instead of being used as a last resort. I have never in 20 years used an agent that (1) was effective so quickly; (2) restored patients so completely to the persons they had been and their partners had known; and (3) was so entirely without side effects.
A 1987 review article on 5-HTP in depression highlighted the need for well-designed, double-blind, head-to-head studies of 5-HTP vs. standard antidepressant drugs.110 Although 5-HTP was viewed as an antidepressant agent with few side effects, the authors of this review felt that the big question to answer was how 5-HTP compared with the new breed of antidepressant drugs, SSRIs such as Prozac, Paxil, and Zoloft. In 1991 a double-blind study comparing 5-HTP with an SSRI, fluvoxamine (Luvox), was conducted in Switzerland.112 Fluvoxamine is used primarily in the United States as a treatment for obsessive-compulsive disorder, an anxiety disorder that affects an estimated 5 million Americans. Fluvoxamine exerts antidepressant activity comparable to (if not better than) other SSRIs such as Prozac, Zoloft, and Paxil.
In the study, subjects received either 5-HTP (100 mg) or fluvoxamine (50 mg) three times per day for 6 weeks. The assessment methods used to judge effectiveness included the HDS, a self-assessment depression scale, and a physician’s assessment. As seen in the data below, the percentage decrease in depression was slightly better in the 5-HTP group (60.7 vs. 56.1%). 5-HTP was quicker-acting than the fluvoxamine, and a higher percentage of patients responded to 5-HTP than to fluvoxamine.
One of the most important advantages of 5-HTP may be its ability to not just reduce insomnia but improve the quality of sleep. By contrast, antidepressant drugs greatly disrupt sleep processes.
The data clearly show that 5-HTP is equal to or better than standard antidepressant drugs, and the side effects are much less severe. In the study comparing 5-HTP with fluvoxamine, the two treatment groups did not differ significantly in the number of patients experiencing adverse events, but the degree of severity was highly significant: fluvoxamine predominantly produced moderate to severe side effects, while 5-HTP produced primarily mild side effects. The most common side effects with 5-HTP were nausea, heartburn, and gastrointestinal problems (flatulence, feelings of fullness, and rumbling sensations).
Saint-John’s-Wort
Extracts of Saint-John’s-wort (Hypericum perforatum) standardized for hypericin are the most thoroughly researched natural antidepressants. More than 30 double-blind, randomized trials involving more than 2,200 patients with mild to moderately severe depression have shown that standardized Saint-John’s-wort extracts yield excellent results with far fewer side effects than standard antidepressant medications, lower cost, and greater patient satisfaction.122–126
In these studies, Saint-John’s-wort extract was shown to produce improvements in many psychological symptoms:
• Depression
• Anxiety
• Apathy
• Sleep disturbances
• Insomnia
• Anorexia
• Feelings of worthlessness
Improvement in Specific Depression Symptoms |
||
SYMPTOM |
5-HTP (%) |
FLUVOXAMINE (%) |
Depressed mood |
65.7 |
61.8 |
Anxiety |
58.2 |
48.3 |
Physical symptoms |
47.6 |
37.8 |
Insomnia |
61.7 |
55.9 |
GBE exerts good antidepressant effects, especially in patients older than 50. Researchers became interested in the antidepressant effects of GBE as a result of the improvement in mood reported by patients suffering from cerebrovascular insufficiency who were treated with ginkgo in double-blind studies.130–133 In a recent double-blind study, 40 older patients (ranging in age from 51 to 78) with depression who had not benefited fully from standard antidepressant drugs were given either 80 mg GBE three times per day or a placebo.134 By the end of the fourth week of the study, the total score on the HDS was reduced on average from 14 to 7. At the end of the 8-week study, the total score in the GBE group had dropped to 4.5. In comparison, the placebo group’s score dropped only from 14 to 13. This study indicates that GBE can be used with standard antidepressants and may enhance their effectiveness, particularly in older patients.
