In Chapter 1, in addition to head and neck soft tissue examination techniques, there is information about overall screening and diagnosis adjunct options as well detailed information about some diagnostic adjunctive procedures such as chemiluminescent reflectance and narrowband autofluorescence. This chapter provides detailed information about oral mucosal cytology and biopsy indications. The surgical biopsy remains the current gold standard of tissue diagnosis.
Oral Mucosal Cytology Indications and Contraindications
Oral mucosal cytology is a screening procedure unique and different from uterine cervical cytology screening (i.e., traditional Pap smear or liquid cytology Pap smear with or without HPV testing). The uterine cervix and oral/oropharyngeal mucosa are composed of similar stratified squamous epithelial cells; however, the biologic nature and behavior of the cells differ because of a substantially different physiological milieu. This is an important point to keep in mind, particularly with indication criteria, microscopic interpretation, and future management considerations.
Studies in the 1960s and 1970s confirmed routine Pap smears of the oral cavity had too many false positives and negatives. We acknowledge the improved sampling of oral cavity epithelial cells with the late 1990s Oral CDx brush biopsy cytobrush (described in Chapter 1) and some investigators reported improved specificity, sensitivity, and positive predictive value compared with conventional cytology. In addition, after reading encouraging results of liquid-based cytology results from uterine cervix studies, one of us (MAK) concluded that methodology could be useful for oral cytology specimens. Currently, the cytology method we support combines the advantages of a nylon-bristle cell collection device with liquid fixative for chairside cell transfer and immersion, transport, and slide preparation.
The following oral cytology indications and contraindications are based on our use of a liquid-based cytology process. It is important to remember the indications for cytology screening of the oral and oropharyngeal mucosa are very limited. Unlike the original Oral CDx brush biopsy's indication of “nonsuspicious” oral “red or white spots” we recommend the indication should be for lesions suspicious for squamous cell carcinoma (e.g., unexplained nonhealing ulcer, erythroplakia, or speckled leukoplakia), especially when occurring in high-risk oral mucosal sites and the patient refuses or is unable to undergo a surgical biopsy. It should be emphasized that we consider the brush biopsy a form of cytology since architectural intact tissue from the surface and underlying connective tissue is not obtained. Additionally, leukoplakias should be investigated in a similar manner; however, it is more difficult to harvest deeper level keratinocytes due to the variable thickened keratin layer. In addition, indications include two infectious diseases: herpes simplex and candidiasis. Candidiasis can be diagnosed by cytology because the surface epithelial cells are associated with superficially embedded spores and/or hyphae of Candida albicans. Herpes simplex infection (primary or recurrent) can be diagnosed with cytology by sampling an intact vesicle or the peripheral area of a ruptured one (i.e., erosion or ulceration), which possesses infected keratinocytes. Epithelial cells infected with Herpesviridae exhibit microscopic pathognomonic morphological changes that, when combined with the viral infection's clinical signs and symptoms, can result in an accurate diagnosis.
Leukoplakias and erythroplakias can have variable amounts of epithelial dysplasia involving the thickness of the surface epithelium or just benign cellular atypia secondary to mucosal inflammation within the epithelium (i.e., inflammatory exocytosis). It is imperative for the clinician to understand that the histological interpretation of an oral cytology sample of a leukoplakia or erythroplakia is limited to stating whether abnormal cellular changes are present or not. Thus, the cytology procedure does not confirm the presence or absence of epithelial dysplasia; dysplasia is a subjective microscopic diagnosis that requires architecturally intact stratified squamous epithelium (i.e., surgical biopsy) so that the width of dysplasia within the epithelium can be determined. In a cytology procedure, conventional or liquid technique, the epithelial cells are disaggregated as individual cells and/or small clumps of cells; therefore, a pattern of disruption of the normal epithelial maturation process (i.e., dysplasia) cannot be appreciated. Any positive atypical cellular finding that is not due to herpes infection or candidiasis must undergo a diagnostic biopsy procedure.