THE DEATH OF AN HERBAL SHINING STAR
In the late 1990s the brightest star in herbal medicine was without question Saint-John’s-wort extract. In fact, in Germany it was estimated that in 1996 physicians prescribed Saint-John’s-wort extract eight times more frequently than the drug Prozac for the treatment of depression. In the United States, on June 27, 1997, the television news show 20/20 aired a segment called “Nature’s Rx: Using Herb St. John’s Wort to Treat Depression.” This airing brought considerable attention to not only Saint-John’s-wort extract but also the entire herbal medicine category. The increased popularity of this safe and effective natural product certainly did not go unnoticed by drug manufacturing executives.
In April 2001, however, a blaring headline on the cover of Time magazine stated “St. John’s What?” The article went on to highlight the results of a study demonstrating that Saint-John’s-wort didn’t work any better than a placebo.127 However, this particular study featured 200 patients who had had severe depression for at least two years, not the typical mild to moderate depression in which other studies had clearly demonstrated significant benefits from Saint-John’s-wort. Many experts felt that the entire study seemed as if the researchers were stacking the deck against Saint-John’s-wort. Interestingly, funding for the study came from the giant drug company Pfizer, the maker of Zoloft—the number one antidepressant drug at the time. Also interesting is that usually a study of this type would have compared the Saint-John’s-wort group and the placebo group with a third group taking a well-known antidepressant drug. The failure to include that third group indicated to many that the researchers knew that this patient group was not likely to respond to the antidepressant drug either.
Since then, there have been several double-blind studies of Saint-John’s-wort extract comparing it with standard SSRIs including Zoloft in mild to moderate depression.122,128,129 These studies have shown that Saint-John’s-wort is more effective and has fewer side effects. The message from all of this research is that for severe cases of depression, Saint-John’s-wort may not be strong enough. These patients may be better off focusing on cognitive therapy and other means to improve their mood.
In addition to human studies, GBE has also demonstrated antidepressant effects in a number of animal models. The most interesting of these studies demonstrated that GBE was able to counteract one of the major changes in brain chemistry associated with aging—the reduction in the number of serotonin receptor sites.135 Because of this reduction, the elderly are typically more susceptible to depression, impaired mental function, insomnia, and sleep disturbances. The study was designed to determine whether GBE could alter the number of serotonin receptors in old (24-month-old) and young (4-month-old) rats. At the beginning of the study, the older rats had 22% fewer serotonin binding sites compared with the younger rats. The results of treatment with GBE for 21 consecutive days demonstrated that there was no change in receptor binding in young rats, but in the older rats there was a statistically significant increase (33%) in the number of serotonin binding sites. These results suggest that GBE may counteract at least some, if not all, of the age-dependent decline in serotonin binding sites in the aging human brain as well.
Saffron (Crocus sativus) is the world’s most expensive spice because the stigma (the portion of the flower used for cooking) must be hand-picked off the flower. To obtain one pound of saffron, at least 50,000 flowers are needed. Iran is the world’s largest producer of saffron and has been investing in research into its potential medicinal uses. In Persian traditional medicine, saffron is used for depression. Studies have shown that saffron is safe and effective for mild to moderate depression, and one study showed efficacy equal to Prozac.136,137 The petal of the saffron crocus is much less expensive than the stigma and has also recently been shown to be effective in the treatment of mild to moderate depression. In the first double-blind study, 40 patients with mild depression received 30 mg per day of extract of saffron petals or a placebo for 6 weeks.138 Results showed a significant reduction in depression with the saffron extract. In another study, 40 patients with mild to moderate depression were randomly assigned to receive saffron petal extract (15 mg morning and evening) or fluoxetine (Prozac, 10 mg morning and evening) in an eight-week study.139 At the end of trial, the saffron was found to be as effective as the drug.
Lavender (Lavender officinalis) has long been used by herbalists as a treatment for anxiety, nervous exhaustion, and depression. Recently, this historical use has been verified in a detailed double-blind clinical trial.140 The findings of the study indicated that taking a moderate amount of lavender can reduce feelings of depression, anxiety, and helplessness. In the study, 45 adults between the ages of 18 and 54 who were diagnosed with depression were assigned to one of three groups. The groups received either (1) lavender extract plus a placebo tablet, (2) a placebo extract plus 100 mg per day of the antidepressant drug imipramine, or (3) lavender extract and 100 mg per day of imipramine. The study lasted for four weeks, and scores on a depression rating scale were evaluated initially and then weekly after the start of treatment. What the results indicated was that the lavender extract was just as effective as the drug, but lavender was without the side effects common in drug treatment for depression (dry mouth, weight loss or weight gain, low blood pressure, arrhythmias, and decreased sexual function).