It is also critical for the clinician to understand that cytology procedures are only able to examine epithelial cells and thus any pathology that exists within the lamina propria (i.e., the connective tissue and its elements below the epithelium's basement membrane) cannot be evaluated. The brush simply does not sample deeply enough to gather the pathological cells and/or substances. Examples of cytology sampling contraindications include amalgam tattoo, fibroma, mucocele, neuroma, and minor salivary gland tumors. Also, other specific epithelial proliferations such as squamous papilloma and verruca vulgaris cannot be diagnosed via cytology because they require the overall intact histological pattern and features only provided by surgical biopsy.
Cytology Technique Tips and Pitfalls
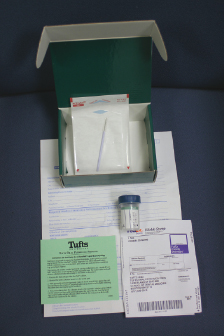
A suitable liquid cytology kit can be obtained from several oral pathology laboratories in the United States (Fig. 6.1). The free kit will typically be enclosed in a corrugated box or shipping tube that includes a specimen bottle filled with 10 mL of alcohol-based fixative (e.g., ThinPrep® or SurePath® brands), cytobrush (e.g., Medscand's Cytobrush Plus®), requisition form, small plastic bag, and a prepaid overnight mailer and outer shipping bag. The requisition form is filled out completely with patient, doctor, and lesion information (details of the latter are discussed in the biopsy section, “Scalpel Biopsy Dos and Don'ts”).
Figure 6.1 A typical available liquid cytology kit composed of instructions, requisition form, prepaid overnight mailer and shipping container, alcohol-based transport/fixative media container, and sterile nylon or plastic bristle collection device.
It is very important to obtain an adequate harvest of keratinocytes from all levels of the oral mucosa's stratified squamous epithelium. Whether the cytobrush selected has soft or firm bristles, the clinician must apply enough downward and back-and-forth force to obtain a transepithelial specimen. Once the harvested area demonstrates pinpoint bleeding, then the clinician has clinical verification of adequate depth since the vasculature resides only within the lamina propria below the basement membrane zone. As soon as the cells have been harvested it is crucial that they are immediately immersed in the liquid fixative container so that the cell sample does not air dry and destroy cellular detail. With the bristles of the brush immersed, the handle/shaft of the brush should be vigorously twirled with the fingers to agitate harvested cells off the bristles and into the liquid fixative. To retain as many harvested cells as possible for processing and analysis, the handle/shaft is cut off and the brush's bristles are left within the specimen container for use during specimen processing. The cap of the fixative container is secured and the container is placed in the provided small plastic bag. The plastic bag is placed in the corrugated box or tube, and lastly the box or tube is placed in the overnight delivery service shipping bag with the prepaid mailing label affixed on its surface.
Biopsy Indication and Contraindications
Biopsy of oral and oropharyngeal tissues is the gold standard for diagnosis and is defined as the removal for diagnostic study of a piece of tissue from a living body. It has been used for more than 150 years to establish the diagnosis of an unknown medical condition and is the oldest and most reliable method currently available that can establish the definitive diagnosis of a clinical abnormality in dentistry. The practice of modern dentistry requires evidence-based treatment decisions and therapeutic outcomes, and an accurate diagnosis is the most basic step to initial treatment. Recently, the American Academy of Oral and Maxillofacial Pathology (AAOMP), the American Association of Endodontists, and the American Association of Oral and Maxillofacial Surgeons endorsed tissue biopsy as the paramount procedure in order to obtain a definitive diagnosis of a discovered soft tissue lesion. This maxim is equally applicable to general dentists and dental specialists who elect to remove abnormal tissue in the course of patient care.