![]()
QUICK REVIEW
• Approximately 17 million Americans suffer true clinical depression each year and over 28 million Americans take antidepressant drugs or anxiety medications.
• One of the most powerful techniques to produce the necessary biochemical changes in the brain of depressed individuals is teaching them to be more optimistic.
• Low levels of serotonin contribute to depression.
• It is important to rule out the simple organic factors that are known to contribute to the depression, i.e., nutrient deficiency or excess, drugs (prescription, illicit, alcohol, caffeine, nicotine, etc.), hypoglycemia, consumption, hormonal derangement, allergy, environmental factors, and microbial factors.
• Cognitive therapy has been shown to be as effective as antidepressant drugs in treating moderate depression.
• Depression is often a first or early manifestation of thyroid disease.
• Increased cortisol levels are common in depression.
• Elimination of sugar and caffeine has been shown to produce significant benefits in clinical trials.
• Increased participation in exercise, sports, and physical activities is strongly associated with decreased symptoms of anxiety, depression, and malaise.
• A deficiency of any single nutrient can alter brain function and lead to depression, anxiety, and other mental disorders.
• Hypoglycemia can cause depression.
• An insufficiency of omega-3 oils in the diet has been linked to depression.
• Several double-blind studies have shown 5-hydroxytryptophan (5-HTP) to be as effective as antidepressant drugs but better tolerated and associated with fewer and much milder side effects.
• Extracts of Saint-John’s-wort standardized for hypericin (usually 0.3%) are the most thoroughly researched natural antidepressants.
• Over 25 double-blind studies have shown Saint-John’s-wort to produce equally good or better results compared with standard antidepressant drugs, but with signficantly fewer side effects.
![]()
TREATMENT SUMMARY
Treatment of depression is largely dependent on a few central elements: balancing of errant neurotransmitter levels and optimizing nutrition, lifestyle, and psychological health.
If you wish to discontinue any antidepressant drug, we recommend that you work with your physician on this goal. In general, discontinuing a SSRI has to be done gradually. Stopping too quickly is associated with symptoms such as dizziness, loss of coordination, fatigue, tingling, burning, blurred vision, insomnia, and vivid dreams. Less often, there may be nausea or diarrhea, flu-like symptoms, irritability, anxiety, and crying spells.
To help support patients as they wean themselves off SSRIs, either 5-HTP or Saint-John’s-wort extract can be used. A concern when antidepressant drugs are mixed with Saint-John’s-wort or 5-HTP is producing what is referred to as “serotonin syndrome,” characterized by confusion, fever, shivering, sweating, diarrhea, and muscle spasms. Although it is theoretically possible that combining Saint-John’s-wort or 5-HTP with standard antidepressant drugs could produce this syndrome, to our knowledge no one has experienced this syndrome with simultaneous use of Saint-John’s-wort extract or 5-HTP and an SSRI. Nonetheless, our recommendation is that when using Saint-John’s-wort or 5-HTP in combination with standard antidepressant drugs, you should be closely monitored by your doctor for any symptoms suggestive of the serotonin syndrome. If these symptoms appear, elimination of one of the therapies is indicated.
In mild cases of depression, we recommend using either 5-HTP (50 mg per day) or Saint-John’s-wort extract (900 mg per day) while you work with your doctor to reduce the drug to half the daily dosage for two to four weeks. After four weeks, the drug can be discontinued. For more severe cases, keep the dosage of the antidepressant as it is and add the Saint-John’s-wort extract. Evaluate at the end of one month and begin tapering off the drug if sufficient mood-elevating effects have been noted. If additional support is necessary, add 5-HTP at a dosage of 50 mg three times per day.