The biopsy procedure is well within the scope of training and ability for a general dentist; however, each must determine their comfort level and refer patients to those with more biopsy experience when appropriate. No matter who performs the biopsy procedure, the determination of when it is performed is most important. It is the professional obligation of the dentist to inform the patient in need of a biopsy and attempt to gain patient acceptance. A patient may be reluctant to undergo a biopsy for fear that it is only used to test for cancer and/or that common oral conditions do not require biopsy verification because the clinical judgment and experience of the clinician is sufficient. Although it is correct that a cancer diagnosis typically is based on a biopsy finding, the reason for the procedure is to obtain a definitive diagnosis since clinical findings are usually insufficient and cancer is just one of hundreds of possible diagnoses that can be made from biopsy tissue examination. For both the clinician and the patient, it can be a catastrophic result for the clinician to base the final diagnosis on a single clinical working diagnosis rather than formulate a differential diagnosis and then perform the biopsy to determine the definitive diagnosis.
The biopsy is not a substitute for thoughtful evaluation of the patient's condition—the clinician should initially develop a differential diagnosis and then perform the biopsy. When the biopsy tissue specimen is submitted, the clinician should include a differential diagnosis to aid the pathologist in his or her thought processes. In approximately 80–90% of cases, the pathologic diagnosis of the biopsy specimen will be consistent with the clinical diagnosis but, if not, the dentist should contact the oral pathologist to ensure that a laboratory error has not occurred. A timely and accurate final diagnosis is beneficial for both the clinician and the patient whether in agreement or not with the clinical diagnosis. Benefits include increased clinical confidence in diagnostic skills, increased patient respect, and satisfaction that treatment performed was appropriate. The final written diagnosis usually brings closure to the clinical situation.
The two types of biopsy most commonly performed in order to obtain a definitive diagnosis are incisional and excisional. An excisional biopsy is a surgical procedure that removes the entire lesion for microscopic examination; conversely, an incisional biopsy is a surgical procedure that removes a portion of the lesion for microscopic examination. An excisional biopsy is performed when the lesion is relatively small and its clinical working diagnosis is thought to be benign; it can also be used to ensure that a previously diagnosed lesion has been removed completely. Other factors that are considered when deciding which type of surgical biopsy to perform include the lesion's site and the clinician's experience and comfort level. These are the same factors that determine whether the dentist performs the biopsy or refers to a specialist. Certainly, it is perfectly acceptable for a clinician to elect not to perform the biopsy in his or her practice but it is, likewise, totally unacceptable to ignore that a biopsy needs to be performed.
Scalpel Biopsy Dos and Don'ts
The specific site for an excisional biopsy is not a concern, but when an incisional biopsy is to be performed it is usually important that a portion of normal adjacent tissue is also included (i.e., perilesional). By including at least a small portion of normal mucosa the oral pathologist is aided in interpreting the microscopic features of the disease. If the lesion is very large, then multiple incisional biopsies should be performed; each biopsy should be placed in a separate 10% formalin container or, alternatively, each specimen can be differentiated within a single container by placing sutures of different length or composition. Sutures can also be used to denote a particular margin of a specimen so the oral pathologist can accurately orient the specimen during accessioning and gross preparation prior to tissue processing. When microscopic information about the lesional margins is requested by the submitting clinician, it is also helpful to include a diagram of the biopsy specimen that denotes the sutures and margins (e.g., anterior, posterior, distal).
Unless medically contraindicated, when applying local anesthetic to the area of the planned biopsy, it is advantageous to use a type with epinephrine to aid in capillary constriction prior to incising the tissue. The local anesthetic of choice is deposited adjacent to the lesion but never directly into the affected tissues. If the latter is done, then it creates significant artifactual change of the tissue, and the biopsy specimen is often not diagnosable under light microscopy.
The basic shape of the biopsy specimen, from above, should appear elliptical and, in cross-section, should appear V-shaped. By obtaining this three-dimensional conformation the biopsy tissue flaps area can be easily sutured without creating tension. This will promote the most ideal healing by primary intention and will avoid or minimize secondary healing by the slower process of extensive granulation tissue fill-in.
It is critical, particularly for an incisional biopsy, that enough tissue in length, width, and depth is obtained so that selection bias does not compromise the biopsy's microscopic interpretation due to insufficient yield. A very small tissue sample also can be lost during tissue processing or can make tissue embedding and sectioning very difficult.