Individuals with depression should consider seeing a psychotherapist for help in developing a positive, optimistic attitude. This can be accomplished by helping them set goals, use positive self-talk and affirmations, identify self-empowering questions, and find ways to inject humor and laughter into their lives. For more information, see the chapter “A Positive Mental Attitude.”
The recommendations in the chapter “A Health-Promoting Diet” are important in depression. It is very important to eat a low-glycemic Mediterranean-style diet, increase consumption of fiber-rich plant foods (fruits, vegetables, grains, legumes, and raw nuts and seeds), and avoid caffeine and alcohol. Food allergies must be identified and controlled (see the chapter “Food Allergy”).
• Exercise at least 30 minutes at least three times a week, but preferably every day.
• Spend 10 to 15 minutes per day on relaxation/stress reduction techniques.
• Follow the recommendations in the chapter “A Positive Mental Attitude.”
• A high-potency multiple vitamin and mineral formula as described in the chapter “Supplementary Measures”
• Key individual nutrients:
![]() Vitamin B6: 25 to 50 mg per day
Vitamin B6: 25 to 50 mg per day
![]() Folic acid: 800 mcg to 2,000 mcg per day
Folic acid: 800 mcg to 2,000 mcg per day
![]() Vitamin B12: 800 mcg per day
Vitamin B12: 800 mcg per day
![]() Vitamin C: 500 to 1,000 mg per day
Vitamin C: 500 to 1,000 mg per day
![]() Magnesium (bound to aspartate, citrate, fumarate, malate, or succinate): 150 to 250 mg two times per day
Magnesium (bound to aspartate, citrate, fumarate, malate, or succinate): 150 to 250 mg two times per day
![]() Vitamin D3: 2,000 to 4,000 IU per day (ideally, measure blood levels and adjust dosage accordingly)
Vitamin D3: 2,000 to 4,000 IU per day (ideally, measure blood levels and adjust dosage accordingly)
• Fish oils: 1,000 mg EPA + DHA per day
• One of the following:
![]() Grape seed extract (>95% procyanidolic oligomers): 100 to 300 mg per day
Grape seed extract (>95% procyanidolic oligomers): 100 to 300 mg per day
![]() Pine bark extract (>95% procyanidolic oligomers): 100 to 300 mg per day
Pine bark extract (>95% procyanidolic oligomers): 100 to 300 mg per day
![]() Some other flavonoid-rich extract with a similar flavonoid content, super greens formula, or another plant-based antioxidant that can provide an oxygen radical absorption capacity (ORAC) of 3,000 to 6,000 units or higher per day
Some other flavonoid-rich extract with a similar flavonoid content, super greens formula, or another plant-based antioxidant that can provide an oxygen radical absorption capacity (ORAC) of 3,000 to 6,000 units or higher per day
• Consider one of the following:
![]() 5-HTP: 50 to mg three times per day
5-HTP: 50 to mg three times per day
![]() SAM-e: 200 mg twice a day up to 400 mg three times a day
SAM-e: 200 mg twice a day up to 400 mg three times a day
• One of the following:
![]() Saint-John’s-wort extract (0.3% hypericin content): 900 to 1,800 mg per day (probably the best choice for people younger than 50); in severe cases, can be used in combination with 5-HTP 50 to 100 mg three times per day
Saint-John’s-wort extract (0.3% hypericin content): 900 to 1,800 mg per day (probably the best choice for people younger than 50); in severe cases, can be used in combination with 5-HTP 50 to 100 mg three times per day
![]() Ginkgo biloba extract (24% ginkgo flavonglycosides content): 240 to 320 mg per day (perhaps the best choice for people older than 50); in severe cases, can be used in combination with Saint-John’s-wort, 5-HTP, or both
Ginkgo biloba extract (24% ginkgo flavonglycosides content): 240 to 320 mg per day (perhaps the best choice for people older than 50); in severe cases, can be used in combination with Saint-John’s-wort, 5-HTP, or both
![]() Saffron petal extract: 15 mg twice per day
Saffron petal extract: 15 mg twice per day
![]() Lavender extract (4:1): 150 mg twice per day
Lavender extract (4:1): 150 mg twice per day