If the provisional clinical diagnosis includes a condition for which the patient is taking systemic or topical medication, the treatment should cease several days before the biopsy procedure in order to avoid a “masking” therapeutic effect, unless the risk of medication cessation outweighs the benefit of avoiding sampling bias. The area to be biopsied should not be cleaned with colored antiseptics or similar materials prior to biopsy, although toluidine blue does not interfere with the tissue staining process.
The most frequent pathology morphology seen within the oral cavity is an ulcer. It is important that, when an ulcer is biopsied, both its margins and adjacent normal tissue are included so that the submitted specimen does not consist solely of the ulcer's bed of granulation tissue and overlying inflammation, necrotic debris, and fibrinopurulent membrane. If the tissue biopsied is part of a sloughing-type disease (e.g., mucous membrane pemphigoid), then a suture can be passed through the sloughed area into the underlying connective tissue and out through a nonsloughed area. The specimen obtained may be placed in the formalin container with the suture still attached. In fact, depending on the biopsy site, it is often advisable to place a traction suture in the lesion prior to removal so that, when the suture is gently pulled by the assistant, the incising of the tissue is facilitated. Furthermore, the traction suture can prevent an accidental loss of the tissue by the suction device.
Most clinicians continue to biopsy with a sharp, sterile, stainless steel surgical blade, typically a #15; however, a laser is an acceptable device if the clinician determines its proper settings. If the settings are too high, then it can cause significant thermal artifactual change that renders some or all of the biopsied tissue undiagnosable. Therefore, if a laser is used, the margins of the specimen should be larger than the biopsy site of interest; this is particularly true if the purpose of the biopsy is to confirm the lack of dysplasia at the epithelium's lateral or inferior margins.
During the biopsy procedure, and particularly once the tissue has been freed from the surgical bed, it should be handled very gently so that, for example, tissue forceps do not leave a damaging crush artifact within the tissue. It is helpful to place the removed tissue on a sheet of paper, connective-tissue side down, prior to immersion in the formalin container. This step helps prevent the biopsied tissue from curling into the shape of a ball during transport, which could hinder the oral pathologist performing the subsequent orientation of the specimen during its accession and grossing.
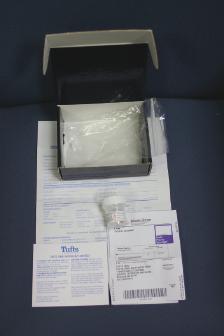
It is critical that the clinician and pathologist work as a team to minimize potential errors during the multistep biopsy diagnostic process. The biopsy tissue is immediately immersed in a container of 10% formalin to avoid tissue autolysis. The container's label must have the patient's and doctor's names as well as the site and date of the biopsy. State law requires the patient's name on the specimen container and a pathology lab is legally obligated to return an unlabeled specimen. A dentist should always have enough formalin containers on hand since oral pathology laboratories supply them free of charge (Fig. 6.2). If the formalin in the container has evaporated so that only powder remains, the dentist should dispose of the bottle rather than attempt rehydration. Alcohol is a poor second choice as an intact tissue fixative but it can be used in an emergency. Tap or distilled water should never be used as a fixative since it will destroy the tissue by hydrolysis and, thus, render it useless for microscopic evaluation. Following the biopsy, pressure with gauze should be applied to promote clotting. The surgical bed should be carefully inspected to ensure that no foreign body material has been left that will delay or compromise healing.
Figure 6.2 A typical available biopsy kit composed of instructions, requisition form, prepaid overnight mailer and shipping container, and 10% neutral buffered formalin container.
As the health-care professional, it is the dentist's responsibility to ensure that the fixative container's label and requisition forms are filled out in their entirety. The patient demographic information and billing information must be included as well as dental office contact information. The clinician must use his or her oral pathology knowledge to accurately describe the lesion as well as to provide a suitable differential diagnosis. Pertinent medical, dental, and social histories should also be included. After the biopsy specimen has been securely packaged appropriately within the oral pathology laboratory's kit, the clinician should verify the office's return address is on the shipping label whether or not a shipping company's bar code and tracking number are present.
Oral pathology laboratories attempt to provide accurate diagnoses in the minimum amount of time. If the diagnosis of the pathology report does not correlate substantially with the clinical situation, it is the clinician's responsibility to investigate. Call and speak to the oral pathologist and express your concerns. The oral pathologist will verify the accuracy of the diagnosis or make the necessary changes.
Punch Biopsy Dos and Don'ts
The punch biopsy is a popular and convenient method used by dermatologists for skin biopsies and it is also suitable for performing small surgical biopsies of the oral mucosa. Typically, the punch instrument is a disposable, single-use device that makes a circular cut. The handle/shaft is plastic with a widened hub that extends into a very sharp, circular, surgical steel blade. The punch can be purchased from several medical and dental supply vendors and typically comes in color-coded diameters ranging from 2 to 8 mm. A popular punch size for an incisional biopsy is 4 mm, but a smaller lesion can be totally excised by using a larger diameter punch.
The punch procedure begins with a small amount of local anesthetic deposited adjacent to the lesion. Then the biopsy punch is held vertically above the lesion and is precisely and firmly pushed down into the tissue and simultaneously rotated clockwise or counterclockwise. The tissue to be biopsied is finger supported if it is not supported by bone; in the case of the tongue, firmly grasp it with gauze to immobilize the punch biopsy site. Usually the plastic hub is approximately 6 mm from the edge of the circular blade and thus the incising depth can be controlled. Once the tissue has been incised, the punch is removed, leaving a visible rim of blood that is confirmation of adequate depth into the lamina propria's superficial capillaries. The clinician should then gently hold the still attached specimen with tissue forceps and carefully free its base by gently pulling up along its long axis and simultaneously cutting the base with a pair of small, curved iris scissors or a surgical blade. Once the specimen has been freed it should be placed, connective-tissue side down, on a small piece of paper and immersed in a 10% formalin container with its cap subsequently replaced and retightened. As with a scalpel biopsy, direct pressure should be applied with surgical gauze until clotting occurs; a topical coagulant can be used for any persistent hemorrhage. Unlike a scalpel biopsy, no sutures can be placed in the circular (nonelliptical) surgical wound and it will heal entirely by granulation tissue formation; alternatively, some clinicians opt to place sutures to encourage faster healing. A small drop of clear cyanoacrylate resin (Dermabond®) can be placed on top of the wound to keep it clean while healing occurs.
The rest of the punch procedure is identical to a scalpel biopsy with regard to container labeling and requisition form completion. Also, the same standard patient instructions are given—to avoid injury to the biopsy site from food or toothbrush, gently rinse with warm salt water several times a day, and use nonsteroidal anti-inflammatory medications (NSAIDs) to relieve postoperative pain.
The AAOMP has stated that the routine submission of abnormal tissue to an oral pathologist for diagnosis is a vital link in the development of truly evidence-based clinical practice. It is not a panacea for protection against claims of malpractice, but its timely and routine use will likely substantially reduce the success rate of claims.
Recommended Reading
Afrogheh A, Wright CA, Sellars SL. An evaluation of the Shandon Papspin liquid-based oral test using a novel cytologic scoring system. Oral Surg Oral Med Oral Pathol Oral Radiol 2012;113:799–807.
Lorenzato M, Bory JP, Cucherousset J, et al. Usefulness of DNA ploidy measurement on liquid-based smears showing conflicting results between cytology and high-risk human papillomavirus typing. Available at: http://www.ajcp.com/volume_118/issue_5/202176.html (accessed April 17, 2008).
Magro CM, Robets-Barnes J, Crowson AN. Direct immunofluorescence testing the diagnosis of immunobullous disease, collagen vascular disease, and vascular injury syndromes. Dermatol Clin 2012;30:763–798.
Poh CF, Ng S, Berean KW, Williams PM, Rosin MP, Zhang L. Biopsy and histopathologic diagnosis of oral and premalignant and malignant lesions. JCDA 2008;74:283–288.
Wood NK, Goaz PW. Differential Diagnosis of Oral and Maxillofacial Lesions, 5th edition. St. Louis, MO: Mosby; 1997.